Back to Journals » Infection and Drug Resistance » Volume 15
Staphylococcal Cassette Chromosome mec Typing and Multilocus Variable Number Tandem Repeat Analysis of Methicillin Resistant Staphylococcus aureus Clinical Isolates with Vancomycin Creep Phenomenon
Authors Arshad F ![]() , Saleem S, Tahir R, Jahan S
, Saleem S, Tahir R, Jahan S ![]() , Jabeen K, Khawaja A, Huma Z, Roman M, Shahzad F
, Jabeen K, Khawaja A, Huma Z, Roman M, Shahzad F ![]()
Received 31 March 2022
Accepted for publication 2 July 2022
Published 25 July 2022 Volume 2022:15 Pages 3927—3938
DOI https://doi.org/10.2147/IDR.S368912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Faiqa Arshad,1 Sidrah Saleem,1 Romeeza Tahir,2 Shah Jahan,2 Kokab Jabeen,3 Aneela Khawaja,4 Zille Huma,1 Muhammad Roman,1 Faheem Shahzad2
1Department of Microbiology, University of Health Sciences, Lahore, Punjab, Pakistan; 2Department of Immunology, University of Health Sciences, Lahore, Punjab, Pakistan; 3Department of Pathology, Ammer ud Din Medical College, PGMI, Lahore, Punjab, Pakistan; 4Department of Pathology, Rahbar Medical & Dental College, Lahore, Punjab, Pakistan
Correspondence: Faiqa Arshad, Department of Microbiology, University of Health Sciences, Khayaban-e-Jamia, Block D Muslim Town, Lahore, Punjab, 54600, Pakistan, Email [email protected]
Background: The association of treatment failure and mortality with vancomycin minimum inhibitory concentration creep (MIC) is a matter of serious concern in patients with severe methicillin resistant Staphylococcus aureus (MRSA) infections. The purpose of the study was to identify and characterize staphylococcal cassette chromosome mec (SCCmec) and clonal types of MRSA strains, exhibiting the vancomycin MIC creep phenomenon.
Methods: A total of 3305 S. aureus strains were isolated from various clinical samples of Lahore General Hospital, Lahore, Pakistan. MRSA strains were identified by cefoxitin resistant (≤ 21mm) followed by mecA and mecC gene genotyping. Vancomycin MIC creep was determined by E-test. Isolates having MIC values > 1.5 μg/mL were further subjected for SCCmec typing (I–V and XI) and multiple-locus variable number tandem repeat analysis (MLVA) by amplification of spa, sspA, clfA, clfB, and sdrCDE genes. A dendrogram was created based on the similarity index using bioneumerics software.
Results: About 13.3% (440/3305) isolates were MRSA with 99.3% (437/440) and 0.7% (3/440) carried mecA and mecC genes, respectively. In 120 MRSA isolates, the MIC of vancomycin was > 1.5μg/mL. In MRSA isolates with high vancomycin MIC (> 1.5μg/mL), the most common SCCmec type was SCCmec III (38.3%), followed by SCCmec IVa (15.8%), SCCmec IIIa (13.3%,), SCCmec IVc (7.5%), SCCmec IVe (5.8%), SCCmec IVd (5.8%), SCCmec IVb (4.2%), SCCmec II (2.5%), SCCmec V (1.7%), SCCmec I (1.7%) and SCCmec XI (1.7%). MLVA revealed 60 genotypic groups of MRSA isolates having a 92% similarity index.
Conclusion: SCCmec III was the most common type in genetically related MRSA isolates showing vancomycin MIC creep. The presence of SCCmec XI may further add burden to infection control measures.
Keywords: methicillin resistant Staphylococcus aureus, staphylococcal chromosomal cassette, multilocus variable number tandem repeat analysis
Introduction
MRSA is the leading cause of morbidity and mortality in both healthcare and community-acquired settings.1 The emergence and spread of MRSA strains with multidrug resistance genes have severely limited the treatment options for staphylococcal infections around the world.2
For many years, vancomycin has been a staple of treatment for serious MRSA infections.3 An increase in vancomycin minimum inhibitory concentration (MIC) values in MRSA strains even within the susceptible range (MIC creep) is the cause of serious concern.4 This phenomenon of vancomycin MIC creep may be a significant risk factor for public health, posing additional challenges in the management of MRSA infections.5 Microbiological and clinical data indicate treatment failure in infections with MRSA strains exhibiting vancomycin MIC creep. Several studies found poor clinical outcomes despite a vancomycin MIC in the susceptible range of ≤2μg/mL especially when ranging MIC 1.5–2 μg/mL.6 Rapid and reliable typing methods are thus required for the identification of such precarious MRSA clones, particularly those with high vancomycin MIC values.7 SCCmec typing is one of the most important methods for studying not just MRSA epidemiology but also the evolution and global spread of MRSA clones.8 SCCmec acquisition by methicillin-sensitive S. aureus strains has the potential to transform them into hazardous multidrug resistant pathogens with the ability to adapt and thrive in a hospital setting with poor infection control.9 Several different SCCmec types have been recognized worldwide.10 Thirteen allotypes of SCCmec have been identified, ranging from I to XIII, based on the combination of complexes of the mec and ccr gene.11 Human infections have been linked to SCCmec types from I–VIII.12 However, SCCmec types IX and X, are linked to livestock infection.13 All these SCCmec types have now been disseminated worldwide and new variants are constantly emerging.14
Analysis of variable number tandem repeats (VNTR) loci identified in the genomes of several bacterial species has resulted in advances in molecular typing. Multiple-locus VNTR analysis (MLVA) refers to a molecular typing system established by analysing the number of repeats on different VNTR loci. The MLVA system is used to determine the relationship of isolates and can also provide insights into population structure.15 MLVA can well differentiate between phylogenetically unrelated strains.16 For the major clonal complexes of S. aureus, the MLVA scheme has high-quality type ability and excellent discriminatory power.17 MLVA has also been reported as a reliable tool for understanding the evolution of MRSA.18
The current study aimed to identify and characterize SCCmec and clonal types of MRSA strains that exhibited vancomycin MIC creep in clinical isolates.
