Back to Journals » Clinical Ophthalmology » Volume 19
Standalone Canaloplasty and Trabeculotomy Using the OMNI Surgical System: A Subgroup Analysis from the American Academy of Ophthalmology IRIS® Registry (Intelligent Research in Sight)
Authors Pyfer MF, Funke C, Mosaed S, Zwick E ![]() , Toth J
, Toth J ![]() , Garcia K, Radcliffe NM
, Garcia K, Radcliffe NM ![]()
Received 9 August 2025
Accepted for publication 23 October 2025
Published 1 November 2025 Volume 2025:19 Pages 4043—4052
DOI https://doi.org/10.2147/OPTH.S559620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mark F Pyfer,1,2 Christine Funke,3 Sameh Mosaed,4 Erin Zwick,5 Jennifer Toth,5 Kristian Garcia,5 Nathan M Radcliffe6
1Northern Ophthalmic Associates, Jenkintown, PA, USA; 2Wills Eye Hospital, Philadelphia, PA, USA; 3Barnet, Dulaney & Perkins Eye Center, Mesa, AZ, USA; 4Gavin Herbert Eye Institute, University of California, Irvine, Irvine, CA, USA; 5Verana Health, San Francisco, CA, USA; 6Ophthalmology, Mt Sinai School of Medicine, New York, NY, USA
Correspondence: Nathan M Radcliffe, Email [email protected]
Purpose: To characterize clinical outcomes of canaloplasty and trabeculotomy using the OMNI Surgical System (Sight Sciences) as a standalone procedure in primary open-angle glaucoma (POAG) subgroups (phakic, pseudophakic; mild, moderate, severe disease).
Design: Retrospective, observational cohort study utilizing the American Academy of Ophthalmology (Academy) IRIS® Registry (Intelligent Research in Sight).
Methods: Patients with POAG undergoing standalone OMNI surgery with known laterality between January 2018 and December 2021 and followed for a minimum of 6 months and up to 36 months were included. Analyses divided the cohort into mild, moderate, and severe glaucoma subgroups (International Classification of Disease-10 coding), and lens status (phakic and pseudophakic) subgroups. Outcomes included changes in intraocular pressure (IOP) and glaucoma medication class use.
Results: Data from 220 eyes of 187 patients were analyzed. Mean IOP reductions from baseline were clinically and statistically significant at every time point across disease severity groups; mild, 5.5– 9.4 mmHg (p < 0.0026); moderate, 5.3– 7.4 mmHg (p < 0.0001 at all time points); severe, 5.8– 7.6 mmHg (p < 0.0004). Mean IOP reductions were 5.1– 7.4 mmHg in phakic eyes and 5.8– 6.7 mmHg in pseudophakic eyes; p < 0.0001 all time points, both subgroups. Mean medication reductions from baseline were clinically and statistically significant at month 6 and month 12 in the mild and severe groups, and insignificant at all other time points in the three groups. Medication reductions averaged 0.3– 0.4 in phakic eyes (non-significant) and statistically significant reductions of 0.4– 0.6 in pseudophakic eyes (months 6, 12, and 18 [p < 0.01]), with non-significant reductions (0.3– 0.4 medications) at later time points.
Conclusion: In this study, standalone OMNI surgery significantly decreased IOP for up to 3 years regardless of disease severity or lens status. This procedure may be considered for phakic or pseudophakic patients with all stages of glaucoma whose therapeutic goals fall within the ranges achievable with standalone surgery.
Keywords: MIGS, canaloplasty, primary open-angle glaucoma, pseudophakic, OMNI
Introduction
The advent of minimally invasive glaucoma surgery (MIGS) has expanded interest in early surgical intervention for primary open-angle glaucoma (POAG) patients who might benefit from surgical control of intraocular pressure (IOP) but whose therapeutic goals may not warrant traditional filtering surgery and the accompanying risks. Some procedures are labeled for use at the time of cataract surgery while others can be deployed as standalone therapy. For pseudophakic and non-cataractous phakic eyes, standalone surgery offers the opportunity to reduce or eliminate topical medical therapy and its associated limitations that include high rates of nonadherence and side effects such as ocular surface disease.1
Many MIGS procedures are approved for use in eyes with mild to moderate POAG.2,3 While some eyes with advanced glaucoma may warrant large IOP reductions or low target IOP not generally attainable with MIGS, others may have more modest therapeutic needs and may benefit from MIGS. There are fewer options—and little supporting evidence—for the use of standalone MIGS procedures in eyes with more advanced glaucoma.2 While many studies include eyes with advanced glaucoma, only a few report outcomes by disease severity, and in those studies, the IOP and medication reductions are typically similar in eyes with mild, moderate, and severe disease.4–6
Lens status at the time of standalone MIGS may affect the outcome of surgery. Most MIGS procedures rely on the passage of aqueous humor from the anterior chamber to Schlemm’s canal via either a surgically created opening in the trabecular meshwork (TM) or an implant that shunts aqueous humor across the TM. Therefore, a deeper anterior chamber angle—as is typically seen in pseudophakic versus phakic eyes—might better facilitate access of aqueous humor to the angle and into the canal. In fact, a larger anterior chamber depth was associated with a trend toward lower IOP following trabecular ablation surgery.7 However, there are very few studies that have explored the relationship between phakic status and outcomes following standalone MIGS surgery.
We have conducted a retrospective, observational study of real-world data from the American Academy of Ophthalmology IRIS® Registry (Intelligent Research in Sight) to characterize clinical outcomes in eyes with mild, moderate, and severe glaucoma and to assess clinical outcomes for both phakic and pseudophakic eyes following standalone ab interno canaloplasty and trabeculotomy with the OMNI Surgical System (Sight Sciences).
Methods
This was a retrospective, observational real-world cohort study using electronic health records (EHR) from the Academy IRIS Registry. The IRIS Registry contains de-identified data from nearly 24% of the United States population and comprises data from nearly 670 million encounters between 78.9 million unique patients and over 15,000 ophthalmologists and the clinicians working with them in the US.8 The data were extracted by Verana Health in July 2024. Ocular hypotensive medication usage data was obtained from a deidentified third-party commercial medical and pharmacy claims database linked to IRIS Registry data using anonymized tokens. The study was reviewed and deemed exempt under 45 CFR § 46.104(d)(4) by the WIRB-Copernicus Group (WCG) Institutional Review Board (Puyallup, WA).
