Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Study on the Changes in Circadian Rhythm Before and After Treatment and the Influencing Factors in Patients with Depression
Authors Guo P, Fang Y, Feng M, Shen Y, Yang S, Wang S, Qian M
Received 3 August 2022
Accepted for publication 22 October 2022
Published 10 November 2022 Volume 2022:18 Pages 2661—2669
DOI https://doi.org/10.2147/NDT.S384879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Ping Guo1,2 *, Yu Fang1 *, Min Feng,1 Yue Shen,1 Shengliang Yang,1 Shikai Wang,1 Mincai Qian1
1Department of Psychosomatic Medicine, Huzhou Third Municipal Hospital, Huzhou, People’s Republic of China; 2Huzhou Third Municipal Hospital Affiliated with Huzhou University, Huzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shikai Wang; Mincai Qian, Department of Psychosomatic Medicine, Huzhou Third Municipal Hospital, No. 2088 in Tiaoxi East Road, Wuxing District, Huzhou, Zhejiang Province, 313000, People’s Republic of China, Tel +86 13665752769 ; +86 13757289002, Email [email protected]; [email protected]
Objective: To investigate the circadian rhythms of patients with major depressive disorder (MDD) pre-treatment and post-treatment to analyse possible influencing factors.
Methods: In this study, we recruited 154 patients in the acute phase of MDD from 10 psychiatric centers in the province. The patients were divided into a morning chronotype group (16– 41 points), an intermediate chronotype group (42– 58 points) and an evening chronotype group (59– 86 points), according to the total scores obtained from the morningness–eveningness questionnaire (MEQ). They were treated randomly with antidepressants, either selective serotonin reuptake inhibitors or agomelatine, for 12 weeks and were evaluated using the MEQ, the 17-item Hamilton Depression Rating Scale (HAMD-17), the Hamilton anxiety scale, the Snaith–Hamilton pleasure scale (SHAPS), the multidimensional fatigue inventory (MFI-20) and the Pittsburgh sleep quality index at the baseline and then at 2, 4, 8 and 12 weeks. The results were analysed by Logistic regression analysis and repeated-measures analysis of variance.
Results: The baseline detection rates for the evening, intermediate and morning types were 14.93%, 56.5% and 28.57%, respectively. HAMD-17 scores were significantly lower at weeks 2, 4, 8, and 12 after treatment in patients with different concurrent phenotypes compared with those before treatment (P< 0.05). There were significant differences in gender, age, body mass index, whether depression was first-episode, type of medication, baseline-MEQ and baseline-SHAPS in the chronotype change group compared with the post-treatment chronotype unchanged group (p< 0.05). Logistic regression analysis showed that medication type (P=0.047), baseline MEQ (P=0.001) and baseline SHAPS (P=0.001) were risk factors for improvement in circadian rhythm after treatment for depression.
Conclusion: Circadian rhythm disturbances can be adjusted to a normal pattern with effective antidepressant therapy. The medication type, baseline MEQ and baseline SHAPS scores were the influencing factors for the recovery of circadian rhythm disorders.
Keywords: major depressive disorder, morningness–eveningness questionnaire, circadian rhythm, chronotype, antidepressant
Background
Depression is one of the most common psychiatric disorders and the leading cause of disability worldwide. The clinical features of depression mainly manifest as a significant and lasting loss of interest or emotional depression, accompanied by cognitive, behavioural, biological and somatic disorders.1 Depression prevalence rates have ranged from 10–77%.2 Although many researchers have shown that the pathogenesis is related to genetic, physiological or biological, it is difficult for antidepressants to be fully effective, and there is little progress in drug research.3 In addition, there are several studies that focus on psychological factors in the pathogenesis of depression.4 The primary drugs used in the treatment of depression are tricyclic antidepressants, monoamine oxidase inhibitors and selective serotonin reuptake inhibitors (SSRIs).5
Sleep problems and depression are highly comorbid conditions. A large number of studies have shown that there are obvious sleep disturbances and abnormal circadian rhythms during major depressive episodes.6 Circadian rhythm refers to physical, mental and behavioural changes throughout a 24-hour cycle, and it plays a central role in both mental and physical health.7 It has been reported that disturbances in circadian rhythms could be a unique clinical manifestation of mood disorders, and phase shift of circadian rhythms can serve as a marker for mood disorders.8 In recent years, there have been many hypotheses about the relationship between major depressive disorders and circadian rhythms. These hypotheses focus on the elaboration of the sleep process (slow-wave deficiency and slow-wave activity), the study of neurotransmitter systems (cholinergic and aminergic imbalance) or environmental behaviour factors (irregular work and rest patterns that lead to the disruption of the biological rhythm).9 Moreover, many studies have monitored the circadian rhythms of patients with major depressive episodes by measuring melatonin secretions at night and during intermediate sleep times. The results show that the sleep phase of patients with major depressive episodes was significantly delayed proving that circadian rhythms are closely related to major depressive episodes.10 Furthermore, many drugs used for the treatment of depression shift or stabilize circadian rhythms, which may be important for their therapeutic efficacy.11 A better understanding of the circadian rhythmicity of depression will help to identify the relationship between depression treatment and altered circadian rhythms, which can ultimately guide more accurate treatment decisions.
Although the link between the circadian rhythm system and depression has been well established, the basic biology of the interaction is far from being understood, and until now, the specific factors that affect circadian rhythm changes have not been clear. Our study analyzed the changes and influencing factors of circadian rhythms in patients with depression before and after treatment, aiming to provide new evidence and insights for clinical treatment strategies for depression.
