Back to Journals » Journal of Asthma and Allergy » Volume 15
Study on the Relationship Between Bronchoalveolar Lavage Fluid Cell Count, Th1/Th2 Cytokines and Pulmonary Function in Patients with Cough Variant Asthma
Authors Chen J, Lin W, Gu H, Ying K, Li T, Shao H
Received 26 July 2022
Accepted for publication 6 November 2022
Published 24 November 2022 Volume 2022:15 Pages 1713—1720
DOI https://doi.org/10.2147/JAA.S383128
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Junfeng Chen,* Wei Lin,* Haiting Gu, Kangtai Ying, Tingjian Li, Haiyan Shao
Department of Respiration, The First People’s Hospital of Wenling, Wenling, Zhejiang, 317500, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haiyan Shao, Department of Respiration, The First People’s Hospital of Wenling, 333 Chuanan Nan Road, Chengxi Street, Wenling, Zhejiang, 317500, People’s Republic of China, Tel +86 057689668688, Email [email protected]
Objective: This study aimed to compare lung function and airway inflammation among cough variant asthma (CVA), chronic cough and classical asthma (CA) and investigate the relationship between these indicators and their possible mechanisms of action in the progression of CVA to CA.
Methods: 36 patients with chronic cough, 39 patients with CA, and 57 patients with CVA were included in this study. Pulmonary function tests, bronchial provocation tests and FeNO tests were performed. The patients’ bronchoalveolar lavage fluid (BALF) was collected, the cells in BALF were counted, and the levels of Th1 and Th2 cytokines were detected.
Results: The neutrophils, lymphocytes, and eosinophils in BALF in the CA and CVA groups were significantly higher than those in the chronic cough group. Also, they were negatively correlated with FEV1, FVC, and FEV1/FVC and positively correlated with IgE and FeNO. The expression of Th2-related cytokines was increased in CVA and CA patients, and it was positively correlated with FEV1, FVC and FEV1/FVC and negatively correlated with IgE and FeNO, while the results of Th1-related cytokines were the opposite of those for Th2-related cytokines.
Conclusion: CVA differs from asthma and chronic cough in terms of Th1/Th2 cytokines and lung function and provides a reference for understanding the disease mechanism of early clinical progression of CVA to CA.
Keywords: cough variant asthma, cytokines, pulmonary function, Th1/Th2 balance, cell classified count
Introduction
Chronic cough is defined as a disabling complaint affecting 5~10% of the general population,1 and about 33.3% of chronic cough cases are caused by cough variant asthma (CVA), a specific and atypical asthma phenotype.2,3 CVA is characterized by an irritating cough at night or early in the morning, which will affect the quality of life of patients. According to a previous study, around 30~40% of CVA patients will develop classic asthma (CA).4 However, CVA is easily overlooked and misdiagnosed clinically because, unlike CA patients who present with wheezing, its patients present with only cough. More importantly, the mechanism of evolution from CVA to CA has not been fully elucidated. Thus, studying CVA is helpful to better understand the pathogenesis of asthma, improve the quality of life for CVA sufferers, avoid further development of CA, and preserve lung function.
The pathogenesis of CVA is the same as that of CA and is mostly associated with chronic inflammation in the airway, often mediated by a variety of inflammatory factors.3,5 Studies indicated that there is an imbalance of helper T cell 1 (Th1) / Th2 in CAV, which manifests as an immune response dominated by Th2.6 Th2-related cytokines can induce the release of inflammatory mediators and lead to local airway inflammatory cell infiltration. Th2 cells can secrete various inflammatory factors, including interleukin-4 (IL-4), IL-5, IL-13 and IL-25.7 This continuous infiltration of inflammatory factors increases airway sensitivity and leads to asthma attacks. Interferon-γ (IFN-γ) is an important cytokine secreted by Th1 cells, which interacts or restricts with Th2-related cytokines in the occurrence and development of asthma to jointly regulate the synthesis and conversion of immunoglobulin E (IgE).8 Earlier research found that the serum levels of IL-4, IL-5, IL-6 and IL-13 were significantly increased in CVA patients and can be used as an indicator of the extent of the disease.9 Additionally, CVA patients have less severe airway inflammation than CA patients.10 Thus, Th1/Th2-associated cytokines have clinical significance in the diagnosis of early CVA and may avoid misdiagnosis and missed diagnosis to better understand the progression of the disease.
Taken together, for the diagnosis, treatment, and prognosis of CVA, the level of inflammatory factors in the body of patients is of great relevance. In this study, we detected the classified count of cells and the levels of Th1 and Th2 cytokines in bronchoalveolar lavage fluid (BALF) of patients with a chronic cough in our hospital to investigate the possible mechanisms of these factors in the evolution from CVA to CA and to provide a theoretical basis for the disease progression and treatment of CVA.
