Back to Journals » Risk Management and Healthcare Policy » Volume 19
Student-Led Health Education Intervention Package Enhanced Tuberculosis Prevention in Colleges: A Quasi-Experimental One-Group Pre-Test/Post-Test Study
Authors Chen X ![]() , Wang M, Peng L, Zhou L, Wang F, Zu Z, Peng Y, Wang Y, Chen B
, Wang M, Peng L, Zhou L, Wang F, Zu Z, Peng Y, Wang Y, Chen B ![]()
Received 14 April 2026
Accepted for publication 5 June 2026
Published 12 June 2026 Volume 2026:19 616517
DOI https://doi.org/10.2147/RMHP.S616517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Keon-Hyung Lee
Xinyi Chen,1,2,* Min Wang,3,* Liai Peng,4,* Lin Zhou,1,2 Fei Wang,1 Zhipeng Zu,1 Ying Peng,1,2 Yinan Wang,5 Bin Chen1,2
1Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang, People’s Republic of China; 2Zhejiang Key Laboratory of Vaccine, Infectious Disease Prevention and Control, Hangzhou, Zhejiang, People’s Republic of China; 3Quzhou Center for Disease Control and Prevention, Quzhou, Zhejiang, People’s Republic of China; 4Department of Tuberculosis Control and Prevention, Shenzhen Baoan Center for Chronic Diseases Control, Shenzhen, Guangdong, People’s Republic of China; 5Department of Chronic Diseases Control and Prevention, Yuhuan Center for Disease Control and Prevention, Taizhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Chen, Email [email protected]
Objective: Tuberculosis (TB) remains a major public health threat, and colleges are crucial yet challenging settings for sustainable TB control. This study evaluated a standardized, student-led, multi-component intervention package designed to improve TB-related knowledge, attitudes, and practices (KAP) among college students in Zhejiang Province, China.
Methods: Conducted across 20 colleges from March 2022 to June 2023, this quasi-experimental one-group pre-test/post-test design study implemented a novel health education intervention package that integrated five activities. KAP data were collected using an electronic questionnaire at baseline and post-intervention. Data on TB patients and delays were collected through the Tuberculosis Information Management System. The Mann–Whitney U-test was used for delay time analysis.
Results: Valid responses included 4414 pre- and 4133 post-intervention. Overall, core knowledge of TB increased from 81.6% to 83.4% (P < 0.001). Significant improvements were seen in symptom recognition and care-seeking intent (P < 0.05). Regarding beliefs, the proportion who considered TB health education in schools “very necessary” increased from 53.5% to 57.8% (P = 0.001), while the proportion willing to proactively share knowledge with others rose from 90.9% to 92.5% (P = 0.007). Regarding behaviors, the proportion of current smokers decreased from 3.3% to 2.2% (P = 0.002), and the proportion of students frequently resting after 11 p.m. decreased from 70.2% to 64.3% (P < 0.001). Voluntary care-seeking among TB patients increased from 69.1% to 76.6%, while median patient delay decreased from 3 days to 0 (P < 0.001).
Conclusion: This report adds to the literature by demonstrating the effectiveness of a participatory, multi-faceted health education model within the college population. The findings provide a replicable example for campus-based health promotion and offer clear implications for strengthening institutional public health strategies.
Keywords: tuberculosis, health education, college students, knowledge attitudes practices, quasi-experimental study, health promotion
Introduction
Tuberculosis (TB), a chronic respiratory infectious disease caused by Mycobacterium tuberculosis (MTB), has its determinants firmly rooted in social and health factors. According to the World Health Organization’s (WHO) Global Tuberculosis Report 2023, an estimated 10.6 million people contracted TB in 2022, with the annual incidence declining at an alarmingly slow pace and even increasing by 3.9% during 2020–2022.1 Particularly, men and women aged ≥15 years accounted for nearly 88% of the people who developed TB,1 highlighting adolescents and young adults as a critical demographic for targeted interventions.
China, ranking as the forth highest TB burden country among the 30 high-burden nations worldwide, faces significant challenges in TB control. In 2022, the country reported an estimated 748,000 new TB cases, corresponding to an incidence rate of 52 cases per 100,000 population.1 Between 2004 and 2021, a total of 908,171 student TB cases were reported nationwide in China, accounting for 5.37% of all reported TB cases in the general population. Notably, a significant upward trend in reported incidence was observed specifically during the period 2015–2019.2 In recent years, the dramatic expansion of higher education enrollment in China has led to sustained growth in the college student population, making infectious disease prevention and control on college campuses a critical public health priority.2,3 The educational environment, characterized by prolonged close contact in classrooms, dormitories, and social gatherings, creates highly conducive conditions for TB transmission.4 In this context, college students (aged 18–25 years) represent one of the most vulnerable groups for TB infection and transmission.5 Successive outbreaks of TB in colleges across different provinces underscore the urgency of developing effective campus-based prevention and control strategies.6,7
Beyond screening and treatment interventions, health promotion constitutes a critical component of comprehensive TB prevention strategies. Effective health education aims to increase awareness of disease prevalence, transmission routes, symptoms, and preventive measures, thereby enabling early detection, reducing stigma, promoting timely health-seeking behavior, and fostering protective habits.8,9 However, the effectiveness of traditional top-down TB health education in Chinese colleges is hampered by its typically ad-hoc nature, inconsistent delivery, and passive student participation.10,11 These constraints significantly undermine the potential for developing sustained student awareness and proactive prevention behaviors.
The study region, Zhejiang Province, a densely populated and economically developed region of China, exemplifies these challenges. Despite implementing measures aligned with the WHO’s “End TB Strategy”, the province reported over 30 school-related TB outbreaks in 2021, with approximately one-third occurring specifically within higher education institutions.12 Colleges in this region face heightened risk due to high population density, significant student mobility, and a pre-intervention TB awareness rate of only 38% – well below the national target (above 85%).13 Additionally, previous campus TB education in the study province mainly relied on top-down lectures and the distribution of informational materials that failed to engage students or produce sustained behavioral change. Research indicates that the effectiveness of one-off health education diminishes over time; therefore, TB health education in schools must emphasize long-term, systematic, and continuous efforts.
