")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Structured follow-up of frail home-dwelling older people in primary health care: is there a special need, and could a checklist be of any benefit? A qualitative study of experiences from registered nurses and their leaders
Authors Næss G, Wyller TB, Kirkevold M
Received 15 April 2019
Accepted for publication 2 July 2019
Published 21 August 2019 Volume 2019:12 Pages 675—690
DOI https://doi.org/10.2147/JMDH.S212283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Gro Næss,1–3 Torgeir Bruun Wyller,1,4,5 Marit Kirkevold1,3
1Charm Research Centre for Habilitation and Rehabilitation Models & Services, Institute of Health and Society, University of Oslo, Oslo, Norway; 2Department of Nursing and Health Sciences, Faculty of Health and Sciences, University of South- Eastern Norway, Kongsberg, Norway; 3Department of Nursing Science, Institute of Health and Society, University of Oslo, Oslo, Norway; 4Institute of Clinical Medicine, University of Oslo, Oslo, Norway; 5Department of Geriatric Medicine, Oslo University Hospital, Oslo, Norway
Correspondence: Gro Næss
Department of Nursing and Health Sciences, Faculty of Health and Social Sciences, University of Southeastern-Norway, PO Box 4, Kongsberg, Norway
Tel +47 4 775 2986
Email [email protected]
Aim: To identify experiences and opinions about the need for a structured follow-up and to identify potential benefits and barriers to the use of a checklist (Sub Acute Functional decline in the Older people [SAFE]) when caring for frail home-dwelling older people.
Background: The complexity of older peoples’ health situation requires more coordinated health care across health care levels and a better structured follow-up than is currently being offered, especially in the transitional phase between hospital discharge and primary care, but also in more stable phases at home.
Design: This was a qualitative study using focus group interviews.
Methods: Data were collected during six focus group interviews in three districts in a municipality. Nineteen registered nurses (RNs) and seventeen leaders responsible for the follow-up of frail home-dwelling older people participated. Participants were representatives of the RNs in homecare and their leaders.
Results: Our results highlight that although most RNs and their leaders saw a number of significant benefits to conducting a structured assessment and follow-up of frail older people home care recipients, a number of barriers made this difficult to realize on a daily basis.
Conclusion: There is no common perception that a structured follow-up of frail home-dwelling older people in primary health care is an important and contributing factor to better quality of health care. Despite this, most RNs and leaders found that the use of a structured checklist such as SAFE was a benefit to achieving a structured follow-up of the frail older people. We identified several factors of importance to whether a structured follow-up with a checklist is conducted in home care.
Keywords: community health services, home care, frail elderly, multimorbidity, polypharmacy, functional decline, geriatric assessment, methods
Introduction
The oldest home-dwelling older people often live with frailty, multimorbidity, and polypharmacy. They are therefore at risk of experiencing functional decline and worsening of symptoms and are at increased risk of adverse drug reactions.1,2 The complexity of older persons’ health situation requires more coordinated health care across health care levels and a better structured follow-up than is currently being offered, especially in the transitional phase between hospital discharge and primary care, but also in more stable phases at home.3–7 General practitioners (GPs) are responsible for drug prescription and follow-up of prescribed medications. However, the frail older people visit their GPs less frequently than younger patients,7 with the consequence that such follow-up is left with the home care services. Several studies have shown that home care services frequently fail to discover health care needs and subtle changes in the health state of frail older people.8,9 Contributing factors might be the frequent changes in caregivers occurring within primary care10 and lack of adequate knowledge about geriatric nursing care.8,11,12 Structured follow-up and adequate documentation are necessary when caring for frail patients.13 Unfortunately, there is limited knowledge about which factors impact on structured assessment and follow-up of older people with multimorbidity and frailty by registered nurses (RNs) working in home care services.
A list system ensures all Norwegian inhabitants their own GP. The GPs have a contract with their municipality, and most practices are organized as independent enterprises with a combination of public funding and fees for services. The GP is responsible for the overall medical treatment. The RNs working in home health care have the responsibility for updating information, such as the drug regime, in the patient’s home care journal. They also have the responsibility for observing how the patient responds to medications, observing any changes in the patient’s health condition, and reporting to the GP when necessary.
RNs responsible for health care for this group of patients need to identify and document functional decline. Functional decline in the older people might be caused by interactions between aging and disease, interactions between diseases, or synergies between medical management of different diseases and aging. Such advanced geriatric health care might be difficult to achieve in primary care because the focus might be on covering primary needs such as personal hygiene, serving food, and delivery of medication rather than identifying early signs of further functional decline.14 Multimorbidity with comprehensive symptom burdens, advanced medical treatment, and necessary follow-up might easily be overlooked.
One study found that formal decisions regarding help provided by the municipality mostly focused on tasks related to basic needs and seldom on complex needs like structured observation and assessments of risks of further functional decline.15 Other studies have shown that this patient group in particular could benefit from the structured follow-up to prevent further decline.14,16–18
The qualitative study presented here is part of a larger mixed-methods study to evaluate a quality improvement (QI) project (Acute and Subacute dysfunction in the elderly, 2012–2013) in the municipality of Oslo, Norway. A previous study from the evaluation of the QI project15 revealed unmet patient needs related to their diagnoses, medications, and functional status. To address this problem, Oslo municipality initiated the QI project to improve the health care to frail home-dwelling older people. The project focused on persons aged 75 years or older, home-dwelling, receiving home care on a daily basis, having three or more chronic diagnoses recorded in the home nursing service’s patient record, and being hospitalized at least once during the last year. Specifically, the goal was to identify early signs of functional decline, acute illness, or worsening of chronic illness order to provide more timely treatment and follow-up of the patients. A multidisciplinary team with members from both primary care and specialist geriatric care at the local hospital developed a checklist to secure early identification of functional decline (Sub Acute Functional decline in the Older people [SAFE], see Figure S1). The goal of the checklist was to facilitate the systematic observation and assessment of patients at risk of functional decline, increase the home care RNs’ clinical assessment competence, and improve the quality of the home health care for this group of patients.
As part of the process evaluation of the QI project, this qualitative study was designed to evaluate the participating home care RNs’ and their leaders’ experiences with initiating and conducting structured observations and assessments of older patients using the SAFE checklist.
Aim
To identify experiences and opinions about the need for structured follow-up and to identify potential benefits and barriers to the use of SAFE when caring for frail home-dwelling older people.
Methods
Design
We designed a qualitative research approach aiming to obtain, explore, and interpret attitudes, motivations, and experiences of nurses and leaders in the home care service. Experiences of and factors of influence with regard to conducting necessary assessments were sought from focus group interviews performed between October 2013 and February 2014.
Setting
The study was carried out in three districts of Oslo, the largest city and capital of Norway. The participating districts are comparable to the other districts in the city with regard to the number of older people between 67 and 79 years of age, but they have a somewhat higher percentage of those aged 80+ years. The local municipal health authority in each district is responsible for providing home care to all inhabitants in need of such services. The care is based upon formal assessments and decisions by a local administrative unit designated for this purpose. These decisions also include the number of minutes per week of home nursing care each patient is allotted.
