Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Standardized Glycemic Management versus Conventional Glycemic Management and Postoperative Outcomes in Type 2 Diabetes Patients Undergoing Elective Surgery
Authors Vongsumran N ![]() , Buranapin S
, Buranapin S ![]() , Manosroi W
, Manosroi W ![]()
Received 15 May 2020
Accepted for publication 2 July 2020
Published 22 July 2020 Volume 2020:13 Pages 2593—2601
DOI https://doi.org/10.2147/DMSO.S262444
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Nuttawut Vongsumran, Supawan Buranapin, Worapaka Manosroi
Division of Endocrinology, Department of Internal Medicine, Faculty of Medicine, Chiang Mai University, Chiang Mai 50200, Thailand
Correspondence: Worapaka Manosroi Tel +66 53 936453
Email [email protected]
Purpose: Optimized postoperative blood glucose control can minimize postoperative complications. Conventional perioperative glycemic control protocol (CG), which has been routinely used in our institution, lacks detailed perioperative glycemic management. A new standardized glycemic control protocol (SG) was designed which employs frequent postoperative monitoring of blood glucose, more tightly targeted blood glucose control, and adjustment of insulin dosage prior to surgery. This study compared the efficacy of postoperative glycemic control and complications with the two protocols, CG and SG.
Patients and Methods: Three hundred and eighty type 2 diabetes patients who underwent elective surgeries were included in the study. Of those, 182 patients with CG were identified retrospectively as a historical control cohort. Additional 198 patients with SG were prospectively enrolled. Covariate imbalance was controlled using propensity score matching. Outcomes were evaluated using regression analysis clustered by type of surgery.
Results: The SG group had lower mean levels of postoperative 24-hr blood glucose than the CG group (β =− 8.6 mg/dL; 95% CI (− 16.5 to − 7.9), p=0.042). In SG group, the incidence of ICU admission and of acute kidney injury after surgery was lower than in the CG group (OR 0.36; 95% CI (0.18– 0.74), p=0.005 and OR=0.59; 95% CI (0.41– 0.85), p=0.005, respectively). There was no significant difference in postoperative hypoglycemia, infection, cardiovascular complications, stroke, or mortality rate between the two groups.
Conclusion: For type 2 diabetes patients undergoing elective surgery, the SG protocol is more effective in controlling blood glucose. The protocol can also reduce the incidence of some postoperative complications compared to CG with no increased risk of hypoglycemia.
Keywords: diabetes mellitus, perioperative management, blood glucose control protocol, postoperative complications
Introduction
Type 2 diabetes is a chronic disease that can lead to multiple complications in patients with long-term poorly controlled blood glucose levels.1 Complications include retinopathy, neuropathy, nephropathy and cardiovascular complications.1 The worldwide incidence of diabetes has risen from 108 million in 1980 to 422 million in 2014. In Thailand, the estimated prevalence of diabetes in adults in 2009 was 8.4%, rising to 9.6% in 2016.2,3 People with diabetes have a higher lifetime probability of undergoing surgery than those without diabetes.4 The frequent types of surgeries performed in diabetic patients include general surgery, colorectal surgery, vascular surgery and oncologic surgery.5
Suboptimal blood glucose control has been reported to be related to multiple adverse perioperative outcomes such as postoperative mortality, cardiovascular complications, stroke, infection, poor wound healing and prolonged length of hospital stay.6–8 Hyperglycemia is commonly documented in surgical patients. It has been reported that 20% to 40% of general surgery patients9 and 80% of heart surgery patients have hyperglycemia.10 Hypoglycemia has been reported to be a contributing factor for poor perioperative outcomes including arrhythmia, delirium, increased mortality rate and prolonged length of hospital stay.11 The risk of serious adverse perioperative outcomes in diabetic patients is increased if the blood glucose is not at the appropriate level, so maintaining blood glucose concentration at the optimal value can improve perioperative outcomes. A pilot study compared perioperative outcomes in diabetes patients who underwent cardiac surgery using the proposed glycemic control protocol combined with educational sessions on the standard care protocol.12 Compared to the standard care protocol, the proposed protocol better optimized blood glucose level postoperatively, but no significant difference in length of hospital stay or risk of infection was observed.12 Another study that compared the use of an intensive insulin management protocol and the standard protocol in cardiac surgery patients found lower blood glucose levels and lower risk of atrial fibrillation and postoperative infection with the intensive insulin management protocol.13 Data on the use of an optimized perioperative glucose control protocol and outcomes in general surgery, however, are still lacking.