Based on these lessons learned, this study developed a novel, student-led, multi-component health education intervention package. This package integrates five standardized, mandatory core activities. This approach aims to create a sustained, engaging, and student-centered ecosystem for TB prevention, moving beyond one-off campaigns to foster long-term behavioral change. Therefore, this study aimed to assess the impact of the package on TB knowledge, attitudes and practices (KAP) among undergraduates, and explore optimization strategies for campus TB prevention.
Methods
Study Design and Setting
A quasi-experimental, one-group pre-test/post-test study was conducted from March 2022 to June 2023 in Zhejiang Province, eastern China. The intervention package was delivered to the campus of the colleges. Pre-intervention data were collected at baseline (pre-intervention phase), followed by implementation of the intervention package (intervention phase), after which post-intervention data were collected (post-intervention phase).
Zhejiang Province, comprising 11 prefecture-level cities and 90 counties, stands as one of the most densely populated and economically advanced regions in China. As of the end of 2023, its resident population reached 66.27 million, marking an increase of 500,000 from the previous year. As of 2023, Zhejiang Province ranks 11th nationally in the number of higher education institutions, with a total of 109 colleges, primarily located in the southern and northern regions.
Participants and Sampling
A multi-stage stratified cluster sampling method was employed. Sample size was calculated assuming an expected intervention effect size of 5%, α = 0.05, and power = 0.8, and a design effect of 2.5 to account, yielding a required sample size of approximately 4000 participants per survey round. In the first stage, four prefecture-level cities were selected from the study province to ensure representativeness across geographic regions and varying TB incidence levels (Figure 1). In the second stage, from these four selected cities, a total of 20 colleges were randomly selected from the official registry of higher education institutions using a computer-generated random number sequence, stratified by institution type (comprehensive, science/engineering, medical, and arts) to reflect the diversity of the provincial student body. In the third stage, within each selected college, approximately 8 to 10 first- and second-year classes were randomly selected. Finally, following informed consent procedures, 20–25 students (balanced by gender) were randomly selected from these classes for study inclusion (Figure S1). All participants were full-time undergraduate students aged 18–25 years. Non-student individuals, students refusing to participate: students on long‑term leave or exchange programs outside the province during the study period, or students unable to complete the questionnaire independently were excluded. The post-intervention survey targeted students from the same 20 colleges, using the same sampling approach to select second- and third-year students, aiming to capture the cohort exposed to the intervention during the academic year.
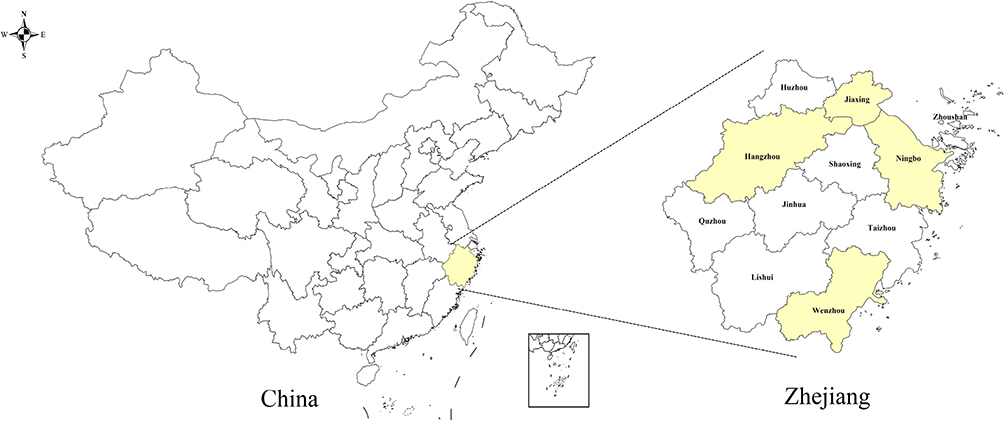 |
Figure 1 Geographic location of the study site. |
Procedures
During pre-intervention phase, professionals from TB department of local Center for Disease Control and Prevention (CDC) trained school health education coordinators, student volunteers, and medical staff on the purpose of the study and the intervention measures to be taken. Subsequently, a pre-designed structured electronic questionnaire was used to collect the following data from the respondents: socio-demographic data, respondent’s KAP regarding TB. Data on students with TB in 2021 from each college were collected through the Tuberculosis Information Management System (TBIMS), including health-seeking behaviors, date of symptom onset, date of initial medical consultation, and date of diagnosis.
Following the baseline survey, youth volunteer groups at each participating college implemented the intervention measures. The intervention package was newly developed, drawing on national TB control guidelines and a literature review of effective campus health education strategies adapted for college contexts, and was subsequently implemented as a standardized package across all participating colleges. The selection prioritized activities with proven feasibility and scalability in Chinese college settings, which comprised the following five components: (1) themed publicity around World Tuberculosis Day; (2) regular in-campus promotion via new media platforms (one issue per month); (3) annual campus TB prevention knowledge competition; (4) during the September back-to-school season, combine TB awareness campaigns with freshmen health check-ups; (5) special TB prevention and control activities on important disease prevention days (no less than three times).
The intervention spanned a period of fifteen months. Upon its completion, participants were asked to complete the same questionnaire used in the baseline survey to evaluate changes in their TB-related knowledge, attitudes, and health behaviors. Similarly, data on student TB cases from each college in 2022—including treatment-seeking behavior, dates of symptom onset, first medical consultation, and diagnosis—were also collected via the TBMIS.
Data Collection
This study utilized standardized electronic questionnaires to collect data before and after the intervention period, which were developed based on the Technical Specifications for Tuberculosis Prevention and Control in China (2020 Edition) and the Work Standards for Tuberculosis Prevention and Control in Schools (2017 Edition), supplemented by comprehensive literature review and expert consultation. The questionnaire encompassed three key domains: sociodemographic characteristics, assessment of core KAP regarding TB in the school setting, and the acceptance of TB health education. The assessment of TB knowledge comprised eight core questions (Table S1). The evaluation of attitudes and practices toward TB mainly encompasses the following dimensions: perceived necessity of TB education, risk perception, disease-related stigma, willingness to share knowledge, and self-reported health behaviors such as smoking, sleep habits, and hygiene practices. Each item presented in a multiple-choice format with only one correct answer per question, ensuring precise evaluation of participants’ understanding.
