Back to Journals » Drug Design, Development and Therapy » Volume 19
Standardized Ginkgo Biloba Extract (EGb 761) for Knee Osteoarthritis: A Narrative Review
Authors Wang Y ![]() , Liu Z
, Liu Z ![]() , Liu Y
, Liu Y ![]() , Chu H
, Chu H ![]()
Received 30 June 2025
Accepted for publication 5 December 2025
Published 16 December 2025 Volume 2025:19 Pages 11217—11225
DOI https://doi.org/10.2147/DDDT.S550540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tamer Ibrahim
Yunqing Wang,1,2 Ziyu Liu,1,2 Yong Liu,1 Hongshang Chu1,3
1Department of Traumatic Orthopedics, Affiliated Hospital of Shandong Second Medical University, Weifang, 261031, People’s Republic of China; 2School of Clinical Medicine, Shandong Second Medical University, Weifang, 261053, People’s Republic of China; 3Clinical Research Center, Affiliated Hospital of Shandong Second Medical University, Weifang, 261042, People’s Republic of China
Correspondence: Hongshang Chu, Email [email protected] Yong Liu, Email [email protected]
Abstract: Knee osteoarthritis (KOA), a prevalent degenerative joint disorder characterized by progressive cartilage degradation, synovial inflammation, and joint dysfunction, remains a major cause of disability worldwide with limited therapeutic options. Ginkgo biloba extract (EGb 761), a standardized multi-component natural product containing flavonoid glycosides and terpene lactones, has demonstrated anti-inflammatory, antioxidant, anti-apoptotic, and Chondroprotection. This narrative review synthesizes current experimental and clinical findings on the potential therapeutic role of EGb 761 in KOA. To provide a comprehensive overview, relevant literature published up to 2025 was identified through searches in PubMed, Scopus, and Web of Science, as well as by screening reference lists of key studies. Considering the complex pathogenesis of KOA and the multi-target pharmacological actions of EGb 761, this review aims to consolidate existing findings and clarify its potential role as an adjunctive therapy. Preclinical and clinical studies suggest that EGb 761 may reduce inflammation, oxidative stress, and chondrocyte apoptosis, leading to modest improvements in pain relief and joint function, while demonstrating a favorable safety profile. However, current evidence is limited by small sample sizes, methodological heterogeneity, short study durations, and risk of bias. While the available evidence is promising, it remains inconclusive that EGb 761 offers significant therapeutic benefits for individuals with KOA. Further high-quality randomized controlled trials are warranted.
Keywords: ginkgo biloba extract, EGb 761, knee osteoarthritis, KOA, efficacy and therapeutic effect
Introduction
Osteoarthritis (OA) is a multifactorial joint disorder primarily affecting weight-bearing joints, characterized by intractable chronic joint pain that significantly impairs patients’ mobility and diminishes their quality of life.1 Among the various subtypes of OA, KOA has emerged as a focal point in clinical research due to its high disability rate.2 Not only does KOA substantially reduce patients’ quality of life, but it also poses a significant global public health challenge exacerbated by the increasing trend of population aging.3 Furthermore, the disease burden is further complicated by surgical interventions, which while effective for symptom management, present their own set of clinical limitations. Current treatment strategies encompass pharmacological approaches, including intra-articular injections or oral administration of glucocorticoids, paracetamol, or viscoelastic supplements, as well as surgical options such as arthroplasty and tissue engineering.4,5 However, existing therapies exhibit universal limitations: pharmacological interventions provide only transient symptomatic relief, while prosthetic implants face clinical challenges including their limited service life.6
The EGb 761, prepared through a “dual adsorption-elimination” process, represents a promising therapeutic avenue. This formulation is enriched with bioactive components, including flavonoid glycosides and terpene trilactones, which contribute to its multifaceted therapeutic effects. These include lipid metabolism regulation, free radical scavenging, and inflammatory cascade suppression.7 Recent investigations have underscored the growing therapeutic significance of EGb 761 in diverse domains, ranging from neuroprotection and oxidative stress modulation and oxidative stress modulation to articular inflammation alleviation.8–10
Although EGb 761 has demonstrated therapeutic potential across a variety of diseases,8 its application in KOA remains in the preliminary stages of investigation. The current body of evidence is limited and heterogeneous, with most studies involving small sample sizes, short follow-up durations, and inconsistent clinical outcomes.11 Moreover, relatively few studies have explicitly identified the use of the EGb 761, as opposed to non-standardized Ginkgo biloba preparations, which are known to differ substantially in composition, bioactivity, and pharmaceutical quality. This lack of specification may compromise the reliability, reproducibility, and translational relevance of existing findings.12
Therefore, this review aims to summarize and critically appraise the current evidence regarding the therapeutic potential of the EGb 761 in KOA, with a particular focus on its anti-inflammatory, anti-oxidant, anti-apoptotic, and chondroprotection mechanisms.
