Back to Journals » Journal of Inflammation Research » Volume 18
Study on the Effects of Tranexamic Acid on Perioperative Inflammation, Long-Term Functional Recovery, and Satisfaction in Total Knee Arthroplasty: A Follow-up Study
Authors Lin S, Zhang X, Xia X, Xu G, Pan H
Received 12 May 2025
Accepted for publication 9 September 2025
Published 15 September 2025 Volume 2025:18 Pages 12769—12781
DOI https://doi.org/10.2147/JIR.S532632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Justin Jacob
Silong Lin, Xianqi Zhang, Xishang Xia, Guishui Xu, Hong Pan
Orthopedic Surgery, Anqing First People’s Hospital of Anhui Medical University, Anqing, Anhui, People’s Republic of China
Correspondence: Hong Pan, Anqing First People’s Hospital of Anhui Medical University, Anqing, Anhui, People’s Republic of China, Tel +86 18133027706, Email [email protected]
Purpose: To explore the anti-inflammatory effects and safety of Tranexamic Acid (TXA) during the perioperative period of Total Knee Arthroplasty (TKA) in patients with Knee Osteoarthritis (KOA), and to follow-up on long-term knee joint function and patient satisfaction.
Methods: A prospective non-randomized controlled cohort study evaluated TXA efficacy in 130 unilateral TKA patients with KOA between January 2019 and March 2021. Patients were randomized into TXA (n=65) and control (n=65) groups. The TXA group received both intravenous and intra-articular TXA as required Postoperative coagulation profiles, day-3 systemic inflammatory markers, 6-month DVT/complication rates, and 2-year functional outcomes (knee function, QoL [Quality of Life], satisfaction) were assessed.
Results: No significant differences in demographics, clinical data, or KOA severity were observed between the control and TXA groups (P> 0.05). Only TXA group showed decreased post-operative Fibrinogen (FIB) levels, while Erythrocyte Sedimentation Rate (ESR)(decreased to 15.41 ± 4.39 mm/h), C-reactive Protein (CRP) (decreased to 33.32 ± 11.56 mg/L), and Interleukin 6 (IL-6) levels significantly decreased (decreased to 111.38 ± 30.14 μg/mL) on the third day post-operation (P< 0.001). During the 6 months, specific complications did not significantly differ, but the overall complication rate notably decreased in the TXA group (OR=0.23, 95% CI 0.08 to 0.61, P = 0.012). At 2-year follow-up, TXA group showed significantly better joint function and QoL (P< 0.05). Postoperative satisfaction correlated with preoperative TXA use, neutrophil count, NLR, ESR, and CRP. Multivariate analysis identified TXA as an independent predictor of satisfaction (P< 0.05). TXA group exhibited reduced inflammation, lower complication rates, and improved long-term outcomes, demonstrating favorable perioperative and long-term outcomes in KOA management.
Conclusion: TXA has a significant effect on perioperative inflammation, long-term functional recovery and satisfaction in TKA.
Keywords: total knee arthroplasty, tranexamic acid, observational study, quality of life, inflammatory response
Introduction
Knee osteoarthritis (KOA) is a prevalent degenerative joint disease characterized by chronic inflammation, progressive cartilage loss, and significant pain and functional impairment.1 Inflammatory activation of synovial tissue occurs early in KOA, with macrophages and fibroblasts releasing pro-inflammatory cytokines such as IL-1β, TNF-α, and IL-6.2 These molecules accelerate the degradation of cartilage extracellular matrix by activating the NF-κB pathway and promoting the expression of matrix metalloproteinases (MMPs) and platelet-responsive protein-containing deintegrin metalloproteinases (ADAMTS).3 The infrapatellar fat pad (IFP) is a fibrous adipose tissue of the knee joint that plays an important role in the mechanisms that induce osteoarthritis (OA) disease onset and progression.4 Critically, this inflammatory state is not confined to the joint; it contributes to systemic metabolic and immune dysfunction, exacerbating symptoms like muscle atrophy and pain sensitization.5–7 While early-stage management involves lifestyle changes and physical therapy, total knee arthroplasty (TKA) remains the definitive solution for severe KOA to relieve pain and restore function.8,9 However, TKA itself triggers a significant systemic inflammatory response due to surgical trauma, ischemia-reperfusion injury, and infection risk.10–12 This response contributes to postoperative complications such as pain, swelling, reduced mobility, and potentially compromised outcomes.13 Therefore, strategies mitigating perioperative inflammation are crucial for improving recovery.
Tranexamic acid (TXA), a potent antifibrinolytic agent, is a mainstay for reducing blood loss in TKA.14 Beyond hemostasis, emerging evidence suggests TXA possesses direct anti-inflammatory properties. Animal models demonstrate TXA’s protective effects against post-traumatic OA progression,15 and clinical studies indicate its perioperative use in TKA may correlate with reduced systemic inflammatory markers like IL-6 and CRP, potentially contributing to decreased postoperative pain and swelling.16,17 This positions TXA as a promising candidate for repurposing to address the inflammatory burden inherent in both KOA and TKA.15 Despite this potential, a significant research gap exists. Previous studies primarily focus on TXA’s blood-sparing effects or are limited to retrospective analyses or animal models of OA.18 Crucially, the long-term functional consequences and the specific impact of TXA’s anti-inflammatory action on patient-reported outcomes and joint function following TKA remain inadequately explored.
This study addresses this gap directly. We employ a prospective non-randomized controlled cohort design to specifically investigate the anti-inflammatory effects and safety of perioperative TXA in TKA patients. By comparing systemic inflammatory marker levels, detailed postoperative recovery metrics, and crucially, tracking knee joint function and patient satisfaction over a two-year follow-up period, this study aims to provide robust clinical evidence on TXA’s potential benefits beyond hemostasis. Our prospective, longitudinal approach focusing on functional outcomes distinguishes this work from prior retrospective reviews or preclinical studies. The findings will offer new insights for optimizing perioperative management in TKA and the broader treatment of KOA inflammation.
Materials and Methods
General Materials
Selection
This is a prospective non-randomized controlled cohort study. A total of 130 patients who underwent unilateral TKA for OA at the Anqing Hospital affiliated with Anhui Medical University from January 2019 to March 2021 were selected. Patients were divided into a TXA group (intravenous TXA, n=65) and a control group (intravenous saline only, n=65) on the basis of preoperative doctor-patient shared decision-making. Grouping was based on patient acceptance of TXA and contraindication assessment, with non-randomized assignment. This study was approved by the Medical Ethics Committee of Anqing Hospital affiliated with Anhui Medical University (Medical Ethics Review (2019) No. 21). All procedures were performed in compliance with the Declaration of Helsinki, and informed consent was obtained from all participants and their close relatives.
Inclusion Criteria
Patients diagnosed with OA, indicating surgery, planning to undergo unilateral TKA for the first time; normal preoperative hemoglobin and coagulation markers; preoperative bilateral lower limb Doppler ultrasound showing no thrombosis.
The diagnosis of OA was confirmed by clinical evaluation (persistent knee pain, morning stiffness <30 minutes, and functional limitation) combined with radiographic evidence (Kellgren-Lawrence grade ≥2 on preoperative X-ray). In cases of diagnostic uncertainty, MRI was utilized to exclude other pathologies (such as meniscal tears) and assess cartilage degeneration (Outerbridge grade).
Exclusion Criteria
Previous history of TKA; preoperative anemia or coagulation dysfunction; history of allergy to TXA; severe underlying diseases that could not withstand surgery. Patients with other rheumatic diseases or autoimmune inflammatory diseases were also excluded.