Quality Control
The provincial CDC oversaw sampling and supervision, while the county-level CDCs managed on-site implementation and questionnaire collection. All investigators received a 2-day provincial-level training covered study purpose, study protocols, questionnaire administration, and survey norms, followed by a unified assessment to ensure consistency. Permission was obtained from the administrative office of each participating college through a formal letter from the provincial CDC. All schools provided written approval. Participants were briefed on the study purpose and required to independently complete the survey independently with a minimum response time of 5 minutes. The provincial CDC conducted daily checks of electronic responses for quantity, completeness, and logical consistency, with all data consolidated into a unified provincial database for final quality verification.
Definitions
Pre- and post-intervention knowledge levels were assessed using awareness rates, and the formula was as follows:14



Changes in student health-seeking behaviors were quantitatively assessed through two primary metrics: rate of active visit for symptoms and delays. “Rate of active visit for symptoms” referred to the proportion of individuals who, upon self-recognition of TB suspicious symptoms, voluntarily sought diagnosis and treatment at local TB dispensary, among all TB cases confirmed within the year.
Delays were systematically categorized and quantified as follows: patient delay (the interval between initial symptom onset and first healthcare-seeking behavior), health facility delay (the duration between the first contact with health facility and the confirmation of the diagnosis), and total delay (the sum of both).15
Statistical Analysis
Data management was performed in Microsoft Excel 2019, followed by statistical analysis in R (version 4.3.2; R Foundation for Statistical Computing). Descriptive analysis was performed to describe the characteristics and variables based on two pre and post surveys. The package’s impact on TB knowledge awareness was evaluated across demographic subgroups through pre-post intervention analysis. The delay time of student TB patients was statistically analyzed by Mann–Whitney U-test and compared before and after the intervention. P-values were 2-tailed with statistical significance set at 0.05.
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Institutional Review Board of Zhejiang Provincial CDC, with approval number [AF/SC-06/01.0]. The study complies with the Declaration of Helsinki. All study methods were carried out in accordance with relevant guidelines and regulations. All participants were given a detailed explanation about the study with the emphasis that participation was completely voluntary. Data confidentiality was maintained throughout the study.
Results
Basic Information of Participants
Application of the package yielded 4427 pre-intervention and 4142 post-intervention returned questionnaires. Following quality control, 4414 (99.7%) and 4133 (99.8%) valid questionnaires were retained for analysis. The general profile of the participants in the two surveys was shown in Table 1. The mean age of participants at baseline and post-intervention was 19.9 (standard deviation 1.1) years and 20.4 (standard deviation 1.5) years, respectively. Socio-demographic characteristics revealed significant differences in sex, age, grade, major, student origin, monthly living expenses, previous TB health education and self-reported contact history with TB patients between the two surveys (all P < 0.05). These two surveys remained homogeneous in Han ethnicity predominance (96.1% vs 96.2%), rural residency (64.4% vs 64.6%), and parental education levels (nearly 40.0% of fathers and more than 38.0% of mothers completed junior high school).
 |
Table 1 Socio-Demographic Characteristics of the Participants |
Respondents’ Awareness of TB Knowledge
Pre-intervention, the mean number of correctly answered knowledge items among all participants was 6.53 (median = 7, IQR: 6–8). Post-intervention, the mean score improved to 6.67 (median = 7, IQR: 6–8). The distribution of correct responses post-intervention differed from baseline (Wilcoxon signed-rank test, P < 0.001) (Figure 2).
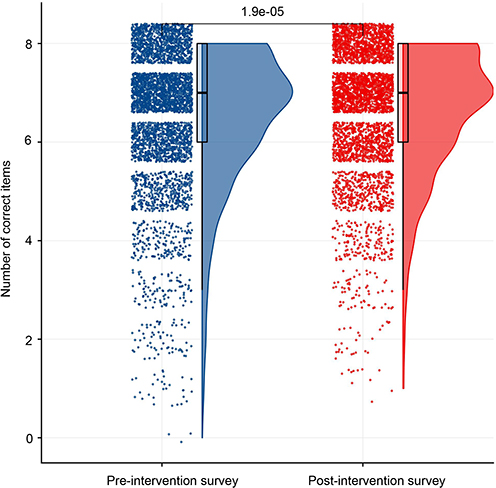 |
Figure 2 Distribution of correct answers before and after the intervention. |
Pre-intervention, 2680 participants (60.7%) correctly answered more than 6 items, while 3 individuals (0.1%) provided incorrect responses for all core information. The entire awareness rate was 25.3%. Post-intervention, the proportion of participants responding ≤4 items correctly was lower, with no cases (0%) of complete misinformation. Notably, 2649 participants (64.1%) achieved > 6 correct responses, including a 29.1% full awareness rate (Figure 3).
