Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Staff Experiences in Managing Incidents in Nursing Homes: A Descriptive Qualitative Study
Authors Fauziningtyas R ![]() , Chong MC
, Chong MC ![]() , Setiawan HW, Tan MP
, Setiawan HW, Tan MP
Received 23 August 2023
Accepted for publication 30 October 2023
Published 9 November 2023 Volume 2023:16 Pages 3379—3392
DOI https://doi.org/10.2147/JMDH.S436766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Rista Fauziningtyas,1– 3,* Mei Chan Chong,1,* Herley Windo Setiawan,4 Maw Pin Tan5,*
1Department of Nursing Science, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Malaysia; 2Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia; 3Center of Excellence Patient Safety and Quality, Universitas Airlangga, Surabaya, Indonesia; 4Department of Pulmonology and Respiratory Medicine, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia; 5Department of Medicine, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Malaysia
*These authors contributed equally to this work
Correspondence: Mei Chan Chong, Department of Nursing Science, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, 50603, Malaysia, Tel +603-79492806, Email [email protected]
Introduction: Adverse incidents in nursing home (NH) may occur as the result of inadequate monitoring for signs of unobservable initial complications, medical errors, improper nursing interventions, lack of communication, and inadequate reporting.
Purpose: This study explores incident types, causes, handling, and documentation in Indonesian NHs through a qualitative approach.
Patients and Methods: In-depth interviews were conducted with 23 NH staff members, including managers, nurses, and support staff.
Results: Five themes and 17 sub-themes emerged, with falls and resident-to-resident abuse as common adverse incidents. Causes included older adults’ conditions, environment, and misunderstanding. Follow-up action included first aid, hospital referrals, and assertive communication. Adverse incidents were actively reported through verbal and written reports or WhatsApp groups. Reports and documentation remain unstructured, however, as there were no standard operating procedures regarding incident reporting, documentation, and the types of adverse incidents that staff should report.
Conclusion: Improvements in management, documentation, and reporting adverse incidents are highlighted in this research. Practitioners, nurses, and social workers should develop guidelines for handling, reporting, and documenting adverse incidents in NHs.
Plain Language Summary: This study aimed to explore adverse incidents and events in nursing homes (NHs) in Indonesia, particularly focusing on falls and resident-to-resident abuse (RRA). With a growing older adult population and an increasing demand for long-term-care (LTC) facilities, the study aimed to understand the types of adverse incidents, their causes, approaches for handling them, incident reporting, and documentation practices within NHs.
The study employed qualitative methods, conducting in-depth interviews with 23 staff members from four NHs in East Java, Indonesia. Falls and RRA were found to be the most commonly encountered adverse incidents. Falls were primarily caused by older adults’ physical conditions and environmental factors. Strategies for fall prevention included initial treatment, coordination with nursing staff, referrals to health services, and minimizing falls risk. RRA incidents were typically triggered by misunderstanding related to daily activities. Incident reporting methods varied, including verbal, written, and WhatsApp-based reporting, with varying levels of documentation practices.
The study underscores the need for effective incident management and prevention strategies in NHs. Falls and RRA are significant concerns that demand attention. The findings highlight the importance of standardized protocols, comprehensive reporting systems, and structured documentation practices to enhance the safety and well-being of older adults in NHs. These insights can inform the development of strategies to improve incident handling, thus improving the quality of care provided to older adults in LTC facilities.
Keywords: handling adverse incidents, reporting, fall, safety, older adult, quality of life
Introduction
As in other healthcare settings, adverse events and incidents related to safety issues are common in nursing homes (NHs). These incidents stem from various factors, including inadequate monitoring, unobservable initial complications, medical errors, improper nursing interventions, lack of communication, and incomplete patient reporting.1,2 The concept of safety is defined as a process that reduces the likelihood of adverse events or incidents. Adverse incidents or events are defined as harm occurring to a resident as the result of inadequacies in the care provision or environment. Unexpected death, falls, pressure ulcers, medication errors, and problems with nasogastric tubes are adverse incidents that are commonly reported in long-term care (LTC).3
Furthermore, there is a recognition that adverse incidents in NHs are often underreported, and mistakes resulting in severe adverse outcomes are reported more frequently than near-miss events. “Near-miss events” denote incidents that did not result in harm but held the potential to do so.4,5 Research on reporting adverse incidents in LTC has focused mainly on falls and medication errors.3
Despite the more organized approach to managing NH and LTC facilities in countries like the United States, there are still gaps in delivering adequate care.6 In 2014, the United States reported an average of 7.96 deficiencies in care per NH facility. These deficiencies cover a spectrum of issues, such as lapses in infection control, environmental safety, food sanitation, quality of care, and unnecessary drug use. It is crucial to recognize that deficiencies in care do not always directly signify adverse incidents or events; nevertheless, they can function as valuable indicators of potential hazards within a facility.7
One of the common frequently reported adverse incidents occurring in LCT facilities is falling.8 According to data from the World Health Organization (WHO) in 2021, falls account for an estimated 684,000 deaths globally each year, with more than 80% of these incidents occurring in low and middle-income countries. Among fatal falls, the highest number of cases is observed among individuals aged 60 years and older. Additionally, there are approximately 37.3 million falls each year that are severe enough to require medical attention.9
A study conducted in Indonesia in 2020, revealed that a significant proportion of older adults had experienced incidents of falls within the past 12 months. An overall prevalence 32.7% has been reported among older adults living in residential care facilities. Furthermore, the study found that 45.4% of older adults were at risk of falling, with higher rates observed among those residing in residential care facilities (50.5%) compared to those in the community (40.4%).10 It is worth noting, however, that this particular study only recorded a single type of incident, highlighting the need for further exploration of various adverse incidents occurring within NHs.