Patient Data Collection
Demographic data of the patients, including age, gender, smoking and drinking history, Body Mass Index (BMI), and records of systemic comorbidities, such as diabetes and dyslipidemia, were collected.
TXA Intervention
All patients were given either spinal or general anesthesia, with a tourniquet applied preoperatively at a pressure of 35 kPa. A pneumatic tourniquet was applied to the proximal thigh at 35 kPa (≈263 mmHg), determined by adding a safety margin of 130 mmHg to the average preoperative systolic blood pressure (130 mmHg) to minimize tissue injury while ensuring effective hemostasis.19 This pressure aligns with international guidelines for tourniquet use in lower limb arthroplasty. Anesthesia type (spinal or general) was selected based on patient contraindications and anesthesiologist evaluation. Spinal anesthesia was preferred unless contraindicated. All patients were treated with the LINK Gemini MK II posterior stabilized cemented prosthesis (Link, Germany) including femoral condylar component, tibial plateau and polyethylene liner, with preservation of the posterior cruciate ligament (PCL) and intramedullary localization system to ensure alignment of the lines of force (<3° deviation from the target mechanical axis). All TKA surgeries were performed by 3 senior orthopedic surgeons (all with more than 10 years of experience in joint replacement), using a standardized surgical procedure and instrumentation to ensure technical consistency. The lateral 1/3 of the fat pad was resected only when it was severely fibrotic or prevented exposure of the surgical field to avoid anterior knee pain and release of inflammatory factors due to complete resection. The IFP vascular nerve bundle was protected intraoperatively by blunt dissection and no IFP repair was performed postoperatively.
Preoperative Use
TXA was administered 10 minutes before releasing the tourniquet. The observation group received 1 g of TXA (produced by Zhejiang Jinhua Conba Pharmaceutical Co., Ltd., with the National Medicine Certificate number H20031172, batch number: DK1812002-3) dissolved in 100 mL of 0.9% sodium chloride solution intravenously. The control group was given 100 mL of 0.9% sodium chloride solution intravenously. After the prosthesis was installed and the bone cement had fully solidified, the tourniquet was released, hemostasis was achieved with electrocoagulation, the area was rinsed and sutured, and a drainage tube was placed. The surgery was controlled within 90 minutes.
Postoperative Maintenance
Intra-articular continuous infusion of 3 g of TXA dissolved in 100 mL of saline at a rate of 12.5 mL/hour through a drain tube over 24 hours postoperatively.20 Postoperative intravenous maintenance is 1 g of TXA dissolved in 100 mL of saline every 8 hours for a total of three injections. Postoperative anticoagulation therapy was administered according to the standard treatment protocol. In patients with contraindications to TXA, the alternate antifibrinolytic drug aminocaproic acid (EACA) was used.
Laboratory Test Indicators
Venous blood was collected for routine blood analysis (used fasting blood sample), recording RBC count, Neutrophil count, Lymphocyte count, Monocyte count, and Platelet count. Additionally, the level of systemic inflammation was assessed using the following formula:21



Additionally, the levels of plasma prothrombin time (PT), plasma fibrinogen (FIB), and activated partial thromboplastin time (APTT) were measured preoperatively and 24 hours postoperatively for both groups. The level of inflammation was indicated by analyzing perioperative erythrocyte sedimentation rate (ESR), interleukin 6 (IL-6), and C-reactive protein (CRP) levels. Venous blood levels of ESR, IL-6, and CRP were measured preoperatively and on the third day postoperatively for both groups using the enzyme-linked immunosorbent assay (ELISA) method. CRP and IL-6 were detected using a Roche Cobas 8000 automatic biochemical immunoassay analyzer (Roche, Switzerland) with immunoturbidimetric (CRP) and chemiluminescent (IL-6) assays, respectively. ESR was detected using an Alifax Test 1 automatic ambulatory hemocytometer (Alifax, Italy). A 4 mL venous blood sample from all patients was centrifuged at 3000 r/min for 10 minutes, and the serum was stored at −80°C for testing. All operations were strictly carried out by professional laboratory personnel according to the instruction manual. Systemic Inflammatory markers (ESR, CRP, IL-6) were measured preoperatively and on the third postoperative day (POD3) based on the dynamic trajectory of postoperative inflammation, where POD3 represents a critical phase for evaluating sustained inflammatory responses beyond the acute surgical stress period.
Deep Vein Thrombosis (DVT)
Both groups of patients underwent bilateral lower limb venous color Doppler ultrasound examinations preoperatively (LOGIQ E20, General Electric Company, America), one week postoperatively, and four weeks postoperatively to ascertain the presence of thrombus formation.
Follow-up Study
Postoperative follow-up was conducted routinely, with visits every 1–2 months during the first half-year and outpatient visits every 3 to 6 months after one year. At 6 months postoperatively, complications of TKA were tallied, including deep vein thrombosis (DVT), cerebrovascular accidents, myocardial infarction, pneumonia, pulmonary embolism, urinary tract infections, transfusions, and superficial skin infections, in both groups of patients. The occurrence of total complications was calculated. Patient revision cases were recorded for subsequent analysis. Two years after surgery, knee joint function was assessed using The Hospital for Special Surgery (HSS) Knee Score Questionnaire and range of motion (ROM). The first postoperative follow-up visit was made to assess the grade of healing and the presence of redness, swelling or oozing. The HSS knee score and SF-36 quality of life (QoL) scale were completed by a blinded assessor at the 3-month postoperative follow-up. The HSS score, SF-36 scale and 6-minute walk test (6MWT) were repeated at 6-month and 1-year postoperative follow-up. Final 2-year postoperative follow-up included a patient satisfaction survey (5-point Likert scale), need for revision surgery, and survival analysis.
Knee function (HSS score) and QoL (SF-36) were systematically assessed at multiple time points: preoperatively, 3 months, 6 months, 1 year, and 2 years postoperatively. However, the 2-year data were prioritized in the main analysis to reflect long-term outcomes and align with international consensus on TKA efficacy evaluation. Data from earlier time points (3 days, 6 weeks, 6 months) focused on monitoring acute recovery parameters.
QoL and Satisfaction
The SF-36 scale, a validated and widely accepted tool, was used to assess QoL in both physical and mental domains.22 The physical health category includes the following subscales: physical functioning, role limitations due to physical health, bodily pain, and general health perceptions. The mental health category includes vitality, social functioning, role limitations due to emotional problems, and mental health. Scores range from 0 (worst health condition) to 100 (best health condition). The Chinese version of the SF-36 was used for assessing the QoL. The SF-36 questionnaire was administered preoperatively (baseline) and postoperatively at 3 months, 6 months, 1 year, and 2 years to track longitudinal changes in health-related QoL (HRQoL). HRQoL was evaluated using the validated Chinese version of the SF-36 Health Survey (version 2.0), which has demonstrated high reliability and validity in Chinese populations with knee osteoarthritis.23
Treatment satisfaction was assessed through patient ratings, ranging from 0 (least satisfied) to 100 (most satisfied), with a cutoff point of 90 for treatment satisfaction for analysis. Patient satisfaction was evaluated using a 5-point Likert scale specifically designed for postoperative TKA outcomes, with the following anchors: 1 = Very dissatisfied, 2 = Dissatisfied,3 = Neutral,4 = Satisfied, 5 = Very satisfied. Treatment satisfaction is the most crucial outcome variable.
