Back to Journals » Clinical Ophthalmology » Volume 18
Prospective Study of Canaloplasty and Trabeculotomy Performed by Trainees
Authors Smith AK ![]() , Kwan CC, Fox A, Noh S, Gustafson K, Lin KY
, Kwan CC, Fox A, Noh S, Gustafson K, Lin KY ![]() , Mosaed S
, Mosaed S
Received 25 September 2023
Accepted for publication 20 November 2023
Published 3 January 2024 Volume 2024:18 Pages 17—26
DOI https://doi.org/10.2147/OPTH.S441834
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Andrew K Smith,1– 3 Changyow C Kwan,1– 3 Austin Fox,1– 3 Stephanie Noh,1– 3 Kevin Gustafson,1– 3 Ken Y Lin,1,2,4 Sameh Mosaed1,2
1School of Medicine, University of California, Irvine, CA, USA; 2Department of Ophthalmology, Gavin Herbert Eye Institute, Irvine, CA, USA; 3Department of Ophthalmology, Tibor Rubin Veteran Affairs Medical Center, Long Beach, CA, USA; 4Department of Biomedical Engineering, University of California, Irvine, CA, USA
Correspondence: Andrew K Smith, Gavin Herbert Eye Institute, University of California, 850 Health Sciences Road, Irvine, CA, 92697-4375, USA, Tel +1-949-824-7944, Fax +1-949-824-2073, Email [email protected]
Purpose: To evaluate outcomes of new adopters of the OMNI® Surgical System (Sight Sciences, Inc.) by prospectively evaluating intermediate-term outcomes of patients operated by trainees.
Patients and Methods: This was a prospective study of surgeries performed by trainees on patients with open angle glaucoma undergoing simultaneous cataract surgery and ab interno canaloplasty and trabeculotomy using the OMNI Surgical System. Pre-operative intraocular pressure (IOP) and number of glaucoma medications were recorded. Only patients with a minimum of 6-month follow up were included. Baseline IOP was used to separate subjects into two groups: Group 1 (IOP ≥ 18 mmHg) and Group 2 (IOP < 18 mmHg). Mean decrease in IOP and medications was calculated and compared with paired t-tests for the overall sample as well as the subgroups. Success was defined as those with a ≥ 20% reduction from pre-operative IOP or with an IOP ≤ 18 mmHg and ≥ 6 mmHg and on the same or fewer number of medications while not requiring additional surgery. Adverse events were also recorded.
Results: Forty-two eyes of 31 patients were included. Mean pre-operative IOP was 17.2 ± 4.8 mmHg and mean number of medications was 2.4 ± 1.2. The primary endpoint was reached in 83.3% of patients at 12 months. IOP was reduced by 22.3% to 13.4 ± 2.4 (p< 0.001). Mean number of medications decreased to 1.7 ± 1.6 (p< 0.001). Group 1 mean IOP decreased 35.4% from 22.2 ± 4.6 mmHg to 14.3 ± 2.8 mmHg (p< 0.001). Group 2 mean number of medications decreased from 2.3 ± 1.1 to 1.6 ± 1.5 (p< 0.001).
Conclusion: When operated on by the novice MIGS surgeon, the OMNI device provides effective IOP and glaucoma medication reduction with minimal adverse events. Efficacy and safety of the device in the hands of trainees was comparable to experienced glaucoma surgeons suggesting its ease of adoption.
Keywords: OMNI, canaloplasty, trabeculotomy, goniotomy, MIGs, minimally invasive glaucoma surgeries
Introduction
Minimally invasive glaucoma surgeries (MIGs) have provided relatively safe and efficacious interventions to lower intraocular pressure (IOP) in the treatment of glaucoma.1 Numerous devices have come to market that target the conventional outflow system and offer lower-risk interventions for glaucoma patients as compared to traditional glaucoma surgery.2, 3
One such device is the OMNI® Surgical System. The OMNI is a device developed to perform ab interno microcatheterization and transluminal viscodilation of Schlemm’s canal (SC; canaloplasty) followed by ab interno transluminal trabeculotomy (goniotomy or trabeculotomy).4–9 The device addresses outflow resistance at the level of the collector channels (CC), SC, and the trabecular meshwork (TM). To perform ab interno canaloplasty and trabeculotomy with this device, the surgeon need only to access the SC through the TM, and the device self-directs along SC as it is advanced via a control wheel on the handpiece to complete the procedure.
The OMNI has been shown to be safe and effective as a standalone procedure as well as when it is used in conjunction with cataract surgery.5–9 The prospective multi-center GEMINI trial and retrospective ROMEO studies established the efficacy of the procedure, reporting 12-month success rates of 76% and 73%, respectively.6, 9 More recently, the ROMEO study showed similar success rates after 24 months of follow up.7 In these studies however, the procedures were performed by experienced glaucoma surgeons with years-long exposure to MIGS, and little is known about the learning curve of adopting this procedure. Outcomes of other glaucoma surgeries such as trabeculectomy have been shown to vary depending on surgeon experience.10,11 Although MIGS procedures have become increasingly popular, some devices are still dependent on surgical skill, individual surgeon technique, and experience in order to be utilized effectively. We hypothesized that new adopters of the OMNI would have similar outcomes to seasoned glaucoma surgeons based on the self-directed deployment of the device once SC has been entered.