Criteria for inclusion in this analysis included the following: a documented OMNI procedure (using Current Procedural Terminology [CPT] coding and provider-entered procedure text description) with known laterality between 01/01/2018 and 12/31/2021 and >6 months of follow-up postoperatively; a diagnosis of POAG with severity specified using International Classification of Disease 10th edition (ICD-10) coding in the same eye within 6 months prior to surgery; phakic status reported; a documented baseline IOP within 6 months preoperatively; and at least one pharmacy claim in the postoperative period. Criteria for exclusion from this analysis included the following: evidence of cataract surgery in the study eye on the same day as OMNI surgery; missing key demographic information (age or sex); evidence of laser trabeculoplasty within 90 days preoperatively in the study eye; absence of a glaucoma diagnosis or any glaucoma diagnosis not consistent with US Food and Drug Administration (FDA)-approved indications for use of OMNI (ie, glaucoma types other than POAG).
Study eyes were categorized according to POAG severity at baseline as determined by ICD-10 code. Eyes with unspecified POAG severity were excluded from analyses stratified by severity. Study eyes were separately categorized by phakic status.
Results include demographics, including age, sex, race and ethnicity, payor type, and study eye laterality; clinical characteristics including glaucoma severity based on ICD-10 codes, lens status, presence of dry eye disease, history of prior MIGS surgery and/or trabeculoplasty; surgeon subspecialty; IOP and medication use at baseline and 6 (±60 days), 12 (±90 days), 18 (±90 days), 24 (+180 days/-90 days), and 36 (±180 days) months postoperatively. Demographics are presented at the patient level. Medication usage is also presented at the patient level because of lack of laterality in the pharmacy claims database and by medication class rather than individual drug.
The IOP measurement in closest proximity and prior to the OMNI surgery was taken as the baseline IOP. Where there was more than one IOP measurement made within a follow-up period window, the measurement nearest to the follow-up time point (eg 24 months) was used. If there were two or more IOP measurements on a particular day (at baseline or follow-up), the mean was used.
The purpose of this analysis is to describe IOP reduction and medication use up to 3 years postoperatively following OMNI surgery in eyes with mild versus moderate versus severe POAG and to describe these same outcomes for phakic versus pseudophakic eyes. Eyes were not censored at the time of or after a secondary surgical intervention (SSI). Mean (standard deviation) IOP and mean number of IOP-lowering medication classes used for each of these subgroups were calculated at each time point and compared to baseline using paired t-tests. P-values less than 0.05 were considered to be statistically significant across all analyses, except for pairwise comparisons where the Bonferroni correction was applied (p < 0.01 or p < 0.0083, depending on number of comparisons, as noted). All p-values are presented unadjusted. Between-group comparisons were descriptive without inferential statistics because no specific hypotheses were proposed or tested.
Results
Outcomes by Disease Severity
Overall, data from 220 eyes of 187 patients were analyzed. Demographic data for the study group by glaucoma severity are given in Table 1. Glaucoma severity was coded as mild in 29 patients (15.5%), moderate in 76 patients (40.6%), and severe in 82 patients (43.9%). The mean age (74.1–76.1 years), sex distribution (51.3–58.6% female), racial and ethnic distributions (50.0–69.0% White patients, 65.8–86.2% not Hispanic or Latino patients), and laterality (80.3–86.2% unilateral) for the three groups were generally similar.
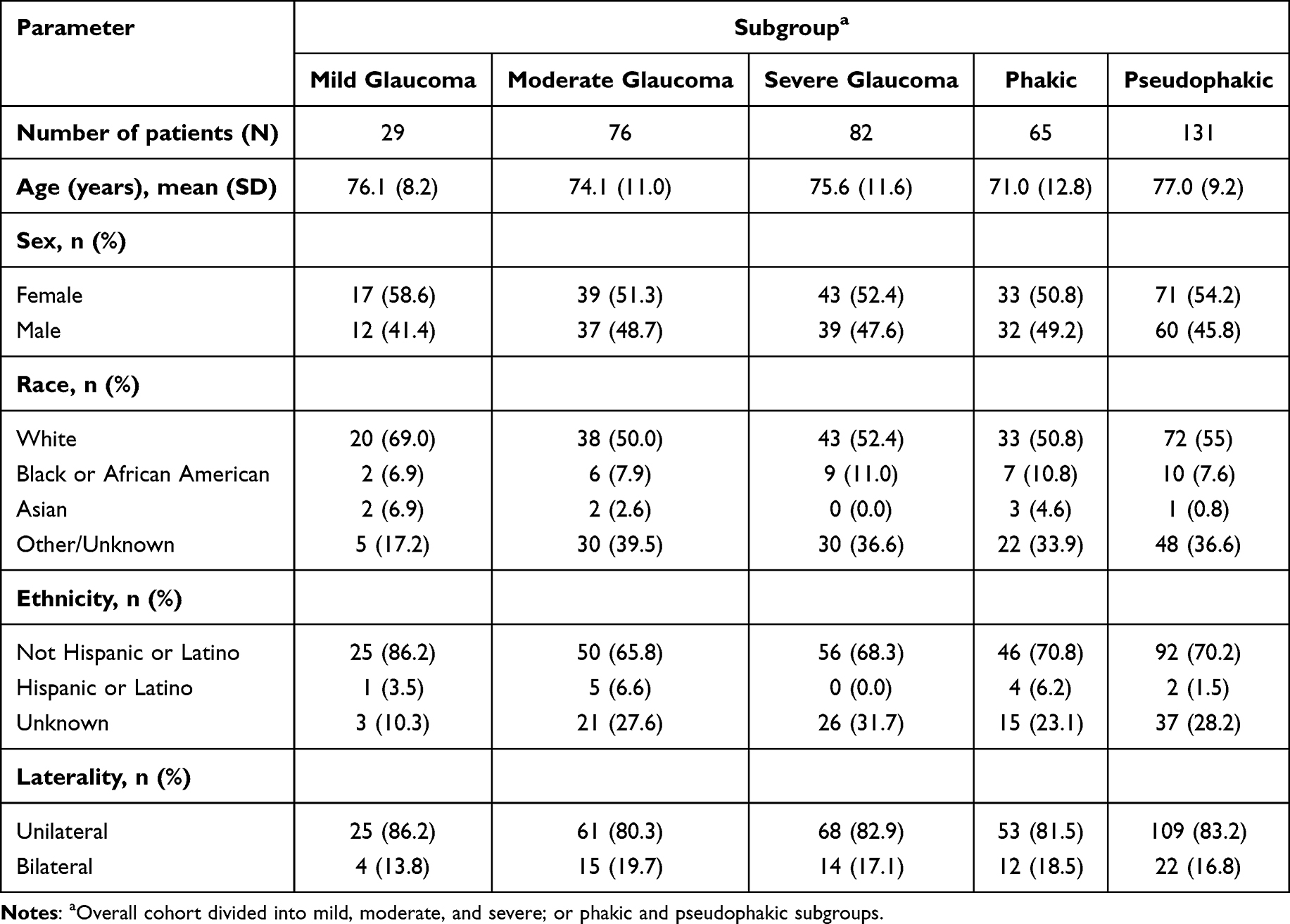 |
Table 1 Demographic Data for the Study Group |
The clinical characteristics of eyes in the three glaucoma severity categories were also similar (Table 2). Approximately one-third of eyes in each group (29.5–35.9%) were phakic and the remainder pseudophakic. Just under half of eyes in each group had comorbid dry eye disease (44.6–49.5%). Only 2 eyes had undergone prior MIGS surgery: one iStent in the mild group and one Hydrus in the moderate group. Trabeculoplasty had low utilization rates in all three groups (9.5–24.2%) and was least likely to have been performed in eyes with severe glaucoma (9.5%). The relative proportions of surgeries in each group performed by glaucoma specialists (39.4–45.7%) versus others was generally similar across the spectrum of glaucoma severity.