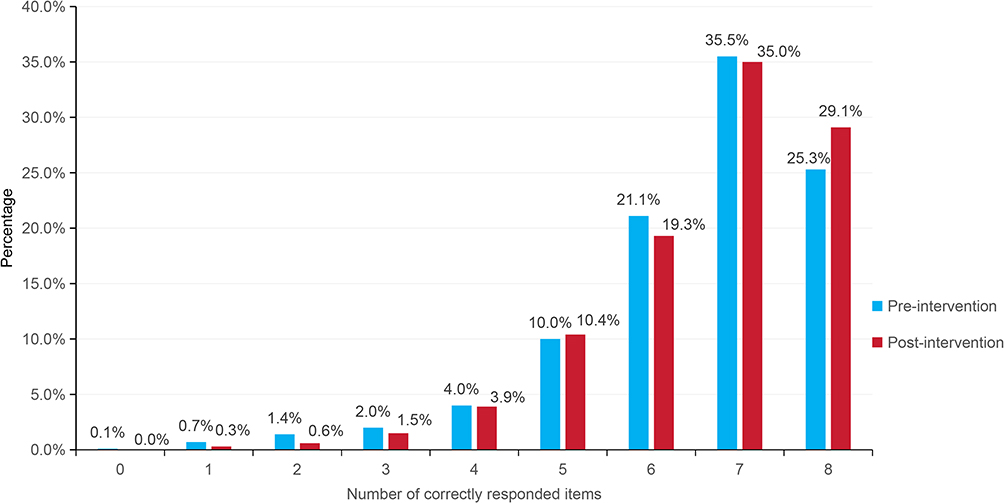 |
Figure 3 Percentage of correct TB knowledge items answered pre- and post-intervention. |
The overall TB knowledge awareness rate increased from 81.6% pre-intervention to 83.4% post-intervention (P < 0.001) (Figure 4). Changes in specific knowledge items are presented in Table S2. The proportion correctly identifying “coughing with sputum for ≥2 weeks or bloody sputum” as a TB indicator increased from 91.1% to 93.6% (χ2 = 23.918, P < 0.001). Participants selecting “visit a designated TB medical institution” rose from 96.2% to 97.0% (χ2 = 16.679, P = 0.001). Certainty about TB curability increased from 75.7% to 78.2% (χ2 = 9.509, P = 0.023). And correct responses to “report to school authorities without concealing symptoms” increased from 83.5% to 85.1% (χ2 = 20.592, P < 0.001). Awareness of “frequent ventilation” as an effective measure improved from 76.1% to 78.8% (χ2 = 9.140, P = 0.027). Correct identification of “balanced diet, regular sleep, and exercise” improved from 88.2% to 90.7% (χ2 = 20.850, P < 0.001). Regarding knowledge of TB classification, the majority of participants correctly identified TB as a chronic infectious disease both pre- (51.0%) and post-intervention (51.7%), with no statistically significant change (χ2 = 0.713, P = 0.870). While 90.7% (pre) and 91.7% (post) recognized respiratory transmission, confusion about bloodborne (1.4% vs 1.3%) and digestive routes (1.8% vs 2.0%) persisted (χ2 = 6.284, P = 0.099).
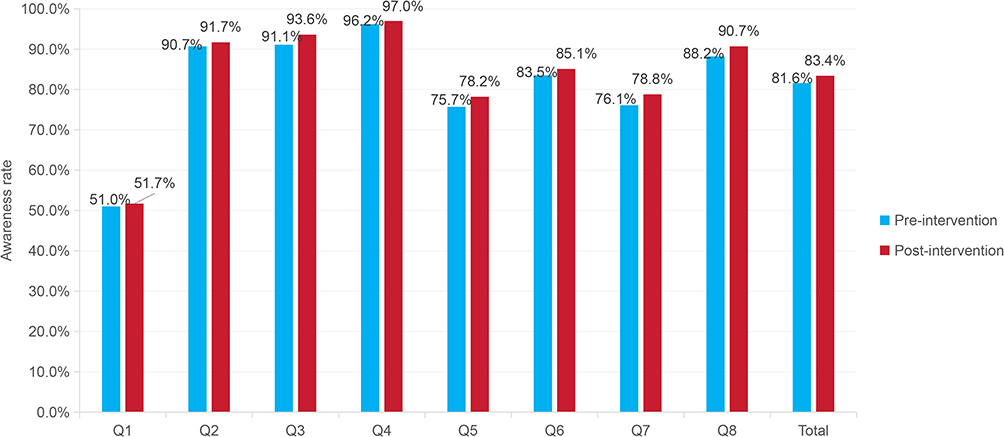 |
Figure 4 Awareness rates of each TB core information item pre- and post-intervention. |
Analysis of awareness rates for TB prevention and control core information across demographic subgroups revealed heterogeneous intervention effects (Table S3). Female participants demonstrated consistently higher awareness rates compared to males across multiple domains. Upper-grade participants exhibited improvements across multiple knowledge domains, such as Q2 (93.6% vs 89.9%), Q3 (95.6% vs 91.3%) and Q4 (97.3% vs 95.9%). After intervention, medical majors achieved post-intervention accuracy of 99.9% for Q4 and 89.3% of Q5, compared with 96.1% and 75.5% for humanities students, and 92.5% and 70.0% for arts students. Participants with prior TB health education maintained higher awareness rates both pre- and post-intervention compared to unexposed counterparts. Individuals with TB patient contact achieved higher post-intervention Q8 awareness (92.1% vs 90.4% in unexposed groups).
TB-Related Beliefs
Table 2 presents the distribution of TB-related beliefs among participants before and after the intervention. Following the intervention, the proportion of participants who perceived it as “highly necessary” for their college to conduct TB prevention and control publicity and education increased (57.8% vs 53.5%, P = 0.001). Regarding willingness to participate in university TB awareness activities, the proportion reporting they were “highly willing” rose from 45.4% to 49.9% (P = 0.001). Furthermore, the proportion of participants who perceived themselves as “at risk” of TB was 14.9% post-intervention, compared with 11.8% pre-intervention (P < 0.001). Concurrently, a greater proportion reported they would “try to keep distance” from TB patients (13.6% vs 10.4%, P < 0.001). In terms of knowledge dissemination, willingness to actively share acquired TB knowledge with others significantly improved (92.5% vs 90.9%, P = 0.007). However, no statistically significant changes were observed in certain behavioral intentions, such as willingness to undergo “proactive annual TB screening” (P = 0.125), or in “volunteering willingness” (P = 0.076).
