Back to Journals » Infection and Drug Resistance » Volume 19
Spontaneous Conception After Integrated Traditional Chinese and Western Medicine Treatment for Chronic Endometritis with Recurrent Implantation Failure: A Case Report and Literature Review
Authors Jin Y ![]() , Shen T, Hong R, Yu X, Liang Y
, Shen T, Hong R, Yu X, Liang Y ![]() , Jin B
, Jin B ![]()
Received 17 November 2025
Accepted for publication 26 January 2026
Published 4 February 2026 Volume 2026:19 579367
DOI https://doi.org/10.2147/IDR.S579367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hazrat Bilal
Yihan Jin,1,2 Tao Shen,1 Renyun Hong,1 Xiaoxiao Yu,1 Yuanjiao Liang,1 Baofang Jin3
1Reproductive Medicine Center, Zhongda Hospital Affiliated to Southeast University, Nanjing, Jiangsu, People’s Republic of China; 2Faculty of Chinese Medicine, Macau University of Science and Technology, Macau, People’s Republic of China; 3External Medicine in Chinese Medicine Department, The Chinese Medicine Hospital of Hong Kong, Hong Kong, People’s Republic of China
Correspondence: Baofang Jin, Email [email protected]
Abstract: Recurrent implantation failure (RIF) is a challenging issue in in vitro fertilization and embryo transfer (IVF-ET). Chronic endometritis (CE) is one of the causes of RIF. For patients with CE and RIF, antibiotic therapy is currently the first-line and most widely used treatment. Nevertheless, it often fails to achieve the desired therapeutic outcomes. This case report presents a woman diagnosed with CE and RIF, who did not achieve pregnancy after four embryo transfers involving a total of seven embryos during IVF-ET treatment. However, after receiving a integrated therapy of Traditional Chinese Medicine (TCM) and antibiotics for CE, the patient achieved a spontaneous conception and subsequently delivered a healthy baby. This case suggests that an integrated approach of TCM and antibiotics may represent a safe and effective therapeutic strategy for patients with CE and RIF, offering a potential alternative to overcome the limitations of conventional antibiotic therapy alone. This finding warrants further investigation.
Keywords: chronic endometritis, recurrent implantation failure, endometrial receptivity, integrative Chinese and Western medicine therapy
Introduction
Embryo implantation is a complex process that involves two critical factors: high-quality embryos and a receptive endometrium. Endometrial receptivity refers to the ability of the endometrium to allow embryo implantation.1 Recurrent implantation failure (RIF) is defined as the failure to achieve pregnancy despite multiple transfers of high-quality embryos in patients undergoing in vitro fertilization and embryo transfer (IVF-ET). The incidence of RIF among IVF-ET patients is approximately 10%,2 leading to significant psychological and financial burdens for infertile couples. The causes of RIF are multifactorial, including maternal, paternal, and embryonic factors. Nowadays, with the continuous improvement of embryo culture systems and the maturation of preimplantation genetic testing, embryonic factors account for only one-third of implantation failures, while endometrial factors contribute to the remaining two-thirds.3
CE is a chronic reproductive tract inflammation characterized by stromal plasma cell infiltration of the endometrium. It is recognized as a significant risk factor for RIF. One study reported the prevalence of CE in infertile women to be between 2.8% and 56.8%, with an incidence of 14% to 67.5% in RIF patients.4 In CE, dysbiosis of the endometrial microbiota disrupts the normal intrauterine microenvironment, leading to alterations in local endometrial immune status. This disturbance triggers abnormal immune responses and dysregulated expression of immune factors, ultimately contributing to embryo implantation failure.5 Additionally, aberrant angiogenesis represents another significant pathological alteration associated with CE. Endometrial nutrition and oxygen supply depend on adequate vascularization,6 and appropriate angiogenesis is considered a crucial marker of endometrial receptivity. Consequently, impaired angiogenesis is regarded as a key factor in the development of RIF.7 Antibiotic therapy is a commonly used treatment for CE. While it can partially eliminate local inflammation and improve the cure rate of CE, it may not significantly improve pregnancy outcomes in patients with CE and RIF.8 Further research is needed to identify safer and more effective pharmacological treatment options.
Here, we report a case of a patient with RIF due to CE, who successfully achieved a spontaneous conception and successfully delivered a healthy full-term male infant after treatment with oral Traditional Chinese Medicine (TCM) and antibiotics. The patient initially sought IVF-ET treatment for infertility, undergoing ovarian stimulation and oocyte retrieval twice, with 4 embryo transfers, totaling 7 embryos, none of which resulted in pregnancy. After being diagnosed with CE, she received a combined treatment with TCM and antibiotics, resulting in a subsequent spontaneous conception. To our knowledge, it is rare for patients with recurrent implantation failure in IVF-ET treatment to achieve spontaneous conception. The entire treatment process of the patient is illustrated in Figure 1.