Materials and Methods
This was a prospective study that was approved by the Institutional Review Board at the Veteran Affairs Hospital in Long Beach, California, and adhered to the Declaration of Helsinki. All patients underwent cataract surgery with intraocular lens implantation combined with ab interno canaloplasty and trabeculotomy with the OMNI and informed consent was obtained from all participants. Procedures were performed between March 2022 and February 2023. Patients with ocular hypertension, mild to severe open angle glaucomas, including those with pseudoexfoliation and pigmentary glaucoma, were included; however, 90.4% of patients had a diagnosis of primary open angle glaucoma. Patients were excluded if they had any prior intraocular surgery or prior laser trabeculoplasty procedures. Patients were also excluded if they did not complete at least 6 months of follow up. All patients were included regardless of degrees of canaloplasty and trabeculotomy performed.
Pre-operative Assessment
All patients underwent a complete pre-operative examination within 30 days of surgery which included best-corrected visual acuity (BCVA), IOP measurement using Goldmann applanation tonometry, un-dilated gonioscopy, and dilated fundus examination. All patients were deemed to have a visually significant cataract before surgery. Each patient was required to have open angles based on the gonioscopic exam (Shaffer grade 3 or 4) to be included. The IOP measurement and the number of ocular hypotensive medications in use at this appointment were recorded as the patient’s pre-operative baseline. Patients’ medical charts were reviewed and each patient’s age, sex and ethnicity were recorded.
Procedure in Detail
All surgeries in this study were performed by ophthalmology residents or ophthalmologists completing a fellowship year in glaucoma. No trainee had prior intraoperative experience with the OMNI. Each trainee was required to complete a single wet-lab where they practiced on a model eye with a representative from Sight Sciences before performing surgery on a patient.
After cataract extraction with intraocular lens implantation was completed intracameral Acetylcholine Chloride was administered. Next, the microscope was tilted approximately 30 degrees away from the surgeon sitting temporally, the patient’s head was rotated away from the surgeon, and a goniolens was placed on the cornea. The OMNI handpiece was introduced through the main clear corneal incision toward the nasal TM. A small goniotomy was made with the tip of the device, the catheter was inserted into SC, and advanced using the gear wheel on the handpiece. As the catheter was retracted into the device, viscoelastic was injected to perform viscodilation of SC. The catheter was then re-introduced into SC through the original goniotomy site and advanced again to the full extent of the catheter. As the device was removed from the clear corneal incision, the ab interno trabeculotomy was completed. The degrees of treatment of the outflow system was left to the discretion of the surgeon, but was typically 180 degrees. After completion, viscoelastic was then removed from the eye and water-tight closure of the incisions as typically performed after cataract surgery was accomplished. Patients were treated with topical moxifloxacin and prednisolone acetate four times per day for one week, after which the antibiotic was discontinued and the steroid was tapered by one drop per week for a total treatment of one month. Glaucoma medications were adjusted post-operatively to maintain individual target IOP.
Statistical Analysis
Patients were followed for 6 to 12 months after surgery. Post-operative IOP was recorded at months 1, 3, 6, 9, and 12. Number of medications and BCVA were recorded at the patient’s last visit. Mean IOP and number of medications were calculated. The mean percent change of IOP was calculated for post-operative months 1, 3, 6, 9, and 12. Percent change in the number of medications was also calculated. Paired t-tests were run to compare pre- and post-operative mean IOP and number of medications. The percentage of patients with post-operative BCVA worse than pre-operative BCVA as well as those with post-operative BCVA of 20/30 or better were calculated. Lastly, all charts were reviewed for the intraoperative and post-operative adverse events and their rates were calculated.
At 12 months, success in meeting the primary endpoint was defined as those with ≥20% reduction from pre-operative IOP or those with an IOP ≤18 mmHg and ≥6 mmHg on the same or fewer number of ocular hypotensive medications compared to baseline. Additionally, if patients required further glaucoma surgery, they were not considered to meet the primary success endpoint. Patients were then divided into those who had a pre-operative IOP ≥18 mmHg (Group 1) and those who had a pre-operative IOP <18 mmHg (Group 2). Again, mean IOP and number of medications were calculated and compared using paired t-tests. The number and percentage of patients meeting the primary success endpoint was calculated for Group 1 and Group 2. A more stringent primary end point was used for Group 2. Subjects were required to have ≥20% reduction in IOP or reduce at least one glaucoma medication to meet the primary end point.
Results
There were 44 eyes of 33 patients who met inclusion criteria. Two patients who had enrolled 1 eye each in the study were lost to follow-up and were excluded, leaving 42 eyes of 31 patients for analysis. Group 1 consisted of 15 eyes from 12 patients while Group 2 included 27 eyes from 21 patients. Mean age of the cohort was 72.5-years-old and all patients were male (Table 1). Patients with primary open angle glaucoma made up 90.4% of subjects. There were 15 patients who identified as White (35.7%), 19 patients who identified as African American (45.2%), 3 patients who identified as Hispanic (7.1%), 1 patient who identified as Asian (2.4%), and 4 declined to answer (9.5%).
