Back to Journals » Clinical Interventions in Aging » Volume 18
Study of Morpho-Functional Characteristics of the Cardiovascular System According to Electrocardiography, Phonocardiography, Echocardiography in Masters Athletics
Authors Safonicheva O ![]() , Kryuchkova K
, Kryuchkova K ![]() , Lazareva I, Chekulaev P, Ovchinnikova M, Kurshev V, Budanova E, Gameeva V, Gavrilov V, Epishev V
, Lazareva I, Chekulaev P, Ovchinnikova M, Kurshev V, Budanova E, Gameeva V, Gavrilov V, Epishev V ![]() , Zaborova V
, Zaborova V
Received 25 July 2023
Accepted for publication 18 November 2023
Published 13 December 2023 Volume 2023:18 Pages 2079—2092
DOI https://doi.org/10.2147/CIA.S432202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Olga Safonicheva,1 Kira Kryuchkova,1 Irina Lazareva,1 Pavel Chekulaev,1 Marina Ovchinnikova,1 Vladislav Kurshev,1 Elena Budanova,2 Victoria Gameeva,3 Victor Gavrilov,4 Vitaly Epishev,5 Victoria Zaborova1
1Institute of Clinical Medicine, Sechenov First Moscow State Medical University (Sechenov University), Moscow, Russia; 2Institute of Public Health, Sechenov First Moscow State Medical University (Sechenov University), Moscow, Russia; 3Luzhniki Sports Clinic, Moscow, Russia; 4Moscow Institute of Physics and Technology (National Research University), Moscow Region, Russia; 5Research Center for Sports Science, South Ural State University, Chelyabinsk, Russia
Correspondence: Olga Safonicheva, Institute of Clinical Medicine, I.M. Sechenov First Moscow State Medical University (Sechenov University), Trubetskaya Street, 8/2, Moscow, 119991, Russia, Tel +7 926 534-62-65, Fax +7 495 609-14-00, Email [email protected]
Background: Many authors have noted the lack of knowledge on the causal relationship between the degree of physical activity, the dynamics, and outcomes of diseases, as well as the influence of sports history on the rehabilitation potential of former athletes.
Purpose: Assessment of the functional state of the cardiovascular system according to the indicators of electrocardiography, polycardiography, echocardiography and the level of physical performance in masters athletes.
Patients and Methods: The study included a main group consisting of 100 athletes, who had undergone electrocardiography, poly-electrocardiography, ultrasound echocardiography, heart rate and blood pressure measurement to determine their level of physical performance. The subjects were then divided into 2 groups. The first group included 75 people who continue to be active in regular sports activities. The second group consisted of 25 people who completely stopped training or had only occasional, unsystematic physical activities. A control group of 31 people, consisting of people of the same age who had not been involved in sports earlier, was examined according to the same program.
Results: The data obtained by us show that sports activities do contribute to the increasing stability of the body and maximize the deployment of the capabilities of the circulatory system, including their long-term preservation in masters athletic. Athletes who have stopped training have signs of age-related changes in the heart and blood vessels, which seem to be more frequent and earlier than those who continue training. A higher degree of myocardial contractility (in 90.67% of cases) can also be seen in the main group.
Conclusion: Masters athletes and those who stopped training after completing their sports career, should have notably thorough medical supervision and undergo regular annual in-depth examination.
Keywords: blood pressure, heart rate, PWC170, physical work capacity, cardiodynamics, hemodynamic parameters
Introduction
Rational physical activity is one of the main and most effective ways to promote health and enhance performance, helps to increase the adaptive capacity of the person at any age.1 In this connection, the data on the functional state of people who have been engaged in physical culture and sports for many years over a long period of time are of interest.
Achieving high results in world sports is associated with an increase in the volume of the training process and the intensity of physical loads. Accordingly, their impact on the athlete’s body increases, the adaptation processes are more intense and complex2,3 One of the most stressed systems of the organism when doing sports is the cardiovascular system, which causes the need for its more detailed study using modern research methods.4,5
Literature data on the effect of high-performance sports on human health with age and its circulatory system are contradictory. Some authors believe that sports have an inhibitory effect on the development of age-related changes in the cardiovascular system, in particular atherosclerotic process.6 According to other researchers, sports training, without delaying the development of age-related changes in the heart and blood vessels and without preventing circulatory system diseases, provides the necessary compensation, which contributes to an easier course of diseases and preservation of a high level of performance.7,8 And only some works note a higher frequency of heart disease than in the rest of the population.9–11
It has been proven that the health of most professional athletes deteriorates at the abrupt end of their sports careers. Many authors note the lack of information on the causal relationship between the degree of physical activity, the dynamics, and outcomes of diseases, as well as the influence of sports history on the rehabilitation potential of former athletes.12 Thus, it was revealed that for a personalized approach in the selection of treatment and rehabilitation programs for patients with CHD, it is necessary to take into account the presence of a sports history. It has been demonstrated that patients with CHD and sports history have higher rehabilitation potential, the possibility of intensification of subsequent physical rehabilitation program and its earlier start.8
In this regard, one of the topical problems of sports medicine and geriatrics is the study of physical performance and morphofunctional state of the heart of athletes over the age of 40. It is not yet clear enough what changes the cardiovascular system undergoes in a highly qualified athlete after the end of systematic training with large volume and intensity of physical exertion. It is important to identify how long and to what extent the high level of adaptive capacity of the circulatory system achieved in the process of long-term special training is preserved. The period after the end of active sports training, its regime at that time and in the following years of life are especially important for making recommendations about the rational training regime of sports veterans.
Thus, the purpose of the present study is to evaluate the functional state of the cardiovascular system according to the indicators of electrocardiography, polycardiography, echocardiography and the level of physical performance in veterans of game sports.
Materials and Methods
The study was conducted in accordance with the provision of the Declaration of Helsinki and approved by the local ethical committee of Sechenov Moscow State Medical University (protocol №173 of October 30, 2020). Informed written consent was obtained from all patients before their inclusion in this study.