The Epidemiological Characteristics of KOA
OA is a degenerative disease characterized by three core pathological features: progressive destruction of articular cartilage, inflammatory responses in synovial tissue, and structural degeneration of joints. It predominantly affects the weight-bearing joints of the lower extremities that are subject to substantial biomechanical loading.10,13–15 Metabolic dysregulation of the cartilage matrix, inflammatory imbalance within the synovial microenvironment, and persistent pain constitute its core clinical features. The multifactorial pathogenesis of OA involves aberrant mechanical loading, metabolic dysfunction, and genetic susceptibility.6,16–18 Key pathological processes include subchondral bone remodeling, excessive secretion of synovial inflammatory mediators, and loss of extracellular matrix (ECM) integrity, ultimately leading to chronic pain and joint dysfunction.19 KOA, the most prevalent subtype, presents with knee pain, swelling, morning stiffness, and restricted movement.2 Pain-induced immobility exacerbates muscle atrophy and joint instability, creating a vicious cycle of pain, dysfunction, and progressive structural damage.18,20–22 In China, KOA accounts for 14.6% of all OA cases. With the aging population, the disease burden associated with KOA is expected to continue increasing.6,16,23,24 Current management strategies for KOA follow a tiered pharmacologic framework. Topical nonsteroidal anti-inflammatory drugs (NSAIDs) are recommended as first-line therapy for mild-to-moderate symptoms. Refractory cases may require oral analgesics, intra-articular corticosteroids, or other injection therapies for temporary relief.25–27 When conservative management fails, surgical interventions such as arthroplasty or arthrodesis are performed to restore joint function and alleviate chronic pain.4
Despite these strategies, current therapeutic modalities exhibit significant limitations in both symptom alleviation and disease progression retardation.6,10 Consequently, advancing our understanding of the underlying pathogenesis and developing more efficacious therapeutic approaches have become critical challenges in contemporary medical research.
The Historical Medicinal Value of Ginkgo and Modern Extract Research
Traditional Chinese Medicine (TCM), as a holistic medical system with over two millennia of clinical practice, has demonstrated therapeutic efficacy validated through multiple dimensions.28 The advancement of modern research technologies has catalyzed the establishment of the TCM Integrated Database (TCMID) and the Systems Pharmacology Platform (TCMSP), providing novel research paradigms for deciphering the molecular targets of herbal formulations.29 In OA management, TCM has developed distinctive intervention strategies, including bone metabolism regulation using Cornus officinalis,30 and anti-inflammatory formulations derived from Carthamus tinctorius.31 Herbal preparations, such as compound formulations containing artificial tiger bone powder and Psammosilene tunicoides components, have shown promise in analgesia and disease progression retardation.32–34 However, their underlying molecular mechanisms and long-term therapeutic outcomes and safety profiles still require rigorous evidence-based validation through well-designed preclinical and clinical studies.
Ginkgo biloba, a “living fossil” in the plant kingdom, has its medicinal value systematically recorded as early as the Song Dynasty in the “Shennong Bencao Tujing”. Subsequent classic medical texts such as Li Shizhen’s “Compendium of Materia Medica” and Wang Ang’s “Bencao Fengyuan” further refined its clinical application system.35 As the sole extant representative of the Ginkgoaceae family, Ginkgo biloba’s ecological continuity is attributed to its robust environmental adaptability, pest and disease resistance, as well as close associations with religious/cultural conservation practices.36 Modern pharmacological research has identified over 60 bioactive compounds in standardized Ginkgo biloba extracts, including flavonoids (approximately 24%) and terpenoid lactones (about 6%), which are considered the primary active constituents. Additionally, the leaves contain organic acids, proanthocyanidins, tannins, sitosterols, carotenoids, polysaccharides, glucose, minerals, vitamins, and other bioactive compounds.37 Notably, 10 characteristic diterpene lactones, collectively referred to as ginkgolides (including Ginkgolide A(GA), Ginkgolide B(GB), Ginkgolide C(GC), Ginkgolide J(GJ)) have been isolated and characterized from the terpenoid fraction.38