Materials and Methods
General Information
A total of 154 patients with depression in 10 psychiatric hospitals of Zhejiang Province from March 1, 2019 to June 30, 2019 were selected as subjects, with an average age of 44.3 ±12.2, 45 males and 109 females. Inclusion criteria: (1) the diagnostic criteria for the major depressive episodes were in line with the International Classification of Diseases, Tenth Revision; patients were diagnosed with major depressive disorder (MDD) according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; (2) the Chinese version of the Mini International Neuropsychiatric Interview was used for diagnosis and screening; (3) patients with acute depressive episodes; both an initial episode and a recurrence were acceptable, and patients with recurrences had not been taking antidepressant medication and had not experienced convulsions, electrical spasms, or received physical therapy within two weeks prior to enrolment; (4) patients of Han ethnicity, with no gender restrictions, and between the ages of 18 and 65 years old; (5) patients that had signed the informed consent form. Exclusion criteria: (1) patients with other psychiatric disorders, such as schizoaffective psychosis, schizotypal (personality) disorder or bipolar depression; those with any other anxiety disorder as a main diagnosis within one year; patients with substance dependence or personality disorders; (2) patients with or carriers of hepatitis B or hepatitis C; patients with abnormal liver function, cirrhosis or active liver disease; (3) patients with severe heart, brain, kidney or endocrine organ diseases or other serious physical diseases; (4) previous standard treatment of agomelatine had failed, or the use of two or more antidepressants during the current episode had been ineffective following an appropriate course of treatment; (5) current major depressive episode had lasted more than two years; (6) patients with obvious suicide attempts or behaviours with a Hamilton Depression Rating Scale article 3 (for suicide) score ≥3; (7) women who were breastfeeding or pregnant; women who had fertility requirements during the study or could not take safe and effective contraceptive measures.
This study was approved by the ethics committee of the Third People’s Hospital of Huzhou City (ethics number: 2019 Ethics Review No. 028). All patients signed informed consent.
Study Design
This study was an observational study. The basic information and clinical data of the 154 patients included in the study were collected, including age, gender, body mass index, and whether it was the first episode of depression. On admission, the patients were assessed with MEQ scale, the 17-item Hamilton Depression Rating Scale (HAMD-17), Hamilton anxiety scale (HAMA), Snaith-Hamilton Pleasure Scale (SHAPS), multidimensional fatigue inventory-20 (MFI-20) and Pittsburgh sleep quality index (PSQI). According to the MEQ score, the circadian rhythms of all patients were divided into three phases, including morning type (early sleep and early awakening type), intermediate type (ordinary type) and evening type (late sleep and late awakening type). The circadian rhythm disorders of patients with depression were evaluated by comparing the baseline data of patients with three phases. According to the random number table method, all patients were given antidepressant therapy with agomelatine or SSRI for a period of 12 weeks. Administration time of different groups is related to chronotype. All patients were evaluated by the HAMD-17, HAMA, SHAPS, MFI-20, PSQI and MEQ scale at 2, 4, 8, and 12 weeks after treatment. Changes in circadian rhythms in depressed patients were assessed by comparing pre- and post-treatment HAMD-17 and MEQ scores. After 12 weeks of treatment, according to whether the circadian rhythm of patients changed at the end of the study, the patients were divided into chronotypes change group and non-change group. The differences of various indexes between the two groups were analyzed to explore the potential factors affecting the improvement of circadian rhythm in patients with depression before and after treatment. Potential factors with differences were selected as independent variables, and changes in the temporal phase of circadian rhythms were used as dichotomous variables, and we performed a Binary logistic regression analysis to explore the risk factors for circadian rhythm improvement.
Research Methods
The psychological scale was assessed by two physicians, mid-level or above, in the psychiatric department in each centre. Without knowing their grouping, patients were evaluated by a cross-blind method. The consistency test Kappa value was 0.89.
Morning and Evening Questionnaire (MEQ)
MEQ is often used to evaluate circadian rhythm.12 This questionnaire contains a total of 19 items. Each item is scored from 0 to 6 points, and the total score ranges from 16 to 86 points. Based on these scores, individuals were categorised as being a morning type (score of 59–86), an intermediate type (score of 42–58) or an evening type (score 16–41).
Snaith-Hamilton Pleasure Scale (SHAPS)
The Snaith-Hamilton-Pleasure-Scale (SHAPS) is a self-reported scale evaluating anhedonia for neuropsychiatric disorders.13 The SHAPS contains a total of 14 items, including interest/entertainment, social interaction, sensory experience and diet. Participants were required to score between 1 and 4 points according to the degree of their agreement with the happiness responses to different pleasant situations. The total score of the scale is between 14 and 56 points. The higher the total score, the more severe the anhedonia.
Multidimensional Fatigue Inventory-20 (MFI-20)
The MFI-2014 evaluated the fatigue status of the subjects from multiple perspectives. The scale is moderate in length and easy to understand. It includes 20 items in five dimensions: general fatigue, physical fatigue, reduced activity, reduced motivation and mental fatigue, generating a total score of 20–100 points. The higher the score, the higher the degree of fatigue.
Pittsburgh Sleep Quality Index (PSQI)
The PSQI15 was used to assess the sleep quality of the subjects during the previous month. It includes 19 self-evaluation and five other evaluation items, which are combined into seven factors: subjective sleep quality, time taken to fall asleep, sleep time, sleep efficiency, sleep disorder, hypnotic drugs and daytime function. Each factor is scored on a scale of 0 to 3, and the total score ranges from 0 to 21, with 7 being the boundary value of sleep quality. The higher the score, the worse the quality of sleep.