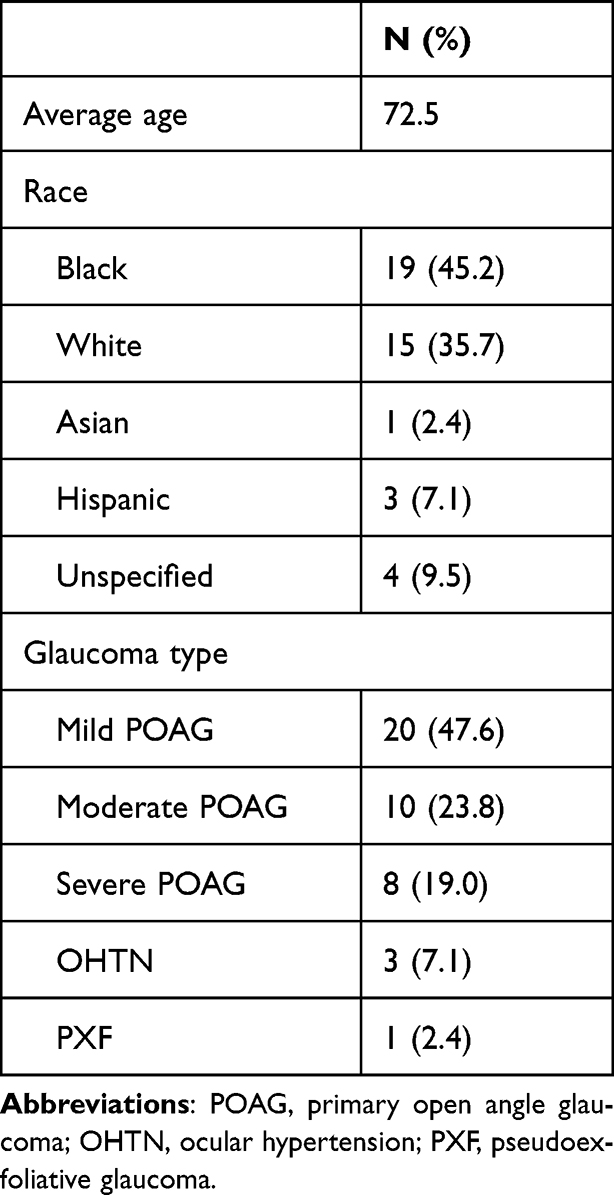 |
Table 1 Patient Demographics |
Mean pre-operative IOP was 17.2 ± 4.8 mmHg and mean number of medications was 2.4 ± 1.2. At post-operative month 6, IOP declined 21.3% to 13.5 ± 2.5 mmHg (p<0.001), and by post-operative month 12, IOP decreased 22.3% to 13.4 ± 2.4 (p<0.001; Figure 1). At 12 months, mean number of medications decreased by 28.0% to 1.7 ± 1.6 (p<0.001; Figure 2). At 12 months, 83.3% of patients met the primary endpoint, and 1 patient required additional glaucoma surgery.
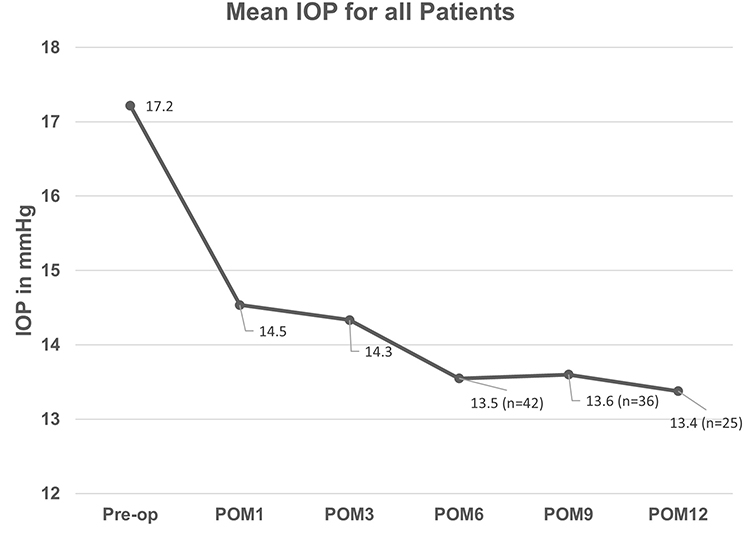 |
Figure 1 Mean IOP for all patients over time. Abbreviations: IOP, intraocular pressure; POM, post-operative month. Note: Mean IOP for all patients pre-operatively and at each follow up visit. |
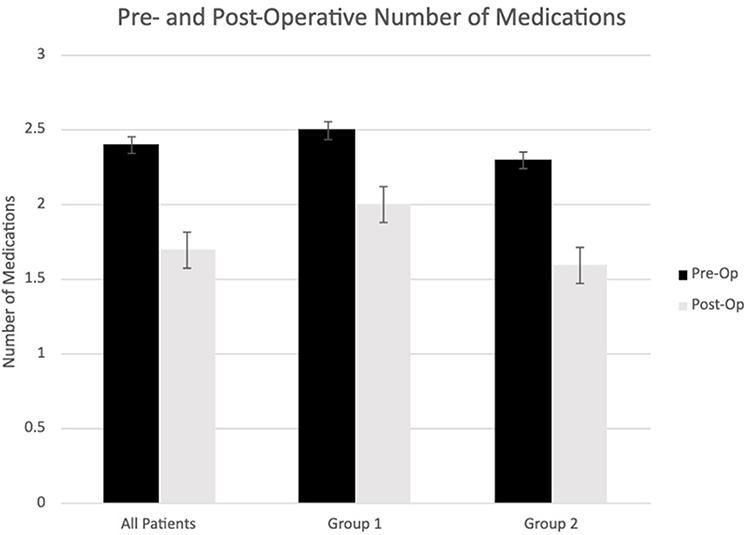 |
Figure 2 Pre- and post-operative number of medications. Notes: Mean number of ocular hypotensive medications pre-operatively and at 12 months post-operative for all patients, Group 1 (baseline IOP ≥18 mmHg) and Group 2 (baseline IOP <18 mmHg). Error bars represent standard error. |
Group 1 had a mean pre-operative IOP of 22.2 ± 4.6 mmHg and mean number of medications was 2.5 ± 1.5. At post-operative month 6, IOP was reduced by 36.5% to 14.1± 2.1 mmHg (p<0.001), and by post-operative month 12, IOP decreased by 35.4% to 14.3 ± 2.8 mmHg (p < 0.001; Figure 3). At 12 months, mean number of medications also decreased to 2.0 ± 1.8 (p = 0.07; Figure 2). In Group 1, 86.7% of patients met the primary endpoint and all patients had a decrease in IOP ≥20% at 6 months. Additionally, 33.3% of patients were able to decrease the number of medications used by at least 1 ocular hypotensive medication. At 12 months, there were 2 patients (13.3%) who did not have an IOP decrease of ≥20%. Of those 2 patients, 1 patient required additional glaucoma surgery. The patient requiring surgery had an initial decrease in IOP from 18 mmHg to 13 mmHg after 6 months; however, the IOP increased to 18 mmHg after 12 months and he subsequently underwent trabeculectomy.
