Back to Journals » International Journal of General Medicine » Volume 14
Study of Early Postoperative Doppler Changes Post Living Donor Liver Transplantation and Their Impact on Early Mortality and Small-for-Size Syndrome: A Retrospective Study
Authors Salman A ![]() , Sholkamy A
, Sholkamy A ![]() , Salman M
, Salman M ![]() , Omar M
, Omar M ![]() , Saadawy A
, Saadawy A ![]() , Abdulsamad A, Tourky M
, Abdulsamad A, Tourky M ![]() , Sarhan MD, Shaaban HED
, Sarhan MD, Shaaban HED ![]() , Abd Allah N, Shawkat M
, Abd Allah N, Shawkat M
Received 11 September 2020
Accepted for publication 12 January 2021
Published 28 January 2021 Volume 2021:14 Pages 309—317
DOI https://doi.org/10.2147/IJGM.S280456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ahmed Salman,1 Amany Sholkamy,1 Mohamed Salman,2 Mahmoud Omar,1 Amr Saadawy,3 Ahmed Abdulsamad,4 Mohamed Tourky,5 Mohamed D Sarhan,2 Hossam El-Din Shaaban,6 Nesrin Abd Allah,7 Mohamed Shawkat8
1Internal Medicine Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 2General Surgery Department, Faculty of Medicine, Cairo University, Cairo, Egypt; 3Radiology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 4Surgical Oncology, Alzahra Cancer Center, Dubai, United Arab Emirates; 5General Surgery Department, Omm Elmisrien General Hospital, Cairo, Egypt; 6Gastroenterology Department, National Hepatology and Tropical Medicine Research Institute, Cairo, Egypt; 7Anatomy and Embryology Department, Faculty of Medicine, Menoufia University, Shebin El-Kom, Menoufia, Egypt; 8Internal Medicine Department, Faculty of Medicine, Minia University, Minia, Egypt
Correspondence: Ahmed Salman Tel + 201000468664
Email [email protected]
Background: Adult-to-adult living donor liver transplantation (LDLT) has been a common practice because of the deficiency of deceased donor liver transplants. Liver hemodynamics differ substantially between cases with end-stage liver disease undergoing LT because of various degrees of hepatic affection, nature of implicated causative factors, and pathogenesis of the hepatic disorder. The present retrospective study primarily aimed to study the early postoperative doppler changes after adult to adult LDLT. The secondary aim was to assess these hemodynamics’ impact on early in-hospital deaths and small for size syndrome (SFSS) development.
Methods: This retrospective work was done on 123 adult cases with end-stage liver disease for whom adult LDLT was performed after exclusion of pediatric patients and those with vascular complications.
Results: Postoperative (PO) mean portal vein velocity (PVV), hepatic artery (HA) peak systolic velocity (PSV), and HA resistivity index (RI) declined gradually but significantly post adult LDLT. Phasicity of hepatic veins changes towards the triphasic waveform gradually in the early PO period. There is a notable negative relationship between PO mean PVV with PO mean HA PSV. Higher PO HA RI affected PO mortality, while higher PO PVV and lower HA PSV increased the incidence of SFSS.
Conclusion: Early postoperative Doppler changes post-LDLT (PO PVV, HA RI, and HA PSV) can affect both mortality and SFSS development.
Keywords: postoperative doppler, LDLT, small-for-size syndrome, mortality
Introduction
Adult-to-adult living donor liver transplantation (LDLT) has been a common practice because of the deficiency of deceased donor liver transplants. The percentage of adult living donor transplants is rising because of the promising results and the growing demand.1
In normal liver, several evidence-based data showed an inverse relationship between alterations in the hepatic artery (HA) blood flow and the portal vein (PV). An assumption was put that HA has a passive role, meaning that changes in portal blood flow (PBF) are counteracted by reciprocal alterations in arterial flow. Such hemodynamic interplay is known as the hepatic arterial buffer response (HABR).2
These hemodynamics differ widely between cases with end-stage liver disorders for whom LT is performed because of various degrees of hepatic dysfunction, nature of implicated causative factors, and pathogenesis of the hepatic disease.3
Orthotopic liver transplantation (OLT) usually results in increased blood flow, mainly in the portal vein. This increase results in a rise in the PV bloodstream and velocities in addition to the hepatic arterial resistance. In LDLT, the hemodynamic alterations are even more complex than the alterations in deceased donor liver transplantation (DDLT), with a more notable increase in portal blood flow and velocity.4
Post-DDLT, a high-resistance arterial bloodstream can be seen in cases with a normal hepatic artery. This phenomenon restores to baseline within a short time and is not usually linked to worsening in the general condition or impaired graft functions.5 The raised resistivity index (RI) may be due to the regulatory response and the hepatic arterial buffer mechanisms, which causes HA vasoconstriction due to increased portal blood flow, which causes a high RI with inadequate arterial blood flow.6
This series’s primary aim is to study the early postoperative doppler changes post adult to adult LDLT (namely velocities of both HA and PV, resistivity indices of HA, and phasicity of the hepatic vein). The secondary aim is to assess these hemodynamics’ impact on early in-hospital deaths and small for size syndrome (SFSS) development.
