Back to Journals » Advances in Medical Education and Practice » Volume 8
Student-selected component in the medical curriculum: investigations and psychiatric referral for paracetamol overdose in an accident and emergency department
Received 7 June 2017
Accepted for publication 10 August 2017
Published 23 August 2017 Volume 2017:8 Pages 611—617
DOI https://doi.org/10.2147/AMEP.S143399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
James G Cowman, Manuel Bakheet
Royal College of Surgeons in Ireland – Medical University of Bahrain, Manama, Bahrain
Background: A student-selected component (SSC) of the medical curriculum requires the student to be self-directed in locating and undertaking a placement in a clinical specialty of their choosing and completing a project. The clinical area for experience was an accident and emergency department, and our topic was a focused audit on the investigations and referral for paracetamol overdose. The purpose of this paper is twofold: to reflect on the education value to medical students of an SSC in a medical curriculum, and to highlight learning and understanding through completion of an audit.
Materials and methods: An audit approach was applied. The aim of the project study was to investigate the level of compliance with best-practice guidelines for investigations and psychiatric referral in paracetamol overdose.
Results: A total of 40 cases meeting the inclusion criteria were randomly selected. The sample had a mean age of 27 years, of whom 70.5% were female, and the ingested dose of paracetamol ranged from 0.864 to 80 g. Paracetamol abuse may present as intentional and unintentional overdose. In our study, 85% of cases were identified as intentional overdose and 76% had a history of psychiatric illness. Generally, medical management was compliant with guidelines, with some minor irregularities. The international normalized ratio was the most underperformed test.
Conclusion: Our choice of topic, paracetamol overdose, contributed to our understanding of the breadth of factors to be considered in the emergency medical management of a patient. In this regard, we had the benefit of understanding how the diagnostic and therapeutic factors, when applied in accordance with best-practice guidelines, work very effectively. The SSC impacted positively on our cognitive, personal, and professional development. In facilitating the student with choice, the SSC encouraged self-direction and proactivity. We gained experience in the discipline of research and acquired some skills in independent thinking and analysis.
Keywords: self-directed learning, medical curriculum, student-selected component, paracetamol overdose, investigations, psychiatric referral
Introduction
As part of the undergraduate medical program, medical students are required to undertake a student-selected component (SSC). As a student-option component of the program, the SSC requires the student to be self-directed in locating and undertaking a placement in a clinical specialty of their choosing. This element of the medical curriculum typically takes place in the final years of medical education, once students have commenced their clinical rotations. The aim of the SSC placement is to provide the student with experience that will facilitate exposure to clinical practice, under supervision. The early years of the program are strongly focused on the biomedical and social sciences, with minimal clinical contact, and the SSC provides the student the opportunity to integrate theory and practice. The specific objectives of our SSC were:
- to allow students choice in their medical education;
- to encourage students to be self-directed learners and to develop the skills of independent study;
- to gain experience in the discipline of research and develop the skills of critical thinking and analysis;
- to expose students in a structured way to an area/subject that they might otherwise not experience;
- to provide students with the opportunity to improve their written and verbal presentation skills;
- to explore an area of possible future career interest.
Besides providing medical students with the experience of the realities of clinical practice, the SSC also opens opportunities for the development of teamwork and interpersonal and communication skills. Importantly, the SSC provides the student with a focused clinical experience and gives them the opportunity to experience the discipline of professional behavior. In this regard, the student guidelines for the SSC require the student to commit to confidentiality, attendance, punctuality, communication, and professional behavior.
While undertaking the SSC, the student is required to identify and investigate a clinical topic of interest through the application of an empirical framework. Having a student-option component to the program requires the student to be self-directed in their learning approach. This provides a recognition of the student as an autonomous learner and stakeholder.