Hamilton Anxiety Scale (HAMA)
The HAMA16 was compiled by Max Hamilton in 1959 and is particularly suitable for the determining the severity of anxiety symptoms. The HAMA has 14 items, using a five-level scoring method of 0 to 4 points: (0) asymptomatic, (1) mild, (2) moderate, (3) severe, (4) extremely severe. No anxiety is present when the total score is less than or equal to 7, possible anxiety is present when the total score is between 8 and 14, positive anxiety is present when the total score is between 15 and 21, obvious anxiety is present when the total score is between 22 and 29 and serious anxiety is present when the total score is more than 29.
The 17-Item Hamilton Depression Rating Scale (HAMD-17)
The HAMD-1717 is an alternative scale that includes 17 items. Each item is scored with 0–2 points or 0–4 points, with a total score of 0–52 points. The higher the total score, the more severe the depression. A score of 0–7 indicates no depression, a score of 8–17 indicates mild depression, a score of 18–24 indicates moderate depression and a score of 25–52 indicates severe depression.
Statistical Analysis
SPSS 22.0 statistical software was used to process data. Continuous variables were described by means ± standard deviation (range) if they were normally distributed. Categorical variables are expressed as counts (percentage). Continuous variables were compared using the Student’s t-test or the Mann–Whitney U-test, depending on their distribution. Categorical variables were compared using the chi-squared (χ2) test or Fisher’s exact test. Binary logistic regression analysis was used to analyse the possible influencing factors of the circadian rhythm of patients with baseline depression; the baseline MEQ score was used as the dependent variable, and other baseline measurement results and demographic data were used as independent variables. The repeated-measures analysis of variance was performed to evaluate the changes in HAMD-17 and MEQ scores over time. When significance was indicated, a post hoc test with pairwise comparisons was applied. Bonferroni corrections were made to account for multiple comparisons. The test level α was 0.05. P<0.05 indicated a statistically significant difference.
Results
Circadian Rhythm (Time Pattern) of Patients with Depression
A total of 154 patients with depression were enrolled in this study. The baseline measure shows that the detection rates of evening, intermediate and morning types were 14.93% (n=23), 56.5% (n=87) and 28.57% (n=44), respectively. The baseline demographic data and clinical evaluation of patients with various types of depression are shown in Table 1.
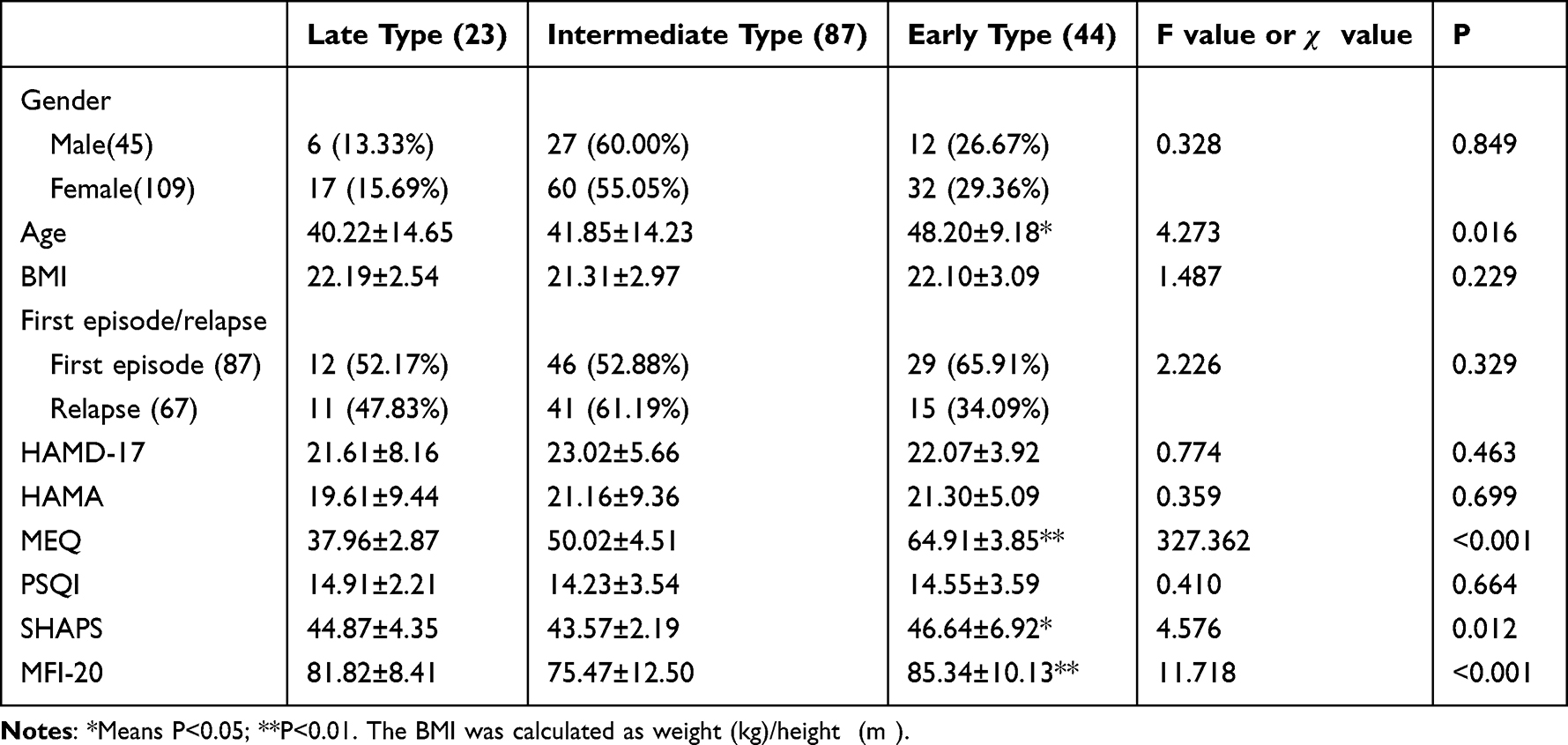 |
Table 1 Demographic Data and Clinical Evaluation of Patients with Depression of Different Time Types at Baseline: N (%) |
Morning type subjects were older than the intermediate and evening type subjects (F(2,0) = 7.987, P = 0.019; F(2,1) = 6.354, P = 0.009). The intermediate group had the lowest SHAPS and MFI-20 scores, and the morning group had the highest scores (P < 0.05). However, there were no statistically significant differences between the three groups of subjects in terms of demographic data, such as gender, body mass index and recurrence, or in terms of PSQI, HAMA and HAMD-17 scores (P > 0.05).
