Back to Journals » Vascular Health and Risk Management » Volume 22
Spatiotemporal Mortality Patterns and Temperature-Associated Risk of Aortic Dissection in the United States: A National CDC WONDER Database Analysis
Authors Wang H ![]() , Wang S
, Wang S ![]() , Fan K
, Fan K ![]() , Li Y, Wang Z, Mawas M
, Li Y, Wang Z, Mawas M ![]() , Chu W, Musleh G, Zheng G
, Chu W, Musleh G, Zheng G
Received 23 September 2025
Accepted for publication 12 February 2026
Published 17 February 2026 Volume 2026:22 569639
DOI https://doi.org/10.2147/VHRM.S569639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Heng Wang,1,2,* Shule Wang,3,* Keyi Fan,4,* Yaling Li,5 Ziyan Wang,6 Mohamed Mawas,1,2 Wenyi Chu,7 Gamal Musleh,8 Guoping Zheng1,2
1Centre for Transplant and Renal Research, Westmead Institute for Medical Research, The University of Sydney, Sydney, NSW, Australia; 2Faculty of Medicine and Health, The University of Sydney, Camperdown, NSW, Australia; 3Neuroscience Institute, JFK University Medical Center, Edison, NJ, USA; 4Department of Vascular Surgery, The Second Hospital of Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 5Department of Vascular Surgery, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China; 6Department of Endovascular Surgery, The First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 7Department of Anesthesiology, SUNY Downstate Health Sciences University, Brooklyn, NY, USA; 8Department of Internal Medicine, Trinitas Regional Medical Center, Elizabeth, NJ, USA
*These authors contributed equally to this work
Correspondence: Guoping Zheng, Centre for Transplant and Renal Research, Westmead Institute for Medical Research, The University of Sydney, Sydney, NSW, Australia, Email [email protected]
Purpose: Aortic dissection (AD) is a life-threatening aortic emergency that progresses rapidly and carries a high mortality rate. We characterised contemporary patterns and long-term trends in AD mortality in the United States and examined associations between ambient temperature and AD mortality.
Patients and Methods: We obtained mortality data for AD from United States CDC WONDER for 1999– 2023 and calculated age-adjusted mortality rates (AAMR). Temporal trends were assessed using Joinpoint regression to estimate annual percent change (APC) and average annual percent change (AAPC). Monthly air temperature data for the period 1999– 2023 were obtained from the North America Land Data Assimilation System (NLDAS). Associations between temperature and AD mortality were evaluated across census regions using correlation analyses and Poisson regression models. To explore the future burden, subgroup-specific time series models (ARIMA or ETS) were applied to generate 20-year forecasts.
Results: In 2023, there were 4,418 AD deaths (AAMR 1.73 per 100,000; 95% CI 1.68– 1.78); rates were highest in the Midwest (1.96), in male (2.19 vs 1.24 in female), in non-Hispanic Black individuals (2.75), and in adults ≥ 85 years (11.67). From 1999– 2023, 86,943 deaths occurred and the overall AAMR declined (AAPC − 0.37), but reversed to sustained increases after 2013. Across the four census regions, the monthly AAMR was lowest in summer and highest in winter during 1999– 2023 (P < 0.05). A 10°F increase in temperature was associated with lower mortality risk (eg, South RR 0.889).
Conclusion: AD mortality has rebounded since 2013 with marked demographic and regional disparities. Lower temperatures and greater thermal variability are linked to higher mortality, supporting seasonally and region-tailored prevention and health-system preparedness.
Keywords: aortic dissection, mortality, ambient temperature, seasonality, health disparities
Introduction
Aortic dissection (AD) is a severe acute aortic syndrome associated with a high immediate mortality rate and a high incidence of complications among survivors in the acute phase.1 AD is defined by an intimal tear that allows blood to enter the space between the intimal and medial layers of the aortic wall, creating true and false lumens and resulting in separation of the vessel wall.2 According to the Stanford classification, involvement of the ascending aorta is classified as Stanford type A, whereas involvement confined to the descending aorta is classified as Stanford type B.3 However, the incidence, patient characteristics, and risk factors of AD are not fully understood.4,5 Current research highlights that AD is not uniformly distributed across populations. Factors such as age, sex, race, and geographic location significantly influence its incidence and outcomes. For instance, studies have shown that males are disproportionately affected compared to female, and that certain genetic conditions, such as Marfan syndrome, increase the risk of AD.6–9 Furthermore, the incidence of AD appears to be rising in many regions, particularly among older adults, which could be attributable to an aging population and increasing rates of hypertension and other cardiovascular risk factors.10,11
Epidemiological data on AD in the United States have been reported, but most series end before 2019 and therefore lack contemporary perspective.12–14 Our study provides an updated, nationwide characterisation of AD mortality with comprehensive subgroup analyses by census region, sex, race, urbanisation, and age. The association between ambient temperature and an increased incidence of AD has also attracted growing attention. Low ambient temperatures may induce sympathetic nervous system activation, peripheral vasoconstriction, and acute elevations in blood pressure, thereby increasing mechanical stress on the aortic wall.15 Temperature-related inflammatory and oxidative stress responses may further impair endothelial function and compromise the structural integrity of the aorta.16 Together, these haemodynamic and inflammatory processes increase susceptibility to intimal tearing and the development of AD. A multicenter case-crossover study from China showed that low ambient temperature and temperature decreases between adjacent days were associated with an increased risk of AD.17 Similarly, a nationwide time-stratified case-crossover study from Japan confirmed that low ambient temperature was associated with an increased risk of hospitalization for AD.18 Importantly, the increased risk of AD–related mortality attributable to low temperatures remains substantial even in predominantly tropical countries, such as Brazil.19 However, most existing studies have focused primarily on incidence or hospital admissions and are often limited to single cities, raising concerns about temporal and geographic confounding.17–21
The primary objective of this study is to elucidate the epidemiological characteristics of AD-related mortality in the United States, identifying high-risk groups and environmental determinants that could contribute to the development of targeted prevention strategies. Understanding these dynamics is crucial for improving clinical outcomes and resource allocation within healthcare systems, particularly in the context of an aging population susceptible to cardiovascular diseases. Furthermore, the findings from this study are intended to support future research efforts aimed at mitigating the burden of AD and enhancing patient care through tailored management approaches.
Materials and Methods
Mortality Data Source and Collection
Data for this study were obtained from the United States Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research (CDC WONDER). This population-based analysis included all deaths recorded in the CDC WONDER Multiple Cause of Death database that met the following inclusion criteria: (1) age at death ≥25 years; (2) underlying cause of death coded as AD; and (3) death occurring between 1999 and 2023 within the United States. Deaths not meeting these criteria were excluded from the analysis.
We extracted counts of deaths and AAMR attributable to AD among adults aged ≥25 years for the period 1999–2023. AD deaths were identified using the International Classification of Diseases, 10th Revision (ICD-10) code I71.0 as the underlying cause of death.22 Because CDC WONDER provides aggregated, de-identified mortality data without individual-level clinical information, no additional exclusion criteria (eg, comorbidities or treatment characteristics) could be applied.
AD mortality data were stratified by demographic and geographic characteristics, including census region, state, sex, race/ethnicity, level of urbanization, and age group.23 The four United States Census regions were Northeast, Midwest, South, and West. Race/ethnicity categories were Hispanic or Latino; Not Hispanic or Latino–Black or African American (NH Black); Not Hispanic or Latino–White (NH White); and Not Hispanic or Latino–Other (NH Other). Age was categorized into 10-year bands: 25–34 years, 35–44 years, 45–54 years, 55–64 years, 65–74 years, 75–84 years, and ≥85 years.
Temperature Data Source and Collection
From the CDC WONDER North America Land Data Assimilation System (NLDAS) Daily Air Temperatures and Heat Index (1979–2011) request, we obtained temperature data for the four United States census regions for the period 1999–2011. We subsequently conducted a separate analysis using NLDAS to obtain the corresponding temperature data for 2012–2023. The downloaded dataset was the NLDAS Primary Forcing Data L4 Monthly 0.125×0.125 Degree V2.0 (NLDAS_FORA0125_M).24
Ambient air temperature metrics included monthly mean maximum temperature (Max Temp), monthly mean minimum temperature (Min Temp), monthly mean temperature (Mean Temp), the within-month temperature range (Monthly Range, defined as Max Temp-Min Temp), and the month-to-month temperature range (Month-to-Month Range, defined as the absolute difference between consecutive months’ Mean Temp). All temperatures are expressed in degrees Fahrenheit (°F).