Statistical Methods
Statistical analysis was performed using Graphpad (Graphpad Prism version 10.1.0 America). Quantitative data were presented as mean ± standard deviation (sd). Comparisons of baseline data and pre- and post-operative coagulation functions between groups were conducted using independent sample t-tests, while count data comparisons used chi-square tests. Changes in postoperative ESR, IL-6, and CRP peak levels and their levels on the third postoperative day were analyzed by binary and multiple logistic regression analyses in relation to TXA use. Normality of continuous variables was assessed using the Shapiro–Wilk test (for sample sizes <50) or the Kolmogorov–Smirnov test (for sample sizes ≥50), and statistical significance was set at P>0.05 to indicate a normal distribution. For non-normally distributed data, appropriate transformations were performed before parametric analysis, and if the transformation did not normalize the distribution, non-parametric tests (Mann–Whitney U, Wilcoxon signed rank) were used. All missing values were not included in the final statistical analysis.
Results
General Analysis
421 potential candidates were screened in this study, and after excluding those not meeting the inclusion criteria and unable to participate, a total of 130 patients were ultimately included and evenly divided into the observation and control groups (Figure 1). The observation group comprised 65 patients, including 22 males and 43 females, with an average age of 65.32 ± 4.17 years and a BMI of 26.03 ± 3.40 kg/m2, and an HSS score of 46.52 ± 9.15, and an VAS at rest score of 1.47 ± 0.62, and an VAS at movement of 2.14 ± 1.02, and an ROM(°) of 80.79 ± 17.83, and an SF-36 Physical score of 42.77 ± 15.29, and an SF-36 Mental score of 45.99 ± 16.68. The TXA treatment group consisted of 65 patients, with 31 males and 34 females; the average age was 65.48 ± 7.23 years, with a BMI of 24.95 ± 3.73 kg/m2, and an HSS score of 45.73 ± 7.50, and an VAS at rest score of 1.43 ± 0.58, and an VAS at movement of 2.19 ± 0.97, and an ROM(°) of 84.22 ± 19.34, and an SF-36 Physical score of 45.16 ± 17.22, and an SF-36 Mental score of 47.19± 17.83. The distribution of anesthesia types was balanced between groups and adjusted for in statistical analyses to minimize confounding. No statistically significant differences were observed in these metrics between the groups (all P > 0.05). Furthermore, there were no statistically significant differences in demographic data, routine blood tests, and systemic inflammation indices between the two groups (Table 1, P > 0.05), indicating comparability.
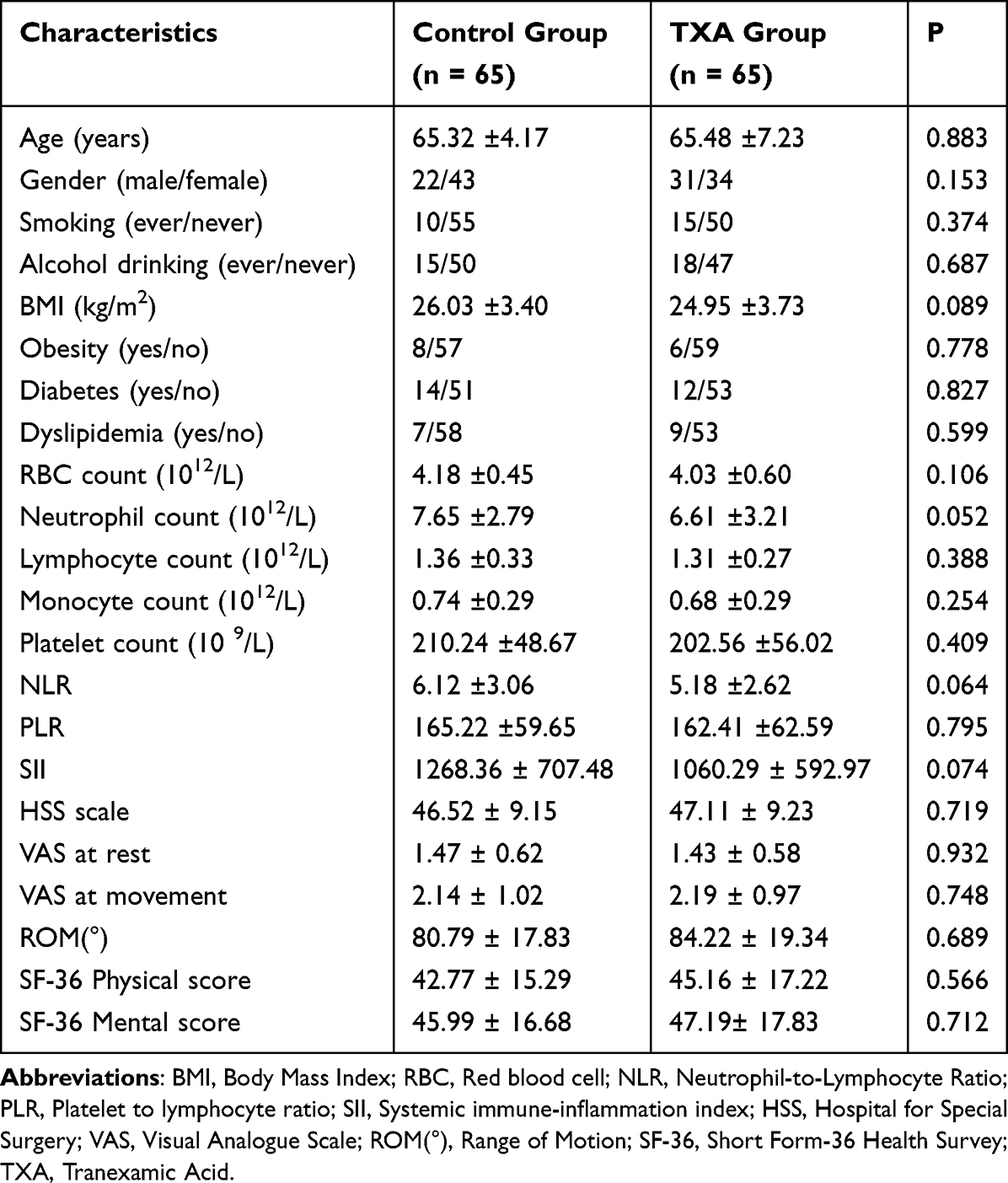 |
Table 1 Basic Characteristics of KOA Patients Treated by TKA with or without TXA |
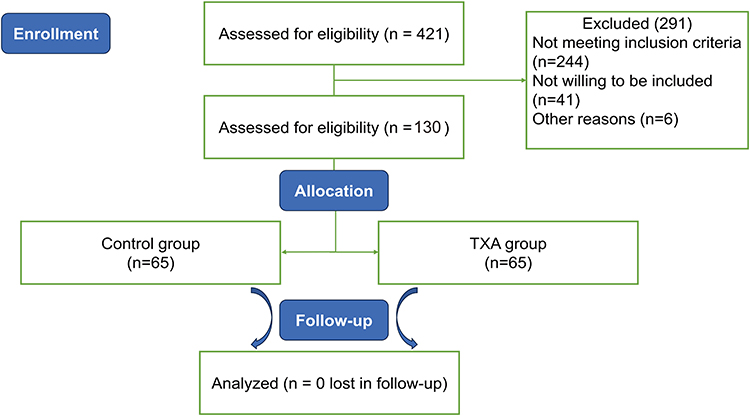 |
Figure 1 Study flow chart showing the data collection methodology and excluded cases. |
Postoperative Coagulation Function
Given that TXA is an important medication for coagulation disorders, preoperative and postoperative coagulation markers were analyzed for both groups. As shown in Table 2, there were no statistically significant differences in preoperative PT, FIB, and APTT between the groups (P > 0.05). However, postoperative FIB levels in the TXA group (2.95 ± 1.16 g) were significantly lower than those in the control group (3.35 ± 0.90 g, P = 0.031).