A review of some of seminal higher education theory supports the learning potential of the SSC, which recognizes students as stakeholders in the education process. Stakeholders are those whose lives are in some way affected by the education program.1 Traditional models of medical education have been strongly directed by medical schools, with limitations in terms of student choice. The literature suggests that when educators are more supportive of student autonomy, students not only display a more humanistic orientation toward patients but also show greater conceptual understanding and better psychological adjustment.2
Also, the notion of student evaluation as a performance indicator of quality3 has been insufficiently reflected in medical education. One of the major proponents of learning argued that success in a discipline is more likely if learning style and learning environment are matched.4 Therefore, approaches to student learning are very much influenced by the prevailing education methods and the learning culture. The learning environment has a major influence on student learning, and thus learning is context-dependent.5 Lack of choice in education content and methods are factors in reducing the quality of learning.6
The learning environment, rotational characteristics, and personal characteristics are likely to contribute to burnout among students.7 Importantly, the aspects of the learning environment that appear to have the greatest influence on student burnout are likely to be modifiable, and involve the educational climate, level of perceived support, and autonomy among students.
The purpose of this paper is twofold: to highlight and reflect on the educational value to medical students of an SSC in a medical curriculum, and to highlight the achievement of learning outcomes expected by reporting on the outcomes of an audit project. The paper also outlines the medical content of the project with the intention of guiding other medical students on the level of expectation for a similar project requirement in other medical schools. It is also believed that the content of the paper will be educationally helpful to other medical students in their studies, by demonstrating how the combination of biomedical and psychosocial elements of a case provides for a comprehensive approach to patient care.
The authors of this paper are two medical students from the Royal College of Surgeons in Ireland Medical University of Bahrain, who as part of the SSC undertook a clinical elective in the accident and emergency (A&E) department of a British hospital in February and March 2016. This specialty was of particular interest to us, as emergency medicine is not a mandatory core rotation in the medical curriculum, and thus we regarded this as an opportunity to broaden our clinical exposure and understanding of acute patient management. Following an initial period of adaptation, we commenced our clinical audit project with the support and encouragement of hospital staff.
Choice of topic: paracetamol overdose
We were encouraged to identify a patient-care topic of interest that could also benefit the work of A&E. Having encountered an interesting case of paracetamol poisoning during the first week of our attachment, we decided to focus on paracetamol overdose and conduct our audit project on the related investigations and psychiatric referral. The choice of audit area was agreed upon with our mentor and staff, who confirmed that paracetamol poisoning was a relatively common presentation to A&E. A subsequent review of the literature on paracetamol poisoning confirmed the importance of investigations in determining the best course of treatment, and given the scale of overdose, how risk assessment and psychiatric referral contribute to positive health outcomes. Our project was developed to examine the level of compliance with the guidelines and standard protocol for the investigations and psychiatric referral in paracetamol overdose.
Paracetamol is a widely used analgesic and antipyretic available as an over-the-counter medication. It is known to be very effective in therapeutic doses of 500–1,000 mg three to four times daily, with very few adverse effects. However, as an over-the-counter drug, it has been subject to abuse, and dosages in excess of 150 mg/kg carry a risk of hepatotoxicity and liver failure.8 While it is most frequently abused by 15- to 24-year-olds, death and fulminant hepatic failure are more common in those aged 40 years and above.9 Paracetamol overdose is the most common cause of hepatic failure requiring liver transplant in the UK, accounting for 48% of poisoning admissions and 100–200 deaths per year.10
An overdose of paracetamol may present initially with aspecific symptoms of nausea, vomiting, abdominal pain, diaphoresis, and malaise.11 These effects are mediated by a toxic by-product, N-acetyl-p-benzoquinone imine (NAPQI), which is formed in the metabolism of paracetamol by several P450 cytochromes. Normally, in sufficient quantities, this intermediate is effectively eliminated by the body’s natural stores of glutathione and excreted into the urine. However, in much larger doses, glutathione becomes saturated, causing a rise in the level of NAPQI that subsequently induces hepatic necrosis.12
