Back to Journals » Drug Design, Development and Therapy » Volume 15
Stability of Aprepitant Injectable Emulsion in Alternate Infusion Bags, in Refrigerated Storage, and Admixed with Dexamethasone and Palonosetron
Authors Ottoboni T, Lerner L, Santhouse A
Received 19 September 2020
Accepted for publication 31 May 2021
Published 15 June 2021 Volume 2021:15 Pages 2519—2527
DOI https://doi.org/10.2147/DDDT.S282058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Thomas Ottoboni, 1 Laura Lerner, 1 Arlene Santhouse 2
1Pharmaceutical and Translational Science, Heron Therapeutics, Inc, San Diego, CA, USA; 2Medical Affairs, Heron Therapeutics, Inc, San Diego, CA, USA
Correspondence: Thomas Ottoboni
Pharmaceutical and Translational Science, Heron Therapeutics, Inc, 4242 Campus Point Court, Suite 200, San Diego, CA, 92121, USA
Tel +1 650-261-3003
Fax +1 650-365-6490
Email [email protected]
Purpose: The stability of aprepitant injectable emulsion is evaluated in various admixture bags and solutions, under different storage conditions, and when combined with other antiemetics.
Methods: A volume of 18 mL aprepitant injectable emulsion was added to infusion bags (either non-di-(2-ethylhexyl) phthalate [DEHP], polyvinyl chloride [PVC]-containing bags or non-DEHP, non-PVC bags) containing 100, 130, or 250 mL of 0.9% normal saline solution (NSS) or 5% dextrose in water (D5W). Bags were stored at controlled room temperature (20– 25°C) for up to 12 hours or refrigerated (2– 8°C) for up to 72 hours. Compatibility/stability was also assessed in admixtures combined with either dexamethasone or palonosetron. At specified time points, bags were tested for appearance, pH, assay for aprepitant (ie, percent label claim of aprepitant) and aprepitant-related substances, Z-average particle size, globule size distribution, particulate matter, and DEHP content (PVC bags). In separate analyses to assess microbial burden, bags containing aprepitant were inoculated with seven different organisms and assessed for microbial growth.
Results: There was no detectable impact on the physicochemical properties or potential to promote microbial growth of aprepitant when diluted with various amounts of either NSS or D5W and when admixed with either dexamethasone or palonosetron at room temperature for at least 6 hours or during refrigeration for up to 72 hours in either PVC- or non-PVC-containing bags.
Conclusion: Aprepitant-containing admixtures are stable under these conditions, a finding that may improve patient and provider convenience and reduce medication wastage.
Keywords: chemotherapy-induced nausea and vomiting, di-(2-ethylhexyl) phthalate, DEHP, microbial growth, physicochemical, polyvinyl chloride, PVC
Introduction
Aprepitant is a substance P/neurokinin-1 (NK-1) receptor antagonist approved by the US Food and Drug Administration (FDA) for use in combination with other antiemetic agents for the prevention of acute and delayed nausea and vomiting associated with initial and repeat courses of highly emetogenic chemotherapy (HEC), including high-dose cisplatin, and of nausea and vomiting associated with initial and repeat courses of moderately emetogenic chemotherapy (MEC).1–3 Aprepitant injectable emulsion (CINVANTI®, Heron Therapeutics, Inc., San Diego, CA, USA) is a novel formulation that contains 130 mg of aprepitant in an 18 mL emulsion, which contains egg lecithin, ethanol, sodium oleate, soybean oil, sucrose, and water for injection.2 It is free of polysorbate 80 and other synthetic surfactants. Prescribing guidelines recommend that aprepitant be admixed in 0.9% saline (NSS) or 5% dextrose in water (D5W) at concentrations of 130 mg/100 mL (HEC regimen) or 100 mg/100 mL (MEC regimen) only in non−polyvinyl chloride (PVC) infusion bags and administered with non-di-(2-ethylhexyl) phthalate (DEHP) tubing or administered without further dilution via a 2-minute intravenous (IV) push injection.2 Aprepitant IV is now approved as a 130 mg single-dose regimen for HEC or MEC or as a 3-day MEC regimen of a 100 mg single dose followed by 2 days of oral aprepitant. Current package labeling states that dilutions are stable at ambient room temperature for 6 hours in NSS injection or 12 hours in D5W, or up to 72 hours if stored under refrigeration in NSS injection or D5W.2
Patients receiving chemotherapy are often receiving multiple medications, and they may have a limited number of IV lines for parenteral access. Aprepitant is recommended for use in combination with other antiemetics, including a 5-hydroxytryptamine type 3 (5-HT3) receptor antagonist and dexamethasone sodium phosphate (dexamethasone) for the prevention of HEC and MEC chemotherapy-induced nausea and vomiting (CINV).1–5 In many treatment settings, an injectable NK-1 receptor antagonist is preferred, providing the convenience of an IV formulation, along with better patient adherence. The ability to mix multiple agents in a single IV bag may reduce the time to deliver the treatment regimen and increase patient convenience. Several drug formulations require storage at specific temperatures, and it is imperative to understand the stability of formulations at typical storage temperatures to avoid product wastage. In addition, acute shortages of IV fluids and bags due to manufacturing delays have resulted in significant disruption to the medical products industry.6,7
The objective of this study was to evaluate the stability of the aprepitant injectable emulsion in different types of infusion bags and diluents, under refrigerated and room temperature storage, and when admixed with other antiemetics, such as dexamethasone and palonosetron.