Patients and Methods
The present retrospective cohort work was done on 123 grown-up cases with end-stage liver disease for whom adult LDLT was performed from March 2008 to June 2014.
All patients who underwent LDLT during the study period were enrolled in the analysis. Exclusion criteria were pediatric patients, split liver transplantation, those who developed vascular complications such as PV or HA thrombosis, and those with incomplete or missing relevant data.
The research steps adhered to ethical instructions of the 1975 Declaration of Helsinki, confirmed by the responsible research ethical board (of Cairo University Hospitals). Patient’s consent to review their medical records was waived due to the retrospective nature of the study; however, patient data confidentiality was confirmed through data collection.
The selection of donors and recipients was made by the agreement of the liver transplant team members.
The procedure was explained to recipients and donors with possible related morbidity and mortality. All organs were donated voluntarily with written informed consent, and that this was conducted in accordance with the Declaration of Istanbul.
Child-Turcotte-Pugh (CTP) and MELD scores were used for preoperative recipient evaluation. In patients who had hepatocellular carcinoma (HCC), Milan guidance was adopted to choose patients. Assessment of recipients comprised full history, detailed clinical evaluation, relevant laboratory, and radiological evaluation involving preoperative Doppler US.
The recipient surgery included total hepatectomy of the native liver ensued by implantation of the donor’s liver.
Anastomoses were performed between the donor liver and the recipient patient. Once the PV was reconstructed, the clamps were taken out, and the liver was perfused with portal venous blood.
IOUS
IOUS was conducted after the vascular anastomoses and prior to the biliary reconstruction. Examination was done after waiting for few minutes till settlement of the early post-reperfusion hemodynamic changes. The apparatus was placed to the recipient’s right side and the lighting sources were optimized. The non-sterilized left hand was always kept in contact with the apparatus. The abdominal cavity was then filled with warm saline as a media for the US beam (the operating table was tilted to the left side to avoid fluid spillage).
BK multifrequency 7.5–10 MHz T-shaped convex array transducers with color Doppler and pulsed Doppler capabilities was used.
The hepatic veins anastomoses were identified cranially (main hepatic veins or grafts for segments 5 or 8), while the probe was placed in a transverse midline position and adjusted toward the beating heart. The PV and the HA anastomoses were situated more caudally. The main segmental branches of the HA and PV were examined by holding the transducer at the raw surface near the porta hepatis and adjusted accordingly.
Postoperative (PO) Evaluation
Patients were retrospectively observed from PO day one until their discharge or until their death. In the early PO period, patients were meticulously assessed in the ICU and then in the department when their condition stabilized.
During their hospital stay, monitoring of cases was performed by liver transplantation team.
PO evaluation included comprehensive complaint evaluation, clinical assessment, investigations, including Doppler ultrasound evaluation of the hepatic circulation.
SFSS was characterized by the presence of the following post LT: Persistently high bilirubin, coagulopathy, ascites, alteration in conscious level and/or gastrointestinal hemorrhage and/or renal impairment in more advanced cases (However, it should be noticed that there are other etiologies for renal impairment, coagulopathy, and altered conscious level other than SFSS). In the current analysis, we defined SFSS in the presence of total bilirubin > 171 µmol/L and/or output of ascitic fluid > 1 L/d two weeks after LT.7
Doppler ultrasound (US) was done every 12 hours during the first seven days and then every 24 hours till the end of the period of hospitalization or whenever clinically indicated. It was done using an ultrasonic apparatus (BK with Color Doppler equipment) employing a 3.75 MHz convex probe. The examination was done in all patients by experienced sonographers of the transplant team. The assessment was done with the cases sitting supine following a fasting period of at least 4 hours.
US was employed to evaluate the graft’s appearance, any focal masses, intrahepatic bile ducts, intra-abdominal fluid collections, and pleural effusion.
Pulsed Doppler was used to study the vascular anastomoses and hepatic perfusion. Spectral waveforms were obtained at measured angles of insonation of <60°. At first, a longitudinal cut of the artery or the vein was obtained. Afterward, the sample volume of the Doppler US system was placed in the midpart of the vessel.