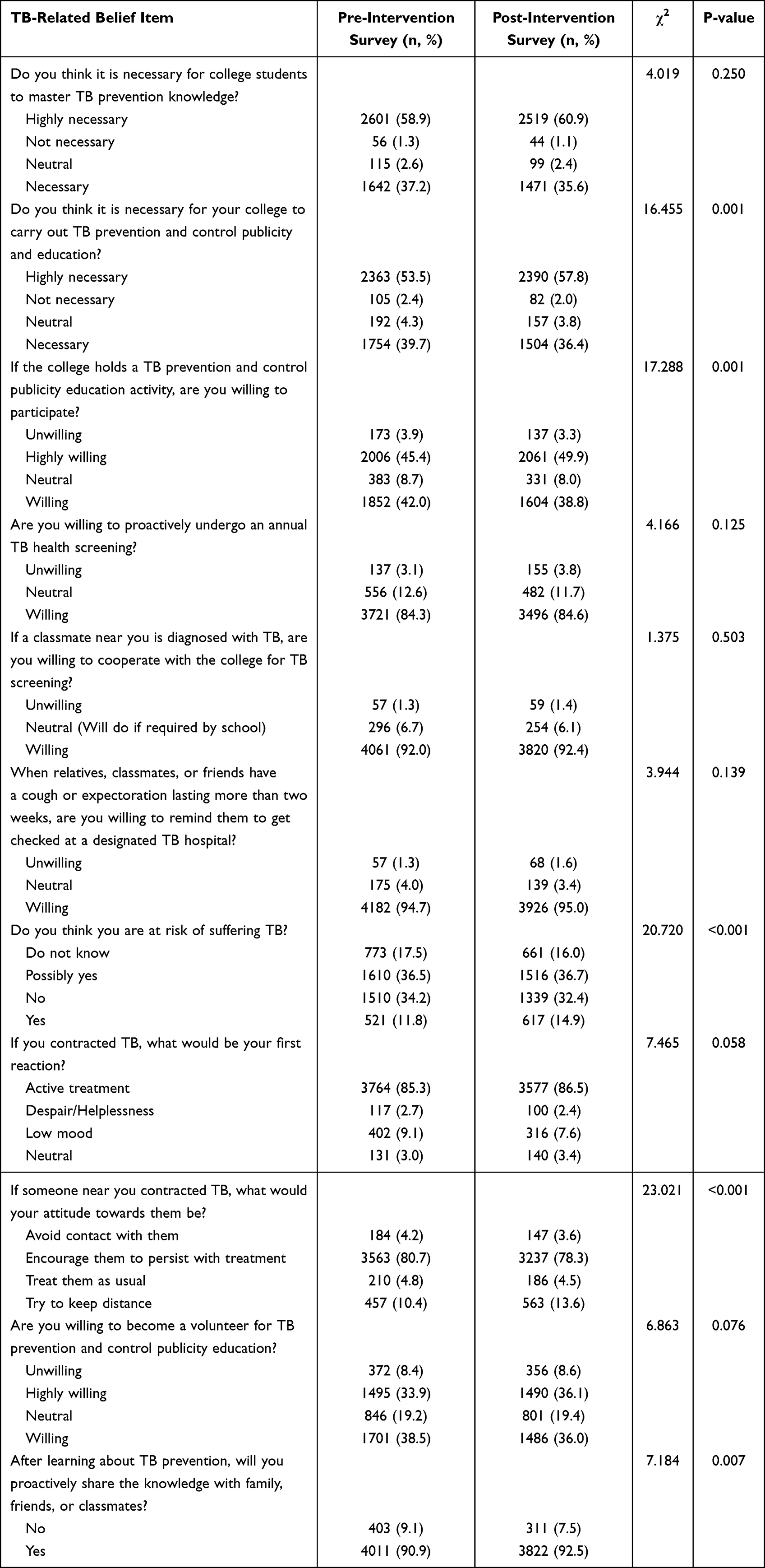 |
Table 2 TB-Related Beliefs Among Participants Before and After the Intervention |
TB-Related Behaviors
As presented in Table 3, changes in TB-related behaviors were observed. Post-intervention, the proportion perceiving no classmates spitting indiscriminately increased from 48.8% to 50.4% (P = 0.027). However, the proportion reporting observing such behavior also slightly increased (20.7% vs 19.7%). A higher proportion of participants reported always covering their mouth and nose with an elbow or tissue when coughing or sneezing (61.9% vs 59.7%, P = 0.013), while the proportion reporting doing so only occasionally decreased (8.1% vs 10.1%). Additionally, participants demonstrated improvements in smoking behavior and late-night habits post-intervention. The proportion of current smokers decreased (2.2% vs 3.3%, P =0.002). Concurrently, the prevalence of frequently staying up late (resting after 23:00) declined substantially (64.3% vs 70.2%, P < 0.001). Although the proportion reporting insufficient sleep (less than 7 hours) increased from 37.7% to 39.3%, this difference did not reach statistical significance (P = 0.141).
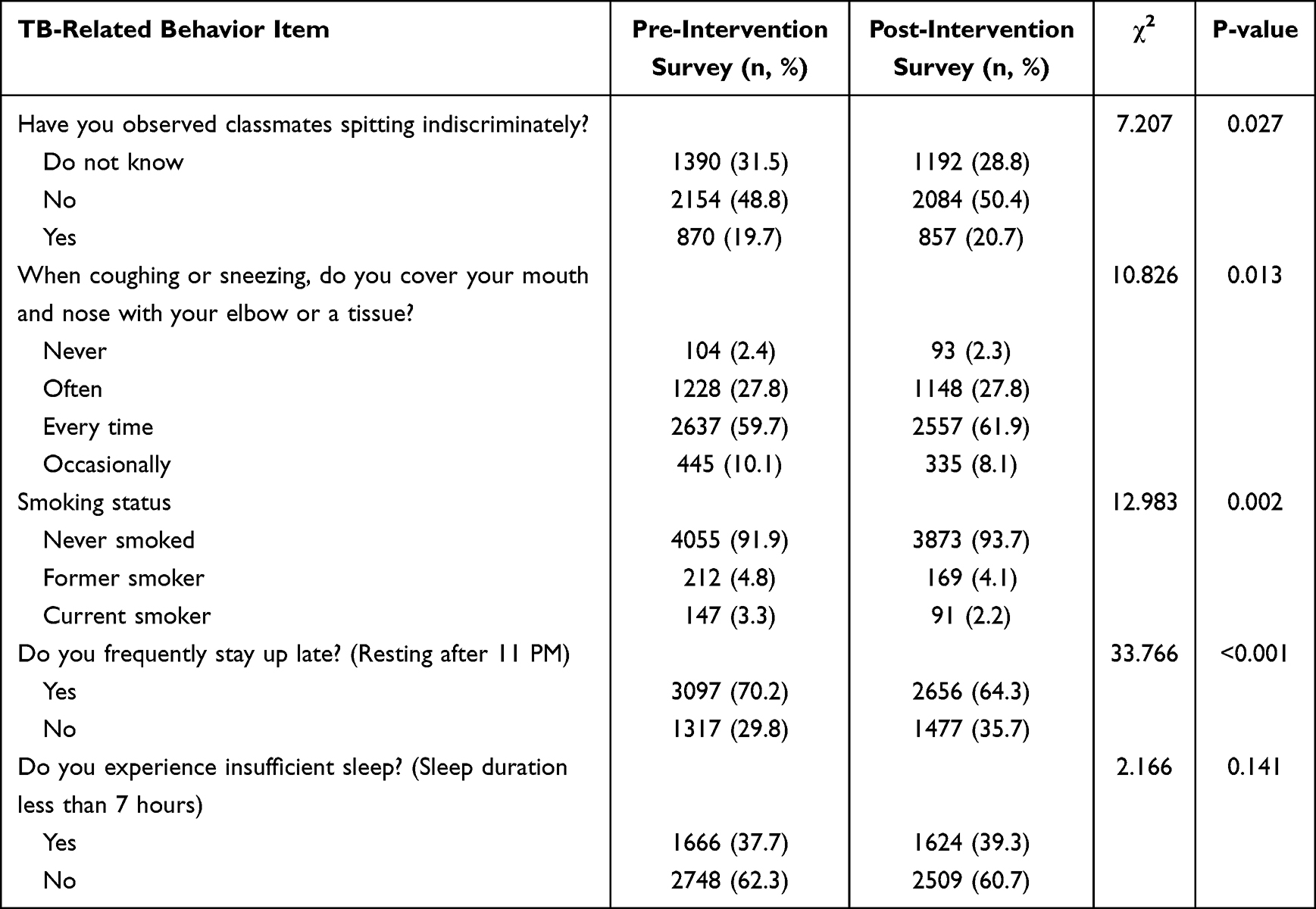 |
Table 3 TB-Related Behaviors Among Participants with Different Characteristics Before and After the Intervention |
Active Seeking Care and Diagnostic Delays Among TB Patients
In the pre-intervention survey, among 94 diagnosed student TB cases, 65 (69.1%) sought treatment at designated medical institutions on their own initiative following symptom onset, 25 (26.6%) were identified after being referred from non-designated medical institutions, and 4 (4.3%) via close-contact screening; a total of 49 student TB patients were diagnosed in 20 colleges in the post-intervention survey, and voluntary presentation increased to 76.6% (n=37), while transfer-in accounted for 23.4% (n=12).