EGb 761, a widely used standardized Ginkgo biloba extract, has been extensively studied for its pharmacological properties. It is derived from Ginkgo leaves and standardized to contain 24% ginkgo-flavone glycosides and 6% terpenoid lactones with the following major constituents (greater than 0.1%):flavonol monoglycosides (eg, quercetin-3-0-glucoside, quercetin-3-0-rhamnoside, and 30-0-methylmyricetin-3-0 glucoside), flavonol diglycosides, flavonol triglycosides, coumaric esters of flavonol diglycosides, flavonoidic compounds, terpenes (eg, BB, GA, GB, GC,GJ), organic acids, and steroids.39–41 The flavonoid glycosides are primarily composed of quercetin, kaempferol, and isorhamnetin glycosides. The terpene trilactones are primarily composed of bilobalide, Ginkgolides A, B, C, and J.42 Flavonoid glycosides are the major constituents of EGb 761 and are well known to be an antioxidant for inhibiting tumor growth, also has anti-aging, anti-cancer, anti-inflammatory, anti-microbial, cardioprotective, neuroprotective, and UV-protective effects and so on.42
Unlike non-standardized Ginkgo preparations, EGb 761 is manufactured through tightly controlled processes, ensuring batch-to-batch consistency, stability, and safety.43 Its production involves innovative separation and purification technologies, supported by a stringent quality control system that ensures the purity, stability, and clinical efficacy of its active constituents. These features contribute to its superior safety and therapeutic performance compared to non-standardized extracts.43 Its pharmacological profile includes potent antioxidant and neuroprotective effects, mediated through free radical scavenging, mitochondrial protection, and modulation of signaling pathways.44 While EGb 761 has been most thoroughly studied in neurodegenerative disorders such as dementia, Alzheimer’s disease, and stroke,45–50 growing preclinical data support its relevance in OA, which including KOA.51
EGb 761 and its main bioactive components—flavonoids and ginkgolides—exert anti-inflammatory, antioxidant, and anti-apoptotic effects through preservation of mitochondrial function52–55 (Table 1). These mechanisms help protect chondrocytes, reduce synovial inflammation, and preserve ECM integrity.10,51
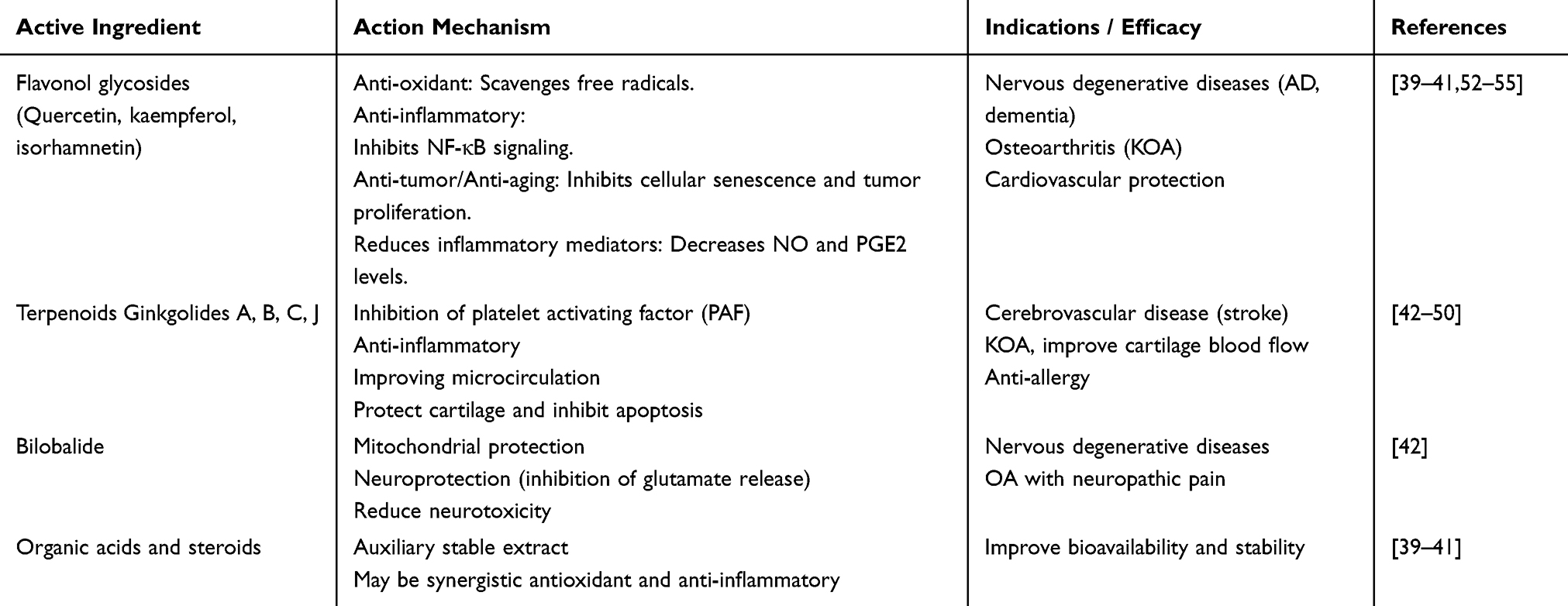 |
Table 1 The Main Active Ingredients and Functions of EGb 761 |
Although clinical trials in KOA are limited, EGb 761 has been safely used for decades, with a well-characterized pharmacological profile. Its pleiotropic properties offer promising therapeutic potential for KOA, warranting further clinical investigation.
The Therapeutic Potential of EGb 761 in KOA
EGb 761 has garnered significant attention due to its mechanisms of action aligning closely with the pathological features of KOA. EGb 761 may attenuate joint degeneration through anti-inflammatory, anti-apoptotic, and antioxidant mechanisms, thereby providing a theoretical foundation for its potential application in the treatment of joint diseases51,56–58 (Figure 1).
 |
Figure 1 The multiple action mechanisms of EGb 761 in KOA. |
Anti-Inflammatory Effect and Anti-Apoptotic Effect
EGb 761 has been shown to inhibit the release of inflammatory mediators such as tumor necrosis factor-alpha (TNF-α) and interleukin-1β (IL-1β), thereby alleviating arthritis symptoms, reducing pain and swelling in patients with KOA, and improving joint function.59,60 Studies have demonstrated that EGb 761 protects chondrocytes from IL-1β-induced damage and significantly downregulates the expression of key inflammatory markers, including inducible nitric oxide synthase (iNOS), cyclooxygenase-2 (COX-2), and TNF-α.58,61 EGb 761 not only suppresses the production of inflammatory mediators by downregulating these markers but also modulates immune responses by promoting apoptosis of effector T cells, thereby reducing excessive immune activation and the risk of chronic inflammation.62
Moreover, EGb 761 decreases the levels of prostaglandin E2 (PGE2) and nitric oxide (NO) in the bloodstream, attenuates histopathological changes, and inhibits the expression of COX-2 and nitrotyrosine in cartilage, thereby exerting anti-inflammatory effects on both human articular chondrocytes and OA animal models.10 Additionally, EGb 761 reduces the expression of phosphorylated nuclear factor κB p65 (p-NF-κB p65) and prevents TNF-α-induced activation of the NF-κB pathway in human chondrocytes, which is the mechanism essential for mitigating joint inflammation.63
Given the pharmacological profile of EGb 761 and the inflammatory nature of OA pathogenesis, this extract shows strong potential in modulating inflammatory responses in KOA. Together, these findings suggest EGb 761 may modulate both local inflammation and systemic immune activation in KOA.