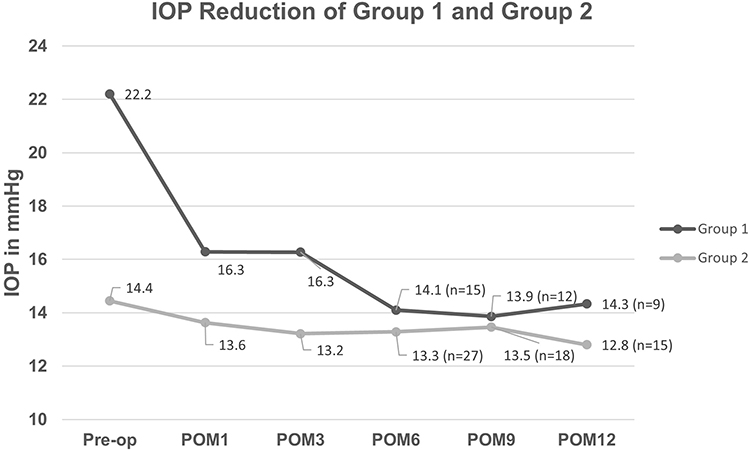 |
Figure 3 IOP of group 1 and group 1 over time. Abbreviations: IOP, intraocular pressure; POM, post-operative month. Notes: Mean IOP pre-operatively and at each follow up visit for group 1 (baseline IOP ≥18mmHg) and group 2 (baseline IOP < 18mmHg). Error bars represent standard error. |
Group 2 had a mean pre-operative IOP of 14.4 ± 1.8 mmHg and mean number of medications of 2.3 ± 1.1. At post-operative month 6, IOP was reduced by 8.0% to 13.3 ± 2.7 mmHg (p = 0.04), and by post-operative month 12, IOP decreased 11.4% to 12.8 ± 2.0 (p = 0.007; Figure 3). At 12 months, mean number of medications also decreased 32.3% to 1.6 ± 1.5 (p<0.001; Figure 2). In Group 2, 88% of patients met the more stringent primary endpoint of either achieving ≥ 20% reduction in IOP or decreasing at least one ocular hypotensive medication. Furthermore, 63% of patients were able to decrease at least one ocular hypotensive medication. Additionally, 37% of patients in Group 2 were no longer taking medication after surgery. No patient required additional surgery.
Safety
The adverse events of the procedure were recorded for each eye regardless of causation (i.e., cataract extraction vs. OMNI procedure). The reported adverse events can be found in Table 2. All patients had an improvement in vision from baseline and 87% of patients had a BCVA of 20/30 or better. A posterior capsular tear occurred in 1 eye (2.4%) requiring anterior vitrectomy and sulcus intraocular lens placement, and 1 eye (2.4%) had post-op macular edema that resolved with topical anti-inflammatory drops. Transient hyphema occurred in 2 eyes (4.8%) in the early post-operative period that resolved by the week 1 visit. Both measured less than 1 mm, and neither were associated with IOP elevations. An IOP spike occurred in 1 eye (2.4%) which resolved after re-starting topical medications. A focal iridodialysis occurred in 2 eyes (4.8%), which were asymptomatic and not visible without slit lamp biomicroscopy. There were no incidences of cyclodialysis cleft formation or hypotony.