Materials and Methods
Participants
Patients with asthma and chronic cough who were first diagnosed in our hospital from April 2020 to October 2021 were selected, with 57 in the CVA group, 36 with non-CVA chronic cough patients in the cough group, and 39 in the asthma group.
Inclusion criteria: patients with chronic cough meet the diagnostic criteria of the Chinese Guidelines for Diagnosis and Management of Cough (2015)11 and the CA and CVA diagnosis meets the requirements of the 2018 Global Initiative for Asthma (GINA) Guidelines of Asthma Management and Prevention12 the Chinese Guidelines for Diagnosis and Management of Cough (2015).11 CVA was diagnosed with a cough but without wheezing for more than 8 weeks and the presence of bronchial hyperresponsiveness (BHR, stimulating concentrations of acetylcholine resulting in a 20% decrease in FEV1 (PC20) at excitation, (PC20) below 16 mg/mL); patients older than 18 years. All patients had no anti-asthma treatment, including oral or inhaled corticosteroids, leukotriene receptor antagonists, or antihistamines within the last 4 weeks.
Exclusion criteria: patients with coexisting pulmonary tuberculosis, diabetes as well as heart, brain, liver, kidney or blood system and other serious primary diseases; patients with mental illness and obvious cognitive impairment; those who have poor compliance for inspection and intolerance in cooperation.
This study was conducted according to the Helsinki Declaration and approved by the Ethics Committee of Wenling first people’s Hospital.
Study Procedures
The operation of the bronchoalveolar lavage method was strictly in accordance with the draft technical specification for cytological detection of bronchoalveolar lavage fluid issued by the Respiratory Branch of the Chinese Medical Association. All patients underwent routine examinations, such as blood routine, coagulation function, electrocardiogram, hepatitis B surface antigen, chest CT and lung function, and underwent bronchoscopy in the morning with an empty stomach. Half an hour before the operation, 4 mg of alprazolam was given orally, followed by a 2% lidocaine hydrochloride (Shanghai Zhaohui Pharmaceutical H31021072) injection sprayed into the oropharynx and bilateral nasal cavities of patients 3 times. Ten minutes later, 2% lidocaine was used for cricothyroid membrane puncture anesthesia, and the bronchoscope was inserted through the nasal cavity following the patient had numbness in the mouth and tongue. After routine examination, 1~2 mL of 2% lidocaine was applied to anesthetize the bronchi to be lavaged, the bronchoscope was incarcerated and fixed in the bronchus of the middle lobe of the right lung. Then, the total amount of sterilized saline at 37 ℃ was quickly injected in several fractions through the operating channel and the recovered lavage solution was immediately absorbed with appropriate negative pressure. A total recovery rate of ≥ 30% was appropriated and the recovered lavage fluid was immediately sent for testing. After BALF was centrifuged at 1500 r/min for 10 min, the supernatant was stored in a refrigerator at −80℃ for determination. The cell suspension was prepared by suspending cell precipitation with 3–5 mL 0.9% sodium chloride injection, and the total number of cells was then calculated with the counting board. If the number of cells is too high, it can be diluted and adjusted to 5 × 106/mL with 0.9% sodium chloride injection. The 50 μL of fully suspended cell suspension was dripped on a slide, which was dried in cold air and stained with hematoxylin-eosin staining (HE) by two technically competent inspectors. For each sample, the examiners counted 200 cells under the light microscope and classified the cells.
IFN-γ secreted by Th1 cells and interleukin 4 (IL-4), IL-5, IL-13, IL-18, and IL-25 secreted by Th2 cells in the supernatant of BALF were detected using enzyme-linked immunosorbent assay (ELISA). The kit was purchased from Shanghai Tuojing Life Technology Co., Ltd.
Statistical Analysis
All the statistical variables were conducted with SPSS version 20 (IBM Corporation, Armonk, NY, USA). Enumeration data were expressed as cases (percentages) and analyzed using the chi-square test. The measurement data were analyzed by the Kolmogorov-Smimov test, those that do not conform to the normal distribution were expressed as M (P25, P75). The Kruskal–Wallis test was applied in the comparison of the three groups due to the variability of the sample size and the non-normal distribution of the samples, and Spearman correlation analysis was utilized to analyze the correlation between two variables. The correlation coefficient R represents the strength of the correlation and the value range was [−1, +1], the closer the value is to −1 or +1, the stronger the correlation. A negative number represents a negative correlation, a positive number represents a positive correlation, and 0 means no correlation. According to the test level, P < 0.05 was considered a statistically significant difference.
Results
A total of 132 patients with CVA (n=57), CA (n=39), and non-CVA chronic cough (n=36) were included in the study (Table 1). There was no significant difference in sex and age between the three groups (P > 0.05), while in IgE and pulmonary function indexes (FEV1, FVC, FEV1/FVC ratio, and FeNO), there were significant differences among them (P < 0.05).