Statistical Analysis
We calculated age-adjusted mortality rates (AAMRs) per 100,000 population using direct standardisation to the 2000 United States standard population to account for temporal changes in age structure and ensure comparability across years.25 From AAMRs at each time point, we derived the average annual percent change (AAPC) with corresponding 95% confidence intervals (CI).
To assess trends in AAMR, we applied the Joinpoint Regression Program, version 5.0.2 (National Cancer Institute), fitting log-linear models to evaluate temporal patterns. The optimal number of joinpoints was selected by the software’s model-selection procedure. Annual percent changes (APC) and 95% CIs were estimated using a grid-search strategy allowing 0–2 joinpoints, with permutation testing and parametric methods for inference.
AAMR for AD from 1999 to 2023 were extracted and converted into annual time series. Variance stabilization was performed using Box-Cox transformation with bias-adjusted back-transformation. The minimum order of differencing was determined using the KPSS test to ensure stationarity. Three candidate models were fitted for each subgroup (sex and the United States census region): non-seasonal autoregressive integrated moving average (ARIMA), exponential smoothing state space models (ETS, including damped trend forms), and TBATS. Model performance was evaluated through rolling-origin cross-validation with a 3-year forecast horizon, using root mean squared error (RMSE) as the selection criterion. The best-performing model for each subgroup was refitted on the full dataset and used to generate 20-year forecasts (through 2043), with both 80% and 95% prediction intervals. The COVID-19 period (2019–2021) was indicated graphically but not incorporated as a predictor.
For the association between crude AD mortality and season, we stratified analyses by the United States census region (Northeast, Midwest, South, West) and by season-spring (March-May), summer (June-August), autumn (September-November), and winter (December-February). Within each stratum, we computed the mean monthly crude mortality rate (per 100,000) and its 95% CI using the t distribution. Between-season differences within regions were evaluated using one-way analysis of variance (ANOVA), followed by Tukey’s honestly significant difference (HSD) post-hoc comparisons; multiplicity-adjusted P values are reported.
For correlations between crude mortality and temperature metrics, we calculated Spearman’s rank correlation coefficients (r) and two-sided P values within each stratum. To visualise exposure–response patterns without excessive smoothing, we fitted separate generalized additive models (GAM) in each stratum using mgcv with a smooth term for temperature.
For lagged temperature–mortality analyses, monthly mean temperature was centred within each United States census region and scaled per +10 °F. We specified a lag structure of 0–3 months within regions (not pooled across regions). In single-lag models, each lag (0–3) entered a Poisson log-linear regression with a log(population) offset; we report relative risks (RR) per +10 °F with 95% CIs. In multi-lag models, lags 0–3 were entered simultaneously; we report lag-specific partial effects and the cumulative effect over lags 0–3, obtained by summing the relevant coefficients, estimating variance via the delta method, and exponentiating to yield the cumulative RR.