Nursing home services in Indonesia provide both social care services and rehabilitation services. Social care provisions within these settings are intended to fulfill physiological needs. These services, therefore, include nutrition, health, and hygiene. Housing services provide accommodation and other supporting facilities for residents, such as places of worship, sports and recreation rooms, and polyclinics for the older adults. Health services are provided to older adults for general check-ups (once a month) and care when residents are sick (slightly or seriously ill). In addition, necessities for healthy living, such as clean water and bathrooms, and the availability of health facilities, sanitation, and adequate air circulation, are provided by NHs. Rehabilitation services, on the other hand, are intended to create and change the residents’ physical, cognitive, and social behavior.11
As of 2021, Indonesia’s older adult population has reached 29.3 million, constituting 10.8% of the total population. Eight provinces within the country have entered an “aging population” phase, where more than 10% of the population comprises older adults.12 With this demographic shift, there’s a surging demand for LTC facilities. Both the government and private sector face the imperative of prioritizing the establishment of secure and high-quality facilities for the aging population in LTC settings. The delivery of safe and good quality services, measured through a reduced incidence of adverse incidents and events, hinges on the implementation of effective incident handling and prevention strategies.
The escalating number of older adults in Indonesia underscores the pressing need for LTC facilities. This demographic shift requires a concerted effort from both the government and private sector to prioritize the establishment of secure and high-quality facilities for the older adult in LTC settings. Achieving safe and quality services, as gauged by a diminished incidence of adverse incidents and events, heavily relies on the adept execution of incident handling and prevention strategies. However, the current dearth of comprehensive information regarding adverse incidents in NHs in Indonesia underscores the necessity of this study. The aims of this study are, therefore, to explore the firsthand experiences of staff members in NHs, shedding light on various aspects, including the types of adverse incidents, their potential root causes, approaches to handling them, incident reporting procedures, and documentation practices.
Materials and Methods
Design
This study employed descriptive qualitative methods to explore the experiences of staff dealing with adverse incidents in NHs. This design was chosen because it allowed researchers to use a pre-existing conceptual framework.13 The findings will then be presented in simple language that is easily understood by readers.
Setting and Participants
Four NHs were purposively selected from three municipalities with the highest number of NHs in East Java, Indonesia. East Java has the second highest number of older adults in Indonesia.12 In addition, East Java Province has 104 private NHs and 12 public NHs. Researchers chose two public NHs (government-owned) and two private NHs (managed by the private sector). The four NHs had nurses, nurse aides, and social workers as caregivers for residents. The four facilities varied in bed capacity and in the number of residents and staff. The total bed capacity ranged from 40 to 160 beds. Residents living in the four NHs had varying levels of dependency, from independent to totally dependent. Public NHs in Indonesia specialize in providing services to neglected older adults. These residents do not need to pay for any of the facilities in the NHs. Private NHs, however, provide services for the residents for a range of fees, from a full fee-waiver to full fees.
The participants involved in this study were all NH staff, including managers, nurses, social workers, physiotherapists, and administrative and support staff. Snowball sampling was used to select the participants. We contacted NH managers to recommend two to three potential participants, after which each participant would recommend another participant. The inclusion criteria for this study were that staff had worked at least three months in NHs, were full-time staff, and were willing to share their experiences regarding adverse incidents in NHs. Before the interview, written informed consent was obtained including the consent for audio recording and publication. A total of 23 NH staff were involved in this study.
Data Collection
Qualitative data collection was conducted through in-depth interviews to explore participants’ experiences regarding adverse incidents and errors in NHs. Each interview took 30 to 45 minutes conducted by first and third author. A total of four meetings was held with each participant. In the first meeting, the research process was explained, informed consent was requested, and a second session was arranged. The aim of the second meeting was to fill in demographic data, build a trusting relationship with the participant, and observe their activities during a shift at the NH. The third meeting entailed an in-depth interview, and the fourth involved the validation and clarification of findings.
Data collection took place during the COVID-19 pandemic (October – December 2021). While interviews and meetings were conducted face-to-face, standard health protocols were observed in visiting the NHs. Conversations were recorded in the audio format using a mobile recording device. Interviews were conducted in the Indonesian language. Field notes were used to facilitate recall and for further exploration of non-verbal language. The interviewers involved in this study had for more than five years of experience in qualitative research. Care and sensitivity were maintained throughout the interview process.
The semi-structured questions were developed based on previous research and discussions with nurses, managers, and supporting staff at NHs.5,14–16 The questions were developed from pilot interviews with three participants, but the results were not included in the data analysis. The list of questions that were used in the interview process is presented in Table 1.