Materials and Methods
Sample Collection
The study was approved by the ethical review board of the University Health Sciences and Lahore General Hospital (LGH), Lahore, Pakistan (UHS/REG-18/ERC/3590). A total number of 3305 S. aureus isolates were collected from the laboratory of LGH during five years (2016–2020). Isolates were recovered from different clinical samples such as pus, wound swabs, blood, sputum, urine, and aspirates from patients admitted to the wards such as medicine, surgery, gynecology, eye, ear, nose and throat, pediatric, and intensive care units.
Culture and Identification of S. aureus Isolates
S. aureus isolates were identified after observing colony morphology on blood agar plates and biochemical testing (catalase, coagulase, and DNase positive). ATCC 12600 S. aureus was used as control strains.
Identification of MRSA by Kirby-Bauer Disc Diffusion Method
Antimicrobial susceptibility was accomplished according to clinical laboratory and standard institute (CLSI) guidelines (2019) using cefoxitin disc (30μg). All the strains with cefoxitin zone diameter of ≤21 mm were considered methicillin resistant. MRSA ATCC 33591 and MSSA ATCC 25923 were used as control strains.
Extraction of DNA from Isolates
DNA was extracted by the boiling method as described previously.19 The quality and quantity of extracted DNA were determined by nanodrop (spectrophotometer, Bio Rad, USA). The quality of the extracted DNA was predicted from the ratio of absorbance at 260 and 280 nm.
Amplification of mecA and mecC Gene
mecA and mecC genes were amplified using 50ng extracted genomic DNA.20,21 MRSA ATCC 33591 and BAA 2312 were used as a control strain for the mecA and mecC genes, respectively.
Determination of Vancomycin MIC for MRSA Isolates
Vancomycin MICs for MRSA isolates were determined using the E-test method. Based on MIC results, isolates were classified as susceptible or resistant according to criteria set by CLSI. Isolates with vancomycin MICs ≤2µg/mL were considered as sensitive, 4–8µg/mL were regarded as vancomycin intermediate S. aureus (VISA), and ≥16µg/mL were considered as vancomycin resistant S. aureus (VRSA). Isolates with vancomycin MIC >1.5 µg/mL were subjected for molecular characterization by SCCmec typing and MLVA.
Determination of SCCmec Types 1-V and XI
SCCmec gene identification I–V and SCCmec XI were carried out as described previously by Zhang et al and Stegger et al, respectively.22,23 The primers for SCC mec I–V and SCCmec XI are given in the Supplementary Table. BAA 2312 was used as a control strain for SCCmec XI.
MLVA
MLVA was performed by multiplex PCR to simultaneously amplify the hypervariable VNTR regions of the spa, sspA, clfA, clfB, and sdrCDE genes.16 The primers for MLVA are given in the Supplementary Table.
Data Analysis
SPSS version 27.0 was used to analyze the data. The MIC population distribution for each year was graphically evaluated to assess vancomycin MIC creep. The SCCmec typing findings for each year were given in the form of percentages for each SCCmec category including SCCmec type I–V and SCCmec XI. A dendrogram was built based on variation in the base pairs (bp) of repeats for MLVA using the bionumerics 8.0 program to show the relatedness and genetic diversity among MRSA. Number of repeats that were obtained at specific loci for isolated strains were fed into Bionumeric software version 8.0 to draw the minimum spanning tree (MST), also known as a phylogenetic tree. In this program, the order of each allelic repeat that fed into software was (clfA, clfB, sdrD, sdrC, sdrE, spa, and sspa).
Results
Genotypic evaluation of cefoxitin resistant S. aureus isolates confirmed 440 MRSA harboring the mecA and mecC genes. About 13.3% (440/3305) isolates were MRSA with 99.3% (437/440) and 0.7% (3/440) carried mecA and mecC genes, respectively. Percent of MRSA isolates with vancomycin MIC 0.5 µg/mL, 0.75 µg/mL, 1 µg/mL, 1.5 µg/mL and 2 µg/mL is depicted in Figure 1. The vancomycin MIC “1.0”µg/mL had declined from 28.6% of isolates in 2016 to 14.8% in 2020. The percentage of isolates with MIC “2.0”µg/mL increased from 19.0% to 39.8% during 5 years. A total of 120 MRSA isolates were found to have MIC values of >1.5µg/mL during 5 years. However, none of the isolates was found to be VISA and VRSA.