Two-sided P<0.05 was considered statistically significant. All analyses and visualisations were performed in R version 4.4.0.
Results
Characteristics of Aortic Dissection Mortality in the United States in 2023
In 2023, there were 4,418 deaths from AD among adults aged ≥25 years in the United States, corresponding to an AAMR of 1.73 (95% CI: 1.68–1.78) (Figure 1A and Table 1 and Supplementary Table S1). Across census regions, mortality was highest in the Midwest (1,054 deaths; AAMR 1.96, 95% CI: 1.84–2.08), followed by the South (1,636 deaths; AAMR 1.66, 95% CI: 1.58–1.75), West (1,017 deaths; AAMR 1.71, 95% CI: 1.60–1.82), and Northeast (711 deaths; AAMR 1.52, 95% CI: 1.40–1.64). Marked geographic variation was observed at the state level. California reported the largest absolute number of AD deaths (n=371), followed by Florida (n=317) and Texas (n=314). Vermont had the highest AAMR (3.35, 95% CI: 1.72–5.28), followed by Alaska (3.28, 95% CI: 1.63–5.24) and Hawaii (3.05, 95% CI: 2.14–4.22) (Figure 1B–E and Supplementary Figure S1A–C).
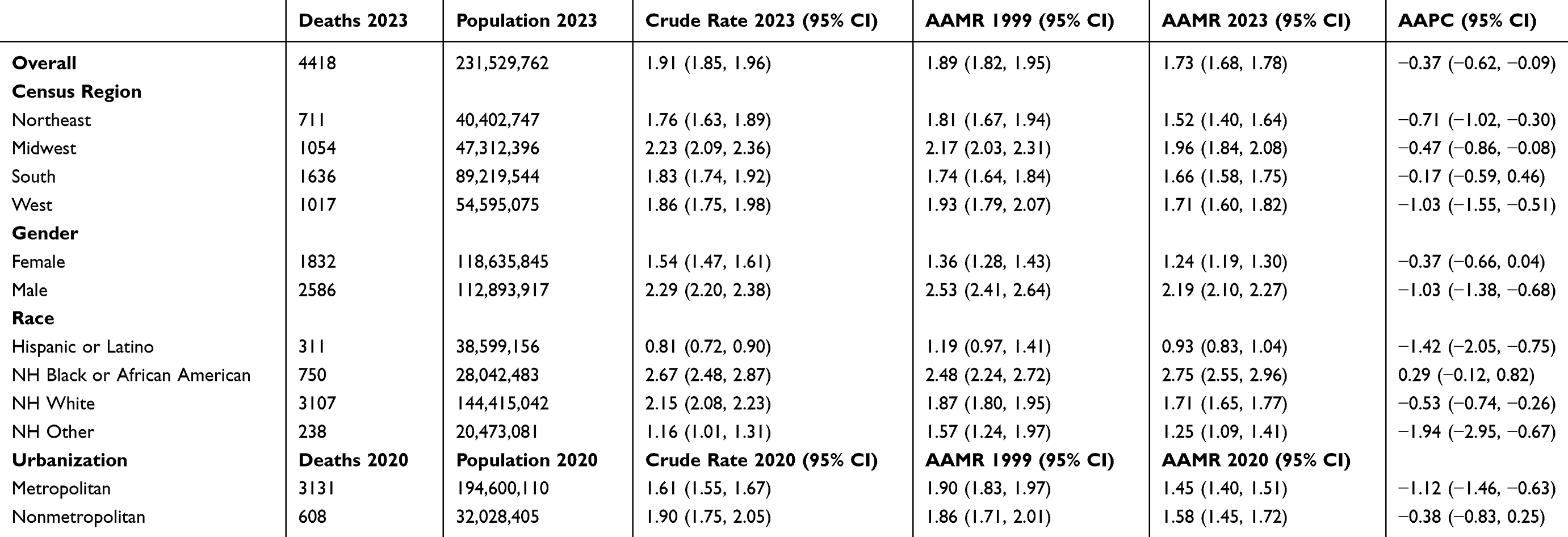 |
Table 1 Counts and Age-Adjusted Mortality Rates (per 100,000) from Aortic Dissection Among ≥ 25 years Adults, Stratified by Sex, Race, Census Region, and Urbanization Level |
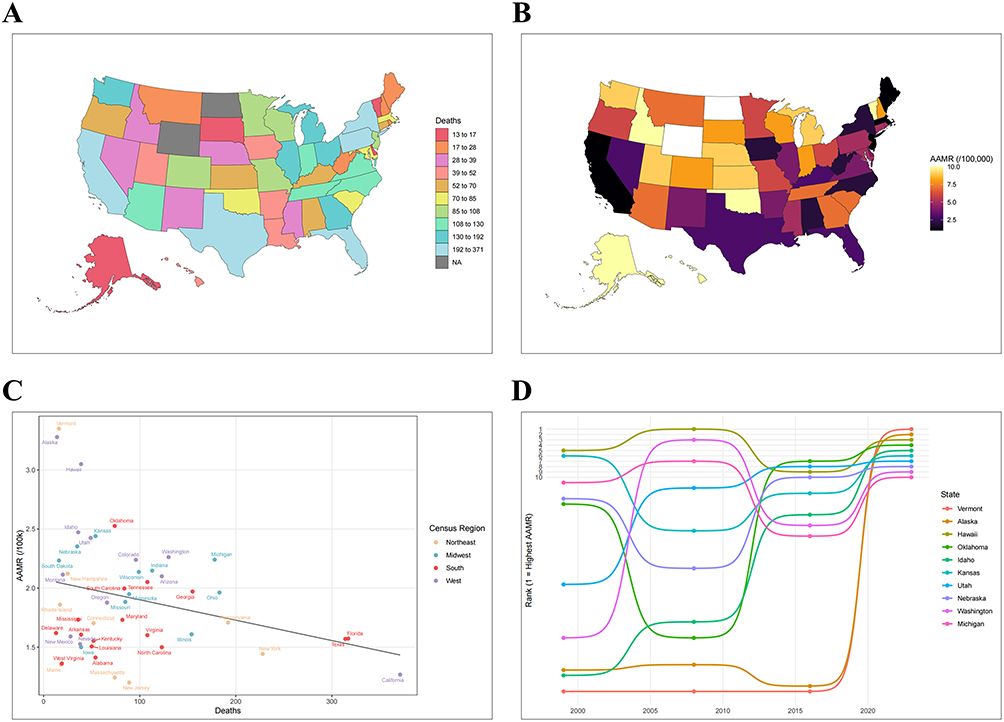 |
Figure 1 continued. |
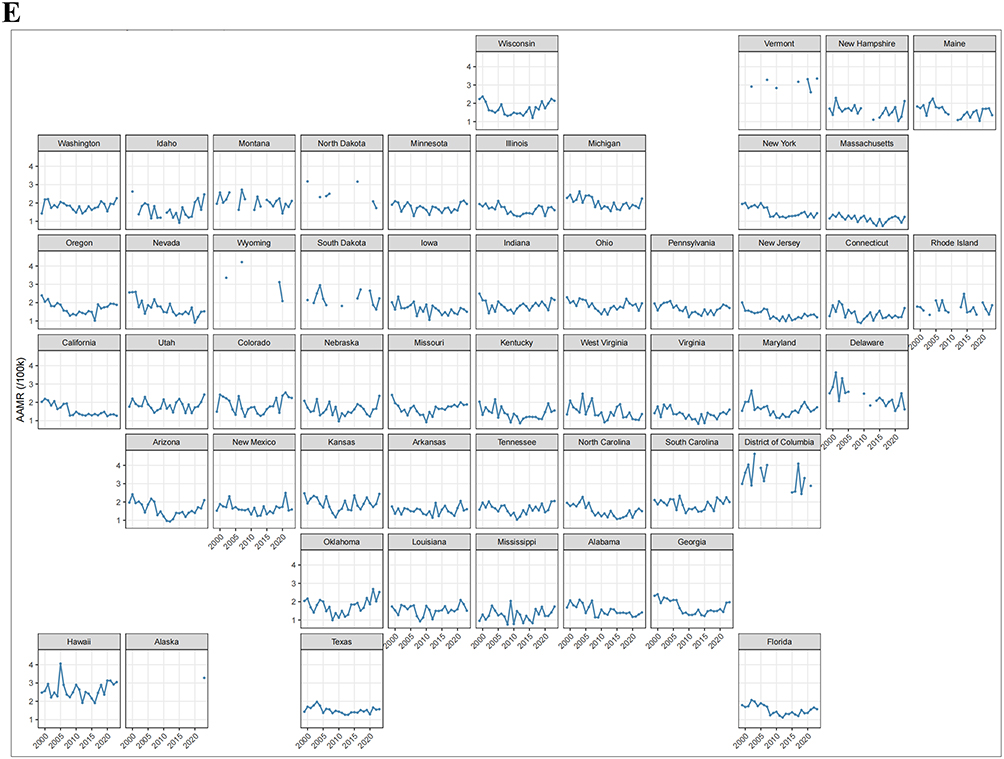 |
Figure 1 The United States aortic dissection (AD) mortality, 1999–2023. (A) State-level AD death counts in 2023. (B) State-level age-adjusted mortality rates (AAMR) in 2023 (per 100,000; directly standardised to the 2000 United States population). (C) Scatterplot of 2023 state death counts versus AAMR. (D) Top 10 states by AAMR in 2023. (E) State-level AAMR trajectories, 1999–2023. |
Sex-specific differences were notable: females accounted for 1,832 deaths (AAMR 1.24, 95% CI: 1.19–1.30), whereas males accounted for 2,586 deaths (AAMR 2.19, 95% CI: 2.10–2.27) (Table 1 and Supplementary Table S1). Racial disparities were also evident: non-Hispanic Black or African American individuals had the highest AAMR (2.75, 95% CI: 2.55–2.96), whereas Hispanic or Latino individuals had the lowest (0.93, 95% CI: 0.83–1.04). By level of urbanization, AAMR was slightly higher in nonmetropolitan areas (1.58, 95% CI: 1.45–1.72) than in metropolitan areas (1.45, 95% CI: 1.40–1.51).
Age-stratified analyses showed the largest number of deaths among individuals aged 75–84 years (n=978), followed by those aged 65–74 years (n=862) and 55–64 years (n=826) (Table 1 and Supplementary Table S1). The highest mortality rate occurred among adults aged ≥85 years (AAMR 11.67, 95% CI: 10.82–12.52), followed by those aged 75–84 years (AAMR 5.32, 95% CI: 4.99–5.66).
Temporal Trends in Aortic Dissection Mortality
From 1999 through 2023, a total of 86,943 AD deaths occurred among the United States adults aged ≥25 years. Although the absolute number of deaths increased during this period, the overall AAMR declined, with an average annual percent change (AAPC) of −0.37 (95% CI: −0.62 to −0.09) (Supplementary Table S2). Regionally, the most pronounced declines were observed in the West (AAPC −1.03, 95% CI: −1.55 to −0.51) and Northeast (AAPC −0.71, 95% CI: −1.02 to −0.30) (Figure 2A). At the state level (Figure 1E), California experienced the steepest decline (AAPC −2.07, 95% CI: −2.84 to −1.36), followed by Alabama (AAPC −1.75, 95% CI: −2.57 to −0.94). In contrast, several states-including Tennessee, South