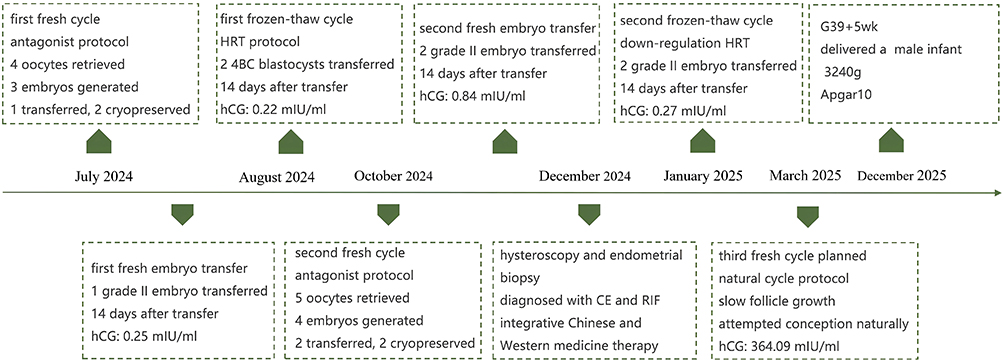 |
Figure 1 Timeline of the patient’s entire treatment process. The patient has undergone assisted reproductive technology treatment since July 2024. The treatment course included 2 ovarian stimulation cycles with oocyte retrieval, resulting in 4 embryo transfers of 7 embryos in total, none of which led to a successful pregnancy. In December 2024, she was diagnosed with CE and RIF. Following a combined treatment of TCM and antibiotics, she achieved a spontaneous conception and successfully delivered a full-term, healthy male infant. Both the mother and child are in good health. Abbreviations: hCG, human chorionic gonadotropin; HRT, hormone replacement therapy; CE, chronic endometritis; RIF, recurrent implantation failure; TCM, Traditional Chinese medicine. |
Case Presentation
The patient is a 34-year-old woman who married in 2019. She has regular menstrual cycles and normal sexual activity. In 2019, she underwent laparoscopic right salpingotomy with embryo removal for a right ectopic pregnancy. In 2020, a hysterosalpingogram indicated that both fallopian tubes were patent but with limited flow. Later that year, she underwent a combined hysteroscopic and laparoscopic pelvic adhesion removal and bilateral fallopian tube cannulation. During the surgery, the right fallopian tube was found to be twisted and adhered to the right ovary, while the left fallopian tube appeared normal. The tubal patency test showed that the left fallopian tube was patent, while the right fallopian tube was obstructed.
In April 2021, the patient’s anti-Müllerian hormone (AMH) level was measured at 2.55 ng/mL, and she began undergoing ovulation induction treatment. Four cycles of follicular monitoring were performed, with dominant follicle growth and ovulation observed in each cycle. Despite guidance for timed intercourse, pregnancy was not achieved. Subsequently, due to the impact of the COVID-19 pandemic, the patient attempted conception independently for two years without success. In July 2024, the patient’s AMH level was rechecked at 1.21 ng/mL. She sought consultation at the Reproductive Medicine Center of Zhongda Hospital, Southeast University, requesting IVF-ET treatment.
Before initiating controlled ovarian stimulation (COS), the patient and her partner underwent a series of evaluations to assess their overall health and fertility. No other systemic diseases were identified in either partner. The basic information of the couple, along with the fertility-related test results, are presented in Table 1.
