")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 12
Sodium-Glucose Cotransporter-2 (SGLT2) Inhibitors: A Clinician’s Guide
Authors Simes BC , MacGregor GG
Received 15 May 2019
Accepted for publication 11 September 2019
Published 14 October 2019 Volume 2019:12 Pages 2125—2136
DOI https://doi.org/10.2147/DMSO.S212003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Bryce C Simes, Gordon G MacGregor
Alabama College of Osteopathic Medicine, Dothan, AL, USA
Correspondence: Bryce C Simes
Alabama College of Osteopathic Medicine, 445 Health Sciences Blvd., Dothan, AL 36303, USA
Tel +1 205 904-504-8897
Fax +1 205 334-699-2268
Email [email protected]
Abstract: This comprehensive review covers the historical background, physiology, application in type 2 diabetes, novel uses, cardiovascular benefits, side effects and contraindications of sodium-glucose cotransporter-2 (SGLT2) inhibitors. SGLT2 inhibitors are an insulin-independent class of oral antihyperglycemic medication that clinicians use in the treatment of type 2 diabetes. Multiple landmark clinical trials support the effectiveness of SGLT2 inhibitors in reducing blood glucose levels, but it is important to understand when to properly utilize them. SGLT2 inhibitors are the most beneficial as an adjunct medication in addition to metformin in patients with a history of cardiovascular or renal disease who need further hemoglobin A1c reduction. The novel mechanism of action also demands clinicians be aware of the side effects not typically experienced with other oral antihyperglycemic drugs, such as genital tract infections, lower leg amputations, electrolyte disturbances and bone fractures. On top of their benefits in type 2 diabetes, novel uses for SGLT2 inhibitors are being uncovered. Diabetic patients with non-alcoholic fatty liver disease, who are at an increased risk of cirrhosis and hepatocellular carcinoma, experience a clinically significant reduction in serum alanine aminotransferase levels. SGLT2 inhibitors are also effective at lowering body weight in obese individuals and decreasing systolic blood pressure. Dual SGLT1/SGLT2 inhibitors are currently being investigated as possibly the first oral medication for type 1 diabetes.
Keywords: SGLT2 inhibitors, type 2 diabetes, canagliflozin, empagliflozin, dapagliflozin, ertugliflozin
Background And Physiology
The kidney’s role in glucose homeostasis has been observed by researchers as early as the 1930’s. This research documented that almost all of the glucose filtered by the glomerulus was then reabsorbed by the proximal tubule of the kidney. They also found that glucose reabsorption could be inhibited with the use of phlorizin, a naturally occurring phenolic glycoside found in the bark of apple trees.1,2 A healthy kidney can reabsorb up to 180 g of glucose from the glomerular filtrate each day.3 However, the exact mechanism of this glucose reabsorption has not been completely understood until recently.
Scientists studying cells in the lining of the intestine found two distinct categories of glucose transporters: Glucose transporters (GLUTs) and Sodium-glucose cotransporters (SGLTs). GLUTs are passive transporters where the substrate follows its concentration gradient without the use of energy. In contrast, SGLTs are secondary-active transporters that utilize the energy of one substrate going down the concentration gradient to drive the transport of the second substrate uphill, hence coupling glucose transport to the inwardly-directed sodium gradient.4,5 In humans, there are six SGLTs and 14 GLUTs in total.5,6
Three of these glucose transporters have been found to be responsible for the reabsorption of glucose at the proximal tubule: SGLT1, SGLT2 and GLUT2.7,8 With respect to location, SGLT1 is found mostly in the small intestine and kidney while SGLT2 is found almost exclusively in the kidney.9 SGLT2 is a low-capacity, high-affinity glucose transporter while SGLT1 is high-capacity, low-affinity.10,11 Familial Renal Glycosuria (FRG) is a genetic condition where glycosuria is present in the absence of hypoglycemia and renal tubular dysfunction. A molecular analysis of these patients found mutations in the SGLT2 gene, also known as SLC5A2.12
Early research suggested that SGLT2 accounts for 90% of the glucose reabsorption while SGLT1 plays a clean-up role for the remaining 10%.13 However, further research has supported a more complimentary model where SGLT1 plays a substantial role reabsorbing glucose in the S3 segment of the proximal tubule.14 SGLT2 inhibitor drugs are only capable of 50% inhibition of glucose reabsorption despite possessing high affinity for SGLT2.15,16 This suggests future drugs blocking both SGLT1 and SGLT2 have the potential to be more effective in the treatment of type 2 diabetes.
Phlorizin ultimately could not be used as an antihyperglycemic drug because of its poor oral bioavailability, short half-life and lack of SGLT1/SGLT2 selectivity.17 Drug researchers were able to overcome this by developing phlorizin derivatives that prevent the hydrolysis of molecules through chemical C-glycosylation.18 These phlorizin C-glucoside analogs are the current SGLT2 inhibitors used today by clinicians in the treatment of type 2 diabetes.