One hundred athletes, members of national teams, were included in the study. All subjects were under the supervision of a sports medicine physician. Inclusion criteria: male sex, age over 40 years, past participation in high-performance sports, athlete level (highest sport qualification, participation in international competitions – World Championships, European Championships), sport specialization (sports games), total sport experience – 10 to 20 years or more. Exclusion criteria: female gender, age less than 40 years and over 70 years.
100 athletes who made up the main group were examined according to an extended program, which included the study of morphofunctional features of the central and peripheral circulation using functional diagnostic methods (pre- and post-load electrocardiography, polyelectrocardiography, ultrasound echocardiography).
A control group of 31 persons, consisting of persons of similar age who had not participated in sports before, was examined according to the same program.
100 athletes were divided into 2 groups depending on the mode of motor activity. The first group consisted of 75 veteran athletes who continued regular sports activities. The second group consisted of 25 people who had completely stopped training or had only occasional, haphazard physical activity.
Most of the sports veterans (53.3%) trained daily for 1.5–2.5 hours, 17.6% trained 5 times a week, and 27.1% trained 3–4 times a week.
The test with load – PWC170 – was used to reveal the general level of physical performance capacity (PFC) and functional capabilities of the cardiovascular system. The subjects performed two loads of increasing power (duration of each load was 5 min) with a rest interval of 3 min on a Monark 874-E cycloergometer (Monark, Vansbro, Sweden). The frequency of pedalling was 60 rpm. HR was recorded auscultatively at the end of each exercise (last 30s of work at a certain power level). The value of FR was calculated according to Karpman V.L. formula.
We studied the adaptation of the circulatory system to the loads and the recovery period according to the indices of well-being, heart rate (HR), blood pressure (BP), electrocardiography (ECG). Blood pressure (BP) was measured using an automatic M3 Expert pressure meter (OMRON, Japan) on the right arm twice at 5-min intervals in the sitting position. The average value of 2 measurements were included in the analysis.
Registration of 12 leads of electrocardiogram (ECG) at rest was performed after a 5-minute rest on a computer ECG complex PADSY (Medset Medizintechnik GmbH, Hamburg, Germany) in the supine position. ECG and BP were recorded before exercise and during the first minutes of the recovery period.
Polycardiogram (PCG) was recorded at rest before the test. For this purpose, we used phono- and sphygmographs attached to the electrocardiograph. The PKG was assessed on the basis of cardiac cycle phase duration calculation according to V.L. Karpman’s method.
Ultrasound electrocardiography (ECHO-CG) was performed according to a standard protocol on an EPIQ ultrasound machine (Philips Ultrasound, Inc., USA).
The data were processed using Microsoft Excel and Statistica 8.0 for Windows. The results of the study were processed by the method of variation statistics with estimation of reliability according to the Student’s criterion (t). The relationship of the signs was evaluated by Pearson correlation coefficient. The probability of error not exceeding 5% (p<0.05) was considered significant.
Results
The Health Status of the Subjects According to the results of a Comprehensive Medical Examination
During a comprehensive medical examination, diseases of the musculoskeletal system and osteochondrosis of the spine were found most frequently (Figure 1). This can be explained by frequent injuries during intensive sports training. Coronary heart disease (CHD) was detected in 8% of cases. History of myocardial infarction (MI) was noted in 5%, all of them from the second group. In all cases, MI was obtained not earlier than 10 years after cessation of intensive sports activities. Hypertensive disease (HT) of I–II stages was detected in 7% of the subjects.
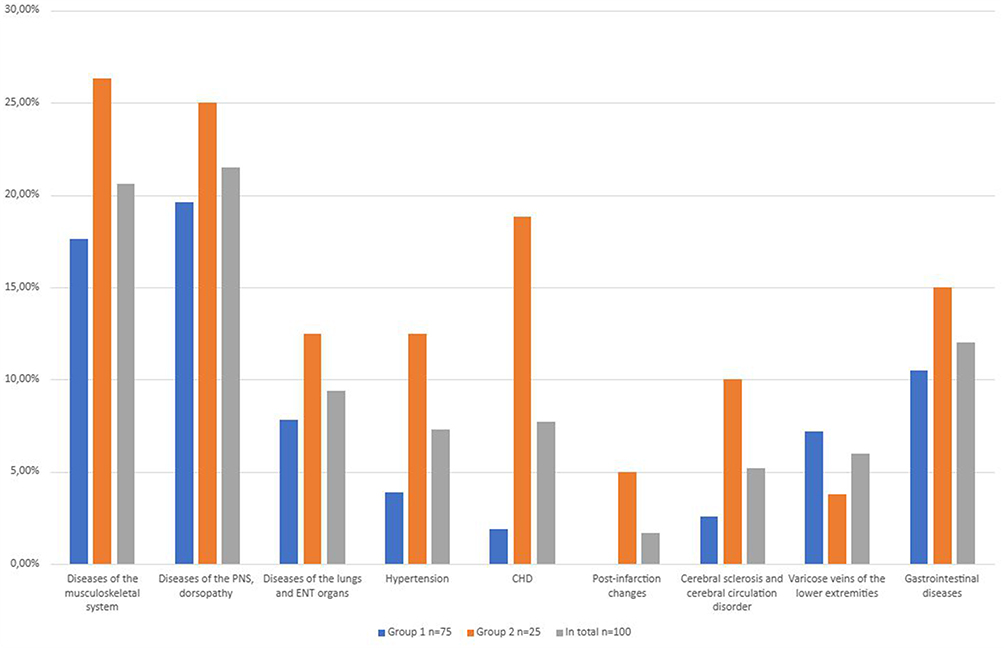 |
Figure 1 The main diseases detected in the subjects during a comprehensive medical examination (%). Note: In most cases, the same persons were included in different columns of the table. |
Basic Hemodynamic Indices at Muscle Rest
In the examined subjects the HR corresponded to 36–90, in most cases (97%) it was up to 75 bpm. Figure 2 shows that there were significant differences (p<0.05) in HR between the main and control groups in all age groups (Figure 2). The more pronounced bradycardia in the main group is explained not so much by age-specific features as by the persistent influence of years of sports training on autonomic innervation. There were no significant differences in HR between subjects in different age groups, while there were significant differences (p<0.05) between athletes of the first and second groups. This difference is more pronounced in older age groups and in veterans, who train with primary development of endurance quality. HR in persons continuing sports training does not change with age, and in those who stopped training has a tendency to increase compared to the period of active sports training in representatives of the first group, HR has changed little (frequency not more than 2–9 beats/min), while in the second group – by 7–15 beats/min and more.