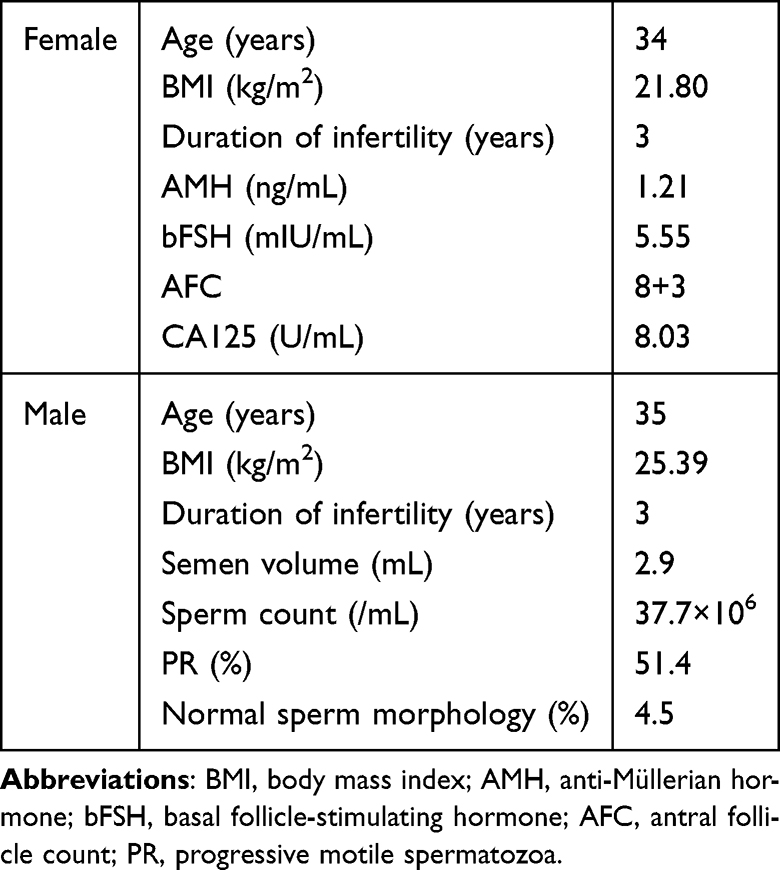 |
Table 1 Characteristics and the Fertility-Related Test Results of the Couple |
In July 2024, for the first fresh cycle, an antagonist protocol was selected for COS. On the third day of the patient’s menstrual cycle, gonadotropin (Gn) was used to initiate ovarian stimulation, with daily subcutaneous injections of recombinant human follicle-stimulating hormone 225IU (r-hFSH, Gonal-f, Merck Serono GmbH, Germany). Regular vaginal ultrasounds were conducted to assess follicular growth and adjust Gn dosage accordingly. On the 6th day of Gn administration, ganirelix 0.25mg (Orgalutran, Organon, Netherlands) was added. After 9 days of Gn treatment, human chorionic gonadotropin 10,000IU (hCG, Qingdao Guanlong Biopharmaceutical Co., Ltd., China) was injected as a trigger, and oocyte retrieval took place 36 hours later, yielding 4 oocytes. Three embryos were generated, with one grade II cleavage-stage embryo transferred on day 3 post-retrieval, and the remaining two blastocysts (4BC) were cryopreserved. The blood test conducted 14 days post-transfer indicated a negative pregnancy.
In August 2024, during the first frozen-thaw cycle, a hormone replacement therapy (HRT) protocol was used. Estradiol (Femoston red tablets, Abbott Biologicals B.V., USA) were taken starting on day 2 of the patient’s menstrual cycle to prepare the endometrium. When the endometrial thickness reached 8.2mm, a combination of vaginal progesterone gel 90mg (Crinone, Merck KGaA, Germany) and Femoston yellow tablets was administered for luteal phase support. After 6 days, the embryos were thawed and two 4BC blastocysts were transferred, but the pregnancy was not achieved.
In October 2024, for the second fresh cycle, an antagonist protocol was again chosen for COS. Ovarian stimulation started on day 2 of the patient’s menstrual cycle with daily subcutaneous injections of r-hFSH 225IU, recombinant human luteinizing hormone 75IU (r-hLH, Luveris, Merck Serono GmbH, Germany), and recombinant human growth hormone 4IU (rhGH, Jintropin, Changchun Jinsai Pharmaceutical Co., Ltd., China). On day 5 of Gn treatment, ganirelix 0.25mg was added. After 10 days of Gn therapy, hCG 10,000U and triptorelin 0.1mg (Decapeptyl, Ferring Pharmaceuticals Co., Ltd., Switzerland) were injected as trigger. Oocyte retrieval was performed 36 hours later, yielding 5 oocytes. A total of 4 cleavage-stage embryos were formed, and on day 3 post-retrieval, one grade I and one grade II cleavage-stage embryo were transferred, while the remaining two grade II cleavage-stage embryos were cryopreserved. The blood test result 14 days after the transfer still indicated no pregnancy.
In December 2024, following three failed embryo transfers, the patient underwent hysteroscopy and endometrial biopsy with pathological and immunohistochemical analysis, which revealed CE, with positive results for both CD38 and CD138. The patient typically presents with symptoms such as easy fatigue, generalized weakness, abdominal distension after meals or in the afternoon, and occasional loose stools. Physical examination reveals a pale tongue with a thin white coating and a fine, weak pulse. Based on TCM diagnostics, the condition was identified as spleen deficiency with dampness obstruction. The patient was prescribed oral TCM for strengthening the spleen and eliminating dampness, in combination with doxycycline hyclate 100mg (Jiangsu Lianhuan Pharmaceutical Co., Ltd., China), twice daily, for a duration of 2 weeks.
