")
Back to Journals » Infection and Drug Resistance » Volume 15
Study of the Drivers of Inappropriate Use of Antibiotics in Community Pharmacy: Request for Antibiotics Without a Prescription, Degree of Adherence to Treatment and Correct Recycling of Leftover Treatment
Authors Zarauz JM, Zafrilla P , Ballester P, Cerda B
Received 28 May 2022
Accepted for publication 20 September 2022
Published 23 November 2022 Volume 2022:15 Pages 6773—6783
DOI https://doi.org/10.2147/IDR.S375125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
José María Zarauz,1 Pilar Zafrilla,2 Pura Ballester,2 Begoña Cerda2
1Health Sciences PhD Program, Faculty of Health Sciences, Catholic University of Murcia, Guadalupe, Murcia, Spain; 2Faculty of Health Sciences, Catholic University of Murcia, Guadalupe, Murcia, Spain
Correspondence: Pilar Zafrilla, Faculty of Health Sciences, Catholic University of Murcia, Los Jerónimos Campus, Guadalupe, Murcia, Spain, Email [email protected]
Introduction: The WHO considered antibiotic resistance as 1 of the 10 greatest threats to global health in 2019. The inappropriate and indiscriminate use of antibiotics, together with the lack of new therapeutic alternatives, may eradicate their effectiveness in the closest future.
Objective: The general objective is to analyze the different causes attributable to patients, providers and pharmacists that could be drivers of irrational use of antibiotics, and responsible for the appearance of bacterial resistance, in community pharmacies. To this end, the different processes or indicators were studied: patients’ requests of antibiotics at the pharmacy, their degree of adherence, satisfaction with the prescribed treatment and antibiotics’ surplus recycling.
Methods: This study was observational, descriptive, and cross-sectional, carried out in 2 pharmacy offices, including 333 participants. At the time of dispensing, first phase, surveys to collect patients’, providers’ and pharmacists’ data were carried out over the counter. The second phase, with the aim of checking adherence, degree of satisfaction and recycling.
Results: There were 333 requests for antibiotic regardless prescription availability, 17% of the patients requested an antibiotic without having one. 38% of patients did not have full adherence to antibiotics. Exploring non-adherence reasons, 24% forgot to take the treatment, 2% experienced adverse effects; 8% improved infection symptoms and 21% had problems to follow schedule. Regarding the recycling habits, 57% of patients had leftover treatments at home, but only 11% recycled it. 10% of medical prescriptions were forced by the patient, and significant gender differences were observed in adherence and knowledge of treatment.
Conclusion: The results of this study suggested that there may be a significant level of antibiotic inappropriate use locally, potentially related to patients’ sex, finding significant deficiencies in prescription by doctors, in the dispensing act carried out in community pharmacies, and finally in patient compliance with treatment.
Keywords: drug resistance, anti-bacterial agents, adherence, pharmacy
Introduction
In 2019, antibiotic resistance was included in the list of the 10 greatest threats to global health, placing it on the same level as climate change, HIV or Ebola by the WHO.1
The inappropriate and indiscriminate use of antibiotics, together with the lack of new therapeutic alternatives,2 may turn them into ineffective treatments for serious infections by year 2050 according to some authors.3 Aberrant forms of usage favor the appearance of bacteria antibiotic resistant, as they can alter their genome to reduce their sensitivity to treatment. This phenomenon, if not stopped, could lead to a post-antibiotic era, where surgery could entail death risk, and health alerts in the food industry would be usual.4,5
In Spain, 3000 people die every year due to antibiotic resistance (ABR),6 in Europe this figure rises to 33,000.7 Up to date, according to the largest study carried out worldwide, 1,200,000 people died in 2019 for ABR. The leading infections underlying were in lower respiratory tract, bloodstream, and intra-abdominal ones.3 If current trend continues, it is estimated that it will rise to 10 million deaths per year by 2050, even surpassing cancer death rates, becoming world’s leading cause of death.8
According to the latest data from the European Center for Disease Prevention and Control (ECDC), in the European ranking of antibiotic consumption, Spain ranks 5th in ambulatory prescriptions and 14th in hospitals (2019).9 A study carried out in Spain determined that more than half of the patients (53.2%) did not have enough knowledge to ensure a correct antibiotic use.10
In addition, the complacent attitude of the prescriber towards the patient, the absence of rapid sensitivity tests to antibiotics contribute to the inappropriate use of them.11,12
All data highlight the urgent need for informative campaigns and monitoring the correct use of antibiotics. The cooperation among governments, pharmaceutical industries, providers, and pharmacists is essential to raise awareness among the population about the real problem.13 In October 2016, all 193 UN member states signed a global agreement to tackle ABR.14 The European Commission issued guidelines for prescribers, pharmacists, and patients.15
In Spain, which in antibiotic consumption ranks fifth place among European Union countries.9 Ministry of Health launched the awareness campaign “You can help prevent antibiotic resistance” of the National Antibiotic Resistance Plan (PRAN) in which patients are recommended to purchase antibiotics at the pharmacy, always with prescription; respect the indicated administration guidelines; not store antibiotics’ surplus at home and recycle them at Pharmacy Office.16
The general aim of this study is to analyze the different causes attributable to patients that could be drivers of irrational use of antibiotics, responsible for the appearance of ABR, in pharmacy offices. To this purpose, the different processes or indicators were studied: requesting antibiotics at the pharmacy, degree of adherence and satisfaction with the prescribed treatment and antibiotics surplus recycling habits by the patient. As a secondary objective, we checked whether the prescriptions carried out by the different practitioners and dispensations by pharmacists were compliant with the European Commission guidelines.15
Methods
The design was an observational, descriptive, and cross-sectional study.