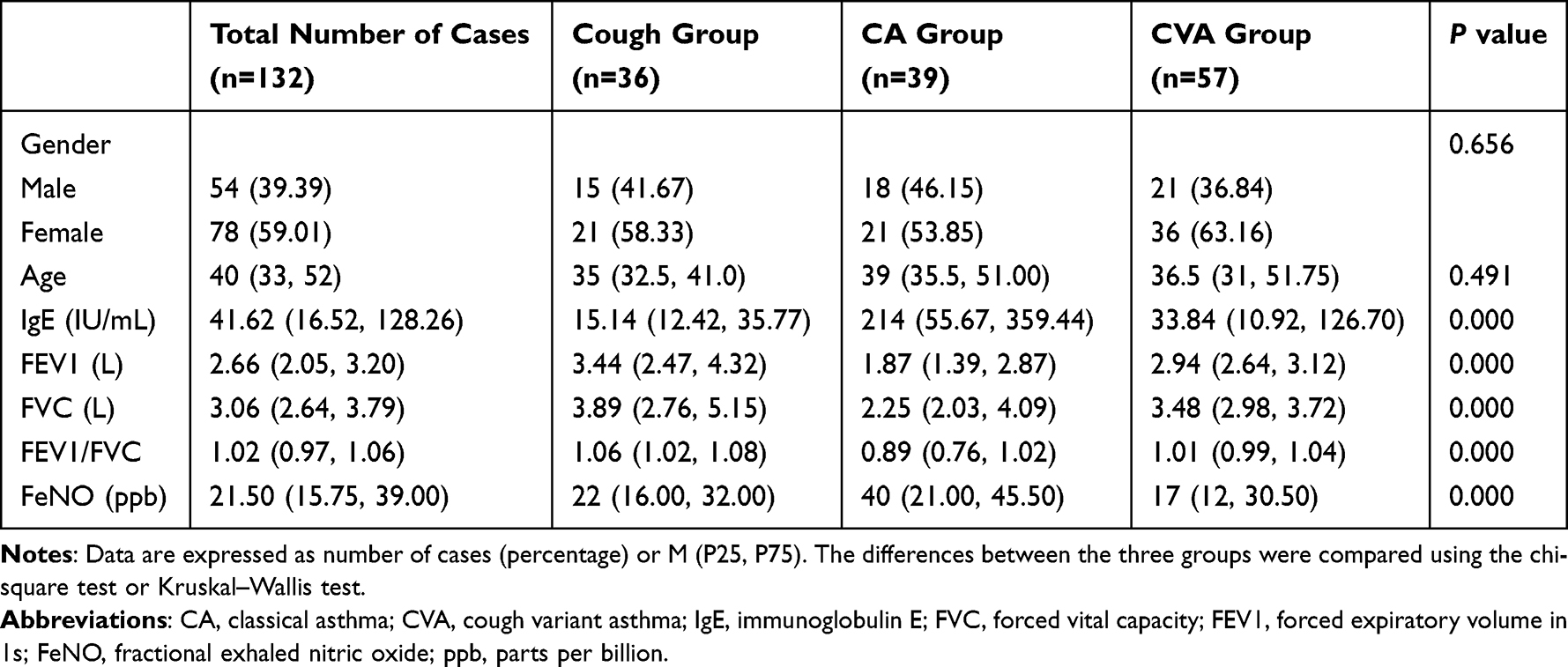 |
Table 1 Baseline Table: Comparison of Three Groups of Basic Information |
Differential cells in bronchoalveolar lavage fluid were counted. As shown in Figure 1, the number of neutrophils, lymphocytes, and eosinophils in the CA and CVA groups were significantly higher than those in the chronic cough group (P < 0.05), and those in the CA group were higher than that in the CVA group (P < 0.05). Additionally, the macrophage count in the CA and CVA groups was prominently lower than that in the chronic cough group, while the CA group had a higher macrophage count than the CVA group (P < 0.05).