Mechanism Of Action
The flux-coupling of sodium and glucose transport in epithelia was proposed about 60 years ago by Robert Crane and eventually the identity of the first SGLT protein was determined by expression cloning in the late 1980’s.19,20 Since then 12 members of this larger SLC5 gene family (including the six SGLT members) have been cloned from humans and their physiological functions are still being determined.7,21 Although SGLT2 was cloned over 25 years ago, the pharmacology and functioning of the transporter at a molecular level has only become apparent in the last few years.7,22 SGLT2 inhibitors differ from other antihyperglycemic oral agents by offering an insulin-independent mechanism of action. They reduce blood glucose though glycosuria and natriuresis initiated by the inhibition of glucose reabsorption at the proximal tubule of the kidney.15 Pharmacodynamic studies have revealed that SGLT2 inhibitors are filtered from the blood through the glomerulus and exhibit their inhibitory effects exclusively on the extracellular side of the plasma membrane.23 Recent work determining the differences between SGLT2 and SGLT1 has identified an additional Na+ binding site in SGLT1 that is not present in SGLT2. Using a molecular modeling approach, it was proposed that the second Na+ binding site in SGLT1 prevents the current therapeutic phlorizin derivative drugs from binding to SGLT1, explaining the lower inhibitory effect on transport function.22
Current SGLT2 Inhibitors
There are four SGLT2 inhibitors approved by the Food and Drug Administration since 2013: canagliflozin, dapagliflozin, empagliflozin and ertugliflozin. (Table 1) There are also combination drugs available for patients with type 2 diabetes. They include either metformin or a dipeptidyl peptidase-4 (DPP-4) inhibitor as the second active drug. The SGLT2 inhibitors differ mostly in their binding, affinity and selectivity for SGLT transporters.24,25
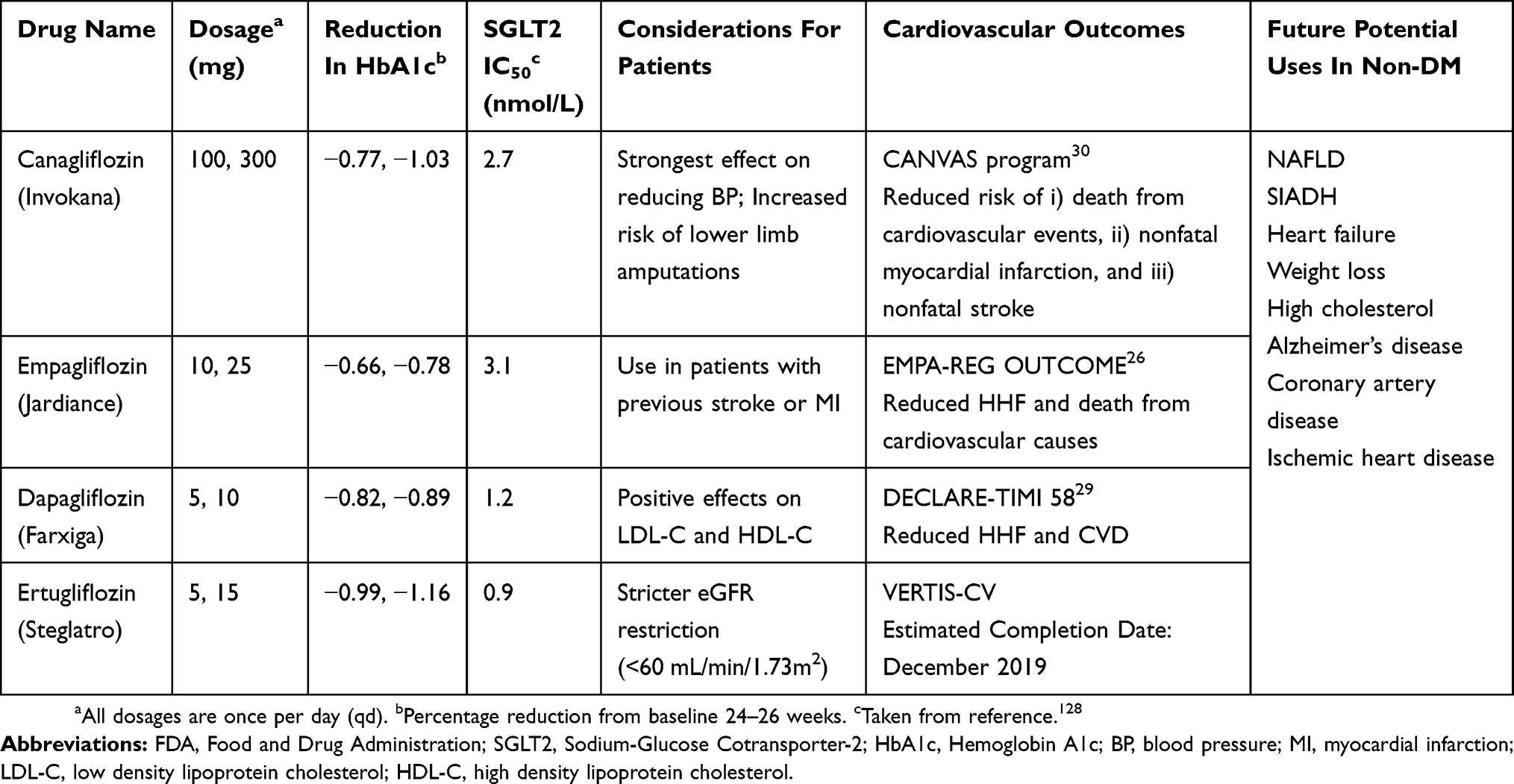 |
Table 1 FDA Approved SGLT2 Inhibitors |
In most situations, cost and insurance will dictate which SGLT2 inhibitor is selected. However, there is evidence that empagliflozin should be used in patients with previous stroke or myocardial infarction. The EMPA-REG (EMPAgliflozin Removal of Excess of Glucose) OUTCOME study found those using empagliflozin experienced a 38% relative risk reduction in cardiovascular related deaths vs placebo.26 Studies have shown that Canagliflozin has a slightly more pronounced reduction in HbA1c, but showed a higher risk of lower limb amputations.27,28
Recently, results from the largest SGLT2 inhibitor trial to date, DECLARE-TIMI 58 (Dapagliflozin Effect on CardiovascuLAR Events), have been analyzed and published.29 This was a study of 10 mg once daily dapagliflozin assessing cardiovascular outcomes and safety in patients with type 2 diabetes. This study investigated primary prevention (diabetes and multiple risk factors such as dyslipidemia, hypertension and current tobacco use) and secondary prevention (diabetes and established cardiovascular disease). Importantly this study also included a group of more than 10,000 diabetic patients without atherosclerotic cardiovascular disease. Dapagliflozin reduced the rate of cardiovascular death and hospitalization for heart failure irrespectively of underlying presence of atherosclerotic vascular disease.29 This trial also showed no evidence of an increased risk of stroke, limb amputations or fractures when compared to placebo. This study did show an increased rate of diabetic ketoacidosis and genital infection, similar to previously published studies with other SGLT2 inhibitors.26,30,31
The disease burden from diabetes extends to the heart, blood vessels and the kidney, with increased complications of heart failure, atherosclerosis and renal disease.32 Three clinical trials have published their outcomes on SGLT2 inhibitors, the EMPA-REG OUTCOME trial,26 the CANVAS Program (CANagliflozin cardioVascular Assessment Study)30 and DECLARE-TIMI 58.29 The results from a meta-analysis of these three trials indicate that SGLT2 inhibitor’s benefits include, reduced hospitalization for heart failure, renal disease and major adverse cardiovascular events.33 An important observation was that the reduction in hospitalization for heart failure and renal disease was seen in the groups with and without vascular disease. This rather importantly implies that it may be beneficial to broaden SGLT2 inhibitor use to individuals with type 2 diabetes for first line therapy, together with metformin in type 2 diabetics without a history of vascular disease, kidney disease or heart failure.32
Use In The Treatment Of Type 2 Diabetes
The American Diabetes Association (ADA) recently published their 2019 guidelines for using glucose lowering medications in the treatment of type 2 diabetes.34 Comprehensive lifestyle modifications and the use of metformin remain the first line therapy to achieve a target HbA1c of less than 7.0. If this fails, the clinician should then decide the next therapy based on if there is established atherosclerotic cardiovascular disease (ASCVD), congestive heart failure (CHF) or chronic kidney disease (CKD) present. SGLT2 inhibitors are a preferred adjunct medication in patients with these conditions, assuming there is an acceptable eGFR. The ADA guidelines also recommend SGLT2 inhibitors when there is a compelling need to promote weight loss.34
Monotherapy Vs Combination Therapy
SGLT2 inhibitors are typically reserved as a second or third-line drug in the treatment of type 2 diabetes, but they can also be used as monotherapy when metformin is contraindicated. A study assessing the efficacy of ertugliflozin as a monotherapy in type 2 diabetes reported a placebo-adjusted HbA1c mean reduction of −0.99% to −1.16% for ertugliflozin 5 mg and 15 mg respectively.35 The EMPA-REG MONO trial found empagliflozin 10 and 25 mg as a monotherapy reduced HbA1c −0.74% to −0.85% respectively on average at 24 weeks.36 A subsequent extension study found the antihyperglycemic effect was sustained past 72 weeks and empagliflozin was well tolerated by the trial participants.37
A meta-analysis of 15 randomized controlled trials compared metformin monotherapy vs the initiation of combination therapy with an SGLT2 inhibitor. This analysis reported adding an SGLT2 inhibitor resulted in an additional HbA1C reduction of −0.43%, an increase in achieving an HbA1C goal of less than 7.0 and reduction in fasting plasma glucose levels.38
A meta-analysis of 804 diabetic patients found the combination of an SGLT2 inhibitor with DPP4 inhibitors demonstrated the strongest antihyperglycemic effect.39 Another study comparing the addition of an SGLT2 inhibitor as a third drug or initiating isophane insulin in treatment resistant diabetic patients found that the long-term benefits of SGLT2 inhibitors likely offset the startup cost difference.40
Cardiovascular Effects
Congestive Heart Failure