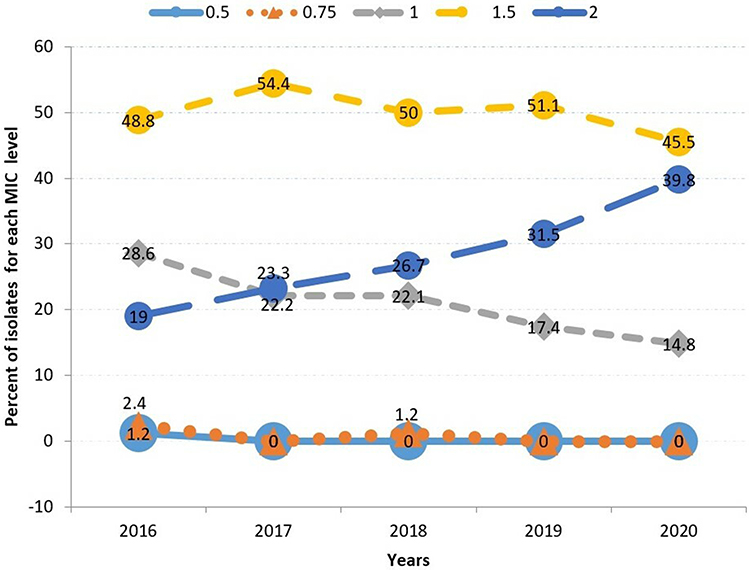 |
Figure 1 Distribution trend of vancomycin MIC values (2016–2020) (n = 440). MRSA isolates with vancomycin MIC values of 0.5µg/mL and 0.75µg/mL remained at very low levels throughout the years (lower two lines). Isolates with MIC 1µg/mL show an evident decline as indicated with the grey line while isolates with MIC value of 2µg/mL show a clear rising trend (dark blue line). At the top of the figure, the yellow line depicts the highest percentage of MRSA isolates with vancomycin MICs values of 1.5 µg/mL. |
When isolates with vancomycin MIC >1.5µg/mL were tested for SCCmec typing, it was observed that SCCmec III was found to be the most common type in 38.3% of these isolates, followed by SCCmec IVa (15.8%), SCCmec IIIa (13.3%), SCCmec IVc (7.5%), SCCmec IVe (5.8%), SCCmec IVd (5.8%), SCCmec IVb (4.2%), SCCmec II (2.5%), SCCmec V (1.7%), SCCmec I (1.7%) and SCCmec type XI (1.7%). In addition, 1.7% of MRSA isolates were untypeable [Table 1]. Amplification of SCCmec types I–V and SCCmec XI elements are depicted in Figures 2 and 3, respectively.
 |
Table 1 Distribution of SCCmec Gene in MRSA Isolates (2016–2020) |
 |
Figure 2 Gel electrophoresis pattern for identification of SCCmec types and subtypes by multiplex PCR for clinical isolates of MRSA. Lane 1 is negative control. Lanes 2 represents SCCmec type IVe (175bp); lane 3 represents SCCmec type IVb (493bp); lane 4 represents SCCmec type IVd (881bp); lane 5 represents SCCmec type Iva (776bp); lane 6 represents SCCmec type I (613bp); lane 7 represents SCCmec type IVc (200bp); lane 8 represents SCCmec type II (398bp). SCCmec type III a (257bp); lane 10 represents SCCmec III type (280bp) and lane 11 represents SCCmec type V (325bp). Lane 12 is empty. M is the 100 bp DNA ladder (Thermo Scientific). |
 |
Figure 3 Gel electrophoresis pattern for identification of SCCmec type XI by multiplex PCR for clinical isolates of MRSA. M is a 100 bp DNA ladder (Thermo Scientific). Lane 1: negative control; lane 2 represents positive control of SCCmec XI ATCC- BAA 23122, Lane 3: MRSA strain represents SCC mec type XI carrying mec1 (344bp); mecR1 (710bp); blaZ (809bp); ccrA1 (932bp) and ccrB3 (1499bp). |
By MLVA analysis using Bionumeric 8.0 software, all the tandem repeats of 120 isolated strains get shuffled and presented the relatedness by amplified bands at their specific loci (clfA, clfB, sdrD, sdrC, sdrE, spa, and sspa) in the dendrogram [Figure 4]. Sixty MLVA haplotypes were reported out of 120 MRSA stains with vancomycin MIC value >1.5µg/mL [Figure 4]. Concerning to 100% similarity between the strains, the stains having the same genetic clusters were placed under one genotype. The strains with the same genotype were exactly like each other for their band position at specific loci although they have different strain sources. Therefore, using MLVA analysis even a slight difference of base pairs and their position at specific loci was detected and placed in the separate genotypic category. MLVA shuffled all the tandem repeats of strains and then arranged them according to the similarity pattern. This makes closely related or similar genotypic strains lie close together while unidentical repeats at their loci go apart.
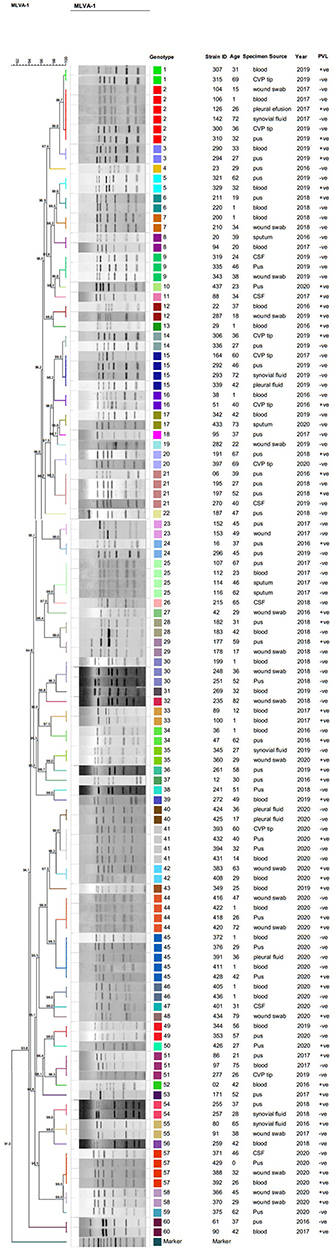 |
Figure 4 Dendrogram based on the clustering of strains according to similarity index (by Dice coefficient and UPGMA approach) through MLVA analysis of MRSA strains. By MLVA analysis 120 isolates were clustered into 60 haplotypes based on similarity index due to slight variations in VNTRs using Bionumerics Software version 8.0. A dendrogram was produced with the settings of position tolerance (optimization 1% and band position tolerance 0.75%). All strains were shuffled according to their similarity index and clustered into genotypes. |
In the analysis of MST, order of each allelic repeats that fed into software was (clfA, clfB, sdrD, sdrC, sdrE, spa, and sspa). Out of 120 isolated strains, a total of 60 clusters were connected following the distribution of VNTRs. The distribution of strains occurred based on the variation in the base pair size of each strain at single or multiple loci and lead to the formation of a new MLVA strain [Figure 5]. In this MST it was seen that circles represent the number of isolates; circles of similar colors represent that they belong to one or the same genotype. Furthermore, more closely related genotypic clusters of isolated MLVA strain were connected with a solid bold line. On the other hand, distant or less closely related genotypes were joined with thin or light lines. In this phylogenic tree, closely related genotypes were encoded with same color such as strain ID 416, 418, 422 and 420 clustered and connected with solid lines and represented with orange color and it belong to genotypic group 44.