Materials and Methods
Physicochemical Stability at Different Dilutions in Different Bags
The materials and chemicals used in these studies are listed in Supplemental Table 1 and Supplemental Table 2. Sample preparations were intended to simulate admixtures, diluents, concentrations, and bags or tubing that would be anticipated in the clinic setting. Details of sample preparation are summarized in Table 1, but briefly, 18 mL of aprepitant injectable emulsion (Lot number B150355) was added to infusion bags that contained either 100 mL, 130 mL, or 250 mL of NSS or D5W. The bag size was 150 mL for the lower volumes (100 mL or 130 mL) and 250 mL for the largest volume (250 mL). Bags were either latex-free, non-PVC and non-DEHP, or made of PVC. Infusion bags and sample collections were performed in laminar flow hoods, with the flow being vertical. Bags of each type and dilution were prepared in triplicate for the 100 mL and 130 mL dilutions, and in duplicate for the 250 mL dilutions, and were stored at controlled room temperature (20–25°C) or refrigerated at 2–8°C. Because of difficulty in obtaining a sufficient number of 250 mL non-PVC, non-DEHP infusion bags, only NSS was tested as the diluent for this bag type.
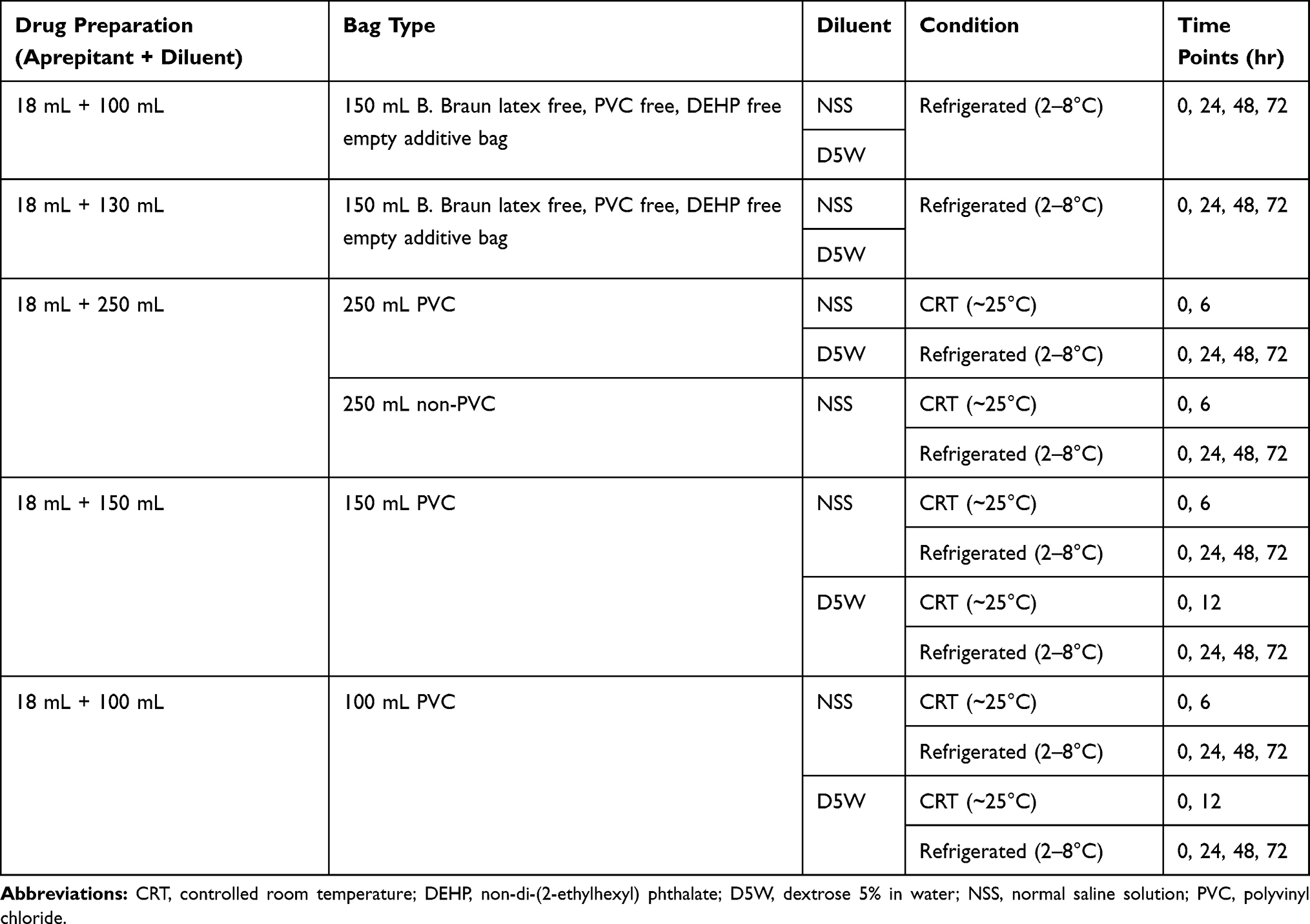 |
Table 1 Sample Preparation for Determining the Physicochemical Stability of Aprepitant Injectable Emulsion |
Compatibility with Other CINV Drugs
A volume of 18 mL of aprepitant injectable emulsion was added to 130 mL of either NSS or D5W, and then 5 mL of either dexamethasone (4 mg/mL) or palonosetron (Aloxi, 0.05 mg/mL; Helsinn Therapeutics, Inc., Iselin, NJ, USA) was added to 150 mL of B. Braun partial additive, non-PVC and non-DEHP bags (B. Braun Medical Inc., Bethlehem, PA, USA). The admixtures were gently mixed, and the bags were stored at ambient room temperature or refrigerated at 2–8°C. Their contents were tested for physicochemical properties after storage at room temperature for 6 or 12 hours for dilutions in NSS or D5W, respectively, or after storage for 24 hours under refrigeration. Physicochemical stability was also assessed after the solutions were pumped through infusion sets at ~2.5 mL/min.
Determination of Physicochemical Stability