Intentional and unintentional abuse
Paracetamol abuse presents in two main forms: intentional and unintentional. Intentional is associated with the ingestion of large amounts of paracetamol, usually with the intention of suicide, while unintentional is generally associated with patients who overuse the drug while trying to relieve pain.9 It is estimated that intentional abuse contributes to about 86% of overdoses, while unintentional abuse contributes to around 14% of cases.13
As intentional paracetamol abuse has been associated in most cases with suicidal ideation, there may be an association between psychiatric illness and the likelihood of paracetamol abuse. In a large study of 663 paracetamol-induced severe acute hepatotoxicity patients, only 110 patients had presented with unintentional abuse of paracetamol, and 75% of those were an overdose for the relief of pain. In the study, 92% of patients were willing to provide a psychiatric history and 82% reported an intentional overdose with the intent of suicide.14
Standards for paracetamol overdose
Early investigation and diagnosis of paracetamol intoxication is important. The National Institute for Health and Care Excellence (NICE)15 and ToxBase guidelines16 recommend that serum paracetamol levels, urine and creatinine (U&E), liver-function tests (LFTs), and international normalized ratio (INR) be measured at 4–15 hours after ingestion of the paracetamol overdose (NICE 1.5.1.18). If the serum paracetamol level is deemed significant, the patient should be administered the antidote, a titrated dose of N-acetylcysteine (NAC) (NICE 1.5.2.2).15 Following treatment with NAC, the blood tests (serum paracetamol, U&E, LFTs, and INR) should be repeated prior to discharge (ToxBase).16
Measured plasma concentration levels are usually plotted on a nomogram to determine the need for treatment with NAC. Previously, the threshold for NAC treatment was 150 mg/L at 4 hours; however, in 2012 the UK’s Commission on Human Medicines reviewed their guidelines and advised the administration of NAC at a lower threshold on the nomogram – 100 mg/L. This is to reduce the risk of withholding antidote administration to patients of borderline risk and also reduce the subsequent risk of developing hepatotoxicity.17
For a patient who has presented with self-harm, the NICE guidelines recommend that a psychosocial assessment be undertaken prior to discharge. This includes an assessment for mental capacity and mental illness. This pertinent information should be recorded clearly in the patient’s notes and made available to their general practitioner and the relevant mental health services for rapid follow-up (NICE 1.4.3.1).15
Materials and methods
An audit approach was utilized in this study as a means of providing feedback on the level of compliance with predetermined A&E standards and guidelines for investigation and psychiatric referral in cases of paracetamol overdose. Guidelines for clinical practice are increasingly utilized in health care and promote the enhancement of standards; however, the uptake of practice guidelines is often very low.18 Concern has also been expressed that the proliferation in published guidelines has prompted questioning of credibility and that the use of clinical guidelines could be undermined by a lack of robustness in the development of criteria.19
The authors searched the most utilized and authoritative guidelines used for paracetamol poisoning in the UK as per the NICE and ToxBase guidelines.15,16 The aim of the study was to investigate the level of compliance with the NICE and ToxBase guidelines, and accordingly three key research questions related to best practice were agreed upon:
- were the relevant blood tests (serum paracetamol levels, U&E, LFTs, INR) measured after the 4 hours postingestion? (NICE 1.5.1.18);
- in cases where NAC was administered, were follow-up blood tests (serum paracetamol levels, U&E, LFTs, INR) performed before discharge? (ToxBase);
- in cases of intentional overdose, was there evidence of psychiatric referral for a psychosocial assessment? (NICE 1.4.3.1).
An examination of current practice, including a retrospective documentary analysis of handwritten clinical records of patients presenting with paracetamol overdose, was conducted. Using the hospital’s Symphony database of patient records, a sample of 40 A&E attendees with a final diagnosis of paracetamol overdose who met the inclusion criteria in the year 2015 was generated. An independent person not associated with the study (an IT technician) selected the first 40 patients for the same period during the previous year, which would reflect a time of year similar to our attachment. At this point, the 2016 records had not been fully uploaded onto the electronic medical record system.