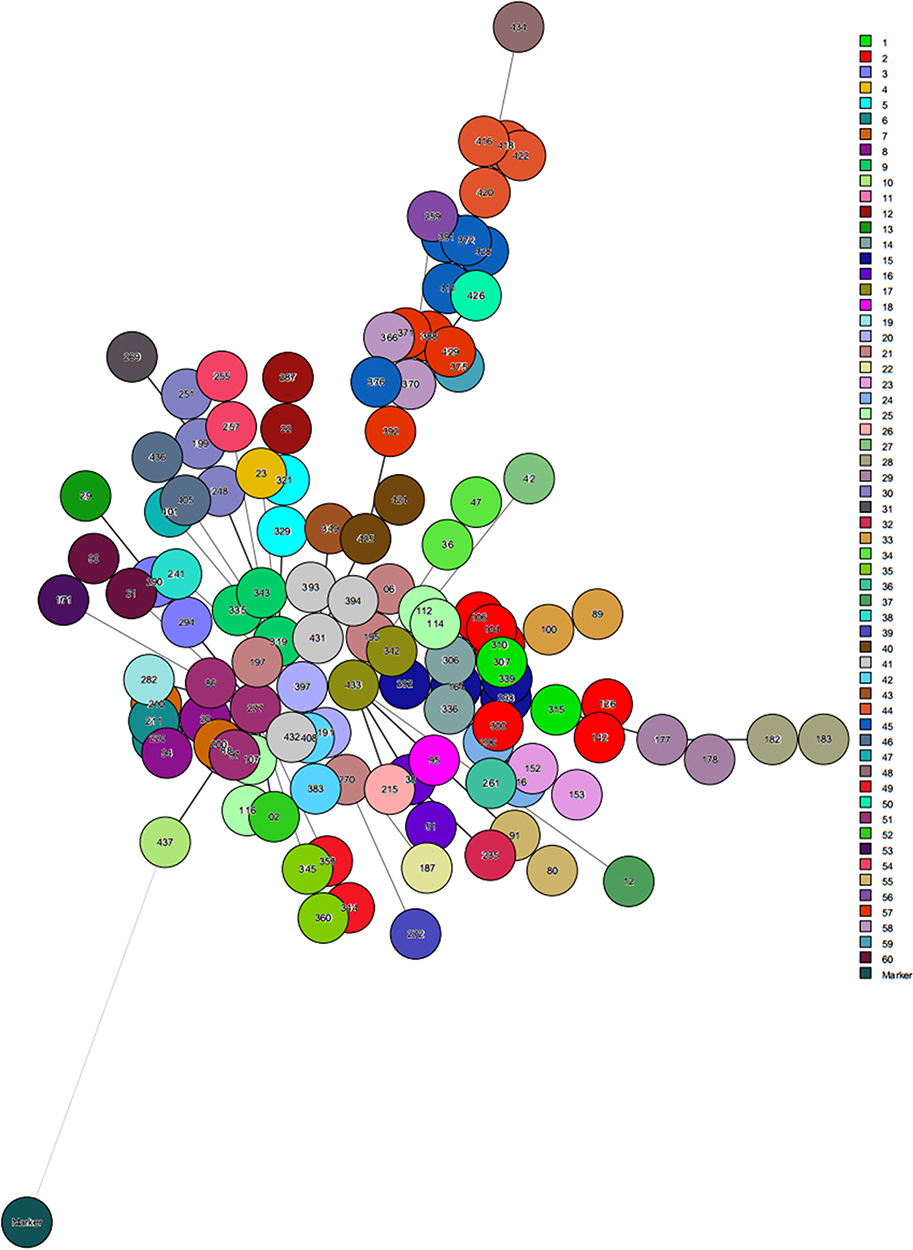 |
Figure 5 Minimum Spanning Tree analysis of MRSA isolates depicting their phylogenetic relationship according to VNTRs (clfA, clfB, sdrD, sdrC, sdrE, spa and sspa) distribution index. It is based on slight base pair variations leading to a new MLVA type strain using Bionumerics software version 8.0. In this MST analysis total 60 clusters were found. Circles are representing MRSA isolates and the same colored circles belong to one genotype. Furthermore closely related genotypes were connected with bold lines while distantly related were connected with thin lines. |
Discussion
A significant shift toward higher vancomycin MIC values (MIC creep) has been observed, which raises serious concerns.24 MIC creep has been associated with therapeutic failure in patients with serious MRSA infections. High mortality was seen in patients of MRSA bacteremia having vancomycin MIC ≥ 1.5 µg/mL. The physician must be warned of the potential risk of treatment failure at high MIC value and alternative treatments should be opted if necessary.25,26 It is critical to assess the occurrence and trend of vancomycin MIC creep phenomenon in settings to generate evidence-based knowledge for clinicians and better management of patients. Even though new drugs such as dalbavancin and ceftaroline have been developed to be an effective alternative therapy for multi-drug resistance MRSA strains, vancomycin remains the first choice in the majority of countries around the world.27 Moreover, by determining the molecular characteristics of such infectious and treatment challenging strains exhibiting MIC creep with high MIC values, we will be able to focus on our infection control practices to avoid their dissemination in the hospital and community.