The angle correction was done manually during US evaluation. The lowest obtainable velocity scale and the least obtainable wall filter were employed. The measurements were assessed three times, and an average of measurements was considered for each variable.
The hepatic artery bloodstream was evaluated at the extra-hepatic and intrahepatic levels. The Peak systolic velocity (PSV) was assessed at an aligned part of the HA “mostly at the hilum” to decrease mistakes that may be caused by angle correction or twisting of the vessel. The RI was calculated (PSV– end-diastolic velocity “EDV” divided by PSV). The sample size was 2 mm, the wall filter was 100 Hz, and the pulse repetition frequency “PRF” was 3–4.5 kHz.
PV
The diameters of the recipient side, donor side and anastomosis were measured by grey scale US. Portal vein waveform was obtained pre- and post-anastomotic and the velocity ratio was estimated to assess the extent of anastomotic narrowing. The portal velocity was measured typically in the anterior branch of the PV through a longitudinal intercostal scanning. The posterior branch of the PV was not used because the angle of incidence tends to be larger than 60°.
Hepatic Vein
Visualization of the right hepatic vein was optimized from a lateral intercostal approach near the midaxillary line. The transducer was usually placed so that forward flow in the hepatic veins (ie, out of the hepatic hilum and toward the heart) is away from the probe and is shown below the baseline, while opposite flow is above the baseline. Waves were subtyped into triphasic, biphasic, and monophasic waves. Evaluation of venous grafts or accessory veins was done in case they were reconstructed.
Statistical Analysis
Data were registered using the statistical package SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA) version 21. Qualitative variables were presented as frequency and percentage and analyzed with the Chi-square or Fisher Exact tests. Quantitative variables were presented as the mean and standard deviation and were compared to t-test or Mann Whitney test.
For comparing serial measurements, the non-parametrical Friedman test and Wilcoxon test were used. For contrasting categorical variables, Chi-square (χ2) test was used. Exact test was used instead if the anticipated frequency is lower than 5. P-values less than 0.05 were considered as statistically significant.
Results
This retrospective work was done on 123 adult cirrhotic cases who underwent adult LDLT.
Within the study group, 89.4% were males, and 10.6% were females. The age of the cases ranged from 19 to 63 years (with a mean ± SD 48.7 ± 7.58 years).
Studied patients body mass index “BMI” ranged from 18.9 to 34 kg/m2 (with a mean ± SD 27.32 ± 3.18 kg/m2).
Indications for transplantation included: Post-viral hepatitis C end-stage liver disease in 62.6% and post-Hepatitis B Virus {HBV} end-stage liver disease in 5.7%”, HCC in 22% (70.3% of them were HCV, 29.7% of them were HBV), idiopathic end-stage liver disease in 7.3%. End-stage liver disease due to an autoimmune cause, alcoholism, and primary biliary cholangitis “PBC” were equally present in 0.8% of the cases.
The CTP value before LDLT ranged from 5 to 13, while the MELD score ranged from 9 to 26 (with a mean ± SD 18.2 ± 3.76).
In all studied patients, liver grafts consisted of a right-lobe graft, excluding the middle hepatic vein (MHV).
Preoperative graft size (gm) ranged from 433 to 1300 gm (with a mean ± SD 918.04 ± 118.92 gm) and preoperative graft-recipient weight ratio “GRWR” ranged from 0.78 to 1.57 (with a mean ± SD 1.02 ± 0.17).
As to co-morbidities, 32.5% of the studied patients had diabetes mellitus, 11.4% had hypertension, and 7.3% had dyslipidemia.
Regarding CTP score, 0.8% of the studied cases were child A, 17.1% Child B, and 82.1% Child C.
Moreover, 33.3% of the studied patients had recurrent hepatic encephalopathy, 36.3% recurrent spontaneous bacterial peritonitis, 38.2% refractory ascites, and 34.1% recurrent GI bleeding.
As regards intra-operative “IO” data, studied patients received a number of units of packed red blood cells “RBCs” that ranged from 3 to 37 units (with a mean ± SD 9.47 ± 4.88). Number of received plasma units ranged from 0 to 24 (with a mean ± SD 9.15 ± 4.7), and number of received platelet units ranged from 0 to 42 (with a mean ± SD 14.7 ± 7.87), while number of cryoprecipitate units ranged from 0 to 4 (with a mean ± SD 0.39 ± 0.08).
Intra-operative “IO” US and Doppler results of the whole studied patients are illustrated in Table 1.