At the specified time points, bags were removed from storage, equilibrated to room temperature if necessary, and tested for the following: appearance (visual appearance in ambient lighting [not placed in front of white or black background]), pH, assay for aprepitant (ie, percent of label claim of aprepitant) and aprepitant-related substances (ie, aprepitant-related compound A and desfluoro aprepitant), Z-average particle size as determined by dynamic light scattering (Malvern Zetasizer Nano S90), globule size distribution as assessed by the percent of fat globules larger than 5 µm (PFAT5), and particulate matter as determined by particle count utilizing microscopic examination. Measurements were compared to drug product that had not been diluted.
Aprepitant was analyzed by high-performance liquid chromatography (HPLC) using an Agilent Poroshell 120 Bonus-RP column (2.7 µm, 4.6×150 mm; Agilent Technologies, Wilmington, DE, USA) and the conditions outlined in Supplemental Table 3. The HPLC method was originally developed for the assay of aprepitant, and the determination of related substances. Due to the number of excipients in the formulation, a 50-minute gradient separation was used to ensure separation of aprepitant (approximate retention time 19 minutes), impurities and potential degradation products. The assay for determination of aprepitant identity and aprepitant-related substances by HPLC was validated for specificity and repeatability, per International Conference on Harmonisation (ICH) Q2(R1)8 and is summarized in Supplemental Table 4. With the extended gradient used for the HPLC analysis of Cinvanti (aprepitant approximate retention time 27 minutes), palonosetron (approximate retention time 7 minutes) and dexamethasone (approximate retention time 10 minutes) were resolved from components in Cinvanti. A representative chromatogram of the three species is shown in Figure 1A and B. The specificity of the research method was confirmed from the drug substance peaks being well resolved from each other and recoveries in Supplemental Table 4 acted as surrogate accuracy for the spiked samples. DEHP content in PVC bags was quantitated against a DEHP linearity standard curve over the range of 1–100 µg/mL. The results were expressed as a concentration (µg/mL). Detailed information about the methods used for determination of physicochemical stability is provided in Supplemental Table 5.