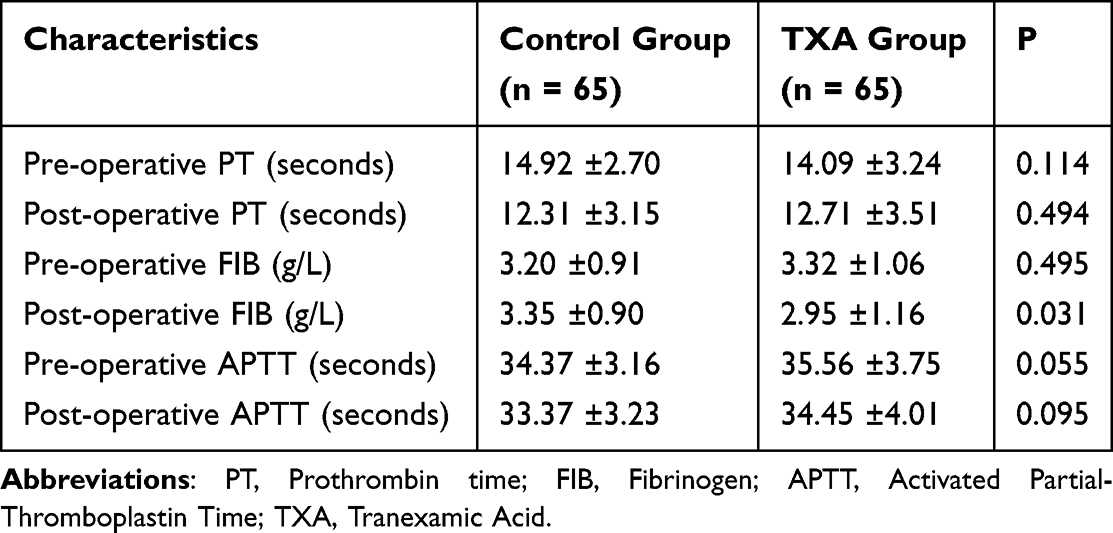 |
Table 2 The Coagulation Indexes of KOA Patients Treated by TKA with or without TXA |
Postoperative Inflammation Markers
To further clarify the effect of TXA on postoperative inflammatory responses, blood samples were collected preoperatively and on the third day postoperatively to analyze ESR, CRP, and IL-6 levels. Preoperative results showed no significant differences between the two groups (P > 0.05). However, on the third day postoperatively, significant reductions in ESR, CRP, and IL-6 levels were observed in the TXA intervention group (P < 0.05, Table 3).
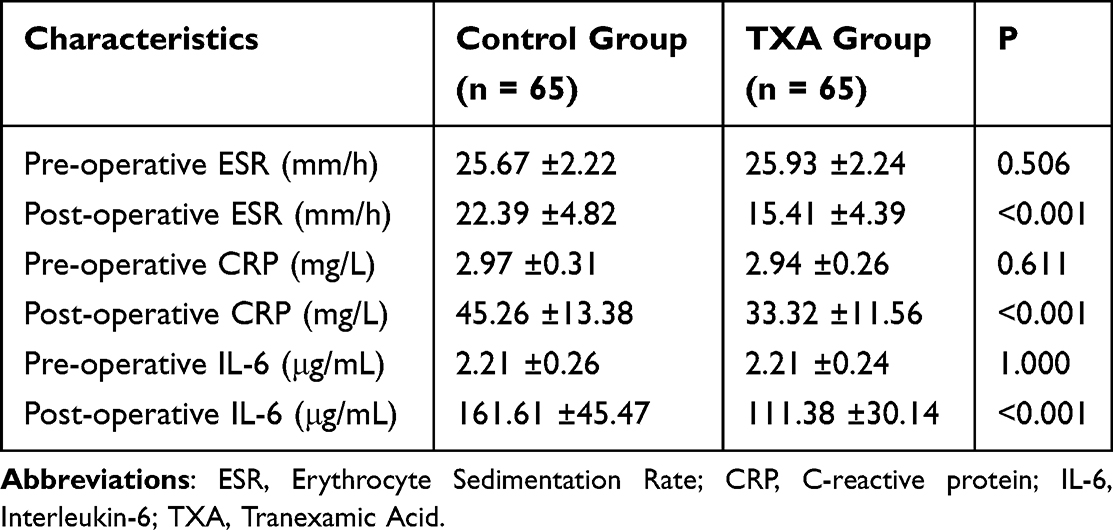 |
Table 3 The Inflammatory Indexes of KOA Patients Treated by TKA with or without TXA |
Postoperative Complications and Revision
An analysis of postoperative complications and revisions was conducted at the 6-month follow-up. As shown in Table 4, at 6 months postoperatively, there were no significant differences in DVT, cerebrovascular accident, myocardial infarction, pneumonia, pulmonary embolism, urinary tract infection, transfusions, and superficial skin infections (P > 0.05). Moreover, the overall incidence of total complications significantly decreased in the TXA group (OR = 0.23, 95% CI 0.08 to 0.61, P = 0.012). At 6 months postoperatively, 2 patients in the control group and 1 patient in the TXA group underwent revision, with no significant difference between the groups (OR = 0.49, 95% CI 0.04 to 5.57, P = 1.000). During the 2-year follow-up period, 8 patients (3 in the TXA group and 5 in the control group) underwent revision of the TKA. 3 cases had a delayed chronic infection, 1 case had an acute postoperative deep infection, 2 cases of aseptic loosening both with tibial prosthesis loosening, 1 case of polyethylene liner wear, and 1 case of joint stiffness. All revision cases were performed after confirmation of indications by a multidisciplinary team.