Carolina, Washington, Arkansas, Louisiana, Minnesota, Colorado, and Oklahoma-showed increasing trends, with the largest rise in Oklahoma (AAPC 0.60, 95% CI: −0.95 to 2.40). Figure 2 continued. Figure 2 Temporal evolution of aortic dissection (AD) deaths and mortality, 1999–2023. Trends in annual death counts and age-adjusted mortality rates (AAMR) stratified by (A) census region (Northeast, Midwest, South, West), (B) sex, (C) urbanisation (metropolitan vs nonmetropolitan), and (D) age group (25–34, 35–44, 45–54, 55–64, 65–74, 75–84, ≥85 years).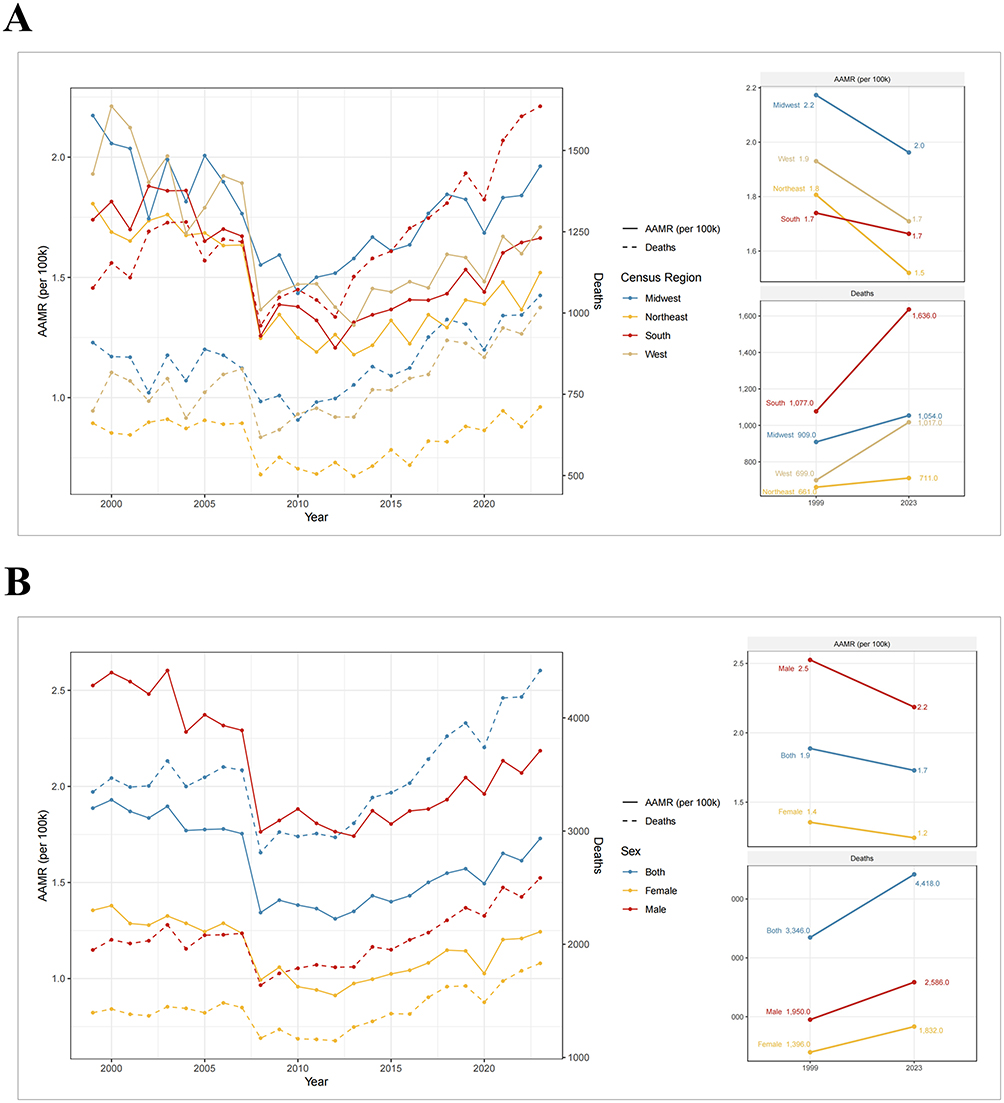
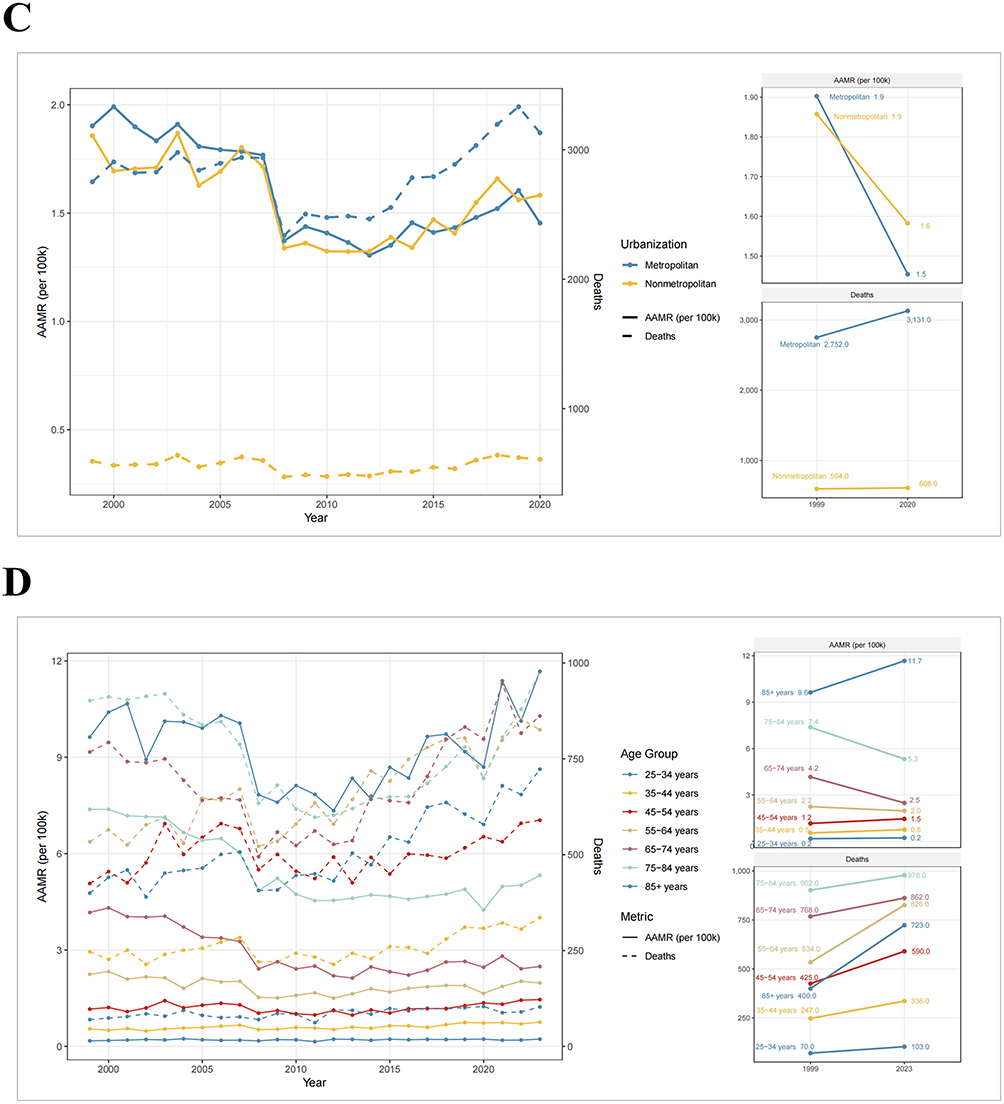
Sex-stratified analyses demonstrated declining AAMRs in both female (AAPC −0.37, 95% CI: −0.66 to 0.04) and male (AAPC −1.03, 95% CI: −1.38 to −0.68) (Figure 2B and Supplementary Table S2). Among racial groups, only non-Hispanic Black or African American individuals showed an increasing trend (AAPC 0.29, 95% CI: −0.12 to 0.82) (Supplementary Figure S2A). By urbanization, declines were steeper in metropolitan areas (AAPC −1.12, 95% CI: −1.46 to −0.63) than in nonmetropolitan areas (Figure 2C).
Age-specific analyses revealed decreasing trends in AAMR among adults aged 55–84 years, with the steepest decline among those aged 65–74 years (AAPC −2.33, 95% CI: −2.98 to −1.65) (Figure 2D and Supplementary Table S2). In contrast, mortality increased among adults aged 25–54 years, most prominently in the 35–44 years group (AAPC 1.44, 95% CI: 0.89–2.03).
Joinpoint Analyses of Aortic Dissection Mortality
Joinpoint regression identified inflection points in recent years. Since 2013, AAMRs have begun to rise across all census regions, with the sharpest increase in the South (APC 2.71, 2012–2023) (Figure 3A and Supplementary Table S3). Sex-stratified analyses showed mortality rising after 2011 in female (APC 2.52, 2011–2023) and after 2012 in male (APC 1.86, 2012–2023) (Figure 3B). Racial disparities persisted, with non-Hispanic Black or African American individuals showing a consistent increase from 2009 onward (APC 2.67, 2009–2023) (Supplementary Figure S2B). Both metropolitan (APC 1.47, 2010–2023) and nonmetropolitan (APC 2.49, 2010–2023) areas demonstrated significant upward trends (Figure 3C).
 |
Figure 3 Joinpoint analysis of aortic dissection (AD) mortality, 1999–2023. Joinpoint regression of age-adjusted mortality rates (AAMR) with estimated annual percent change (APC) within segments, stratified by (A) census region, (B) sex, (C) urbanisation, and (D) age group. *Indicates that the APC is significantly different from zero at the alpha = 0.05 level. |
By age, mortality in adults aged 25–44 years increased steadily without identifiable joinpoints (Figure 3D and Supplementary Table S3). Other age groups showed a shift from declining to rising trends after 2012, with the sharpest increase among adults aged 45–54 years (APC 3.36, 2011–2023).
Forecasting of Mortality for Aortic Dissection by Sex and Census Region
Figure 4A–F illustrates historical and forecasted AAMR for AD stratified by sex and the United States census region. Among females and males (Figure 4A and B), AD-related AAMR showed a modest decline in the early 2000s, stabilization in the 2010s, and a plateau during the COVID-19 period (2019–2021). Forecasts generated by damped ETS models indicated a gradual increase in AD mortality over the next two decades, with males consistently projected to have higher rates than females.