As detailed in Table 4, the median patient delay was 3 days (IQR: 0–142) pre-intervention and 0 days (IQR: 0–181) post-intervention (P < 0.001). However, health system delays increased by 2 days (median: 8d vs 6d, P = 0.030). The median total delay was 13.5 days (IQR: 0–148) pre-intervention and 11 days (IQR: 0–198) post-intervention (P = 0.409).
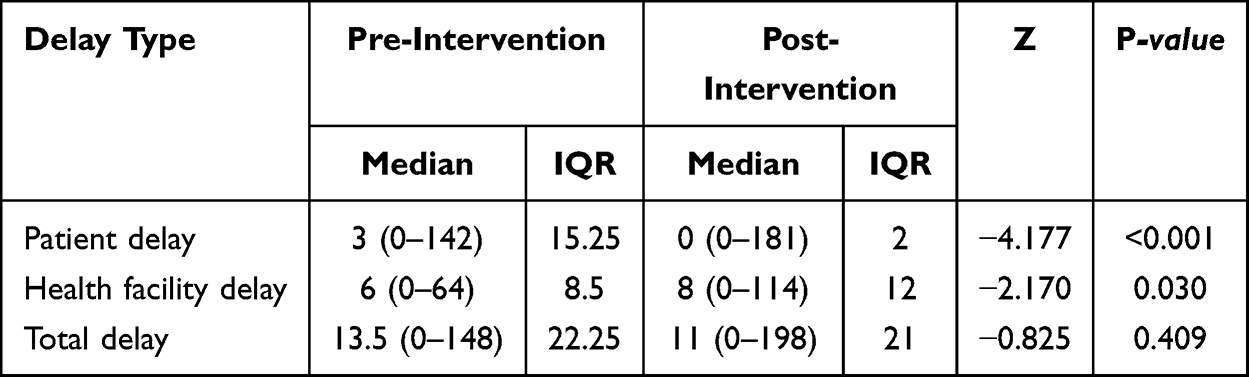 |
Table 4 Diagnostic Delays Among Student TB Patients Pre- and Post-Intervention |
Discussion
This study evaluated a standardized, multi-component TB health education package in real-world college settings using a pre-post design. The intervention was associated with significant improvements in overall TB knowledge, several key attitudes, and health-related behaviors among students, as well as a reduction in patient care-seeking delay. The success of this approach offers valuable insights for optimizing campus-based TB control strategies.
The intervention resulted in statistically significant but modest improvements in overall TB knowledge awareness (83.4% vs 81.6%), eliminated extreme misinformation and boosted full awareness rates by 3.8%. These findings were similar to those of intervention studies conducted in Philippine, Malaysia and Tanzania.16–18 Specifically, recognition of TB symptoms (Q3) and proactive reporting behaviors (Q6) increased by 2.5% and 1.6%, respectively, indicating enhanced student understanding of critical prevention practices. However, limited progress was observed for certain items, such as identifying TB as a chronic communicable disease (51.7% vs 51.0%), which fell below the 2022 national survey data for the general Chinese population (75.3%).19 This suggested ineffective knowledge transfer via conventional education methods for complex concepts. Persistent gaps in foundational pathological knowledge underscore the need to refine health communication strategies to address these cognitive blind spots.