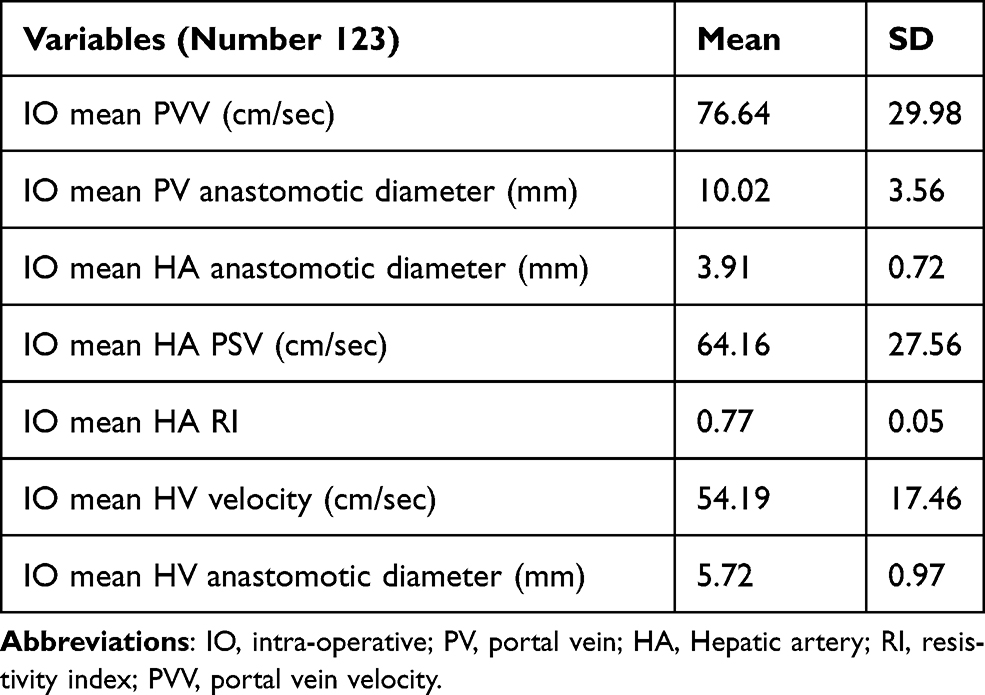 |
Table 1 Intra-Operative Doppler Parameters of the Whole Studied Patients |
Postoperatively, the duration of intensive care unit “ICU” stay ranged from 3 to 12 days (with a mean ± SD 3.77 ± 4.99), while the duration of total hospital stay ranged from 5 to 14 days (with a mean ± SD 10.52 ± 3.38). The number of PO transfused packed RBCs ranged from four to seven (with a mean ± SD 3.3 ± 1.7).
Laboratory workup of the enrolled cases early after surgery is illustrated in Table 2.
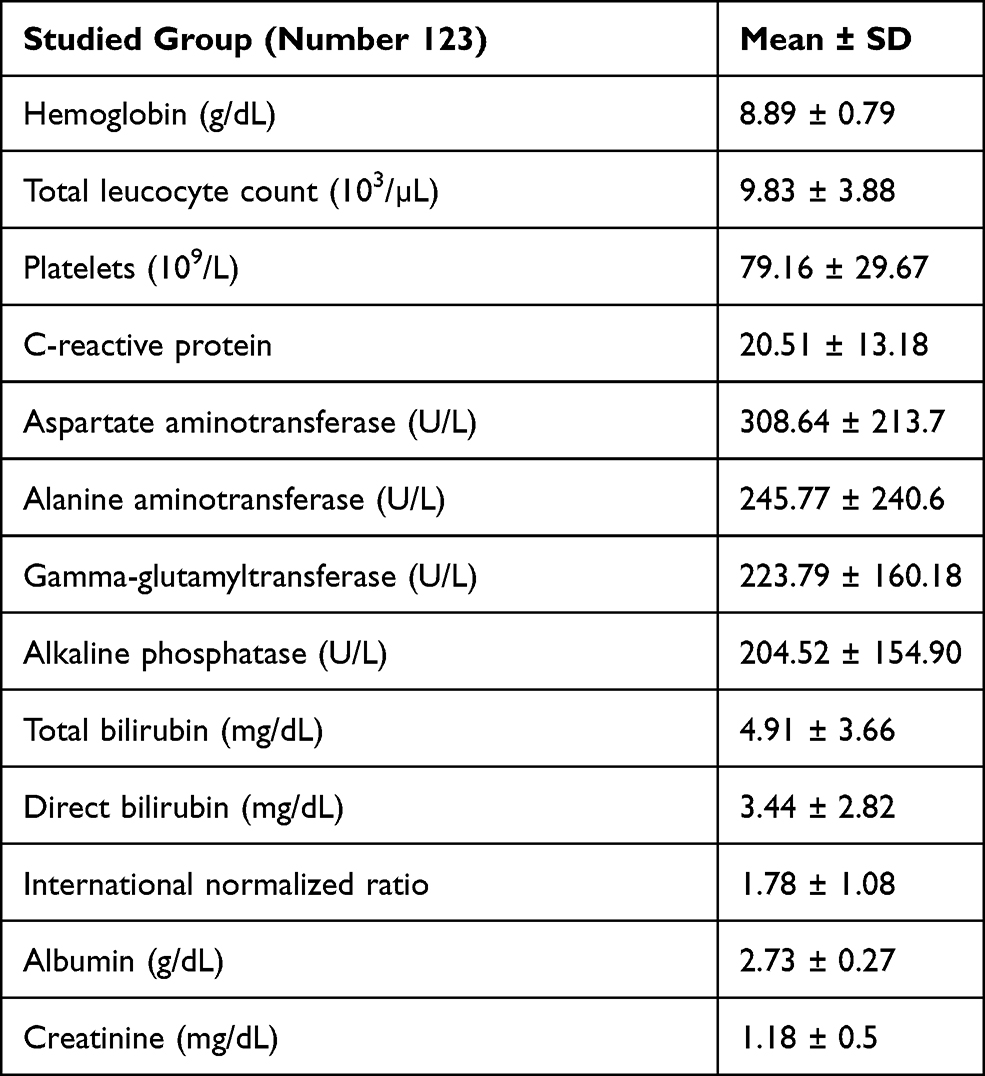 |
Table 2 Laboratory Work-Up of the Enrolled Cases Early After Surgery (First Week) |
The current work revealed that portal vein velocity (PVV) raised just post LT “in comparison to preoperative velocity” then declined gradually but significantly (P value <0.001) in the early PO period.
Mean PVV in the studied patients in the perioperative period is shown in Figure 1, while the PVV trend in the enrolled cases early after surgery is shown in Figure 2. An example of a gradual decrease of PVV after surgery in one of the studied cases is shown in Supp. Figure 1
 |
Figure 1 Mean PVV in the studied patients in the perioperative period. |
 |
Figure 2 PVV trend in the enrolled cases early after surgery. |
The present study showed that HA PSV declined gradually but significantly (P value <0.001) early after surgery. HA PSV trend in studied patients within the early PO time is shown in Figure 3
 |
Figure 3 HA PSV trend in studied patients within the early PO time. |
The present study showed that HA RI declined gradually but significantly (P value < 0.001) in the early PO period.
HA RI trend in the enrolled cases during the early PO time is shown in Figure 4, while an example of changes occurring in both RI and PSV early in the PO period in one of the studied patients is demonstrated in supp. Figure 2.
 |
Figure 4 HA RI trend in whole enrolled cases during the early PO time. |
The present study showed that the phasicity of the hepatic veins changed towards the triphasic waveform gradually in the early PO period.
HV trend in the studied patients during the early PO period is shown in Figure 5, and the typical triphasic hepatic veins waveform in one of the studied patients is demonstrated in Supp Figure 3.
 |