Changes of Circadian Rhythm in Patients with Depression Before and After Treatment
During the 12-week antidepressant treatment, the HAMD-17 scores of the three groups of subjects of different chronotypes decreased with the prolongation of treatment time (Table 2).
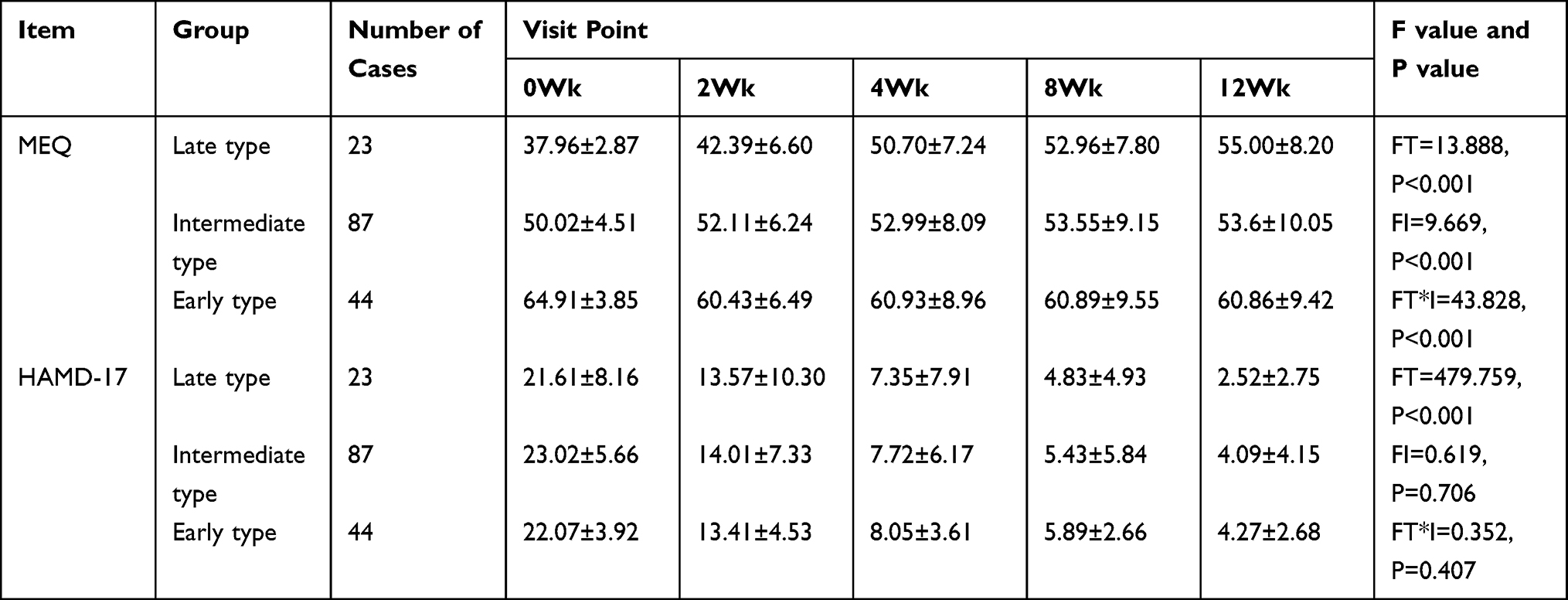 |
Table 2 MEq Score Trend of Three Groups of Subjects with Different Time Types |
During the 12-week antidepressant treatment, the MEQ scores of the three groups of subjects of different chronotypes also showed different changes with the prolongation of treatment time. The analysis of the variance of repeated measurements showed that there were statistically significant changes in MEQ scores within each group and between the three groups at five time points (FT = 13.888, P < 0.001; FI = 9.669, P < 0.001), and there was interaction between the time and different chronotypes (FT*I = 43.828, P < 0.001; see Table 2).
Data Differences Between Chronotypes Change Group and Non-Change Group
Patients were divided into change and non-change groups according to whether there was a shift in circadian rhythm pattern at the end of the study. Among the 154 patients, the number of patients with changes in chronotype after treatment was 75, and the number of patients with no changes was 79. Compared with the non-change group, the change group had significant differences in gender, age, body mass index, first-episode, Type of medication, baseline-MEQ and baseline-SHAPS. The difference was statistically significant (P<0.05) (Table 3).