Study Population
It was carried out in 2 pharmacy offices located in Águilas (Murcia), during 10-months. Data collection period was from March 2021 to January 2022. Inclusion criteria: all patients or caregivers attending to the 2 pharmacy offices requesting antibiotic treatment, with or without prescription. Minors were included, provided that the parents or legal guardian gave their consent. Exclusion criteria: people who were neither patient nor caregiver; patients who did not sign their informed consent, complying with the Declaration of Helsinki; patients who were not in optimal conditions to complete the evaluation tests or surveys (due to illiteracy, not understanding the language, cognitive impairment and visual or writing disability).
Study Procedure
The Research Project was approved by the UCAM Ethics Committee, the code of which is CE042003. All study participants were given the study information sheet and signed the informed consent form.
In the first phase, during dispensations, 333 surveys were carried out to collect patients’, prescribers’, and pharmacists’ data. All the information was collected by pharmacists previously trained in the matter, through the Responsible Use of Antibiotics course, accredited by the General Council of the College of Pharmacists of Spain. In addition, the principal investigator (JMZ) gave guidelines to follow when completing the questionnaires, to avoid possible intra- or inter-examiner errors. The second phase was a telephone interview done after 15 days, with the aim of checking patients’ adherence, degree of satisfaction and recycling intentions. Participants who did not complete the second interview were only included in the demographic results.
Study Variables
First phase: carried out at the time of dispensing and data are collected on the patient/caregiver. The questionnaire for data collection is the one used in the General Protocol of the I National Pharmaceutical Care Program for the Rational Use of Antibiotics, see Annex 1.17
Patient and Caregiver Variables
The socio-demographic data of the patient; the treatment requested and if they brought providers’ prescription; whether they know the antibiotics’ indication; and their degree of treatment knowledge at that time: posology, precautions and conservation; if they would store at home or recycle the surplus if any; awareness of the current ABR problem; reason for not having a prescription; patient’s action if not dispensing an antibiotic without a prescription.
Variables Related to Prescriber
Type (provider, dentist, veterinarian or podiatrist); type of prescription (National Health System, Mutual, Official Private or individual); correct completion of the prescription, in relation to the data: whether the prescribed medicine is insufficient, adjusted or surplus according with the treatment duration indicated; the antibiotic prescribed and type of infection diagnosed; the diagnostic method used; if it is an induced prescription (forced by the patient); and administration schedule has been explained to the patient.
Variables Relating to the Pharmacist
If the requested medicine was dispensed according to prescription availability; if patient was informed about administration schedule, possible interactions, adverse effects, contraindications, and antibiotic storage conditions; and if rational use of antibiotics was encouraged to avoid resistance; and if recycling possibility was recommended. Antibiotic dispensing guidelines from previous studies conducted in Spain were used for this purpose.17 Dispensing followed a protocol proposed by the Ministry of Health through the PRAN.18
Second Phase
After 15 days, patient-related variables of adherence to treatment, degree of satisfaction and treatment surplus recycled were checked.
Adherence
To assess adherence, the Morisky-Green test was used.19 This questionnaire is already translated and validated for use in Spanish.20 It consists of 4 contrasting questions with a dichotomous yes/no response, where it allows to find out quickly and easily whether the patient is adherent or not.
Satisfaction
The degree of satisfaction was measured using the questionnaire Treatment Satisfaction Questionnaire with Medication (TSQMH) which explores 4 dimensions: effectiveness, adverse effects, ease, and comfort of use.21
Statistical Analysis
Quantitative parametric data are presented as mean ± standard deviation (SD) while median (interquartile range) was used for non-parametric data. Comparisons for continuous or categorical data between two groups were conducted using an independent t-test or chi-square test (or Fischer exact test), respectively, to explore potential differences among groups related to sex. A p ≤ 0.05 was considered statistically significant. In all cases, multiple testing was adjusted using Bonferroni correction. All statistical analyses were carried out with the use of R 3.2.0 version. All the data management, storage and graph creation were performed using Excel Version 19.0 (Microsoft, USA) and a simple and affordable color code in tables and graphs.