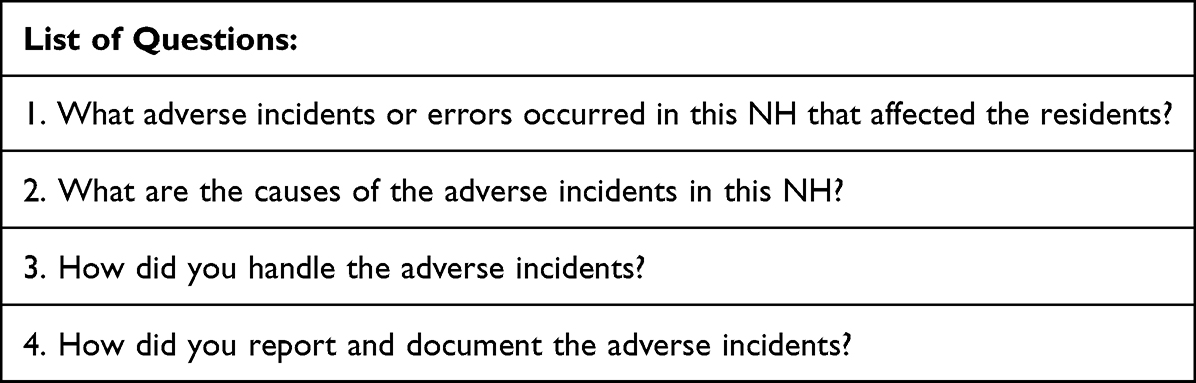 |
Table 1 List of Questions for in-Depth Interview |
Analysis
Data analysis was conducted with the assistance of the Excel TM software (Microsoft Inc, USA). After each interview was completed, the researcher transcribed the conversations verbatim and stored them in a separate folder, along with audio recording files and field notes. After compiling the transcripts, the researcher read over them several times to develop a comprehensive picture of the staff’s experience of adverse incidents in NHs. The appropriate code and quotation were written alongside the respondent’s code. We made a table in Microsoft Excel to help with the analysis, as well as highlighting meaningful words. Deductive analysis was performed by compiling codes based on research objectives and previous theories regarding adverse incidents in NHs (ie types of adverse incidents, reporting, and documenting systems). New codes were added from the appropriate quotations through an inductive analysis.
Next, the themes and sub-themes of meaningful statements and codes were formulated. The relationship between each theme and sub-theme was compiled and discussed with the peer team. If there were any changes to the themes and sub-themes, these were discussed until a consensus was reached. The results were then presented and discussed with external examines in order to check the correctness and consistency of the process. The experts determined whether the themes and sub-themes extracted from the interviews reflected the experiences of the participants. In the final step, emails and hard copies of the findings and transcripts were sent to the participants for validation. A follow up telephone conversation was held after participants had their transcript. All participants expressed their satisfaction and agreement with the data and conclusions.
We performed data analysis without utilizing specialized analytical tools, opting for Microsoft Excel to streamline the organization of pertinent themes and quotes. Data saturation was attained with the 21st participant, revealing a significant redundancy and absence of new information. To ensure the completeness of data saturation, the researcher interviewed the subsequent two participants, bringing the total number of participants to 23. The characteristics of participants, including age, gender, education, type of work, and work experience, are detailed in Table 2.
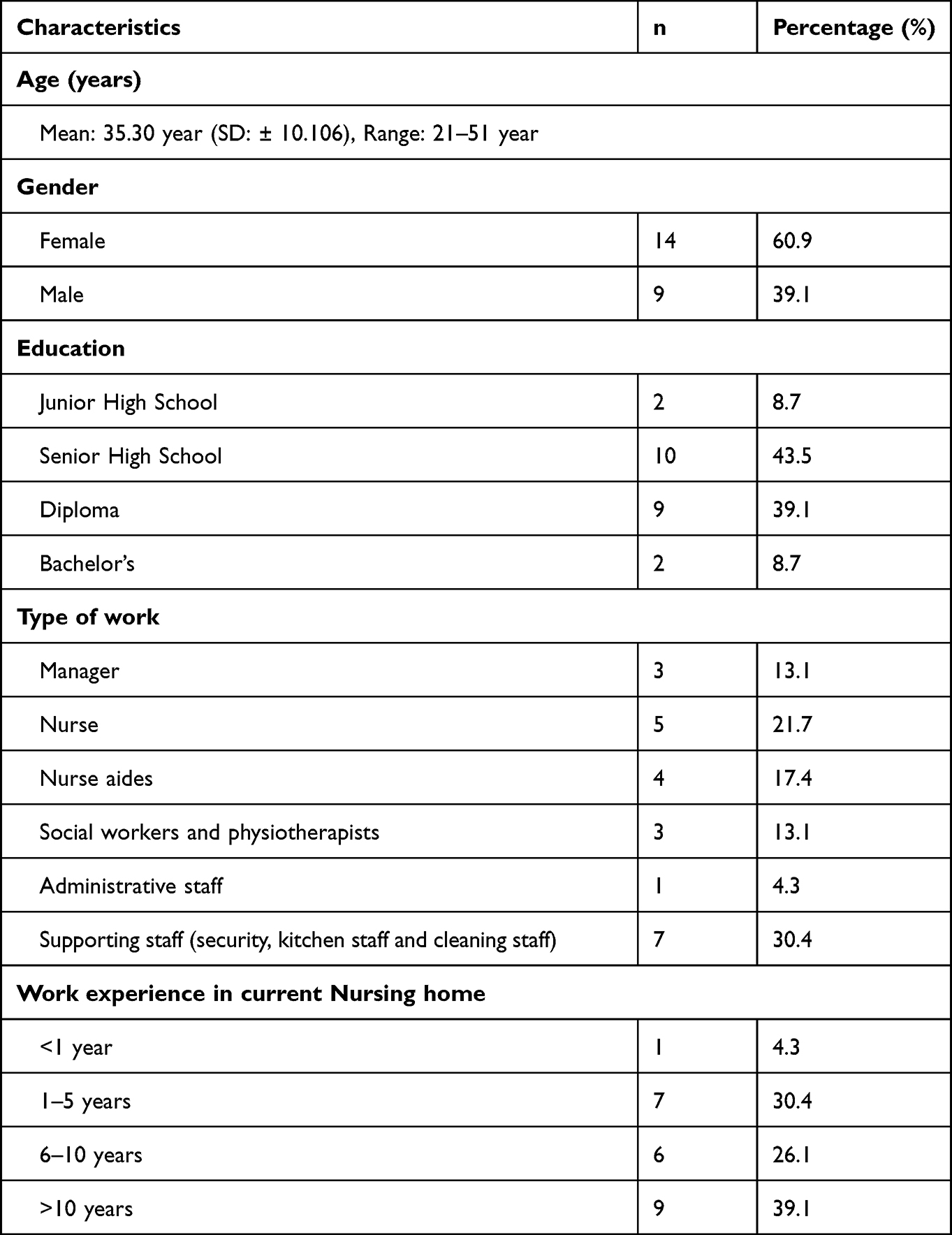 |
Table 2 Characteristics of Participants (N=23) |
Trustworthiness
Study trustworthiness was ensured through member checking and prolonged engagement.17,18 Participants met the interviewer four times to enhance involvement. Interview transcripts were shared with participants to confirm alignment with their experiences. Their feedback was incorporated, affirming accuracy. Researchers, supervisors, and peer experts discussed and validated themes and sub-themes from transcripts.