Presently there are some inconsistencies in perioperative management such as differences in recommendations for discontinuing diabetes medications during the preoperative period, insulin adjustment strategies, target blood glucose ranges and postoperative blood glucose management. In our institution, the conventional perioperative glycemic control protocol (CG) has been routinely employed. However, this protocol has not been validated in general practice, includes a wide range of glycemic targets and provides no details regarding diabetes medications and insulin adjustment during the pre- and postoperative periods. In this study, a newly developed standardized glycemic control protocol (SG) which was designed and created by multiple committees and was intended to eliminate pitfalls of the current glycemic control protocol was evaluated. The present study compared the SG protocol and the CG protocol in terms of efficacy of postoperative glycemic control, incidence of hypoglycemia and clinical outcomes in diabetes patients who underwent a variety of elective surgeries.
Patients and Methods
This ambispective study was conducted between April and November 2019 in a tertiary medical care center in northern Thailand. The study protocol was approved by the Faculty of Medicine, Chiang Mai University, Ethical Committee (Ethical number: MED-2562-06286). All procedures were conducted in accordance with the ethical standards of the responsible committees on human experimentation (institutional and national) and with the Declaration of Helsinki 1975 as revised in 2008. The study involved comparing a prospective group with a historical control group. The control group of 182 patients was identified from a retrospective review of electronic medical records of diabetes patients who had undergone elective surgery with the CG protocol between April and August 2019. This control group was exempted from the informed consent requirements as this is a retrospective arm and all recorded data were kept confidential. Eligibility requirements for both groups included age ≥18 years, having type 2 diabetes and hospital admission for elective surgical procedures. The exclusion criteria were patients with type 1 diabetes, estimated glomerular filtration rate (eGFR) by CKD-EPI of <45 mL/min/1.73m2, emergency surgery and pregnancy. The prospective group included 198 diabetes patients who had elective surgery with the new SG protocol from September to November 2019. Individuals who meet all the inclusion criteria gave their informed consent. Baseline characteristics, including age, sex, body mass index (BMI), underlying diseases, diabetes complications, anti-diabetes agents used prior to surgery and type of surgery, were collected. Biochemical data prior to surgery, including HbA1c, fasting blood glucose, creatinine and LDL levels, were also acquired. Information regarding glycemic control, hypoglycemic events, insulin requirement, length of hospital stay, intensive care unit (ICU) admission and postoperative complications within seven days following surgery were collected. Data was also obtained on postoperative complications including organ infection, cardiovascular disease, stroke, acute kidney injury and health status at discharge. Types of surgery were classified as minor, moderate or major following the 2014 ESC/ESA guidelines on non-cardiac surgery.14
The SG protocol was developed through discussions among endocrinologist consultants and nurses from our hospital. The newly developed protocol is based on current guidelines for perioperative hyperglycemia management.15,16 The SG protocol consists of perioperative order sets for intravenous (IV) or subcutaneous (SC) insulin management and instructions for diabetes medication adjustment during the pre- and postoperative period (Supplementary Appendix). Introductory instruction was provided to the physicians, nurses, and anesthesiologists responsible for the patients’ care prior to the use of the SG protocol. The SG preoperative instructions were also provided to all SG patients.
Following the SG protocol, anti-diabetic agents, including metformin, sodium-glucose cotransporter 2 inhibitor (SGLT-2i) and glucagon-like peptide-1 receptor agonist (GLP-RA), were reviewed and medications were discontinued at least 24 hours before surgery; other medications were continued until the night before the surgery. For patients who used insulin, the dose of basal or premixed insulin was reduced to 80% of the usual dose; if a patient had a poor oral intake, was on bowel preparation, or on a liquid diet to prevent hypoglycemic events, insulin was reduced to 50% of the usual dose. Patients undergoing minor to moderate surgery with a short (<4 hours) operative time and who had HbA1c <8% and fasting blood glucose <250 mg/dL were candidates for SC insulin administration algorithms. Following the SC insulin algorithms, serial capillary blood glucose (CBG) was measured every 4 hours, with regular insulin administered subcutaneously if CBG was >180 mg/dL. During the postoperative period, patients who were unable to eat received regular insulin every 6 hours subcutaneously if CBG was >180 mg/dL (critical care ward) or >140 mg/dL (general ward). For patients who could eat but who had a reduced appetite, subcutaneous regular insulin was administered before meals. If a patient regained the ability to eat, antidiabetic medications were resumed. The IV insulin algorithms were introduced in patients undergoing procedures where hemodynamic changes were anticipated or where a major operation or surgeries with a longer operative time was planned. CBG was measured every 2 hours and intravenous insulin was administered if CBG was >180 mg/dL. A bolus followed by continuous infusion of regular insulin was administered and adjusted every 2 hours according to changes in CBG; the target CBG range was 140–180 mg/dL. During the postoperative period, patients who were unable to eat required continued intravenous insulin; for patients with a decreased appetite, switching to subcutaneous regular insulin was advised. On subsequent days, if the patient was able to eat, antidiabetic medications were resumed prior to discharge. The study flow for the prospective cohort with the SG protocol is shown in Figure 1. The CG protocol includes an algorithm only for intravenous insulin adjustment which is based on CBG and which has a wider target glycemic range (100–180 mg/dL) than the SG protocol. Moreover, the CG protocol provides no details regarding which oral medications need to be discontinued before surgery; the duration of discontinuation of those medications is also not clearly specified. Additionally, insulin dose reduction strategy prior to surgery is not mentioned in this CG protocol. In the CG protocol, oral glycemic agents and insulin dose adjustments are managed using an individualized approach by endocrinologists with no standard practice specified. Management during the postoperative period, including insulin dosage adjustment in patients with poor oral intake, hyperglycemic correction by subcutaneous regular insulin dose based on patients’ insulin resistance status and contraindications for restarting oral medications were not clearly specified in the previous CG protocol (Supplementary Appendix).