In addition to its anti-inflammatory role, EGb 761 exhibits anti-apoptotic properties that contribute to cartilage preservation. It attenuates TNF-α-induced apoptosis in osteoarthritic chondrocytes by preserving mitochondrial membrane potential and modulating apoptotic regulators such as increasing Bcl-2 expression and inhibiting caspase-3 activity.10,64–66 Moreover, EGb 761 reduces the expression of matrix-degrading enzymes including matrix metalloproteinases (MMP-1, MMP-3, and MMP-13), and inhibits type II collagen breakdown, highlighting its anti-catabolic potential in OA.51
Anti-Oxidative Stress
Oxidative stress plays a pivotal role in the progression of KOA, contributing to chondrocyte dysfunction, ECM degradation, and mitochondrial impairment.67 EGb 761 exhibits potent antioxidant activity, as demonstrated in various preclinical models. It enhances endogenous antioxidant defenses by upregulating key enzymes such as superoxide dismutase (SOD), glutathione peroxidase (GPx), and catalase (CAT), which are essential for the neutralization of reactive oxygen species (ROS).68,69
In addition, EGb 761 reduces levels of malondialdehyde (MDA) while increasing the activity of glutathione (GSH) and SOD. In erythrocyte models, it counteracts hydrogen peroxide (H2O2)-induced oxidative injury by preserving membrane cytoskeletal integrity. In KOA chondrocytes, ROS accumulation contributes to cellular dysfunction, and EGb 761 may exert protective effects via similar antioxidative pathways.70
Furthermore, EGb 761 stabilizes mitochondrial membrane potential and attenuates oxidative stress-induced apoptosis. As mitochondrial dysfunction is a major contributor to cartilage degeneration in KOA, EGb 761 may delay chondrocyte death by preserving mitochondrial energy metabolism.8
Taken together, these findings support the antioxidative potential of EGb 761 in joint tissues, although most mechanistic data to date derive from preclinical studies. Further investigation is needed to determine whether these antioxidant effects translate into clinical benefits for KOA patients.
Chondroprotection
Though direct data in KOA remain limited, EGb 761 is known neuroprotective actions—such as inhibition of oxidative stress-induced apoptosis and mitochondrial dysfunction—suggest overlapping mechanisms that may be relevant in joint tissues.64 EGb 761 exerts neuroprotective effects on both sensory and motor neurons following peripheral nerve injury,71,72 which may contribute to the alleviation of OA-related neuropathic pain and thereby improve patient symptoms. Additionally, EGb 761 has been shown to inhibit glutamate release, potentially reducing neuroexcitotoxicity and indirectly protecting periarticular tissues from excitotoxic damage73 (Figure 2). These findings support its potential role in delaying cartilage degeneration by targeting shared apoptotic and oxidative stress pathways implicated in KOA progression.
 |
Figure 2 The chondroprotection, antioxidant, anti-apoptotic, and anti-inflammatory mechanisms of EGb 761.Red arrows: Indicating an increase or decrease. Black arrows: Indicating signal pathway direction. |
In addition to its neuroprotective actions, EGb 761 exerts direct chondroprotective effects. In an in vitro–in vivo study, EGb 761 significantly attenuated inflammatory responses in human articular chondrocytes stimulated with lipopolysaccharide (LPS) or IL‑1β, as evidenced by reductions in PGE2 and NO production, alongside downregulation of COX‑2, iNOS, Toll-like receptor 4 (TLR4)/tumor necrosis factor receptor-associated factor 6 (TRAF6), and nuclear factor‑κB (NF‑κB) signaling. Consistently, in a rat model of OA, systemic administration of EGb 761 led to decreased circulating levels of PGE2 and NO, improved cartilage histopathological scores, and reduced COX‑2 and nitrotyrosine immunoreactivity in joint tissues. These findings suggest that EGb 761 protects cartilage by modulating pro-inflammatory mediators and preserving structural integrity in the osteoarthritic joint.10,58
Safety and Drug Interactions
EGb 761 is generally regarded as safe and well-tolerated when administered at recommended therapeutic doses. Its safety profile is supported by decades of clinical use and extensive pharmacovigilance data. Reported adverse effects are typically mild and transient, including gastrointestinal discomfort, headache, dizziness, skin allergies, elevated blood pressure, and occasional respiratory tract infections.74 Most adverse events have been documented in case reports involving doses ranging from 80 to 150 mg/day for treatment durations spanning from one week to one year, often in patients with comorbidities or those concurrently using other medications.41
Notably, several case studies have raised concerns regarding bleeding abnormalities potentially associated with Ginkgo biloba, including postoperative hemorrhage and increased bleeding risk during anticoagulant therapy75 These effects are thought to be mediated by ginkgolides and bilobalide—constituents of EGb 761—which function as Platelet-Activating Factor (PAF) receptor antagonists. Although the absolute risk remains low, clinicians should exercise caution when EGb 761 is used concomitantly with anticoagulants (eg, warfarin), antiplatelet agents (eg, aspirin, clopidogrel), or nonsteroidal NSAIDs, especially in elderly individuals or those undergoing surgical procedures.76
Conclusion
KOA is a multifactorial degenerative disease with complex pathogenesis involving inflammation, oxidative stress, chondrocyte apoptosis, and ECM degradation. Current treatment strategies remain limited, prompting the search for novel adjunctive therapies. EGb 761, exhibits multiple pharmacological activities—including anti-inflammatory, antioxidant, anti-apoptotic, and chondroprotective effects—supported by extensive preclinical research.59,60
However, the clinical evidence for EGb 761 in KOA remains limited. Only a small number of randomized trials have been conducted, with small sample sizes, variable designs, short follow-up durations, and inconsistent outcome measures. Most mechanistic insights stem from in vitro or animal models, and their translation into clinical benefit is not yet established. While safety data appear generally favorable, they are mostly derived from non-OA populations, and long-term safety in OA patients remains insufficiently characterized.75
Therefore, EGb 761 should not yet be considered a practice-changing intervention for KOA. Instead, it represents a hypothesis-generating candidate that warrants further investigation. Future studies should employ standardized EGb 761 formulations, include adequately powered randomized controlled trials with prespecified pain and functional outcomes, long-term follow-up, and systematic safety reporting—including drug interaction monitoring—especially in elderly OA populations. A more robust evidence base is required before EGb 761 can be recommended for routine use in KOA management.