 |
Figure 1 Representative chromatogram of palonosetron, dexamethasone, and aprepitant. (A) Upper: full scale, (B) Lower: expanded view. |
Preparation and Sampling of Solutions for Microbial (Bioburden) Assays
Bags of diluted aprepitant injectable emulsion were prepared under aseptic conditions as described above, except that the intermediate dilution was 18 mL plus 132 mL. Suspensions of seven different organisms were prepared such that the inoculum concentration was 103–104 colony-forming unit (CFU)/mL. The organisms tested were Escherichia coli, Pseudomonas aeruginosa, Staphylococcus aureus, vancomycin-resistant Enterococcus faecalis (VREF), methicillin-resistant S. aureus (MRSA), Candida albicans, and Aspergillus brasiliensis. Bags containing diluted emulsion were inoculated with 1 mL of microbial suspension (one organism type per bag) to yield not more than 100 CFU/mL of diluted emulsion, then stored at room temperature or refrigerated at 2–8°C for 72 hours. At specified time points, 1 mL of the inoculated emulsion was removed from each bag, pipetted into a sterile petri plate, and diluted in phosphate buffer. Growth medium was added to the petri plate: Sabouraud dextrose agar for C. albicans and A. brasiliensis, and tryptic soy agar for the other organisms. The petri plates were incubated at the appropriate growth temperatures for 5–7 days and then counted to evaluate growth.
Results
Stability Across Admixtures, Bag Types, and Temperatures
For admixtures of aprepitant injectable emulsion in either NSS or D5W, there were no significant changes in appearance, pH, aprepitant assay, total percent-related substances, particulate matter, Z-average particle size, or particles larger than 5 μm (globule size distribution, PFAT5) at all dilutions in all bag types tested at all time points; the results conformed with the acceptance criteria for the drug product. Specific results for non-PVC, non-DEHP infusion bags that were stored under refrigeration are summarized in Table 2; dynamic light scattering particle size curve is illustrated in Supplemental Figure 1. For example, aprepitant concentrations were >94% of the label claim with both NSS and D5W in all dilutions for up to 72 hours. Z-average particle size values were slightly higher in D5W admixtures (range, 89.8–91.1 nm) than in NSS admixtures (range, 85.2–87.2 nm), although these values remained within the acceptance criterion. Similar results were observed for bags stored at room temperature for 6 hours (data not shown).
 |
Table 2 Physicochemical Stability Test Results for Aprepitant Injectable Emulsion (18 mL + 100 mL, 130 mL, or 250 mL) Diluted in NSS or D5W in Non-PVC, Non-DEHP Infusion Bags in Refrigerated Storage |
Physicochemical stability studies of aprepitant admixed in NSS or D5W in PVC-containing bags also showed no significant changes in appearance, pH, aprepitant assay or total percent-related substances (not including DEHP), particulate matter, Z-average particle size, or particles larger than 5 μm (globule size distribution, PFAT5) after refrigeration for up to 72 hours (Table 3) or at room temperature for 6–12 hours (data not shown). Aprepitant assay concentrations were within the acceptance criteria (ie, 90–110% of label claim) in all cases with the exception of the 24-hour measurement in 250 mL of D5W (88.5%). Other parameters were within the acceptance criteria in all cases. Concentrations of DEHP from PVC bags increased over time. The maximum amounts of DEHP were observed in 150 mL bags with 100 mL of diluent stored at 2–8°C for 72 hours with values of 84.9 µg/mL and 82.2 µg/mL, respectively, for NSS and D5W, which fall within acceptable limits (Table 3).