Translation
The translation process is essential to analyzing qualitative research data.19 As interviews were conducted in Indonesian, themes, sub-themes, quotations, and field notes were translated into English. A reverse translation was made back into Indonesian (Bahasa), and the differences between the two versions were examined and discussed. The researchers collaborated with two bilingual translators to conduct the translation process. The first translated everything word for word, including the field notes, and the second translated these documents back into Indonesian.20 If any discrepancies arose, these were discussed until a consensus was reached.
Ethics Approval and Consent to Participate
The researchers ensured that this study complied with the Declaration of Helsinki. The Universiti Malaya Research Ethics Committee (UMREC) approved this research protocol with reference number UM.TNC2/UMREC_1218. Written informed consent was obtained from all participants before starting the interviews, and participants were informed of the voluntary nature of their participation and their rights to withdraw consent and any time during and after the study. The publication of anonymous responses was also explicitly mentioned during the informed consent process. The researchers provided appropriate compensation for participants during this study. Interviews were discontinued if any participant showed signs of fatigue, physical discomfort, or psychological distress, and appropriate management provided if required.
Results
Themes are arranged based on answers from participants, including types of adverse incidents, potential cause of adverse incidents, handling, reporting, and documenting the adverse incidents. Quotations from NH staff supporting the emergent themes are presented in Table 3.
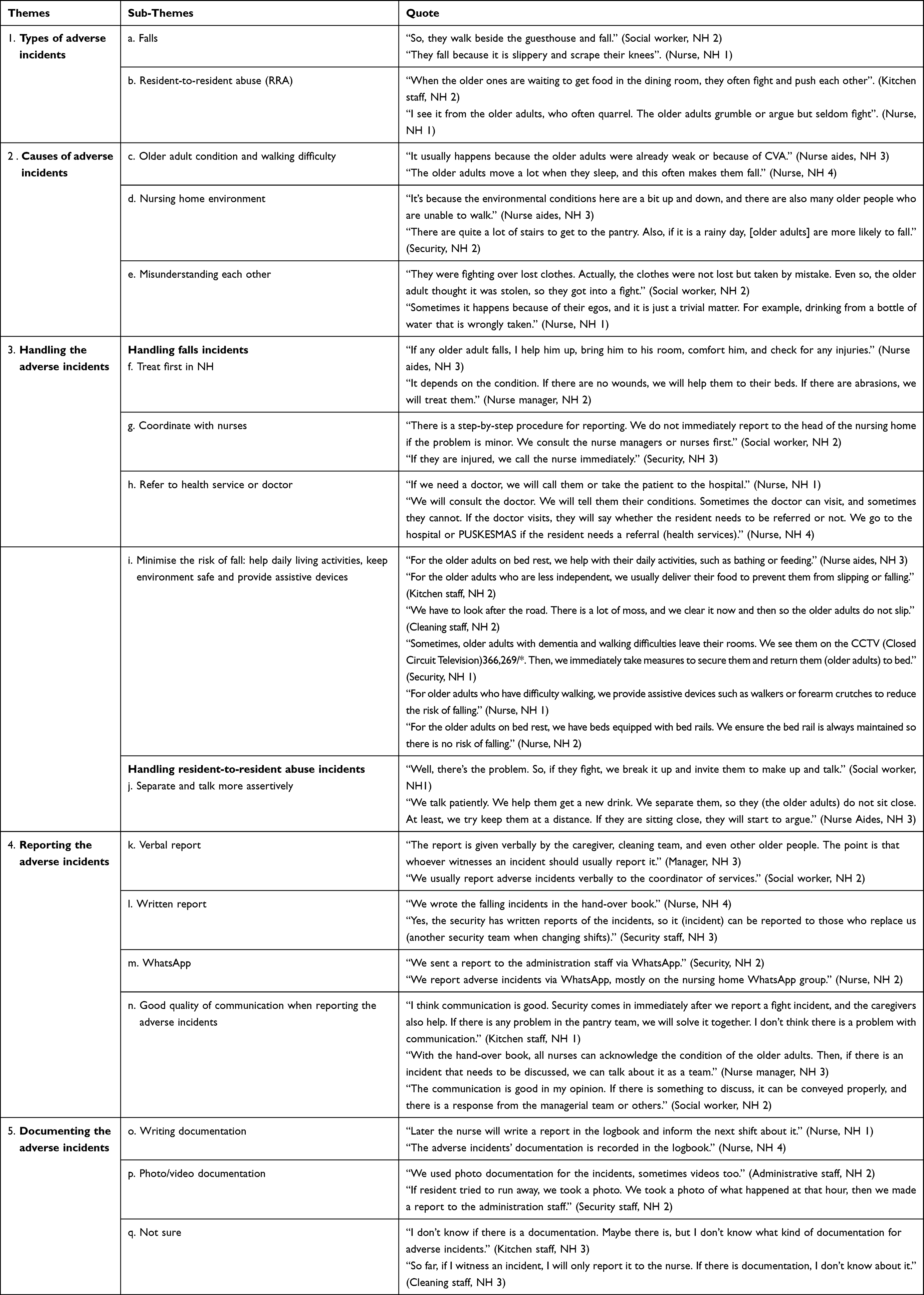 |
Table 3 Quotations of Nursing Home Staff Illustrating the Emerging Themes |
Types of Adverse Incidents That Occur in Nursing Homes
During the interviews conducted with the participants, a total of 23 participants shared their experiences regarding the adverse incidents they commonly encountered in their respective work units within the NHs. Among the various adverse incidents discussed, five adverse incidents emerged as the most frequently encountered: falls, resident-to-resident abuse (RRA), choking, residents running away from the NH, and pressure ulcers. It is important to note that falls and RRA were the two adverse incidents that NH staff members reported encountering most frequently.