Abbreviations
KOA, Knee osteoarthritis; EGb 761, Ginkgo biloba extract; OA, Osteoarthritis; ECM, Extracellular Matrix; NSAIDs, Nonsteroidal anti-inflammatory drugs; TCM, Traditional Chinese Medicine; TCMID, TCM Integrated Database; TCMSP, TCM Systems Pharmacology Platform; BB, Bilobalide; GA, Ginkgolide A; GB, Ginkgolide B; GC, Ginkgolide C; GK, Ginkgolide K; GJ, Ginkgolide J; TNF-α, Tumor Necrosis Factor-alpha; IL-1β, Interleukin-1β; iNOS, Inducible Nitric Oxide Synthase; PGE2, Prostaglandin E2; COX-2, Cyclooxygenase-2; NO, nitric oxide; P-NF-ΚB P65, Phosphorylated Nuclear Factor ΚB P65; MMps, Matrix Metalloproteinases; SOD, Superoxide Dismutase; Gpx, Glutathione Peroxidase; CAT, Catalase; ROS, Reactive Oxygen Species; MDA, Malondialdehyde; GSH, Glutathione; H2O2, hydrogen peroxide; LPS, Lipopolysaccharide; TLR4, tumor Toll-like receptor 4; TRAF6, necrosis factor receptor-associated factor 6; NF‑κB, nuclear factor‑κB; PAF, Platelet-Activating Factor.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Scientific Research Foundation for doctoral of Affiliated Hospital of Shandong Second Medical University (2024BSQD08),Taishan Scholars Project of Shandong Province (tsqnz20240857), and Shandong Second Medical University Affiliated Hospital (Teaching Hospital) Scientific Research Development Fund Project (2025FYQ001) to H.C.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu D, Cai Z-J, Yang Y-T, et al. Mitochondrial quality control in cartilage damage and osteoarthritis: new insights and potential therapeutic targets. Osteoarthritis Cartilage. 2022;30(3):395–405. doi:10.1016/j.joca.2021.10.009
2. Bin L. Progress in Traditional Chinese Medicine Treatment of Knee Osteoarthritis. Yunnan J Trad Chin Med Mater Med. 2024;45(11):93–97.
3. Hodgkinson T, Kelly DC, Curtin CM, et al. Mechanosignalling in cartilage: an emerging target for the treatment of osteoarthritis. Nat Rev Rheumatol. 2022;18(2):67–84. doi:10.1038/s41584-021-00724-w
4. Kan HS, Chan PK, Chiu KY, et al. Non-surgical treatment of knee osteoarthritis. Hong Kong Med J. 2019;25(2):127–133. doi:10.12809/hkmj187600
5. da Costa BR, Pereira TV, Saadat P, et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and Hip osteoarthritis: network meta-analysis. BMJ. 2021;375:n2321. doi:10.1136/bmj.n2321
6. Katz JN, Arant KR, Loeser RF. Diagnosis and treatment of hip and knee osteoarthritis: a review. JAMA. 2021;325(6):568–578. doi:10.1001/jama.2020.22171
7. Jiang X. Research progress on anti-inflammatory active ingredients and action mechanisms of ginkgo biloba leaf extracts. J Pharm Res. 2024;43(05):473–479.
8. Singh SK, Srivastav S, Castellani RJ, et al. Neuroprotective and antioxidant effect of ginkgo biloba extract against ad and other neurological disorders. Neurotherapeutics. 2019;16(3):666–674. doi:10.1007/s13311-019-00767-8
9. Wan W, Zhang C, Danielsen M, et al. EGb761 improves cognitive function and regulates inflammatory responses in the APP/PS1 mouse. Exp Gerontol. 2016;81:92–100. doi:10.1016/j.exger.2016.05.007
10. Chen YJ, Tsai KS, Chiu CY, et al. EGb761 inhibits inflammatory responses in human chondrocytes and shows chondroprotection in osteoarthritic rat knee. J Orthop Res. 2013;31(7):1032–1038. doi:10.1002/jor.22339
11. Al-Haddad M, Bairam A, Hussain H, Majeed S, Al-Jalehawi A. Evaluation of clinical efficacy of Ginkgo biloba extract in the treatment of knee osteoarthritis: a randomized clinical trial. F1000Research. 2022;11.