SCCmec characterization of these isolates revealed that SCCmec III and IIIa were the most prevalent mec types among MRSA isolates as indicated in studies of Iran and Malaysia.28,29 A high prevalence of SCCmec type III/IIIa has been reported in three different geographical areas of India and Pakistan.30 A previous study of 11 Asian countries revealed that SCCmec type II was the most prevalent in Japan and Korea while SCCmec type III was most prevalent in Saudi Arabia, Singapore, Indonesia, Vietnam, Sri Lanka, Thailand, India, and the Philippines. A low prevalence of SCCmec type I in these Asian countries.31 SCCmec III is commonly carried by healthcare associated MRSA (HA-MRSA). HA-MRSA is multidrug resistant and causes infections commonly in elderly patients with underlying bronchopulmonary and cardiovascular diseases.32
The predominance of SCCmec III and IIIa in our setting might be because of antibiotic selective pressure, which led to clonal selection and dissemination. SCCmec is important not only in antimicrobial resistance but also in the molecular epidemiology and evolution of MRSA. As a result, a thorough understanding of the prevalence and characteristics of SCCmec types may play a potential role in the investigation, surveillance, and implementation of MRSA, ultimately assisting in the development of precautionary and therapeutic methodologies.33 Similarly, another study in Pakistan reported a high percentage of SCCmec type III and its variants.34 SCCmec type IV, sub types (Iva-IVe) were the next leading types in this study. Similarly, another study reported that SCCmecIV types and subtypes were most common after SCCmec type III.35 However, a study in Pakistan revealed that the most prevalent SCCmec type was SCCmec type IV followed by SCCmec type II and then III.36 Another study reported majority of isolates carrying SCCmec type IV followed by SCCmec type V.14 SCCmec IV and V are main types in community-acquired MRSA (CA-MRSA). CA-MRSA is well recognized for its ability to cause diseases, such as skin and soft tissue infections and necrotizing pneumonia.37
Concerning the significance of SCCmec typing, a study described that SCCmec associated virulence factors may have an impact on disease outcome, with SCCmec type IVa being associated with more metastatic diseases and SCCmec II being associated with increased patient mortality. The study recommended that more research is needed to determine which virulence factors of SCCmec types influence disease outcomes.38
SCCmec I and II were shown to have a very low prevalence in the current study. In Europe, however, there was a higher frequency of SCCmec I and II, as well as a predominance of SCCmec IV and V in hospital settings, but a surprising paucity of SCCmec III.39 Another study reported a high frequency of SCCmec type IA and IIC among MRSA isolates for the first time in Asian countries.40
The discrimination of HA-MRSA and CA-MRSA has become more complicated due to changing epidemiology as the community-acquired SCCmec types infiltrate in hospital settings and vice versa. This transmission, intermingling, and increasing diversity of SCCmec types carrying multiple drug-resistant genes among the community and hospital settings can worsen the clinical outcomes thus limiting the therapeutic options.41 The detection of mecA and mecC genes at the molecular level demonstrates an ongoing evolutionary process in MRSA strains. Simultaneous detection of mecA and mecC genes is critical for correct MRSA strain identification.42 If MRSA is not detected in time, it can lead to treatment failure and the spread of resistant strains in the community.43 The situation may impose an additional medical and financial burden.44
The situation has become more complicated due to the emergence of the SCCmec type XI disseminating mecC gene in animals and humans.45 SCCmec type XI has a wide geographical distribution and has adapted to a variety of host species, including livestock and wildlife. This could be a potential source of zoonotic infections and may complicate accurate diagnosis, thus adding medical and financial burdens.2,46 A less frequent SCCmec XI was also found in 1.7% of MRSA isolates. SCCmec XI is characterized by different components including mecI, mecR1, blaZ, ccr A, and ccrB genes. SCCmec XI has also been reported in Ireland, Germany, and Japan.47–49
Another study documented that even though SCCmec type XI is uncommon in human isolates, its presence can be misjudged, necessitating molecular typing to confirm its presence.50 Another study also stated that SCCmec XI containing toxigenic virulence factors raises the alarm for MRSA isolates with high virulence potential in Europe, emphasizing the importance of proper molecular detection.46 Furthermore, a study identified SCCmec XI by detecting its various components, but few of those isolates lacked ccrA and ccrB genes, contrary to our findings. They did, however, speculate that isolates with ccrA and ccrB genes might have minor sequence differences in their SCCmec type XI ccr specific alleles.23
MLVA was performed on MRSA isolates in this study to obtain phylogenetic relationships in the form of a dendrogram. By using the MLVA technique with Bionumeric software 8.0 we were able to separate the PCR amplicons even with small differences in a band size that allowed us to obtain an accurate product size. MRSA isolates produce a PCR product with specific VNTRs converted into tandem repeats at their specific loci. The genotypes were formed by MLVA and shrunk down to 60 haplotypes. A minor change in the base pair of the VNTR created a new MLVA strain, which now belongs to a different genotypic group. Similarly, 63 MLVA types were identified in 123 MRSA isolates in an earlier study in Pakistan. MLVA was found an effective technique to understand the phylogenetic relationship and distribution of MRSA isolates.18 Moreover, in another study, MLVA was used to type S. aureus isolates. MLVA performed exceptionally well in distinguishing between unrelated isolates.51
Low genetic diversity was found among MRSA strains in this study because all strains had a similarity index above 92%. A similar observation of diversity was documented by another study but in different bacterial species in India.52 MLVA can be used as a standardized and portable molecular typing technique. This technique can contribute to our understanding of the genetic diversity of various pathogens, particularly in areas where new isolates are emerging.53 A previous study also documented that MLVA can differentiate between strains of similar lineages in clonal complexes.15
Conclusion
In conclusion, SCCmec III was found to be the most common type in MRSA isolates exhibiting the vancomycin MIC creep phenomenon. Discovery of mecC gene and the presence of SCCmec XI indicates zoonotic origin of these MRSA isolates which highlights the complexity of the antimicrobial resistance scenario. A similarity index above 92% by MLVA analysis indicated that genetic diversity among the MRSA population was very low and strains were related to each other. Data on identification and characterization of clones of MRSA with high MIC values will provide insight to clinicians and health professionals to formulate local antibiotic policy in each hospital and implementation of infection control measures which consequently will hamper the distribution and spread of MRSA in Pakistan.