Participants
We recruited RNs and nursing leaders who had participated in the quality improvement project. An invitation to attend was sent to all RNs with defined patient responsibilities for frail elderly patients included in the quality improvement study.
The participants had practiced in health care from one to more than twenty years.
Nineteen RNs (one male) and seventeen nursing leaders (only females) from the three home care units (one from each district in the units) participated. The RNs were all so-called “patient-responsible RNs”, which meant that they had a number of patients they had a special responsibility for following up. This included contacting and cooperating with other professionals when needed. They were also in charge of the patients’ care plans and for documenting the home-services provided. Some of the leaders had an overall responsibility in the actual district, while others were group leaders with responsibility for a team of RNs in the home care unit and their patients.
Data collection
Six semi-structured focus group interviews were conducted with RNs and nursing leaders in three districts in the municipality.
Focus groups gave our participants the opportunity to explore conditions contributing to or hampering their follow-up of sick elderly people. We chose to have different focus groups for RNs and leaders because mixed groups might hamper the RNs willingness to speak freely. Furthermore, we assumed that the experiences of the leaders and the RNs were quite different due to their different responsibilities and placement in the organization, so bringing them together might not have given sufficient opportunity to explore these differences in detail.
Focus groups are particularly useful for exploring people’s common experiences, attitudes, and views in environments where people interact. Group interaction is an explicit part of the method and is aimed at sharing different experiences and viewpoints.19 Data were collected in six focus group interviews. One moderator (GN) and one co-moderator (MK) performed the focus group interviews. There were no relationship between the participants and the moderator or the co-moderator. The focus group interviews were conducted at the home care office in the included districts. An interview guide with open-ended questions focusing on the themes is shown in Table 1.
 |
Table 1 Focus group interview guide |
The interview guide was developed informed by a thorough review of the literature as well as the major goals and implementation processes of the development project. The questions were therefore developed to embrace the experiences of RNs “and their leaders” by initiating and conducting structured follow-up of home-dwelling older people using the SAFE checklist.
When necessary, follow-up questions were asked by the moderator. All interviews were recorded and then transcribed verbatim by a project RN with knowledge both of the actual setting and the patient group. Field notes regarding participant interactions and contextual information were collected as well. The focus group interviews lasted approximately one and a half hours.
Ethics
The study followed the ethical guidelines outlined in the revised Declaration of Helsinki.20 The Regional Committee for Medical and Health Research Ethics in Norway (REK) approved the study (number 2012/1891). Participants were provided with written and oral information about the study and were informed that they could withdraw at any time. Written informed consent was obtained from the participants before the interviews were conducted.
Data analysis
The interviews were checked, anonymized, and corrected against the audio files by the first author (GN). In accordance with Malterud’s method for systematic text condensation,21 GN and MK independently first read all the interviews to get an overview of the material and to identify preliminary themes associated with the aim of the study and then discussed these preliminary themes. GN then identified “meaning units” that were classified into themes and subthemes. These were subsequently refined through discussions among all the authors in an iterative process. GN wrote a summary of the subtheme contents and identified illustrative quotations and possible connections between the factors that were identified.
The themes and the analysis were discussed among the authors several times. Throughout the whole process, the authors went back to the original transcripts to ensure congruence between themes, subthemes, and the raw data.
For our theoretical interpretation, the themes were reflected on according to the study’s aims and the relevant literature. Specific theoretical perspectives were not decided on in advance but emerged throughout the analysis and interpretation phases. The theoretical reflections extended our understanding of factors of influence and the possible connections between them. Excerpts from the focus groups illustrate our findings.
Results
All three districts had implemented a new routine using a checklist (SAFE) every fortnight or whenever the patient’s condition changed. In general, we found small differences between the RNs’ and their leaders’ opinions, and they were thus analyzed together. Most RNs and leaders in all three districts thought the checklist was useful for systematic follow-up. However, we identified two relatively distinct views. One group considered systematic observation of home-dwelling seniors with multimorbidity to be a unique need and an important and complex nursing task, whereas the other group was of the opinion that older people with multimorbidity had no different needs for follow-up than younger patients. In the following, we first delineate the experiences and opinions of those who favored using the checklist and thereafter the reasons given for not favoring the use of the checklist. Finally, we highlight factors that seemed to threaten the systematic follow-up of home-dwelling older people with multimorbidity.
Reported benefits of using a checklist in structured follow-up of the frail older people
Observations are more structured with the checklist
Several RNs found themselves working in a more structured manner when using the checklist. Similarly, several leaders found that the checklist made the RNs work in a more structured manner through all relevant functional areas like nutrition, circulation, pain, and so on. They experienced that the RNs had to “think through and do their work properly” and not be in a rush as they often were without the checklist. They claimed that by using the checklist regularly, the RNs also carried out more frequent assessments. They reported that the RNs had conducted registrations more systematically, and not just due to changes in medications and so on. As one leader stated:
I think the RNs are good at doing assessments of the patients; I am quite sure about that. However, by using the checklist they are forced, in a way, to document their observations.
Several RNs supported this view. As one of them explained:
Yes, I think perhaps that we do measure more blood pressures and so on, [and] we do them more often than we did before. Before we only took blood pressure because of a diagnosis, medication, or other condition that made it necessary.
Several RNs in addition claimed that using checklists helped them to get a good overview of the patient’s condition and to discover more subtle changes. One said:
If there were obvious changes, we would have seen it [before]. Now [using the checklist] we map more than we otherwise might have done … plus it is documented. You get a very good overview like that.
Two other RNs said:
Earlier we wrote down notes in “message books” [to our colleagues] … and wrote a short note in the EPR. Now we have to give a complete overview. [RN 1]
By using a checklist we have a great baseline to compare with when there is a change in the patient’s condition. [RN 2]
Accordingly, RNs as well as leaders told that their patients felt safer by being followed-up systematically with the checklist. One leader said:
Our patients say: You know, they follow me up so very well, the RNs ask me about almost everything repeatedly, and I feel so well taken care of!
The checklist moves the observation from “the head of the RN”
An experience often recounted was that the checklist moved the observation from “the head of the RN” to a structured assessment documented in the patient’s record. As several of the RNs said:
This makes information viewable to other staff members and makes changes in conditions more visible both to the RN herself and to other staff members. [RN 1]
The observations are becoming more systematic and they are documented better. I have always made these observations, but now they are better documented. [RN 2]
Acute illness and functional decline are more readily identified
Using the checklist, one of the RNs told how she had become aware of an acute illness and had the patient sent to the emergency room:
The patient had diffuse ailments for a few weeks, but she is a person who does not complain. I did a [SAFE] screening, and then I discovered that she had more problems than she had expressed. I am with her daily, but I did not see the change before I did a systematic screening. As a consequence, she was sent to the emergency room.
In this case, use of the checklist resulted in a hospital admission for the patient because of the changes in condition that were identified. Other RNs told how the checklist prompted them to carry out assessments that they needed to convey to the GP. These were assessments they otherwise would not have done, and the GP would not have been informed of the changes.