Figure 5 HV trend in the whole studied patients during the early PO period. |
The studied cases were categorized into two arms, the first arm who died during the PO hospitalization period, first month (Group A, 24 patients), and the second who survived this period (Group B, 99 patients). HA RI in group A was more elevated than group B, and the difference was statistically considerable (P value <0.001).
Apparent reasons for mortality were septicemia in 10 patients, acute rejection in 3 patients, biliary leak in 3 patients, myocardial infarction in 3 patients, pulmonary embolism in 4 patients, and cardiac arrhythmia in 1 patient.
Besides, PO mean PVV was more elevated in group A than group B. However, the difference has not shown a statistical significance (P value 0.342).
Moreover, the studied cases were categorized into two arms, the first one who developed SFSS (Group 1, 28 patients) and the second arm who did not develop SFSS (Group 2, 95 patients).
The current work results demonstrated that mean PV velocities were more elevated in group 1 than group 2, while, HA PSV was lower in group 1 than group 2, with statistically highly significant differences (P value <0.001).
Correlation between PO mean PVV found a statistically notable negative relationship with PO HA PSV (r = −0.575 P < 0.001)
The relationship between PO mean PVV and HA PSV is shown in Figure 6.
 |
Figure 6 Relationship between PO mean PVV and HA PSV. |
Discussion
LT is the most successful strategy for cases that have irreversible acute or chronic hepatic decompensation. In the last years, it has turned from a novel treatment with an elevated death rate to a widespread approach that has excellent survival rates.8
Postoperative Doppler evaluation of liver transplant hemodynamics provides valuable data in terms of the existence or the lack of blood flow, bloodstream orientation, velocity, and spectral waveform evaluation. It permits periodic assessment of hepatic perfusion indices.9
The current analysis demonstrated that PO mean PVV, HA PSV, and HA RI decreased slowly yet considerably post LDLT. It also displayed a notable negative relationship between PO mean PVV and PO mean HA PSV. Moreover, higher PO HA RI affected PO mortality, while higher PO PVV and lower HA PSV increased the incidence of SFSS.