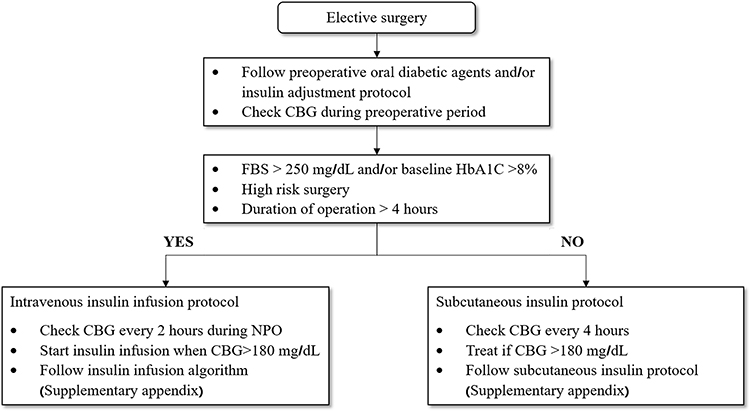 |
Figure 1 Study flow in standardized protocol group. Abbreviations: CBG, capillary blood glucose; FBS, fasting blood glucose; NPO, nothing per oral. |
The primary outcomes were the differences in the postoperative mean blood glucose levels in the first 24 hours after the operation and the number of hypoglycemic events (serum blood glucose and/or CBG <70 mg/dL) between CG and SG protocols. Secondary outcome included the occurrence of postoperative complications within the first seven days of the postoperative period.
Statistical Analysis
Statistical analysis was performed using STATA version 16.0. Continuous variables are presented as mean ±SD. Categorical variables are presented as counts and percentages. For continuous variables, univariable analysis was conducted with the independent t-test. For categorical variables, univariable analysis was conducted using the Fisher exact test. To control for covariate imbalance, propensity scores for sex, age, BMI, HbA1C, preoperative blood glucose level, duration and complications of diabetes and current insulin therapy were calculated. To compare outcomes between the two protocols, the propensity score covariate model was used by including the propensity score as one of the adjusted variables in the regression analysis model. The regression analysis was clustered by type of surgery (minor, moderate and major surgeries). For continuous outcomes, linear regression analysis with reported coefficient values was performed; for categorical outcomes, logistic regression analysis with reported odds ratio was used. The statistical significance level was defined as two-tailed with a p-value of <0.05. A sample size of at least 360 patients with at least 180 patients per arm was estimated to give 80% power at the 5% significance level (two-sided) to detect a difference of at least 10 mg/dL in pre- and postoperative blood glucose levels.17
Results
Baseline characteristics of the patients are shown in Table 1. Of the 380 patients, 198 were in the SG group and 182 were in the CG group. The mean age was 62.5 ±11.4 years, the mean duration of diabetes was 7 ±4.7 years and the mean HbA1C was 6.9 ±0.8%. Screening found most of the patients (82.4%) were being treated with metformin while 12% were being treated with insulin. Apart from diabetes retinopathy, which was more common in the SG group, demographic data showed no significant differences between the two groups. All patients in the CG group had received intravenous insulin infusions perioperatively, while in SG group only 89.3% of the patients had received perioperative insulin infusions (p= 0.001).