12. Kulic Z, Lehner MD, Dietz GPH. Ginkgo biloba leaf extract EGb 761((R)) as a paragon of the product by process concept. Front Pharmacol. 2022;13:1007746. doi:10.3389/fphar.2022.1007746
13. Nelson AE. Osteoarthritis year in review 2017: clinical. Osteoarthritis Cartilage. 2018;26(3):319–325. doi:10.1016/j.joca.2017.11.014
14. Mabey T, Honsawek S. Cytokines as biochemical markers for knee osteoarthritis. World J Orthop. 2015;6(1):95–105. doi:10.5312/wjo.v6.i1.95
15. Bortoluzzi A, Furini F, Scire CA. Osteoarthritis and its management - Epidemiology, nutritional aspects and environmental factors. Autoimmun Rev. 2018;17(11):1097–1104. doi:10.1016/j.autrev.2018.06.002
16. Vina ER, Kwoh CK. Epidemiology of osteoarthritis: literature update. Curr Opin Rheumatol. 2018;30(2):160–167. doi:10.1097/BOR.0000000000000479
17. Rice SJ, Beier F, Young DA, et al. Interplay between genetics and epigenetics in osteoarthritis. Nat Rev Rheumatol. 2020;16(5):268–281. doi:10.1038/s41584-020-0407-3
18. Zhang Z, Schon L. The current status of clinical trials on biologics for cartilage repair and osteoarthritis treatment: an analysis of clinicaltrials.gov data. Cartilage. 2022;13(2):19476035221093065. doi:10.1177/19476035221093065
19. Zhu J. Research progress on pain mechanisms of osteoarthritis and treatment with related traditional chinese medicines. J. Xinxiang Med. Univ. 2024;41(10):996–1000.
20. Glyn-Jones S, Palmer AJR, Agricola R, et al. Osteoarthritis. Lancet. 2015;386(9991):376–387. doi:10.1016/S0140-6736(14)60802-3
21. Carlson AK, Rawle RA, Wallace CW, et al. Characterization of synovial fluid metabolomic phenotypes of cartilage morphological changes associated with osteoarthritis. Osteoarthritis Cartilage. 2019;27(8):1174–1184. doi:10.1016/j.joca.2019.04.007
22. Li D, Li S, Chen Q, et al. The prevalence of symptomatic knee osteoarthritis in relation to age, sex, area, region, and body mass index in china: a systematic review and meta-analysis. Front Med. 2020;7:304. doi:10.3389/fmed.2020.00304
23. Allen KD, Thoma LM, Golightly YM. Epidemiology of osteoarthritis. Osteoarthritis Cartilage. 2022;30(2):184–195. doi:10.1016/j.joca.2021.04.020
24. Minnig MCC, Golightly YM, Nelson AE. Epidemiology of osteoarthritis: literature update 2022-2023. Curr Opin Rheumatol. 2024;36(2):108–112. doi:10.1097/BOR.0000000000000985
25. Guideline for the Diagnosis and Treatment of Osteoarthritis (2007 Edition). Chin. J. Orthop Surg. 2014;22(03):287–288.
26. Hochberg MC, Altman RD, April KT, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, Hip, and knee. Arthritis Care Res. 2012;64(4):465–474. doi:10.1002/acr.21596
27. da Costa BR, Nüesch E, Kasteler R, et al. Oral or transdermal opioids for osteoarthritis of the knee or Hip. Cochrane Database Syst Rev. 2014;2014(9):CD003115. doi:10.1002/14651858.CD003115.pub4
28. Tang G, Li S, Zhang C, et al. Clinical efficacies, underlying mechanisms and molecular targets of Chinese medicines for diabetic nephropathy treatment and management. Acta Pharm Sin B. 2021;11(9):2749–2767. doi:10.1016/j.apsb.2020.12.020
29. Xue R, Fang Z, Zhang M, et al. TCMID: traditional Chinese Medicine integrative database for herb molecular mechanism analysis. Nucleic Acids Res. 2013;41:D1089–95. doi:10.1093/nar/gks1100
30. Yu H, Yao S, Zhou C, et al. Morroniside attenuates apoptosis and pyroptosis of chondrocytes and ameliorates osteoarthritic development by inhibiting NF-kappaB signaling. J Ethnopharmacol. 2021;266:113447. doi:10.1016/j.jep.2020.113447
31. Wang C, Gao Y, Zhang Z, et al. Safflower yellow alleviates osteoarthritis and prevents inflammation by inhibiting PGE2 release and regulating NF-kappaB/SIRT1/AMPK signaling pathways. Phytomedicine. 2020;78:153305. doi:10.1016/j.phymed.2020.153305
32. Jiangang C. Clinical study on jintiange capsule in the treatment of knee osteoarthritis. Chin. J. Osteoporos. 2015;21(01):84–87.
33. Ruan Haijun ZD, Fengwei L. 40 cases of osteoarthritis treated with jingu lian capsule. Clin J Chin Med. 2016;8(21):68–69.
34. Tang K, Sun J, Dong Y, et al. Topical Chinese patent medicines for chronic musculoskeletal pain: systematic review and trial sequential analysis. BMC Musculoskelet Disord. 2023;24(1):985. doi:10.1186/s12891-023-07072-8
35. Yang Yang ZB, Wenjie Z. A history of ginkgo biloba leaves: a paradigm for research and development of traditional chinese medicine/phytomedicines. Chin Traditional Herbal Drugs. 2016;47(15):2579–2591.