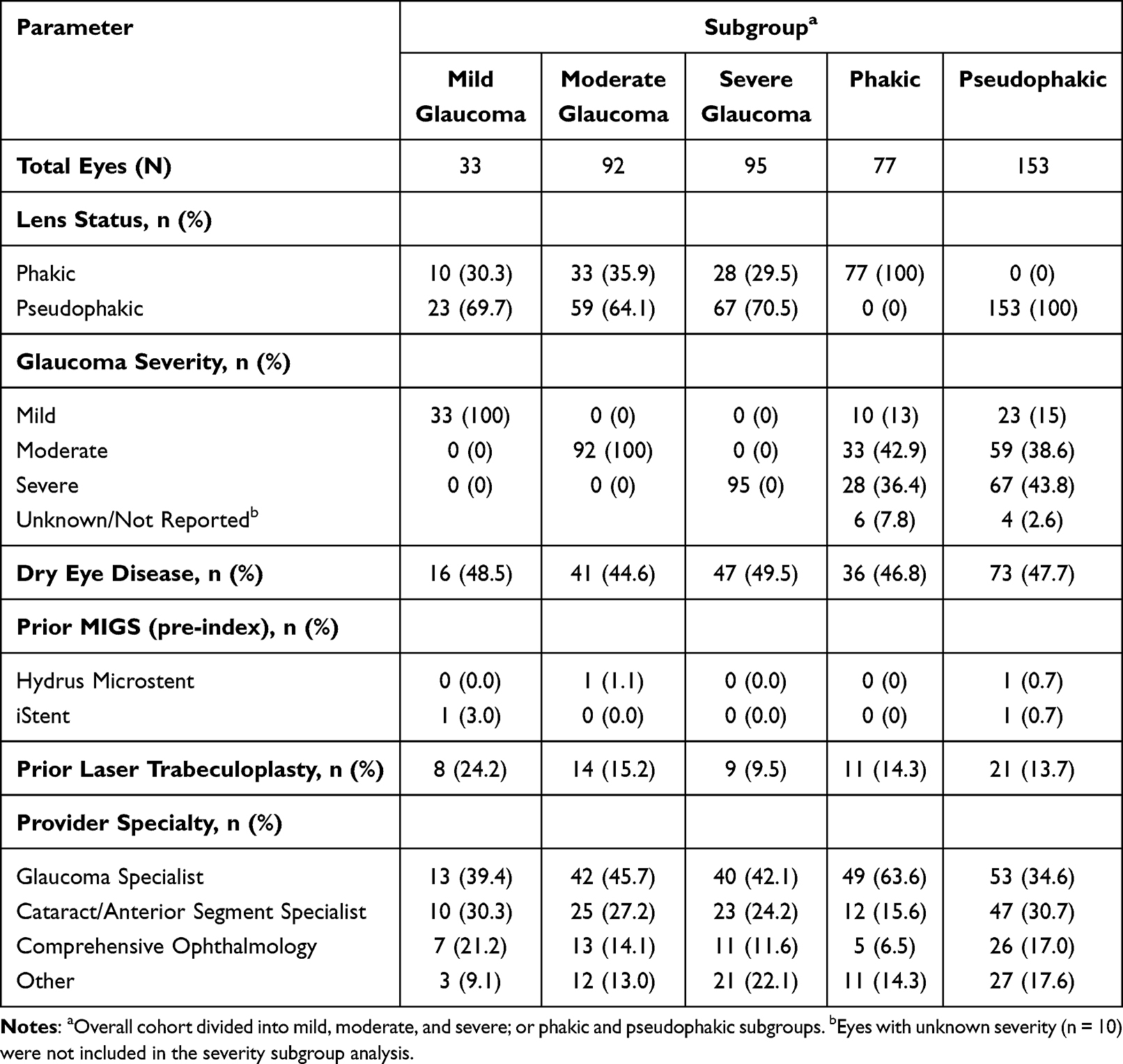 |
Table 2 Clinical Characteristics of the Eyes in the Study Group |
Baseline IOP was generally similar (21.3–23.0 mmHg) between the three severity groups (Table 3). Mean IOP reductions from baseline were clinically and statistically significant at every time point in all three groups. In eyes with mild glaucoma, mean IOP from months 6–36 ranged from 14.2 to 17.9 mmHg (p < 0.0026, Bonferroni corrected significance threshold p < 0.01) representing mean reductions of 5.5–9.4 mmHg. In moderate glaucoma, mean IOP ranged from 15.0 to 16.2 mmHg (p < 0.0001 at all time points) representing mean reductions of 5.3–7.4 mmHg. In severe glaucoma, mean IOP ranged from 14.1 to 16.8 mmHg (p < 0.0004) representing mean reductions of 5.8–7.6 mmHg.