Results
Study Population
The total number of participants in the study is 333. Of these, 273 had a prescription (83%) and 60 did not (17%). Of the 273 patients who brought the prescription, 246 completed the second survey after 15 days (90%). The rest of the population variables can be seen in Table 1. The demographic variables corresponding to the 27 participants who did not answer the second survey (10%) were used only for the first part of the study results. However, they were not considered as participants in the second phase of the study: the calculation of the degree of adherence, satisfaction with the antibiotic treatment, or recycling of the excess treatment.
 |
Table 1 Characteristics of the Study Population |
Results of Patient-Related Variables
Our study shows that 38% of patients do not have full adherence to the antibiotic treatment prescribed by their provider, being omission and timing the main causes (Figure 1).
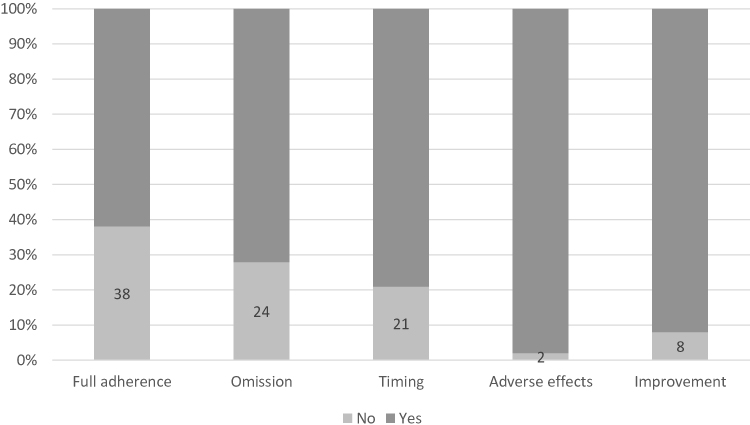 |
Figure 1 Degree of patient adherence to antibiotic treatment and reasons for non-adherence. |
Regarding the results related to the degree of satisfaction with the treatment, the patients expressed a high degree of satisfaction according to the TSQMH Test: The effectiveness obtained an average score of 6 out of 7, which means a “very satisfied” status. Adverse effects were 4 out of 5, meaning “little discomfort”. Ease of planning medication schedule 6 out of 7, “very easy”. Finally, the comfort of use in its current form, 5 out of 7, “easy”.
It was also observed that 17% of the patients request antibiotic treatment without a doctor’s prescription. From them, 90% had the intention of self-medication, 4% stated that they had been prescribed it orally and 6% that the prescription quantity was insufficient, and they needed more antibiotic to finish the treatment (Figure 2). 27% of patients without prescription accept referral to a doctor, 43% accept an alternative treatment and 30% reject both alternatives and went to another pharmacy office.
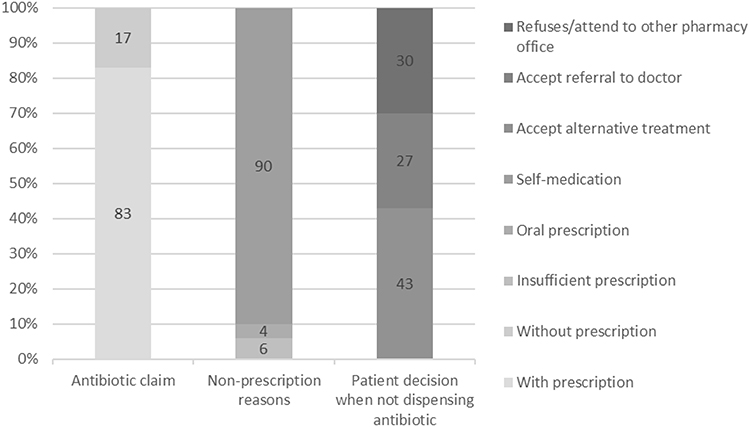 |
Figure 2 Antibiotics request in pharmacy. |
Regarding recycling habit of antibiotic surplus treatment, 74% of patients were not aware that they should recycle it. After 15 days, 57% of patients had leftover treatment, and only 11% had recycled it.
The Phase 1 survey conducted shows the degree of patient knowledge regarding antibiotic treatment (Table 2). When considering the influence of sex variable on the results, we found significant differences, females had higher medication knowledge than men in the following items: (a) medication precautions, considerations, and side effects (p = 0.043); (b) medicine conservation (p = 0.017). When evaluating patients’ adherence to drug administration timing, significant differences between males and females were found (p = 0.006), being women more compliant with adherence to medication schedule than men. Finally, according to participants’ gender the habits of recycling the surplus medicine were different, women were prescribed more accurately than men, the surplus of medication occurred on fewer occasions in female patients (p = 0.004).