The EMPA-REG OUTCOME trial reported that empagliflozin use resulted in a 35% risk reduction in hospitalizations for congestive heart failure and a 38% risk reduction in death from cardiovascular causes.26 This study did not differentiate between systolic and diastolic heart failure outcomes.26 It is hypothesized that the diuretic and natriuretic effects of empagliflozin are responsible for the cardiovascular risk reduction effects.41 A recent animal study found empagliflozin reduced blood pressure, increased left atrial dilatation and improved left ventricular contractility. There was also a statistically significant improvement in cardiac fibrosis and modulation of the genes involved in fatty acid metabolism.42 The RECEDE-CHF (REnal and Cardiovascular Effects of SGLT2 inhibition in combination with loop Diuretics in diabetic patients with Chronic Heart Failure) trial is currently investigating the diuretic and natriuretic effect of Empagliflozin 25mg when combined with furosemide.43
In a large observational analysis of cardiovascular outcomes in over 300,000 patients (CVD-REAL) newly treated with SGLT2 inhibitors, a significant cardiovascular benefit was observed in glucose lowering drugs in diabetic patients.44 This benefit in lowering the risk of cardiovascular death and heart failure was also observed in patients without previous cardiovascular disease. In the EMPA-REG trial, treatment with empagliflozin in a population of diabetic patients with cardiovascular disease showed reductions in major adverse cardiovascular events, including death and hospitalization for heart failure.26 In the DECLARE-TIME 58 trial,45 dapagliflozin treatment showed large reductions in cardiovascular deaths and hospitalization for heart failure, irrespectively of the presence of baseline atherosclerotic cardiovascular disease. However, the reductions in cardiovascular death were not explained by decreases in myocardial infarctions, interestingly the SGLT2 inhibitor appeared to prevent cardiovascular death primarily by reducing death from heart failure. Dapagliflozin also led to a greater reduction in cardiovascular deaths in heart failure patients with a reduced left ejection fraction compared to heart failure patients without a reduced ejection fraction.45
The mechanisms by which SGLT2 inhibitors could be beneficial in heart failure with reduced ejection fraction include a reduction in the strain and stress on the heart walls and by protective metabolic and anti-inflammatory effects.46–48 The most logical mechanism is that SGLT2 inhibitors increase glycosuria, natriuresis and osmotic diuresis, which will reduce effective circulating volume and reduce preload. The decrease in blood pressure will in parallel reduce cardiac afterload.45,47,48
Blood Pressure
When compared to placebo, multiple studies have shown that SGLT2 inhibitors are associated with both a systolic and diastolic blood pressure reduction. In the EMPA-REG BP trial, researchers investigated the effect of empagliflozin on patients with type 2 diabetes and hypertension. Participants in the study received one of the three possible interventions: empagliflozin 10 mg, 25 mg, or placebo. At the end of the 12 weeks, those who received 10 mg of empagliflozin saw a −3.44 and −1.36 mm Hg reduction in systolic and diastolic blood pressure respectively compared to placebo. For 25 mg of empagliflozin vs placebo, the reduction was −4.16 and −1.72 mm Hg, respectively.49
A meta-analysis done by Vasilakou et al found a mean reduction of −3.77 mm Hg and −1.75 mm Hg in systolic and diastolic blood pressure respectively compared to placebo. Canagliflozin was found to have the strongest overall effect on blood pressure out of the SGLT2 inhibitors.50
Cardiovascular Fitness
Increasing physical activity is one of the primary lifestyle changes recommended for the treatment of type 2 diabetes. Patients with diabetes show decreased cardiovascular fitness, skeletal muscle mass and overall physical activity levels.51,52 Multiple studies have demonstrated that glitazones and glucagon-like peptide-1 (GLP-1) agonists have positive effects on cardiovascular fitness.53–55 Two pilot studies have been implemented to investigate if empagliflozin improved cardiovascular fitness levels in patients with type 2 diabetes with congestive heart failure. In patients who were taking loop diuretics, both studies found a significant improvement in VO2peak. However, those not on loop diuretics did not experience the same benefit. It is hypothesized that the synergistic effect of the two medications is due to increased sodium delivery to the distal tubules, which amplifies the natriuretic effect of diuretics.56,57
Novel Uses
Non-Alcoholic Fatty Liver Disease
Non-alcoholic fatty liver disease (NAFLD) is defined as fat accumulation in the liver associated with insulin resistance and the presence of steatosis in >5% of hepatocytes on histological analysis. This includes hepatic steatosis caused by non-alcoholic steatohepatitis (NASH), cirrhosis or simple steatosis. NAFLD does not include disease due to excessive alcohol consumption, hepatitis, drugs or other rare conditions.58 Type 2 diabetes and insulin resistance are strongly associated with NAFLD. It is estimated that the prevalence of NAFLD in type 2 diabetes is 69–87% depending on the imaging modality used vs 30% in the general population.59 Patients with NAFLD experience an increased risk of cirrhosis and hepatocellular carcinoma.60
A reduction in serum alanine aminotransferase (ALT) of 30% or greater from baseline was found to be predictive for improvement in liver fibrosis progression in NASH patients.61 A pilot study by Seko et al investigated the use of 100 mg canagliflozin over 12 weeks in type 2 diabetic patients with NASH of varying stages. They found that canagliflozin reduced ALT by 23.9 U/L on average and the greatest benefit was for those in early stage NASH compared to later stage fibrosis. The authors also encouraged a larger, more robust study to confirm their results as they had a small sample size.62 Animal studies have revealed insight into the mechanism behind the protective effects SGLT2 inhibitors have on NASH. Canagliflozin was shown to upregulate zinc-α2-glycoprotein (ZAG) levels, reduce hepatic inflammatory cytokines and enhance Bcl-2 expression. It also reduced oxidative stress in the liver and boost antioxidant capacity.63
Weight Loss/Obesity
SGLT2 inhibitors cause weight loss in a dose dependent manner. Meta analyses estimate the weight loss effect to be approximately 1.5–2.5 kg.28 However, these weight loss effects are curbed by an increase in energy intake.64 Another study reported 150 mg of licogliflozin, a Japanese dual SGLT1/SGLT2 inhibitor, significantly reduced the body weight of obese individuals without diabetes by 5.7% vs placebo. A positive effect on incretin hormones was also observed.65 There are multiple clinical trials currently investigating the utility of SGLT2 inhibitors on obese individuals without diabetes. While likely not effective enough as a monotherapy for obesity, SGLT2 inhibitors could potentially be effective in weight loss when combined with other drugs that reduce the consumption of food.