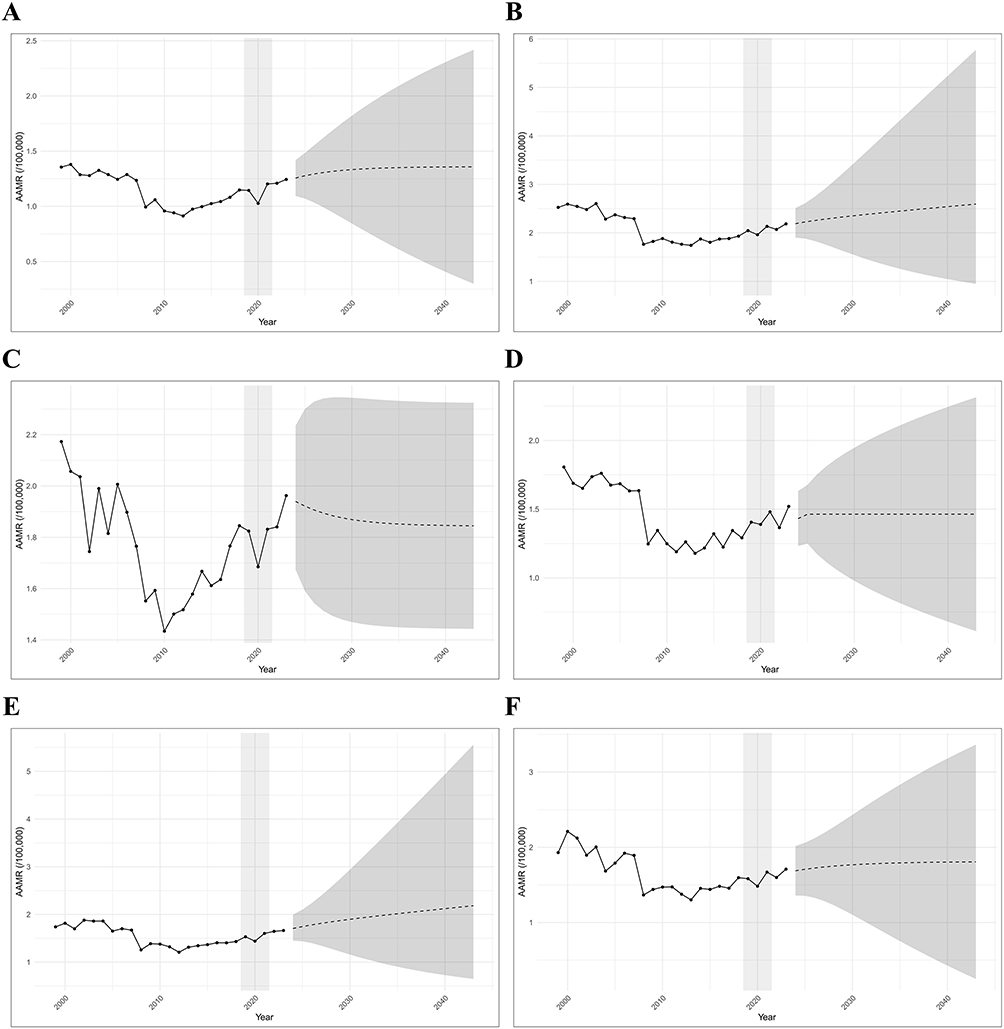 |
Figure 4 Forecasts of age-adjusted mortality rates (AAMR) for aortic dissection (AD) by sex and census region. Observed AD-related AAMR are presented as solid black lines, with model-based forecasts shown as dashed lines and 95% prediction intervals shaded in gray. The vertical shaded bar denotes the COVID-19 period (2019–2021). Subgroups are displayed as: (A) female (best-fitting model: ETS), (B) male (best-fitting model: ETS), (C) Midwest (best-fitting model: ARIMA), (D) Northeast (best-fitting model: ARIMA), (E) South (best-fitting model: ETS), and (F) West (best-fitting model: ETS). The shaded area denotes COVID-19 period (2019–2021). |
Regional analyses revealed pronounced heterogeneity. The Midwest and Northeast demonstrated declines in AD mortality after the mid-2000s; however, ARIMA-based forecasts suggested a mild rebound in subsequent years, albeit with widening uncertainty over time (Figure 4C and D). The South exhibited persistently elevated mortality throughout the study period, and forecasts predicted a continued upward trajectory under a damped ETS model (Figure 4E). By contrast, the West maintained the lowest observed AAMR but was still projected to experience gradual increases in the future (Figure 4F). Collectively, these projections highlight the persistence and potential escalation of the AD burden across sexes and regions, with particularly concerning trends in the South and Midwest.
Effects of Temperature and Temperature Variability on Aortic Dissection Mortality
Mortality from AD exhibited pronounced seasonal variation. Between 1999 and 2011, monthly AAMRs were inversely correlated with average monthly temperatures across census regions (Figure 5A). Seasonal aggregation confirmed that AAMRs were lowest in summer and highest in winter. Compared with summer, winter AAMRs were significantly elevated across all regions (P < 0.001), suggesting that lower temperatures are associated with higher mortality risk (Figure 5B).Correlation analyses demonstrated significant negative associations between AAMR and temperature indicators (average high, low, mean, and variability) in all census regions, indicating that mortality risk decreased with rising temperature (Figure 5C and Supplementary Table S4). Lagged analyses showed strong contemporaneous associations between lower temperatures and higher mortality (Lag 0 correlation coefficients ranging from −0.44 to −0.55). By Lag 3 (three months later), correlations weakened or became slightly positive (eg, West region, r=0.13) (Figure 5D and Supplementary Table S5).Poisson regression models indicated that a 10°F increase in temperature was associated with significantly reduced mortality risk in most regions under all-lags models (eg, South, RR=0.889; 95% CI: 0.849–0.931) (Figure 5E). Similar results were observed in single-lag models.
 |
Figure 5 Associations between temperature metrics and aortic dissection (AD) mortality, 1999–2011. (A) Monthly time series of mean air temperature and monthly AD age-adjusted mortality rates (AAMR) by census region. (B) Seasonal comparison of mean monthly crude AD mortality (per 100,000) across spring (Mar–May), summer (Jun–Aug), autumn (Sep–Nov), and winter (Dec–Feb). (C) Spearman correlations between monthly AD AAMR and temperature indicators: monthly mean maximum (Max Temp), mean minimum (Min Temp), mean (Mean Temp), within-month range (Monthly Range = Max−Min), and month-to-month range (Month-to-Month Range = |Mean Temp_{m} − Mean Temp_{m−1}|). (D) Lagged Spearman correlations between monthly AD AAMR and Mean Temp at lags 0–3 months. (E) Poisson regression estimates of relative risk (RR) per +10 °F increase in temperature under single-lag and all-lags specifications (lag 0–3). |
Subsequently, because the temperature data were derived from different sources, we used the period 2012–2023 as a validation analysis (Supplementary Figure S3A–D). When month-to-month temperature changes were analysed by direction, cooling (ΔTemp < 0) was consistently associated with increases in crude mortality in the Northeast (r = −0.34, p = 0.0037) and the West (r = −0.38, p = 0.0014), whereas warming showed no significant associations (Supplementary Figure S3C). This directional asymmetry suggests a dominant cold-related effect. In contrast, analyses based on the absolute magnitude of temperature change (|ΔTemp|) demonstrated significant positive associations with mortality variability in the Northeast (r = 0.25, p = 0.0026) and the West (r = 0.19, p = 0.023), indicating that larger temperature fluctuations, irrespective of direction, were associated with greater mortality instability. No significant associations were observed in the Midwest or the South, highlighting substantial regional heterogeneity (Supplementary Figure S3B).