The leaders agreed that without checklists and systematic assessment signs of functional decline could be overlooked. As one of them said:
The RNs have become more aware that some hospitalizations are avoidable if we observe signs in an early phase, for example, when a patient is not drinking or eating as usual, and then the patient becomes acutely ill due to dehydration. Dehydration takes some time to develop, you know.
The checklist contributes to a common language and promotes professional cooperation
Several RNs and leaders said that a benefit of using the checklist was better cooperation by using common language in their contacts with the GPs. One of the RNs explained:
Systematic assessment with the checklist makes us use more professional expressions in documentation that we might have lost in home nursing. Because we work with unskilled and staff with different backgrounds, we simplify our language and skip the professional expressions. The requests to the doctors have become more professional. [after the introduction of the checklist]
A leader said:
I hear that the doctors think that the PLO messages [electronic messages between GP and RNs] now have a much greater professional weight than before. That they [GPs] find it easier to relate to home care. Earlier, the PLO messages might be expressed like “the patient is in bad shape”, but now they are more precise and specific and use more professional expressions.
Reasons for not seeing any benefits to using the checklist
Completing the checklist adds nothing to current practice and is a waste of time
Whereas most RNs and leaders embraced the checklist, some of the RNs said that they used the checklists only because they were forced to, not because they believed it was a tool with any purpose. As one of the RNs said:
We have experienced that the structured-follow up has been implemented because the leaders have decided that we need to do so and not [because it is] in the best interest of the patient … . This is especially the case when there is no change in the patient’s situation, and you just sign off that you have completed the procedure.
Another RN explained:
I perceive the documentation of the structured follow-up to be unsuitable; it covers something that is already covered in our health care. We write daily reports on the patients, but the documentation of the structured follow-up comes in addition.
In accordance with these statements, some of the RNs claimed that structured observations in healthy older people were a “waste of time”:
But just to go to [patients] and check their respiration and circulation when they’re well, I feel is like throwing away time.
I know my patients and will discover changes – all this documentation is unnecessary.
Several leaders supported this view:
We have experienced that it is for the sake of the project and not for the patient, especially if there is no change and you just sign off that you have done it. [Leader 1]
You know when your user/patient is doing poorly or when he needs a doctor. [leader 2]
You do not have time to sit in peace and quiet and look at this; it is ‘the Wild West’ out there! [Leader 3]
A frequently repeated statement among this group of RNs was that “I have it in my head”
When asked about this, they said that all the information that they needed was in their head, and they had no need of reading the electronic patient journal (EPR) or documenting their observations. As one RN explained:
Before the checklist, we had the list in our head, you know. We observed the patient from head to toe, but in our head. Now, we have it on paper. Things like pulse and so on, we did not register before. We talked to the patient and so on, and at the same time we observed him.
Among the RNs, there seemed to be a perception that “knowing the patient” was sufficient and of more value than performing structured follow-up in a more proactive way. Several RNs expressed statements indicating the following:
I know my patients well, so I will know if something is wrong with them. [RN 1]
There is no need for systematic observation, you will be aware if there are any changes. [RN 2]
Factors that threaten structured follow-up of frail older home care recipients
The focus group discussions highlighted several factors that could threaten the conduct of structured follow-up of frail older people home care recipients.
Lack of adequate geriatric competence hinders interpretation and understanding of the patient’s condition
Some leaders as well as RNs claimed that the follow-up of frail older people at home was a rather complex task and of great importance for ensuring quality of care to the frail older people. Several leaders emphasized the need for special knowledge in order to be able to perform structured follow-up:
It would be easier for those who shall perform the structured follow-up if they had been given maybe a few hours instruction on why these points are particularly suitable for uncovering functional decline in the frail older people. [Leader 1]
I am quite sure actually, because with knowledge you become more conscious, and you get familiar with why things are so important to follow up. [Leader 2]
In line with this, RNs said:
Geriatric knowledge could provide a better understanding of why this is important, what can develop rapidly, and what my role as a nurse is in this. [RN 1]
I think it is a good idea with geriatric knowledge to better understand what you observe with SAFE. [RN 2]
These statements indicate, to some degree, acknowledgment of the need for geriatric knowledge. In contrast, other RNs and leaders considered the structured follow-up to require no more than basic nursing knowledge:
We are talking about just basic nursing knowledge … from nursing school. [Leader]
Organizational issues impeding systematic observation and follow-up
Lack of a common strategy for follow-up of home-dwelling older people among GPs and the home care service
Despite the goal of improved collaboration between the GPs and the home care services in the QI project, none of the participants told of shared plans for follow-up between RNs and GPs where the responsibility for the patient’s needs was clarified for the participating professionals. Instead, both RNs and leaders indicated uncertainty about the roles and responsibility of the RNs and the GPs. One RN said:
What is the purpose of doing this assessment and documenting when I speak to deaf ears? That I report that the changes are so and so, and nothing happens! It is like filling out papers and then putting them in a drawer … . Then you see that the pile grows and nothing happens. So, then you lose some motivation … Why should I do this when it goes into the drawer and is no longer used?
The QI project aimed to identify early signs of patient deterioration and to ensure expedient cooperation between the home RNs and GPs in order to initiate a timely and adequate response. However, both RNs and their leaders experienced that the RNs’ inquiries to the GPs were often not responded to before the patient’s situation became serious. One RN stated:
Here by us we do nothing until the situation becomes acute! I report changes in the patient’s situation to the doctor … but then nothing happens.
Another RN related the following story:
We had registered changes in one patient and reported it to the GP, but the doctor did nothing. Then we asked the doctor again, but he did nothing. Eventually the patient ended up falling as we recorded lower and lower blood pressure, and she had received new medicines for her angina. It was pain medications, which actually affected her blood pressure. She fell, did not recover, and died after some time.
Some RNs and leaders pointed out that a possible explanation for the lack of responsiveness from GPs might be lack of time:
The doctors are often too busy. They do not have the time to respond to us. It takes too long.
Several RNs pointed out a lack of patient information as a difficulty in follow-up.
We usually do not get all the diagnoses from the doctor, just some.
Nevertheless, the main issue seemed to be a lack of a common understanding about how the collaboration should be carried out.
Challenges in documenting systematic observations and follow-up in the EPR
Both RNs and leaders experienced that the performed observations were not always documented. The reasons given were lack of time allocated for necessary documentation and that the hand-held personal computers that the RNs brought with them to the patients were not adapted to the kind of systematic documentation that might provide an overview of the patients’ health situation. Instead, the RNs had to complete the documentation from the checklist after returning to the office later in the day:
You don’t always have the time to write it in the EPR, and then the observations from the checklist stay unwritten …
Nursing leaders explained the missing documentation of observations, and economic reasons were frequently mentioned. Several leaders said that they were evaluated on how they managed their budgets, and not on the quality of content in patient documentation to secure structured follow-up. As one of them said:
More and more requirements for documentation – worse and worse working conditions.
Another leader said:
It is decided that we do not get a formal decision on doing SAFE, so this is in a way something we do at our own cost; it is a task that we really do not have money to perform.