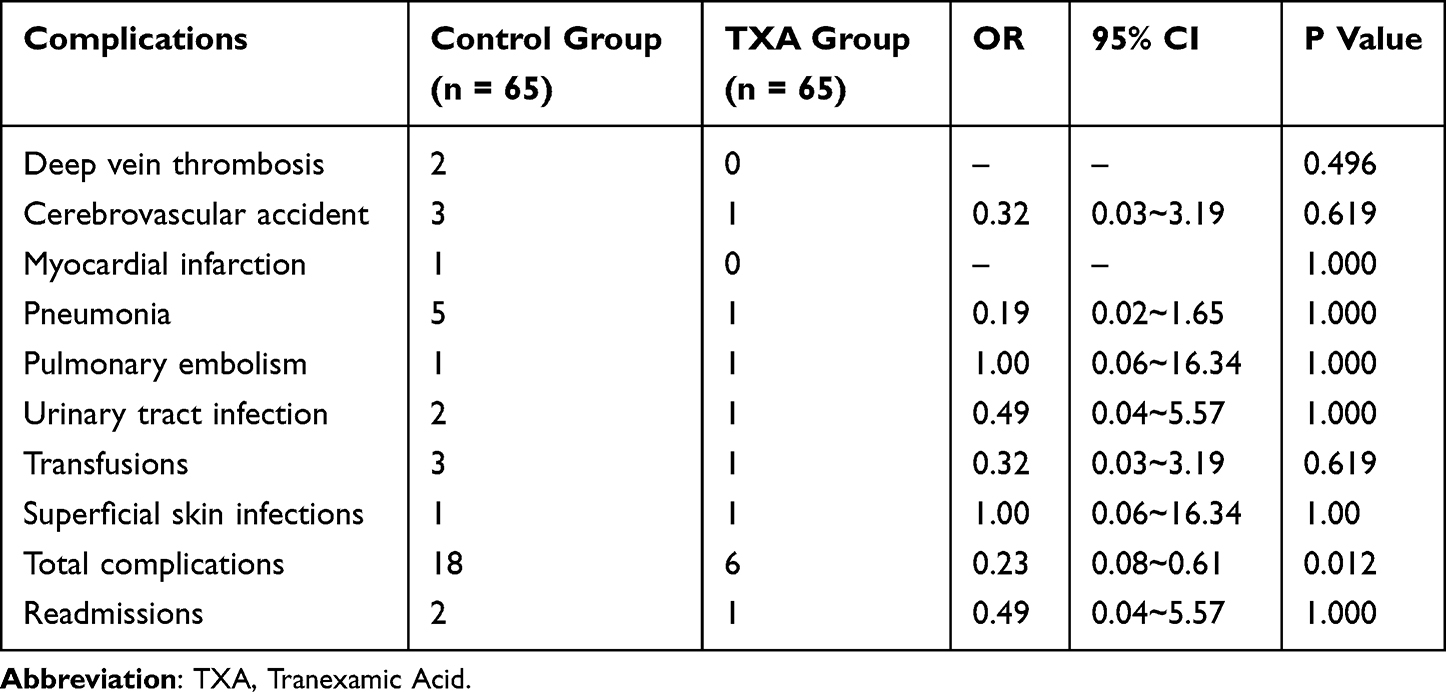 |
Table 4 Comparison of 6-month Complications and Readmissions in TKA Cases with or without TXA Treatment |
Postoperative Knee Function and QoL
The HSS score, VAS score, and ROM levels of both groups of patients were analyzed 2 years post-surgery. The HSS score in the TXA intervention group (92.43 ± 7.45) was significantly higher than that in the control group (86.38 ± 8.04, P<0.001), indicating that TXA intervention contributes to the long-term functional recovery of the knee joint post-TKA in KOA patients. Additionally, the long-term QoL, assessed through the SF-36, showed significant improvements in both physical and mental aspects in the TXA intervention group (P<0.001, Figure 2). We compared the changes in the HSS scale, VAS at rest, VAS at movement, ROM(°), SF-36 Physical score, and SF-36 Mental score between postoperative and preoperative assessments. The results revealed statistically significant differences in the change in HSS scale (P=0.011) and the change in ROM(°) (P=0.036), which further demonstrates the beneficial effect of TAX on patient outcomes (Table 5).
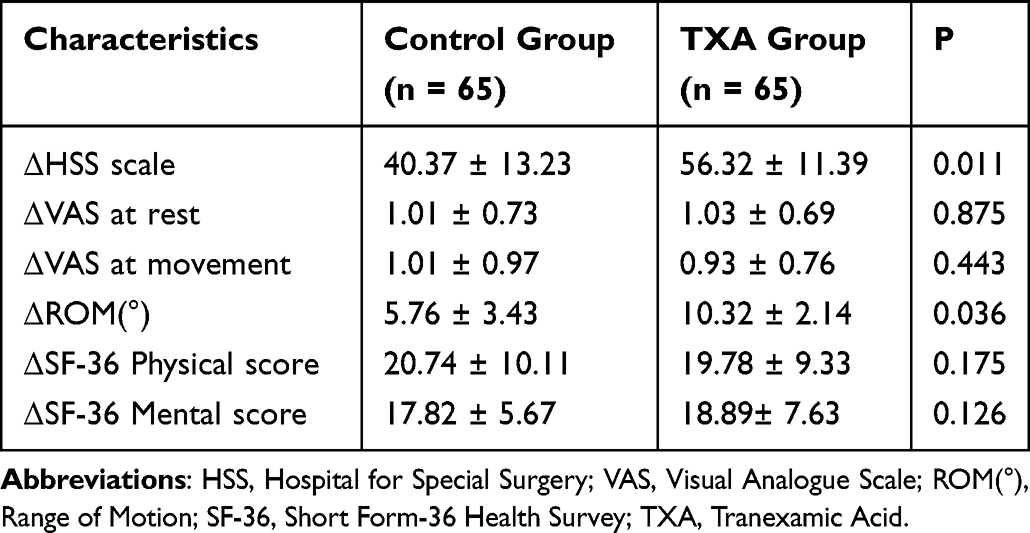 |
Table 5 Comparison of Changes in Key Outcome Measures at 6 Months in TKA Patients Treated with versus without TXA |
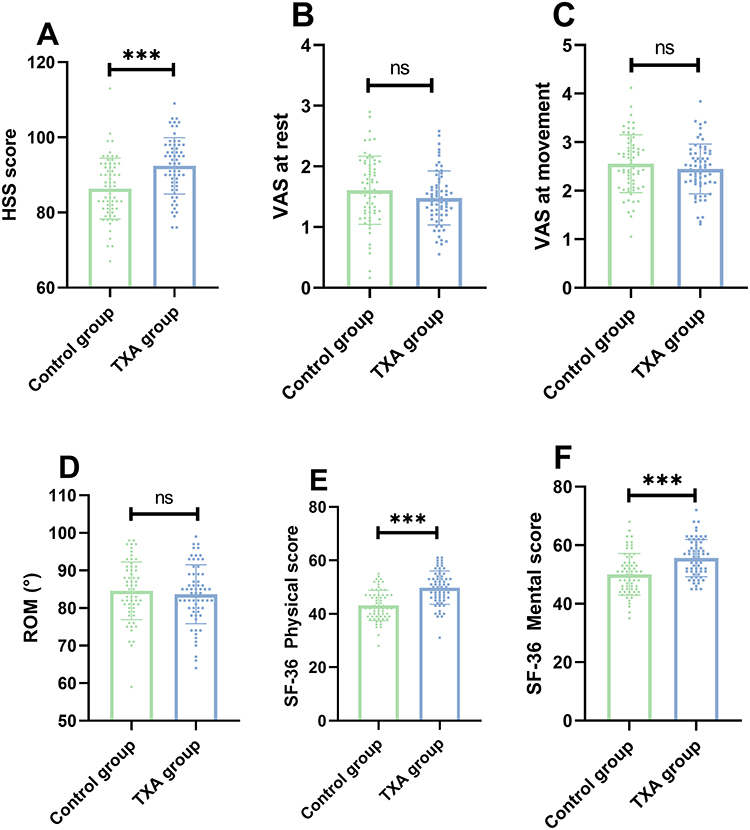 |
Figure 2 The long-term knee function and life quality in control and TXA group. (A) HSS score; (B) VAS at rest; (C) VAS at movement; (D) ROM; (E) SF-36 physical score; (F) SF-36 mental score. ***p < 0.001, ns: p>0.05. |
Treatment Satisfaction Analysis
To analyze long-term patient satisfaction post-surgery, satisfaction scores were compared between the control and TXA groups. The satisfaction score in the TXA group (94.66 ± 2.85) was significantly higher than that in the control group (92.58 ± 4.89, P=0.004). Moreover, using a satisfaction threshold of 90 points, 63 patients in the TXA group were satisfied, compared to 53 in the control group, showing a statistical difference (P=0.009).
Further correlation analysis between satisfaction scores and preoperative baseline data revealed that postoperative satisfaction was associated with TXA treatment, neutrophil count, NLR, SII, ESR, and CRP (P<0.05, Table 6). Multivariate logistic regression analysis, including these factors, identified TXA intervention as an independent factor for postoperative satisfaction (OR=0.192, 95% CI 0.028 to 0.798, P=0.0419, Table 7). In addition, the Nagelkerke R² value is 0.512, indicating that the model has a relatively good predictive value. Hence, the intraoperative use of TXA plays a role in enhancing patient satisfaction.