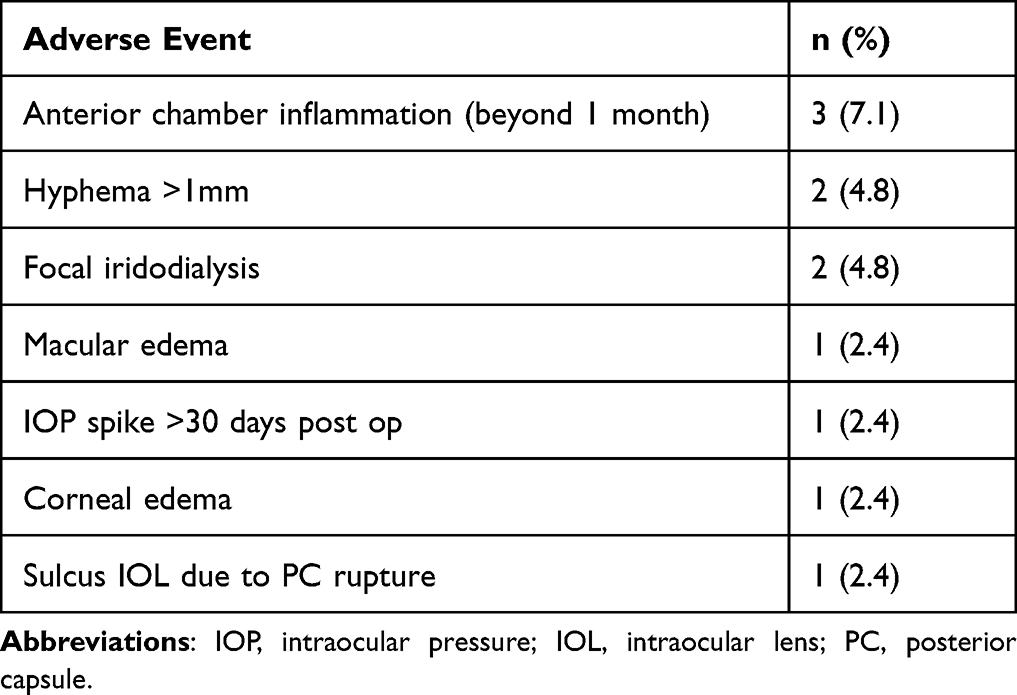 |
Table 2 Number and Frequency of Adverse Events |
Discussion
The introduction of numerous MIGs devices has provided a diverse set of options for safe and efficacious surgical interventions of the conventional aqueous outflow system.1,2,12 Results from our study, where procedures were performed by trainees, essentially reproduced the success rates of the pivotal GEMINI trial and ROMEO studies.5–9 In the prospective GEMINI trial, Gallardo et al showed that 84.2% of those undergoing ab interno viscodilation and trabeculotomy in conjunction with cataract surgery achieved an IOP reduction over 20% after 12 months of follow up.9 In this study, the pre-operative mean IOP was 23.8 ± 3.1 mmHg which decreased 38% and 35% at 6 and 12 months respectively.8,9 This was similar to Group 1 in the current study who had a pre-operative mean IOP of 22.2 ± 4.6 mmHg and experienced a 36.5% reduction in IOP at 12 months. At 12 months follow up in the ROMEO study, mean IOP decreased 28% and 33% for those with a baseline IOP > 18 mmHg who underwent the procedure in conjunction with cataract surgery and as a standalone respectively.5,6 Moreover, 80.2% of patients undergoing simultaneous cataract surgery and 72.9% of patients having a standalone procedure met the primary end point.5,6 Similar results were also seen for both groups with 2-year follow up data reported in the recent ROMEO 2 study.7 When the same procedure was performed by trainees in this study, 83.3% met the same primary endpoint.
There are several other recent retrospective case series demonstrating outcomes of OMNI surgery performed by different groups using similar success criteria.13–19 Yadgarov et al retrospectively reviewed 171 eyes with similar mean age and glaucoma severity to patients in our study, with baseline IOP of 17.2 mmHg which was reduced to 14.3 ± 5.5 mmHg after 12 months of follow up. Toneatto et al report a success rate of 67.9% in a series of 30 eyes undergoing combined cataract extraction and ab interno canaloplasty with the OMNI device.16 In this study however, a stricter success criterion was used defined as ≥25% reduction in mean IOP and a final IOP ≤ 18 mmHg on the same or fewer medications. Furthermore, Hughes and Traynor report an IOP reduction of 36% in a retrospective series of 89 patients where 41 patients reached the 12-month follow-up period.17 Klabe and Kaymak report a 40% IOP reduction in a retrospective series of 30 eyes receiving canaloplasty alone that were followed for 12 months.18 All of these studies share similar success rates or IOP reductions compared to our group of patients who were operated on by trainees, thus supporting the theory that this device has a small learning curve that does not compromise efficacy in the hands of novice surgeons.
Reduction in the number of glaucoma medications was also comparable to prior studies that were performed by experienced glaucoma surgeons. 63.0% of patients in Group 2 whose baseline IOP was <18 mmHg were able to reduce at least one glaucoma medication. Of those with IOP ≤ 18 mmHg in the ROMEO study, 52.8% were able to reduce at least one glaucoma medication.6 There are however, other reports showing a larger decrease in glaucoma medication use as compared to our study. Klabe and Kaymak reported that 84.6% of patients reduced at least one glaucoma medication after 24 months of follow up.18 Gallardo et al showed an 80% decrease in medication use from 1.9 ± 0.9 to 0.4 ± 0.9.9 By contrast, this study showed a more modest decrease in medication use from 2.4 ± 1.2 to 1.7 ± 1.6. This may be secondary to the patients in our study population having a higher baseline number of medications, without having undergone a baseline washout period, unlike the prior studies, which might indicate more severe glaucoma and less margin to reduce medication use.
Our study also showed that the adverse event rates were similar to other prior published studies from experienced glaucoma surgeons.5–9 The most common adverse event associated with angle-based MIGS is hyphema, although this phenomenon is expected, physiologic, and typically transient. Hence microhyphemas are often not recorded as adverse events. However, some hyphema are associated with significant IOP elevation and may require additional medications or surgery to alleviate. In some series published on the OMNI procedure, the rates of hyphema have been reported to be as high as almost 50%.19 A recent study by Grabska-Liberek et al reported that 6 out of 17 eyes treated developed hyphema and 50% of those required anterior chamber washout for uncontrolled IOP resulting from the hyphema. Still another series by Toneatto et al reported that 2.5% of subjects required anterior chamber washout for hyphema with or without IOP elevation.16 In the ROMEO study, 2.5% of patients undergoing combined cataract surgery and 4.2% of patients undergoing the procedure as a standalone experienced a hyphema.5,6 Similarly, the GEMINI study reported a hyphema rate of 6%.9 In our study, 4.8% of patients had hyphema, none of whom experienced an IOP spike or required anterior chamber washout.
IOP spikes have also been noted to occur in the absence of hyphema. In the ROMEO and GEMINI studies, 5% and 2% of patients experienced an IOP spike respectively.7,9 In our study one patient experienced an IOP spike at post-operative week one which was thought to be secondary to medication noncompliance and resolved after the patient restarted the same topical glaucoma medications taken prior to surgery.