Most RNs and their leaders also highlighted factors that made systematic assessment and follow-up difficult. The health care services in the municipality were organized into a two-part system. A local health care allocation office assessed the patients and decided on the services to be provided, and an “executive unit” with home care RNs and assistants provided the actual care. According to both leaders and RNs, lack of adequate cooperation between the two parts of the system influenced structured follow-up. Several nurse leaders explained:
The formally assigned healthcare services to be provided to each patient, conducted by the local health care allocation office, determine the amount of staff on duty on a daily basis … … .The “executive unit” then must be able to defend its use of time in accordance with the decisions made by the local health care allocation office. [Leader 1]
The local health care allocation office and the executive unit do not act according to shared goals – they have different perceptions of patient needs. [Leader 2]
In addition, the RNs experienced this organizational condition as a hampering factor:
We are being evaluated on the time we spend with the patients in their home, not on other tasks that we perform, i.e. in the office, that are necessary for the structured follow-up.
To summarize, our results highlight that although most RNs and their leaders saw a number of significant benefits to conducting structured assessment and follow-up of frail older people home care recipients, a number of barriers made this difficult to realize on a daily basis.
Discussion
To improve structured follow-up in health care, a checklist (SAFE) was developed. Checklists aim to standardize a process and thus to improve patient outcomes.22 Checklists for preventing risk of falls,23 pressure ulcers,24 pain assessment,25 and surgical safety are well known and widely used in nursing. It is important though to understand that checklists are reminders of what to do. They have to be followed by work regarding attitudes, and most often great effort needs to be made to remove barriers to actually using them. Otherwise, they will have only limited impact.22
To our knowledge, there is little research on the use of checklists in home care (HC) when patients are in a stable phase. Checklists are often used in acute or critical care to detect inconspicuous changes and to prevent adverse events and to achieve patient security.22 Concerning acute situations in health care, checklists that help to observe, ensure, and document vital functions have been developed and tested, including ABCDE26 and NEWS2.27 Preventing adverse events in transitional situations and interventions to achieve patient safety in the frail older people have been the aims in several studies.28,29 Adverse events in home health care are less well described, although home-dwelling older people might be particularly vulnerable to iatrogenic injury due to their multimorbidity, polypharmacy, and frailty. Comprehensive geriatric assessment (CGA) is a well-known concept in geriatric health care and is mostly used by specialists in hospitals.30 This is an interdisciplinary assessment process that embraces many factors, and it has been found to be successful in gathering the most important information in care planning. CGA and SAFE are not competing assessments but should be considered complementary because SAFE is developed as a short assessment tool to identify small things that often occur in the older people as early signs of further functional decline. Use of SAFE might also lead to increased awareness of the need to conduct a CGA. In other situations, there is a need for structured geriatric assessment to clarify whether or not the active treatment is to be terminated and replaced with palliative care in the last phase of life.
We found that both leaders and RNs experienced that the SAFE checklist helped to make the observation and assessment of the frail old patient more systematic. Observations that can help identify early signs of poor function were systematically conducted by using SAFE, and interventions to prevent further functional decline could then be implemented. The observations were thus no longer based upon the RNs’ personal perception of their relative importance. Rather, structured observations of the frail older people were made a part of the regular routine. This provided a foundation for making the information accessible both for the caregiver and other health care workers by documenting it in the EPR.
The checklist also helped the RNs to achieve a good overview of the patient’s situation because small changes could be identified. These are changes that previously might have been overlooked. Previous research has shown that identifying these small changes is particularly important in the follow-up of the frail older people because they might be the first sign of the development of an acute illness.31,32 In the SAFE checklist, such small changes are described in precise values (ie, “blood pressure as dropped more than 40 mmHg or more”, “BP <110/70 mmHg”, “clearly more unstable than usual”, “fell once within the last week and does not usually fall”, “new wound” or “worsening of existing wounds”, and so on). Such changes might in other patient groups be of no consequence. In SAFE, small changes are categorized as being in need of follow-up immediately or in some days depending on their severity. Both RNs and leaders reported that health care providers previously could have failed to discover such small changes and only discovered changes that are more eye-catching when the situation had become acute.
Both RNs and managers experienced that patients felt safe when health care professionals regularly used the SAFE checklist. Frail older people living at home with multimorbidity experience great symptom burden related to the aging process, disease process, and medical treatment.18 Their life situation can be unstable, and relatively small incidents or minor illnesses can turn into acute functional decline. In addition, pain, anxiety, and sleep problems are common symptom burdens in many patients. Knowing that your health condition is regularly surveyed might help create a sense of security, as pointed out by participants in this study.
Another finding was that the checklist contributed to a more common and professional language among the health care professionals. This was evident both in the patient’s EPR and in the electronic communication between RNs and GPs. Precise indications and a professional language in general might contribute to increased patient safety by ensuring a common view of patient situations. Changing disease patterns and growing complexity of primary care delivery now require teamwork, including open communication and cooperation across providers in order to reduce preventable errors and improve safety outcomes.33 A common and professional language also contributes to increased respect and confidence in interdisciplinary collaboration.34
Contrary to those who saw benefits to using the checklist in stable phases, several participants experienced documenting that there was no change as a “waste of time”. This might be explained by the fact that checklists are most often used in acute situations where changes are clear and the need for follow-up and documentation is obvious. Another explanation could be that the use of SAFE simply entails that other important patient tasks cannot be performed on a tight schedule. This objection to SAFE might also be due to the design and scope of SAFE. Though easier than a full CGA, SAFE is rather comprehensive and thus demands some time to conduct. A validation of SAFE is necessary to secure its appropriateness in clinical praxis. Another view was that systematic observation was already covered in their documentation routines.
Others asked why they should make such systematic observations of a patient they knew well. The experience of “knowing the patient” led them to not see the need for systematic observation using a checklist. Their experience was that they had all the information they needed “in their heads” and that they would notice any changes that occurred without any helping tools. This statement could be understood as lack of knowledge of the RN`s comprehensive responsibility in geriatric health care. On the other hand, this could be a consequence of insufficient teaching and training related to the checklist. Training in the QI project was mainly related to the practical use of the SAFE checklist and not to explanations of why SAFE was necessary. A recent study found that adequate training, clear management, and extensive facilitation for use in daily work over time was necessary to create sufficient understanding, engagement, and commitment to implement a new routine in health care.35
Barriers that prevent the use of SAFE
Checklists can be useful tools to improve health care, but there is little understanding of the barriers to using checklists.22,36 We found several barriers that must be addressed in order to succeed in implementing a checklist such as SAFE.
No common preventive strategy
The SAFE checklist was introduced as part of a new procedure to strengthen the cooperation between home care and GPs in order to ensure the quality of the follow-up of home-dwelling older people. However, several of the informants experienced that GPs did not respond when they reported changes and that nothing was done before the patient situation became acute, despite repeated inquiries to the patient’s GP. This might be because of lack of a common strategy between the home care service and GPs regarding follow-up of home-dwelling older people. RNs told of patients worsening due to lack of response to their worries, but the RNs also did nothing other than continuing their requests to the GP. There seem to be a lack of routines to secure patient safety in such situations. The RNs’ motivation to use the checklist decreased when they did not get a response from the GP before the situation turned acute. Lack of response might be a sign of GPs experiencing too many inquiries from home care reporting small changes. This study has no data to explore this. Hansson and colleagues have described GPs as reluctant to such collaboration because they consider it time-consuming and because their role in the team is unclear. The same study indicates that nurses and nurse managers support multidisciplinary teams in health care, whereas GPs seem to be less interested in this.37 Clear responsibilities, shared facilities, written procedures, shared communication tools, accessibility, trust, and leadership are necessary to facilitate professional collaboration in primary health care.2,38 In this study, clear responsibilities, accessibility, and trust seemed to be missing in some cases.