In January 2025, the second frozen-thaw cycle was conducted using a down-regulation HRT approach. On day 4 of the patient’s menstrual cycle, a subcutaneous injection of leuprorelin acetate 3.75mg (Boenleu, Beijing Bontac Pharmaceutical Co., Ltd., China) was administered. After 28 days, estradiol were taken to prepare the endometrium. When the endometrial thickness reached 8mm, vaginal progesterone gel, estradiol and dydrogesterone (Femoston yellow tablets, Abbott Biologicals B.V., USA) were given to support luteal phase. Four days later, two grade II cleavage-stage embryos were thawed and transferred, but the pregnancy was negative. The treatment details during the assisted reproductive technology cycles are presented in Table 2.
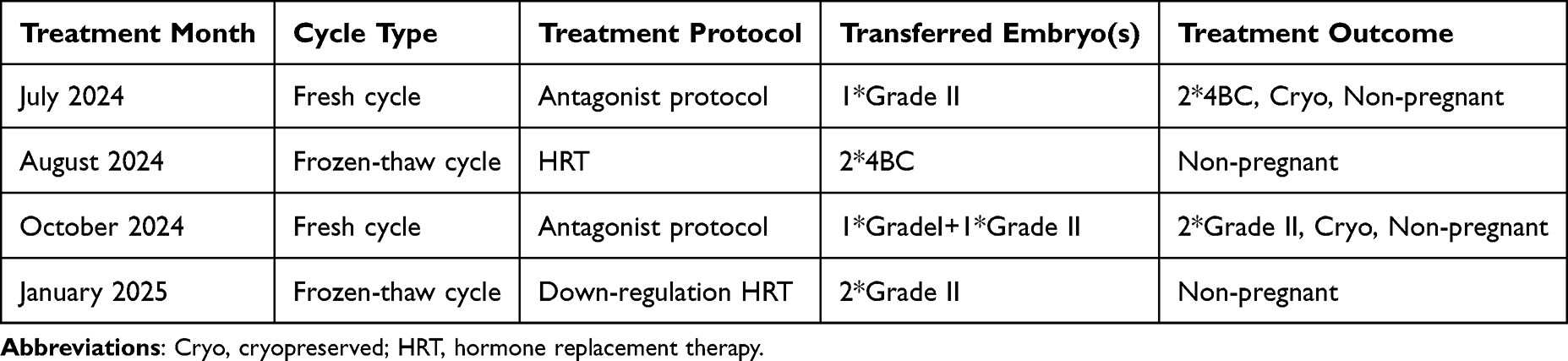 |
Table 2 Treatment Details During Assisted Reproductive Technology Cycles |
In March 2025, a natural cycle protocol was planned for another oocyte retrieval attempt. Ovulation monitoring began on day 3 of the menstrual cycle, but due to slow follicular growth and a decreasing trend in estrogen levels, the retrieval was canceled. An injection of hCG 10,000IU and triptorelin 0.1mg were administered to induce ovulation. The patient attempted conception naturally, and after ovulation, oral dydrogesterone 30mg/day (Duphaston, Abbott Biologicals B.V., the Netherlands) was prescribed for luteal phase support. Fourteen days later, the patient’s serum hCG level was 364.09 mIU/mL, which rose to 1162.22 mIU/mL upon re-examination two days later. Follow-up ultrasound examination confirmed a single intrauterine pregnancy. At 12 weeks of gestation, transvaginal ultrasound confirmed a continuing intrauterine pregnancy, after which luteal support medication was discontinued. The patient underwent regular prenatal check-ups in the obstetrics clinic. On December 21, 2025, at 39 weeks and 5 days of gestation, she successfully delivered a healthy male infant weighing 3240 g, with an Apgar score of 10.
Discussion
Although IVF-ET technology has advanced rapidly in recent years, bringing hope to numerous couples struggling with infertility, RIF continues to be a major challenge and pressing issue in the field of reproductive medicine. So far, a standardized definition of RIF has not been established; however, two diagnostic criteria are widely applied and acknowledged in clinical practice. The first defines RIF as failure to achieve pregnancy after two or more embryo transfer attempts, involving at least two high-grade blastocysts or four high-grade cleavage-stage embryos.9 The second criterion describes RIF as the inability to achieve a clinical pregnancy in women younger than 40 years after transferring at least three high-quality embryos across three fresh or frozen cycles.10 The etiology of RIF is complex, and any factor that affects embryo quality or endometrial receptivity may serve as a potential cause. As one of the conditions that disrupts the intrauterine environment, CE is a common and significant cause of RIF that should not be overlooked.