Other potential risks of angle-based MIGS surgery include inadvertent damage to the cornea, iris, and other nearby structures with any device in the angle paired with an inexperienced gonio-surgeon.12,20,21 This includes the possibility of creating an inadvertent cyclodialysis cleft with resultant hypotony. This complication has been reported with the OMNI procedure and a recent retrospective case series.22 Yadgarov et al reported a hypotony rate of 1.2% with 0.6% cyclodialysis cleft formation.13 Additionally, 1 patient in the ROMEO study experienced a cyclodialysis cleft.7 In our study, there were no cases of post-operative hypotony or cyclodialysis cleft formation, however two patients (4.8%) did experience focal iridodialysis. These were asymptomatic and only visible with slit lamp biomicroscopy. It is unclear if these occurred via forceful or inadvertent iris root manipulation with entry through the TM, or during the trabeculotomy portion of the procedures. Transient corneal edema occurred in 1 patient (2.4%) after 1 week which resolved after one month; this however may likely have been a result of the phacoemulsification portion of the procedure. Corneal edema, cystoid macular edema and anterior chamber inflammation rates were also similar compared to other prior studies.5–7 While the additional risk of infection also exists with any intraocular procedure, no cases of endophthalmitis have yet been reported after the OMNI procedure, nor were they encountered in our study. Lastly, one posterior capsular tear (2.4%) occurred during the cataract portion of the surgery in this study, and after anterior vitrectomy and sulcus intraocular lens placement, the canaloplasty and trabeculotomy portions of the case were able to be executed without incident.
These results stand in contrast to outcomes and adverse events of trabeculectomy which have been shown to be less favorable in inexperienced hands.6, 7 Adverse events for surgeons who perform more trabeculectomies are reported to be less than those who perform trabeculectomies infrequently.10 Furthermore, the risk of failure of trabeculectomies has been linked to inexperienced or non-glaucoma surgeons performing the procedure.11 When performed by resident physicians with attending physician supervision, success rates of trabeculectomy are comparable to attending physicians; however the rates of adverse events and additional surgery were higher in resident groups.22, 23 Similarly, outcomes of tube shunt surgery performed by residents and attendings were comparable though resident physicians had longer intraoperative times.24 Regarding angle-based implants, a retrospective case series of 31 patients showed that results of microstent iStent placement were similar between resident and attending physicians.25
While the trabeculectomy surgery is a multi-stepped surgery dependent on the skill of the surgeon during the surgery and post-operative management, performing ab interno canaloplasty and trabeculotomy with the OMNI device is relatively straightforward. Post-operative management is fairly standardized in comparison to trabeculectomy as scleral flap management via laser suture lysis or releasable sutures, 5-FU injections, aggressive steroid regimens, digital massage, and bleb needling are not required. There is little-to-no difference in the post-operative management of cataract surgery alone and cataract surgery accompanied by canaloplasty and trabeculotomy with the OMNI. During the surgery, once the catheter accesses SC, the device self-directs to complete the procedure requiring little variation in technique from the surgeon. Additionally, once the canal is properly accessed, the catheter typically deploys without resistance, indicating to the surgeon that the device is in the proper location. If any resistance is encountered, this suggests that the catheter is not in the proper orientation, or is detouring out of the canal, signaling to the surgeon to cease deployment and retract the catheter. The fact that almost no modification of the technique is possible also allows for a standardized approach, minimizing variations in individual surgeon techniques. This is in contrast to implant-based MIGS devices where the implants can be either superficially lodged into trabecular tissue, iris root, and other incorrect locations without significant feedback to the surgeon.26,27
The learning curve of this procedure may be more manifest not with patient outcomes, but perhaps with gonioscopy-related metrics. The inexperienced surgeon needs more time to develop intraoperative gonioscopy skills in order to be efficient with gonio-based surgery. This involves understanding what angle to rotate the patient’s head and microscope depending on the anatomy and presentation of each individual eye, understanding how to coordinate goniolens movements to pair with alternate-hand manipulations, how much pressure to apply in order to couple with the cornea and not create corneal striae, how to modify the gonioscopic view based on which specific lens is offered at the surgical center, etc. Models for practicing angle based glaucoma surgery using cadaveric corneoscleral rims have been shown to be an effective way to introduce and enhance the skill sets needed for gonio-based surgeries.28–30 Specifically, the amount of time to perform goniotomy procedures improved after practicing with the model.28 A study by Dang et al using an ex vivo pig-eye model for gonioscopic surgery found that trainees’ surgical times decreased by 1.4 minutes with each subsequent eye, reducing total operative times from 25 minutes with the first procedure to 5 minutes at the end of the training.31 Unfortunately, since our series included simultaneous cataract surgery also being performed by trainees, this compounded the variables, and this particular metric was not analyzed.
This study is not without limitations. Firstly, this study examines the outcomes and adverse events of trainees supervised by attending physicians and does not represent outcomes for new adopters outside the academic setting where no trained coaching is available. While no rescue maneuvers performed by the attending physician were required in any case, trainees benefit from the supervision and coaching of an experienced glaucoma surgeon. Second, this study was limited by a sample population that lacked diversity. All patients were male which is not unexpected as the study was completed at a Veteran Affairs Hospital where a majority of patients are male. Additionally, the patients overwhelmingly carried a diagnosis of primary open angle glaucoma and results may vary for those with secondary open angle glaucomas, or eyes with atypical angle anatomy. Lastly, this study did not evaluate surgical time as an outcome for novice surgeons. A follow-up study measuring the amount of time required to perform individual MIGS procedures compared to trained surgeons would also be an interesting metric to further evaluate the ease-of-adoption of individual devices.