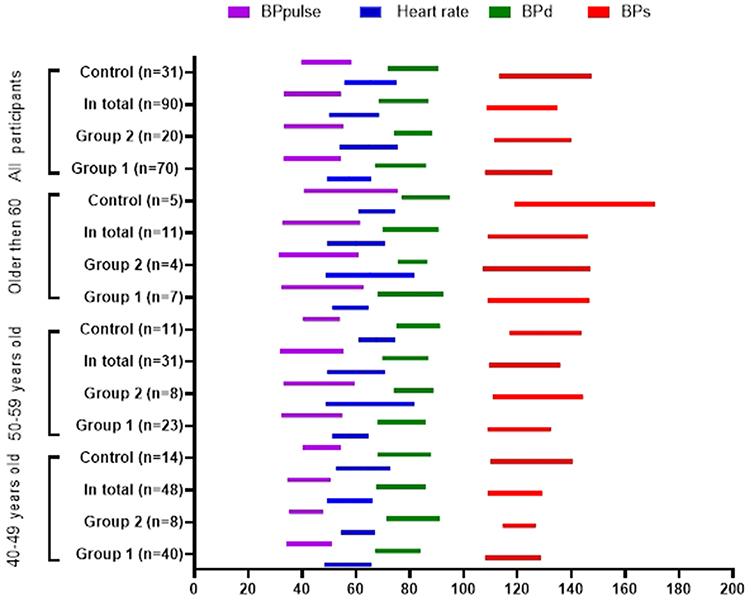 |
Figure 2 Heart rate and blood pressure in subjects of different ages, depending on the motor mode after the cessation of active training. |
Average BP values in sports subjects were lower than in non-sports subjects of the same age. Except for isolated cases, they did not exceed the limits of age fluctuations, being at the lower limit of the age norm or lower in the majority of those examined. The increase in both BPs and BPd with age was insignificant. The BPs of those who continued exercising were lower than those of those who stopped exercising.
Cardiodynamics According to the Results of the Study of the Phase Structure of the Cardiac Cycle
With age, there is a restructuring of cardiac cycle phase structure, which is explained by the peculiarities of hemodynamics and myocardial contractility state. Statistically significant (p<0.05) increase of tension period (T) duration was revealed in the control group in the age over 60 years old in comparison with 40–49 and 50–59 years old persons (Table 1). This was associated with both a lengthening of the isometric contraction phase (IC) and an increase in the duration of the asynchronous contraction phase (AC). The ejection period (E) in persons 40–49 years old corresponds to the proper value for the given rhythm, in subsequent age groups it increased by more than 0.02 seconds. Correspondingly, the values of intraphase indicators changed: the intra-systolic index (ISI), the mechanical coefficient (MC), the electromechanical difference (EMD), the initial rate of increase in intraventricular pressure (Vj) decreased, myocardial tension index (MTI) increased. This reflects age-related changes of the myocardium and indicates a gradual decrease of its contractile function.
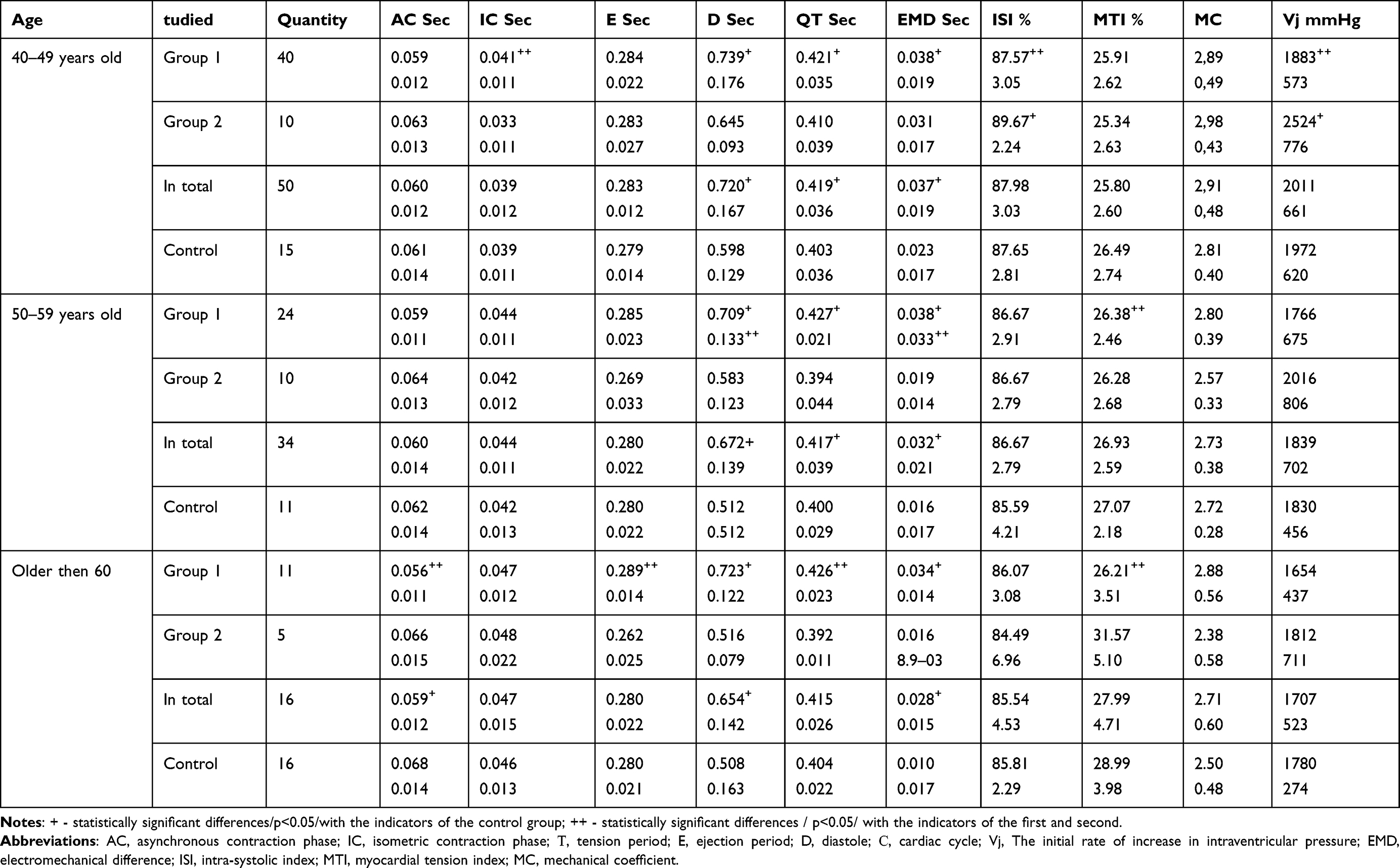 |
Table 1 The Duration of the Phases of the Cardiac Cycle and the Values of Intraphase Indicators in Subjects of Different Ages, Depending on the Motor Mode After the Cessation of Active Sports Training (M ± δ) |
The subjects also had a statistically significant (p<0.05) increase in the T period with age. The AC phase in all age groups was at the upper limit of the norm, not increasing, in contrast to the IC phase, which does not lengthen with age. The E period in all age groups, unlike the control group, corresponded to the proper value for the given rhythm. The values of intraphase indices naturally changed with increasing age: ISI, MC, EMD, Vj decreased, MTI, and the time of minute volume expulsion (TMVE) increased. But these changes compared to the control group were expressed to a lesser extent. In sports, veterans significantly (p<0.05) longer cardiac cycle (C), EMD, which indicates a greater functional reserve.