Contemporary understanding holds that the endometrium harbors hundreds of microbial communities that dynamically modulate its microecological balance, thereby maintaining the microenvironment essential for maternal–fetal interface formation. CE is a condition characterized by localized active infection of the endometrium, which disrupts the balance between the endometrial microbial environment and the immune system. Microbial infections are regarded as the main etiological factor of CE, and the commonly acknowledged pathogens include Streptococcus species, Escherichia coli, Staphylococcus, Enterococcus faecalis, and Mycoplasma. In recent years, CE has garnered increasing attention in the field of assisted reproduction due to its negative impact on embryo implantation. Numerous studies have demonstrated that CE adversely affects embryo implantation and is closely associated with adverse pregnancy outcomes.11,12
CE can reduce endometrial receptivity through multiple mechanisms, thereby impairing embryo implantation. Firstly, microbial infection in CE patients leads to dysbiosis of the endometrial microbiota, primarily characterized by altered abundance of Lactobacillus,13 which is the main factor affecting embryo implantation. Secondly, microbial infection within the uterine cavity of CE patients leads to immune microenvironmental alteration,14,15 where dysregulated expression of immune and inflammatory cytokines diminishes endometrial receptivity. In addition, CE interferes with endometrial decidualization by modulating the expression of estrogen and progesterone receptors, thus preventing successful embryo implantation.16
The majority of patients with CE present with no typical clinical symptoms or only mild, nonspecific manifestations such as increased vaginal discharge or pelvic discomfort. These subtle manifestations are frequently overlooked in clinical practice, constituting a major diagnostic challenge. The main pathological features of CE include endometrial mucosal edema, separation of epithelial cells and stroma, increased stromal cell density, and infiltration of plasma cells in the stroma,17 among which the presence of plasma cells in the stroma is the most specific and sensitive indicator. The diagnostic methods for CE include hysteroscopic examination, histopathological evaluation, pathogenic microbial culture, and next-generation sequencing (NGS) techniques. Although characteristic hysteroscopic findings of CE, such as punctate hemorrhage or the “strawberry sign” are relatively intuitive, a study by Song et al18 reported that the overall diagnostic accuracy of hysteroscopy for CE is only 67%. Therefore, hysteroscopy alone cannot be used as a definitive diagnostic method for CE. The current preferred diagnostic approach is a combination of hysteroscopic examination, endometrial histopathological assessment, and immunohistochemical staining for CD138.15 However, there is still no consensus regarding the required density of plasma cells in the endometrial stroma (ie, the number of plasma cells within a given area). In practice, the presence of more than five plasma cells per high-power field is generally used as the diagnostic criterion.
At present, oral antibiotics are the first-line and most widely used treatment option in clinical practice,10,19 which can improve endometrial receptivity and thereby increase the success rate of subsequent transfer cycles. In a 2017 prospective study, Kitaya et al20 evaluated pregnancy outcomes in 118 women with RIF and concomitant CE following antibiotic treatment. They found that the live birth rate in the first embryo transfer cycle (32.8%) and the cumulative live birth rate over three cycles (38.8%) in the CE-cured group were both higher than those in the non-CE group (22.1%, P = 0.031; 27.9%, P = 0.037). Management of CE has likewise been shown to enhance in vitro fertilization (IVF) outcomes among patients with RIF.21 However, due to the limitations of endometrial microbial pathogen culture, the treatment of CE remains largely empirical. There is still no standardized guideline regarding the selection, duration, dosage, or administration of antibiotics, and prolonged or high-dose regimens may lead to antibiotic resistance and compromise therapeutic efficacy. Evidence indicates that despite undergoing three courses of antibiotic therapy, 18.75% of patients continue to exhibit persistent CE.22 Additionally, a separate study demonstrated that even following antibiotic therapy, the embryo implantation rate in subsequent transfer cycles of RIF patients with CE (11.5%) was still markedly lower than that of RIF patients without CE (32.7%).23 Thus, in cases with widespread plasma cell infiltration or antibiotic resistance, antibiotic therapy alone may play a limited role in managing CE. In recent years, multiple strategies including combined antibiotic therapy, oral antibiotics with intrauterine infusion, and antibiotics combined with corticosteroids have been applied for the treatment of CE with concurrent RIF, yet their therapeutic effectiveness still requires further investigation. One study demonstrated that a new treatment strategy combining oral antibiotics (doxycycline and metronidazole) with intrauterine infusion (gentamicin and dexamethasone) could enhance pregnancy outcomes in CE patients with RIF, compared with oral antibiotic therapy alone.24 Nevertheless, the study by Zou et al25 revealed that oral co-administration of prednisone acetate and doxycycline might be an effective treatment option for patients with RIF accompanied by CE and could enhance reproductive outcomes, although it did not improve the CE cure rate compared with doxycycline monotherapy. Moreover, a subset of CE cases may be linked to non-infectious etiologies. In these patients, antibiotics show no therapeutic effect, and effective alternative treatment strategies are still unavailable.