Vital information from the assessments using the checklist remains invisible to others
In this study, RNs and their leaders supported findings from other researchers6 by stating that documentation of observations from SAFE was a task that was very often postponed or not done at all.39,40 They explained this by referring to lack of time and access to the EPR at the time of the assessment. On the other hand, both RNs and leaders told that through structured follow-up by a checklist, the documentation of health care in patient’s EPRs had improved. This experience indicates that a significant barrier to the effective use of a checklist in stable patient situations is the timely documentation of the observations in the EPR.
Although performed in hospital settings, other studies have shown that nursing records usually do not include all caring activities that nurses perform.39 Patient documentation in terms of care plans is intended to facilitate continuity and individual nursing care through documentation of the conducted assessment of the patient’s health condition and care needs. However, researchers have found that nursing documentation does not always serve these objectives. Paans and colleagues state that effective documentation systems that support nurses in linking diagnoses, medications, interventions, and progress and outcome evaluations are important.41 This is especially the case in health care to the frail older persons living with multimorbidity and polypharmacy. In spite of this, several researchers have reported that the patient records contain relatively few precisely formulated diagnoses, vital signs, symptoms, and related factors,40 and that the details of interventions and outcomes are poorly documented.15,40,42 Devik and colleagues found that older people in home care had significantly more drug-related problems compared to older people in nursing homes and that unclear documentation of medication was most frequent in patients receiving home care services.43 Cheevakasemsook and colleagues found that factors hindering adequate and timely nursing documentation include disruption during charting and incomplete charting.44 They found that limited competence, motivation, and confidence; ineffective nursing procedures; and inadequate nursing audit, supervision, and staff development contributed to the situation. These findings are in line with ours. We found indications of a lack of geriatric competence, which made it difficult for the nurses and leaders to understand why the SAFE checklist could be useful despite their knowledge of the patient. Performing observations when the patient seems “as always”, and then documenting no change, can easily be seen as a waste of time. Geriatric knowledge, however, highlights the importance of knowing the onset of older peoples changes in function. Changes might occur due to worsening of disease, new disease, or the use of medications. For health care providers, it is of great importance to be able to read in the EPR if the change is a new situation, or when the change started, in order to be able to decide if there is a sub-acute or acute functional decline. Unfortunately, descriptions of such changes are often missing in the EPR, as this study indicates.45 This lack of documentation of the patient’s common condition and possible deterioration could be a threat to patient safety.
Limited access to the patient’s complete medical history and relevant monitoring data can be perceived as a barrier for sufficient follow-up of medical treatment and functional status in primary care.2 Limited access to patient information thus can contribute to the experience of structured follow-up as being important or not. In home care to frail older people, knowledge of functions, diagnoses, and medications must be present to be able to prevent further functional decline or to identify acute situations. Several RNs and leaders told of a lack of such crucial information. Other studies have supported this.2 The RNs’ crucial role in providing clinical information about the patient’s functional or medical condition to other health care providers then can thus be difficult to execute.
The SAFE checklist was specifically designed to capture small changes in physical and cognitive function to detect acute malfunction or acute illness in elderly people, as small changes in function may be the only sign of the development of serious disease. Therefore, the checklist does not include psychological, social, and environmental aspects of the patient’s health and does not cover all assessments that need to be done in frail older patients. The checklist should not replace, but supplement, the RNs assessment of the patients.
Our findings are indeed reflecting the Norwegian health care system. Health care and social services in Norway are based on what is called “the classic Scandinavian Welfare model”, and the services are accessible to everyone. Central state authorities organize specialist health care whereas the municipalities are responsible for primary medical services (GPs) and home-based services. Home-based services are publicly financed and mainly publicly provided. The GPs in Norway (as in Denmark and England) most often are self-employed on contract with the municipality, while this is not the situation in other countries, ie, Sweden, where public health centers organize the delivery of primary health care.46
Mur-Veeman and colleagues found that coordination problems exist in many European countries representing different types of health care systems.47 Several studies have investigated both structural and cultural dimensions of coordination weaknesses.46,47 Decentralization of health services where local authorities are given freedom to develop local solutions with regard to working procedures, collaboration, communication processes, etc., is common, but may be challenging. Different legislative frameworks and different administrative units with separate budgets (as is the situation to RNs in home care and GPs) may hamper collaboration. This may explain some of the difficulties the RNs and leaders in our study experienced. In addition, cultural factors such as different working cultures and protection of own professional domains have been identified as contributing factors to lack of collaboration.46 Limited understanding for other actors’ needs (eg, with regard to information as in our findings) has been linked to lack of coordination.46 These are challenges that may arise regardless of the organization of the service. Accordingly, our findings may be of interest also in countries with differently organized home care services.
A limitation of our study is that we only approached the formal care providers, although informal careers are of large relevance for the welfare of frail patients. The reason for this is that we wanted to explore aspects that could be of relevance for improvement of the formal services.
Conclusion
From the perspective of nurses and their leaders, there is no common perception that structured follow-up of frail home-dwelling older people in primary health care is an important and contributing factor to better quality of health care. Despite this, most RNs and leaders found that the use of a structured checklist such as SAFE was a benefit to achieving structured follow-up of the frail older people. We identified several factors of importance to whether structured follow-up with a checklist is conducted in home nursing. The RNs and their leaders experienced this to be due to factors at both the individual and system levels. Knowledge of advanced geriatric health care to the frail older people and RNs’ role in the health care, having a common preventive strategy with the collaborating GP, and having time to perform assessments and patient documentation were experienced as contributing to improving RNs’ practice of early identification of functional decline or acute illness in the older people.
Abbreviations
RN, registered nurse; GP, general practitioners; SAFE, Sub Acute Functional decline in elderly; EPR, electronic patient record, HC, home care.