Data regarding PO PV velocity suggested that it increased early after LT, relative to the preoperative status. This may be due to the continuation of the hyperkinetic splanchnic blood flow in cases with end-stage liver disease, high portal pressure, decrease in the hepatic vasculature, and narrow PV anastomosis.10 Data reported a broad extent of PV speed (15–400 cm/s) in the early post-LT time in cases with no vascular problems.11
The current work revealed that PVV raised just post LT and later decreased slowly but considerably early after surgery. Gondolesi et al, 2002, found that, immediately after LT, the mean PVV was significantly higher than before LT and decreased slowly but notably in the early post-LT period after.12
Also, Bolognesi et al, 2002 found that PVV increased immediately after transplantation and that elevated portal velocity was noted in these patients for 24 months post LT, possibly due to the persistence of high splenic blood flow.13 (yet in our study, we were limited to studying hemodynamics in the first month after LT). Moreover, Han et al, 2014 concluded that a gradual decrease of PVV was the typical change observed in the first few weeks post LT.14
The current series confirmed that HA PSV decreased slowly yet considerably in the first month after LT. The same findings were presented by Sanyal et al, 2014, who demonstrated that HA PSV decreased gradually in the early PO period.15 Besides, another study found that HA PSV decreased slowly but significantly after LT.14
It was noticed that immediately after LT, there may be decreased diastolic arterial flow, and this can cause transient hepatic arterial wave for abnormalities with subsequent changes in hepatic arterial RI.16
In the current analysis, HA RI fell slowly yet respectably post LT, and this agrees with García-Criado et al, 2009, who concluded that the presence of transient high RI in normal hepatic arteries is a common finding after LT.17 In addition, Sanyal et al, 2012 noticed a transient PO elevation of RI; nonetheless, the majority of these alterations returned to normal within the following days.16
Lack of the triphasic waves of the HV and loss of the retrograde flow pattern are thought to mirror elevated hardness of the hepatic parenchyma around the HVs and possessed a 98.4% negative predicted value for venous occlusion. On the contrary, maintained triphasic flow on Doppler ultrasound pictures can eliminate the probability of severe narrowing.18
Our results revealed that the phasicity of hepatic veins changed towards the triphasic waveform gradually in the early PO period in patients without HV complications. In line with this, a previous work demonstrated mono- or biphasic flow of the hepatic veins immediately after LT with most of these changes reverted soon to the triphasic waveform in those with no HV complications.15
On the other hand, the study presented by Han et al, 2014, showed that all the three blood flow patterns were noted in the hepatic veins without complications, and so they suggested that the aberrations in the hepatic vein waves pattern are not sure signs of hepatic vein problems as graft edema and alterations in cardiac contractility can result in odd Doppler waveforms within the hepatic veins.14
To our knowledge, few published studies correlated between PO HA RI and mortality post-adult LDLT. The current series demonstrated that HA RI was considerably higher in the mortality arm. The same finding was confirmed in a previous study revealing that HA RI elevation correlated with early PO mortality after LT.15
In contrary to these findings, Jamieson et al, 2014 concluded that low, not high, HA RI may predict early post-LT mortality “yet, their study was limited to the pediatric patients’ group.”19
For cases with end-stage liver disease, just post LT, the mechanical aspect of elevated portal pressure is alleviated by the healthy graft, yet without prompt return of the systemic or the splanchnic blood flow to average values.20 The splanchnic flow exhibits quick and possibly unsteady alterations in the portal and arterial blood flow, which may not be clinically relevant.21 However, the alterations in the portal indices by Doppler ultrasound and its effects on mortality are still under debate.