In recent years, TCM has demonstrated considerable therapeutic value and remarkable clinical effectiveness in managing CE associated with RIF.26 In TCM, CE is classified as a type of “dai xia disorder” (abnormal vaginal discharge). It is believed that weakness of spleen qi results in impaired transformation and transportation of fluids, causing dampness to flow downward to the lower burner. As noted in Fu Qingzhu’s Gynecology: “All vaginal discharge syndromes originate from dampness”. Zhu Danxi remarked, “When damp-heat invades the blood, prolonged exposure leads to turbidity and stagnation”. The primary pathogenesis of CE involves spleen deficiency, qi stagnation, and damp-heat with blood stasis. Hence, therapeutic principles emphasize tonifying qi, strengthening the spleen, nourishing and invigorating the blood, and resolving dampness and swelling. A study reported that the treatment principle of invigorating qi, activating blood circulation, clearing heat, and resolving dampness was effective in managing female infertility induced by CE.27 Jing Wenjun et al28 demonstrated that the modified Danggui Shaoyao San could alleviate endometrial inflammation in CE patients with RIF by improving the development of endometrial pinopodes and downregulating the expression of inflammation-related factors, thereby enhancing endometrial receptivity.
This patient underwent four embryo transfer procedures, with a total of seven embryos transferred (including five high-quality embryos), yet none resulted in successful pregnancy. Throughout the entire IVF-ET treatment process, except for the diagnosis of CE confirmed by hysteroscopy combined with endometrial pathology and immunohistochemistry, no additional abnormalities were found that might have negatively influenced embryo implantation. Following treatment with a spleen-strengthening and dampness-resolving prescription in combination with doxycycline, the patient conceived naturally, which was an unanticipated yet encouraging result for individuals suffering from CE associated with RIF. The spleen-strengthening and dampness-resolving formula consists of 12 herbs, including raw Astragalus membranaceus (Huangqi), stir-fried Atractylodes macrocephala (Baizhu), Saposhnikovia divaricata (Fangfeng), Dioscorea opposita (Huai Shanyao), raw Coix lacryma-jobi (Yiyiren), Cinnamomum cassia twig (Guizhi), Pseudostellaria heterophylla (Taizishen), Poria cocos (Fuling), honey-fried Glycyrrhiza uralensis (Zhigancao), Angelica sinensis (Danggui), Spatholobus suberectus (Jixueteng), and processed Cyperus rotundus (Zhixiangfu). It is a prescription formulated by Professor Jin Baofang based on his clinical experience in treating chronic endometritis. Huangqi functions as the chief herb, invigorating qi, relieving stagnation, and promoting diuresis to alleviate edema. Baizhu fortifies the spleen and promotes fluid metabolism; Taizishen and Shanyao replenish qi and support spleen function; Fuling and Yiyiren reinforce the spleen, leach out dampness, induce urination, and expel pus. Acting synergistically, these herbs aid the principal herb in strengthening qi and spleen function, resolving dampness, and alleviating edema, thus serving as the minister herbs. Guizhi, Xiangfu, Danggui, and Jixueteng collectively warm yang, unblock the meridians, regulate qi, and invigorate blood. Fangfeng dispels wind and overcomes dampness, reinforcing the damp-resolving effects of the minister herbs; these ingredients together constitute the assistant herbs in the formula. Zhigancao coordinates and harmonizes the other components of the prescription, functioning as the messenger herb. The prescription as a whole functions to fortify the spleen, tonify qi, activate blood circulation, dredge meridians, resolve dampness, and relieve swelling. By employing the gentle “sweet and bland” method to remove dampness and emphasizing spleen-strengthening and qi-invigorating herbs, it achieves dampness elimination without injuring yin. In addition, the combined use of strategies that promote blood flow, regulate qi, and dispel wind enhances inflammation resolution through multiple mechanisms, fundamentally treating chronic endometritis. Despite the failure to achieve pregnancy in the first transfer cycle after combined Chinese and Western medical therapy, this outcome does not invalidate the effectiveness of the pharmacological treatment. In reality, no large-sample systematic studies have yet determined the ideal time after CE treatment for achieving the most receptive endometrial condition to maximize implantation success, and performing embryo transfer immediately after treatment does not guarantee satisfactory pregnancy results. According to the study by Xie et al29 antibiotic therapy in CE associated RIF patients led to a marked improvement in the one-year clinical pregnancy rate compared with untreated RIF patients without CE, with the most pronounced effect observed after the fourth month post-treatment. Thus, we are convinced that the combined application of traditional Chinese and Western medicine in treating CE enhanced the patient’s endometrial receptivity, which ultimately allowed for spontaneous conception.