Discussion
In this nationwide, population-based study drawing on the United States CDC WONDER data from 1999–2023, we report several key observations regarding AD mortality. First, the overall AD mortality rate declined initially but has risen continuously since 2013. Second, males have higher AD mortality than female, although the post-2013 increase has been steeper in female. Third, Black or African American individuals exhibit the highest AD mortality, with an upward trajectory over time. Compared with metropolitan areas, nonmetropolitan areas show lower AD mortality and a faster rate of decline. Fourth, AD mortality increases with age; however, since 2012, upward trends are evident across age strata, most prominently in those aged 45–54 years. In analyses integrating monthly temperature metrics (1999–2023), colder conditions and abrupt temperature changes were associated with higher AD mortality risk, whereas warmer temperatures appeared protective. To our knowledge, this study provides the most up-to-date characterization of AD mortality in the United States and is the first to evaluate the contribution of month-to-month temperature variation to AD mortality risk.
Epidemiological evidence on AD in the United States remains limited. Salik et al described demographic and geographic disparities in AD mortality from 1999–2019, noting an initial decline followed by a persistent increase from 2012–2019, with particularly marked rises among female and non-Hispanic Black or African American populations.12 Other series pre-date 2019.26–28 Additional reports have addressed AD-related mortality in the context of specific comorbidities-including pregnancy, hypertension, heart transplantation, mental health disorders, and diabetes.29–34 Against this background, our study offers essential, contemporary updates to the epidemiology of AD in the United States.
Beyond epidemiology, identifying risk factors for the onset and mortality of AD is also crucial. Multiple studies have shown that male sex, aging, hypertension, and hyperlipidemia are independent risk factors for AD.6,8,35 Among patients with AD, male account for approximately 65%, which may be attributed to the protective effects of estrogen on the cardiovascular system in females, as well as a higher prevalence of risk factors such as smoking, hypertension, and atherosclerosis in males.36–38 Aging promotes AD by inducing progressive medial degeneration, characterized by elastic fiber fragmentation, loss of the contractile phenotype of vascular smooth muscle cells (VSMCs), chronic low-grade inflammation, and extracellular matrix dysregulation, ultimately rendering the aging aorta structurally fragile and more susceptible to acute hemodynamic stress.39,40 In addition, non-Hispanic Black individuals tend to be diagnosed with AD at a younger age and are more likely to have histories of cocaine use, hypertension, and diabetes.7,41 Collectively, these studies highlight a close association between AD development and lifestyle-related factors.
The impact of ambient temperature on vascular disease is increasingly recognised.42–45 In a case-crossover analysis from the Registry of AD in China encompassing 8,182 acute aortic dissection (AAD) cases across 14 tertiary hospitals in 11 cities (2009–2019), lower ambient temperatures and day-to-day temperature drops were associated with higher AAD incidence.17,46 A separate nationwide Chinese study including 40,270 AAD patients likewise demonstrated significant associations between low temperature, falling temperature, and AAD onset.20 Consistent findings were reported in Japan, where a nationwide time-stratified case-crossover study linked lower ambient temperature with increased AAD-related hospitalisation risk.18 Additional reports corroborate associations between AD incidence or operative volume and low ambient temperature or hypothermia.21,47–53 Notably, a single nationwide case-crossover analysis from Brazil (a predominantly tropical country) found that lower temperatures were associated with increased mortality from aortic aneurysm and dissection.19 Against this backdrop, our study is, to our knowledge, the first nationwide, population-based analysis in the United States leveraging CDC WONDER to examine, using time-series methods, the association between monthly temperature patterns and AD mortality.
Globally, the incidence and mortality of AD exhibit marked geographic heterogeneity. The global incidence of AD is estimated at approximately 2.6 to 3.5 cases per 100,000 person; however, it is higher in certain countries, including about 6 per 100,000 person in the United Kingdom,54 7.2 per 100,000 in Sweden,55 4.99 per 100,000 in New Zealand,56 and 2.35 per 100,000 person in China.8 Nevertheless, owing to the lack of comprehensive, global prospective population-based studies, high-quality epidemiological data on AD remain limited. Nationally representative or global data on AD mortality are also scarce. Even within the Global Burden of Disease (GBD) database, which covers more than 300 conditions, only mortality data for aortic aneurysm are available.57,58 In addition, differences in global climate zones and patterns of temperature exposure further exacerbate the burden of AD. Although global warming is associated with rising mean temperatures, climate change is increasingly characterized by amplified temperature variability and more frequent extreme weather events, including sudden cold spells.59,60 Such temperature fluctuations adversely affect the cardiovascular system and may remain a key driver of future AD incidence and mortality.42,61
From a mechanistic perspective, low ambient temperature and abrupt temperature fluctuations may increase the risk of AD onset and mortality through a pathway of acute triggering superimposed on underlying vulnerability. First, cold exposure rapidly activates the sympathetic nervous system and induces peripheral vasoconstriction, leading to increased blood pressure variability and acute elevations in aortic wall stress and shear forces, thereby facilitating intimal tearing.21,62 Second, winter is accompanied by seasonal changes in blood rheology and coagulation tendency, such as increased plasma viscosity, fibrinogen levels, and coagulation factor activity, together with enhanced inflammation and endothelial dysfunction.63,64 These changes render the aortic media more susceptible to stress and may aggravate organ hypoperfusion and the risk of complications. Finally, behavioral factors associated with cold seasons, including infections, reduced or altered physical activity, and delays in seeking medical care, may further contribute to an increased risk of AD.65,66
There were several limitations in this study. First, this study spans a long time horizon and a large population, but it lacks granular, patient-level clinical information-such as pre-existing comorbidities and treatments-that is essential for disentangling the complexity of outcomes in AD. Second, the absence of mechanistic laboratory validation constrains the biological inferences that can be drawn from the epidemiological findings. In addition, heterogeneity in state-level data collection practices may introduce bias and obscure true regional differences in mortality. Third, our analysis of monthly temperatures across the four United States census regions may be subject to regional bias in the averaged values, and the use of monthly means may obscure diurnal variation and abrupt temperature changes within a month. Analyses conducted at the level of the four United States census regions may also be susceptible to spatial aggregation and ecological bias.
Despite these limitations, our time-series framework, multiple subgroup analyses, and complementary statistical approaches support the robustness of the results. We show that, although the United States AD mortality declined overall, a rebound has emerged in recent years, with pronounced heterogeneity by region, sex, race, urbanisation, and age. Importantly, we identify seasonality in AD mortality, with low ambient temperature emerging as a key risk factor for increased mortality. Given the abrupt presentation and high lethality of AD, these findings have practical implications for prevention and preparedness—including cold-weather protection strategies, winter hospital surge planning, and clinician-led cold-weather health education.
Conclusion
The United States AD mortality exhibits a recent upswing superimposed on long-term declines, with disproportionate burdens in males, Black populations, and older adults, and heterogeneity across regions and urbanisation levels. Winter-dominant seasonality and inverse temperature–mortality relationships indicate that cold exposure and thermal volatility are important population-level hazards. These findings support targeted cold-weather protection (patient education, community alerts, and home-heating support), winter surge planning for hospitals, and geographically tailored adaptation strategies. Future work should integrate patient-level clinical data with high-resolution meteorological exposures (including diurnal variability) to refine risk estimates and inform precision prevention.
Data Sharing Statement
The datasets analysed during the current study are available in the public database, https://wonder.cdc.gov/; https://ldas.gsfc.nasa.gov/nldas/. The data used during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This study used publicly available, de-identified, and aggregated mortality data from the CDC WONDER database. No individual-level or identifiable information was accessed, and no attempt was made to re-identify individuals. In accordance with the National Statement on Ethical Conduct in Human Research (Australia, 2023), Section 5.1.17 (a) and (d), this research is eligible for exemption from ethics review, and it was confirmed with the Ethics Committee of the Western Sydney Local Health District that no additional ethics approval was required.