The 40 patients who met the inclusion criteria presented to A&E over the course of 5 months: included March–July. The same sample size, considered representative, was agreed upon with our mentor and deemed acceptable by our university professor, coordinating the program. Data were collected from the selected records in a comprehensive, prepared grid on Microsoft Excel. The inclusion criterion for a case was any patient with a final diagnosis of paracetamol overdose. Any record that contained inadequate recording of data was excluded. Indeed, a secondary objective of the study was to examine the standard of record keeping among the cases reviewed.
As provided by the university, the SSC project guidelines stipulate the requirement for the student to conduct an audit or research project. However, students were encouraged to undertake projects based on an audit to avoid the necessity of submission to a research-ethics committee, which would have been prohibitive, given the limited time frame of the SSC. We were accepted onto the placement by the hospital, with the understanding of our requirement to undertake an audit to achieve the learning objectives. The authors adhered to best-practice principles in managing data, including confidentiality and anonymity, storage, and access to data. We declared a commitment to patient confidentiality and anonymity in all data related to this project. The project involved documentary analysis, and did not engage patients or staff in the data-collection process. No record of personal patient information was retained or used for any purpose other than the audit.
Results
A total of 40 cases were selected from the Symphony database. To aid data collection and recording, a grid was created to document findings clearly, concisely, and objectively. From the 40 records reviewed, six were excluded on the basis of inadequate recording of data. The exclusion of the six records left a sample of 34 cases to be included in the study. The sample consisted predominantly of women (70.5%) and had a mean age of 27 years with a range of 1–65 years. The ingested dose of paracetamol ranged from 0.864 to 80 g, and 85% (n=29) of cases were identified as intentional overdose.
Of the 34 patients, 33 had their blood taken for testing appropriately, at least 4 hours postingestion, in accordance with the NICE guidelines. There was one incident where bloods were taken at the third hour, but this error was soon recognized and the bloods repeated later that day. In only one case of the 34, a child with accidental overdose, was blood not taken, due to difficulty accessing a vein and perceived negligible ingestion. The practice of performing the four different blood tests at presentation and after treatment with NAC is outlined in Table 1.
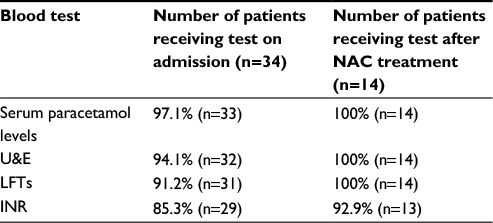 | Table 1 Blood tests performed on admission of patients to the Accident and Emergency Department and following N-acetylcysteine (NAC) treatment Abbreviations: U&E, urine and creatinine; LFTs, liver-function tests; INR, international normalized ratio. |
Serum paracetamol level was the most performed test at initial presentation to A&E, with recorded testing in 97.1% (n=33) of cases. U&E followed by LFTs were completed in 94.1% (n=32) and 91.2% (n=31) of patients, respectively. The most underperformed blood test was the INR, with no clear indication of testing in 14.7% of cases (n=5). Of the 34 cases, 14 patients appropriately received NAC due to significant levels of paracetamol in their blood. Serum paracetamol levels, U&E, and LFTs were appropriately checked in all of these cases before discharge. However, the INR was shown to be underperformed, with 7.1% of cases (n=1) not having any clear record of completion.
Intentional overdose accounted for 85% (n=29) of cases, of which 76% (n=22) had a previous history of psychiatric illness, such as depression, unstable personality disorders, and anorexia nervosa. Furthermore, 38% (n=11) of the intentional overdoses had a medical history of previously attempted overdose. Table 2 shows the practice of psychiatric referral of cases where intentional overdose was involved. In 6.9% (n=2) of cases, there was no indication in the clinical notes of the patients being referred for psychiatric assessment. Only one patient “left the department”, which infers that the patient did not wait to be seen by the attending doctor.
 | Table 2 Psychiatric referral for psychosocial assessment in intentional overdose cases prior to discharge |
Discussion
The SSC greatly enhanced our learning in a number of significant ways by impacting positively on our cognitive, personal, and professional development. In facilitating the student with choice, the SSC encouraged self-direction and proactivity. We had to decide on a clinical specialty area and then proceed to identify a hospital and a medical consultant who would accept us for the 6-week clinical placement.