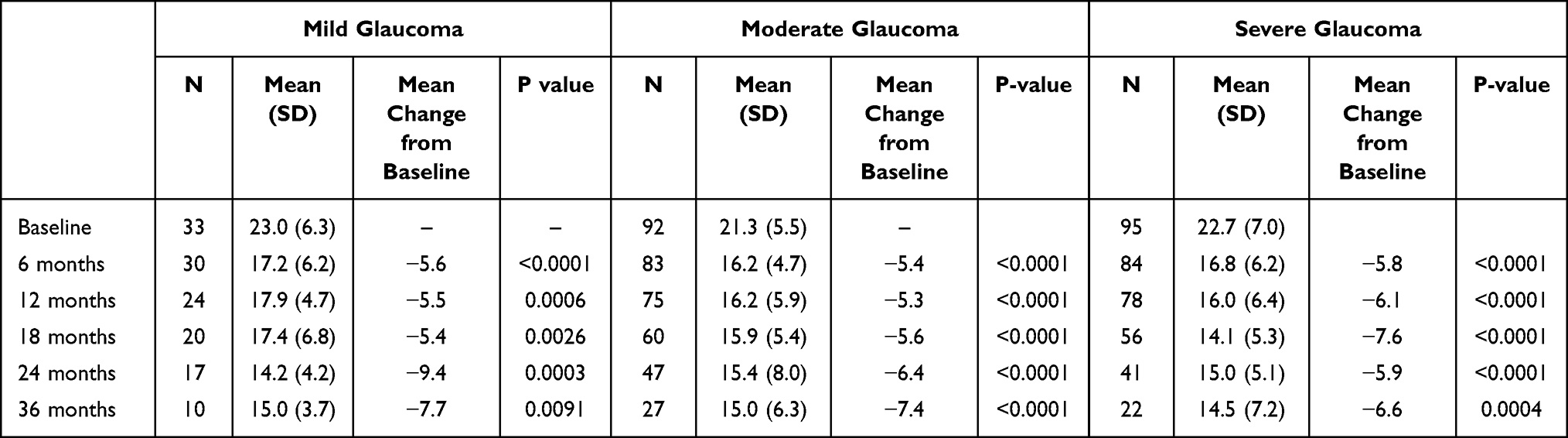 |
Table 3 Mean IOP and Changes from Baseline at Each Postoperative Time Point (mmHg); Severity Subgroups |
Baseline medication use was lowest in patients with mild glaucoma (1.7 [1.5] medications) and highest in eyes with severe glaucoma (2.4 [1.6] medications) (Table 4). Mean medication reductions from baseline were clinically and statistically significant at month 6 and at month 12 in the mild and severe glaucoma groups, and insignificant at all other time points in the three groups. The only time point in any group that mean medication classes used was higher than at baseline was at month 24 in eyes with severe glaucoma, with a nominal mean increase of 0.03 medication classes.
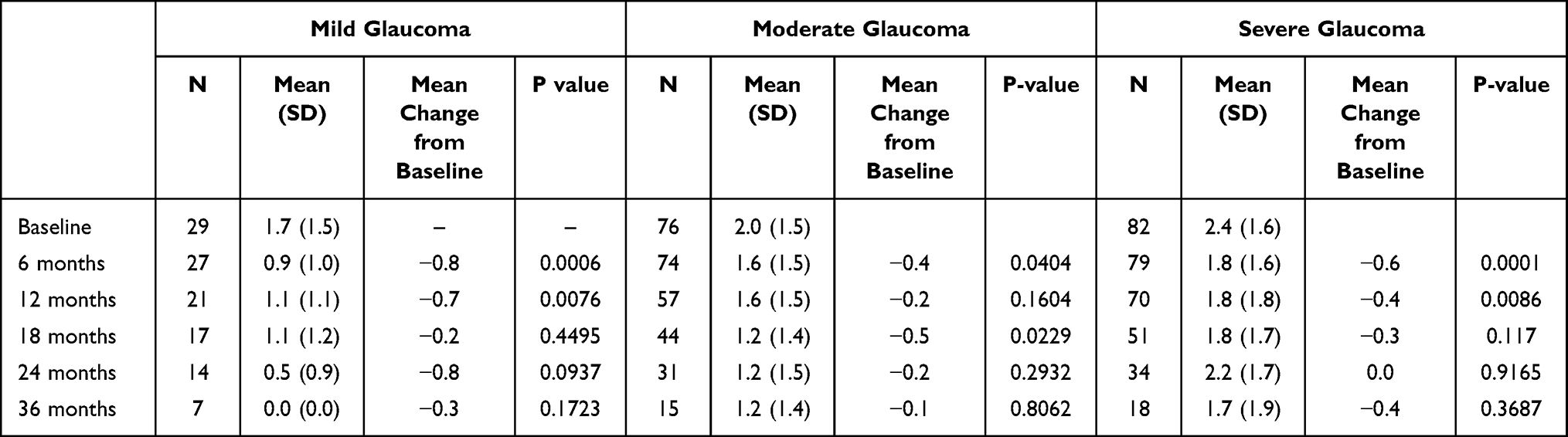 |
Table 4 Mean Medication Use and Changes from Baseline at Each Postoperative Time Point; Severity Subgroups |
Outcomes by Phakic Status
This analysis included 230 eyes of 196 patients, of which 77 (33.5%) were phakic and 153 (66.5%) were pseudophakic. Demographic data for patients are given in Table 1. Patients who had pseudophakic eyes operated on were older than patients who had phakic eyes operated on (mean age 77.0 versus 71.0 years) and approximately half in each group (50.8–54.2%) were female. Approximately half in each group were White (50.8–55.0%) and most were not Hispanic or Latino (70.2–70.8%). A minority of patients in each group had both eyes enrolled in the study (16.8–18.5%).
Clinical characteristics of the eyes in both groups are given in Table 2. The distribution of glaucoma severity was similar between groups, with most having moderate (38.6–42.9%) or severe glaucoma (36.4–43.8%). Few eyes had undergone prior laser trabeculoplasty (13.7–14.3%) and only 2 eyes (both in the pseudophakic group; 1.4%) had undergone a prior MIGS procedure. Glaucoma specialists performed the majority of surgeries in phakic eyes (63.6%) but fewer surgeries in pseudophakic eyes (34.6%), where a plurality of surgeries were performed by cataract/anterior segment specialists or comprehensive ophthalmologists (47.7% combined).
Mean IOP at baseline was similar in phakic (21.9 [5.7] mmHg), Figure 1A, and pseudophakic eyes (22.3 [6.7]), Figure 1B. Likewise, mean IOP throughout follow-up and mean IOP reductions at each time point were similar between groups. In phakic eyes, mean postoperative IOP ranged from 14.3 to 16.8 mmHg over 3 years of follow-up, representing statistically significant mean IOP reductions of 5.1–7.4 mmHg (p < 0.0001 at all time points, Bonferroni corrected threshold p < 0.01). In pseudophakic eyes, mean postoperative IOP ranged from 15.0 to 16.6 mmHg during follow-up, representing statistically significant mean IOP reductions of 5.8–6.7 mmHg (p < 0.0001 at all time points).