Early Stage Lung Adenocarcinoma
A recent study has implicated SGLT2 expression in early lung tumor development in both premalignant lung lesions and early stage adenocarcinoma. Scafoglio et al found that selectively targeting SGLT2 with canagliflozin significantly prolonged survival rates in mice.66 However, the effect was not permanent as tumor growth eventually escaped SGLT2 inhibition, likely due to upregulation of SGLT2. The researchers were also able to modify proton emission tomography (PET) scans to track activity of SGLT2, which has potential to be useful in the evaluation of response of early stage lung lesions to SGLT2 inhibitor treatment. Further studies testing the use of SGLT2 inhibitors in early stage lung adenocarcinoma need to be done before the clinical significance can be determined.66
Contraindications
Clinicians should assess renal function before the initiation of SGLT2 inhibitors and periodically after prescribing them. Empagliflozin, dapagliflozin and canagliflozin should not be initiated in patients with an eGFR persistently less than 45 mL/min/1.73m2, and those on treatment should be discontinued if eGFR drops below this threshold. Ertugliflozin should not be initiated or continued in patients with an eGFR consistently less than 60 mL/min/1.73m2. The entire class of SGLT2 inhibitors are absolutely contraindicated in patients with an eGFR less than 30 mL/min/1.73m2.67–70
Side Effects
Genital Tract Infections
There is an increased risk of genital tract infections of mycotic origin in those with type 2 diabetes. Glycosuria, impaired immunity, and the hyperglycemia combined with a warm, moist environment all are contributing factors.71,72 Besides genital tract infections, patients with type 2 diabetes are at a two-fold or worse risk of osteomyelitis, skin and soft tissue infections, sepsis and post-operative infections.73,74
The negative effect SGLT2 inhibitors have on genital tract infection incidence has been studied extensively. The FDA also recently issued a safety announcement regarding the use of SGLT2 inhibitors after 12 cases of Fournier’s gangrene were reported.75 One meta-analysis of 12 randomized, placebo-controlled Phase 2b/3 trials found dapagliflozin significantly increased the risk of vulvovaginitis and balanitis infections.76 Another double-blind, placebo-controlled study reported a higher incidence of genital infections among those using dapagliflozin.77 The infections in these studies were mostly mild to moderate, responsive to standard treatments and generally did not require discontinuation of the SGLT2 inhibitor. Compiled data on the use of canagliflozin and genital tract infections indicate a high incidence of infection at the initiation of a SGLT2 inhibitor (first 24–26 weeks), but the frequency of infection significantly decreased over time.78
Amputations
The CANVAS trial reported canagliflozin use increased the risk of lower limb amputation by 97% compared to placebo.30 The mechanism is not well understood, but it is hypothesized that volume depletion induced by SGLT2 inhibitors contribute to circulatory failure in the distal arterial beds.79 The amputations were primarily located at the level of the toe or metatarsal and the risk vs placebo remained consistent among those with peripheral vascular disease and a history of previous amputations.30 The increased risk of amputation with canagliflozin was similar when calculated using both the difference in restricted mean survival time (RMST) and hazard risk (HR).80 Empagliflozin has not been associated with a risk of lower limb amputation.81
A retrospective cohort study of 953,906 diabetic patients found an association between the initiation of SGLT2 inhibitors with an increased risk of amputation when compared to metformin, sulfonylureas and thiazolidinediones. However, this difference was not significant when new use of SGLT2 inhibitors were compared to DPP-4 inhibitors or GLP-1 agonists.82
Bone Fractures
Type 2 diabetic patients experience paradoxical bone effects as a result of their disease. Multiple studies and meta-analyses support the conclusion that patients with type 2 diabetes have an increased bone mineral density on DEXA scans. However, they are much more susceptible to hip fractures.83–85
The consequences SGLT2 inhibitors have on this paradoxical effect of diabetes is unclear and controversial. There are animal studies that demonstrate canagliflozin adversely affects bone microarchitecture, bone strength and bone mineral density.86,87 Likewise, one clinical trial with canagliflozin observed a reduction in hip bone mineral density, but not at other bone locations on DEXA scan. There is evidence that the reduction in bone mineral density may be related to weight loss and decrease in estradiol.88 Kohan et al described fractures with the administration of dapagliflozin, but the location of the fractures was more indicative of falls rather than bone density problems.89 In the Canagliflozin Cardiovascular Assessment Study (CANVAS), the incidence of fracture vs placebo was statistically significantly higher (4.0% vs 2.6%). However, further analysis of the data in CANVAS found the statistical significance no longer existed after excluding the fractures not associated with osteoporosis or skeletal fragility.90 In contrast, there are multiple meta analyses that conclude SGLT2 inhibitors are not associated with an increased risk of fractures. These analyses include 58 peer-reviewed studies and 38,670 patients in total.91
Electrolyte Imbalance
Multiple meta-analyses have found that SGLT2 inhibitors cause a small percentage change in serum electrolyte levels. Canagliflozin was associated with a statistically significant increase in serum magnesium levels, which operated in a dose-dependent manner. Empagliflozin and dapagliflozin were also found to have a statistically significant increase in magnesium levels. However, dapagliflozin only increased serum magnesium levels at the 10 mg dose. With respect to sodium levels, there was a difference noted between empagliflozin and canagliflozin. Empagliflozin 25 mg increased serum sodium and canagliflozin 300 mg decreased sodium levels. Serum phosphate levels are slightly increased using SGLT2 inhibitors. The analyses found that potassium and calcium levels were unaffected by SGLT2 inhibitors.92–94
It is possible that the increase in magnesium and phosphate levels is partially responsible for the cardiovascular event reduction found in the EMPA-REG OUTCOME trial through the prevention of arrythmias.26 However, the increase in phosphate might also be responsible for the negative bone density and fracture side effects noted with SGLT2 inhibitors in the CANVAS trial. The increased phosphate causes an increase in parathyroid hormone levels, which accelerates bone resorption. Rising fibroblast growth factor 23 (FGF-23) levels also are associated with the increased phosphate levels, leading to a decrease in serum vitamin D concentration.95