36. Major RT. The ginkgo, the most ancient living tree. The resistance of Ginkgo biloba L. to pests accounts in part for the longevity of this species. Science. 1967;157(3794):1270–1273. doi:10.1126/science.157.3794.1270
37. Liu L, Wang Y, Zhang J, et al. Advances in the chemical constituents and chemical analysis of Ginkgo biloba leaf, extract, and phytopharmaceuticals. J Pharm Biomed Anal. 2021;193:113704. doi:10.1016/j.jpba.2020.113704
38. Feng Z, Sun Q, Chen W, et al. The neuroprotective mechanisms of ginkgolides and bilobalide in cerebral ischemic injury: a literature review. Mol Med. 2019;25(1):57. doi:10.1186/s10020-019-0125-y
39. McKeage K, Lyseng-Williamson KA. Ginkgo biloba extract EGb 761((R)) in the symptomatic treatment of mild-to-moderate dementia: a profile of its use. Drugs Ther Perspect. 2018;34(8):358–366. doi:10.1007/s40267-018-0537-8
40. Clostre F. [Ginkgo biloba extract (EGb 761). State of knowledge in the Dawn of the year 2000]. Ann Pharm Fr. 1999;57(Suppl 1):1S8–88.
41. Diamond BJ, Bailey MR. Ginkgo biloba: indications, mechanisms, and safety. Psychiatr Clin North Am. 2013;36(1):73–83. doi:10.1016/j.psc.2012.12.006
42. Intharuksa A, Kuljarusnont S, Sasaki Y, et al. Flavonoids and other polyphenols: bioactive molecules from traditional medicine recipes/medicinal plants and their potential for phytopharmaceutical and medical application. Molecules. 2024;29(23):5760. doi:10.3390/molecules29235760
43. Siting X. Pharmaceutical research progress of ginkgo biloba leaf extracts. Chinese Pharm Affairs. 2022;36(04):429–443.
44. DeFeudis FV, Drieu K. Ginkgo biloba extract (EGb 761) and CNS functions: basic studies and clinical applications. Curr Drug Targets. 2000;1(1):25–58. doi:10.2174/1389450003349380
45. Chen Yanzhong SZ, Wenfeng Q. Research progress on ginkgo biloba leaf extracts and percutaneous balloon compression in the treatment of trigeminal neuralgia. Shaanxi Med J. 2024;53(10):1438–1441.
46. Hui W, Huang W, Zheng Z, et al. Ginkgo biloba extract promotes Treg differentiation to ameliorate ischemic stroke via inhibition of HIF −1α/ HK2 pathway. Phytother Res. 2023;37(12):5821–5836. doi:10.1002/ptr.7988
47. Singh M, Jindal D, Kumar R, et al. Molecular docking and network pharmacology interaction analysis of gingko biloba (EGB761) extract with dual target inhibitory mechanism in alzheimer’s disease. J Alzheimers Dis. 2023;93(2):705–726. doi:10.3233/JAD-221222
48. Yang TH, Young YH, Liu SH. EGb 761 (Ginkgo biloba) protects cochlear hair cells against ototoxicity induced by gentamicin via reducing reactive oxygen species and nitric oxide-related apoptosis. J Nutr Biochem. 2011;22(9):886–894. doi:10.1016/j.jnutbio.2010.08.009
49. Huang X, Whitworth CA, Rybak LP. Ginkgo biloba extract (EGb 761) protects against cisplatin-induced ototoxicity in rats. Otol Neurotol. 2007;28(6):828–833. doi:10.1097/MAO.0b013e3180430163
50. Barth SW, Lehner MD, Dietz GPH, et al. Pharmacologic treatments in preclinical tinnitus models with special focus on Ginkgo biloba leaf extract EGb 761(R). Mol Cell Neurosci. 2021;116:103669. doi:10.1016/j.mcn.2021.103669
51. Wang X, Zhao X, Tang S. Inhibitory effects of EGb761 on the expression of matrix metalloproteinases (MMPs) and cartilage matrix destruction. Cell Stress Chaperones. 2015;20(5):781–786. doi:10.1007/s12192-015-0600-5
52. Morato X, Tartari JP, Pytel V, et al. Pharmacodynamic and clinical effects of ginkgo biloba extract egb 761 and its phytochemical components in alzheimer’s disease. J Alzheimers Dis. 2024;101(s1):S285–S298. doi:10.3233/JAD-231372
53. Eckert A, Keil U, Kreßmann S, et al. Effects of EGb 761 Ginkgo biloba extract on mitochondrial function and oxidative stress. Pharmacopsychiatry. 2003;36(Suppl 1):S15–23.
54. Brunetti C, Di Ferdinando M, Fini A, et al. Flavonoids as antioxidants and developmental regulators: relative significance in plants and humans. Int J Mol Sci. 2013;14(2):3540–3555. doi:10.3390/ijms14023540
55. Qa’dan F, Mansoor K, AL-Adham I, et al. Proanthocyanidins from Ginkgo biloba leaf extract and their radical scavenging activity. Pharm Biol. 2011;49(5):471–476. doi:10.3109/13880209.2010.523831
56. Shen JG, Zhou DY. Efficiency of Ginkgo biloba extract (EGb 761) in antioxidant protection against myocardial ischemia and reperfusion injury. Biochem Mol Biol Int. 1995;35(1):125–134.