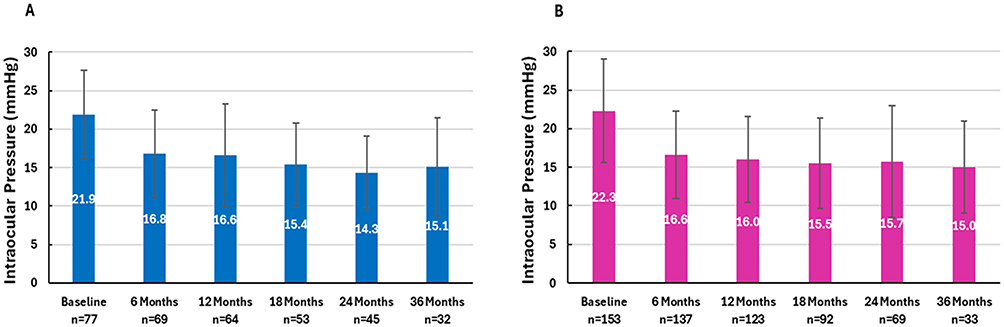 |
Figure 1 Mean Intraocular pressure (IOP) at each timepoint through 36 months. (A) Phakic eyes; (B) Pseudophakic eyes. P < 0.0001 versus baseline for both phakic and pseudophakic at all timepoints. Error bars are 1 standard deviation. |
Mean medication use (Table 5) at baseline was similar in phakic (2.0 [1.6] medication classes per eye) and pseudophakic eyes (2.2 [1.5] medication classes per eye). In phakic eyes, mean medication use ranged from 1.3 to 1.7 medication classes per eye during follow-up, representing reductions of 0.3–0.4 medications per eye. In pseudophakic eyes, medication use ranged from 0.9 to 1.6 medication classes per eye during follow-up, representing statistically significant reductions of 0.4–0.6 medications per eye at months 6,12 and 18 (p < 0.0083 [Bonferroni corrected threshold]) and reductions of 0.3–0.4 medications per eye at later time points (p > 0.05).
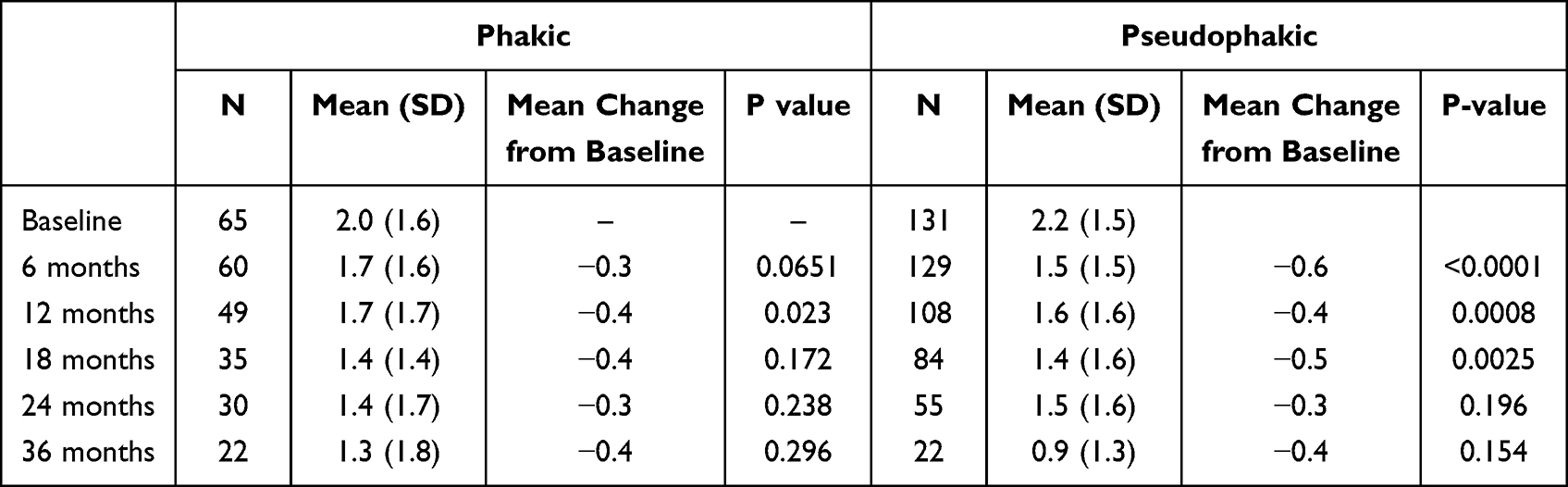 |
Table 5 Mean Medication Use and Changes from Baseline at Each Postoperative Time Point; Phakic and Pseudophakic Subgroups |
The rate of SSI for the full cohort has been reported previously, 86 of 230 eyes, 37%.9 Laser trabeculoplasty accounted for 17 (7.4%) while traditional invasive glaucoma surgery (eg trabeculectomy or tube shunt) and transscleral cyclophotocoagulation together accounted for about half (41 of 86) with the majority (35) in eyes with a higher baseline IOP (>18 mmHg).9 Interestingly, in the present subgroup analysis by disease severity, the rate for these advanced procedures was mild (6%), moderate (22%), and severe (18%). The rates in phakic and pseudophakic eyes were 30% and 14%, respectively.
Discussion
This analysis of real-world data from the IRIS Registry demonstrates that ab interno canaloplasty and trabeculotomy performed with the OMNI Surgical System provides clinically and statistically significant reductions in IOP through 3 years postoperatively in eyes with mild, moderate, and severe glaucoma and for both phakic and pseudophakic eyes. Early reductions in medication use were also observed in eyes across the severity of glaucoma, but medication use was unchanged at later time points in these groups. Medication use decreased for both phakic and pseudophakic eyes, but the changes were statistically significant only for the pseudophakic cohort through the first 18 months.
Glaucoma can be diagnosed at any level of severity and, largely because of its asymptomatic nature in the early stages, is often diagnosed late in its course.10–13 In addition, because many patients will experience disease progression even with multimodal therapy,14 many patients with mild or moderate glaucoma progress to more advanced glaucoma over time. Many treatment guidelines advocate for different therapeutic approaches for patients at different stages of the disease.15–17 However, there remains a paucity of data comparing clinical outcomes of glaucoma therapies at the various stages of the disease, which, in turn, hinders an evidence-based approach to therapy selection based on glaucoma stage. Ahmed et al demonstrated comparable 12-month IOP reductions and surgical success rates for eyes with mild and moderate/severe glaucoma undergoing trabecular ablation.4 Chansangpetch et al demonstrated greater IOP reductions but smaller medication reductions with more advanced glaucoma 12 months after undergoing iStent implantation at the time of cataract surgery.18 Yadgarov et al compared outcomes in eyes with mild, moderate, and advanced glaucoma undergoing OMNI surgery and found greater IOP reductions through 24 months in eyes with advanced glaucoma (26.9%) than mild or moderate glaucoma (11.1% and 16.2%, respectively), and significant medication reductions at month 24 only in the advanced glaucoma group.5 In contrast, Dickerson et al reported similar IOP and medication reductions at month 12 among eyes with mild, moderate, and severe glaucoma undergoing OMNI surgery.6 Many other studies have included eyes at all stages of glaucoma but have not analyzed or reported outcomes by severity.