 |
Table 3 Physicochemical Stability Test Results for Aprepitant Injectable Emulsion (18 mL + 100 mL or 250 mL) Diluted in NSS or D5W in PVC Infusion Bags in Refrigerated Storage |
Stability in Admixtures with Dexamethasone or Palonosetron
For admixtures of aprepitant injectable emulsion with dexamethasone and palonosetron, no significant changes were observed in appearance, pH, Z-average particle size, or PFAT5, with no crystals or other changes in appearance observed in any samples when admixed in NSS or D5W. (Table 4). In addition, no new degradants were observed for aprepitant injectable emulsion, dexamethasone, or palonosetron. Although a decrease in pH was observed when palonosetron was added to aprepitant injectable emulsion, the final pH of the admixture was still within the acceptable range (≥7). The drop in pH could be ascribed to the low pH of palonosetron in solution (4.5–5.5).9
 |
Table 4 Percentage of Active Pharmaceutical Ingredient Relative to Time Zero Values for Aprepitant Emulsion for Injection Diluted in 150 mL Non-PVC, Non-DEHP Infusion Bags (18 mL + 130 mL NSS or D5W) ± Dexamethasone or Palonosetron |
Microbial Assays in Admixtures with D5W and NSS
In the microbial assays, microbiological media passed growth promotion testing, with the negative media control and the aprepitant injectable emulsion in diluent without inoculations showing no growth. Microbial test−positive inoculum controls showed visible growth and contained 10–100 CFUs, indicating that the correct inocula were prepared. Specifically, the aprepitant injectable emulsion admixtures with D5W and NSS when stored at 2–8°C did not promote proliferation of E. coli, S. aureus, MRSA, VREF, C. albicans, or A. brasiliensis over a 48-hour hold time, while the growth of P. aeruginosa was reduced (Table 5). In general, the aprepitant injectable emulsion admixtures with NSS and D5W showed significantly less than 0.5 log growth for the test organisms up to a 72-hour hold time under refrigeration.
 |
Table 5 Microbial Challenge Testing of Aprepitant Injectable Emulsion (18 mL + 100 mL; 18 mL + 132 mL) Diluted in NSS or D5W in Refrigerated Storage |
Discussion
Aprepitant injectable emulsion is a guideline-recommended antiemetic that is indicated, in combination with other antiemetics (ie, 5-HT3 antagonists, dexamethasone), for the prevention of CINV.1–5 The emulsion delivers 130 mg of aprepitant per 18 mL and is infused diluted over 30 minutes or injected undiluted via IV push over 2 minutes.2 There are limited data on the stability of aprepitant admixtures in various types of bags and storage conditions and in combination with other agents. The need for admixture stability information can be driven by a number of factors, including manufacturing shortages of IV bags, and situations in which patients are receiving multiple drug infusions and parenteral access is limited.6,10
The current study evaluated the physicochemical and microbial stability of aprepitant injectable emulsion when admixed with other antiemetics such as dexamethasone and palonosetron along with routine diluents such as NSS and D5W. There was no detectable impact on the physicochemical properties of aprepitant injectable emulsion diluted in 100 mL, 130 mL, or 250 mL of NSS or D5W in infusion bags, whether non-PVC or PVC, during refrigerated storage for up to 72 hours at 2–8°C. Likewise, all these dilutions are stable for at least 6 hours at room temperature. Z-average particle size values were slightly higher in D5W admixtures than in NSS admixtures (yet still within the acceptance criteria), but this finding is likely caused by electrostatic interactions of sodium ions with the positively charged particles of the emulsion.
In addition, the concentration of DEHP introduced into the infusion admixture is dependent on the time in storage and the size of the bag. The maximum amounts measured were for emulsion diluted in 250 mL bags stored at 2–8°C for 72 hours with values of approximately 25 µg/mL for NSS and approximately 24 µg/mL for D5W. This would correspond to a maximum of approximately 7.3 mg per dose, well below the tolerable intake limit of 0.6 mg/kg/day for DEHP administered parenterally.11
The results also indicate that aprepitant injectable emulsions are stable for at least 6 hours at room temperature or 24 hours refrigerated when mixed with either dexamethasone (95 mL at 4 mg/mL) or palonosetron (5 mL at 0.05 mg/mL) in NSS or D5W dilutions intended for push administration. The ability to admix other injectable agents in a single IV bag of aprepitant injectable emulsion may reduce the time required to deliver the antiemetic regimen and increase patient convenience, particularly for those who have limited parenteral access. These stability results also have the potential to reduce medication wastage by allowing storage of admixtures for future use. Further, microbial stability assays showed no microbial proliferation in aprepitant injectable emulsion diluted in NSS or D5W, at 2–8°C for hold times up to 72 hours.
While all assays were performed in a nonclinical setting, the conditions and procedures employed in the current study do not materially differ from those used in hospitals or clinics, and the results are thus likely transferable to a real-world patient setting. However, the safety of the admixed combinations in this study remains to be assessed.