Acknowledgments
We would like to thank all informants for participating in the study. Furthermore, we thank Edith L. Roth Gjevjon for important input from her work with SAFE and the permission to translate and enclose SAFE.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Formiga F, Ferrer A, Sanz H, Marengoni A, Alburquerque J, Pujol R. Patterns of comorbidity and multimorbidity in the oldest old: the Octabaix study. Eur J Intern Med. 2013;24(1):40–44. doi:10.1016/j.ejim.2012.11.003
2. Bell HT, Granas AG, Enmarker I, Omli R, Steinsbekk A. Nurses’ and pharmacists’ learning experiences from participating in interprofessional medication reviews for elderly in primary health care - a qualitative study. BMC Fam Pract. 2017;18(1):30. doi:10.1186/s12875-017-0607-3
3. Beswick A, Rees K, Dieppe P, et al. Complex interventions to improve physical function and maintain independent living in elderly people: a systematic review and meta-analysis. Lancet. 2008;371(9614):725–735. doi:10.1016/S0140-6736(08)60342-6
4. Boyd CM, Boult C, Shadmi E, et al. Guided care for multimorbid older adults: kathleen Walsh Piercy, PhD, editor. Gerontologist. 2007;47(5):697–704. doi:10.1093/geront/47.5.697
5. Fortin M, Soubhi H, Hudon C, Bayliss EA, van Den Akker M. Multimorbidity’s many challenges. Bmj. 2007;334(7602):1016–1017. doi:10.1136/bmj.39201.463819.2C
6. Rosstad T, Garasen H, Steinsbekk A, Haland E, Kristoffersen L, Grimsmo A. Implementing a care pathway for elderly patients, a comparative qualitative process evaluation in primary care. BMC Health Serv Res. 2015;15:86. doi:10.1186/s12913-015-0718-2
7. Rytter L, Jakobsen HN, Ronholt F, et al. Comprehensive discharge follow-up in patients’ homes by GPs and district nurses of elderly patients. A randomized controlled trial. Scand J Prim Health Care. 2010;28(3):146–153. doi:10.3109/02813431003764466
8. Metzelthin SF, Daniels R, van Rossum E, et al. A nurse-led interdisciplinary primary care approach to prevent disability among community-dwelling frail older people: a large-scale process evaluation. Int J Nurs Stud. 2013;50(9):1184–1196. doi:10.1016/j.ijnurstu.2012.12.016
9. Bleijenberg N, Ten DVH, Steunenberg B, et al. Exploring the expectations, needs and experiences of general practitioners and nurses towards a proactive and structured care programme for frail older patients: a mixed-methods study. J Adv Nurs. 2013;69(10):2262–2273. doi:10.1111/jan.12110
10. Gjevjon ER, Romøren TI, BØ K, Hellesø R. Continuity of care in home health‐care practice: two management paradoxes. J Nurs Manag. 2013;21(1):182–190. doi:10.1111/j.1365-2834.2012.01366.x
11. Bayliss EA, Edwards AE, Steiner JF, Main DS. Processes of care desired by elderly patients with multimorbidities. Fam Pract. 2008;25(4):287–293. doi:10.1093/fampra/cmn040
12. Beswick AD, Gooberman-Hill R, Smith A, Wylde V, Ebrahim S. Maintaining independence in older people. Rev Clin Gerontol. 2010;20(2):128–153. doi:10.1017/S0959259810000079
13. Charalambous L, Goldberg S. ‘Gaps, mishaps and overlaps’. Nursing documentation: how does it affect care? J Res Nurs. 2016;21(8):638–648. doi:10.1177/1744987116678900
14. Røsstad T, Garåsen H, Steinsbekk A, Sletvold O, Grimsmo A. Development of a patient-centred care pathwayacross healthcare providers: a qualitative study. BMC Health Serv Res. 2013;13:121. doi:10.1186/1472-6963-13-438
15. Næss G, Kirkevold M, Hammer W, Straand J, Wyller TB. Nursing care needs and services utilised by home-dwelling elderly with complex health problems: observational study. BMC Health Serv Res. 2017;17(1):645. doi:10.1186/s12913-017-2600-x
16. Wallace E, Salisbury C, Guthrie B, Lewis C, Fahey T, Smith SM. Managing patients with multimorbidity in primary care. Bmj. 2015;350:h176. doi:10.1136/bmj.h176
17. Caplan GA, Williams AJ, Daly B, Abraham K. A randomized, controlled trial of comprehensive geriatric assessment and multidisciplinary intervention after discharge of elderly from the emergency department—the DEED II study. J Am Geriatr Soc. 2004;52(9):1417–1423. doi:10.1111/j.1532-5415.2004.52401.x
18. Smith SM, Wallace E, O’Dowd T, Fortin M. Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. Cochrane Database Syst Rev. 2016;3:CD006560.
19. Liamputtong P. Focus Group Methodology: Principle and Practice. London: SAGE Publications; 2011.
20. World Medical Association. Declaration of Helsinki. 2013; Available from: http://www.wma.net/en/30publications/10policies/b3/index.html.
21. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40:795–805. doi:10.1177/1403494812465030
22. Bosk CL, Dixon-Woods M, Goeschel CA, Pronovost PJ. Reality check for checklists. Lancet. 2009;374(9688):444–445. doi:10.1016/s0140-6736(09)61440-9
23. Vlaeyen E, Stas J, Leysens G, et al. Implementation of fall prevention in residential care facilities: a systematic review of barriers and facilitators. Int J Nurs Stud. 2017;70:110–121. doi:10.1016/j.ijnurstu.2017.02.002
24. Jaul E. Assessment and management of pressure ulcers in the elderly. Drugs Aging. 2010;27(4):311–325. doi:10.2165/11318340-000000000-00000
25. Torvik K, Nordtug B, Brenne IK, Rognstad MK. Pain assessment strategies in home care and nursing homes in Mid-Norway: a cross-sectional survey. Pain Manag Nurs. 2015;16(4):602–608. doi:10.1016/j.pmn.2015.01.001
26. Thim T, Krarup NHV, Grove EL, Rohde CV, Løfgren B. Initial assessment and treatment with the Airway, Breathing, Circulation, Disability, Exposure (ABCDE) approach. Int J Gen Med. 2012;5:117–121. doi:10.2147/IJGM.S28478
27. Spångfors M, Arvidsson L, Karlsson V, Samuelson K. The national early warning score: translation, testing and prediction in a Swedish setting. Intensive Crit Care Nurs. 2016;37:62–67. doi:10.1016/j.iccn.2016.05.007
28. Dale B, Hvalvik S. Administration of care to older patients in transition from hospital to home care services: home nursing leaders’ experiences. J Multidiscip Healthc. 2013;6:379–389. doi:10.2147/JMDH.S51947
29. Parke B, Hunter KF, Strain LA, Marck PB, Waugh EH, McClelland AJ. Facilitators and barriers to safe emergency department transitions for community dwelling older people with dementia and their caregivers: a social ecological study. Int J Nurs Stud. 2013;50(9):1206–1218. doi:10.1016/j.ijnurstu.2012.11.005
30. Ellis G, Langhorne P. Comprehensive geriatric assessment for older hospital patients. Br Med Bull. 2004;71:45–59. doi:10.1093/bmb/ldh033
31. Stott DJ, Langhorne P, Knight PV. Multidisciplinary care for elderly people in the community. Lancet. 2008;371(9614):699–700. doi:10.1016/S0140-6736(08)60317-7
32. Buurman BM, Parlevliet JL, van Deelen BA, de Haan RJ, de Rooij SE. A randomised clinical trial on a comprehensive geriatric assessment and intensive home follow-up after hospital discharge: the Transitional Care Bridge. BMC Health Serv Res. 2010;10:296. doi:10.1186/1472-6963-10-302
33. Zaheer S, Ginsburg LR, Wong HJ, Thomson K, Bain L. Importance of safety climate, teamwork climate and demographics: understanding nurses, allied health professionals and clerical staff perceptions of patient safety. BMJ Open Qual. 2018;7(4):e000433. doi:10.1136/bmjoq-2018-000433
34. Rice AH. Interdisciplinary collaboration in health care: education, practice, and research. Nat Acad Pract Forum. 2000;2(1):59–73.