Data Sharing Statement
The database generated and analysed during the current study is available from the corresponding author on reasonable request.
Ethics Approval
Clinical isolates of S. aureus were obtained after getting an ethical approval of the ethical review committee of Lahore General Hospital and University of Health Sciences, Lahore, Pakistan ref# (UHS/REG-18/ERC/3590).
Consent for Publication
Permission was taken from the hospital to publish the findings of study.
Acknowledgments
We would like to acknowledge the Vice-Chancellor and the Office of Research, Innovation, and Commercialization (ORIC) of the University of Health Sciences, Lahore. Pakistan for administrative support.
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; participated in the drafting, revising, or critical review of the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agreed to be accountable for all aspects of the work.
Funding
The research project was partially supported by the university research fund.
Disclosure
The authors have no relevant financial or nonfinancial interest to disclose in this work.
References
1. Garoy EY, Gebreab YB, Achila OO, et al. Methicillin-resistant Staphylococcus aureus (MRSA): prevalence and antimicrobial sensitivity pattern among patients—a multicenter study in Asmara, Eritrea. Can J Infect Dis Med Microbiol. 2019;2019(2):1–9. doi:10.1155/2019/8321834
2. Lakhundi S, Zhang K. Methicillin-resistant Staphylococcus aureus: molecular characterization, evolution, and epidemiology. Clin Microbiol Rev. 2018;31(4):1–103. doi:10.1128/CMR.00020-18
3. Kaleem F, Usman J, Khalid A, Hassan A, Omair M. Comparison of in vitro efficacy of linezolid and vancomycin by determining their minimum inhibitory concentrations against methicillin resistant Staphylococcus aureus (MRSA). J Pak Med Assoc. 2011;61(4):356–359.
4. Tarai B, Das P, Kumar D. Recurrent challenges for clinicians: emergence of methicillin-resistant Staphylococcus aureus, vancomycin resistance, and current treatment options. J Lab Physicians. 2013;5(02):71–78. doi:10.4103/0974-2727.119843
5. Dhawan B, Gadepalli R, Rao C, Kapil A, Sreenivas V. Decreased susceptibility to vancomycin in meticillin-resistant Staphylococcus aureus: a 5 year study in an Indian tertiary hospital. J Med Microbiol. 2010;59(3):375–376. doi:10.1099/jmm.0.011940-0
6. Choi EY, Huh JW, Lim C-M, et al. Relationship between the MIC of vancomycin and clinical outcome in patients with MRSA nosocomial pneumonia. Intensive Care Med. 2011;37(4):639–647. doi:10.1007/s00134-011-2130-7
7. Ghaznavi-Rad E, Shamsudin MN, Sekawi Z, van Belkum A, Neela V. A simplified multiplex PCR assay for fast and easy discrimination of globally distributed staphylococcal cassette chromosome mec types in meticillin-resistant Staphylococcus aureus. J Med Microbiol. 2010;59(10):1135–1139. doi:10.1099/jmm.0.021956-0
8. Deurenberg RH, Vink C, Kalenic S, Friedrich A, Bruggeman C, Stobberingh E. The molecular evolution of methicillin-resistant Staphylococcus aureus. Clin Microbiol Infect. 2007;13(3):222–235. doi:10.1111/j.1469-0691.2006.01573.x
9. Rolo J, Worning P, Boye Nielsen J, et al. Evidence for the evolutionary steps leading to mecA-mediated β-lactam resistance in staphylococci. PLoS Genet. 2017;13(4):1–22. doi:10.1371/journal.pgen.1006674
10. Baig S, Johannesen TB, Overballe-Petersen S, Larsen J, Larsen AR, Stegger M. Novel SCCmec type XIII (9A) identified in an ST152 methicillin-resistant Staphylococcus aureus. Infect Genet Evol. 2018;61:74–76. doi:10.1016/j.meegid.2018.03.013
11. Deurenberg RH, Stobberingh EE. The evolution of Staphylococcus aureus. Infect Genet Evol. 2008;8(6):747–763. doi:10.1111/j.1469-0691.2006.01573.x
12. Ghaznavi-Rad E, Shamsudin MN, Sekawi Z, et al. Predominance and emergence of clones of hospital-acquired methicillin-resistant Staphylococcus aureus in Malaysia. J Clin Microbiol. 2010;48(3):867–872. doi:10.1128/JCM.01112-09
13. Sinlapasorn S, Lulitanond A, Angkititrakul S, et al. SCCmec IX in meticillin-resistant Staphylococcus aureus and meticillin-resistant coagulase-negative staphylococci from pigs and workers at pig farms in Khon Kaen, Thailand. J Med Microbiol. 2015;64(9):1087–1093. doi:10.1099/jmm.0.000119
14. Hannan A, Javed F, Saleem S, Tahira K, Jahan S. Frequency of staphylococcal cassette chromosome mec type IV and type V in clinical isolates of methicillin resistant Staphylococcus aureus. Open J Med Microbiol. 2015;5(02):69–75. doi:10.4236/ojmm.2015.52008
15. Dahyot S, Lebeurre J, Argemi X, et al. Multiple-locus variable number tandem repeat analysis (MLVA) and tandem repeat sequence typing (TRST), helpful tools for subtyping Staphylococcus lugdunensis. Sci Rep. 2018;8(1):1–11. doi:10.1038/s41598-018-30144-y
16. Sabat A, Krzyszton-Russjan J, Strzalka W, et al. New method for typing Staphylococcus aureus strains: multiple-locus variable-number tandem repeat analysis of polymorphism and genetic relationships of clinical isolates. J Clin Microbiol. 2003;41(4):1801–1804.