Admittedly, this case report has certain limitations. In view of the potential adverse effects of repeated hysteroscopy and endometrial scraping on the endometrium, we did not re-examine the patient’s post-treatment endometrial pathology or immunohistochemical findings. This single case does not reflect the full spectrum of similar patients. More extensive clinical data are necessary to confirm the treatment’s effectiveness, and additional research is warranted to clarify the mechanisms responsible for its efficacy.
Conclusion
In conclusion, the combination of TCM with antibiotic therapy may be beneficial in the management of CE. For patients with CE accompanied by RIF, an integrative approach could represent a promising therapeutic strategy to support pregnancy achievement. Nevertheless, more research is required to clarify the impact of integrative therapy on CE and its potential benefits for CE associated RIF.
Abbreviations
AMH, anti-Müllerian hormone; CE, chronic endometritis; COS, controlled ovarian stimulation; Gn, gonadotropin; hCG, human chorionic gonadotropin; HRT, hormone replacement therapy; IVF-ET, in vitro fertilization and embryo transfer; NGS, next-generation sequencing; r-hFSH, recombinant human follicle-stimulating; rhGH, recombinant human growth hormone; r-hLH, recombinant human luteinizing hormone; RIF, recurrent implantation failure; TCM, traditional Chinese medicine.
Data Sharing Statement
Please contact the first author or corresponding author for data requests.
Ethics Approval and Consent to Participate
This case report was reviewed and approved by the Ethics Committee of Zhongda Hospital Affiliated to Southeast University, 2024ZDSYLL091-P01. Written informed consent was obtained from the participant.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from Integrated Traditional Chinese and Western Medicine Research of Zhongda Hospital Affiliated to Southeast University (Grant Number 2023zxyxt06) and National Natural Science Foundation of China (No. 82575070).
Disclosure
All authors declare no competing interests in this work.
References
1. Lessey BA, Young SL. What exactly is endometrial receptivity? Fertil Steril. 2019;111(4):611–8. doi:10.1016/j.fertnstert.2019.02.009
2. Busnelli A, Reschini M, Cardellicchio L, Vegetti W, Somigliana E, Vercellini P. How common is real repeated implantation failure? An indirect estimate of the prevalence. Reprod Biomed Online. 2020;40(1):91–97. doi:10.1016/j.rbmo.2019.10.014
3. Craciunas L, Gallos I, Chu J, et al. Conventional and modern markers of endometrial receptivity: a systematic review and meta-analysis. Hum Reprod Update. 2019;25(2):202–223. doi:10.1093/humupd/dmy044
4. Kimura F, Takebayashi A, Ishida M, et al. Review: chronic endometritis and its effect on reproduction. J Obstet Gynaecol Res. 2019;45(5):951–960. doi:10.1111/jog.13937
5. Kuroda K, Nakagawa K, Horikawa T, et al. Increasing number of implantation failures and pregnancy losses associated with elevated Th1/Th2 cell ratio. Am J Reprod Immunol. 2021;86(3):e13429. doi:10.1111/aji.13429
6. Ates C, Dilbaz B, Ergani SY, Atabay F. The effect of antiangiogenic agent aflibercept on surgically induced endometriosis in a rat model. Cir Cir. 2024;92(1):10–19. doi:10.24875/CIRU.23000072
7. Chen X, Man GCW, Liu Y, et al. Physiological and pathological angiogenesis in endometrium at the time of embryo implantation. Am J Reprod Immunol. 2017;78(2). doi:10.1111/aji.12693
8. Kato H, Yamagishi Y, Hagihara M, et al. Systematic review and meta-analysis for impacts of oral antibiotic treatment on pregnancy outcomes in chronic endometritis patients. J Infect Chemother. 2022;28(5):610–615. doi:10.1016/j.jiac.2022.01.001
9. Zhang Y, Jiang C, Jiang CY, et al. Effect of atosiban on the outcomes of frozen-thawed embryo transfer in patients with repeated implantation failure. J Int Reprod Health/Family Plan. 2023;42(2):95–101.