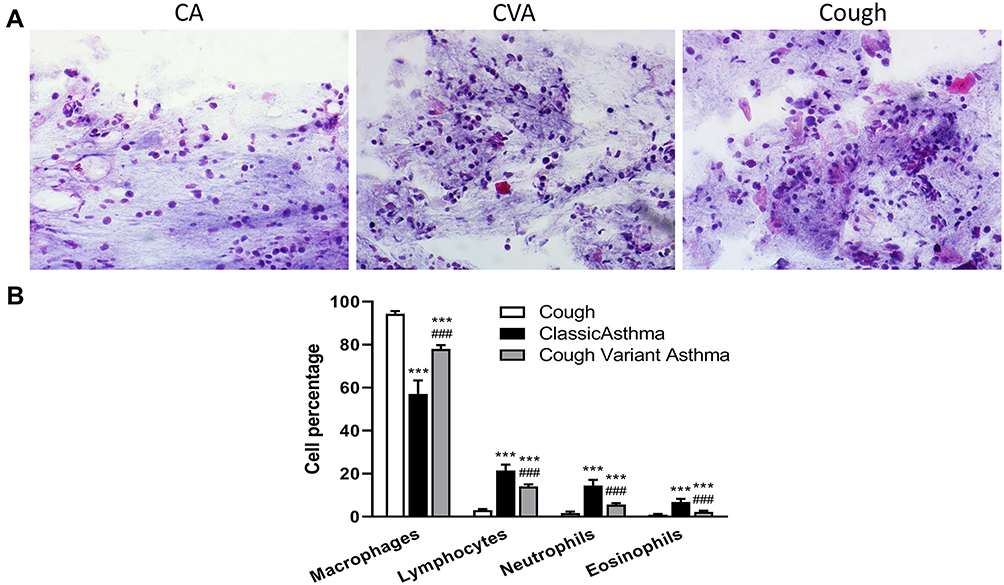 |
Figure 1 Hematoxylin-eosin (HE) staining results of cell count in bronchoalveolar lavage fluid (A) H&E stained images of BALF specimens from patients with cough variant asthma (CVA), chronic cough and classical asthma (CA); (B) the number of macrophage counts, neutrophils, lymphocytes and eosinophils in BALF specimens, differences between the three groups were compared using Kruskal–Wallis test. ***P<0.001 is considered a significant difference compared to the chronic cough group, and ###P<0.001 shows a significant difference compared to the CA group. |
In patients with chronic cough, the main manifestation of CVA is the accumulation and infiltration of airway inflammatory factors, so patients with chronic cough with an unknown diagnosis can be diagnosed by measuring IFN-γ secreted by Th1 cells and IL-4, IL-5, IL-13, IL-18, and IL-25 secreted by Th2 cells in BALF.5,7 As shown in Figure 2, Th1 cytokines IFN-γ in the CA and CVA groups were significantly lower than those in the chronic cough group (P < 0.05), and Th1 cytokines in the CA group were lower than that in the CVA group (P < 0.05). On the contrary, Th2 type cytokines IL-4, IL-5, IL-13, IL-18, and IL-25 in the CA and CVA groups were dramatically higher than those in the chronic cough group (P < 0.05), and the Th2 cytokines in the CA group were higher than that in the CVA group (P < 0.05).
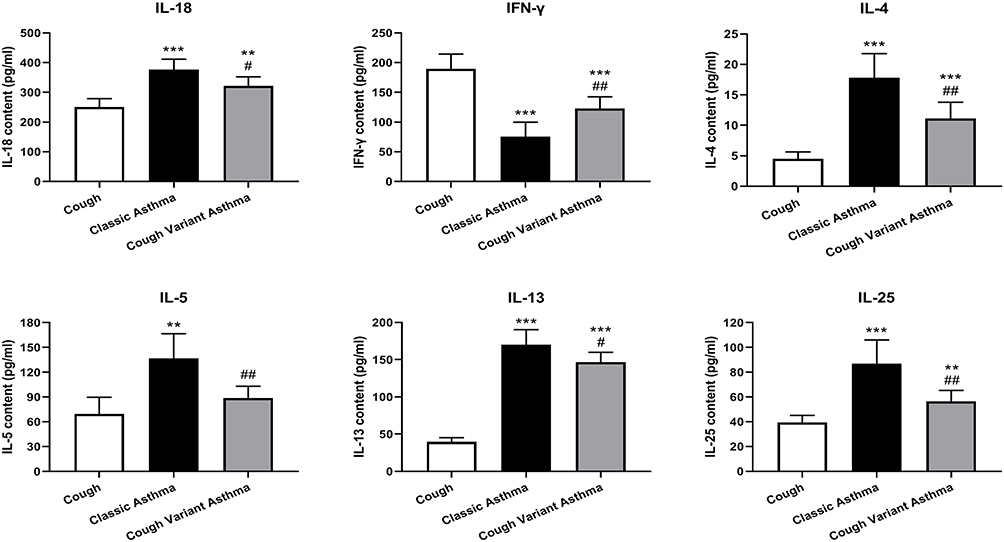 |
Figure 2 Th1 cytokine interferon-γ (IFN-γ) and Th2 cytokines interleukin 4 (IL-4), IL-5, IL-13, IL-18, and IL-25 in bronchoalveolar lavage fluid measured by enzyme-linked immunosorbent assay (ELISA) from cough variant asthma (CVA), chronic cough and classical asthma (CA) patients. Differences between the three groups were compared using the Kruskal–Wallis test. **P<0.01, ***P<0.001 shows a significant difference compared to the chronic cough group, and #P<0.05, ##P<0.01 shows a significant difference compared to the typical asthma group. |
As shown in Tables 2 and 3, the number of neutrophils, lymphocytes and eosinophil and Th2 cytokines IL-4, IL-5, IL-13, IL-18, and IL-25 were negatively correlated with FEV1, FVC and FEV1/FVC, but positively correlated with IgE and FeNO. In contrast, macrophages and IFN-γ were positively correlated with FEV1, FVC and FEV1/ FVC, while negatively correlated with IgE and FeNO.