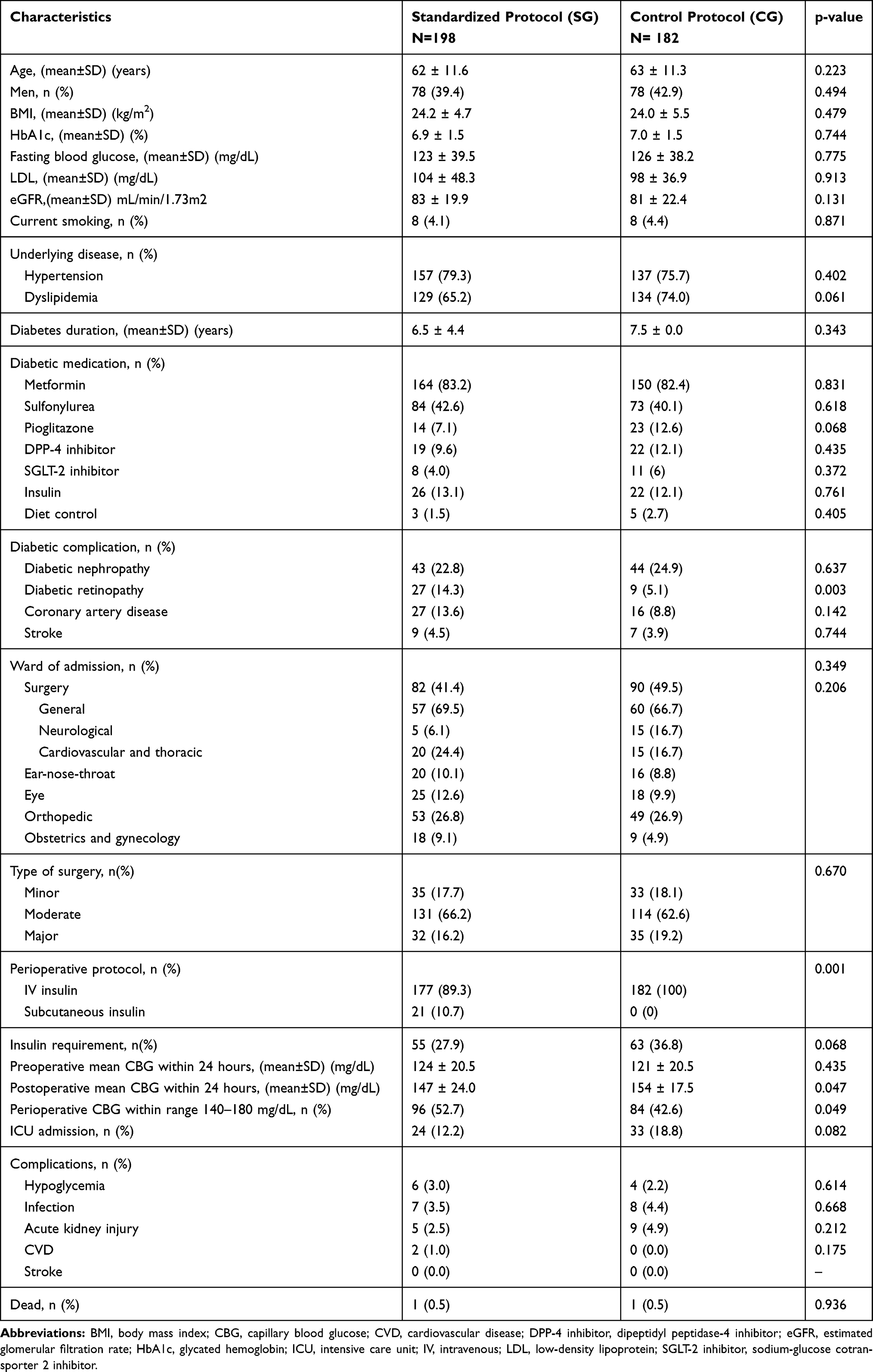 |
Table 1 Baseline Characteristics |
Preoperative blood glucose levels were similar in both groups. Preoperative mean blood glucose in the SG group was 124 ±20.5 mg/dL versus 121 ±20.5 mg/dL in the CG group (p=0.43). The SG group was associated with lower postoperative 24-hr blood glucose levels than the CG group (β = −8.6 mg/dL; 95% CI (−16.5 to −7.9), p=0.042) (Figure 2A). In SG group, there was a statistically higher number of patients with perioperative blood glucose in the range of 140–180 mg/dL compared to the CG group (OR 1.85; 95% CI (1.11–3.12), p=0.05). There was no significant difference in the incidence of postoperative hypoglycemic events between the SG and CG groups (OR 1.29; 95% CI (0.98–1.70), p=0.065).