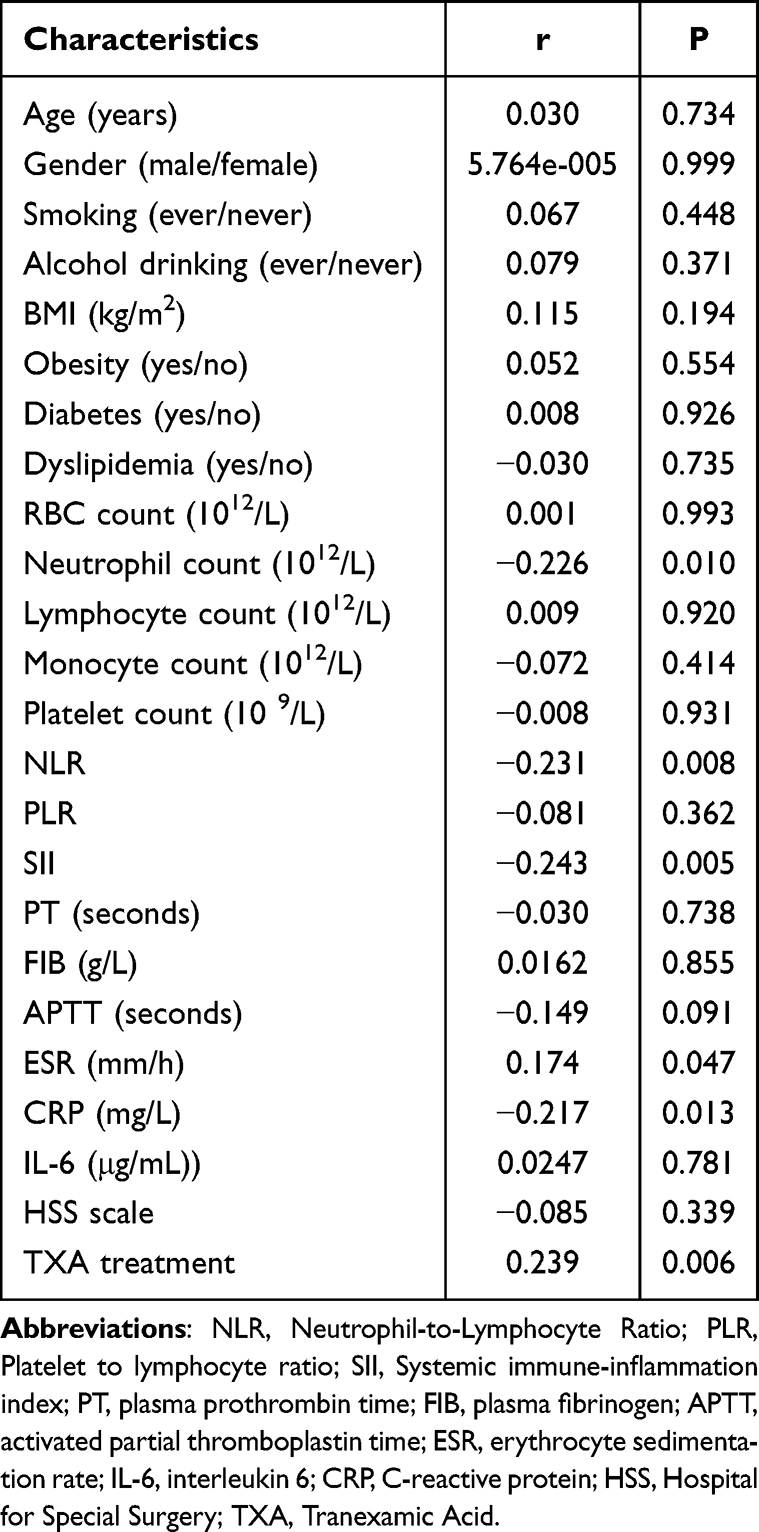 |
Table 6 The Correlations Between Baseline Characteristics and Satisfaction Score in All the Participants |
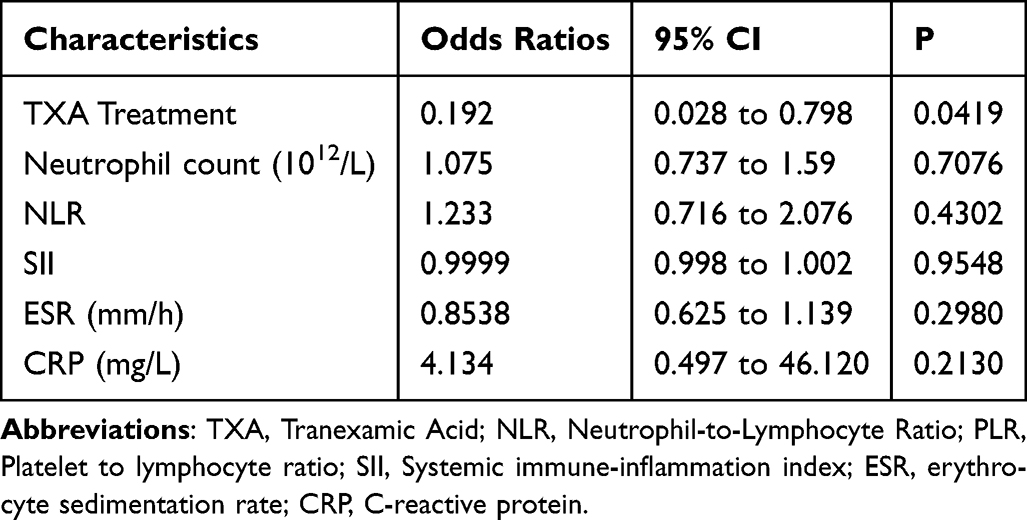 |
Table 7 The Effects of Based Characteristics on the Long-Term Satisfaction Status Using a Logistic Regression Model |
Discussion
Principal Findings
This study demonstrates that intravenous TXA administration in knee osteoarthritis (KOA) patients undergoing TKA effectively reduces postoperative inflammation (IL-6, TNF-α) and hidden blood loss without impairing coagulation function or increasing deep vein thrombosis (DVT) incidence, consistent with its known safety profile even at high doses (30 mg/kg).24,25 Crucially, TXA intervention was associated with enhanced functional recovery and identified as an independent protective factor for long-term patient satisfaction. We also found that elevated systemic inflammation markers (NLR, SII, ESR, CRP) correlated with reduced satisfaction—a novel observation underscoring the multifaceted impact of inflammation on recovery.
Comparison with Literature
Originally used to treat postpartum hemorrhage (PPH) due to its effective hemostatic properties, TXA has become a commonly used antifibrinolytic agent in clinical practice. Early studies found that TXA also has a role in reducing perioperative inflammatory responses, mainly in cardiac surgery, and has gradually been applied to other areas including cerebral and ocular hemorrhages.26,27 Moreover, TXA intervention has potential orthopedic hemostatic applications; recent systematic reviews and network meta-analyses have shown TXA to be one of the most effective interventions for preventing bleeding in hip or knee replacement surgeries.25 In this study, by comparing coagulation function and DVT incidence rates between two groups of patients postoperatively, results showed that TXA had little impact on coagulation function and did not increase the risk of venous thrombotic complications.
Clinical Implications
As TXA’s application in orthopedics becomes more widespread, increasing research has focused on its potential anti-inflammatory effects, offering additional benefits to patients. In 2016, Xie et al included 151 patients undergoing TKA in a study and found that multiple postoperative intravenous infusions of TXA could effectively reduce postoperative serum CRP and IL-6 levels. Most importantly, by adding one more intravenous push of TXA, patients could achieve smaller decreases in Hb, less postoperative inflammatory response, less pain, and less knee joint swelling.28 Moreover, multiple intravenous pushes of TXA effectively reduced hidden blood loss after primary THA.29 Another study evaluating 640 patients undergoing surgery after elbow trauma found that the use of TXA was associated with a lower incidence of heterotopic ossification compared to not using TXA.30 The results of this study showed that TKA surgeries with TXA intervention had lower levels of inflammation and higher functional recovery. Therefore, TXA has the potential for deeper application in the field of KOA.