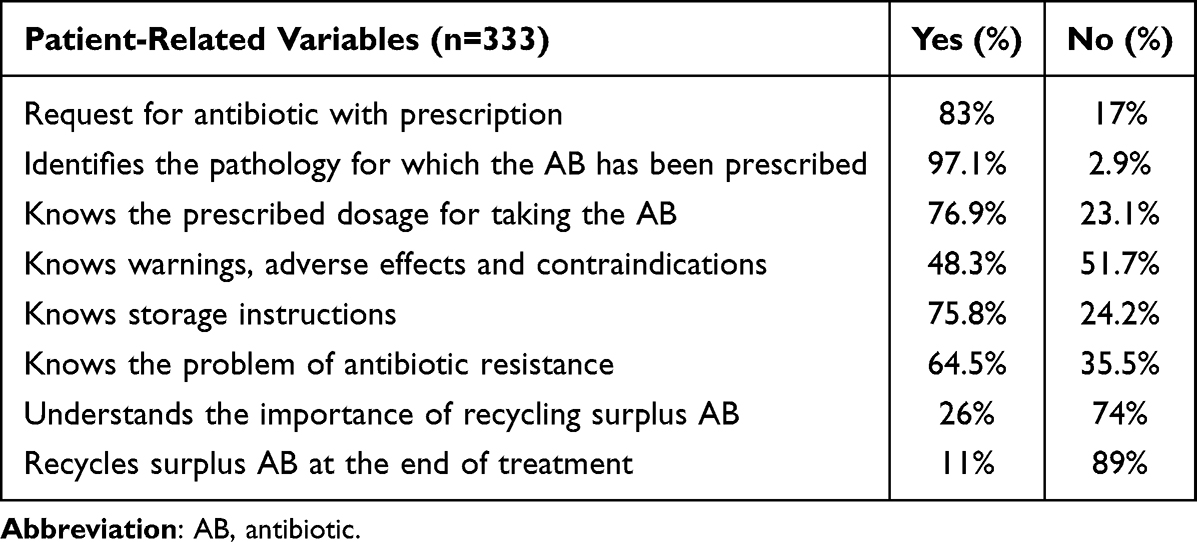 |
Table 2 Patient-Related Variables |
Results of the Variables Related to the Prescribing Physician
Most antibiotic prescriptions correspond to practitioners (78%), followed by dentists 18% and finally veterinary prescriptions for use in pets account for 4%. Of all prescriptions, 66% correspond to social security; 27% were private prescriptions and 7% from mutual insurance companies.
The quantity reflected in the prescription was insufficient in 11% of the cases to comply with the indicated treatment duration, in 36% of the cases it was perfectly adjusted and in 53% of the prescriptions there was a treatment excess (Table 3).
 |
Table 3 Variables Relating to the Physician Prescribing the Antibiotic |
Results of the Variables Relating to the Dispensing Pharmacist
Following the guidelines, 100% of the antibiotics dispensed have been on prescription (Table 4).
 |
Table 4 Variables Relating to the Dispensing Pharmacist |
Discussion
The irrational and excessive use of antibiotics is the main cause of the increase in bacterial resistance, this is a clearly established fact.22 For this reason, in this study we want to jointly analyze the drivers of the inappropriate use of antibiotics by doctors, pharmacists and patients in order to have a global vision of the problem. Results in this work highlight the different causes by which patients may be responsible for the appearance of bacterial resistance during their pharmacological treatment. The main reason for the inadequate use of antibiotics is the lack of adherence to treatment.
In our study, 38% of patients showed a lack of adherence when assessed using Morisky-Green test. Our results are in line with those observed in the Incumat study,23 carried out in two emergency rooms in Spain. In this study, a lack of adherence of 33% was recorded, using the same questionnaire. Forgetfulness was the main reason for non-adherence to treatment (24%), a result that matches with what authors described in the Incumat study.23 Kardas and collaborators published a meta-analysis where they reviewed 2848 articles and observed that 38% of patients were nonadherent, higher percentages were reached when adherence was assessed by other methods rather than Morisky-Green.24 Furthermore, if adherence to antibiotic treatment is assessed by an objective monitoring technique that records each opening of the medication package (MEMS), only 30% of patients had excellent adherence, which could be due to a trend of overestimate adherence when a self-reported method is used.25 Other groups explored also adherence with objective measures, Navarro-Gómez and collaborators, assessed adherence by determining the serum values of the antibiotic with liquid chromatography. They observed that 48% of the patients had not correctly complied with the prescription guidelines.26
Chen et al27 analyzed adherence to antibiotic treatment and observed that 60% of patients were non-adherent, due to several factors such as demographics, type of disease, or knowledge of antibiotic treatment. Lack of knowledge about antibiotic treatment showed a higher relationship with non-adherence. This result coincides with that observed in our study at the time of dispensing. In addition to non-adherence, we observed high self-medication rates by patients. This increase is related to the requests for antibiotics without prescription and the surplus antibiotics stored in households. Regarding patient satisfaction, the results showed a very good evaluation in terms of effectiveness, adverse effects, easiness, and comfort of use. A total of 33% of patients did not comply with the indicated dosage. Despite these results, the ease of planning the different antibiotic doses was rated as “very easy”. This fact could be an indicator of the lack of awareness of the current population of the problem of antimicrobial resistance.