Conclusion
In summary, there was no detectable impact on the physicochemical properties of aprepitant injectable emulsion diluted in various amounts of NSS or D5W in either non-PVC or PVC bags during refrigerated storage for up to 72 hours or at room temperature for 6 hours. Aprepitant injectable emulsion was also stable for 24 hours under refrigeration or up to 6 hours at room temperature when admixed with dexamethasone or palonosetron in either NSS or D5W.
Abbreviations
5-HT3, 5-hydroxytryptamine type 3; CFU, colony-forming unit; CINV, chemotherapy-induced nausea and vomiting; CRT, controlled room temperature; D5W, 5% dextrose in water; DEHP, di-2-ethylhexyl phthalate; DLS, dynamic light scattering; FDA, Food and Drug Administration; HEC, highly emetogenic chemotherapy; HPLC, high-performance liquid chromatography; IV, intravenous; LC, label claim; MEC, moderately emetogenic chemotherapy; MRSA, methicillin-resistant S. aureus; NDC, National Drug Code; NK-1, neurokinin-1; NSS, normal saline solution; PFAT5, percent of fat globules larger than 5 µm; PVC, polyvinyl chloride; RT, room temperature; SDA, Sabouraud dextrose sugar; VREF, vancomycin-resistant Enterococcus faecalis.
Acknowledgments
Medical writing support was provided by Phillip Giannopoulos, PhD, and Bret Fulton, RPh, of SciStrategy Communications, and funded by Heron Therapeutics, Inc. Experimental work was performed by Kimeka Douglas, Sarah Goodnight, and Kevin Jones of Alcami (Wilmington, NC) and Elaine Cung of Analytical Lab Group (Acton, MA). Data aggregation was provided by Will Everett of Heron Therapeutics, Inc.
Funding
This study was funded by Heron Therapeutics, Inc., San Diego, CA, USA.
Disclosure
Thomas Ottoboni and Arlene Santhouse report employment by Heron Therapeutics, Inc. Laura Lerner was an employee for Heron Therapeutics, Inc. at the time the study was conducted. The authors report no other conflicts of interest in this work.
References
1. NCCN clinical practice guidelines in oncology: antiemesis―version 2.2020. Available from: https://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf.
2. Heron Therapeutics. CinvantiTM (Aprepitant) Injectable Emulsion, for Intravenous Use [Prescribing Information]. San Diego, CA: Heron Therapeutics; 2019.
3. Herrstedt J, Roila F, Warr D, et al. 2016 Updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following high emetic risk chemotherapy. Supportive Care Cancer. 2017;25(1):277–288. doi:10.1007/s00520-016-3313-0
4. Hesketh PJ, Kris MG, Basch E, et al. Antiemetics: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2017;35(28):3240–3261. doi:10.1200/JCO.2017.74.4789
5. Roila F, Warr D, Hesketh PJ, et al. 2016 updated MASCC/ESMO consensus recommendations: prevention of nausea and vomiting following moderately emetogenic chemotherapy. Supportive Care Cancer. 2017;25(1):289–294. doi:10.1007/s00520-016-3365-1
6. ASHP and the University of Utah Drug Information Service. Small-volume parenteral solutions shortages suggestions for management and conservation. US Food and Drug Administration Web site: 2017. Available from: https://www.fda.gov/downloads/Drugs/DrugSafety/DrugShortages/UCM582461.pdf.
7. US Food and Drug Administration. FDA Commissioner Scott Gottlieb, M.D, updates on some ongoing shortages related to IV fluids (2018 Jan 16). Available from: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm592617.htm.
8. International conference on harmonisation of technical requirements for registration of pharmaceuticals for human use. ICH harmonised tripartite guideline. Validation of analytical procedures: text and methodology Q2(R1). Available from: http://academy.gmp-compliance.org/guidemgr/files/Q2(R1).PDF.
9. Eisai Inc. Aloxi (Palonosetron HCl) Injection for Intravenous Use [Prescribing Information]. Woodcliff Lake, NJ, USA: Eisai Inc; 2020.
10. Bentley J, Heard K, Collins GCC. Mixing medicines: how to ensure patient safety. Pharmaceut J. 2015;25(294). doi:10.1211/PJ.2015.20068289
11. US Food and Drug Administration. FDA Safety Assessment of Di(2-ethylhexyl)phthalate (DEHP) Released from PVC Medical Devices. Available from: https://www.fda.gov/media/114001/download.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.