17. Schouls LM, Spalburg EC, van Luit M, et al. Multiple-locus variable number tandem repeat analysis of Staphylococcus aureus: comparison with pulsed-field gel electrophoresis and spa-typing. PLoS One. 2009;4(4):1–13. doi:10.1371/journal.pone.0005082
18. Arfat Y, Johnson M, Malik S, Morrissey J, Bayliss C. Epidemiology of methicillin resistant Staphylococcus aureus (MRSA) isolates from Pakistan. Afr J Microbiol Res. 2013;7(7):568–576. doi:10.5897/AJMR12.1712
19. Junior JCR, Tamanini R, Soares BF, et al. Efficiency of boiling and four other methods for genomic DNA extraction of deteriorating spore-forming bacteria from milk. Semina. 2016;37(5):3069–3078.
20. Makgotlho PE, Kock MM, Hoosen A, et al. Molecular identification and genotyping of MRSA isolates. FEMS Immunol Med Microbiol. 2009;57(2):104–115. doi:10.1111/j.1574-695X.2009.00585
21. García-Garrote F, Cercenado E, Marín M, et al. Methicillin-resistant Staphylococcus aureu s carrying the mecC gene: emergence in Spain and report of a fatal case of bacteraemia. J Antimicrob Chemother. 2014;69(1):45–50. doi:10.1093/jac/dkt327
22. Zhang K, McClure J-A, Conly JM. Enhanced multiplex PCR assay for typing of staphylococcal cassette chromosome mec types I to V in methicillin-resistant Staphylococcus aureus. Mol Cell Probes. 2012;26(5):218–221. doi:10.1016/j.mcp.2012.04.002
23. Stegger Á, Andersen P, Kearns A, et al. Rapid detection, differentiation and typing of methicillin-resistant Staphylococcus aureus harbouring either mecA or the new mecA homologue mecALGA251. Clin Microbiol Infect. 2012;18(4):395–400. doi:10.1111/j.1469-0691.2011.03715.x
24. Arshad F, Saleem S, Jahan S, Tahir R. Assessment of vancomycin MIC creep phenomenon in methicillin-resistant Staphylococcus aureus isolates in a Tertiary Care Hospital of Lahore. Pak J Med Sci. 2020;36(7):1505–1510. doi:10.12669/pjms.36.7.3273
25. Soriano A, Marco F, Martínez JA, et al. Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin Infect Dis. 2008;46(2):193–200. doi:10.1086/524667
26. Aljohani S, Layqah L, Masuadi E, et al. Occurrence of vancomycin MIC creep in methicillin resistant isolates in Saudi Arabia. J Infect Public Health. 2020;13(10):1576–1579. doi:10.1016/j.jiph.2020.07.008
27. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):18–55. doi:10.1093/cid/ciq146
28. Noordin A, Sapri HF, Sani NAM, et al. Antimicrobial resistance profiling and molecular typing of methicillin-resistant Staphylococcus aureus isolated from a Malaysian teaching hospital. J Med Microbiol. 2016;65(12):1476–1481. doi:10.1099/jmm.0.000387
29. Moosavian M, Shahin M, Navidifar T, Torabipour M. Typing of staphylococcal cassette chromosome mec encoding methicillin resistance in Staphylococcus aureus isolates in Ahvaz, Iran. New Microbes New Infect. 2018;21:90–94. doi:10.1016/j.nmni.2017.11.006
30. Shabir S, Hardy KJ, Abbasi WS, et al. Epidemiological typing of meticillin-resistant Staphylococcus aureus isolates from Pakistan and India. J Med Microbiol. 2010;59(3):330–337. doi:10.1099/jmm.0.014910-0
31. Chongtrakool P, Ito T, Ma XX, et al. Staphylococcal cassette chromosome mec (SCC mec) typing of methicillin-resistant Staphylococcus aureus strains isolated in 11 Asian countries: a proposal for a new nomenclature for SCC mec elements. Antimicrob Agents Chemother. 2006;50(3):1001–1012. doi:10.1128/AAC.50.3.1001-1012.2006
32. Huang Y, Tseng S, Hu J, Tsai J, Hsueh P, Teng L. Clonal spread of SCCmec type IV methicillin-resistant Staphylococcus aureus between community and hospital. Clin Microbiol Lnfect. 2007;13(7):717–724. doi:10.1111/j.1469-0691.2007.01718.x
33. Liu J, Chen D, Peters BM, et al. Staphylococcal chromosomal cassettes mec (SCCmec): a mobile genetic element in methicillin-resistant Staphylococcus aureus. Microb Pathol. 2016;101:56–67. doi:10.1016/j.micpath.2016.10.028
34. Zafar A, Stone M, Ibrahim S, et al. Prevalent genotypes of meticillin-resistant Staphylococcus aureus: report from Pakistan. J Med Microbiol. 2011;60(1):56–62. doi:10.1099/jmm.0.022707-0
35. Amirkhiz MF, Rezaee MA, Hasani A, Aghazadeh M, Naghili B. SCCmec typing of methicillin-resistant Staphylococcus aureus: an eight year experience. Arch Pediatr Infect Dis. 2015;3(4):1–5. doi:10.5812/pedinfect.30632
36. Jamil B, Gawlik D, Syed MA, et al. Hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) from Pakistan: molecular characterisation by microarray technology. Eur J Clin Microbiol Infect Dis. 2018;37(4):691–700. doi:10.1007/s10096-017-3161-y