In all age groups, the subjects had statistically significantly (p<0.05) longer diastole compared to the control group, which reflects more favourable conditions for the heart of a trained person.
C, IC, EMD, MC increase statistically reliably (p<0.05) in those who continue sport activity in comparison with those who stopped it, ISI, TMVE, MTI decrease. This is evidence of keeping phase structure of cardiac cycle typical for active trained athletes. The first group of investigated people revealed higher functional capacity of the myocardium than the second one, but even in those who stopped sports training, myocardial contractility and functional reserve of the heart were higher than in those who had not been engaged in sports earlier.
In the 40–49-year-old group, the differences between the subjects of the first and second groups are less pronounced than in the subsequent groups. A statistically significant difference (p<0.05) is determined only by the indices of IC, ISI, Vj, AC/IC phase. Probably, it is connected with the fact that it is the earliest period of training termination, when its after-effects are most expressed, and those who have stopped sports activities still have a high level of myocardial functional features, achieved in the process of long-term intensive training.
In the group of 50–59 years, there are already great differences between the parameters of contractility of the first and second groups. Thus, statistically significant differences (p<0.05) in: C, diastole period (D), EMD, MTI, TMVE. This reflects deterioration of myocardial contractility in persons who stopped training.
Even greater differences in the phase structure of systole are revealed at the age over 60 years old. Those who continue sports training retain a high level of myocardial functional capacity, whereas those who stop it with increasing age show more pronounced changes, reflecting a gradual decline in myocardial contractility.
In 75 subjects of the first group, 90.67% of cases there were phase syndromes characterizing higher myocardial contractility: phase syndrome of controlled hypodynamia (14.67%), volume loading syndrome against bradycardia (26.67%) and normal PCG, typical for a healthy person of the corresponding age (49.33%). In 9.33% there were changes in the phase structure of cardiac cycle, reflecting the reduction of myocardial contractile function: myocardial hyperdynamic phase syndrome (6.66%) and true myocardial hypodynamia (2.67%).
In the second group, 64% of the subjects had more favourable phase syndromes (phase volume loading syndrome against bradycardia in 12% and unchanged PCG in 52%), and 36% had less favourable phase shifts (phase volume loading syndrome against tachycardia in 12%, myocardial hyperdynamic phase syndrome in 8%, true myocardial hypodynamia in 16%.
Peculiarities of the Heart Condition According to ECG Data
The morphological and functional changes of the heart related to age-related changes of the organism and the influence of systematic sports activities are reflected in the ECG study data. The analysis of ECG of the subjects in comparison with the control group revealed the tendency to some increase in rhythm frequency, decrease in liability of sinus node, decrease in R and T waves voltages, increase in cases with deviation of electrical axis of the heart to the left. In terms of frequency and severity, ECG changes in sports veterans do not exceed those in persons of corresponding age, who were not engaged in sports in the past. On the contrary, in general, they have less degree of morphological changes and more often there are signs indicating a higher functional state of the heart. ECG changes are less common in those who continue sports training, most of them have preserved high functional capabilities of the heart, acquired in the process of many years of intensive training (Table 2).
 |
Table 2 Comparative Frequency of Some Changes in the ECG of the Subjects Depending on the Motor Mode After the Cessation of Active Training (Number of Cases in %) |
Anatomical, Morphological and Functional Features of the Heart According to ECHO-CG Data
Morpho-functional characteristics of the heart of athletes over 40 years old are considered as the result of the combined influence of age and long-term intensive sports training. In the control group (Table 3) with increasing age there is a reliable (p<0.05) increase of left ventricular end-systolic cavity size (ESS), left ventricular cavity volume in systole (ESV); there is a tendency to increase the left ventricular cavity end-diastolic size (EDS), left ventricular cavity volume in diastole (EDV), without reliable changes in relative indices of EDS /s and EDV /s (s is the degree of shortening of the anterior–posterior size of the left ventricle in the systole, %). s – degree of left ventricular anteroposterior dimension shortening in systole, %). There was revealed an increase with age in left ventricular posterior wall myocardial thickness in diastole (TLVD) and left ventricular myocardial mass (LVMM), indicating the development of myocardial hypertrophy with age in the subjects. Indexes characterizing left ventricular contractile function significantly (p<0.05) decrease with age.