Nine participants specifically mentioned the occurrence of falls as a common incident. Falls typically manifest as slips or accidents while walking, contributing to their prevalence within the NH setting.
The second most frequently reported incident, according to the participants, was resident-to-resident abuse. Arguments among older adults often take the form of bickering, resulting in disturbances or commotion without escalating into physical aggression. Seven participants shared their experiences regarding RRA incidents.
Cause of Adverse Incidents
Participants in the study identified various causes for adverse incidents occurring in NHs, with each incident having its unique underlying cause. For example, two participants highlighted that pressure ulcers were primarily caused by immobilization. Incidents involving residents absconding from the NH were commonly attributed to wandering behaviors exhibited by residents with dementia. Difficulty swallowing was cited as a cause of choking incidents, as expressed by the participants.
Regarding falls among residents, five participants elaborated on the causes. Two main causes were identified: the older adult’s physical condition, often associated with walking difficulties, and the NH environment. Participants observed that NHs with inclines and uneven paths were frequently identified as the contributing factors in fall incidents.
Furthermore, five participants revealed that RRA incidents were often triggered by misunderstandings, particularly related to daily activities such as changing clothes or accidental food basket exchanges. These incidents were found to be primarily rooted in misunderstandings and conflicts arising from routine activities.
Handling Adverse Incidents
Various strategies to deal with adverse incidents that occurred in NHs, especially fall management and RRA, were explained by staff.
Handling Falls Incidents
The participants in the study outlined four strategies for addressing falls in NHs: 1) providing initial treatment within the NH, 2) coordinating with the nurse, 3) referring residents to health services or doctors, and 4) implementing various strategies to minimize the risk of falls.
Immediate action is triggered following a fall incident regardless of the presence of injury. This involves assessing the condition of the older adults, providing appropriate treatment based on specific needs, and assistance them to return to bed. Staff members would then report the incident to the nurse or the manager on duty for that day. If there are minor injuries, the staff will call for a nurse to provide necessary treatment. In cases where the initial examination and first aid indicate a more severe condition, the staff will refer the resident to other healthcare services, such as independent practicing doctors, local health service centres (PUSKESMAS), or referral hospitals with which the NH collaborates. Two participants’ responses exemplify this approach.
The staff also shared their implementation of various strategies to prevent falls. One strategy involves assisting residents who face mobility challenges with their daily living activities. Quotations from the participants provide examples of this approach. Furthermore, the staff emphasized their efforts to maintain a safe environment for older adults to engage in their activities. They also ensure that appropriate assistive devices are provided to residents as a preventive measure against falls.
Handling Resident-to-Resident Abuse Incidents
Staff members employed a specific strategy to manage RRA incidents, which involved separating residents engaged in conflicts and adopting a more assertive communication approach. This strategy was mentioned by seven participants, highlighting its significance in addressing RRA situations.
Reporting the Adverse Incidents
Participants in the study identified three primary methods for reporting adverse incidents that occur in NHs: verbal reporting, written reporting, and utilizing a WhatsApp group. In the event of an incident, participants reported it to the personnel-in-charge for that day, including both the nurse and the social worker. Subsequently, the incident would be reported to the service coordinator and then referred to the head of the NH. Nine participants expressed their support for verbal reporting, while six participants favored reporting adverse incidents in writing. Three participants acknowledged the use of the WhatsApp group for incident reporting.
More than half of the participants (14 out of the total) acknowledged that the incident reporting process fostered effective communication. They also mentioned that superiors provided feedback once an incident was reported.
Documenting the Adverse Incidents
The interviews revealed that incident documentation in NHs varied among the staff members. Seven participants mentioned that adverse incidents were documented through written records, photos, or videos. However, one staff member stated that no specific documentation process was in place, and more than ten participants expressed uncertainty regarding the documentation practices for adverse incidents in NHs. Two participants specifically mentioned the use of photos and videos for documentation purposes. Most staff members appeared uncertain with the incident documentation procedures within the NHs.