57. Yan LJ, Droy-Lefaix MT, Packer L. Ginkgo biloba extract (EGb 761) protects human low density lipoproteins against oxidative modification mediated by copper. Biochem Biophys Res Commun. 1995;212(2):360–366. doi:10.1006/bbrc.1995.1978
58. Ho LJ, Hung L-F, Liu F-C, et al. Ginkgo biloba extract individually inhibits JNK activation and induces c-Jun degradation in human chondrocytes: potential therapeutics for osteoarthritis. PLoS One. 2013;8(12):e82033. doi:10.1371/journal.pone.0082033
59. Lee CY, Yang -J-J, Lee -S-S, et al. Protective Effect of Ginkgo biloba leaves extract, EGb761, on Endotoxin-Induced Acute Lung Injury via a JNK- and Akt-Dependent NFκB Pathway. J Agric Food Chem. 2014;62(27):6337–6344. doi:10.1021/jf501913b
60. Knights AJ, Redding SJ, Maerz T. Inflammation in osteoarthritis: the latest progress and ongoing challenges. Curr Opin Rheumatol. 2023;35(2):128–134. doi:10.1097/BOR.0000000000000923
61. Kou S, Wu Y. Meta-analysis of tumor necrosis factor alpha −308 polymorphism and knee osteoarthritis risk. BMC Musculoskelet Disord. 2014;15:373. doi:10.1186/1471-2474-15-373
62. Kotakadi VS, Jin Y, Hofseth AB, et al. Ginkgo biloba extract EGb 761 has anti-inflammatory properties and ameliorates colitis in mice by driving effector T cell apoptosis. Carcinogenesis. 2008;29(9):1799–1806. doi:10.1093/carcin/bgn143
63. Zhang P, Li K, Kamali A, et al. Small molecules of herbal origin for osteoarthritis treatment: in vitro and in vivo evidence. Arthritis Res Ther. 2022;24(1):105. doi:10.1186/s13075-022-02785-y
64. Xiaopei Z. Research progress on neuroprotective effect of ginkgo biloba extract. Mod J Integr Traditional Chin Western Med. 2023;32(10):1451–1456.
65. Serrano-Garcia N, Pedraza-Chaverri J, Mares-Sámano JJ, et al. Antiapoptotic Effects of EGb 761. Evid Based Complement Alternat Med. 2013: 495703. doi:10.1155/2013/495703
66. Shen J, Lee W, Gu Y, et al. Ginkgo biloba extract (EGb761) inhibits mitochondria-dependent caspase pathway and prevents apoptosis in hypoxia-reoxygenated cardiomyocytes. Chin Med. 2011;6:8. doi:10.1186/1749-8546-6-8
67. Christen Y, Maixent JM. What is Ginkgo biloba extract EGb 761? An overview--from molecular biology to clinical medicine. Cell Mol Biol. 2002;48(6):601–611.
68. Chen XJ, Ren S-M, Dong J-Z, et al. Ginkgo biloba extract-761 protects myocardium by regulating Akt/Nrf2 signal pathway. Drug Des Devel Ther. 2019;13:647–655. doi:10.2147/DDDT.S191537
69. Yoshitake T, Yoshitake S, Kehr J. The Ginkgo biloba extract EGb 761(R) and its main constituent flavonoids and ginkgolides increase extracellular dopamine levels in the rat prefrontal cortex. Br J Pharmacol. 2010;159(3):659–668. doi:10.1111/j.1476-5381.2009.00580.x
70. Li Jing LC. Effects of Ginkgo biloba Extract (EGb761) on Lipid Peroxidative Damage of Red Blood Cells. Period Ocean Univ China. 2005;(03):487–490+381.
71. Xue Feng GY, Desong C, Jifeng L. Protective Effect of Ginkgo biloba Extract EGb761 on Sensory Neurons After Peripheral Nerve Injury. Fudan Univ J. 2002(04):251–254.
72. Xue Feng GY, Jifeng L, Desong C, Cisheng Z. Effects of ginkgo biloba extract on ultrastructure of sensory neurons after sciatic nerve injury. Chin J Exp Surg. 2002(05):64–65+96.
73. Mdzinarishvili A, Sambria RK, Lang D, Klein J, et al. Ginkgo extract EGb761 confers neuroprotection by reduction of glutamate release in ischemic brain. J Pharm Pharm Sci. 2012;15(1):94–102. doi:10.18433/J3PS37
74. Yao Y, Zhao J, Li C, et al. Ginkgo biloba extract safety: insights from a real-world pharmacovigilance study of FDA adverse event reporting system (FAERS) events. J Ethnopharmacol. 2025;337(Pt 3):119010. doi:10.1016/j.jep.2024.119010
75. Izzo AA, Ernst E. Interactions between herbal medicines and prescribed drugs: an updated systematic review. Drugs. 2009;69(13):1777–1798. doi:10.2165/11317010-000000000-00000
76. Gardner CD, Zehnder JL, Rigby AJ, Nicholus JR, Farquhar JW, et al. Effect of Ginkgo biloba (EGb 761) and aspirin on platelet aggregation and platelet function analysis among older adults at risk of cardiovascular disease: a randomized clinical trial. Blood Coagul Fibrinolysis. 2007;18(8):787–793. doi:10.1097/MBC.0b013e3282f102b1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024