Diabetic Ketoacidosis
Diabetic ketoacidosis (DKA) is strongly associated with type 1 diabetes but euglycemic DKA is also seen in type 2 diabetics with critical illness or who are ketosis-prone. There are three potential mechanisms for DKA in type 2 diabetics: insulinopenia, creation of counterregulatory stress hormones and free fatty acid elevations. Insulinopenia is the mechanism with the most support in the literature.96 SGLT2 inhibitors lower the insulin to glucagon ratio and enhance lipolysis, which stimulates the production of ketones in the liver.97 A recent study of diabetic rats treated with SGLT2 inhibitors suggested insulinopenia and dehydration are the key factors in the development of DKA.98 Euglycemic DKA has been reported in the literature in patients with type 2 diabetes on SGLT2 inhibitors.99,100 However, multiple meta-analyses have found no increased risk of DKA for patients taking SGLT2 inhibitors vs placebo.101,102
Lipids
SGLT2 inhibitors may cause a slight increase in both HDL and LDL cholesterols levels in a dose dependent manner. Many studies, including the EMPA-REG OUTCOME trial, have associated empagliflozin with an increase in both HDL-C and LDL-C when compared to placebo.26,36,103,104 A meta-analysis of SGLT2 inhibitor trials reported an increase in both HDL-C and LDL-C and a decrease in triglycerides versus placebo.105 Studies investigating canagliflozin, including the CANVAS trial, have also reported similar increases in HDL and LDL cholesterol.30,78 Another study found dapagliflozin increased LDL and HDL cholesterol. However, there was a decrease in atherogenic small density LDL-C and increase in the less atherogenic large buoyant LDL-C.106
The mechanism by which SGLT2 inhibitors alter lipids is not entirely understood, but it is likely a combination of hemoconcentration and a decrease in LDL receptor activity in the liver. The reduction in hepatic LDL receptor expression is likely due to the increase in HMG-CoA reductase activity.107,108
Uric Acid/Chronic Kidney Disease
Chronically high serum uric acid levels are associated with the progression of chronic kidney disease (CKD). Zoppini et al observed that the incidence of CKD more than doubled in the presence of elevated serum uric acid.109 Another study found a similar associated risk between serum uric acid level and CKD, but also found that higher levels encouraged more rapid CKD progression.110 It is thought that elevated serum uric acid levels negatively affect the kidney by increasing inflammation-mediated damage to the glomerular and tubule-interstitial structure.111,112
SGLT2 inhibitors are associated with a substantial reduction of serum uric acid levels. As an adjunct antihyperglycemic medication, they lower serum uric acid levels by approximately 0.60 to 0.75 mg/dL. They could also be effective as a second medication to use in addition to xanthine oxidase inhibitors in the treatment of gout.113,114 A meta-analysis investigating the effect of SGLT2 inhibitors on uric acid found the entire class of drugs significantly lowered serum uric acid levels. Empagliflozin had the strongest effect, and dapagliflozin was found to decrease serum uric acid in a dose-dependent manner. The reduction was most pronounced in patients with early diabetes, and the effect was diminished in those with chronic kidney disease.115 The use of insulin also abates the drugs’ effect, likely due to the hyperuricemic effects of increased insulin levels.116 Chino et al found that the SGLT2 induced glycosuria was accompanied by an increase in the urinary excretion rate of uric acid, which is responsible for the serum uric acid lowering effect.117
Renal Effects
Evidence from large trials primarily investigating cardiovascular outcomes of SGLT2 inhibitors but with renal outcomes as secondary aims are amassing and suggesting that SGLT2 inhibitors are offering renal protective effects, not directly associated with their plasma glucose lowering properties attributed to the inhibition of the SGLT2 transporter.26,29,30 The EMPA-REG OUTCOME trial included subjects with modestly reduced kidney function. In this trial a reduction in albuminuria progression and a decrease in the percentage of patients with acute kidney injury were observed in the empagliflozin treatment groups.26 After an initial decline of 3ml/min, the empagliflozin group showed a marked slower decline in eGFR compared to the placebo group, implying a protective effect on the kidney and preventing the decline of kidney function.118 In the CANVAS Program, in addition to a decrease in the progression of albuminuria, the composite outcome of a 40% reduction in eGFR, need for renal replacement therapy or death from renal causes was also reduced in the canagliflozin group.29 The DECLARE-TIMI 58 trial showed a 46% reduction in a sustained decline of eGFR in the dapagliflozin group. The population in the DECLARE-TIMI 58 trial had better initial renal function than the EMPA-REG and CANVAS trials and it took longer (year 3 and 4 of trial) for protective benefits in eGFR to be observed in the active dapagliflozin treatment group compared to the placebo group.119
The CREDENCE (Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation) trial was specifically designed to assess the effects of the SGLT2 inhibitor canagliflozin on renal outcomes in patients with type 2 diabetes and albuminuric chronic kidney disease120 The subjects in the CREDENCE study had a eGFR of 30 to <90 mL/min and albuminuria. The relative risk of the renal-specific composite of end-stage kidney disease (dialysis, transplantation, or a sustained eGFR or < 15 mL/min), doubling of creatinine levels or death from renal causes was lowered by 34% in the canagliflozin group. Taken together, the evidence is clear that SGLT2 inhibitors offer renal protection and prevent the decline in renal function seen over time in type 2 diabetic patients.121
The current school of thought is that the inhibition of SGLT2 corrects the increased intraglomerular pressure observed in type II diabetics. The SGLT2 mediated inhibition of sodium transport in the proximal tubule results in increased delivery of sodium to the distal nephron. This is sensed as increased tubular perfusion and triggers tubuloglomerular feedback which will cause an increase in vasoconstriction of the afferent arteriole and a decrease in glomerular perfusion. This lowering of the intraglomerular pressure will preserve renal function in renal hypertension caused by type II diabetes.121
Risk Of Cancer