Discussion
This study highlighted the two adverse incidents most frequently encountered by staff: falls and RRA. Falling incidents are common in NHs, which aligns with previous research indicating that falls are a leading cause of both fatal and non-fatal injuries among older individuals. Notably, older adults who have experienced falls in the past are more prone to experiencing them again, and those residing in NHs face a higher risk of falling compared to their counterparts in the community. Statistics reveal that on an annual basis, falls are experienced by 50% to 75% of NH residents.21 Overall, 1.5 falls have been reported to occur per NH bed annually, with published figures ranging from 0.2 to 3.6 falls per bed per year. Primary contributing factors include gait and balance disorders, weakness, dizziness, environmental risks, confusion, visual impairment, and postural hypotension.22
The findings of this study unveiled that the primary factors contributing to falls in Indonesian NHs were the physical condition of the older adults and the uneven flooring within NH facilities. These results are consistent with prior research in the field.22 Previous literature categorizes the risk factors associated with falls into two main groups: intrinsic factors, encompassing mobility issues, cognitive impairment, and weakness, and extrinsic factors, including environmental aspects like inadequate lighting, slippery floors, and conditions that pose hazards to the mobility of older adults, as well as organizational factors such as insufficient staffing.23
The findings of this study shed light on the strategies employed by NHs staff when dealing with residents who have experienced falls. These strategies encompassed several key approaches: 1) providing initial treatment within the NH, 2) coordinating with nursing staff, 3) referring to health services or doctors, and 4) minimizing the risk of future falls. The staff members elaborated further on the three stages involved in the “first treat in the NH” approach, which includes assessing the condition of the older adults, providing appropriate treatment based on their condition, and assisting them in returning to bed.
The assessment of the older adults’ condition encompasses a thorough examination to gauge the extent of injuries, comprehend their specific needs, and evaluate the overall impact on their health. Subsequently, the provision of appropriate treatment based on their condition entails administering first aid for minor injuries or more extensive medical interventions in cases of severe falls. The primary objective is promptly addressing the immediate health concerns stemming from the fall. Following the administration of necessary treatment, the third stage entails safely assisting the older adult in returning to their bed. This assistance may involve physical support, guidance, or any necessary measures to prevent further injury or discomfort. The overarching aim is to facilitate a seamless and secure transition back to their living quarters within the NHs.
Notably, the three initial strategies described by the participants closely align with the guidelines known as the “eight-step fall responses” issued by The Agency for Healthcare Research and Quality (AHRQ). The AHRQ is an organization dedicated to generating evidence promoting safer, higher-quality, accessible, equitable, and affordable healthcare within the United States. The eight stages outlined in these guidelines are as follows: evaluating and monitoring the resident for 72 hours after the fall, investigating the circumstances surrounding the fall, recording the circumstances, resident outcome, and staff response, notifying the primary care provider, implementing immediate interventions within the first 24 hours, conducting a comprehensive fall assessment, developing a personalized plan of care, and monitoring staff compliance and resident response.24
However, a notable distinction is that these guidelines incorporate sustainable standard operating procedures (SOPs) for managing fall incidents, supported by robust documentation and reporting systems. Despite the absence of a formal standard operating procedure (SOP), the participants in this study demonstrated a commendable commitment to assisting residents and mitigating falling incidents within NHs.
While falls themselves are preventable, their successful prevention necessitates the implementation of multiple interventions. The staff members undertook various proactive measures to prevent falls, such as providing appropriate walking aids, implementing environmental modifications to enhance resident mobility safety, and offering assistance with Activities of Daily Living (ADLs) for dependent residents.
Additionally, the staff emphasized the importance of immediate management within the NH or through referrals to other healthcare facilities like hospitals and Community Health Centers to minimize potential disability and morbidity resulting from falls. These findings align with a previous study, which highlighted the multifaceted nature of fall prevention in older adults. Effective fall prevention strategies encompass environmental modifications, exercise regimens, gait and balance training, comprehensive medical assessments, medication reviews, and staff education regarding fall prevention.25
The second most frequent incident encountered by staff was RRA. This may also be due to NHs in Indonesia having residents with varying states of dependency, from older adults who are still independent to those who are totally dependent. Residents who are still independent usually interact and do many activities with other residents, which can often lead to misunderstandings. These results are similar to findings in previous studies, where RRA is an incident that often occurs in LTC.26,27 The frequency of RRA ranges from one to 122 incidents, with insufficient information across studies to calculate its prevalence. Trigger RRA involves general misunderstanding between residents and the invasion of space and can occur without reason.27
Specific techniques were employed to handle RRA incidents, such as separating quarrelling residents and adopting a more assertive communication approach. Previous studies have revealed that effective communication with residents alone was sufficient to resolve RRA incidents in 42 out of 210 cases (20%). These findings are consistent with a qualitative study that highlighted the preference of staff members to employ a compassionate approach, primarily through communication, when dealing with RRA incidents, rather than resorting to medication or physical restraint.27 The findings of this study align with these observations, further supporting the value of communication in managing RRA incidents.
During the interview process, participants related that incident reporting was carried out actively, either in the form of reports, verbal communication, writing, or through WhatsApp groups. The staff also recorded adverse incidents on paper or through photos or videos, but only a small number of participants practiced this. These results indicate that staff have made efforts to report and document adverse incidents, but the process still lacked structure. There was no SOP regarding incident reporting, documentation, and the types of adverse incidents staff must report.
Nurses, the frontline staff, require targeted training programs to address the unique challenges of diverse adverse incidents. Continuous improvement in handling practices, aligning with established guidelines like the eight-step fall responses, is essential. Proactive measures, such as providing walking aids and environmental modifications, can significantly contribute to fall prevention.