Conclusion
This study shows that trainees with no prior experience using the OMNI device can expect outcomes similar to those of experienced glaucoma surgeons. Thus, the OMNI® Surgical System is a relatively straightforward device that is readily learned and utilized. When performed by new adopters such as trainees, IOP reduction and medication outcomes as well as rates of adverse events are comparable to seasoned glaucoma specialists. Further research can focus on following the learning curve of surgeons by evaluating improvement in outcomes as more experience is gained by specific surgeons as well as assessing outcomes of other MIGs devices for trainees and new adopters.
Data Sharing Statement
The authors do not intend to share the data of the participants. Requests should be directed to the corresponding author.
Disclosure
Research reported in this publication was supported by a grant from Sight Sciences Inc, who is the manufacturer of the OMNI® Surgical System, and an unrestricted grant from Research to Prevent Blindness to the Gavin Herbert Eye Institute at the University of California, Irvine. The authors report no other conflicts of interest.
References
1. Saheb H, Ahmed II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96–104. doi:10.1097/ICU.0b013e32834ff1e7
2. Ahmed II. MIGS and the FDA: what’s in a Name? Ophthalmology. 2015;122(9):1737–1739. doi:10.1016/j.ophtha.2015.06.022
3. Gedde SJ, Lind JT, Wright MM, et al. Primary Open-Angle Glaucoma Suspect Preferred Practice Pattern®. Ophthalmology. 2021;128(1):P151–P192. doi:10.1016/j.ophtha.2020.10.023
4. Brown RH, Tsegaw S, Dhamdhere K, Lynch MG. Viscodilation of Schlemm canal and trabeculotomy combined with cataract surgery for reducing intraocular pressure in open-angle glaucoma. J Cataract Refract Surg. 2020;46(4):644–645. doi:10.1097/j.jcrs.0000000000000107
5. Vold SD, Williamson BK, Hirsch L, et al. Canaloplasty and Trabeculotomy with the OMNI System in Pseudophakic Patients with Open-Angle Glaucoma: the ROMEO Study. Ophthalmol Glaucoma. 2021;4(2):173–181. doi:10.1016/j.ogla.2020.10.001
6. Hirsch L, Cotliar J, Vold S, et al. Canaloplasty and trabeculotomy ab interno with the OMNI system combined with cataract surgery in open-angle glaucoma: 12-month outcomes from the ROMEO study. J Cataract Refract Surg. 2021;47(7):907–915. doi:10.1097/j.jcrs.0000000000000552
7. Williamson BK, Vold SD, Campbell A, et al. Canaloplasty and Trabeculotomy with the OMNI System in Patients with Open-Angle Glaucoma: two-Year Results from the ROMEO Study. Clin Ophthalmol. 2023;17:1057–1066. doi:10.2147/OPTH.S407918
8. Gallardo MJ, Sarkisian SR, Vold SD, et al. Canaloplasty and Trabeculotomy Combined with Phacoemulsification in Open-Angle Glaucoma: interim Results from the GEMINI Study. Clin Ophthalmol. 2021;15:481–489. doi:10.2147/OPTH.S296740
9. Gallardo MJ, Pyfer MF, Vold SD, et al. Canaloplasty and Trabeculotomy Combined with Phacoemulsification for Glaucoma: 12-Month Results of the GEMINI Study. Clin Ophthalmol. 2022;16:1225–1234. doi:10.2147/OPTH.S362932
10. Wu G, Hildreth T, Phelan PS, Fraser SG. The relation of volume and outcome in trabeculectomy. Eye. 2007;21(7):921–924. doi:10.1038/sj.eye.6702340
11. Edmunds B, Bunce CV, Thompson JR, Salmon JF, Wormald RP. Factors associated with success in first-time trabeculectomy for patients at low risk of failure with chronic open-angle glaucoma. Ophthalmology. 2004;111(1):97–103. doi:10.1016/j.ophtha.2003.04.005
12. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
13. Yadgarov A, Dentice K, Aljabi Q. Real-World Outcomes of Canaloplasty and Trabeculotomy Combined with Cataract Surgery in Eyes with All Stages of Open-Angle Glaucoma. Clin Ophthalmol. 2023;17:2609–2617. doi:10.2147/OPTH.S422132
14. Bleeker AR, Litchfield WR, Ibach MJ, et al. Short-Term Efficacy of Combined ab Interno Canaloplasty and Trabeculotomy in Pseudophakic Eyes with Open-Angle Glaucoma. Clin Ophthalmol. 2022;16:2295–2303. doi:10.2147/OPTH.S367896
15. Gallardo MJ, Dhamdhere K, Dickerson JE. Canaloplasty and Trabeculotomy Ab Interno Combined with Cataract Surgery: 12-Month Outcomes in Hispanic Patients with Open-Angle Glaucoma. Clin Ophthalmol. 2022;16:905–908. doi:10.2147/OPTH.S358878
16. Toneatto G, Zeppieri M, Papa V, et al. 360° Ab-Interno Schlemm’s Canal Viscodilation with OMNI Viscosurgical Systems for Open-Angle Glaucoma-Midterm Results. J Clin Med. 2022;11(1):259. doi:10.3390/jcm11010259
17. Hughes T, Traynor M. Clinical Results of Ab Interno Canaloplasty in Patients with Open-Angle Glaucoma. Clin Ophthalmol. 2020;14:3641–3650. doi:10.2147/OPTH.S275087