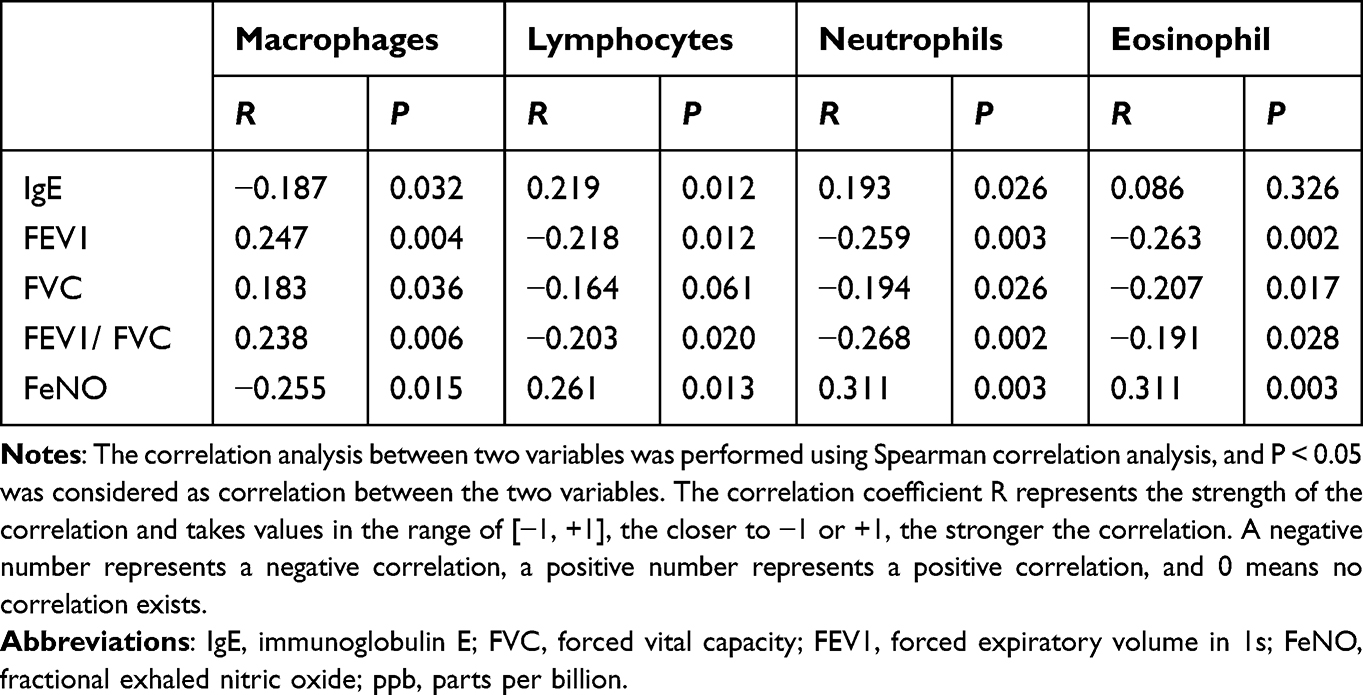 |
Table 2 Relationship Between Cell Count and Pulmonary Function |
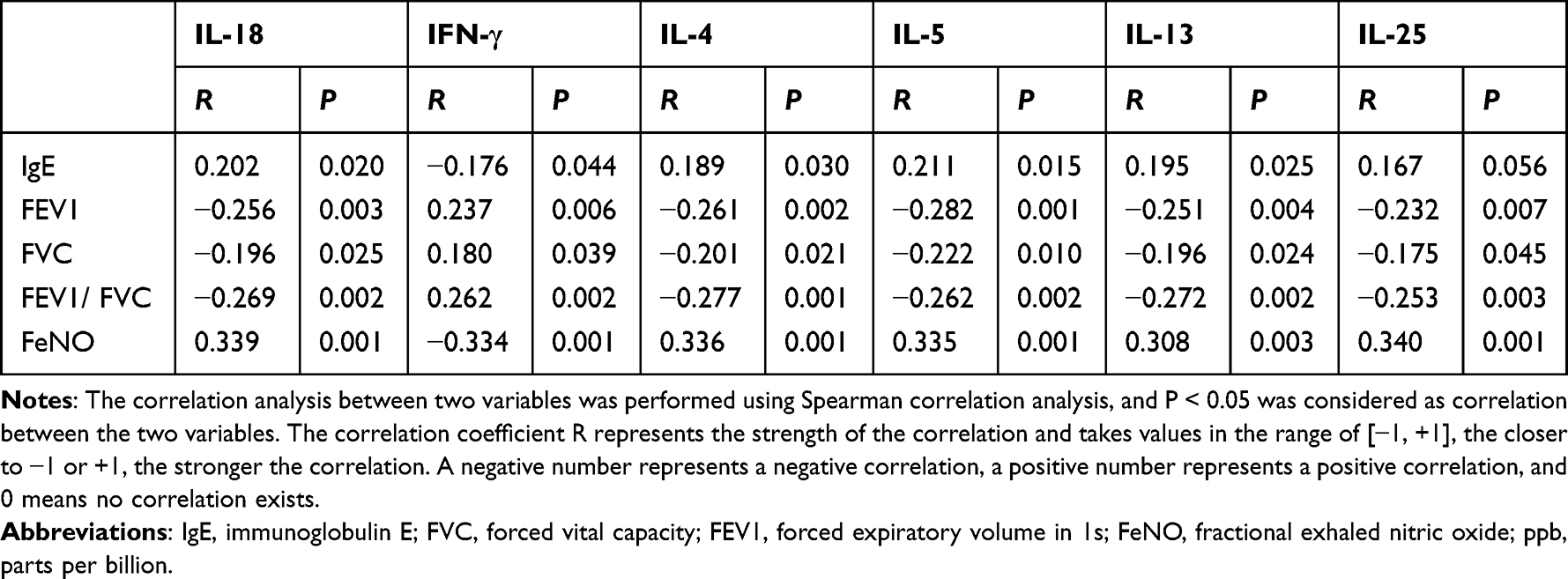 |
Table 3 Relationship Between Cytokines and Pulmonary Function |
Discussion
CVA is a common chronic respiratory disease with a stubborn, persistent, severe dry cough as its main clinical manifestation and other symptoms such as little or no sputum and no obvious wheezing or shortness of breath.4 In this study, evaluation of lung function and FeNO levels was provided for patients with chronic cough, CA and CVA. The results showed that the pulmonary function index of asthma was lower than that of cough variant asthma and chronic cough, while FeNO results were higher in asthma patients than in both CVA and chronic cough patients, which was consistent with a previous report.13 A study by Wang et al10 revealed that patients with CA had prominent higher FeNO than those with CVA, and their detected FeNO values were markedly higher than the normal range, suggesting that CA patients have higher chronic airway inflammation than CVA patients and normal subjects. In patients with chronic cough and asthma, the detection of FeNO can be used as an auxiliary diagnostic aid to predict airway eosinophilic inflammation and is also one of the good markers of airway eosinophilic inflammation.14,15 Some scholars have proposed that the exhaled FeNO can be utilized as an assistant in the diagnosis of CVA diseases.14 The advantages of this method are that it is simple to reform, safe, and repeatable.16 The measurements are of great significance for disease diagnosis, but the clinical instruments applied to detect FeNO are expensive and have not been widely used in most grass-roots hospitals.17