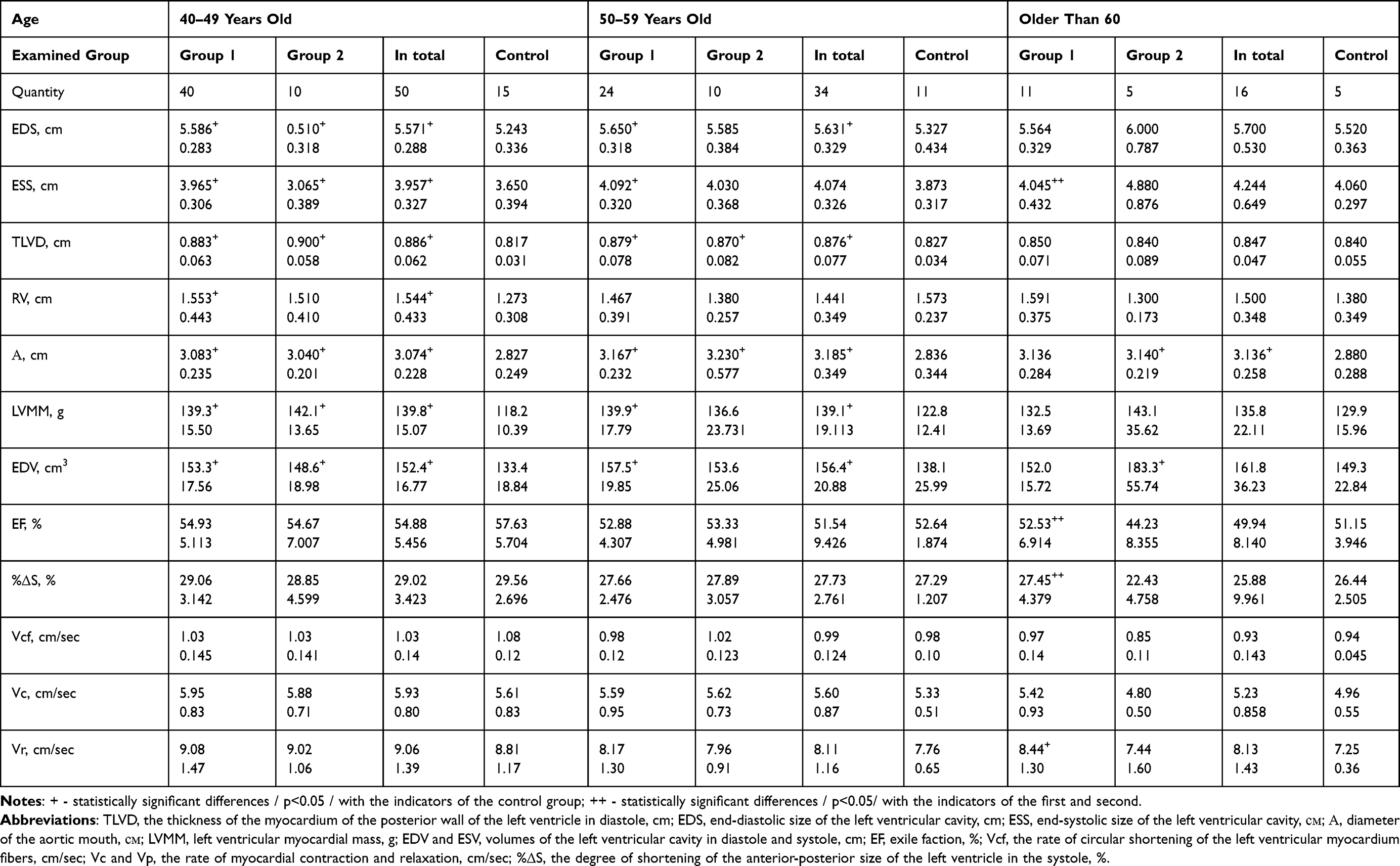 |
Table 3 Electrocardiographic Indicators of Subjects of Different Ages, Depending on the Motor Mode After the Cessation of Active Sports Training (M ± δ) |
Statistically significant (p<0.05) increase of ESS, ESV and indexed indices with age is also observed in the subjects. Moreover, if the subjects of the second group have a statistically reliable (p<0.05) increase in ESS and ESV, ESS in the first group practically does not change with age, which is hemodynamically more favorable. The EDS, EDS/s predominantly increase in veterans. The same regularity is observed for EDV, EDV/s, EDV/kg. Parameters characterizing myocardial contractile function significantly decreased with age (p<0.05); it was most expressed in persons over 60 years old, who stopped sport activities.
The indices characterizing the degree of left ventricular myocardial hypertrophy, in contrast to the age dynamics in healthy non-sportsmen, do not increase. There is a statistically reliable (p<0,05) decrease of TLVD from 40 to 60 years old, LVMM does not change due to the increase of left ventricular cavity. There was no significant difference in TLVD value in the subjects of the first and second groups. Differences in LVMM over 60 years of age are explained by the variability of EDV values.
The index EDV/LVMM, characterizing the ratio of left ventricular cavity dilatation and myocardial hypertrophy, tended to increase with age. In the second group, it was an increase in dilatation over hypertrophy.
In age groups 40–49 and 50–59, reliable differences (p<0.05) in indices characterizing left ventricular cavity size and degree of myocardial hypertrophy were revealed in relation to control group persons. This indicates the preservation of structural changes of the heart, achieved in the process of prolonged sports training, in the subjects. Over the age of 60 years, this pattern is lost.
In the indices characterizing myocardial contractility, there were no significant differences in the subjects compared to the control group.
Aortic diameter in all age groups in sport subjects was significantly larger (p<0.05) than in control subjects. Age dynamics of indices characterizing mitral valve function does not seem to be clear, there is no connection neither with age nor with degree of motor activity.
Adaptive Capabilities of the Cardiovascular System in Athletes Over 40 Years Old
In all age groups (Figures 3 and 4) the value of PWC170 was significantly (p<0,05) higher than in the control group. Moreover, it is higher compared to the control group not only in athletes who continue sports activities, but also in those who have stopped sports activities. But the differences between them are statistically reliable (p<0,05), indicating a significant impact on the level of physical performance, degree of motor activity, lifestyle after quitting sports. With age, the PWC170 value naturally decreases more significantly in athletes who stopped sports training than in those who continue.
 |
Figure 3 Absolute values of PWC170 in subjects of different ages, depending on the motor mode after the cessation of active training. |
 |
Figure 4 Relative values of PWC170 in subjects of different ages, depending on the motor mode after the cessation of active training. |
Thus, the subjects retain a sufficiently high level of physical performance after the end of active sports training. This level, due to age-related changes in the circulatory system and neurohumoral regulation, decreases compared to the current highly qualified athletes, but significantly exceeds that of individuals who have not participated in sports before. This is especially true for the subjects who continue their sports training.