The association between SGLT2 inhibitors and cancer has been extensively studied and remains controversial today. When Dapagliflozin originally applied for FDA approval, it was denied in 2011 due to concerns about the increased risk of bladder and breast cancer. Pooled studies on dapagliflozin showed 9 out of 5478 patients on dapagliflozin vs 1 out of 3156 control patients developed both bladder and breast cancer.122 An early meta-analysis assessing the safety of SGLT2 inhibitors also found an imbalance in bladder and breast cancer incidence when compared to control subjects.50 In order to receive FDA approval, the recently released DECLARE-TIMI 58 trial, which evaluated over 17,000 patients, was created to assess the long-term effects of dapagliflozin. They found that dapagliflozin was associated with a lower rate of bladder cancer than placebo and no difference in breast cancer vs placebo.29
A recent meta-analysis by Tang et al found a statistically significant increased risk of bladder cancer, specifically in empagliflozin (OR 3.87 [95% CI 1.48, 10.09]). Canagliflozin was associated with a statistically significant reduction in the incidence of gastrointestinal cancer.123 However, there have been challenges to the data involved in this analysis. Four events of bladder cancer were not included in the analysis, and a patient-level assessment for causality was also not performed. With the corrected data, the association between bladder cancer and SGLT2 inhibitors became non-statistically significant.124 Another recent meta-analysis of 27 clinical trials found no statistically significant increased risk of any type of cancer with SGLT2 inhibitors.125
Future SGLT2 Inhibitors
Sotagliflozin (LX4211) is unique in that it is a dual inhibitor of SGLT1/SGLT2. Compared to canagliflozin and dapagliflozin, sotagliflozin has similar inhibitory effect on SGLT2, but is about 20 and 40 fold more effective at inhibiting SGLT1 than canagliflozin and dapagliflozin respectively.126–128 In patients with type 2 diabetes treated with metformin, adding sotagliflozin had positive effects on HbA1c, systolic blood pressure, weight loss and post-prandial glucose measurements. The SGLT1 inhibitory effects were determined to be from the intestine as those with renal impairment still saw a significant post-prandial glucose decrease.129,130 The drug is also being investigated as the first oral medication for the treatment of type 1 diabetes. The inTandem trial found that type 1 diabetes patients receiving sotagliflozin were almost twice as likely to have an HbA1c of less than 7.0 without an increased risk of severe hypoglycemia. However, those who received the sotagliflozin were significantly more likely to experience diabetic ketoacidosis (3% vs 0.6%).131
Conclusion
SGLT2 inhibitors are a very useful tool at the disposal of clinicians treating patients with type 2 diabetes, especially in those with underlying cardiovascular or fatty liver disease. Their antihyperglycemic effect is not typically strong enough to be used as monotherapy, but their insulin-independent mechanism of action makes them a powerful adjunct therapy when metformin alone is insufficient. However, the unique mechanism adds further side effects and eGFR monitoring clinicians must be aware of if they prescribe this class of medication. Educating patients on the possibility of genital tract infections is important as cases are very responsive to treatment. Results from recent large studies and meta-analyses indicate that previous associations of SGLT2 inhibitors with some adverse effects such as lower limb amputation are now being called into question. Larger studies and meta-analyses will need to provide additional clarity on the potential risk of adverse effects including lower limb amputation, fracture, cancer and DKA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chasis H, Jolliffe N, Smith HW. The action of phlorizin on the excretion of glucose, xylose, sucrose, creatinine and urea by man. J Clin Invest. 1933;12(6):1083–1090. doi:10.1172/jci100559
2. Himsworth HP. The relation of glycosuria to glycaemia and the determination of the renal threshold for glucose. Biochem J. 1931;25(4):1128–1146. doi:10.1042/bj0251128
3. Wright EM, Hirayama BA, Loo DF. Active sugar transport in health and disease. J Intern Med. 2007;261(1):32–43. doi:10.1111/j.1365-2796.2006.01746.x
4. Kimmich GA, Randles J. Sodium-sugar coupling stoichiometry in chick intestinal cells. Am J Physiol Cell Physiol. 1984;247:1. doi:10.1152/ajpcell.1984.247.1.c74
5. Mueckler M, Thorens B. The SLC2 (GLUT) family of membrane transporters. Mol Aspects Med. 2013;34(2–3):121–138. doi:10.1016/j.mam.2012.07.001
6. Gallo LA, Wright EM, Vallon V. Probing SGLT2 as a therapeutic target for diabetes: basic physiology and consequences. Diabetes Vasc Dis Res. 2015;12(2):78–89. doi:10.1177/1479164114561992
7. Wright EM, Loo DDF, Hirayama BA. Biology of human sodium glucose transporters. Physiol Rev. 2011;91(2):733–794. doi:10.1152/physrev.00055.2009
8. Wright EM, Turk E. The sodium/glucose cotransport family SLC5. Pflugers Archiv Eur J Physiol. 2004;447(5):510–518. doi:10.1007/s00424-003-1063-6
9. Nishimura M, Naito S. Tissue-specific mRNA Expression Profiles of Human ATP-binding Cassette and Solute Carrier Transporter Superfamilies. Drug Metab Pharmacokinet. 2005;20(6):452–477. doi:10.2133/dmpk.20.452
10. Quamme GA, Freeman HJ. Evidence for a high-affinity sodium-dependent D-glucose transport system in the kidney. Am J Physiol Renal Physiol. 1987;253:1. doi:10.1152/ajprenal.1987.253.1.f151
11. Turner RJ, Moran A. Heterogeneity of sodium-dependent D-glucose transport sites along the proximal tubule: evidence from vesicle studies. Am J Physiol Renal Physiol. 1982;242:4. doi:10.1152/ajprenal.1982.242.4.f406
12. Santer R. Molecular analysis of the SGLT2 gene in patients with renal glucosuria. J Am Soc Nephrol. 2003;14(11):2873–2882. doi:10.1097/01.asn.0000092790.89332.d2
13. Vallon V, Platt KA, Cunard R, et al. SGLT2 mediates glucose reabsorption in the early proximal tubule. J Am Soc Nephrol. 2010;22(1):104–112. doi:10.1681/asn.2010030246
14. Hummel CS, Lu C, Loo DDF, et al. Glucose transport by human renal Na/d-glucose cotransporters SGLT1 and SGLT2. Am J Physiol Cell Physiol. 2011;300:1. doi:10.1152/ajpcell.00388.2010
15. Komoroski B, Vachharajani N, Boulton D, et al. Dapagliflozin, a novel SGLT2 inhibitor, induces dose-dependent glucosuria in healthy subjects. Clin Pharmacol Ther. 2009;85(5):520–526. doi:10.1038/clpt.2008.251
16. Ghezzi C, Loo DDF, Wright EM. Physiology of renal glucose handling via SGLT1, SGLT2 and GLUT2. Diabetologia. 2018;61(10):2087–2097. doi:10.1007/s00125-018-4656-5
17. Oku A, Ueta K, Arakawa K, et al. T-1095, an inhibitor of renal Na -glucose cotransporters, may provide a novel approach to treating diabetes. Diabetes. 1999;48(9):1794–1800. doi:10.2337/diabetes.48.9.1794
18. Link J, Sorensen BK. A method for preparing C-glycosides related to phlorizin. Tetrahedron Lett. 2000;41(48):9213–9217. doi:10.1016/s0040-4039(00)01709-3
19. Crane RK, Miller D, Bihler I. The restrictions on possible mechanisms of intestinal active transport of sugars. In: Kleinzeller A, Kotyk A, editors. Membr Transport Metab. 1961:439–449.