Mechanistic Insights
The specific mechanisms of TXA’s anti-inflammatory action are not yet clearly understood. D-dimers can increase the release of inflammatory cytokines. Therefore, although fibrinolysis and inflammation are largely independent processes, they are likely closely connected, and inhibiting the formation of fibrinolysis may help suppress the generation of inflammatory factors.31
Early studies on traumatic brain injury found that only higher doses of TXA could definitively eliminate penumbral leukocyte mobilization, thereby maintaining the integrity of the blood-brain barrier after brain injury and inhibiting cellular activation.32 However, this study did not further explore the mechanisms, which remains a direction for future research by our team.
TXA demonstrates a favorable safety profile, with no evidence indicating that high doses (30 mg/kg) increase deep vein thrombosis risk. While our study confirms TXA does not impair coagulation or elevate thrombotic complications, its anti-inflammatory effects may exhibit dose dependency. Research in traumatic brain injury indicates that only higher TXA doses definitively suppress inflammatory pathways like penumbral leukocyte mobilization.33 In orthopedics, TXA reduces systemic inflammatory markers (CRP, IL-6) and improves outcomes,32 yet whether doses exceeding current regimens (eg, 30 mg/kg) could enhance anti-inflammatory efficacy remains unexplored. Future studies should investigate TXA’s dose-response relationship for anti-inflammatory benefits in knee surgery.
Satisfaction-Inflammation Correlation
This study also focuses on the postoperative QoL and satisfaction with surgery among patients with KOA undergoing TKA. Patients with KOA are often older, have declining physical functions, poor psychological resilience, and a lack of exercise awareness and discipline. This can lead to non-compliance with medical advice on exercise and excessive rest during home rehabilitation, increasing the risk of complications such as joint stiffness. These complications are detrimental to postoperative recovery and can lead to a decrease in QoL. Research has shown that satisfaction improves within the first six months after TKA treatment, supporting the early identification of patients at risk of low satisfaction with TKA. This enables clinicians to provide timely targeted treatment and supportive interventions to improve patient outcomes.34 Another multicenter cohort study indicated that low preoperative HRQoL scores, older age, severe obesity, certain comorbidities (such as depression and rheumatism), readmission or complications without discharge rehabilitation, are good predictors of long-term low benefits in HRQoL.33 Unlike previous findings, our study focused on systemic inflammation levels, identifying multiple NLR, SII, ESR, and CRP as candidate factors leading to poor patient satisfaction. A unique aspect of this study was its focus on TXA, finding that TXA intervention plays a role in enhancing long-term patient satisfaction rates and acts as an independent protective factor. Thus, this study provides new evidence for the use of TXA in KOA interventions from a novel perspective.
Limitations
This study has the advantages of a wide range of test indicators and a long follow-up period, focusing on TXA as a potential key candidate adjunctive medication. However, there are some limitations to this study. Firstly, it is not a randomized controlled double-blind experiment, and the absence of blinding may introduce bias in subjective testing and scoring. Additionally, the sample size is still not large enough, and some results, such as complications, cannot provide more convincing conclusions. Moreover, the individual differences among patients and the technical gaps among surgeons cannot be simply ignored. Finally, the knee joint scoring is not detailed enough, and future research should incorporate imaging and structural-functional analysis. Furthermore, there is no evidence to suggest that high doses (30 mg/kg) of TXA pose a risk of deep vein thrombosis formation, making TXA a relatively safe hemostatic strategy with potential for further application. As for the study of drug efficacy, the most appropriate dosage of medication needs to be confirmed in future strict large-sample clinical cohort studies.
Conclusion
TXA has a certain inhibitory effect on perioperative inflammatory responses in TKA, alleviates patient discomfort, promotes functional recovery, and improves long-term knee joint function and patient satisfaction without increasing the risk of thrombosis formation. The observed weak correlations may be attenuated by measurement error or unaccounted mediators. Future studies incorporating repeated biomarker sampling and mixed-effects models could better delineate these relationships. The conclusions of this study require further confirmation through well-designed, large-sample research. In addition, there is a potential connection between satisfaction and inflammation, and this is also the direction we will continue to explore next.
Abbreviations
KOA, Knee Osteoarthritis; TKA, Total Knee Arthroplasty; TXA, Tranexamic Acid; OA, Osteoarthritis; PT, plasma prothrombin time; FIB, plasma fibrinogen; APTT, activated partial thromboplastin time; ESR, erythrocyte sedimentation rate; IL-6, interleukin 6; CRP, C-reactive protein; ELISA, enzyme-linked immunosorbent assay; DVT, Deep Vein Thrombosis; HSS, Hospital for Special Surgery; ROM, range of motion; PPH, postpartum hemorrhage; HRQoL, Health-Related Quality of Life; BMI, Body Mass Index. NLR: Neutrophil-to-Lymphocyte Ratio; PLR: Platelet to lymphocyte ratio; SII: Systemic immune-inflammation index.
Funding
This study was supported by University-level scientific research program of Wannan Medical College Research Fund (JXYY202278) and Anhui Medical University Research Fund (2022XKJ094).
Disclosure
The authors declare that they have no conflicts of interest regarding this work.
References
1. Sharma L. Osteoarthritis of the Knee. N Engl J Med. 2021;384(1):51–59. doi:10.1056/NEJMcp1903768
2. Li X, Mei W, Huang Z, et al. Casticin suppresses monoiodoacetic acid-induced knee osteoarthritis through inhibiting HIF-1α/NLRP3 inflammasome signaling. Int Immunopharmacol. 2020;86:106745. doi:10.1016/j.intimp.2020.106745
3. Chen P, Zhou J, Ruan A, et al. Synovial tissue‐derived extracellular vesicles induce chondrocyte inflammation and degradation via NF‐κB signalling pathway: an in vitro study. J Cell Mol Med. 2022;26(7):2038–2048. doi:10.1111/jcmm.17227
4. Emmi A, Stocco E, Boscolo-Berto R, et al. Infrapatellar fat pad-synovial membrane anatomo-fuctional unit: microscopic basis for Piezo1/2 mechanosensors involvement in osteoarthritis pain. Front Cell Develop Biol. 2022;10. doi:10.3389/fcell.2022.886604
5. Ma Z, Huang Z, Zhang L, et al. Vanillic Acid reduces pain-related behavior in knee osteoarthritis rats through the inhibition of NLRP3 Inflammasome-related synovitis. Front Pharmacol. 2021;11. doi:10.3389/fphar.2020.599022
6. Dainese P, Wyngaert KV, De Mits S, Wittoek R, Van Ginckel A, Calders P. Association between knee inflammation and knee pain in patients with knee osteoarthritis: a systematic review. Osteoarthritis Cartilage. 2022;30(4):516–534. doi:10.1016/j.joca.2021.12.003
7. Puts S, Liberman K, Leysen L, et al. Exercise-induced effects on inflammatory markers and brain-derived neurotrophic factor in patients with knee osteoarthritis. A systematic review with meta-analysis. Exerc Immunol Rev. 2023;29:22–53.