The requirement to undertake a structured project for our assessment encouraged us to negotiate and agree with the unit on an appropriate topic for investigation. Our choice of topic, paracetamol overdose, contributed to our understanding of the breadth of factors to be considered in the management of a patient. In this regard we had the benefit of understanding how the diagnostic and therapeutic factors, when applied in accordance with best-practice guidelines, work very effectively. Best practice (NICE and ToxBase guidelines) recommends that plasma paracetamol levels and other blood tests be measured between 4 and 15 hours. Outside this range, they are deemed unreliable. Having the opportunity to observe the interplay among practice guidelines, medical practice, and monitoring was a new and important learning experience, in particular the circumstances surrounding the engagement of mental health services and the multifaceted concept of teamwork in the reality of clinical practice.
An objective of the SSC was to gain experience in the discipline of research and develop the skills of independent thinking and analysis. In undertaking a structured project for assessment, we were required to review and select an appropriate inquiry method that was consistent with the research process. We had to undertake a review of the literature, including best-practice guidelines, data collection, and data analysis, and this provided us with a sense of the challenges of applying a methodological and systematic approach in reviewing a clinical problem. Our verbal communication skills were enhanced through being placed in the reality of clinical practice and having to interact and communicate with other members of the health-care team and develop a sense of the importance of teamwork. Our writing and verbal skills were sharpened through writing a report and providing an oral presentation on our project. We believe that the additional efforts in preparing a paper publication in an indexed journal would set a standard for other students, and it is a fitting approach that medical students aim for publication in reporting on substantial work.
On a personal level, our attachment in A&E offered some invaluable insights. It served as an opportunity to broaden our sense of future career prospects and exposed us to a specialty that we may not otherwise have encountered in our curriculum. By the end of our attachment, we both agreed that we would be more likely to pursue a career in the field of emergency medicine. This was partly due to having an experienced mentor who provided structured exposure to the clinical activity in A&E with robust teaching and research direction. We felt very much in control of our own education in our responsibility to organize our attachment and project area, which was consistent with our learning objectives for the SSC.
From a professional and health-service perspective, we were very satisfied to note the high level of compliance of the services with best-practice guidelines for paracetamol overdose. There was an effective acute medical management approach and an efficient psychiatric referral system for patients with paracetamol overdose. Given the exclusion of six records on the basis of inadequate recording of data, perhaps policy and further direction to staff in relation to the maintenance of clinical records is encouraged. The INR was found to be the most underperformed test at initial presentation and after NAC treatment. To address this issue, we would recommend the use of a simple form with checkboxes to be completed at the time of care.
Conclusion
The SSC was a very positive learning experience. Its strengths are that it provides choice and self-direction to students and thus encourages the growth of interpersonal learning skills. Early in the program, the medical student is exposed in a structured way to an area/subject that they might otherwise not experience. Early exposure to working with the medical team is very valuable, and allowed the students to explore an area of possible future career interest.
A limitation of this paper and study is that it was an audit, and thus lacked an empirical approach; however, this may be counteracted by the fact that it aimed to provide in-depth reflections incorporating the personal and professional understanding of two medical students. The study was based on a small sample population and a short time frame, and this may have introduced limitations in representativeness. However, based on a cursory overview of the overall database, the authors do believe that the cases included in this project do reflect the general profile of patients presenting to A&E with paracetamol overdose. In terms of sampling, ideally a more comprehensive systematic method should have been employed to establish stronger conclusions. Another limitation is the use of a retrospective sample as a basis of making recommendations on clinical practice. A study based on a retrospective review of patient records may inform us if something was not documented; however, this does not indicate definitively that a patient procedure was not conducted.