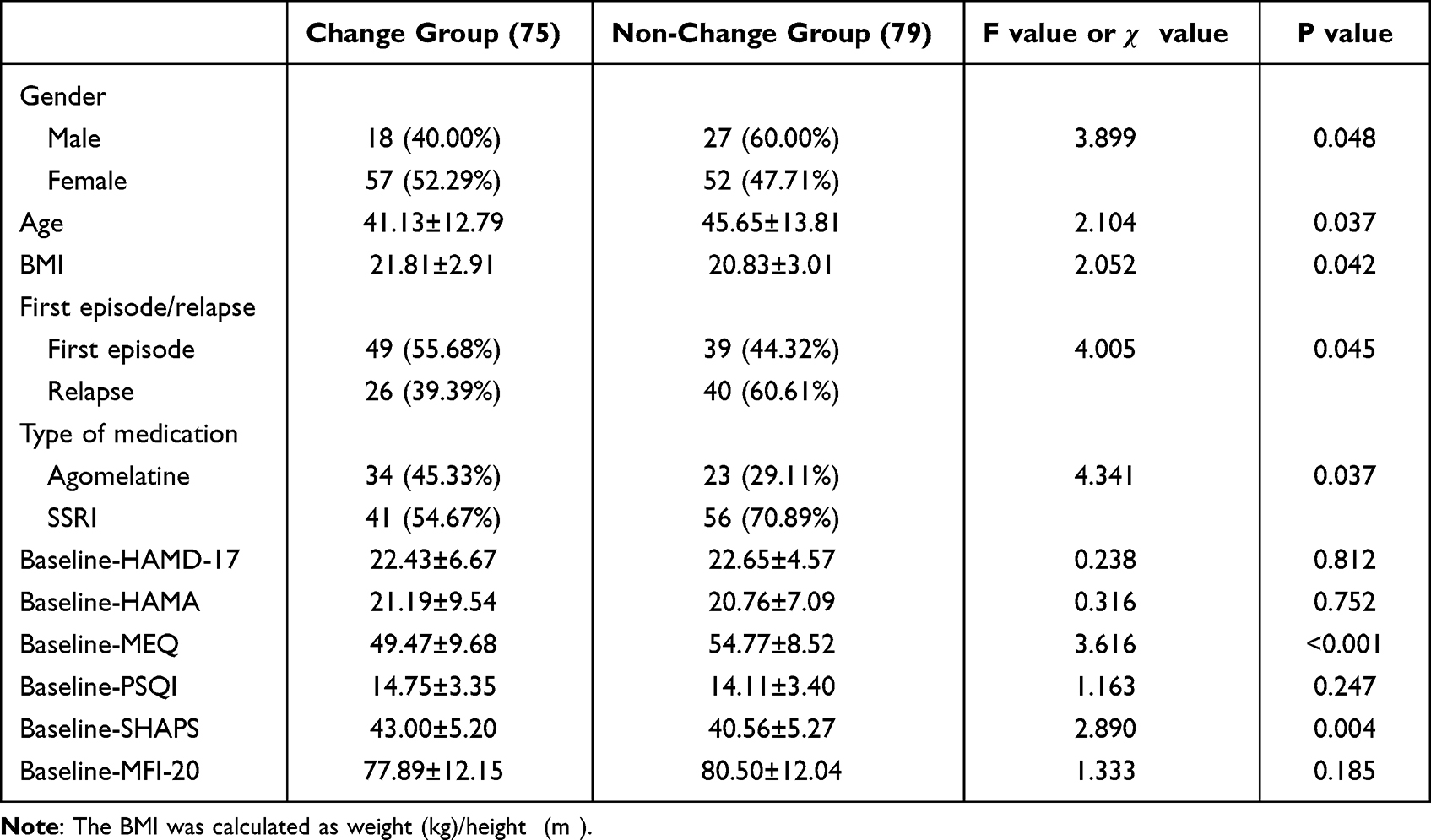 |
Table 3 Data Differences Between Chronotypes Change Group and Non-Change Group |
Influencing Factors for the Recovery of Circadian Rhythm Disorders in Patients with Depression
Binary logistic regression analysis was conducted. Whether the time pattern of circadian rhythm changes or not is taken as a binary variable (0 for those who have not changed their chronotypes, 1 for those who have changed their chronotypes), and gender, age, first episode determination (0 for the first episode and 1 for recurrence), body mass index, HAMD-17, HAMA scores and so on were used as the independent variables. The stepwise method was used when the independent variables were entered into the regression analysis. After excluding the influence of confounding factors and other ineffective factors, the final type of medication, a low baseline MEQ score and a high baseline SHAPS score were statistically significant. The results of the parameter estimation and hypothesis testing are shown in Table 4. After testing, the established logistic regression model was statistically significant (F = 26.405, P < 0.001).
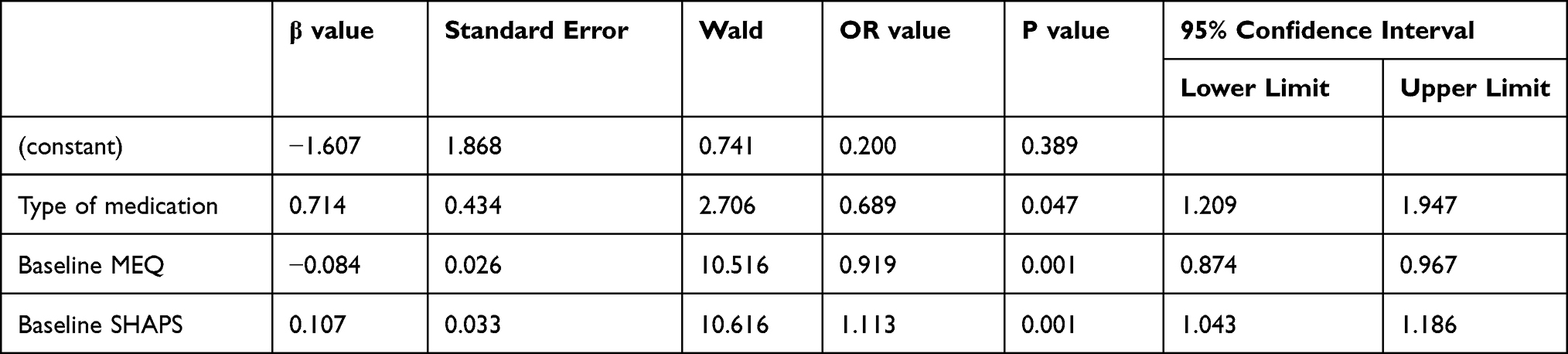 |
Table 4 Logistic Regression Model of Influencing Factors in Depressive Patients’ Circadian Rhythm Returning to Early Type |
The results showed that after three months of antidepressant treatment, for depressive patients with changes in circadian rhythm, type of medication, a low baseline MEQ score and a high baseline SHAPS score were all statistically associated with this return (β values were 0.714, −0.084 and −0.107; OR values were 0.689, 0.919 and 1.113; 95% CI values were 1.209–1.947, 0.874–0.967 and 1.043–1.186, respectively).