In line with our results, the research group lead by Vega-Cubillo, found significant differences in adherence related to patient sex, where women were more adherent to their antibiotic treatments than men.23
Among the results obtained, we found that more than a third of the patients underused antibiotic treatment and despite this, they resolved their health problem. Numerous studies in recent years, such as the one by the group led by Spellberg, have shown that short-term antimicrobial therapies (3 to 5 days) are at least as effective as those lasting 7 to 14 days.28 However, it remains an underused tool by clinicians that will improve adherence compliance and save medical costs.28,29
The Law of Guarantees and Rational Use of Medicines and Health Products, approved in July 2006, classifies as a serious offense, in its article 101.16, “dispensing medicines or health products without a prescription when it is required”.30 In our study, 17% of the patients who requested antibiotic treatment did not have a prescription. This result could be explained by the fact that the study was carried out in two seaside pharmacies, where the population triples during the summer months, which may account for the greater difficulty of the displaced patient to get an appointment with the provider. However, previous publications have described higher rates, such as the observed by Salar31 were a 23% of requests for oral antibiotics were without a prescription. What is more, a recent survey among 1600 pharmacists in the Community of Madrid in 2019 showed that 99% had been asked for an antibiotic without a prescription during the last year.32 This result is higher than what was observed by Molinero and collaborators, with only a 5% of antibiotics without prescription request.33 The population is increasingly aware of the need for a medical prescription for the dispensing of antibiotics in pharmacies.
After completing the treatment prescribed by the doctor, the surplus must be taken to the Punto Sigre that we find in the pharmacy. In Spain, all medicine residues are destroyed, according to the Spanish drug regulatory Agency for Medicines and Health Products (AEMPS) legislation on drug donations.
74% of patients were unaware about of the importance of recycling surplus treatment, and their intention was to store it at home. A random survey of 1000 Spanish households found that 37% of them had one or more packages of antibiotics stored, but only 30% were for an active treatment.34 The research group lead by Arias-Puente, described that 35% of patients attending the pharmacy office had antibiotics in their first-aid kit.35
56% of patients had leftover treatment and only 11% recycled it after the Phase 2 completion. Even data was collected during the COVID-19 public health emergency, Spanish pharmacies remained open, so nothing prevented the patient from recycling their leftover treatment. The high percentage of patients with leftover treatment implies a high risk of self-medication, as demonstrated by the 2008 European study, which showed that dispensing the exact quantity of antibiotic treatment was associated with a decrease in the risk of self-medication.36 In countries such as the United Kingdom, the Czech Republic or the United States, the exact amount of treatment is dispensed to comply with the prescribed treatment.37
After analyzing the prescriptions carried out by the different professionals, it was observed that 10% of the prescriptions were made after patient’s request. A study carried out on 3251 pharmacy office clients showed that 25% admit having forced their physician and/or pharmacist for an antibiotic treatment: a result alike to the one observed in our study (27%).38 Several authors have shown that when the patient goes to medical appointments more frequently, the number of antibiotic prescriptions increases, also if the provider has an enormous work load.39
27% of the prescriptions received were inappropriate because patient’s data were not complete, 24% the treatment data and 3% lacked the professionals’ data, similar rates to a Spanish study with 3569 private prescriptions analyzed, of which 29% did not comply with the legislation.40
A total of 16% of patients were not informed about how to take the antibiotic, 73% of prescriptions were carried out without performing a diagnostic test and 11% of the antibiotics prescribed were insufficient to comply with the indicated dosage. The exceptional situation caused by the pandemic, together with the saturation of health centers and the consequent limitation of doctors’ time per patient, could be related to the deficiencies found.41
When analyzing the role of the pharmacist, according to the European Commission, it is the pharmacist’s role to dispense antibiotics only with a prescription, to check that the patient knows the dosage, duration, possible contraindications, adverse effects and interactions with food or other drugs. We should also promote the correct elimination of surplus treatment, as well as participate in health programs that promote the rational use of antibiotics.15 30% of the patients who requested antibiotics without a prescription assured that they never encountered any problem to acquire them in other pharmacies. A study conducted more than a decade ago in Europe showed that 54% of patients who had self-medicated with antibiotics had obtained them without a prescription directly from the pharmacy.42 In 2008 in Spain, a survey of 286 pharmacists was carried out, and 65% of them stated that they had dispensed antibiotics without a prescription, 36% of them said that they had dispensed antibiotics without a prescription.43 Another study conducted in 2009 in 197 pharmacy offices in Catalonia showed that 45% of dispensed antibiotics did not have a prescription.44
A total of 99% of patients were informed about their treatment, a higher percentage than the 84% found in the previous study44 and in 89% of cases recycling was encouraged. The implementation of the antibiotic dispensing protocol designed by the Ministry of Health made possible to obtain these results.