A positive bronchial provocation test is the gold standard for the diagnosis of CVA.18 The methacholine bronchial provocation test is essential in the diagnosis of chronic cough related to bronchial hyperresponsiveness,19 and FeNO is one of the non-invasive indicators for observing airway inflammation. FeNO cannot replace the bronchial provocation test,20 however, its detection can be employed in conjunction with other indicators to comprehensively consider the causes of CVA in patients.21 Previous studies indicated that infiltration of inflammatory cells such as neutrophils, eosinophils and lymphocytes, and a cytokine network consisting of Th2 cell inflammatory factors such as IL-4, IL-5 and IL-13 are common pathophysiological mechanisms.22 In this study, we found that neutrophils, lymphocytes, and eosinophils in the CA and CVA groups were significantly higher than those in the chronic cough group, and they were negatively correlated with FEV1, FVC and FEV1/FVC and positively correlated with IgE and FeNO. However, CVA patients had milder eosinophilic inflammation compared to CA patients. This was consistent with several studies3,13 which found that the proportion of airway eosinophilic inflammation in CVA patients was significantly lower than that in CA patients. Other studies also suggested that eosinophils in the sputum of patients with CVA were elevated, and a collection between the percentage of sputum eosinophils and FEV1% was also found in CA.5 However, an earlier study reported no significant difference in blood sputum eosinophil counts between CA and CVA, and these inconsistencies may be attributed to different populations and small sample sizes (12 CVA subjects). In contrast, the strength of our data is the “natural state” of the disease, as all subjects were newly diagnosed patients who had not previously received standard anti-asthma treatment.