Discussion
There is a complex relationship between biological rhythms and emotions. Studies have shown that there is a correlation between changes in an individual’s inherent biological rhythms and the appearance of depressive symptoms.8,9 As an important clinical feature and pathophysiological mechanism of depression, biological rhythm disorders are closely related to the onset, clinical manifestation, social function, prognosis and recurrence of depression. With the relief of depressive symptoms, the sleep–wake cycle and biological rhythm disorders will also be gradually improved. This study is a multicentre study focusing on the Chinese population and it therefore provides further race-specific evidence on the relationship between antidepression therapy and circadian rhythm.
Research indicated that individuals show circadian rhythm differences depending on their chronotype or circadian typology (morning-, neither-, and evening-type).18 Previous surveys showed that in the general population aged 30 to 50, the detection rates of the late type, intermediate type and early type were 5.6%, 44.6% and 49.8%, respectively.19 In our study, the detection rates of the above-mentioned chronotypes were 14.93%, 56.5%, and 28.57% at baseline in the patients with depression included in the analysis, indicating that compared with the normal population, the patients with depression in the acute phase have obvious symptoms of abnormal circadian rhythm. Our baseline data showed that there was no statistical difference in HAMD-17 score and HAMA total score among the three groups of patients with different chronotypes, but in terms of SHAPS total score and MFI-20 total score, the early type group > late group Temporal group > Intermediate temporal group. This suggests that early formers have less pleasure and more fatigue. This circadian rhythm disorder characterized by early awakening may be greatly affected by factors such as light. Research shows that light in the morning hours will produce a phase advance in the circadian rhythm.20 Previous studies have suggested that the ability of an individual’s biological rhythms to synchronise with natural rhythms is related to age.21 In this study, the comparison of average age of patients with depression at the baseline during the onset period indicated the individuals who were the morning type were older than those who were the intermediate type who, in turn, were older than individuals who were the evening type. The older the patients, the more likely they were to wake up earlier, suggesting that age is also an important factor driving circadian phase changes.
According to existing research results, the chronotypes that is more likely to have depressive symptoms is still uncertain. Most scholars believe that individuals who are the evening type are more prone to impetuosity, anger, depression, anxiety, nightmares and other behavioural and emotional abnormalities.22–24 However, some researchers believed that those who are intermediate or morning types are more prone to having depressive symptoms because individuals who are evening types are more likely to express their feelings than individuals who are morning types.25 In fact, some studies have proved that circadian orientation is closely related to personality traits.26 The morning type is related to stability, which includes the domains of emotion (neuroticism), sociality (agreeableness) and motivation (conscientiousness). Compared with the morning type, the evening type is more inclined to the domains of behaviour (extraversion) and cognition (openness).27 Therefore, paying close attention to the circadian rhythm of patients plays an important role in the treatment and prevention of depression.
During the 12-week antidepressant treatment of this study, while the subjects’ depressive symptoms tended to be alleviated, changes in patients’ MEQ scores and corresponding shifts in circadian rhythm patterns, indicating that the close relationship between depression and circadian rhythm. Our results were similar to those of Pail et al, who demonstrated that people with circadian rhythm disorders, especially those who get less sleep at night, are prone to depression.28 When an individual’s inherent biological rhythm is disrupted, the original dynamic balance of the internal environment, such as neurological, immune, and endocrine functions, is also altered, which may lead to mental symptoms such as depression and anxiety, as well as hypertension, diabetes, and other physical diseases.29 Conversely, effective treatment of depressive symptoms and psychiatric disorders in patients with depression can have a positive effect on the patient’s biological rhythm. Our results showed that after drug treatment, the patients’ depressive symptoms were relieved, and the MEQ scores of the morning and intermediate types also tended to be stable, while the MEQ scores of the night type maintained an upward trend. It can be seen that there is definitely a correlation between changes in an individual’s internal biological rhythm and the appearance of depressive symptoms.
To investigate the risk factors affecting the recovery of circadian rhythm in depressed patients after treatment, we performed a univariate analysis of the baseline data of two groups of patients with and without a shift in circadian rhythm after treatment. Our results showed that there were significant differences between the two groups with respect to these aspects: age, whether or not first-episode depression, medication regimen, baseline MEQ and baseline SHAPS. This implies that age, whether first-episode depression, medication type, baseline MEQ and baseline SHAPS may be potential influencing factors for circadian rhythm improvement after treatment in depressed patients. Disturbances of biological rhythms can cause major depressive episodes or recurrences in patients. Repeated major depressive episodes will further affect hypothalamus regulation on circadian rhythms, making patients more prone to circadian rhythm disorders30,31 and leading to sleep–wake cycle disruption and mood changes.32 We analyzed potential possible influences through a binary logistic regression model, and the potential factors that eventually entered the model were medication type, baseline MEQ, and baseline SHAPS. Interestingly, medication type was a risk factor for circadian rhythm recovery after treatment for depression. Different drugs have different mechanisms of action in the treatment of depression, which may lead to different effects on the improvement of circadian rhythm in patients with depression.