Acknowledgments
We thank the CDC WONDER and NLDAS project teams for providing free and open-access data. We also thank the YIWANDOU team for their assistance with data analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Health and Medical Research Council (NHMRC) of Australia (Grant No. 2027965).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rylski B, Schilling O, Czerny M. Acute aortic dissection: evidence, uncertainties, and future therapies. Eur Heart J. 2023;44(10):813–16. doi:10.1093/eurheartj/ehac757
2. Mazzolai L, Teixido-Tura G, Lanzi S, et al. ESC Guidelines for the management of peripheral arterial and aortic diseases. Eur Heart J. 2024;45(36):3538–3700. doi:10.1093/eurheartj/ehae179
3. Carrel T, Sundt TM 3rd, von Kodolitsch Y, Czerny M. Acute aortic dissection. Lancet. 2023;401(10378):773–788. doi:10.1016/S0140-6736(22)01970-5
4. Hameed I, Cifu AS, Vallabhajosyula P. Management of thoracic aortic dissection. JAMA. 2023;329(9):756–757. doi:10.1001/jama.2023.0265
5. Hofmann Bowman MA, Eagle KA. Challenges and opportunities in aortic dissection: the journey to personalized medicine. Circulation. 2024;150(15):1155–1157. doi:10.1161/CIRCULATIONAHA.124.071088
6. Hibino M, Otaki Y, Kobeissi E, et al. Blood Pressure, hypertension, and the risk of aortic dissection incidence and mortality: results from the J-SCH Study, the UK biobank study, and a meta-analysis of cohort studies. Circulation. 2022;145(9):633–644. doi:10.1161/CIRCULATIONAHA.121.056546
7. Bossone E, Eagle KA. Epidemiology and management of aortic disease: aortic aneurysms and acute aortic syndromes. Nat Rev Cardiol. 2021;18(5):331–348. doi:10.1038/s41569-020-00472-6
8. Chen D, Fang K, Luo M, Xiao Y, Zhao Y, Shu C. Aortic dissection incidence and risk factor analysis: findings from the china kadoorie biobank. Eur J Vasc Endovascular Surg. 2025;69(4):611–618. doi:10.1016/j.ejvs.2024.12.003
9. Lopez-Sainz A, Mila L, Rodriguez-Palomares J, et al. Aortic branch aneurysms and vascular risk in patients with marfan syndrome. J Am Coll Cardiol. 2021;77(24):3005–3012. doi:10.1016/j.jacc.2021.04.054
10. Suzuki Y, Kaneko H, Yano Y, et al. Dose-dependent relationship of blood pressure and glycaemic status with risk of aortic dissection and aneurysm. Eur. J. Prev. Cardiol. 2022;29(18):2338–2346. doi:10.1093/eurjpc/zwac205
11. Wang R, Yu X, Halvorsen SC, Suki B, Zhang Y. Dissection propagation via avalanches in human descending thoracic aorta: effect of aging. Acta Biomater. 2025;202:305–316. doi:10.1016/j.actbio.2025.06.056
12. Nazir S, Ariss RW, Minhas AMK, et al. Demographic and regional trends of mortality in patients with aortic dissection in the United States, 1999 to 2019. J. Am. Heart Assoc. 2022;11(7):e024533. doi:10.1161/JAHA.121.024533
13. Sen I, Erben YM, Franco-Mesa C, DeMartino RR. Epidemiology of aortic dissection. Semin Vasc Surg. 2021;34(1):10–17. doi:10.1053/j.semvascsurg.2021.02.003
14. Well A, Mizrahi M, Johnson G, et al. Aortic dissection and ruptures in adult congenital heart disease in Texas from 2009 to 2019. Eur J Cardiothorac Surg. 2022;61(2):309–317. doi:10.1093/ejcts/ezab416
15. Goel H, Shah K, Kumar A, Hippen JT, Nadar SK. Temperature, cardiovascular mortality, and the role of hypertension and renin-angiotensin-aldosterone axis in seasonal adversity: a narrative review. J Human Hypertens. 2022;36(12):1035–1047. doi:10.1038/s41371-022-00707-8
16. Awad EM, Khan SY, Sokolikova B, et al. Cold induces reactive oxygen species production and activation of the NF-kappa B response in endothelial cells and inflammation in vivo. J Thromb Haemost. 2013;11(9):1716–1726. doi:10.1111/jth.12357
17. Chen J, Gao Y, Jiang Y, et al. Low ambient temperature and temperature drop between neighbouring days and acute aortic dissection: a case-crossover study. Eur Heart J. 2022;43(3):228–235. doi:10.1093/eurheartj/ehab803
18. Kato K, Nishino T, Otsuka T, Seino Y, Kawada T. Nationwide analysis of the relationship between low ambient temperature and acute aortic dissection-related hospitalizations. Eur. J. Prev. Cardiol. 2025;32(4):317–324. doi:10.1093/eurjpc/zwae278
19. Huang HN, Li X, Peng Z, et al. Mortality risk and burden of aortic aneurysm and dissection attributable to low temperatures: a nationwide case-crossover analysis in Brazil, a predominantly tropical country. Environ. Int. 2024;190:108895. doi:10.1016/j.envint.2024.108895
20. Zhang Q, Peng L, Hu J, et al. Low temperature and temperature decline increase acute aortic dissection risk and burden: a nationwide case crossover analysis at hourly level among 40,270 patients. Lancet Reg. Health West. Pac. 2022;28:100562. doi:10.1016/j.lanwpc.2022.100562
21. Yu X, Xia L, Xiao J, et al. Association of daily mean temperature and temperature variability with onset risks of acute aortic dissection. J. Am. Heart Assoc. 2021;10(13):e020190. doi:10.1161/JAHA.120.020190
22. Paratz ED, Nadel J, Humphries J, et al. The aortic paradox: a nationwide analysis of 523 994 individual echocardiograms exploring fatal aortic dissection. Eur. Heart J. Cardiovasc. 2024;25(10):1423–1431. doi:10.1093/ehjci/jeae140
23. Ingram DD, Franco SJ. NCHS urban-rural classification scheme for counties. Vital and Health Statistics Series 2, Data Evaluation and Methods Research. 2013;2014(166):1–73.
24. Xia Y, Mitchell K, Ek M, et al. Continental-scale water and energy flux analysis and validation for the North American Land Data Assimilation System project Phase 2 (NLDAS-2): 1. Intercomparison and application of model products. Bioresource Technology. 2012;117:72–79. doi:10.1016/j.biortech.2012.04.061
25. Anderson RN, Rosenberg HM. Age standardization of death rates: implementation of the year 2000 standard. National vital statistics reports: from the centers for disease control and prevention, national center for health statistics, national vital statistics system. 1998;47(3):1–16,20.