35. Røsstad TG. Generic Care Pathway for Elderly Patients in Need of Home Care Services after Hospital Discharge A cluster RCT with nested qualitative studies of development and implementation [Doctoral thesis]. Trondheim: NTNU; 2016.
36. Fossum M, Ehnfors M, Svensson E, Hansen LM, Ehrenberg A. Effects of a computerized decision support system on care planning for pressure ulcers and malnutrition in nursing homes: an intervention study. Int J Med Inform. 2013;82(10):911–921. doi:10.1016/j.ijmedinf.2013.05.009
37. Hansson A, Arvemo T, Marklund B, Gedda B, Mattsson B. Working together — primary care doctors’ and nurses’ attitudes to collaboration. Scand J Public Health. 2009;38(1):78–85. doi:10.1177/1403494809347405
38. Supper I, Catala O, Lustman M, Chemla C, Bourgueil Y, Letrilliart L. Interprofessional collaboration in primary health care: a review of facilitators and barriers perceived by involved actors. J Public Health (Oxf). 2015;37:716–727.
39. De Marinis MG, Piredda M, Pascarella MC, et al. ‘If it is not recorded, it has not been done!’? consistency between nursing records and observed nursing care in an Italian hospital. J Clin Nurs. 2010;19(11–12):1544–1552. doi:10.1111/j.1365-2702.2009.03012.x
40. Stevenson JE, Israelsson J, Petersson G, Bath PA. Factors influencing the quality of vital sign data in electronic health records: A qualitative study. J Clin Nurs. 2018;27(5–6):1276–1286. doi:10.1111/jocn.14174
41. Paans W, Sermeus W, Nieweg RM, van der Schans CP. Prevalence of accurate nursing documentation in patient records. J Adv Nurs. 2010;66(11):2481–2489. doi:10.1111/j.1365-2648.2010.05433.x