This work demonstrated that PO mean PVV was elevated in the mortality arm, and this agrees with Spitzer et al, 2010, who found that PO PVV is a substantial risk factor for early post LT mortality.22
After LT, persistently high PVV levels may result in shear stress damage to the transplanted liver; that notice appears to be more pronounced in a small-for-size (SFS) transplant in comparison with a whole liver transplant.23
The present study showed that HA PSV and mean PVV were considerably different in the SFSS arm compared to the other arm. In line with this, Lei et al, 2012, demonstrated statistically considerable variations in PO PVV and HA PSV between the SFSS arm and non-SFSS arm.24 Also, Marcos et al, 2000 noticed higher values of PO PVV in the SFSS arm in their study.25
Hepatic metabolic supply and need adjust hepatic arterial perfusion in the same manner as arterial perfusion is regulated in other systems. The main intrinsic regulation of the hepatic perfusion is the inverse PV-HA flow relationship.26
This analysis showed a negative relationship between PO mean PVV with PO mean HA PSV, and not far from this, Nakanishi et al, 2004 found that when the HA velocity increased, the portal vein velocity decreased; hence, the hepatic arterial flow during the hepatic regeneration was regulated by both the hepatic artery and portal vein.27 Furthermore, Bolognesi et al correlated HA PSV with PVV and found that early alterations in these parameters coincided with the hepatic buffer response mechanism.13
In conclusion, early postoperative Doppler changes post-LDLT, including PO PVV, HA RI, and HA PSV, can affect both mortality and SFSS development.
The present study has some limitations. The study results need to be reproduced in other series on a larger number of LDLT patients for objective validation of early hepatic vasculature changes after LDLT. Moreover, further studies for a prolonged period are needed for long-term hepatic hemodynamics evaluation. It should be noticed that in orthotopic liver transplant from a deceased donor, studying of the suprahepatic vein flow with the transesophageal echo in the operating room is now beginning to be used with promising results.28,29 Unfortunately, we did not use this technique at our center; nonetheless, further studies are warranted to assess the validity of this technique in LDLT.
Novelty of the Study
To our knowledge, few studies addressed the early PO Doppler changes after adult LDLT. Besides, we think also that analyzing the impact of PO PVV, HA RI, and HA PSV on both mortality and SFSS is quite novel in the field of adult LDLT.
This work may allude to additional potential mechanisms that may be underlying post-LT mortality and SFSS. This shall provide new horizons into the value of this work; and possibly make these topics attractive goals of future research for the improvement of the outcome of LDLT. Therefore, raising this topic may be viewed as a genuine, valuable aspect of the present work.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Abu-Gazala S, Olthoff KM. Current status of living donor liver transplantation in the United States. Annu Rev Med. 2019;27(70):225–238. doi:10.1146/annurev-med-051517-125454
2. Anders M, Alvarez D, Quiñonez E, et al. A hemodynamic study to evaluate the buffer response in cirrhotic patients undergoing liver transplantation. ISRN Transpl. 2014;2014:757910.
3. Feng A-C, Fan H-L, Chen T-W, Hsieh C-B. Hepatic hemodynamic changes during liver transplantation: A review. World J Gastroenterol. 2014;20(32):11131–11141. doi:10.3748/wjg.v20.i32.11131
4. Abdelaziz O, Attia H. Doppler ultrasonography in living donor liver transplantation recipients: intra- and postoperative vascular complications. World J Gastroenterol. 2016;22(27):6145–6172. doi:10.3748/wjg.v22.i27.6145
5. Wei WI, Lam LK, Ng RW, et al. Microvascular reconstruction of the hepatic artery in live donor liver transplantation: experience across a decade. Arch Surg. 2004;139:304–307. doi:10.1001/archsurg.139.3.304
6. Eipel C, Abshagen K, Vollmar B. Regulation of hepatic blood flow: the hepatic arterial buffer response revisited. World J Gastroenterol. 2010;16(48):6046–6057. doi:10.3748/wjg.v16.i48.6046
7. Shoreem H, Gad EH, Soliman H, et al. Small for size syndrome difficult dilemma: lessons from 10 years single centre experience in living donor liver transplantation. World J Hepatol. 2017;9(21):930–944. doi:10.4254/wjh.v9.i21.930
8. Hackl C, Schlitt HJ, Kirchner GI, Knoppke B, Loss M. Liver transplantation for malignancy: current treatment strategies and future perspectives. World J Gastroenterol. 2014;20(18):5331–5344. doi:10.3748/wjg.v20.i18.5331
9. Prabhu SJ, Kanal K, Bhargava P, Vaidya S, Dighe MK. Ultrasound artifacts: classification, Applied physics with illustrations, and imaging appearances. Ultrasound Q. 2014;2(30):145–157. doi:10.1097/RUQ.0b013e3182a80d34
10. Piscaglia F, Zironi G, Gaiani S, et al. Systemic and splanchnic hemodynamic changes after liver transplantation for cirrhosis: a long-term prospective study. Hepatology. 1999;30:58–64. doi:10.1002/hep.510300112
11. Bosch J, Pizcueta P, Feu F, Fernández M, García-Pagán JC. Pathophysiology of portal hypertension. Gastroenterol Clin North Am. 1992;21(1):1–14.