37. Peng H, Liu D, Ma Y, Gao W. Comparison of community-and healthcare-associated methicillin-resistant Staphylococcus aureus isolates at a Chinese tertiary hospital, 2012–2017. Sci Rep. 2018;8(1):1–8. doi:10.1038/s41598-018-36206-5
38. Ganga R, Riederer K, Sharma M, et al. Role of SCC mec type in outcome of Staphylococcus aureus bacteremia in a single medical center. J Clin Microbiol. 2009;47(3):590–595. doi:10.1128/JCM.00397-08
39. Valsesia G, Rossi M, Bertschy S, Pfyffer GE. Emergence of SCC mec type IV and SCC mec type V methicillin-resistant Staphylococcus aureus containing the Panton-Valentine leukocidin genes in a large academic teaching hospital in central Switzerland: external invaders or persisting circulators? J Clin Microbiol. 2010;48(3):720–727. doi:10.1128/JCM.01890-09
40. Romeeza T, Naeem R, Nadeem A. Multiplex polymerase chain reaction based typing of staphylococcal chromosomal cassette mec of methicillin resistant Staphylococcus aureus from selected hospitals in Lahore. Int Med J Malays. 2010;9(1):5–8.
41. Henderson A, Nimmo GR. Control of healthcare-and community-associated MRSA: recent progress and persisting challenges. Br Med Bull. 2018;125(1):25–41. doi:10.1093/bmb/ldx046
42. Romero-Gómez MP, Mora-Rillo M, Lázaro-Perona F, Gómez-Gil MR, Mingorance J. Bacteraemia due to meticillin-resistant Staphylococcus aureus carrying the mecC gene in a patient with urothelial carcinoma. J Medical Microbiol. 2013;62(12):1914–1916. doi:10.1099/jmm.0.064683-0
43. Ullah A, Qasim M, Rahman H, et al. High frequency of methicillin-resistant Staphylococcus aureus in Peshawar Region of Pakistan. Springerplus. 2016;5(1):1–6. doi:10.1186/s40064-016-2277-3
44. Sabat A, Budimir A, Nashev D, et al. Overview of molecular typing methods for outbreak detection and epidemiological surveillance. Euro Surveil. 2013;18(4):1–15. doi:10.2807/ese.18.04.20380-en
45. García-álvarez L, Holden MT, Lindsay H, et al. Meticillin-resistant Staphylococcus aureus with a novel mecA homologue in human and bovine populations in the UK and Denmark: a descriptive study. Lancet Infect Dis. 2011;11(8):595–603. doi:10.1016/S1473-3099(11)70126-8
46. Sabat AJ, Koksal M, Akkerboom V, et al. Detection of new methicillin-resistant Staphylococcus aureus strains that carry a novel genetic homologue and important virulence determinants. J Clin Microbiol. 2012;50(10):3374–3377. doi:10.1128/JCM.01121-12
47. Shore AC, Deasy EC, Slickers P, et al. Detection of staphylococcal cassette chromosome mec type XI carrying highly divergent mecA, mecI, mecR1, blaZ, and ccr genes in human clinical isolates of clonal complex 130 methicillin-resistant Staphylococcus aureus. Antimicrob Agents Chemother. 2011;55(8):3765–3773. doi:10.1128/AAC.00187-11
48. Kriegeskorte A, Ballhausen B, Idelevich EA, et al. Human MRSA isolates with novel genetic homolog, Germany. Emerg Infect Dis. 2012;18(6):1016–1018. doi:10.3201/eid1806.110910
49. McClure J-A, Conly JM, Obasuyi O, et al. A novel assay for detection of methicillin-resistant Staphylococcus aureus directly from clinical samples. Front Microbiol. 2020;11:1–15. doi:10.3389/fmicb.2020.01295
50. Petersdorf S, Herma M, Rosenblatt M, Layer F, Henrich B. A novel staphylococcal cassette chromosome mec type XI primer for detection of mecC-harboring methicillin-resistant Staphylococcus aureus directly from screening specimens. J Clin Microbiol. 2015;53(12):3938–3941. doi:10.1128/JCM.02328-15
51. Ikawaty R, Willems RJ, Box AT, Verhoef J, Fluit AC. Novel multiple-locus variable-number tandem-repeat analysis method for rapid molecular typing of human Staphylococcus aureus. J Clin Microbiol. 2008;46(9):3147–3151. doi:10.1128/JCM.00861-08
52. Singh M, Malik MA, Singh DK, Doimari S, Sharma R, Sharma R. Multilocus variable number tandem repeat analysis (MLVA)-typing of Brucella abortus isolates of India reveals limited genetic diversity. Trop Anim Health Prod. 2020;52(3):1187–1194. doi:10.1007/s11250-019-02110-x
53. Pruvost O, Magne M, Boyer K, et al. A MLVA genotyping scheme for global surveillance of the citrus pathogen Xanthomonas citri pv. citri suggests a worldwide geographical expansion of a single genetic lineage. PLoS One. 2014;9(6):1–11. doi:10.1371/journal.pone.0098129
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.