The IOP-lowering achieved with standalone OMNI surgery was similar in phakic and pseudophakic eyes and similar to outcomes reported in prior studies. Bleeker et al reported 6-month IOP reduction of ~7 mmHg after standalone OMNI in pseudophakic eyes.19 In an analysis of standalone data from the ROMEO study (which included only pseudophakic eyes), mean IOP reductions were 6.2 mmHg and 7.4 mmHg at 12 and 24 months, respectively.20,21 Similarly, IOP at 12 months was reduced an average of 5.6 mmHg for standalone patients in ROMEO 2.22 Klabe et al reported 24-month outcomes of standalone OMNI in phakic and pseudophakic eyes separately and found mean IOP reductions of ~10 mmHg in phakic eyes and ~8.5 mmHg in pseudophakic eyes.23 A recent systematic review and meta-analysis by Zhu et al included five studies of OMNI used as a standalone procedure.24 In that analysis, the authors commented on the somewhat greater overall IOP reduction observed in the Klabe study (which had a majority of phakic eyes) and suggested that the lower average age of patients in that study, 67 years, could have contributed to the greater observed IOP reduction because aqueous production might be greater in a younger population.24 While this is possible, the difference in mean age between the phakic patients in our study and in the patients in the Klabe study is quite modest (71 versus 67 years, respectively) and we believe the primary reason for the observed larger IOP reductions in the Klabe study was due to the baseline medication washout which resulted in a greater mean baseline IOP of 24.5 mmHg versus the 21.9 mmHg for the phakic cohort in this study.23 It is worth noting that the mean IOP at 24 months for both the Klabe patients and the present study phakic cohort is a nearly identical ~15 mmHg.
Medication reductions were modest and variably statistically significant across time points, stages of disease severity, and phakic status in this data set. This may be partially explained by limitations of methodology. Pharmacy claims lack laterality data; therefore, medication use must be reported as a patient-level variable rather than as an eye-level variable.25,26 Therefore, if patients were able to discontinue a medication following surgery in the operative eye but continued to require it in the non-operated eye, no reduction in medication use would be recorded. The nature of the patients and the surgical intervention may also partially explain the findings. These were eyes undergoing standalone surgery. The threshold for surgical intervention using a standalone procedure is likely greater than the threshold for adding a MIGS procedure to a planned cataract surgery. In the latter, adding a MIGS procedure in a medically well-controlled eye may reduce medication burden and thus improve patient quality of life with little incremental risk. However, it is less likely that a medically well-controlled patient without medication tolerability problems would undergo a standalone glaucoma surgery with the goal of reducing the medication burden, as the potential benefit generally may not justify the risk. Thus, it is reasonable to assume that reducing the medication burden was not the primary goal of surgery for many or most of the eyes in this analysis. A previous report of outcomes for the full cohort grouped according to baseline IOP (≤18 mmHg and >18 mmHg) showed that there was statistically significant medication reduction through 36 months for the lower baseline IOP group, with >50% of these patients medication free at the end of follow-up.9 In other published studies of standalone OMNI, Klabe et al reported mean medication reductions of ~1.5 at 2 years in both phakic and pseudophakic patients,23 while the ROMEO study reported reductions of only ~0.3 medications per eye at 24 months in mixed phakic and pseudophakic eyes.21
In general, therapy should be selected that is expected to achieve patient-specific IOP goals. The rationale for deploying different treatment modalities at different stages of glaucoma is that more severe glaucoma often warrants greater IOP reduction than eyes with earlier stage disease.15–17 In a prior analysis of this cohort of patients undergoing OMNI surgery, IOP reductions were directly related to baseline IOP; eyes with lower baseline IOP (<18 mmHg; mean 15.5 mmHg) manifested IOP reductions of ~1–3 mmHg over three years of follow-up, while eyes with higher baseline IOP (>18 mmHg; mean 25.1 mmHg) manifested IOP reductions in the range of ~7.5–9.0 mmHg.9 These findings are consistent with prior reports that conducted subgroup analyses by baseline IOP: as with many therapies for glaucoma, OMNI surgery lowers IOP more in eyes with higher baseline IOP than with lower baseline IOP.19,21,23 Coupled with the findings of this analysis that OMNI surgery provides mean IOP reductions of 5.8–7.6 mmHg over three years, this procedure would be a reasonable option for patients with severe glaucoma whose IOP reduction goals fall within this range.
The reoperation rate in this study was higher in eyes with moderate or severe glaucoma compared to mild glaucoma and may reflect the need for greater IOP reduction or lower IOP in more advanced cases. A prior IRIS Registry analysis of data from more than 79,000 eyes revealed 2-year SSI rates of 24%, 24%, and 15% for standalone goniotomy/canaloplasty, XEN gel stent, and endocyclophotocoagulation, respectively.27 Our data reflect the rates of SSI through up to 3 years of follow-up. The overall SSI rate was ~37% (16% considering only tube shunt or trabeculectomy) across all severity groups, thus the majority of patients were able to achieve better disease control and avoid additional procedures. The rates of SSI in both phakic and pseudophakic eyes in this 3-year, real-world IRIS Registry analysis was higher than has been reported in prior studies (5.3–7.1% in two 24-month studies).6,23 One explanation may be the duration of the studies; this is the longest-term study of standalone OMNI outcomes to date of which we are aware, and as such it includes late SSI that would not be captured in shorter-term studies. Disease severity may also affect SSI rates. Klabe’s study included only eyes with mild-moderate POAG which may have had more modest treatment goals and target IOP.23 ROMEO had a sample with a range of glaucoma severity comparable to the current study, albeit with a limited number in the severe category, and found that the rate of SSI was higher in eyes with more advanced disease, likely reflecting the need for greater IOP reduction and lower target IOP in these eyes.6 Similarly, Yadgarov et al reported higher SSI rates with increasing disease severity in a cohort of 171 eyes that had undergone OMNI combined with phacoemulsification.5 It is unclear why phakic eyes had a substantially higher SSI rate than pseudophakic eyes. Patients undergoing phakic surgery in this analysis were younger than patients with pseudophakia and may have warranted lower target IOP because they would be expected to live with the disease longer. Phakic eyes may have additional risk factors for surgical failure, as Wecker et al noted a trend toward less IOP reduction in eyes with shallower anterior chamber angles.7 Also, Creagmile et al reported a high rate of SSI (37.5%) in phakic eyes undergoing combined OMNI and Hydrus implantation.28 Currently, there are too few studies of MIGS procedures in phakic eyes to draw meaningful conclusions about these findings.