12. Gondolesi GE, Florman S, Matsumoto C, et al. Venous hemodynamics in living donor right lobe liver transplantation. Liver Transpl. 2002;8(9):809–813. doi:10.1053/jlts.2002.33690
13. Bolognesi M, Sacerdoti D, Bombonato G, et al. Change in portal flow after liver transplantation: effect on hepatic arterial resistance indices and role of spleen size. Hepatology. 2002;35(3):601–608. doi:10.1053/jhep.2002.31352
14. Han H, Liu R, Wang WP, Ding H, Wen JX, Lin XY. Postoperative hemodynamic changes in transplanted liver: long-term follow-up with ultrasonography. J Int Med Res. 2014;42(3):849–856. doi:10.1177/0300060514521153
15. Sanyal R, Zarzour JZ, Ganeshan DM, Bhargava P, Lall GC, Little MD. Postoperative doppler evaluation of liver transplants. Indian J Radiol Imaging. 2014;24(4):360–366. doi:10.4103/0971-3026.143898
16. Sanyal R, Lall CG, Lamba R, et al. Orthotopic liver transplantation: reversible Doppler US findings in the immediate postoperative period. Radiographics. 2012;32(1):199–211. doi:10.1148/rg.321115006
17. García-Criado A, Gilabert R, Berzigotti A, Brú C. Doppler ultrasound findings in the hepatic artery shortly after liver transplantation. AJR Am J Roentgenol. 2009;193:128–135. doi:10.2214/AJR.07.3919
18. Choi JY, Lee JY, Lee JM, et al. Routine intraoperative Doppler sonography in the evaluation of complications after living-related donor liver transplantation. J Clin Ultrasound. 2007;35(9):483–490. doi:10.1002/jcu.20384
19. Jamieson LH, Arys B, Low G, Bhargava R, Kumbla S, Jaremko JL. Doppler ultrasound velocities and resistive indexes immediately after pediatric liver transplantation: normal ranges and predictors of failure. AJR Am J Roentgenol. 2014;203(1):W110–6. doi:10.2214/AJR.13.11685
20. Hadengue A, Lebrec D, Moreau R, et al. Persistence of systemic and splanchnic hyperkinetic circulation in liver transplant patients. Hepatology. 1993;17(2):175–178. doi:10.1002/hep.1840170202
21. Troisi R, Cammu G, Militerno G, et al. Modulation of portal graft inflow: a necessity in adult living-donor liver transplantation? Ann Surg. 2003;237:429–436. doi:10.1097/01.SLA.0000055277.78876.B7
22. Spitzer AL, Dick AA, Bakthavatsalam HJB, et al. Intraoperative portal vein blood flow predicts allograft and patient survival following liver transplantation. HPB. 2010;12(3):166–173. doi:10.1111/j.1477-2574.2009.00137.x
23. Wu TJ, Dahiya D, Lee CS, et al. Impact of portal venous hemodynamics on indices of liver function and graft regeneration after right lobe living donor liver transplantation. Liver Transpl. 2011;17(9):1035–1045. doi:10.1002/lt.22326
24. Lei JY, Wang WT, Yan LN. Risk factors of SFSS in adult-to-adult living donor liver transplantation using the right liver: a single-center analysis of 217 cases. Hepatogastroenterology. 2012;59(117):1491–1497. doi:10.5754/hge11634
25. Marcos A, Olzinski AT, Ham JM, Fisher RA, Posner MP. The interrelationship between portal and arterial blood flow after adult to adult living donor liver transplantation. Transplantation. 2000;70(12):1697–1703. doi:10.1097/00007890-200012270-00006
26. Lautt WW. Regulatory processes interacting to maintain hepatic blood flow constancy: vascular compliance, hepatic arterial buffer response, hepatorenal reflex, liver regeneration, escape from vasoconstriction. Hepatol Res. 2007;37:891–903. doi:10.1111/j.1872-034X.2007.00148.x
27. Nakanishi S, Shiraki K, Yamamoto K, et al. Early graft hemodynamics in living related liver transplantation evaluated by Doppler ultrasonography. Int J Mol Med. 2004;14(2):265–269.
28. Vetrugno L, Barbariol F, Baccarani U, Forfori F, Volpicelli G, Rocca GD. Transesophageal echocardiography in orthotopic liver transplantation: a comprehensive intraoperative monitoring tool. Crit Ultrasound J. 2017;9:15. doi:10.1186/s13089-017-0067-y
29. Morita Y, Navas-Blanco JR, Isley M, Itani A, Kinoshita H. Hepatic vein flow index during orthotopic liver transplantation as predictive factor for postoperative early allograft dysfunction. Echocardiography. 2019;36(12):2282–2283. doi:10.1111/echo.14552
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.