The subgroup analysis reveals significant demographic variations in TB knowledge acquisition following the package. Medical majors demonstrated near-universal mastery of critical items post-intervention, notably in healthcare-seeking behavior (Q4: 99.9% vs 97.5%) and curability knowledge (Q5: 89.3% vs 81.2%). These aligned with findings from Saudi Arabia and Indonesia that disciplinary relevance enhanced health literacy internalization.4,20 This may be attributed to the inclusion of infectious disease education, including TB, within medical curricula, thereby better preparing students for TB prevention.21 Conversely, non-medical majors showed limited improvement in complex concepts, reinforcing the need for context-adapted educational strategies. Notably, participants with prior TB health education exhibited persistently superior awareness, echoing Hassan’s assertion that baseline health literacy mediates intervention efficacy.22 Prior education provides foundational schema for integrating new information. Students exposed to TB concepts could better contextualize content of the package, reducing cognitive load during knowledge acquisition.23 This explains their superior performance in complex items. Students with TB patient contact achieved higher post-intervention awareness, supporting Bressan et al’s observation that lived experience amplifies health messaging impact.24 Due to the differences in the needs of TB prevention and treatment, the role that playing, and the benefits and ability of acceptance between different groups of people, it is necessary to carry out targeted TB health education.10
Comparison of beliefs before and after the package showed significant improvements in perceived necessity of TB education (57.8% vs 53.5%) and willingness to share knowledge (92.5% vs 90.9%), reflecting enhanced engagement. However, improvements in specific behavioral compliance were limited; for instance, responses to the item “Are you willing to proactively undergo an annual TB health screening” showed only a 0.3% increase in the proportion of participants answering “willing” compared to pre-intervention rates. Similar discrepancies in beliefs and behaviors are common across virtually all fields and have been observed globally.25 Moreover, heightened risk perception (14.9% vs 11.8%) paradoxically coincided with stronger social distancing tendencies (13.6% vs 10.4%), underscoring enduring stigma-related challenges. This reflected deep-seated fear of TB’s infectious label, consistent with findings conducted in South Africa among healthcare workers.26 The absence of change in proactive screening willingness further signaled that knowledge alone might not drive behavior. Knowledge, Attitudes and Practice (KAP) theory asserts that the accumulation of knowledge leads to the formation of attitude, subsequently influencing practice, all three factors are inseparable.27 Therefore, to effect behavioral change, it is essential to initiate with enhancing health education, improving negative attitudes towards TB, and guiding positive behaviors.17
In addition, reductions in smoking (2.2% vs 3.3%) and late-night habits (64.3% vs 70.2%) demonstrate the package’s benefits on TB risk factors. These findings are particularly relevant given smoking’s well-established role in TB susceptibility, as evidenced by a Kelantan-based retrospective cross-sectional study demonstrating threefold higher TB infection risk among smoking youth compared to non-smokers.28 Critically, the intervention’s effectiveness was further substantiated by enhanced health-seeking behaviors, manifested through both increased symptom-driven care-seeking (76.6% vs 69.1%) and reduced patient delay (median reduction from 3 to 0 days). While the overall reduction in total delay (11 vs 13.5 days) did not reach statistical significance, it nevertheless represents a meaningful improvement compared to the 18-day delay reported in Quzhou’s children and adolescents population.29 However, the concurrent increase in health system delays (from 6 to 8 days) may reflect structural inefficiencies in diagnostic pathways, referral bottlenecks, or reduced diagnostic capacity in some facilities, suggesting that future interventions must address facility-level bottlenecks and strengthen process optimization within the health system to accelerate TB case management.
Various health education interventions for students have been implemented globally, each demonstrating unique advantages and limitations - a characteristic equally applicable to the current health education intervention package. First, the study was limited to 20 colleges across four prefecture-level cities, with public institutions comprising majority of the sample. The underrepresentation of private colleges and vocational institutions may restrict the generalizability of our findings. Second, the one-year intervention period precluded assessment of long-term outcomes, including knowledge retention rates and changes in disease incidence, while the lack of post-graduation follow-up limited our understanding of health behavior sustainability - issues warranting further investigation. Third, the absence of a control group limits causal inference, as we cannot completely rule out the influence of secular trends of national TB awareness campaigns or other concurrent public health events. Results should be interpreted as pre-post changes rather than definitive causal effects. Forth, the small number of student TB patients (94 pre-, 49 post-intervention) limits statistical power for delay analyses; these findings should be interpreted cautiously.
Regardless these limitations, our study presents several notable innovations. We pioneered the health education intervention package, systematically integrating five core activities with innovative components to create a sustainable TB prevention framework for college settings. Additionally, the student volunteer-led implementation enhanced traditional unidirectional health education into peer-to-peer knowledge dissemination, significantly enhancing engagement and outreach efficacy. Furthermore, we established a tripartite collaboration network involving CDC experts, college administrations, and student volunteer teams, optimizing resource allocation and providing a replicable organizational package for other regions.
Conclusions
The student-led health education intervention package effectively showed potential to enhance students’ role in TB prevention - shifting them from passive recipients to more active agents - and demonstrated feasibility for provincial-level implementation. Traditional metrics focused solely on knowledge awareness rates (the “knowing” gap) may underestimate the value of interventions that target self-efficacy and social norms (the “doing” gap). Therefore, campus TB control programs should prioritize peer-driven, multi-component behavioral interventions over didactic, knowledge-only campaigns to achieve tangible reductions in transmission risk and delays. Future research should include long-term follow-up to assess knowledge retention and behavioral sustainability, incorporate controlled designs to strengthen causal inference, and evaluate cost-effectiveness to inform scale-up across diverse educational settings. This study provides a replicable practice for student-centric health promotion in global tertiary education settings.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Acknowledgments
We would like to thank the staffs from all the local CDCs for the collection of the questionnaires.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the program of University Volunteers’ TB Prevention and Control Advocacy in Promoting Patient Finding, and “Pioneer” and “Leading Goose” R&D Program of Zhejiang (grant number 2025C01134) and Disease Prevention and Control Innovation Team of Zhejiang Province (2026JKC-05).
Disclosure
The authors have no competing interests to declare for this work.
References
1. World Health Organization. Global tuberculosis report 2023. 2023. Available from: https://www.who.int/publications/i/item/9789240083851.
2. Chen H, Zhang C, Zhang H, Cheng J, Li T. Analysis on the epidemic situation of pulmonary tuberculosis in schools in China from 2004 to 2021. Chin J Antituberculosis. 2022;44(8):768–14.
3. Ministry of Education of the People’s Republic of China. Statistical bulletin on the development of education in China in 2022. 2023. Available from: http://www.moe.gov.cn/jyb_sjzl/sjzl_fztjgb/202307/t20230705_1067278.html.