Strengths of this study include its large sample size as well as the extended follow-up through 3 years postoperatively. Also, this is an analysis of real-world data and reflects the routine clinical practice patterns of many surgeons across the United States; as such, it provides a measure of therapeutic effectiveness that complements the more rigid efficacy data drawn from robust clinical trials. The IRIS Registry is uniquely able to generate such data and is the source of real-world data analyses for more than 149 ophthalmological studies to date (American Academy of Ophthalmology website, May 30, 2025). Specific to this analysis, the evaluation of outcomes based on glaucoma severity subgroups provides important clinical information to guide the selection of therapy based on this important patient characteristic. Similarly, the analysis based on phakic status addresses an unmet need for data on outcomes based on various ocular characteristics to aid in patient selection for the multitude of new glaucoma procedures that have emerged in recent years. The limitations of this study are those inherent to all database studies, including issues related to data quality, accuracy of documentation and coding, and missing data, among others.29 An additional limitation of this study is lack of laterality for medication use, which is common to all pharmacy claims data. As a result, unilateral surgery that decreases medication use in the operative eye may not be reflected as a medication reduction if the medication continues to be used in the fellow eye. Both eyes of a patient were included in the study if both qualified; this could result in an underestimation of variability, however the number of bilateral cases was relatively small, and the resultant larger dataset more than offsets this possibility. Finally, the IOP recorded closest to the index procedure was used as the baseline IOP. A baseline that was the mean of multiple visits could have been used instead but would likely have introduced additional variability based on time of day the measurements were taken, and possible medication changes that may have occurred between the two measures. Moreover, it is likely that in many cases these single IOP measurements were incorporated into the surgeons’ decisions to intervene, which is how decisions are often made in real world clinical practice.
Conclusion
In summary, this study found that standalone ab interno canaloplasty and trabeculotomy using the OMNI Surgical System provides clinically and statistically significant IOP reductions across the spectrum of glaucoma severity. OMNI surgery significantly decreases IOP for up to 3 years in phakic eyes in this study. In pseudophakic eyes, significant reductions in IOP through 3 years and in medication use through 18 months were seen. Based on these findings, this standalone procedure appears to be an effective means of lowering IOP and allows many patients to avoid more high-risk bleb-based procedures like trabeculectomy and tube shunt implantation.
Data Sharing Statement
The authors do not intend to share participant level data. Other queries or requests should be directed to the corresponding author (NR).
Acknowledgments
Dr. Tony Realini (Hypotony LLC) provided medical writing services for a preliminary draft of the manuscript. Dr. Jaime Dickerson assisted in the creation of the current version of the manuscript.
Funding
Sight Sciences Inc. provided financial support.
Disclosure
MP has consulted for Allergan/Abbvie, Glaukos, Johnson & Johnson, Rayner, RxSight, Sight Sciences, Tarsus. CF is a consultant for AbbVie, Alcon, Glaukos, Thea, Sight Sciences, Dompe, New World Medical, Nova Eye Medical, Elios, Apellis, RxSight. SM reports personal fees from Alcon and Skye Bioscience; grants from Sight Sciences. EZ, JT, and KG are employees of Verana Health. NMR is a consultant for AbbVie, Alcon, Bausch + Lomb, BVI International, Glaukos, Iridex, Iantrek, New World Medical, and Sight Sciences. The authors report no other conflicts of interest in this work.
References
1. Radcliffe N. The case for standalone micro-invasive glaucoma surgery: rethinking the role of surgery in the glaucoma treatment paradigm. Curr Opin Ophthalmol. 2023;34(2):138–145. doi:10.1097/ICU.0000000000000927
2. Balas M, Mathew DJ. Minimally invasive glaucoma surgery: a review of the literature. Vision. 2023;7.
3. Dhawale KK, Tidake P. A comprehensive review of recent advances in minimally invasive glaucoma surgery: current trends and future directions. Cureus. 2024;16(7):e65236. doi:10.7759/cureus.65236
4. Ahmed SF, Bhatt A, Schmutz M, Mosaed S. Trabectome outcomes across the spectrum of glaucoma disease severity. Graefes Arch Clin Exp Ophthalmol. 2018;256(9):1703–1710. doi:10.1007/s00417-018-4023-8
5. Yadgarov A, Dentice K, Aljabi Q. Real-world outcomes of canaloplasty and trabeculotomy combined with cataract surgery in eyes with all stages of open-angle glaucoma. Clin Ophthalmol. 2023;17:2609–2617. doi:10.2147/OPTH.S422132
6. Dickerson Jr JE, Harvey AE, Brown RH. Ab interno canaloplasty and trabeculotomy outcomes for mild, moderate, and advanced open-angle glaucoma: a ROMEO analysis. Clin Ophthalmol. 2024;18:1433–1440. doi:10.2147/OPTH.S464233
7. Wecker T, Anton A, Neuburger M, Jordan JF, van Oterendorp C. Trabeculotomy opening size and IOP reduction after trabectome® surgery. Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1643–1650. doi:10.1007/s00417-017-3683-0
8. American Academy of Ophthalmology. IRIS Registry Data Analysis. Available from: https://www.aao.org/iris-registry/data-analysis/requirements.