42. Ehrenberg A, Ehnfors M, Ekman I. Older patients with chronic heart failure within Swedish community health care: a record review of nursing assessments and interventions. J Clin Nurs. 2004;13(1):90–96.
43. Devik SA, Olsen RM, Fiskvik IL, et al. Variations in drug-related problems detected by multidisciplinary teams in Norwegian nursing homes and home nursing care. Scand J Prim Health Care. 2018;36(3):291–299. doi:10.1080/02813432.2018.1499581
44. Cheevakasemsook A, Chapman Y, Francis K, Davies C. The study of nursing documentation complexities. Int J Nurs Pract. 2006;12(6):366–374. doi:10.1111/j.1440-172X.2006.00596.x
45. Wheatley I. The nursing practice of taking level 1 patient observations. Intensive Crit Care Nurs. 2006;22(2):115–121. doi:10.1016/j.iccn.2005.08.003
46. Wadmann S, Strandberg-Larsen M, Vrangbæk K. Coordination between primary and secondary healthcare in Denmark and Sweden. Int J Integr Care. 2009;9:e04–e04. doi:10.5334/ijic.302
47. Mur-Veeman I, van Raak A, Paulus A. Comparing integrated care policy in Europe: does policy matter? Health Policy. 2008;85(2):172–183. doi:10.1016/j.healthpol.2007.07.008
Supplementary material
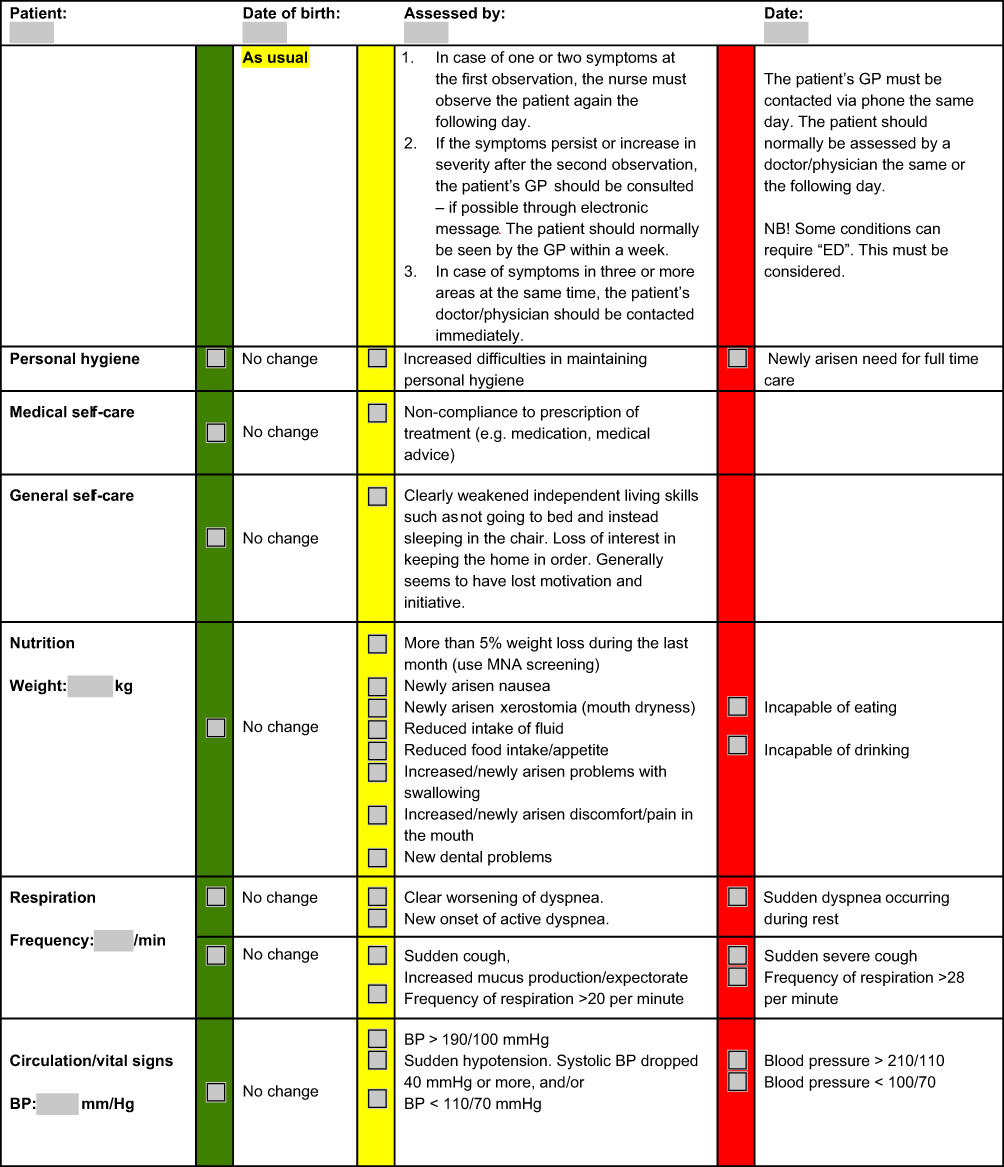 |
Figure S1 (Continued) |
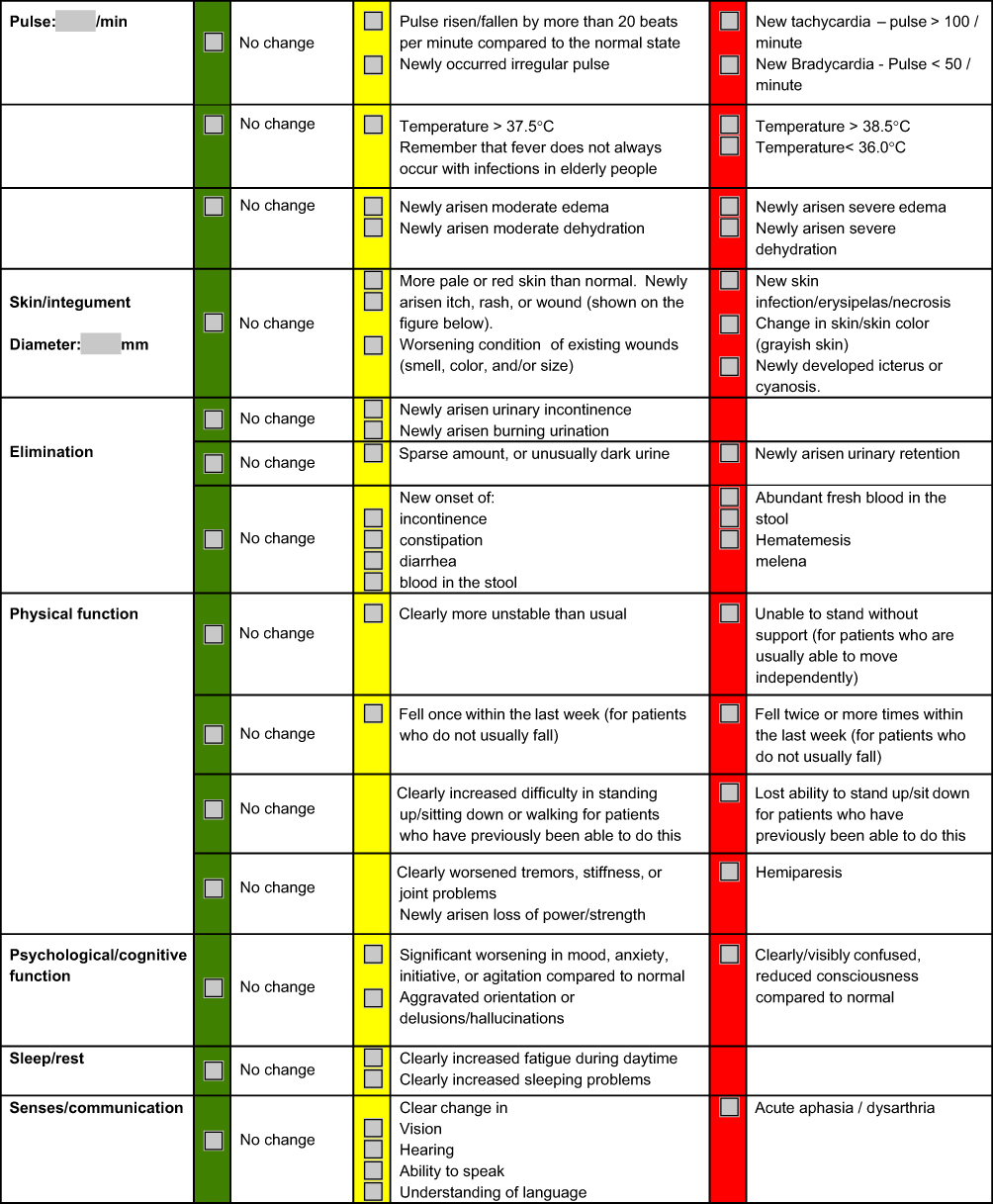 |
Figure S1 (Continued) |
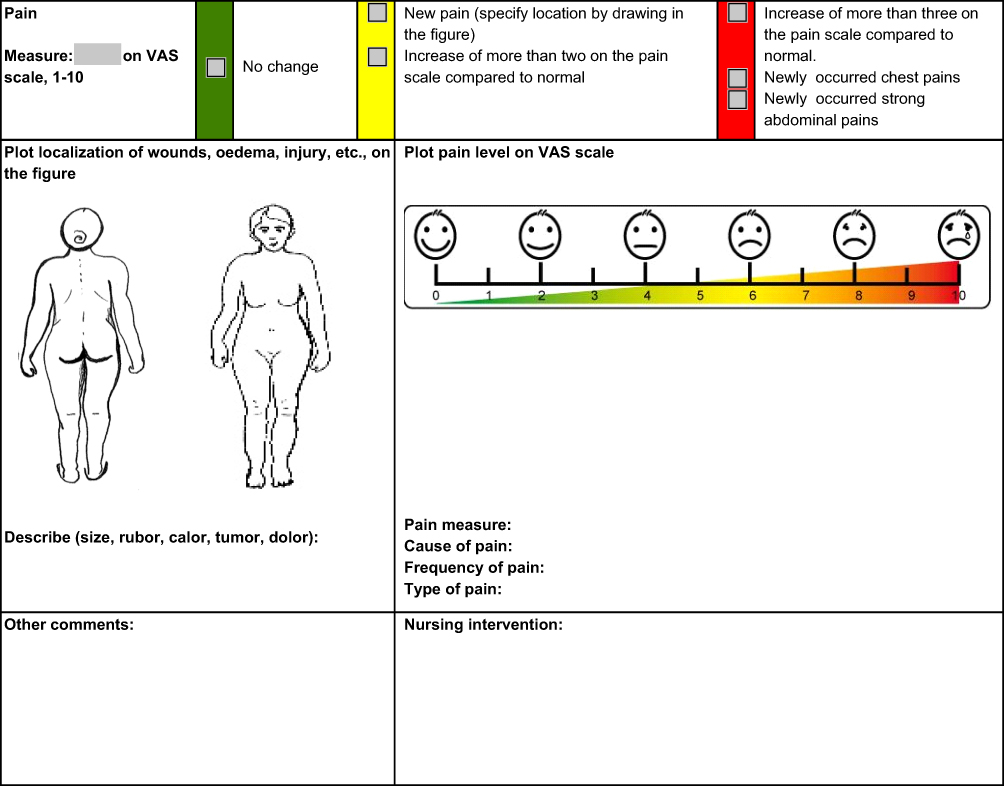 |
Figure S1 Sub Acute Functional decline in the Elderly instrument (SAFE).Note: An interdisciplinary team from Oslo University Hospital, University of Oslo (UiO) and districts in Oslo municipality, developed SAFE. As project manager and responsible for further development and validation of SAFE, Edith L. Roth Gjevjon (Oslo University Hospital) has granted permission to use SAFE (translated into English by the first author). |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.