4. Puspitasari IM, Sinuraya RK, Aminudin AN, Kamilah RR. Knowledge, attitudes, and preventative behavior toward tuberculosis in university students in Indonesia. Infect Drug Resist. 2022;15:4721–4733. doi:10.2147/IDR.S365852
5. Cao D, Zhang Z, Yang Z, et al. The association between tuberculin skin test result and active tuberculosis risk of college students in Beijing, China: a retrospective cohort study. BMC Infect Dis. 2019;19(1):1. doi:10.1186/s12879-019-4238-2
6. Bao H, Liu K, Wu Z, et al. Tuberculosis outbreaks among students in mainland China: a systematic review and meta-analysis. BMC Infect Dis. 2019;19(1):972. doi:10.1186/s12879-019-4573-3
7. Lei R, Zhang T, Wu C, Li J, Sun R, Zhu X. Investigation of a tuberculosis epidemic at a college in Chongqing. China Trop Med. 2022;22(3):289–292. doi:10.13604/j.cnki.46-1064/r.2022.03.19
8. Ma N, Chen L, Ding F, Liu X, Li J, Zhao Y. Identification of the health education targeted susceptible population of tuberculosis in Ningxia, Northwest China. Sci Rep. 2024;14(1):13071. doi:10.1038/s41598-024-63961-5
9. Ma N, Zhang L, Chen L, Yu J, Chen Y, Zhao Y. Demographic and socioeconomic disparity in knowledge, attitude, and practice towards tuberculosis in Northwest, China: evidence from multilevel model study. BMC Health Serv Res. 2024;24(1):948. doi:10.1186/s12913-024-11336-x
10. Wu T, He H, Wei S, et al. How to optimize tuberculosis health education in college under the new situation? Based on a cross-sectional study among freshmen of a medical college in Guangxi, China. Front Public Health. 2022;10:845822. doi:10.3389/fpubh.2022.845822
11. Du G, Li C, Liu Y, et al. Study on the influencing factors of knowledge, attitudes and practice about tuberculosis among freshmen in Jiangsu, China: a cross-sectional study. Infect Drug Resist. 2022;15:1235–1245. doi:10.2147/IDR.S351541
12. Chen X, Peng Y, Zhou L, Wang F, Chen B, Qu Y. The necessity for enhancing awareness of tuberculosis starting from the early college semesters: empirical evidence from a cross-sectional research. Front Public Health. 2023;11:1272494. doi:10.3389/fpubh.2023.1272494
13. Chen X, Wang W, Wang X, et al. Public awareness of tuberculosis in Southeast China: a population-based study. Int J Environ Res Public Health. 2019;16(21):4290. doi:10.3390/ijerph16214290
14. Zhang R, Li Y, Yu H, et al. An analysis of public awareness of core information on tuberculosis in Guizhou Province. Ann Palliat Med. 2021;10(1):333–339. doi:10.21037/apm-20-2473
15. Datiko DG, Jerene D, Suarez P. Patient and health system delay among TB patients in Ethiopia: nationwide mixed method cross-sectional study. BMC Public Health. 2020;20(1):1126. doi:10.1186/s12889-020-08967-0
16. Panaligan R, Guiang J. Impact of health education on the knowledge and awareness of tuberculosis among high school students. Eur Respir J. 2014;40(Suppl 56).
17. Idris NA, Zakaria R, Muhamad R, Nik Husain NR, Ishak A, Wan Mohammad WMZ. The effectiveness of tuberculosis education programme in kelantan, malaysia on knowledge, attitude, practice and stigma towards tuberculosis among adolescents. Malays J Med Sci MJMS. 2020;27(6):102–114. doi:10.21315/mjms2020.27.6.10
18. Holst C, Stelzle D, Diep LM, et al. Improving health knowledge through provision of free digital health education to rural communities in iringa, tanzania: nonrandomized intervention study. J Med Internet Res. 2022;24(7):e37666. doi:10.2196/37666
19. Ni S, Wang J, Li X, et al. Assessment of health promotion action for tuberculosis of end tuberculosis action plan (2019–2022) in China. BMC Public Health. 2024;24(1):2051. doi:10.1186/s12889-024-19413-w
20. Kandasamy G, Almaghaslah D, Almanasef M. Knowledge, attitude and practice towards tuberculosis among healthcare and non-healthcare students at a public university in Saudi Arabia. Front Public Health. 2024;12:1348975. doi:10.3389/fpubh.2024.1348975
21. Zhou C, Li T, Du J, Yin D, Li X, Li S. Toward tuberculosis elimination by understanding epidemiologic characteristics and risk factors in Hainan Province, China - PubMed. Infect Dis Poverty. 2024;27(13):20. doi:10.1186/s40249-024-01188-2
22. Hassan AO, Olukolade R, Ogbuji QC, et al. Knowledge about tuberculosis: a precursor to effective TB control-findings from a follow-up national KAP study on tuberculosis among Nigerians - PubMed. Tuberc Res Treat. 2017;2017:6309092. doi:10.1155/2017/6309092
23. Wilby KJ, Paravattil B. Cognitive load theory: implications for assessment in pharmacy education. Res Soc Adm Pharm RSAP. 2021;17(9):1645–1649. doi:10.1016/j.sapharm.2020.12.009
24. Bressan V, Danielis M, Caruzzo D, et al. The lived experience of healthcare workers in quarantine: findings of a systematic review, meta-synthesis and meta-summary. Scand J Public Health. 2024;52(1):95–107. doi:10.1177/14034948221128158
25. Bano J, Gupta I, Singh G, et al. Combatting antibiotic resistance: identifying gaps in knowledge, attitude, and practice among medical interns. Cureus. 2024;16(7):e64402. doi:10.7759/cureus.64402
26. Sommerland N, Masquillier C, Rau A, et al. Reducing HIV- and TB-Stigma among healthcare co-workers in South Africa: results of a cluster randomised trial. Soc Sci Med. 2020;(266):113450. doi:10.1016/j.socscimed.2020.113450
27. Xie H, Wang W, Chen X, Huang D, Yu Q, Luo L. An analysis of knowledge, attitudes, practice and influencing factors for tuberculosis prevention and control among Hainan University students. Front Public Health. 2025;13:1478251. doi:10.3389/fpubh.2025.1478251
28. Awang H, Husain NRN, Abdullah H. Factors associated with tuberculosis among children and adolescents in kelantan: a cross-sectional study. Malays J Paediatr Child Health. 2018;24(1):1. doi:10.51407/mjpch.v24i1.30
29. Zhang Y, Zhan B, Hao X, et al. Factors associated with diagnostic delay of pulmonary tuberculosis among children and adolescents in Quzhou, China: results from the surveillance data 2011–2021. BMC Infect Dis. 2023;23(1):541. doi:10.1186/s12879-023-08516-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.