20. Hediger MA, Coady MJ, Ikeda TS, Wright EM. Expression cloning and cDNA sequencing of the Na/glucose co-transporter. Nature. 1987;330(6146):379–381. doi:10.1038/330379a0
21. Wright EM, Ghezzi C, Loo DDF. Novel and Unexpected Functions of SGLTs. Physiology. 2017;32(6):435–443. doi:10.1152/physiol.00021.2017
22. Bisignano P, Ghezzi C, Jo H, et al. Inhibitor binding mode and allosteric regulation of Na -glucose symporters. Nat Commun. 2018;9:1. doi:10.1038/s41467-018-07700-1
23. Ghezzi C, Hirayama BA, Gorraitz E, et al. SGLT2 inhibitors act from the extracellular surface of the cell membrane. Phys Rep. 2014;2:6. doi:10.14814/phy2.12058
24. Grempler R, Thomas L, Eckhardt M, et al. Empagliflozin, a novel selective sodium glucose cotransporter-2 (SGLT-2) inhibitor: characterisation and comparison with other SGLT-2 inhibitors. Diabetes Obesity Metab. 2011;14(1):83–90. doi:10.1111/j.1463-1326.2011.01517.x
25. Isaji M. SGLT2 inhibitors: molecular design and potential differences in effect. Kidney Int. 2011;79 (Suppl 120):S14–S19. doi:10.1038/ki.2010.511
26. Zinman B, Wanner C, Lachin JM, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi:10.1056/nejmoa1504720
27. Perkovic V, Zeeuw DD, Mahaffey KW, et al. Canagliflozin and renal outcomes in type 2 diabetes: results from the CANVAS program randomised clinical trials. Lancet Diabetes Endocrinol. 2018;6(9):691–704. doi:10.1016/s2213-8587(18)30141-4
28. Zaccardi F, Webb DR, Htike ZZ, et al. Efficacy and safety of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes mellitus: systematic review and network meta-analysis. Diabetes Obesity Metab. 2016;18(8):783–794. doi:10.1111/dom.12670
29. Wiviott SD, Raz I, Bonaca MP, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347–357. doi:10.1056/nejmoa1812389
30. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644–657. doi:10.1056/nejmoa1611925
31. Khouri C, Cracowski J-L, Roustit M. SGLT-2 inhibitors and the risk of lower-limb amputation: is this a class effect? Diabetes Obesity Metab. 2018;20(6):1531–1534. doi:10.1111/dom.13255
32. Verma S, Jüni P, Mazer CD. Pump, pipes, and filter: do SGLT2 inhibitors cover it all? Lancet. 2019;393(10166):3–5. doi:10.1016/s0140-6736(18)32824-1
33. Zelniker TA, Wiviott SD, Raz I, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31–39. doi:10.1016/s0140-6736(18)32590-x
34. Standards of Medical Care in Diabetes—2019. Abridged for Primary Care Providers. Clin Diabetes. 2018;37(1):11–34. doi:10.2337/cd18-0105
35. Terra SG, Focht K, Davies M, et al. Phase III, efficacy and safety study of ertugliflozin monotherapy in people with type 2 diabetes mellitus inadequately controlled with diet and exercise alone. Diabetes Obesity Metab. 2017;19(5):721–728. doi:10.1111/dom.12888
36. Roden M, Weng J, Eilbracht J, et al. Empagliflozin monotherapy with sitagliptin as an active comparator in patients with type 2 diabetes: a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Diabetes Endocrinol. 2013;1(3):208–219. doi:10.1016/s2213-8587(13)70084-6
37. Roden M, Merker L, Christiansen AV, et al. Safety, tolerability and effects on cardiometabolic risk factors of empagliflozin monotherapy in drug-naïve patients with type 2 diabetes: a double-blind extension of a phase III randomized controlled trial. Cardiovasc Diabetol. 2015;14:1. doi:10.1186/s12933-015-0314-0
38. Phung OJ, Sobieraj DM, Engel SS, et al. Early combination therapy for the treatment of type 2 diabetes mellitus: systematic review and meta-analysis. Diabetes Obesity Metab. 2013;16(5):410–417. doi:10.1111/dom.12233
39. Milder T, Stocker S, Shaheed CA, et al. Combination therapy with an SGLT2 inhibitor as initial treatment for type 2 diabetes: a systematic review and meta-analysis. J Clin Med. 2019;8(1):45. doi:10.3390/jcm8010045
40. Pawaskar M, Bilir SP, Kowal S, et al. Cost-effectiveness of intensification with sodium-glucose co-transporter-2 inhibitors in patients with type 2 diabetes on metformin and sitagliptin vs direct intensification with insulin in the United Kingdom. Diabetes Obesity Metab. 2019;21(4):1010–1017. doi:10.1111/dom.13618
41. Mcmurray J. EMPA-REG – the “diuretic hypothesis.”. J Diabetes Complications. 2016;30(1):3–4. doi:10.1016/j.jdiacomp.2015.10.012
42. Lee H-C, Shiou Y-L, Jhuo S-J, et al. The sodium–glucose co-transporter 2 inhibitor empagliflozin attenuates cardiac fibrosis and improves ventricular hemodynamics in hypertensive heart failure rats. Cardiovasc Diabetol. 2019;18:1. doi:10.1186/s12933-019-0849-6
43. Mordi NA, Mordi IR, Singh JS, et al. Renal and cardiovascular effects of sodium–glucose cotransporter 2 (SGLT2) inhibition in combination with loop Diuretics in diabetic patients with Chronic Heart Failure (RECEDE-CHF): protocol for a randomised controlled double-blind cross-over trial. BMJ Open. 2017;7:10. doi:10.1136/bmjopen-2017-018097
44. Cavender MA, Norhammar A, Birkeland KI, et al. SGLT-2 inhibitors and cardiovascular risk. J Am Coll Cardiol. 2018;71(22):2497–2506. doi:10.1016/j.jacc.2018.01.085
45. Kato ET, Silverman MG, Mosenzon O, et al. Effect of dapagliflozin on heart failure and mortality in type 2 diabetes mellitus. Circulation. 2019;139(22):2528–2536. doi:10.1161/circulationaha.119.040130
46. Verma S, Mcmurray JJV, Cherney DZI. The metabolodiuretic promise of sodium-dependent glucose cotransporter 2 inhibition. JAMA Cardiol. 2017;2(9):939. doi:10.1001/jamacardio.2017.1891
47. Verma S, Mcmurray JJV. SGLT2 inhibitors and mechanisms of cardiovascular benefit: a state-of-the-art review. Diabetologia. 2018;61(10):2108–2117. doi:10.1007/s00125-018-4670-7
48. Verma S, Mcmurray JJ. The serendipitous story of SGLT2 inhibitors in heart failure. Circulation. 2019;139(22):2537–2541. doi:10.1161/circulationaha.119.040514
49. Tikkanen I, Narko K, Zeller C, et al. Empagliflozin reduces blood pressure in patients with type 2 diabetes and hypertension. Diabetes Care. 2015;38(3):420–428. doi:10.2337/dc14-1096
50. Vasilakou D, Karagiannis T, Athanasiadou E, et al. Sodium–glucose cotransporter 2 inhibitors for type 2 diabetes. Ann Intern Med. 2013;159(4):262. doi:10.7326/0003-4819-159-4-201308200-00007