10. Chinese association of reproductive medicine, professional committee of reproductive medicine, China medical women′s association. Expert consensus on diagnosis and treatment of recurrent implantation failure. Natl Med J China. 2023;103(2):89–100. doi:10.3760/cma.j.cn112137-20221105-02317
11. Zargar M, Ghafourian M, Nikbakht R, Mir Hosseini V, Moradi Choghakabodi P. Evaluating chronic endometritis in women with recurrent implantation failure and recurrent pregnancy loss by hysteroscopy and immunohistochemistry. J Minim Invasive Gynecol. 2020;27(1):116–121. doi:10.1016/j.jmig.2019.02.016
12. Kuroda K, Takamizawa S, Motoyama H, et al. Analysis of the therapeutic effects of hysteroscopic polypectomy with and without doxycycline treatment on chronic endometritis with endometrial polyps. Am J Reprod Immunol. 2021;85(6):e13392. doi:10.1111/aji.13392
13. Liu Y, Ko EY, Wong KK, et al. Endometrial microbiota in infertile women with and without chronic endometritis as diagnosed using a quantitative and reference range-based method. Fertil Steril. 2019;112(4):707–717.e1. doi:10.1016/j.fertnstert.2019.05.015
14. Kitazawa J, Kimura F, Nakamura A, et al. Alteration in endometrial helper T-cell subgroups in chronic endometritis. Am J Reprod Immunol. 2021;85(3):e13372. doi:10.1111/aji.13372
15. Li Y, Yu S, Huang C, et al. Evaluation of peripheral and uterine immune status of chronic endometritis in patients with recurrent reproductive failure. Fertil Steril. 2020;113(1):187–196.e1. doi:10.1016/j.fertnstert.2019.09.001
16. Wu D, Kimura F, Zheng L, et al. Chronic endometritis modifies decidualization in human endometrial stromal cells. Reprod Biol Endocrinol. 2017;15(1):16. doi:10.1186/s12958-017-0233-x
17. Opuchlik K, Pankiewicz K, Pierzyński P, et al. Factors influencing endometrial receptivity in women with recurrent implantation failure. BMC Womens Health. 2025;25(1):15. doi:10.1186/s12905-024-03531-z
18. Song D, Li TC, Zhang Y, et al. Correlation between hysteroscopy findings and chronic endometritis. Fertil Steril. 2019;111(4):772–779. doi:10.1016/j.fertnstert.2018.12.007
19. Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1–187. doi:10.15585/mmwr.rr7004a1
20. Kitaya K, Matsubayashi H, Takaya Y, et al. Live birth rate following oral antibiotic treatment for chronic endometritis in infertile women with repeated implantation failure. Am J Reprod Immunol. 2017;78(5). doi:10.1111/aji.12719
21. Vitagliano A, Saccardi C, Noventa M, et al. Effects of chronic endometritis therapy on in vitro fertilization outcome in women with repeated implantation failure: a systematic review and meta-analysis. Fertil Steril. 2018;110(1):103–112.e1. doi:10.1016/j.fertnstert.2018.03.017
22. Cicinelli E, Resta L, Loizzi V, et al. Antibiotic therapy versus no treatment for chronic endometritis: a case-control study. Fertil Steril. 2021;115(6):1541–1548. doi:10.1016/j.fertnstert.2021.01.018
23. Johnston-MacAnanny EB, Hartnett J, Engmann LL, Nulsen JC, Sanders MM, Benadiva CA. Chronic endometritis is a frequent finding in women with recurrent implantation failure after in vitro fertilization. Fertil Steril. 2010;93(2):437–441. doi:10.1016/j.fertnstert.2008.12.131
24. Ma N, Li J, Zhang J, et al. Combined oral antibiotics and intrauterine perfusion can improve in vitro fertilization and embryo transfer pregnancy outcomes in patients with chronic endometritis and repeated embryo implantation failure. BMC Womens Health. 2023;23(1):344. doi:10.1186/s12905-023-02443-8
25. Zou Y, Ming L, Ding J, et al. Low dosage of prednisone acetate combined with doxycycline in the treatment of chronic endometritis in patients with repeated implantation failure. Am J Reprod Immunol. 2023;89(6):e13713. doi:10.1111/aji.13713
26. Hu YR, Cai PP. A meta-analysis of the efficacy of integrated traditional Chinese and western medicine in the treatment of chronic endometritis. Hunan J Trad Chin Med. 2021;37(9):145–151. doi:10.16808/j.cnki.issn1003-7705.2021.09.052
27. Ji XL. Clinical experience of professor Wei Shaobin on treating chronic endometrial inflammatory infertility by combination of both internal and external treatment. J Chengdu Univers Trad Chin Med. 2022;45(2):30–33. doi:10.13593/j.cnki.51-1501/r.2022.02.030
28. Jin WJ, Cai PP, Wang YQ, Li JY, Li KQ. Changes in endometrial pinopodes and NF-κb and TGF-β1 protein expression in rats with chronic endometritis after treatment of modified Danggui Shaoyao powder. Shandong Med J. 2022;62(8):38–41.
29. Xie Q, Zhao C, Jiang W, et al. Antibiotics improve reproductive outcomes after frozen-thaw embryo transfer for chronic endometritis treatment, especially in those with repeated implantation failure. BMC Womens Health. 2024;24(1):430. doi:10.1186/s12905-024-03274-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Uterine NK Cell Polarization Associates with Chronic Endometritis and Predisposition to Recurrent Implantation Failure
Xie Q, Zhang L, Yang J, Yang M, Li Q, Chen Q
International Journal of Women's Health 2025, 17:4255-4266
Published Date: 7 November 2025