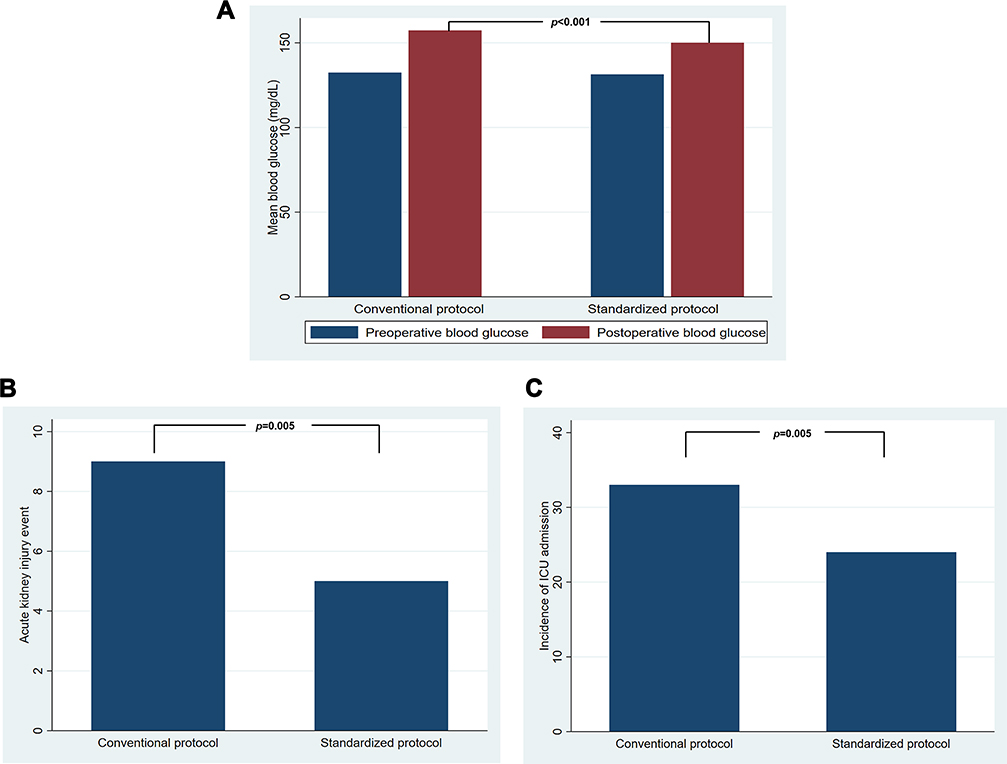 |
Figure 2 (A) Pre- and post-operative mean blood glucose difference between SG and CG. (B) postoperative acute kidney injury events within 7 postoperative days comparing between SG and CG. (C) incidence of ICU admission within 7 postoperative days comparing between SG and CG. |
In terms of postoperative complications within 7 days, the incidence of ICU admission and acute kidney injury in the SG group was lower than in the CG group (OR 0.36; 95% CI (0.18–0.74), p=0.005) and (OR=0.59; 95% CI (0.41–0.85), p=0.005), respectively (Figure 2B and C). There were no significant differences in other postoperative complications including organ infection, cardiovascular complications, stroke and death between the CG and the SG groups (Table 2).
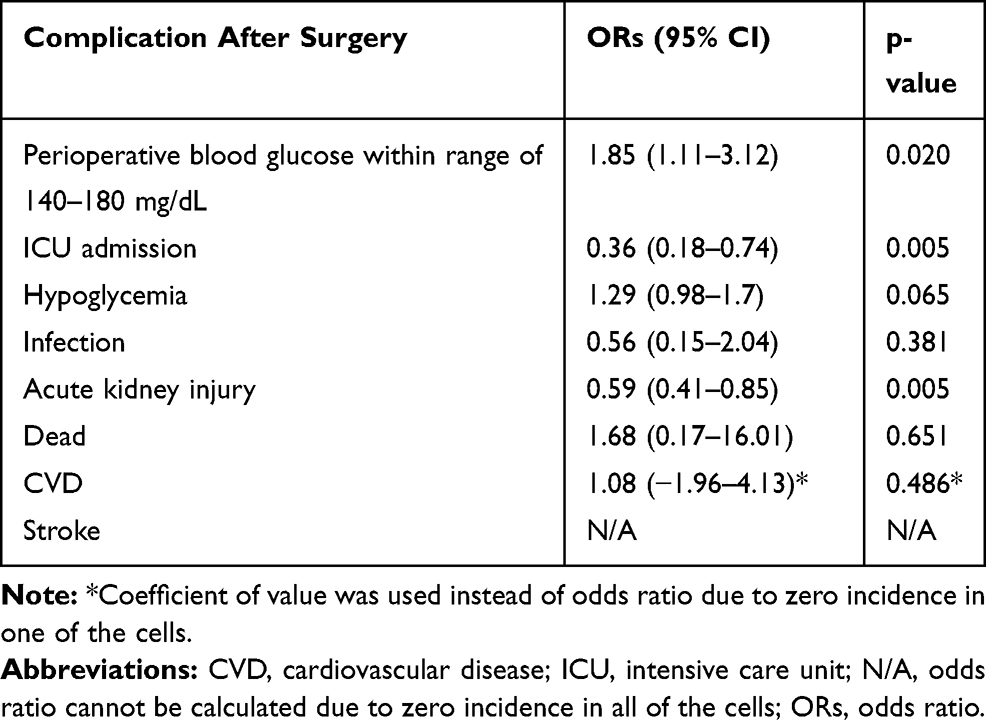 |
Table 2 Multivariable Logistic Regression Analysis of Outcomes Clustered by Type of Surgery and Adjusted by Propensity Score |
Discussion
The present study demonstrates that the proposed SG protocol for diabetes patients undergoing elective surgery showed non-inferiority in safety and greater efficiency in blood glucose control as well as resulting in better clinical outcomes than the CG protocol. Moreover, the subcutaneous regimen in the SG protocol for patients undergoing minor to moderate surgery with a short operative time and who have good blood glucose control offers benefits in terms of convenience and affordability as the use of an infusion pump and frequent CBG monitoring are not required. In the SG group, improvement in postoperative mean blood glucose during the first 24 hours following surgery was observed. A higher percentage of patients in the SG group had a blood glucose level within the desired range of 140–180 mg/dL. Additionally, there was no significant difference in the frequency of hypoglycemic events between the SG and CG groups, demonstrating the safety of the new protocol. The new management protocol was also associated with improvement in clinical outcomes postoperatively, including the incidence of ICU admission and acute kidney injury.
The presumptive explanation for the superior postoperative blood glucose control in the SG group is the comprehensive monitoring of blood glucose during the perioperative period, the frequent adjustments of insulin dose, the tight range of glycemic control and the comprehensive insulin transition strategy during the postoperative period. The observed results are in agreement with the findings of DiNardo et al which reported that the use of a standardized glycemic control protocol in patients with same-day surgery can result in lower postoperative blood glucose values with no increase in the risk of hypoglycemia.17 The present study found lower levels of blood glucose reduction than those reported by DiNardo et al (8.6 mg/dL versus 22.0 mg/dL). A factor that may have contributed to the different results is that the prior study reported a higher