Furthermore, as the use of social media increases, the risk of depression grows. The changes in modern human lifestyles and the widespread use of electronic devices have led to increasing “social jet lag”, which has caused circadian rhythm disorders, incidences of depression and other emotional behavioural abnormalities.33 This may help explain the increasing prevalence of depression over the last 10 years. Therefore, strengthening biological rhythm adjustments in the normal population and managing biological rhythms of patients with depression may be important for the prevention and treatment of depression.
There are some limitations of this study. First, more relevant factors should be included for analysis, including the presence of night shifts, the use of electronic devices at night, and the presence of comorbid underlying physical illnesses. Secondly, although the MEQ scores of the early and intermediate hour types were stable at the end of the 12th week, the MEQ scores of the late hour type showed a continuous improvement, suggesting that this group of patients should be followed up for a longer period of time. Thirdly, the individuals at high risk of obstructive sleep apnea in PSQI were not excluded from the study. They did not respond well to the treatment plan of this study, and this part of patients would cause bias in the results. Finally, lack of medication information for patients, some drugs, such as glucocorticoids, may cause depression and sleep disorders at home.
Conclusions
Circadian rhythm disturbances are common in patients with major depressive disorder and can be adjusted to a normal pattern with effective antidepressant therapy. Type of medicine, baseline MEQ and baseline SHAPS scores were the influencing factors for the recovery of circadian rhythm disorders.
Abbreviations
MDD, major depressive disorder; MEQ, morningness-eveningness questionnaire; HAMD-17, 17-item Hamilton depression rating scale; MFI-20, multidimensional fatigue inventory; TCAS, treatment of depression are tricyclic antidepressants; MAOIs, monoamine oxidase inhibitors; SSRIs, selective serotonin reuptake inhibitors; CGI-S, clinical global impression severity scale; ALT, alanine aminotransferase; HAMA, Hamilton anxiety scale; SHAPS, Snaith–Hamilton pleasure scale; PSQI, Pittsburgh sleep quality index; AST, aspartate aminotransferase.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Huzhou Third Municipal Hospital. All patients signed an informed consent form for inclusion in the study.
Funding
Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (2018KY789); Nonprofit Applied Research Project of Huzhou Science and Technology Bureau (2017GY50, 2021GYB16).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Polyakova M, Beyer F, Mueller K, et al. Serum BDNF levels correlate with regional cortical thickness in minor depression: a pilot study. Sci Rep. 2020;10(1):14524. doi:10.1038/s41598-020-71317-y
2. Rezapour J, Schuster AK, Nickels S, et al. Prevalence and new onset of depression and anxiety among participants with AMD in a European cohort. Sci Rep. 2020;10(1):4816. doi:10.1038/s41598-020-61706-8
3. Patel SS, Mehta V, Changotra H, et al. Depression mediates impaired glucose tolerance and cognitive dysfunction: a neuromodulatory role of rosiglitazone. Horm Behav. 2016;78:200–210. doi:10.1016/j.yhbeh.2015.11.010
4. Van Someren EJW. Brain mechanisms of insomnia: new perspectives on causes and consequences. Physiol Rev. 2021;101(3):995–1046. doi:10.1152/physrev.00046.2019
5. Juang HT, Chen PC, Chien KL. Using antidepressants and the risk of stroke recurrence: report from a national representative cohort study. BMC Neurol. 2015;15(1):86. doi:10.1186/s12883-015-0345-x
6. Yan R, Tao S, Liu H, et al. Abnormal alterations of regional spontaneous neuronal activity in inferior frontal orbital gyrus and corresponding brain circuit alterations: a resting-state fMRI study in somatic depression. Front Psychiatry. 2019;10:267. doi:10.3389/fpsyt.2019.00267
7. Zhou L, Xiao X, Zhang Q, et al. Dietary genistein could modulate hypothalamic circadian entrainment, reduce body weight, and improve glucose and lipid metabolism in female mice. Int J Endocrinol. 2019;2019:2163838. doi:10.1155/2019/2163838
8. Cho CH, Lee T, Kim MG, et al. Mood prediction of patients with mood disorders by machine learning using passive digital phenotypes based on the circadian rhythm: prospective observational cohort study. J Med Internet Res. 2019;21(4):e11029. doi:10.2196/11029
9. Harvey AG, Kaplan KA, Soehner AM. Interventions for sleep disturbance in bipolar disorder. Sleep Med Clin. 2015;10(1):101–105. doi:10.1016/j.jsmc.2014.11.005
10. Bromundt V. Störungen des Schlaf-Wach-Rhythmus bei psychiatrischen Erkrankungen [Circadian rhythm sleep disorders in psychiatric diseases]. Ther Umsch. 2014;71(11):663–670. German. doi:10.1024/0040-5930/a000607
11. Ketchesin KD, Becker-Krail D, Mcclung CA. Mood-related central and peripheral clocks. Eur J Neurosci. 2020;51(1):326–345. doi:10.1111/ejn.14253