26. Brown J, Usmani B, Arnaoutakis G, et al. 10-year trends in aortic dissection: mortality and weekend effect within the US nationwide emergency department sample (NEDS). The Heart Surg Forum. 2021;24(2):E336–e344. doi:10.1532/hsf.3681
27. DeCicco D, Dimachkie ZO, Khan MZ, Khan MS, Khan MU, Khan SU. Trends in location of death in patients with aortic aneurysm and dissection. Omega. 2022;85(3):574–578. doi:10.1177/0030222820951650
28. Sen I, D’Oria M, Weiss S, et al. Incidence and natural history of isolated abdominal aortic dissection: a population-based assessment from 1995 to 2015. J Vascular Surg. 2021;73(4):1198–1204.e1191. doi:10.1016/j.jvs.2020.07.090
29. Wang Y, Yin K, Datar Y, et al. Aortic dissection during pregnancy and puerperium: contemporary incidence and outcomes in the United States. J. Am. Heart Assoc. 2023;12(9):e028436. doi:10.1161/JAHA.122.028436
30. Sawlani N, Shroff A, Vidovich MI. Aortic dissection and mortality associated with pregnancy in the United States. J Am Coll Cardiol. 2015;65(15):1600–1601. doi:10.1016/j.jacc.2014.12.066
31. Tabassum S, Naeem F, Azhar F, Naeem A, Virk HUH, Paul TK. Trends and disparities in aortic dissection-related mortality among hypertensive patients in the United States (1999-2019): a nationwide analysis. Cardiovasc. Endocrinol. Metab. 2025;14(2):e00333. doi:10.1097/XCE.0000000000000333
32. Wang Y, Mohnot J, Yin K, Edwards NM, Dobrilovic N, Zhan Y. Type A aortic dissection in heart transplantation recipients in the United States. Transplant Proc. 2024;56(2):353–357. doi:10.1016/j.transproceed.2024.01.042
33. Blakeslee-Carter J, Menon AJ, Novak Z, Spangler EL, Beck AW, McFarland GE. Association of mental health disorders and aortic dissection. Ann Vasc Surg. 2021;77:217–225. doi:10.1016/j.avsg.2021.05.054
34. Chaudhry H, Dargham S, Mahfoud Z, Jayyousi A, Al Suwaidi J, Abi Khalil C. Diabetes is associated with lower in-hospital mortality in patients undergoing surgical repair for aortic aneurysm rupture. J Clin Med. 2025;14(12):4370. doi:10.3390/jcm14124370
35. Koba A, Yamagishi K, Sairenchi T, et al. Risk factors for mortality from aortic aneurysm and dissection: results from a 26-year follow-up of a community-based population. J. Am. Heart Assoc. 2023;12(8):e027045. doi:10.1161/JAHA.122.027045
36. Bossone E, Carbone A, Eagle KA. Gender differences in acute aortic dissection. J. Pers. Med. 2022;12(7):1148. doi:10.3390/jpm12071148
37. Qi X, Wang F, Chun C, et al. A validated mouse model capable of recapitulating the protective effects of female sex hormones on ascending aortic aneurysms and dissections (AADs). Physiological Reports. 2020;8(22):e14631. doi:10.14814/phy2.14631
38. Zhang R, Wang H, Cheng X, et al. High estrogen induces trans-differentiation of vascular smooth muscle cells to a macrophage-like phenotype resulting in aortic inflammation via inhibiting VHL/HIF1a/KLF4 axis. Aging. 2024;16(11):9876–9898. doi:10.18632/aging.205904
39. Liu ZL, Li Y, Lin YJ, et al. Aging aggravates aortic aneurysm and dissection via miR-1204-MYLK signaling axis in mice. Nat Commun. 2024;15(1):5985. doi:10.1038/s41467-024-50036-2
40. Beeche C, Zhao B, Tavolinejad H, et al. Early vascular aging determined by 3-dimensional aortic geometry: genetic determinants and clinical consequences. Circulation. 2025;152(11):748–761. doi:10.1161/CIRCULATIONAHA.125.074554
41. Bossone E, Pyeritz RE, O’Gara P, et al. Acute aortic dissection in blacks: insights from the international registry of acute aortic dissection. Am J Med. 2013;126(10):909–915. doi:10.1016/j.amjmed.2013.04.020
42. Alahmad B, Khraishah H, Royé D, et al. Associations between extreme temperatures and cardiovascular cause-specific mortality: results from 27 countries. Circulation. 2023;147(1):35–46. doi:10.1161/CIRCULATIONAHA.122.061832
43. Xu R, Huang S, Shi C, et al. Extreme temperature events, fine particulate matter, and myocardial infarction mortality. Circulation. 2023;148(4):312–323. doi:10.1161/CIRCULATIONAHA.122.063504
44. Ni W, Areal AT, Lechner K, et al. Low and high air temperature and cardiovascular risk. Atherosclerosis. 2025;406:119238. doi:10.1016/j.atherosclerosis.2025.119238
45. Achebak H, Rey G, Lloyd SJ, Quijal-Zamorano M, Méndez-Turrubiates RF, Ballester J. Ambient temperature and risk of cardiovascular and respiratory adverse health outcomes: a nationwide cross-sectional study from Spain. Eur. J. Prev. Cardiol. 2024;31(9):1080–1089. doi:10.1093/eurjpc/zwae021
46. Hibino M, Yanagawa B, Pandey AK, Verma S. Ambient temperature and aortic dissection: do pipes burst in freezing weather? Eur Heart J. 2022;43(3):236–238. doi:10.1093/eurheartj/ehab792
47. Ma WG, Li B, Zhang W, et al. Chronologic and climatic factors of acute aortic dissection: study of 1642 patients in two continents. Ann Thorac Surg. 2020;110(2):575–581. doi:10.1016/j.athoracsur.2019.11.013
48. Åström D O, Bjursten H, Oudin A, et al. Temperature effects on incidence of surgery for acute type A aortic dissection in the Nordics. Global Health Action. 2022;15(1):2139340. doi:10.1080/16549716.2022.2139340
49. Sadamatsu K, Sagara S, Oe K, Tashiro H, Yasunaga H. Meteorological and chronobiological factors and the occurrence of acute aortic dissection. Heart and Vessels. 2020;35(7):1003–1011. doi:10.1007/s00380-020-01569-1
50. Kurz SD, Mahlke H, Graw K, et al. Patterns in acute aortic dissection and a connection to meteorological conditions in Germany. PLoS One. 2024;19(1):e0296794. doi:10.1371/journal.pone.0296794
51. Zhang H, Yin L, Zhang Y, et al. Short-term effects of air pollution and weather changes on the occurrence of acute aortic dissection in a cold region. Front Public Health. 2023;11:1172532. doi:10.3389/fpubh.2023.1172532
52. Li Y, Ji C, Zhang J, Han Y. The effect of ambient temperature on the onset of acute Stanford type B aortic dissection. VASA Z Gefasskrankheiten. 2016;45(5):395–401. doi:10.1024/0301-1526/a000555
53. Yamato N, Fujikawa T. Effect of temperature changes between neighboring days on acute aortic dissection in non-heating periods. Lancet Reg. Health West. Pac. 2023;30:100662. doi:10.1016/j.lanwpc.2022.100662
54. Howard DP, Banerjee A, Fairhead JF, Perkins J, Silver LE, Rothwell PM. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford Vascular Study. Circulation. 2013;127(20):2031–2037. doi:10.1161/CIRCULATIONAHA.112.000483
55. Smedberg C, Steuer J, Leander K, Hultgren R. Sex differences and temporal trends in aortic dissection: a population-based study of incidence, treatment strategies, and outcome in Swedish patients during 15 years. Eur Heart J. 2020;41(26):2430–2438. doi:10.1093/eurheartj/ehaa446
56. Lim ET, Khanafer A. A glimpse into the incidence and mortality of aortic dissection in Aotearoa New Zealand. N Z Med J. 2023;136(1583):55–60. doi:10.26635/6965.6207
57. Wang H, Li Y, Fan K, et al. Global epidemiology of early-onset aortic aneurysm: temporal trends, risk factors, and future burden projections. J. Epidemiol. Glob. Health. 2025;15(1):25. doi:10.1007/s44197-025-00369-y
58. Fan K, Wang H, Li Y, et al. Global landscape of mortality and risk factors for aortic aneurysm in adults aged 55 years and older: insights from the global burden of disease study 2021. Criti Public Health. 2025;35(1):2575807. doi:10.1080/09581596.2025.2575807
59. Gao Y, Huang W, Zhao Q, et al. Global, regional, and national burden of mortality associated with cold spells during 2000-19: a three-stage modelling study. Lancet Planet Health. 2024;8(2):e108–e116. doi:10.1016/S2542-5196(23)00277-2
60. Chen K, Nasir K. Balancing the climate equation: the unseen cardiovascular threat of cold spells in a warming world. J Am Coll Cardiol. 2024;84(13):1160–1162. doi:10.1016/j.jacc.2024.07.017
61. Khraishah H, Alahmad B, Ostergard RL Jr, et al. Climate change and cardiovascular disease: implications for global health. Nat Rev Cardiol. 2022;19(12):798–812. doi:10.1038/s41569-022-00720-x
62. Reutersberg B, Pelisek J, Ouda A, de Rougemont O, Rössler F, Zimmermann A. Baroreceptors in the aortic arch and their potential role in aortic dissection and aneurysms. J Clin Med. 2022;11(5):1161. doi:10.3390/jcm11051161
63. Fröhlich M, Sund M, Russ S, et al. Seasonal variations of rheological and hemostatic parameters and acute-phase reactants in young, healthy subjects. Arteriosclerosis Thrombosis Vasc Biol. 1997;17(11):2692–2697. doi:10.1161/01.ATV.17.11.2692
64. Halonen JI, Zanobetti A, Sparrow D, Vokonas PS, Schwartz J. Associations between outdoor temperature and markers of inflammation: a cohort study. Environmental Health. 2010;9:42. doi:10.1186/1476-069X-9-42
65. Ikäheimo TM. Cardiovascular diseases, cold exposure and exercise. Temperature. 2018;5(2):123–146. doi:10.1080/23328940.2017.1414014
66. Takagi H, Ando T, Umemoto T. Meta-analysis of seasonal incidence of aortic dissection. Am J Cardiol. 2017;120(4):700–707. doi:10.1016/j.amjcard.2017.05.040
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Ambient Cold and Mortality in Pan-Arterial Diseases: A Nationwide Ecological Analysis of CDC WONDER Data
Wang H, Fan K, Li Y, Wang Z, Wang S, Zheng G
Vascular Health and Risk Management 2026, 22:589152
Published Date: 23 March 2026