mean baseline blood glucose preoperatively (262–301 mg/dL) compared to the present study (around 120 mg/dL). That is, the magnitude of blood glucose reduction in the prior study may have been greater because of the initially higher baseline blood glucose. The desired range of blood glucose in the present study was 140–180 mg/dL. A higher percentage of patients managed with the SG protocol achieved this goal compared to the CG group. These results demonstrate the effectiveness of the new SG protocol, ie, that it helps reduce postoperative blood glucose levels at a suitable proportion, gradually bringing blood glucose within the ideal range.
There was no significant difference in the percentage of hypoglycemic events between the CG and SG protocols. This was an unexpected result as we had presumed that the more frequent blood glucose monitoring during the postoperative period and the fine insulin adjustment algorithm in the SG group would have provided superior glycemic control and a lower incidence of hypoglycemic events. As insulin treatment is a common risk factor for hypoglycemia in hospitalized patients,18 a plausible explanation for this finding is that the total dosage of insulin administered in the two groups was not statistically significantly different (p=0.06). The small number of insulin users in the study could also be a factor in this unexpected result.
The data regarding whether intensive blood glucose control during the perioperative period can reduce acute kidney injury events or not are still controversial.19 One prospective study reported that intensive blood glucose control to levels of less than 110 mg/dL during the perioperative period in cardiac surgery patients reduced the incidence of acute kidney injury by 41%.20 Another retrospective study of cardiac surgery patients stated that keeping blood glucose between 80 and 110 mg/dL was associated with a reduction in acute kidney injuries.21 However, a recent randomized clinical trial in critically ill surgical and non-surgical patients found that a blood glucose target of 180 mg/dL resulted in lower mortality than a target of 81–108 mg/dL, but that no difference in the incidence of acute kidney injury was observed.22 In the present study, the rate of acute kidney injury was 41% lower in the SG group despite the fact that the mean postoperative blood glucose in that group was higher than 110 mg/dL. That indicates reaching a lower target of blood glucose may not be the only explanation for the lower risk of acute kidney injury. The present study also found that the rate of ICU admissions moves in the same direction as the rate of acute kidney injuries. Specifically, in the CG group, the rate of ICU admissions was significantly associated with a higher risk of acute kidney injury (P<0.001, data not shown). Thus, it could be that the lower risk of acute kidney injury in the SG group could be a result of the lower rate of ICU admissions in that group.