12. Prakash P, Jayan A, Prabhu P. Effects of diurnal changes on temporal processing in morning-type and evening-type individuals with normal hearing. Eur Arch Otorhinolaryngol. 2021;278(8):3073–3079. doi:10.1007/s00405-021-06605-y
13. Liu WH, Wang LZ, Zhu YH, et al. Clinical utility of the Snaith-Hamilton-pleasure scale in the Chinese settings. BMC Psychiatry. 2012;12(1):184. doi:10.1186/1471-244X-12-184
14. Tian J, Hong JS. Validation of the Chinese version of multidimensional fatigue inventory-20 in Chinese patients with cancer. Support Care Cancer. 2012;20(10):2379–2383. doi:10.1007/s00520-011-1357-8
15. Han Q, Liu B, Lin S, et al. Pittsburgh sleep quality index score predicts all-cause mortality in Chinese dialysis patients. Int Urol Nephrol. 2021;53(11):2369–2376. doi:10.1007/s11255-021-02842-6
16. Thompson E. Hamilton Rating Scale for Anxiety (HAM-A). Occup Med. 2015;65(7):601. doi:10.1093/occmed/kqv054
17. Nixon N, Guo B, Garland A, et al. The bi-factor structure of the 17-item Hamilton depression rating scale in persistent major depression; dimensional measurement of outcome. PLoS One. 2020;15(10):e0241370. doi:10.1371/journal.pone.0241370
18. Capella MDM, Martinez-Nicolas A, Adan A. Circadian rhythmic characteristics in men with substance use disorder under treatment. Influence of age of onset of substance use and duration of abstinence. Front Psychiatry. 2018;9:373. doi:10.3389/fpsyt.2018.00373
19. Chung JK, Lee KY, Kim SH, et al. Circadian rhythm characteristics in mood disorders: comparison among bipolar I disorder, bipolar II disorder and recurrent major depressive disorder. Clin Psychopharmacol Neurosci. 2012;10(2):110–116. doi:10.9758/cpn.2012.10.2.110
20. Alkozei A, Dailey NS, Bajaj S, et al. Exposure to blue wavelength light is associated with increases in bidirectional amygdala-DLPFC connectivity at rest. Front Neurol. 2021;12:625443. doi:10.3389/fneur.2021.625443
21. Salvatore P, Indic P, Murray G, et al. Biological rhythms and mood disorders. Dialogues Clin Neurosci. 2012;14(4):369–379. doi:10.31887/DCNS.2012.14.4/psalvatore
22. Bei B, Ong JC, Rajaratnam SM, et al. Chronotype and improved sleep efficiency independently predict depressive symptom reduction after group cognitive behavioral therapy for insomnia. J Clin Sleep Med. 2015;11(9):1021–1027. doi:10.5664/jcsm.5018
23. Dalton EJ, Rotondi D, Levitan RD, et al. Use of slow-release melatonin in treatment-resistant depression. J Psychiatry Neurosci. 2000;25(1):48–52.
24. Knapen SE, Gordijn MC, Meesters Y. The relation between chronotype and treatment outcome with light therapy on a fixed time schedule. J Affect Disord. 2016;202:87–90. doi:10.1016/j.jad.2016.05.009
25. Schlarb AA, Sopp R, Ambiel D, et al. Chronotype-related differences in childhood and adolescent aggression and antisocial behavior--a review of the literature. Chronobiol Int. 2014;31(1):1–16. doi:10.3109/07420528.2013.829846
26. Adan A, Archer SN, Hidalgo MP, et al. Circadian typology: a comprehensive review. Chronobiol Int. 2012;29(9):1153–1175. doi:10.3109/07420528.2012.719971
27. Deyoung CG, Hasher L, Djikic M, et al. Morning people are stable people: circadian rhythm and the higher-order factors of the big five. Pers Individ Dif. 2007;43(2):267–276. doi:10.1016/j.paid.2006.11.030
28. Pail G, Huf W, Pjrek E, et al. Bright-light therapy in the treatment of mood disorders. Neuropsychobiology. 2011;64(3):152–162. doi:10.1159/000328950
29. Chiu WH, Yang HJ, Kuo PH. Chronotype preference matters for depression in youth. Chronobiol Int. 2017;34(7):933–941. doi:10.1080/07420528.2017.1327441
30. Depner CM, Stothard ER, Wright KP
31. Müller MJ, Cabanel N, Olschinski C, et al. Chronotypes in patients with nonseasonal depressive disorder: distribution, stability and association with clinical variables. Chronobiol Int. 2015;32(10):1343–1351. doi:10.3109/07420528.2015.1091353
32. Gaspar-Barba E, Calati R, Cruz-Fuentes CS, et al. Depressive symptomatology is influenced by chronotypes. J Affect Disord. 2009;119(1–3):100–106. doi:10.1016/j.jad.2009.02.021
33. Orchard F, Gregory AM, Gradisar M, et al. Self-reported sleep patterns and quality amongst adolescents: cross-sectional and prospective associations with anxiety and depression. J Child Psychol Psychiatry. 2020;61(10):1126–1137. doi:10.1111/jcpp.13288
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association Between Antidepressant Treatment and Heart Rate Deceleration Capacity in Patients With Mood disorders—A Potential New Predictor of Sudden Cardiac Death
Okayasu H, Sugawara N, Fujii K, Ozeki Y, Yasui-Furukori N
Neuropsychiatric Disease and Treatment 2025, 21:597-607
Published Date: 18 March 2025
Optimizing Identification and Management of Depression in Neurological Diseases: A Narrative Review and Expert Perspective
Bartova L, Beuster ML, Bonetti B, Maina G, Morgado P, Nyberg J
Neuropsychiatric Disease and Treatment 2026, 22:575685
Published Date: 1 May 2026