Discussion
We pay special attention to diseases of the cardiovascular system, which are the main cause of disability and mortality.13 In addition, the importance of studying the structure, function, and regulation of the cardiovascular system is determined by the fact that the developing age-related changes in the circulatory system can cause dysfunction of other organs and systems, which affects the nature and rate of ageing.14 All the more, when doing sports, the CPS is one of the most stressed.15 Our data show that CHD, MI, and HF in members of national teams are not only not more frequent, but even somewhat less frequent than in other categories of the population of the corresponding age. Even lower morbidity is observed in those athletes who continue lifelong physical activity. The vast majority of cardiovascular diseases occur in the second group of athletes, while in the first group these diseases occur only in isolated cases.
Despite the low incidence of cardiac pathology in veterans compared to the general population, CHD remains one of the leading causes of sudden death in sports veterans.16,17 CHD in veterans often manifests itself differently than in people with a sedentary lifestyle. In some cases, cardiac arrest during physical activity or the occurrence of symptoms in the form of fatigue, decreased ability to work in the absence of angina pain behind the sternum are possible. Therefore, it is necessary to rule out CHD in former athletes if any new complaints arise, including subjective decreased performance.18 Interestingly, the presence of a previous sports history in patients with coronary heart disease is a marker of a positive prognosis in the treatment and rehabilitation of patients with this disease, as well as indicating a greater rehabilitation potential compared to patients without a sports history.19,20
It is known that regular physical activity, especially endurance exercise, helps to reduce HR and BP at rest, which has a protective effect on the vascular wall.21,22 Most athletes show bradycardia as a positive adaptation to endurance training.23 According to our study, the main hemodynamic parameters detected in the majority of sports veterans are characteristic not only for the lower limits of age variations, but also for the hemodynamic parameters of people of younger age. This is explained by the increased tone of the parasympathetic nervous system and increased sensitivity of baroreceptors.24 However, prolonged strenuous exercise can potentially lead to cardiovascular dysfunction and hidden hypertension with altered cardiac function, which is an increased risk among veteran athletes.25,26 In addition, veterans who develop predominantly endurance quality (cyclists, runners and swimmers, triathletes) show greater pliability and less vascular wall stiffness, increased endothelial function, improved blood flow, adequate BP regulation at rest and during exercise compared to healthy people of the same age who led a sedentary lifestyle.27–29
According to our data, age-related changes of cardiac cycle phase structure at rest are less pronounced in sports veterans, which indicates a better myocardial contractility and greater reserve capacity of the heart compared to those who were not engaged in sports earlier. This is most clearly manifested in athletes, who continue to do physical exercises throughout their life. One explanation for the above phenomenon could be the fact that patients who regularly participate in sport have higher NO bioavailability and bioactivity than patients without a sporting history of the same age. For example, DeSouza et al demonstrated that, compared with healthy young adults, older men who regularly exercise did not show an age-related decrease in endothelium-dependent dilatation as a result of preserved NO bioavailability.30 Moreover, 12 weeks of brisk walking restored basal endothelium-dependent dilatation by increasing NO bioavailability in previously sedentary middle-aged and elderly men to levels similar to those observed in young healthy men. Thus, maintaining a high level of fitness or engaging in regular exercise can prevent or reverse the age-related decline in microcirculatory function by increasing NO bioavailability.31 In addition, the better cardiovascular adaptive capacity of veteran athletes compared to other populations may be related to the high content of mitochondrial enzymes, as well as the greater development of the vascular network (more capillaries contacting a single muscle fibre).32
ECHO-CG data and their comparison with those in active athletes reflect physiological ideas about age-related changes of the heart, manifested in its increase and relative decrease of myocardial contractility. In veteran-athletes these changes are not greater than in persons of similar age, who were not engaged in sports in the past, with higher myocardial functional state indices in most cases.
Compared to the current ones, veterans have less economical reactions at similar loads with less high work capacity. Adaptation capabilities formed on the basis of improved reactions and establishment of stable connections between the musculoskeletal system, the circulatory and respiratory systems during many years of systematic sports training remain higher than in persons who have not participated in sports before, in all age groups. Those who continue training retain to a greater extent the type of adaptability characteristic of younger age, ie, a more perfect level of regulation. They revealed age-specific reaction features less frequently and to a lesser extent, the physical performance, and adaptability indices characteristic of younger athletes were preserved more often. ECG shifts after physical activity in the subjects do not exceed the limits of age peculiarities and in most cases, especially considering the large volume and intensity of the work performed, can be assessed as more favourable.
It is worth emphasizing the need for preventive measures in all groups of patients to reduce cardiological risk. In the research of et al the effectiveness of changing the image using smartphone technology has been proven. For example, the results of the LIGHT study show that intervention in combination with conventional treatment reduced the risk of cardiovascular disease compared to only conventional treatment for 1 years of observation. In addition, the smart phone health application improved smoking cessation, systolic and diastolic blood pressure, BMI, serum HbA1c, LDL-C and triglyceride levels, and also improved the quality of life and HDL-C levels in the blood serum. These results indicate that mobile medical interventions with their multifaceted application can take a fresh look at improving the primary prevention of cardiovascular diseases, including in sports veterans and former athletes.33–36
Conclusion
The data obtained by us show that sports activities aimed at achieving the highest results contribute to the improvement of specific and non-specific resistance of the body, maximum deployment of the circulatory system capabilities and their long-term preservation, delaying the age-related decline in vitality and thus are essential for strengthening and preserving human health. In addition, the subjects less often and to a lesser extent than people of the same age who have not participated in sports before, reveal age-related changes and diseases of the cardiovascular system with higher functional capabilities of the circulatory system and preservation of ways of adaptation to physical loads, typical for younger age. In addition, the persistent effects of long-term systematic training are observed in sports veterans. With age, there is a tendency to increase the cavity of the left ventricular heart and to decrease the degree of myocardial hypertrophy with a decrease in its contractility. It is worth noting that the motor mode after a period of active sports training, all other things being equal, can significantly affect the rate and degree of development of age-related processes in the body. Athletes who abruptly and completely stopped exercising have more frequent and earlier age-related changes of the heart and blood vessels, with more frequent cardiovascular morbidity than those who continue exercising.