9. Radcliffe NM, Harris J, Garcia K, Zwick E, Chang RT, Mbagwu M. Standalone canaloplasty and trabeculotomy using the OMNI surgical system in eyes with primary open-angle glaucoma: a 36-month analysis from the American academy of ophthalmology IRIS® registry (Intelligent Research in Sight). Am J Ophthalmol. 2025;271:436–444. doi:10.1016/j.ajo.2024.12.015
10. Crabb DP, Saunders LJ, Edwards LA. Cases of advanced visual field loss at referral to glaucoma clinics - more men than women? Ophthalmic Physiol Opt. 2017;37(1):82–87. doi:10.1111/opo.12328
11. Buys YM, Gaspo R, Kwok K. Referral source, symptoms, and severity at diagnosis of ocular hypertension or open-angle glaucoma in various practices. Can J Ophthalmol. 2012;47(3):217–222. doi:10.1016/j.jcjo.2012.03.031
12. Jones PR, Philippin H, Makupa WU, Burton MJ, Crabb DP. Severity of visual field loss at first presentation to glaucoma clinics in England and Tanzania. Ophthalmic Epidemiol. 2020;27(1):10–18. doi:10.1080/09286586.2019.1661499
13. Landers J, Goldberg I, Graham S. Does a family history of glaucoma affect disease severity at the time of diagnosis? J Glaucoma. 2003;12(1):31–35. doi:10.1097/00061198-200302000-00006
14. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the early manifest glaucoma trial. Arch Ophthalmol. 2002;120(10):1268–1279. doi:10.1001/archopht.120.10.1268
15. American Academy of Ophthalmology. Primary Open-Angle Glaucoma: Preferred Practice Pattern. San Francisco: American Academy of Ophthalmology; 2020.
16. European Glaucoma Society. Terminology and Guidelines for Glaucoma.
17. Kyari F. A toolkit for glaucoma management in Sub-Saharan Africa. Available from: https://www.licht-fuer-die-welt.at/app/uploads/sites/8/2021/09/en_glaucoma-toolkit_final_editable_pages.pdf.
18. Chansangpetch S, Ittarat M, Yang S, et al. Comparison of 1-year effectiveness of trabecular microbypass stent implantation (iStent) in conjunction with phacoemulsification among mild, moderate, and severe primary open-angle glaucoma patients. J Glaucoma. 2020;29(7):542–549. doi:10.1097/IJG.0000000000001542
19. Bleeker AR, Litchfield WR, Ibach MJ, et al. Short-term efficacy of combined ab interno canaloplasty and trabeculotomy in pseudophakic eyes with open-angle glaucoma. Clin Ophthalmol. 2022;16:2295–2303. doi:10.2147/OPTH.S367896
20. Vold SD, Williamson BK, Hirsch L, et al. Canaloplasty and trabeculotomy with the OMNI system in pseudophakic patients with open-angle glaucoma: the ROMEO study. Ophthalmol Glaucoma. 2021;4(2):173–181. doi:10.1016/j.ogla.2020.10.001
21. Williamson BK, Vold SD, Campbell A, et al. Canaloplasty and trabeculotomy with the OMNI system in patients with open-angle glaucoma: two-year results from the ROMEO study. Clin Ophthalmol. 2023;17:1057–1066. doi:10.2147/OPTH.S407918
22. Murphy JT, Terveen DC, Aminlari AE, Dhamdhere K, Dickerson Jr JE. A multicenter 12-month retrospective evaluation of canaloplasty and trabeculotomy in patients with open-angle glaucoma: the ROMEO 2 study. Clin Ophthalmol. 2022;16:3043–3052. doi:10.2147/OPTH.S384105
23. Klabe K, Kaymak H. Standalone trabeculotomy and viscodilation of Schlemm’s canal and collector channels in open-angle glaucoma using the OMNI surgical system: 24-month outcomes. Clin Ophthalmol. 2021;15:3121–3129. doi:10.2147/OPTH.S325394
24. Zhu D, Shah P, Zhang C, et al. Standalone canaloplasty and trabeculotomy using the OMNI surgical system in patients with open-angle glaucoma: a systematic review and meta-analysis. J Glaucoma. 2025. doi:10.1097/IJG.0000000000002616
25. Rothman AL, Chang TC, Lum F, Vanner EA. Intraocular pressure changes following stand-alone phacoemulsification: an IRIS® registry analysis. Am J Ophthalmol. 2023;245:25–36. doi:10.1016/j.ajo.2022.09.006
26. Mbagwu M, Chapman R, Garcia K, Masseria C, Dickerson J, Cantor LB. Ab interno minimally invasive glaucoma surgery combined with cataract surgery and cataract surgery alone: IRIS® registry study. AJO International. 2024;1(2):100015. doi:10.1016/j.ajoint.2024.100015
27. Yang SA, Ciociola EC, Mitchell W, et al. Effectiveness of microinvasive glaucoma surgery in the United States: intelligent research in sight registry analysis 2013-2019. Ophthalmology. 2023;130(3):242–255. doi:10.1016/j.ophtha.2022.10.021
28. Creagmile J, Kim WI, Scouarnec C. Hydrus microstent implantation with OMNI surgical system ab interno canaloplasty for the management of open-angle glaucoma in phakic patients refractory to medical therapy. Am J Ophthalmol Case Rep. 2023;29:101749. doi:10.1016/j.ajoc.2022.101749
29. Pershing S, Lum F. The American academy of ophthalmology IRIS registry (Intelligent research in sight): current and future state of big data analytics. Curr Opin Ophthalmol. 2022;33(5):394–398. doi:10.1097/ICU.0000000000000869
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Canaloplasty and Trabeculotomy Combined with Phacoemulsification for Glaucoma: 12-Month Results of the GEMINI Study
Gallardo MJ, Pyfer MF, Vold SD, Sarkisian SR Jr, Campbell A, Singh IP, Flowers B, Dhamdhere K
Clinical Ophthalmology 2022, 16:1225-1234
Published Date: 21 April 2022
A Multicenter 12-Month Retrospective Evaluation of Canaloplasty and Trabeculotomy in Patients with Open-Angle Glaucoma: The ROMEO 2 Study
Murphy III JT, Terveen DC, Aminlari AE, Dhamdhere K, Dickerson Jr JE
Clinical Ophthalmology 2022, 16:3043-3052
Published Date: 14 September 2022
Canaloplasty and Trabeculotomy with the OMNI System in Patients with Open-Angle Glaucoma: Two-Year Results from the ROMEO Study
Williamson BK, Vold SD, Campbell A, Hirsch L, Selvadurai D, Aminlari AE, Cotliar J, Dickerson Jnr JE
Clinical Ophthalmology 2023, 17:1057-1066
Published Date: 6 April 2023
Prospective Study of Canaloplasty and Trabeculotomy Performed by Trainees
Smith AK, Kwan CC, Fox A, Noh S, Gustafson K, Lin KY, Mosaed S
Clinical Ophthalmology 2024, 18:17-26
Published Date: 3 January 2024
Real-World Outcomes of Combined Phacoemulsification and STREAMLINE® Canaloplasty: Interim Analysis of a Longitudinal Single-Center Retrospective Study
Stanke J, Nguyen D
Clinical Ophthalmology 2025, 19:1331-1337
Published Date: 19 April 2025