It is well known that the imbalance of Th1/Th2 cells and the secretion of cytokines are closely associated with the occurrence of asthma.23 Th2 cells mainly produce IL-4, IL-5 and IL-13, which increase the level of IgE in serum and recruit eosinophils.24 Previous studies showed that the proportion and functional imbalance of Th1 and Th2 subsets form the main case mechanism of asthma attack,25 as evidenced by a decline in the function of the Th1 cell subsets and the hyperfunction of theTh2 cell subsets. In line with this, the present study also revealed that the expression of Th2-related cytokines was increased in patients with CVA and CA. Also, it was positively correlated with FEV1, FVC and FEV1/FVC and negatively correlated with IgE and FeNO, while the results for Th1-related cytokines were the opposite of those for Th2-related cytokines. Although the clinical symptoms of CVA are less severe than that of typical asthma, there are still immune disorders of Th1/Th2 and excessive secretion of Th2 in its pathogenesis.6 Thus, early intervention in the differentiation of Th0 to Th2 can serve as a reference for clinical treatment.
Our study has some limitations. First, the analysis sample size was relatively small and the observation period was short. Additionally, the study was a single-center retrospective study and environmental information was difficult to obtain, and environmental exposures of each cohort, such as pets, smoking, crowding per cohort, sp IgE levels for dust mites, pet dander, and pollen were lacking. Therefore, it is hoped that these data will be further collected in a follow-up study to add value to the analysis.
Conclusion
To sum up, neutrophils, lymphocytes, eosinophils, and Th2-associated cytokines in BALF were significantly higher in both the CA and CVA groups than in the chronic cough group. Also, they were negatively correlated with lung function and positively correlated with IgE and FeNO, while the Th1-associated cytokines were the opposite. However, patients with CVA have less eosinophilic inflammation compared to those with CA, suggesting that CVA is an early stage of CA.26 This provides a reference to understand the disease mechanism underlying the progression of CVA to CA at an early clinical stage. However, due to the limited sample size for analysis and the short observation period of the study, sample accumulation is needed to further explore the clinical differences in Th1/Th2 inflammatory indicators in CVA, chronic cough, and asthma.
Data Sharing Statement
All data that support the findings in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study protocol was reviewed and approved by the Ethics Committee of Wenling first people’s Hospital, approval number KY-2019-1011-01. All included patients gave written informed consent before study inclusion, indicating that their patient data may be used for academic research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Basic Public Welfare Research Project of Zhejiang Province (LGF19H010005) and the Zhejiang medical and health science and technology plan project (2020KY1060).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Morice A, Millqvist E, Bieksiene K, et al. ERS guidelines on the diagnosis and treatment of chronic cough in adults and children. Eur Respir J. 2020;55(1):1901136. doi:10.1183/13993003.01136-2019
2. Liu W, Chen H, Zhang D, et al. A retrospective study of clinical features of cough variant asthma in Chinese adults. AACI. 2019;15:3. doi:10.1186/s13223-019-0318-5
3. Lai K, Zhan W, Wu F, et al. Clinical and inflammatory characteristics of the Chinese APAC cough variant asthma cohort. Front Med. 2021;8:807385. doi:10.3389/fmed.2021.807385
4. Miwa N, Nagano T, Ohnishi H, et al. An open-label, multi-institutional, randomized study to evaluate the additive effect of a leukotriene receptor antagonist on cough score in patients with cough-variant asthma being treated with inhaled corticosteroids. Kobe J Med Sci. 2018;64:E134–E139.
5. Gao J, Wu F, Wu S, et al. Inflammatory subtypes in classic asthma and cough variant asthma. J Inflamm Res. 2020;13:1167–1173. doi:10.2147/JIR.S269795
6. Wang Z, Shen G, Huang Y. Regulatory effects of miR-138 and RUNX3 on Th1/Th2 balance in peripheral blood of children with cough variant asthma. Zhongguo dang dai er ke za zhi. 2021;23:1044–1049. doi:10.7499/j.issn.1008-8830.2107029
7. Kwak E, Hong J, Kim M, et al. Chitinase 3-like 1 drives allergic skin inflammation via Th2 immunity and M2 macrophage activation. Clin Exp Allergy. 2019;49:1464–1474. doi:10.1111/cea.13478
8. Wu X, Fang X, Nie M, et al. IL-1β或TNF-α干预的子宫蜕膜细胞对母胎界面Th1/Th2及Th17/Treg平衡的影响 [Effect of IL-1β or TNF-α-treated human decidual cells on balance between Th1 and Th2 or Th17 and Treg immunity]. Zhong Nan da Xue Xue Bao Yi Xue Ban. 2017;42:66–71. Chinese. doi:10.11817/j.issn.1672-7347.2017.01.011
9. Jin L, Gong H, Zhang Q. Zhang Q The clinical differences between cough variant asthma cells and humoral immunology indicators. Cell Mol Biol. 2022;68:188–193. doi:10.14715/cmb/2022.68.4.22
10. Wang Y, Zhao L, Chen F, et al. Diagnostic value of fractional exhaled nitric oxide and small airway function in differentiating cough-variant asthma from typical asthma. Can Respir J. 2021;2021:9954411. doi:10.1155/2021/9954411