The introduction of staff orientation programs is considered essential to enhance preparedness and knowledge in incident reporting and handling within NHs. New staff members should undergo orientation sessions to familiarize themselves with the reporting and documentation systems, safety protocols, and specific incident-handling procedures.28 These orientation programs will contribute to a proactive approach in incident management, ensuring the safety and well-being of residents while fostering a culture of continuous improvement among the staff.
Implications of This Study
Our results suggest several directions for future research. First, the findings cover various adverse incidents that occurred in NHs in Indonesia, namely falls, RRA, pressure ulcers, choking, and absconsion. While each incident type may have unique causes and solutions, this article focused on the two most common adverse incidents, namely falls and RRA. Even though these two adverse incidents frequently occur in NHs, it appears that incident handling still has much room for improvement. The diversity of adverse incidents in NHs in Indonesia opens up opportunities to conduct more in-depth research into the causes, treatments, and intervention modifications of these incidents.
Second, the characteristics of the NH environment in Indonesia also tend to contribute to the adverse incidents encountered by staff. For example, in NHs in Indonesia, independent older adults tend to engage in RRA in ways that dependent residents do not. Independent residents interact a lot and perform activities with other residents. During the interaction process, misunderstandings may arise, which trigger RRA. In addition to the diversity of resident dependencies, comprehensive research is needed to understand the correlation between the environment and RRA, including variables like NH density, stress levels, and the social norms of individual residents.
Third, this article focuses on the forms of reporting and incident documentation in NHs in Indonesia. Based on the results of this research, it is an important task for researchers, practitioners, nurses, and social workers to make improve the reporting and documentation systems for adverse incidents in NHs in Indonesia. Thus far, reporting has not been integrated, and no classification system has been introduced for the types of adverse incidents that have occurred or how to report and document them. Safety protocols surrounding adverse incidents in NHs also need to be introduced as part of staff training to ensure the safety of residents.
These findings stress the necessity for comprehensive policies in Indonesian NHs addressing incident handling, reporting, and documentation. Policymakers should contemplate integrating safety protocols and introducing standardized classification systems to bolster resident safety. Nurses require targeted training programs to tackle the unique challenges posed by diverse adverse incidents, emphasizing continuous improvement in handling practices. The staff must tailor the intervention to address specific incidents prevalent in NHs, considering environmental factors. Moreover, educational programs for healthcare professionals need to incorporate these findings into their curricula, focusing on fostering proactive reporting cultures and implementing safety protocols.
Strengths and Limitation
This study has several advantages. The samples were taken from multiple centers from three municipalities in East Java province so that the results could be generalizable. This study is pioneering in its reporting on the handling of adverse incidents in NHs in Indonesia. There are several limitations, however, including its qualitative research design. As such, it does not draw causal conclusions.
Despite these limitations, we believe that the conceptual framework and data collection strategy yield valuable insights regarding adverse incidents in NHs in Indonesia. This information can be used as the basis for future program development and research on this topic. Practitioners, nurses, governments, and social workers can develop strategies for handling and preventing safety of adverse incidents in NHs to improve the quality of service for older adults, especially in LTC facilities.
Conclusion
This study provides valuable insights into adverse incidents and adverse events in NHs. Falls and RRA were the most frequently encountered incidents, emphasizing the importance of effective prevention and management strategies. Falls were often caused by a combination of older adults’ physical conditions and environmental factors within NHs. The strategies employed by staff to address falls included initial management within the NH, coordination with nursing staff, referrals to health services, and measures to minimize the risk of falls. RRA incidents were typically triggered by misunderstandings related to daily activities. Reporting adverse incidents relied on verbal and written methods, while documentation practices varied among staff. There is a need for standardized protocols and comprehensive reporting and documentation systems in NHs. The findings of this study will contribute to the improvement of incident management and development of prevention strategies, ensuring the safety and well-being of older adults in NHs.
Data Sharing Statement
All data is included in this article and no further data will be available.
Acknowledgments
The authors express gratitude to Universiti Malaya, Universitas Airlangga, and all contributors to this research for the facilities and assistance provided. Many thanks to the respondents and nursing homes involved in this research. Finally, thanks to Proofed for their help in checking for corrections.
Author Contributions
Each author played a substantial role in the research presented, encompassing aspects such as conception, study design, data collection, analysis, and interpretation. They collectively engaged in drafting, revising, and critically evaluating the manuscript, ultimately granting their endorsement for publication. Consensus was reached on the choice of journal for submission, and the authors acknowledge their responsibility for the entire spectrum of the study’s execution.
Funding
This study was funded by Rector Scholarship of Universitas Airlangga.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pazokian M, Zagheri Tafreshi M, Rassouli M. Iranian nurses’ perspectives on factors influencing medication errors. Inter Nurs Rev. 2014;61(2):246–254. doi:10.1111/inr.12086
2. Ammouri AA, Tailakh AK, Muliira JK, Geethakrishnan R, Al Kindi SN. Patient safety culture among nurses. Int Nurs Rev. 2015;62(1):102–110. doi:10.1111/inr.12159
3. Hěib Z, Vychytil P, Marx D. Adverse event reporting in Czech long-term care facilities. Int J Qual Heal Care. 2013;25(2):151–156. doi:10.1093/intqhc/mzt014
4. Anderson JE, Kodate N, Walters R, Dodds A. Can incident reporting improve safety? Healthcare practitioners’ views of the effectiveness of incident reporting. Int J Qual Heal Care. 2013;25(2):141–150. doi:10.1093/intqhc/mzs081
5. Carlfjord S, Öhrn A, Gunnarsson A. Experiences from ten years of incident reporting in health care: a qualitative study among department managers and coordinators. BMC Health Serv Res. 2018;18(1):1–9. doi:10.1186/s12913-018-2876-5
6. Horstman C, Gumas ED, Jacobson G. U.S. and Global approaches to financing long-term care: understanding the patchwork (Commonwealth Fund, Feb. 2023); 2023.