The results allowed us to predict that prevention policies regarding antibiotics are not obtaining the expected changes in patients, prescribing physicians and pharmacists. If we analyze the patient, various studies show their lack of knowledge, their attitude and beliefs about antibiotics are determinants of their incorrect use. Low socioeconomic status and private consultations in which the patient pays are factors that increase the chances of obtaining antibiotics.11
This study highlights the pressure exerted on both doctors and pharmacists to obtain antibiotics without a prescription. Therefore, educational campaigns are necessary to generate changes in the attitude of citizens about the use of antibiotics, as well as to promote infection prevention and control measures for the general population.
If we focus on health professionals, permanent training campaigns on antibiotics are necessary, the use of updated clinical guidelines, optimization of treatment guidelines to avoid remnants, use of rapid diagnostic tests and prohibition and monitoring of the sale of antibiotics without a prescription.
Strengths and Limitations
The large sample size compared with other studies previously conducted in Spain23,45 and the participation of several pharmacists from different pharmacy offices are among the main strengths of the study, as they increase the generalizability of the findings. Since all questionnaires were completed verbally, which also allowed the inclusion of patients with limited reading and writing skills, thus reducing the risk of selection bias.
The study has reliability limitations inherent to studies of therapeutic compliance since it is an indirect and subjective method of measurement. To minimize these limitations, we used the Morisky-Green test, which uses 4 questions with yes/no answers to check whether the patient has been adherent to treatment. The results of non-adherence may be biased, since all patients were informed that we would check their adherence to treatment in phase 1, a fact that may encourage them to comply correctly with providers’ recommendation and recycle the excess treatment.
Conclusions
Excessive and inappropriate usage of antibiotics is the major contributing factor to the emergence of new bacterial resistances to antibiotics. The results of this study suggest that there may be a significant level of antibiotic inappropriate use in the local community, finding significant deficiencies during providers prescription, in the dispensation carried out in pharmacies, and finally with patient compliance of treatment.
Patients are successfully pressuring doctors and pharmacies, leading to use antibiotics inappropriately. Mitigating patient pressure may have the greatest impact in curbing the overuse of antibiotics in Spain.
Optimizing treatment guidelines to shorter cycles, developing training campaigns for the general population, and avoiding medication remnants by dispensing the exact number of tablets needed would considerably improve the correct use of antibiotics.
It is necessary to carry out studies that highlight the limitations of the actual health system, as well as the obligatory implementation of protocols and updated guidelines to help clinicians to prescribe antibiotics and pharmacists to dispense them optimizing the correct use. We are facing a major health threat, so collaboration of governments, pharmaceutical industry, physicians, and pharmacists, is necessary to develop multidisciplinary strategies to stop the current trends.
Abbreviations
AB, antibiotic; PRAN, National Antibiotic Resistance Plan; ABR, antibiotic resistance; UN, United Nations; WHO, World Health Organization; PRM, problems related to medicines.
Acknowledgments
The authors acknowledge the work of all the pharmacists who contributed to the study data collection and thank all the patients and caregivers for their participation in the project.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. World Health Organization (WHO). Ten health issues WHO will tackle this year. World Health Organization (WHO); 2019. Available from: https://www.who.int/es/news-room/spotlight/ten-threats-to-global-health-in-2019.
2. Ministerio de Sanidad y Consumo. 2020 antibacterial agents in clinical and preclinical development: an overview and analysis. Available from: https://www.who.int/publications-detail-redirect/9789240021303.
3. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022:S0140673621027240. doi:10.1016/S0140-6736(21)02724-0
4. Mc Carlie S, Boucher CE, Bragg RR. Molecular basis of bacterial disinfectant resistance. Drug Resist Updat. 2020;48:100672. doi:10.1016/j.drup.2019.100672
5. Alós JI. Resistencia bacteriana a los antibióticos: una crisis global. Enferm Infecc Microbiol Clin. 2015;33(10):692–699. doi:10.1016/j.eimc.2014.10.004
6. Ministerio de Sanidad, Consumo y Bienestar Social - Gabinete de Prensa - Notas de Prensa. Available from: https://www.mscbs.gob.es/gabinete/notasPrensa.do?id=4713.
7. Cassini A, Högberg LD, Plachouras D, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European economic area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66. doi:10.1016/S1473-3099(18)30605-4
8. Rahimi S. Urgent action on antimicrobial resistance. Lancet Respir Med. 2019;7(3):208–209. doi:10.1016/S2213-2600(19
9. Antimicrobial consumption - Annual Epidemiological Report for 2019. European centre for disease prevention and control; 2020. Available from: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-consumption-europe-2019.