11. Cough GF, Da MO. Guidelines for diagnosis and management of cough. Chin J Tubere Respir Dis. 2016;39:323–354.
12. Ahmed M, Munir M, Sufyan A, et al. Metered dose inhaler technique: a priority catch for physicians. Cureus. 2020;12:e10857. doi:10.7759/cureus.10857
13. Shimoda T, Obase Y, Kishikawa R, et al. The fractional exhaled nitric oxide and serum high sensitivity C-reactive protein levels in cough variant asthma and typical bronchial asthma. Allergol Int. 2013;62:251–257. doi:10.2332/allergolint.12-OA-0515
14. Naderi M, Sabour S. Diagnostic value of FeNO and MMEF for predicting cough variant asthma in chronic cough patients: methodological issues. J Asthma. 2021;58:791–792. doi:10.1080/02770903.2020.1741613
15. Chung K. Increasing utility of FeNO as a biomarker of type-2 inflammation in severe asthma. Lancet Respir Med. 2021;9:1083–1084. doi:10.1016/S2213-2600(21)00170-3
16. Lemiere C. Advanced diagnostic studies: exhaled breath and sputum analyses. J Occup Environ Med. 2014;56(Suppl 10):S45–48. doi:10.1097/JOM.0000000000000286
17. Holz O, Buhl R, Hausen T, et al. Messung der Atemwegsentzündung in der pneumologischen Praxis - Anwendung und Interpretation [Measuring airway inflammation in clinical practise - application and interpretation]. Pneumologie. 2007;61:194–201. Romanian. doi:10.1055/s-2007-959175
18. Ng KL, Huan NC, Mohammad FA, et al. A nationwide survey on awareness and knowledge about Bronchial Provocation Test amongst doctors in Malaysia. Med J Malaysia. 2022;77:33–40.
19. Rybka-Fraczek A, Dabrowska M, Grabczak EM, et al. Does bronchial hyperresponsiveness predict a diagnosis of cough variant asthma in adults with chronic cough: a cohort study. Respir Res. 2021;22:252. doi:10.1186/s12931-021-01845-2
20. Louis R, Satia I, Ojanguren I, et al. European respiratory society guidelines for the diagnosis of asthma in adults. Eur Respir J. 2022;60(3):2101585. doi:10.1183/13993003.01585-2021
21. Al-Ahmad M, Mobayed H, Al Busaidi N, et al. Severe asthma treatment patterns: a multicenter observational study in the Gulf region. World Allergy Organ J. 2022;15:100647. doi:10.1016/j.waojou.2022.100647
22. Couillard S, Steyerberg E, Beasley R, et al. Blood eosinophils, fractional exhaled nitric oxide and the risk of asthma attacks in randomised controlled trials: protocol for a systemic review and control arm patient-level meta-analysis for clinical prediction modelling. BMJ Open. 2022;12:e058215. doi:10.1136/bmjopen-2021-058215
23. Shi L, Wang J, Guo HX, et al. Circulating Th2 cell reduction and Th1/Th2 imbalance are correlated with primary Sjogren’s syndrome-associated interstitial lung disease. Arthritis Res Ther. 2022;24:121. doi:10.1186/s13075-022-02811-z
24. Patel N, Padhiyar J, Singh R, et al. Comparative evaluation of host immune response and cytokine signature pertaining to Th1 and Th2 immune arms in serum and tissue among patients of acute localised vs. chronic disseminated dermatophytosis. Mycoses. 2022;65(9):877–886. doi:10.1111/myc.13479
25. Zhou Y, Wang T, Zhao X, et al. Plasma metabolites and gut microbiota are associated with T cell imbalance in BALB/c model of eosinophilic asthma. Front Pharmacol. 2022;13:819747. doi:10.3389/fphar.2022.819747
26. Fujimura M. 咳嗽型喘息の病態、診断、治療について [Pathophysiology, diagnosis and treatment of cough variant asthma]. Rinsho Byori. 2014;62:464–470. Japanese.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of Budesonide Inhalation Treatment on the Expression Levels of Serum IL-6, TGF-β1, and IgE and Pulmonary Function in Patients with Cough Variant Asthma and an Evaluation of Treatment Efficacy
Niu Y, Cao M, Li S, Mo J, Zhu Z, Wang H
International Journal of General Medicine 2024, 17:1253-1261
Published Date: 29 March 2024