18. Klabe K, Kaymak H. Standalone Trabeculotomy and Viscodilation of Schlemm’s Canal and Collector Channels in Open-Angle Glaucoma Using the OMNI Surgical System: 24-Month Outcomes. Clin Ophthalmol. 2021;15:3121–3129. doi:10.2147/OPTH.S325394
19. Grabska-Liberek I, Duda P, Rogowska M, et al. 12-month interim results of a prospective study of patients with mild to moderate open-angle glaucoma undergoing combined viscodilation of Schlemm’s canal and collector channels and 360° trabeculotomy as a standalone procedure or combined with cataract surgery. Eur J Ophthalmol. 2022;32(1):309–315. doi:10.1177/1120672121998234
20. Vinod K, Gedde SJ. Safety profile of minimally invasive glaucoma surgery. Curr Opin Ophthalmol. 2021;32(2):160–168. doi:10.1097/ICU.0000000000000731
21. Cantor L, Lindfield D, Ghinelli F, et al. Systematic Literature Review of Clinical, Economic, and Humanistic Outcomes Following Minimally Invasive Glaucoma Surgery or Selective Laser Trabeculoplasty for the Treatment of Open-Angle Glaucoma with or Without Cataract Extraction. Clin Ophthalmol. 2023;17:85–101. doi:10.2147/OPTH.S389406
22. Nilforushan N, Yadgari M, Astaraki A, Miraftabi A. Comparison of the long-term outcomes of resident versus attending performed trabeculectomy. J Curr Ophthalmol. 2017;29(3):169–174. doi:10.1016/j.joco.2017.02.002
23. Kwong A, Law SK, Kule RR, et al. Long-term outcomes of resident- versus attending-performed primary trabeculectomy with mitomycin C in a United States residency program. Am J Ophthalmol. 2014;157(6):1190–1201. doi:10.1016/j.ajo.2014.02.028
24. Thangamathesvaran L, Crane E, Modi K, Khouri AS. Outcomes of Resident-versus attending-performed Tube Shunt Surgeries in a United States Residency Program. J Curr Glaucoma Pract. 2018;12(2):53–58. doi:10.5005/jp-journals-10008-1245
25. Zheng CX, Copparam S, Lin MM, et al. Outcomes of trabecular microbypass surgery: comparison of resident trainees and attending surgeons. J Cataract Refract Surg. 2019;45(12):1704–1710. doi:10.1016/j.jcrs.2019.07.021
26. Gillmann K, Bravetti GE, Mermoud A, Mansouri K. A Prospective Analysis of iStent Inject Microstent Positioning: schlemm Canal Dilatation and Intraocular Pressure Correlations. J Glaucoma. 2019;28(7):613–621. doi:10.1097/IJG.0000000000001273
27. Gillmann K, Mansouri K, Ambresin A, Bravetti GE, Mermoud A. A Prospective Analysis of iStent Inject Microstent Implantation: surgical Outcomes, Endothelial Cell Density, and Device Position at 12 Months. J Glaucoma. 2020;29(8):639–647. doi:10.1097/IJG.0000000000001546
28. Pujari A, Rakheja V, Dada T, et al. Gonioscopy and Angle-Based Glaucoma Surgical Training on Human Eyes in the Wet Lab. J Glaucoma. 2022;31(10):839–845. doi:10.1097/IJG.0000000000002075
29. Nazarali S, Arora A, Ford B, et al. Cadaver corneoscleral model for angle surgery training. J Cataract Refract Surg. 2019;45(1):76–79. doi:10.1016/j.jcrs.2018.08.023
30. Arora A, Nazarali S, Sawatzky L, et al. K-RIM (Corneal Rim) Angle Surgery Training Model. J Glaucoma. 2019;28(2):146–149. doi:10.1097/IJG.0000000000001131
31. Dang Y, Waxman S, Wang C, et al. Rapid learning curve assessment in an ex vivo training system for microincisional glaucoma surgery. Sci Rep. 2017;7(1):1605. doi:10.1038/s41598-017-01815-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Canaloplasty and Trabeculotomy Combined with Phacoemulsification for Glaucoma: 12-Month Results of the GEMINI Study
Gallardo MJ, Pyfer MF, Vold SD, Sarkisian SR Jr, Campbell A, Singh IP, Flowers B, Dhamdhere K
Clinical Ophthalmology 2022, 16:1225-1234
Published Date: 21 April 2022
A Multicenter 12-Month Retrospective Evaluation of Canaloplasty and Trabeculotomy in Patients with Open-Angle Glaucoma: The ROMEO 2 Study
Murphy III JT, Terveen DC, Aminlari AE, Dhamdhere K, Dickerson Jr JE
Clinical Ophthalmology 2022, 16:3043-3052
Published Date: 14 September 2022
Canaloplasty and Trabeculotomy with the OMNI System in Patients with Open-Angle Glaucoma: Two-Year Results from the ROMEO Study
Williamson BK, Vold SD, Campbell A, Hirsch L, Selvadurai D, Aminlari AE, Cotliar J, Dickerson Jnr JE
Clinical Ophthalmology 2023, 17:1057-1066
Published Date: 6 April 2023
Real-World Outcomes of Combined Phacoemulsification and STREAMLINE® Canaloplasty: Interim Analysis of a Longitudinal Single-Center Retrospective Study
Stanke J, Nguyen D
Clinical Ophthalmology 2025, 19:1331-1337
Published Date: 19 April 2025
Standalone Canaloplasty and Trabeculotomy Using the OMNI Surgical System: A Subgroup Analysis from the American Academy of Ophthalmology IRIS® Registry (Intelligent Research in Sight)
Pyfer MF, Funke C, Mosaed S, Zwick E, Toth J, Garcia K, Radcliffe NM
Clinical Ophthalmology 2025, 19:4043-4052
Published Date: 1 November 2025