7. Simmons SF, Schnelle JF, Sathe NA, et al. Defining safety in the nursing home setting: implications for future research. J Am Med Dir Assoc. 2016;17(6):473–481. doi:10.1016/j.jamda.2016.03.005
8. Agency for Healthcare Research and Quality. Chapter 1. Introduction and Program Overview; 2017. https://www.ahrq.gov/patient-safety/settings/long-term-care/resource/injuries/fallspx/man1.html.
9. World Health Organization. Integrated continuum of long-term care; 2021. https://www.who.int/publications/i/item/9789240038844.
10. Susilowati IH, Nugraha S, Sabarinah S, Peltzer K, Pengpid S, Hasiholan BP. Prevalence and risk factors associated with falls among community-dwelling and institutionalized older adults in Indonesia. Malaysian Fam Physician. 2020;15(1):30–38.
11. Dinas Sosial Provinsi Kalimantan Selatan. Panti Sosial Tresna Wirdha “Budi Sejahtera; 2013. http://dinsos.kalselprov.go.id/pantisosial/pstw-budisejahtera.
12. Badan Pusat Statistik Indonesia. Statistik Penduduk Lanjut Usia; 2021. Availble from: https://www.bps.go.id/publication/2021/12/21/c3fd9f27372f6ddcf7462006/statistik-penduduk-lanjut-usia-2021.html.
13. Colorafi KJ, Evans B. Qualitative descriptive methods in health science research. Heal Environ Res Des. 2016;9(4):16–25. doi:10.1177/1937586715614171
14. Berland A, Holm AL, Gundersen D, Bentsen SB. Patient safety culture in home care: experiences of home-care nurses. J Nurs Manag. 2012;20(6):794–801. doi:10.1111/j.1365-2834.2012.01461.x
15. Prang IW, Jelsness-Jørgensen LP. Should I report? A qualitative study of barriers to incident reporting among nurses working in nursing homes. Geriatr Nurs. 2014;35(6):441–447. doi:10.1016/j.gerinurse.2014.07.003
16. Travers J, Herzig CTA, Pogorzelska-Maziarz M, et al. Perceived barriers to infection prevention and control for nursing home certified nursing assistants: a qualitative study. Geriatr Nurs. 2015;36(5):355–360. doi:10.1016/j.gerinurse.2015.05.001
17. Korstjens I, Moser A. Series: practical guidance to qualitative research. Part 4: trustworthiness and publishing. Eur J Gen Pract. 2018;24(1):120–124. doi:10.1080/13814788.2017.1375092
18. Forero R, Nahidi S, De Costa J, et al. Application of four-dimension criteria to assess rigour of qualitative research in emergency medicine. BMC Health Serv Res. 2018;18(1):1–11. doi:10.1186/s12913-018-2915-2
19. Temple B, Young A. Qualitative research and translation dilemmas. Qual Res. 2004;4(2):161–178. doi:10.1177/1468794104044430
20. World Health Organization. WHO guidelines on translation; 2013. Available from: http://www.who.int/substance_abuse/research_tools/translation/en/.
21. Aguwa H. Nursing Education to Prevent Resident Falls in Long-Term Care. Walden University; 2019.
22. Rubenstein LZ, Josephson KR, Osterweil D. Falls and fall prevention in the nursing home. Clin Geriatr Med. 1996;12(4):881–902. doi:10.1016/S0749-0690(18)30206-4
23. Deandrea S, Bravi F, Turati F, Lucenteforte E, La Vecchia C, Negri E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch Gerontol Geriatr. 2013;56(3):407–415. doi:10.1016/j.archger.2012.12.006
24. Agency for Healthcare Research and Quality. The Falls management program: a quality improvement initiative for nursing facilities chapter 2. Fall Response; 2017. https://www.ahrq.gov/patient-safety/settings/long-term-care/resource/injuries/fallspx/man2.html.
25. Gulka HJ, Patel V, Arora T, McArthur C, Iaboni A. Efficacy and Generalizability of falls prevention interventions in nursing homes: a systematic review and meta-analysis. J Am Med Dir Assoc. 2019;2019:xxx:1–12. doi:10.1016/j.jamda.2019.11.012
26. McDonald L, Sheppard C, Hitzig SL, Spalter T, Mathur A, Mukhi JS. Resident-to-resident abuse: a scoping review. Can J Aging. 2015;34(2):215–236. doi:10.1017/S0714980815000094
27. Ferrah N, Murphy BJ, Ibrahim JE, et al. Resident-to-resident physical aggression leading to injury in nursing homes: a systematic review. Age Ageing. 2015;44(3):356–364. doi:10.1093/ageing/afv004
28. Menteri Kesehatan Republik Indonesia. Peraturan menteri kesehatan republik Indonesia nomor 11 tahun 2017 tentang keselamatan pasien. 2017:1–7.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Retrospective Analysis of the Clinical Characteristics of Patients with Breast Cancer Treated with Telomerase Peptide Immunotherapy Combined with Cytotoxic Chemotherapy
Kim JY, Yang DW, Kim S, Choi JG
Breast Cancer: Targets and Therapy 2023, 15:955-966
Published Date: 21 December 2023