In our limited clinical exposure to date in Bahrain, we have encountered a very small number of paracetamol-overdose cases. There is a paucity of published literature on the topic in Bahrain. A single case–control study from 1997 was located, which reported a prevalence of 105 per 100,000 people in Bahrain, and this is considered lower than the rates reported in the West but higher than those for the region.20 It is thus recommended that this study be repeated with a Bahrain population of patients. This would facilitate an interesting comparative analysis of paracetamol overdose in different jurisdictions.
Acknowledgments
The authors acknowledge the support and guidance of mentors and all clinical staff in the A&E department of the hospital, and also university academic staff for their guidance and reading drafts of this paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
Weiss CH. The stakeholder approach to evaluation: origins and promise. New Dir Program Eval. 1983;1983(17):3–14. | ||
Williams GC, Deci EL. The importance of supporting autonomy in medical education. Ann Intern Med. 1998;129(4):303–308. | ||
Ramsden P. A performance indicator of teaching quality in higher education: the course experience questionnaire. Stud High Educ. 1991;16(2):129–150. | ||
Kolb DA. Experiential Learning: Experience as the Source of Learning and Development. 2nd ed. Upper Saddle River (NJ): Pearson; 2014. | ||
Ramsden P, Entwistle NJ. Effects of academic departments on students’ approaches to studying. Br J Educ Psychol. 1981;51(3):368–383. | ||
Beckwith JB. Approaches to learning, their context and relationship to assessment performance. High Educ. 1991;22(1):17–30. | ||
Dyrbye LN, Thomas MR, Harper W, et al. The learning environment and medical student burnout: a multicentre study. Med Educ. 2009;43(3):274–282. | ||
Qureshi Z, Maxwell SR. Paracetamol overdose. In: The Unofficial Guide to Prescribing. London: Churchill Livingstone; 2014:111–113. | ||
Schmidt LE. Age and paracetamol self-poisoning. Gut. 2005;54(5):686–690. | ||
Tanne J. Paracetamol causes most liver failure in UK and US. BMJ. 2006;332(7542):628. | ||
DynaMed Plus. Acetaminophen poisoning. 1995. Available from: https://www.dynamed.com/topics/dmp~AN~T113862/acetaminophen-poisoning#history-and-physical. Accessed June 1, 2017. | ||
Ben-Shachar R, Chen Y, Luo S, Hartman C, Reed M, Nijhout HF. The biochemistry of acetaminophen hepatotoxicity and rescue: a mathematical model. Theor Biol Med Model. 2012;9:55. | ||
Gyamlani GG, Parikh CR. Acetaminophen toxicity: suicidal vs. accidental. Crit Care. 2002;6(2):155–159. | ||
Craig DG, Bates CM, Davidson JS, Martin KG, Hayes PC, Simpson KJ. Overdose pattern and outcome in paracetamol-induced acute severe hepatotoxicity. Br J Clin Pharmacol. 2011;71(2):273–282. | ||
National Institute for Health and Care Excellence. Self-Harm in Over 8s: Short-Term Management and Prevention of Recurrence. London: NICE; 2004. | ||
ToxBase [website on the Internet]. Available from: https://www.toxbase.org. Accessed April 1, 2016. | ||
Bateman DN, Carroll R, Pettie J, et al. Effect of the UK’s revised paracetamol poisoning management guidelines on admissions, adverse reactions and costs of treatment. Br J Clin Pharmacol. 2014;78(3):610–618. | ||
Sheldon T, Cullum N, Dawson D, et al. What’s the evidence that NICE guidance has been implemented? Results from a national evaluation using time series analysis, audit of patients’ notes, and interviews. BMJ. 2004;329(7473):999. | ||
Grilli R, Magrini N, Penna A, Mura G, Liberati A. Practice guidelines developed by specialty societies: the need for a critical appraisal. Lancet. 2000;355(9198):103–106. | ||
al-Ansari AM, Hamadeh RR, Matar AM, Buzaboon B, Marhoon H, Raees AG. Overdose among youth in Bahrain: psycho-social characteristics, contact with helping agencies and problems. J R Soc Health. 1997;117(6):366–371. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.