To our knowledge, there have been no studies demonstrating a cause and effect relationship between the blood glucose control protocol during the perioperative period and ICU admissions. The imbalance in baseline characteristics in the present study, such as younger age, shorter duration of diabetes and fewer major surgeries performed in SG group, does not account for the lower rate of ICU admissions in SG group as the propensity score was included as one of the adjusted confounders in the multivariate model which was included to correct for any covariate imbalance. Further study of this issue is warranted. The NICE-SUGAR study showed that keeping blood glucose at less than 180 mg/dL but above 108 mg/dL can reduce mortality rates in critically ill surgical patients.22 The range of blood glucose levels in our study was comparable to that in the conventional arm of the NICE-SUGAR study which involved non-intensive blood glucose control. The present study found no difference in mortality rate between the SG and the CG protocols. The mortality rate in the present study was only 0.5% for both arms compared to approximately 20% in the NICE-SUGAR study.22 Differences in the studied populations might account for the dissimilar mortality rates.
A prior study reported that patients with blood glucose levels above 200 mg/dL perioperatively have an increased rate of infection.23 In the present study, there was no difference in the infection rate between the CG and SG groups because the postoperative mean blood glucose levels in both groups were below 200 mg/dL. The numbers of cardiovascular complication events and strokes in the present study were too low to detect differences in outcomes between the groups; we had not included those events in the sample size calculation. Further study with a larger sample should be performed to address this issue.
In March 2020, the US FDA announced that SGLT-2i should be discontinued at least 3 days prior to scheduled surgery to reduce the risk of ketoacidosis.24 This announcement was published after the SG protocol in this study had been developed and after the results of the study had been analyzed. The SG protocol used in this study did, however, advise that SGLT-2i should be discontinued at least 24 hours before surgery. As less than 10% of the patients in the present study were on this agent, this could be expected to have had only a small effect on outcomes. No incidents of ketoacidosis were observed during the present study; however, we recommend that the SG protocol should be updated to incorporate the new US FDA recommendations and suggest that additional analysis of future outcomes is warranted.
The present study had multiple strengths. The new SG protocol was developed by a group of experienced endocrinologists through a process of brainstorming meetings. Also, the protocol is “tailor-made”, ie, the new SG protocol provides for different types of surgeries, different diabetic agents, and different baseline blood glucose levels so each patient receives an individualized diabetes care. The large sample size in the present study provided an adequate power of analysis and the population recruited for the study included a mixture of patients with various types of surgeries, a wide range of baseline blood glucose levels and differences in the severity of their diabetes complications which aids in the application of the results to the general type 2 diabetes population. The unanticipated finding regarding the reduction in ICU admission rate, however, may warrant further study.
We acknowledge some limitations in this study. First, this was an ambispective study. The CG group was a retrospective case collection study; as a result, some data were found to be missing, although the amount of missing data was less than 5% which should not have affected the statistical power and outcomes. Second, this was not a randomized controlled trial study. To compensate, the propensity score of the covariate that could affect study outcomes was included as one of the adjusted confounders in multivariate analysis. Additionally, cluster analysis was conducted to minimize the effect of variation in type of surgery, reducing the imbalance of the covariate and increasing the reliability of the results. As this study included substantial modifications from the then-current CG protocol and also involved multiple concomitant intervention improvements, it is challenging to disambiguate the effect of each of those changes on the observed outcomes. Some of the minor surgeries allowed patients to eat on the day of the operation; thus, a complete record of blood glucose 24 hours postoperatively could not be achieved, introducing a level of inaccuracy in the data. Also, point-of-care capillary blood glucose rather than serum blood glucose values were obtained. That increased the convenience and reduced the cost of the study, although limitations of using this system have been described previously.25
Conclusion
In diabetes patients, the use of the SG protocol is feasible in the practical setting of elective surgery. This new protocol is safe and is effective in reducing mean blood glucose, ICU admission and the risk of acute kidney injury postoperatively. A large-scale, randomized control study is warranted to assess the impact of the SG protocol on the risk of infection, cardiovascular complications, stroke and mortality rates in diabetes patients following elective surgery.
Acknowledgments
The authors are grateful to Dr. G. Lamar Robert, PhD, and Dr. Chongchit S. Robert, PhD, for reviewing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Association AD. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2018. Diabetes Care. 2018;41(Supplement 1):S13–S27. doi:10.2337/dc18-S002
2. Aekplakorn W, Chariyalertsak S, Kessomboon P, et al. Prevalence and management of diabetes and metabolic risk factors in Thai adults: the Thai National Health Examination Survey IV, 2009. Diabetes Care. 2011;34(9):1980–1985. doi:10.2337/dc11-0099
3. Diabetes countries profiles. 2016. World Health Organization. Available from: https://www.who.int/diabetes/country-profiles/tha_en.pdf?ua=1.
4. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract. 2010;87(1):4–14. doi:10.1016/j.diabres.2009.10.007
5. Cruz NI, Santiago E, Abdul-Hadi A. Prevalence of diabetes mellitus in the surgical population of the University of Puerto Rico affiliated hospitals: a study using the surgery database. P R Health Sci J. 2016;35(3):160–164.
6. Association AD. Economic costs of diabetes in the US in 2012. Diabetes Care. 2013;36(4):1033–1046. doi:10.2337/dc12-2625
7. Moghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care. 2009;32(6):1119–1131. doi:10.2337/dc09-9029
8. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002;87(3):978–982. doi:10.1210/jcem.87.3.8341
9. Kwon S, Thompson R, Dellinger P, Yanez D, Farrohki E, Flum D. Importance of perioperative glycemic control in general surgery: a report from the surgical care and outcomes assessment program. Ann Surg. 2013;257(1):8. doi:10.1097/SLA.0b013e31827b6bbc
10. Umpierrez G, Cardona S, Pasquel F, et al. Randomized controlled trial of intensive versus conservative glucose control in patients undergoing coronary artery bypass graft surgery: GLUCO-CABG trial. Diabetes Care. 2015;38(9):1665–1672. doi:10.2337/dc15-0303
11. Kalra S, Bajwa SJ, Baruah M, Sehgal V. Hypoglycaemia in anesthesiology practice: diagnostic, preventive, and management strategies. Saudi J Anaesth. 2013;7(4):447–452. doi:10.4103/1658-354X.121082
12. Lee GA, Wyatt S, Topliss D, Walker KZ, Stoney R. A study of a pre-operative intervention in patients with diabetes undergoing cardiac surgery. Collegian. 2014;21(4):287–293. doi:10.1016/j.colegn.2013.06.001
13. Leibowitz G, Raizman E, Brezis M, Glaser B, Raz I, Shapira O. Effects of moderate intensity glycemic control after cardiac surgery. Ann Thorac Surg. 2010;90(6):1825–1832. doi:10.1016/j.athoracsur.2010.07.063
14. Members ATF, Kristensen SD, Knuuti J, et al. 2014 ESC/ESA guidelines on non-cardiac surgery: cardiovascular assessment and management: the joint task force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J. 2014;35(35):2383–2431. doi:10.1093/eurheartj/ehu282
15. Udovcic M, Castro JC, Apsey HA, Stearns JD, Schlinkert RT, Cook CB. Guidelines to improve perioperative management of diabetes mellitus: assessment of the impact of change across time. Endocrine Pract. 2015;21(9):1026–1034. doi:10.4158/EP15690.OR
16. Duggan EW, Carlson K, Umpierrez GE. Perioperative hyperglycemia management an update. Anesthesiology. 2017;126(3):547–560. doi:10.1097/ALN.0000000000001515
17. DiNardo M, Donihi A, Forte P, Gieraltowski L, Korytkowski M. Standardized glycemic management and perioperative glycemic outcomes in patients with diabetes mellitus who undergo same-day surgery. Endocrine Pract. 2011;17(3):404–411. doi:10.4158/EP10316.OR
18. Hulkower RD, Pollack RM, Zonszein J. Understanding hypoglycemia in hospitalized patients. Diabetes Manage. 2014;4(2):165. doi:10.2217/dmt.13.73
19. Alsabbagh MM, Asmar A, Ejaz NI, Aiyer RK, Kambhampati G, Ejaz AA. Update on clinical trials for the prevention of acute kidney injury in patients undergoing cardiac surgery. Am J Surg. 2013;206(1):86–95. doi:10.1016/j.amjsurg.2012.08.007
20. van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345(19):1359–1367. doi:10.1056/NEJMoa011300
21. Lecomte P, Van Vlem B, Coddens J, et al. Tight perioperative glucose control is associated with a reduction in renal impairment and renal failure in non-diabetic cardiac surgical patients. Critical Care. 2008;12(6):R154. doi:10.1186/cc7145
22. Finfer S, Chittock DR, Su SY, et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360(13):1283–1297.
23. Ata A, Lee J, Bestle SL, Desemone J, Stain SC. Postoperative hyperglycemia and surgical site infection in general surgery patients. Arch Surg. 2010;145(9):858–864. doi:10.1001/archsurg.2010.179
24. Communication FDS. FDA revises labels of SGLT2 inhibitors for diabetes to include warnings about too much acid in the blood and serious urinary tract infections. 2020. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-revises-labels-sglt2-inhibitors-diabetes-include-warnings-about-too-much-acid-blood-and-serious.
25. Rice MJ, Pitkin AD, Coursin DB. Review article: glucose measurement in the operating room: more complicated than it seems. Anesth Analg. 2010;110(4):1056–1065. doi:10.1213/ANE.0b013e3181cc07de
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.