8. Holden MA, Hattle M, Runhaar J, et al. Moderators of the effect of therapeutic exercise for knee and Hip osteoarthritis: a systematic review and individual participant data meta-analysis. Lancet Rheumatol. 2023;5(7):e386–e400. doi:10.1016/S2665-9913(23)00122-4
9. Diekman BO, Loeser RF. Aging and the emerging role of cellular senescence in osteoarthritis. Osteoarthritis Cartilage. 2024;32(4):365–371. doi:10.1016/j.joca.2023.11.018
10. Weinstein EJ, Stephens-Shields AJ, Newcomb CW, et al. Incidence, microbiological studies, and factors associated with prosthetic joint infection after total knee arthroplasty. JAMA Network Open. 2023;6(10):e2340457. doi:10.1001/jamanetworkopen.2023.40457
11. Robin KJ, Maier MA, Leslie LJ, et al. Severity of chronic venous insufficiency on primary total knee arthroplasty outcomes. J Arthroplasty. 2023;38(11):2324–2327e4. doi:10.1016/j.arth.2023.05.040
12. Ran W, Li S, Yuan R, Luo H, Li P, Gao J. Effect of tourniquet technique on postoperative delirium in elderly patients with total knee arthroplasty: a randomized single-blind controlled trial. BMC Anesthesiol. 2022;22(1):396. doi:10.1186/s12871-022-01938-5
13. Melinte RM, Arbanasi EM, Blesneac A, et al. Inflammatory biomarkers as prognostic factors of acute deep vein thrombosis following the total knee arthroplasty. Medicina. 2022;58(10):1502. doi:10.3390/medicina58101502
14. Burleson A, Guler N, Banos A, et al. Perioperative factors and their effect on the fibrinolytic system in arthroplasty patients. Clin App Thrombosis/Hemostasis. 2015;22(3):274–279. doi:10.1177/1076029615611251
15. Brochard S, Boumediene K, Mercier J, Agin V, Conrozier T, Bauge C. A single intraarticular injection of a tranexamic acid-modified hyaluronic acid (HA/TXA) alleviates pain and reduces OA development in a murine model of monosodium iodoacetate-induced osteoarthritis. Front Pharmacol. 2024;15:1456495. doi:10.3389/fphar.2024.1456495
16. Wei Z, Yu M, Xu Y, Weng X, Feng B. Impact of intraosseous regional administration of tranexamic acid in total knee arthroplasty on perioperative blood loss: a protocol for a randomised controlled trial. BMJ Open. 2024;14(2):e077393. doi:10.1136/bmjopen-2023-077393
17. Wu EB, Hung KC, Juang SE, Chin JC, Lu HF, Ko JY. Are risk factors for postoperative significant hemorrhage following total knee arthroplasty potentially modifiable? A retrospective cohort study. J Pers Med. 2022;12(3):434. doi:10.3390/jpm12030434
18. Xie W, Jiang S, Donat A, et al. Tranexamic acid attenuates the progression of posttraumatic osteoarthritis in mice. Am J Sports Med. 2024;52(3):766–778. doi:10.1177/03635465231220855
19. Chan K, Jaibaji R, Barker E, Talwar C, Pang C. A systematic review and meta-analysis of tourniquet pressures in upper limb surgery. J Clin Med. 2025;14(6):1938. doi:10.3390/jcm14061938
20. Prejbeanu R, Mioc ML, Tsiridis E, et al. The influence of Tranexamic Acid (TXA) on postoperative infection rates following Total Hip Arthroplasty (THA)-A systematic review. J Clin Med. 2025;14(9):2910. doi:10.3390/jcm14092910
21. Solak B, Kara RÖ. Systemic inflammation and its relationship with pruritus in early‐stage mycosis fungoides. J Cell Mol Med. 2024;28(4). doi:10.1111/jcmm.18125
22. Chen R, Liu J, Zhao Y, et al. Predictive value of preoperative short form-36 survey scale for postoperative axial neck pain in patients with degenerative cervical myelopathy. GloB Spine J. 2023;15(2):540–547. doi:10.1177/21925682231200136
23. Taskiran G, Eskin Bacaksiz F, Harmanci Seren AK. Psychometric testing of the Turkish version of the health professional education in patient safety survey: h-PEPSSTR. Nurs Edu Pract. 2020;42:102640. doi:10.1016/j.nepr.2019.102640
24. McQuilten ZK, Wood EM, Medcalf RL. When to use tranexamic acid for the treatment of major bleeding? J Thromb Haemost. 2024;22(3):581–593. doi:10.1016/j.jtha.2023.10.001
25. Gibbs VN, Champaneria R, Sandercock J, et al. Pharmacological interventions for the prevention of bleeding in people undergoing elective hip or knee surgery: a systematic review and network meta-analysis. Cochrane Database Syst Rev. 2024;1(1):CD013295. doi:10.1002/14651858.CD013295.pub2
26. Polymeris AA, Karwacki GM, Siepen BM, et al. Tranexamic acid for intracerebral hemorrhage in patients on non-vitamin K antagonist oral anticoagulants (TICH-NOAC): a multicenter, randomized, placebo-controlled, phase 2 trial. Stroke. 2023;54(9):2223–2234. doi:10.1161/STROKEAHA.123.042866
27. Woreta FA, Lindsley KB, Gharaibeh A, Ng SM, Scherer RW, Goldberg MF. Medical interventions for traumatic hyphema. Cochrane Database Syst Rev. 2023;3(3):CD005431. doi:10.1002/14651858.CD005431.pub5
28. Xie J, Ma J, Yao H, Yue C, Pei F. Multiple boluses of intravenous tranexamic acid to reduce hidden blood loss after primary total knee arthroplasty without tourniquet: a randomized clinical trial. J Arthroplasty. 2016;31(11):2458–2464. doi:10.1016/j.arth.2016.04.034
29. Xie J, Hu Q, Ma J, Huang Q, Pei F. Multiple boluses of intravenous tranexamic acid to reduce hidden blood loss and the inflammatory response following enhanced-recovery primary total hip arthroplasty: a randomised clinical trial. Bone Joint J. 2017;99-B(11):1442–1449. doi:10.1302/0301-620X.99B11.BJJ-2017-0488.R1
30. Liu H, Li J, Hu Y, et al. Association between tranexamic acid use and heterotopic ossification prevalence after elbow trauma surgery: a propensity-score-matched cohort study. J Bone Joint Surg Am. 2023;105(14):1093–1100. doi:10.2106/JBJS.22.01212
31. Johnson DJ, Johnson CC, Goobie SM, et al. High-dose versus low-dose tranexamic acid to reduce transfusion requirements in pediatric scoliosis surgery. J Pediatr Orthop. 2017;37(8):e552–e557. doi:10.1097/BPO.0000000000000820
32. Culkin MC, Bele P, Georges AP, et al. Dose-dependent tranexamic acid blunting of penumbral leukocyte mobilization and blood-brain barrier permeability following traumatic brain injury: an in vivo murine study. Neurocrit Care. 2024;41(2):469–478. doi:10.1007/s12028-024-01952-0
33. Gonzalez-Saenz-de-Tejada M, Quintana JM, Arenaza JC, et al. Long-term health related quality of life in total knee arthroplasty. BMC Musculoskelet Disord. 2023;24(1):327. doi:10.1186/s12891-023-06399-6
34. Young-Shand KL, Dunbar MJ, Laende EK, Mills Flemming JE, Astephen Wilson JL. Early identification of patient satisfaction two years after total knee arthroplasty. J Arthroplasty. 2021;36(7):2473–2479. doi:10.1016/j.arth.2021.02.057
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Postoperative Functional Mobility and Quality of Life in Patients with Anteromedial Osteoarthritis of the Knee Treated with MB-UKA versus TKA
Li SM, Liang BR, Xiao K, Fan CY, Li D, Han FF, Chen J
Journal of Pain Research 2026, 19:564539
Published Date: 3 March 2026