Thus, medical supervision of veteran athletes, as well as those who stopped training after the end of their sports career, should be particularly thorough and consist of an annual in-depth examination using a comprehensive clinical and instrumental examination with electrocardiography, polycardiography, echocardiography. An additional examination should be performed when deciding on eligibility for competition.
Abbreviations
А, diameter of the aortic mouth; AC, asynchronous contraction phase; BPs, systolic blood pressure; BPd, diastolic blood pressure; С, cardiac cycle; D, diastole; E, ejection period; EDS, end-diastolic size of the left ventricular cavity; EDV and ESV, volumes of the left ventricular cavity in diastole and systole; EF, exile faction; EMD, electromechanical difference; ESS, end-systolic size of the left ventricular cavity; HTm hypertension disease; IC, isometric contraction phase; ISI, intra-systolic index; LVMM, left ventricular myocardial mass; MTI, myocardial tension index; MC, mechanical coefficient; %ΔS, the degree of shortening of the anterior-posterior size of the left ventricle in the systole; T, tension period; TMDТ, the thickness of the myocardium of the posterior wall of the left ventricle in diastole; TLVD, the time of minute volume expulsion; Vcf, the rate of circular shortening of the left ventricular myocardium fibers; Vc and Vr, the rate of myocardial contraction and relaxation; Vj, the initial rate of increase in intraventricular pressure.
Acknowledgments
We would like to thank all participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sevilla-Lorente R, Carneiro-Barrera A, Molina-Garcia P, Ruiz JR, Amaro-Gahete FJ. Time of the day of exercise impact on cardiovascular disease risk factors in adults: a systematic review and meta-analysis. J Sci Med Sport. 2023;26(3):169–179. doi:10.1016/J.JSAMS.2023.03.004
2. Robbins JM, Gerszten RE. Exercise, exerkines, and cardiometabolic health: from individual players to a team sport. J Clin Invest. 2023;133(11). doi:10.1172/JCI168121
3. Weakley J, Schoenfeld BJ, Ljungberg J, Halson SL, Phillips SM. Physiological responses and adaptations to lower load resistance training: implications for health and performance. Sport Med - Open. 2023;9(1):28. doi:10.1186/S40798-023-00578-4
4. Petrungaro M, Fusco L, Cavarretta E, et al. Long-term sports practice and atrial fibrillation: an updated review of a complex relationship. J Cardiovasc Dev Dis. 2023;10(5). doi:10.3390/JCDD10050218
5. de la Guía-Galipienso F, Ugedo-Alzaga K, Grazioli G, et al. Arrhythmogenic cardiomyopathy and athletes - a dangerous relationship. Curr Probl Cardiol. 2023;48(9):101799. doi:10.1016/J.CPCARDIOL.2023.101799
6. Valenzuela PL, Ruilope LM, Santos-Lozano A, et al. Exercise benefits in cardiovascular diseases: from mechanisms to clinical implementation. Eur Heart J. 2023;44(21):1874–1889. doi:10.1093/EURHEARTJ/EHAD170
7. Isath A, Koziol KJ, Martinez MW, et al. Exercise and cardiovascular health: a state-of-the-art review. Prog Cardiovasc Dis. 2023;79:44–52. doi:10.1016/J.PCAD.2023.04.008
8. Whiteson JH, Bartels MN, Kim H, Alba AS. Coronary artery disease in masters-level athletes. Arch Phys Med Rehabil. 2006;87(3 Suppl 1):79–81. doi:10.1016/J.APMR.2005.12.010
9. Ha FJ, Han HC, Sanders P, et al. Sudden cardiac death related to physical exercise in the young: a nationwide cohort study of Australia. Intern Med J. 2023;53(4):497–502. doi:10.1111/IMJ.15606
10. Sato K, Shiga T, Matsuda N, et al. Mild and short recurrence of type II amiodarone-induced thyrotoxicosis in three patients receiving amiodarone continuously for more than 10 years. Endocr J. 2006;53(4):531–538. doi:10.1507/ENDOCRJ.K06-027
11. Parry-Williams G, Gati S, Sharma S. The heart of the ageing endurance athlete: the role of chronic coronary stress. Eur Heart J. 2021;42(28):2737–2744. doi:10.1093/EURHEARTJ/EHAB095
12. Senefeld J, Hunter S. Are masters athletic performances predictive of human aging in men and women?. Mov Sport Sci. 2019;2(104):5–12. doi:10.1051/sm/2019018
13. Morrison BN, Isserow S, Taunton J, et al. Masters Athlete Screening Study (MASS): incidence of cardiovascular disease and major adverse cardiac events and efficacy of screening over five years. Eur J Prev Cardiol. 2023;30(9):887–899. doi:10.1093/EURJPC/ZWAD090
14. Booth LK, Redgrave RE, Tual-Chalot S, Spyridopoulos I, Phillips HM, Richardson GD. Heart disease and ageing: the roles of senescence, mitochondria, and telomerase in cardiovascular disease. Subcell Biochem. 2023;103:45–78. doi:10.1007/978-3-031-26576-1_4
15. O’Riordan C, Savage E, Newell M, Flaherty G, Hartigan I. Cardiovascular disease risk factor profile of experienced male amateur marathon runners: a systematic review. Sports Health. 2023. doi:10.1177/19417381231176534
16. Kim JH, Malhotra R, Chiampas G, et al. Cardiac arrest during long-distance running races. N Engl J Med. 2012;366(2):28–29. doi:10.1056/NEJMOA1106468
17. Cavarretta E, Pingitore A, Peruzzi M, Sciarra L. Cardiovascular screening of the master athletes: insights from the Master Athletes Screening Study (MASS). Eur J Prev Cardiol. 2023;30(9):884–886. doi:10.1093/EURJPC/ZWAD115