10. Bernabé Muñoz E, Flores Dorado M, Martínez Martínez F. Grado de conocimiento del antibiótico prescrito en pacientes ambulatorios. Aten Primaria. 2015;47(4):228–235. doi:10.1016/j.aprim.2014.04.014
11. Machowska A, Stålsby Lundborg C. Drivers of irrational use of antibiotics in Europe. Int J Environ Res Public Health. 2018;16(1):E27. doi:10.3390/ijerph16010027
12. Karobari MI, Khijmatgar S, Bhandary R, et al. A multicultural demographic study to analyze antibiotic prescription practices and the need for continuing education in dentistry. BioMed Res Int. 2021;2021:e5599724. doi:10.1155/2021/5599724
13. Camcioglu Y, Sener Okur D, Aksaray N, Darendeliler F, Hasanoglu E. Factors affecting physicians’ perception of the overuse of antibiotics. Med Mal Infect. 2020;50(8):652–657. doi:10.1016/j.medmal.2020.01.006
14. Agencia Española de Medicamentos y Productos Sanitarios. Los líderes mundiales reunidos en la Asamblea General de las Naciones Unidas se comprometen a adoptar una estrategia contra la resistencia a los antibióticos. Agencia Española de Medicamentos y Productos Sanitarios. Available from: https://www.aemps.gob.es/informa/notasinformativas/laaemps/2016/ni-aemps_11-2016-reunion-onu-antibioticos/.
15. ECDC. Proposals for EU Guidelines on the Prudent Use of Antimicrobials in Humans; 2017.
16. Ministerio de Sanidad, Consumo y Bienestar Social,, Agencia Española de Medicamentos y Productos Sanitarios, Plan Nacional frente a la Resistencia a los Antibióticos (PRAN) 2019-2021 | PRAN. Available from: https://resistenciaantibioticos.es/es/publicaciones/plan-nacional-frente-la-resistencia-los-antibioticos-pran-2019-2021.
17. Eyaralar Riera MT. Estudio de La Demanda de Antibióticos En La Oficina de Farmacia. El Papel Del Farmacéutico En La Dispensación de Antibióticos Con Receta Médica. - PDF Descargar Libre. CEU Cardenal Herrera; 2009.
18. Consejo General Colegios de Farmacéuticos,, Ministerio de Sanidad, Consumo Bienestar Social,, Agencia Española de Medicamentos y Productos Sanitarios, Campaña frente a la resistencia a los antibióticos. Available from: https://www.farmaceuticos.com/farmaceuticos/farmacia/campanas/campana-frente-a-la-resistencia-a-los-antibioticos.
19. Morisky DE, Green LW, Levine DM. Concurrent and predictive validity of a self-reported measure of medication adherence. Med Care. 1986;24(1):67–74. doi:10.1097/00005650-198601000-00007
20. Rodríguez Chamorro MÁ, García-Jiménez E, Amariles P, Rodríguez Chamorro A, José Faus M. Revisión de tests de medición del cumplimiento terapéutico utilizados en la práctica clínica. Aten Primaria. 2008;40(8):413–418. doi:10.1157/13125407
21. Atkinson MJ, Sinha A, Hass SL, et al. Validation of a general measure of treatment satisfaction, the Treatment Satisfaction Questionnaire for Medication (TSQM), using a national panel study of chronic disease. Health Qual Life Outcomes. 2004;2:12. doi:10.1186/1477-7525-2-12
22. Goossens H, Ferech M, Vander SR, Elseviers M; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. Lancet Lond Engl. 2005;365(9459):579–587. doi:10.1016/S0140-6736(05
23. Vega-Cubillo EM, Andrés-Carreira JM, Cirillo-Ibargüen S, Manzanares-Arnaiz C, Moreno-Moreno G, Redondo-Figuero CG. Incumplimiento del tratamiento antibiótico sistémico prescrito en servicios de urgencias de Atención Primaria (Estudio INCUMAT). Med Fam SEMERGEN. 2017;43(1):4–12. doi:10.1016/j.semerg.2016.03.004
24. Kardas P, Devine S, Golembesky A, Roberts C. A systematic review and meta-analysis of misuse of antibiotic therapies in the community. Int J Antimicrob Agents. 2005;26(2):106–113. doi:10.1016/j.ijantimicag.2005.04.017
25. Llor C, Hernández S, Bayona C, et al. A study of adherence to antibiotic treatment in ambulatory respiratory infections. Int J Infect Dis. 2013;17(3):e168–e172. doi:10.1016/j.ijid.2012.09.012
26. Navarro-Gómez P, Sorlózano-Puerto A, Olmo-Navas MM, et al. [Assessment of adherence to antibiotic treatment in Primary Care by determining levels of the drug using a liquid chromatography technique]. Rev Esp Quimioter. 2017;30(5):341–349. Spanish.