18. Thompson PD, Myerburg RJ, Levine BD, Udelson JE, Kovacs RJ. Eligibility and disqualification recommendations for competitive athletes with cardiovascular abnormalities: task force 8: coronary artery disease: a scientific statement from the American heart association and American college of cardiology. J Am Coll Cardiol. 2015;66(21):2406–2411. doi:10.1016/J.JACC.2015.09.040
19. Dores H, de Araújo Gonçalves P, Monge J, Cardim N. Cardiac remodeling induced by exercise in caucasian male master athletes: a cross-sectional study. Int J Cardiovasc Imaging. 2022;38(1):69–78. doi:10.1007/S10554-021-02368-Z
20. Romano S, Minardi S, Patrizi G, Palamà Z, Sciahbasi A. Sport in ischemic heart disease: focus on primary and secondary prevention. Clin Cardiol. 2023;46(9):1021–1027. doi:10.1002/CLC.24052
21. Borjesson M, Onerup A, Lundqvist S, Dahlof B. Physical activity and exercise lower blood pressure in individuals with hypertension: narrative review of 27 RCTs. Br J Sports Med. 2016;50(6):356–361. doi:10.1136/BJSPORTS-2015-095786
22. J V T, Turner CG, Liu C, et al. Exercise blood pressure changes and aortic dilatation in male masters endurance athletes. Eur J Prev Cardiol. 2023;30(5):e18–e20. doi:10.1093/EURJPC/ZWAC250
23. Latorre-Román P, García-Pinillos F, Sánchez JS, et al. A new approach for evaluation of cardiovascular fitness and cardiac responses to maximal exercise test in master runners: a cross-sectional study. J Clin Med. 2022;11(6):1648. doi:10.3390/JCM11061648
24. Zambolin F, McPhee JS, Duro-Ocana P, Ganse B, Bagley L, Faisal A. The association of elevated blood pressure during ischaemic exercise with sport performance in master athletes with and without morbidity. Eur J Appl Physiol. 2022;122(1):211–221. doi:10.1007/S00421-021-04828-9/TABLES/2
25. Stergiou D, Duncan E. Atrial Fibrillation (AF) in endurance athletes: a complicated affair. Curr Treat Options Cardiovasc Med. 2018;20(12):98. doi:10.1007/S11936-018-0697-9
26. Climstein M, Walsh J, DeBeliso M, et al. Resting blood pressure in master athletes: immune from hypertension?. Sport (Basel, Switzerland). 2023;11(4). doi:10.3390/SPORTS11040085
27. Devan AE, Seals DR. Vascular health in the ageing athlete. Exp Physiol. 2012;97(3):305. doi:10.1113/EXPPHYSIOL.2011.058792
28. Henkin JS, Pinto RS, Machado CLF, Wilhelm EN. Chronic effect of resistance training on blood pressure in older adults with prehypertension and hypertension: a systematic review and meta-analysis. Exp Gerontol. 2023;177(2022):112193. doi:10.1016/J.EXGER.2023.112193
29. Meng J, Geng Q, Jin S, et al. Exercise protects vascular function by countering senescent cells in older adults. Front Physiol. 2023;14. doi:10.3389/FPHYS.2023.1138162
30. DeSouza, C.A., Shapiro, L.F., Clevenger, C.M., Dinenno, F.A., Monahan, K.D., Tanaka, H., Seals, D.R. Regular aerobic exercise prevents and restores age-related declines in endothelium-dependent vasodilation in healthy men. Circulation. 2000;102(20):1351–1357. doi:10.1161/01.CIR.102.12.1351
31. Shannon OM, Clifford T, Seals DR, Craighead DH, Rossman MJ. Nitric oxide, aging and aerobic exercise: sedentary individuals to master’s athletes. Nitric Oxide Biol Chem. 2022;125-126:31–39. doi:10.1016/J.NIOX.2022.06.002
32. Holloszy JO. Cellular adaptations to endurance exercise: master athletes. Int J Sport Nutr. 2001;11SUPPL. doi:10.1123/IJSNEM.11.S1.S186
33. Hayiroǧlu MI, Çinar T, Çinier G, et al. The effect of 1-year mean step count on the change in the atherosclerotic cardiovascular disease risk calculation in patients with high cardiovascular risk: a sub-study of the LIGHT randomized clinical trial. Kardiol Pol. 2021;79(10):1140–1142. doi:10.33963/KP.A2021.0108
34. Hayiroǧlu Mİ, Çinier G, Pay L, et al. The relation between average 1-year home blood pressure and the change in pro-BNP and left ventricle mass index. Blood Press Monit. 2022;27(5):327–333. doi:10.1097/MBP.0000000000000611
35. Hayiroǧlu MI, Çinier G, Yüksel G, et al. Effect of a mobile application and smart devices on heart rate variability in diabetic patients with high cardiovascular risk: a sub-study of the LIGHT randomized clinical trial. Kardiol Pol. 2021;79(11):1239–1244. doi:10.33963/KP.A2021.0112
36. Tekkeşin Aİ, Hayıroğlu Mİ, Çinier G, et al. Lifestyle intervention using mobile technology and smart devices in patients with high cardiovascular risk: a pragmatic randomised clinical trial. Atherosclerosis. 2021;319:21–27. doi:10.1016/J.ATHEROSCLEROSIS.2020.12.020
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Haemodynamic Changes in Adult Patients Transported in Emergency Medical Helicopters. A Systematic Review
Artero-García A, Gómez-Salgado J, Fernández-Carrasco FJ, Vázquez-Lara JM, García-Iglesias JJ, Mérida-Yáñez B, Muñoz-Vela FJ, Rodríguez-Díaz L
Therapeutics and Clinical Risk Management 2024, 20:775-787
Published Date: 23 November 2024
Systolic Pressure and Pulse Rate Range Performance Comparison of Seven Non-Invasive Blood Pressure Monitors
Beard J, Pichard K, Attebery JE, Yapici HO, Coffeng R
Medical Devices: Evidence and Research 2025, 18:241-246
Published Date: 13 April 2025