27. Chen YC, Leu HS, Wu SF, Wu YM, Wang TJ. [Factors influencing adherence to antibiotic therapy in patients with acute infections]. Hu Li Za Zhi. 2015;62(1):58–67. Chinese. doi:10.6224/JN.62.1.58
28. Spellberg B, Rice LB. Duration of antibiotic therapy: shorter is better. Ann Intern Med. 2019;171(3):210–211. doi:10.7326/M19-1509
29. Wald-Dickler N, Spellberg B. Short-course antibiotic therapy—replacing Constantine units with “shorter is better”. Clin Infect Dis. 2019;69(9):1476–1479. doi:10.1093/cid/ciy1134
30. Del Estado J. Ley 29/2006, de 26 de Julio, de Garantías y Uso Racional de Los Medicamentos y Productos Sanitarios. Jefatura del Estado; Vol. BOE-A-2006-13554, 2006:28122–28165. Available from: https://www.boe.es/eli/es/l/2006/07/26/29.
31. Salar Ibañez L. Estudio de la demanda de antibióticos sin receta en la oficina de farmacia. Papel del farmacéutico en la automedicación con antibióticos. Universidad CEU Cardenal Herrera; 2006.
32. Diario M. Madrid: el 99% de las farmacias recibe peticiones para dispensar antibióticos sin receta. DiarioMedico; 2019. Available from: https://www.diariomedico.com/farmacia/comunitaria/profesion/madrid-el-99-de-las-farmacias-recibe-peticiones-para-dispensar-antibioticos-sin-receta.html.
33. Molinero A, Carbajal de Lara JA, Fernández CF, et al. Demanda de antibióticos sin prescripción en la farmacia comunitaria. Descripción de la intervención del farmacéutico. Med Fam SEMERGEN. 2020;46(8):545–552. doi:10.1016/j.semerg.2020.06.025
34. González J, Orero A, Prieto J. Almacenamiento de antibióticos en los hogares españoles. Rev Esp Quimioter. 2006;19:11.
35. Arias Puente M, Huarte Gil P, Jimenez Morales P, Hernández Tomás L, Mateos Lardiés A. Estudio del farmacéutico comunitario del manejo por parte del paciente de antibióticos y su presencia en el botiquín casero. Farmacéuticos Comunitarios. Available from: https://www.farmaceuticoscomunitarios.org/es/journal-article/estudio-del-farmaceutico-comunitario-del-manejo-parte-del-paciente-antibioticos-su.
36. Grigoryan L, Burgerhof JGM, Degener JE, et al. Determinants of self-medication with antibiotics in Europe: the impact of beliefs, country wealth and the healthcare system. J Antimicrob Chemother. 2008;61(5):1172–1179. doi:10.1093/jac/dkn054
37. Grigoryan L, Monnet DL, Haaijer-Ruskamp FM, Bonten MJM, Lundborg S, Verheij TJM. Self-medication with antibiotics in Europe: a case for action. Curr Drug Saf. 2010;5(4):329–332. doi:10.2174/157488610792246046
38. Percepción en el ámbito de la farmacia comunitaria de las resistencias a antibióticos. visión de los usuarios. Farmacéuticos Comunitarios. Available from: https://www.farmaceuticoscomunitarios.org/es/journal-article/percepcion-ambito-farmacia-comunitaria-resistencias-antibioticos-vision-usuarios.
39. Serna MC, Real J, Ribes E, Marsal JR, Godoy P, Galván L. Determinantes de la prescripción de antibióticos en atención primaria. Enferm Infecc Microbiol Clin. 2011;29(3):193–200. doi:10.1016/j.eimc.2010.09.012
40. Proyecto ‘Demanda de antibióticos en farmacia comunitaria con receta privada, prescripción irregular y sin receta (automedicación): intervención del farmacéutico’: tipos de demandas. Farmacéuticos Comunitarios. Available from: https://www.farmaceuticoscomunitarios.org/es/journal-article/proyecto-demanda-antibioticos-farmacia-comunitaria-con-receta-privada-prescripcion-1.
41. Tranche Iparraguirre S, Martín Álvarez R, Párraga Martínez I. El reto de la pandemia de la COVID-19 para la Atención Primaria. Rev Clín Med Fam. 2021;14(2):85–92.
42. Grigoryan L, Burgerhof JGM, Haaijer-Ruskamp FM, et al. Is self-medication with antibiotics in Europe driven by prescribed use? J Antimicrob Chemother. 2007;59(1):152–156. doi:10.1093/jac/dkl457
43. Zapata-Cachafeiro M, González-González C, Váquez-Lago JM, et al. Determinants of antibiotic dispensing without a medical prescription: a cross-sectional study in the north of Spain. J Antimicrob Chemother. 2014;69(11):3156–3160. doi:10.1093/jac/dku229
44. Llor C, Cots JM. The sale of antibiotics without prescription in pharmacies in Catalonia, Spain. Clin Infect Dis. 2009;48(10):1345–1349. doi:10.1086/598183
45. Martínez-Sagrera PG, Cárdenas JM, Martín A, Ortega MG, Somoza B. Estudio del consumo de antibióticos en pacientes de farmacia comunitaria. Pharm Care Esp. 2020;22(1):3–24.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.