51. Park SW, Goodpaster BH, Lee JS, et al. Excessive loss of skeletal muscle mass in older adults with type 2 diabetes. Diabetes Care. 2009;32(11):1993–1997. doi:10.2337/dc09-0264
52. Özdirenç M, Biberoğlu S, Özcan A. Evaluation of physical fitness in patients with Type 2 diabetes mellitus. Diabetes Res Clin Pract. 2003;60(3):171–176. doi:10.1016/s0168-8227(03)00064-0
53. Regensteiner JG, Bauer TA, Reusch JE. Rosiglitazone improves exercise capacity in individuals with type 2 diabetes. Diabetes Care. 2005;28(12):2877–2883. doi:10.2337/diacare.28.12.2877
54. Kadoglou NPE, Iliadis F, Angelopoulou N, et al. Beneficial effects of rosiglitazone on novel cardiovascular risk factors in patients with type 2 diabetes mellitus. Diabetic Med. 2008;25(3):333–340. doi:10.1111/j.1464-5491.2007.02375.x
55. Lepore JJ, Olson E, Demopoulos L, et al. Effects of the novel long-acting GLP-1 agonist, albiglutide, on cardiac function, cardiac metabolism, and exercise capacity in patients with chronic heart failure and reduced ejection fraction. JACC. 2016;4(7):559–566. doi:10.1016/j.jchf.2016.01.008
56. Núñez J, Palau P, Domínguez E, et al. Early effects of empagliflozin on exercise tolerance in patients with heart failure: a pilot study. Clin Cardiol. 2018;41(4):476–480. doi:10.1002/clc.22899
57. Carbone S, Canada JM, Billingsley HE, et al. Effects of empagliflozin on cardiorespiratory fitness and significant interaction of loop diuretics. Diabetes Obesity Metab. 2018;20(8):2014–2018. doi:10.1111/dom.13309
58. EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64(6):1388–1402. doi:10.1016/j.jhep.2015.11.004
59. Saponaro C, Gaggini M, Gastaldelli A. Nonalcoholic fatty liver disease and type 2 diabetes: common pathophysiologic mechanisms. Curr Diab Rep. 2015;15:6. doi:10.1007/s11892-015-0607-4
60. Younossi ZM, Koenig AB, Abdelatif D, et al. Global epidemiology of nonalcoholic fatty liver disease-meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology. 2016;64:73–84. doi:10.1002/hep.28431
61. Seko Y, Sumida Y, Tanaka S, et al. Serum alanine aminotransferase predicts the histological course of non-alcoholic steatohepatitis in Japanese patients. Hepatol Res. 2014;45:10. doi:10.1111/hepr.12456
62. Seko Y, Nishikawa T, Umemura A, et al. Efficacy and safety of canagliflozin in type 2 diabetes mellitus patients with biopsy-proven nonalcoholic steatohepatitis classified as stage 1–3 fibrosis. Diabetes Metab Syndrome Obesity. 2018;(2018(11):835–843. doi:10.2147/dmso.s184767
63. Kabil SL, Mahmoud NM. Canagliflozin protects against non-alcoholic steatohepatitis in type-2 diabetic rats through zinc alpha-2 glycoprotein up-regulation. Eur J Pharmacol. 2018;828:135–145. doi:10.1016/j.ejphar.2018.03.043
64. Ferrannini G, Hach T, Crowe S, Sanghvi A, Hall KD, Ferrannini E. Energy balance after sodium–glucose cotransporter 2 inhibition. Diabetes Care. 2015;38(9):1730–1735. doi:10.2337/dc15-0355
65. He YL, Haynes W, Meyers CD, et al. The effects of licogliflozin, a dual SGLT1/2 inhibitor, on body weight in obese patients with or without diabetes. Diabetes Obesity Metab. 2019. doi:10.1111/dom.13654
66. Scafoglio CR, Villegas B, Abdelhady G, et al. Sodium-glucose transporter 2 is a diagnostic and therapeutic target for early-stage lung adenocarcinoma. Sci Transl Med. 2018;10:467. doi:10.1126/scitranslmed.aat5933
67. Jardiance (empagliflozin tablets, for oral use) [package Insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc.; 2018.
68. Invokana (canagliflozin tablets, for oral use) [package Insert]. Titusvlle, NJ: Janssen Pharmaceuticals, Inc.; 2018.
69. Farixga (dapagliflozin tablets, for oral use) [package Insert]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2019.
70. Steglatro (ertugliflozin tablets, for oral use) [package Insert]. Whitehouse Station, NJ: Merck Sharp & Dohme Corp; 2018.
71. Dryden M, Baguneid M, Eckmann C, et al. Pathophysiology and burden of infection in patients with diabetes mellitus and peripheral vascular disease: focus on skin and soft-tissue infections. Clin Microbiol Infect. 2015;21. doi:10.1016/j.cmi.2015.03.024
72. Geerlings SE. Urinary tract infections in patients with diabetes mellitus: epidemiology, pathogenesis and treatment. Int J Antimicrob Agents. 2008;31:54–57. doi:10.1016/j.ijantimicag.2007.07.042
73. Shah BR, Hux JE. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care. 2003;26(2):510–513. doi:10.2337/diacare.26.2.510
74. Benfield T, Jensen JS, Nordestgaard BG. Influence of diabetes and hyperglycaemia on infectious disease hospitalisation and outcome. Diabetologia. 2006;50(3):549–554. doi:10.1007/s00125-006-0570-3
75. Scheen AJ. An update on the safety of SGLT2 inhibitors. Expert Opin Drug Saf. 2019. doi:10.1080/14740338.2019.1602116
76. Johnsson KM, Ptaszynska A, Schmitz B, et al. Vulvovaginitis and balanitis in patients with diabetes treated with dapagliflozin. J Diabetes Complications. 2013;27(5):479–484. doi:10.1016/j.jdiacomp.2013.04.012
77. Bailey CJ, Gross JL, Pieters A, et al. Effect of dapagliflozin in patients with type 2 diabetes who have inadequate glycaemic control with metformin: a randomised, double-blind, placebo-controlled trial. Lancet. 2010;375(9733):2223–2233. doi:10.1016/s0140-6736(10)60407-2
78. Bode B, Stenlöf K, Harris S, et al. Long-term efficacy and safety of canagliflozin over 104 weeks in patients aged 55-80 years with type 2 diabetes. Diabetes Obesity Metab. 2015;17(3):294–303. doi:10.1111/dom.12428
79. Tanaka A, Node K. Increased amputation risk with canagliflozin treatment: behind the large cardiovascular benefit? Cardiovasc Diabetol. 2017;16(1). doi:10.1186/s12933-017-0611-x
80. Kaneko M, Narukawa M. Effects of sodium-glucose cotransporter 2 inhibitors on amputation, bone fracture, and cardiovascular outcomes in patients with type 2 diabetes mellitus using an alternative measure to the hazard ratio. Clin Drug Investig. 2018;39(2):179–186. doi:10.1007/s40261-018-0731-4
81. Kohler S, Zeller C, Iliev H, et al. Safety and tolerability of empagliflozin in patients with type 2 diabetes: pooled analysis of phase I–III clinical trials. Adv Ther. 2017;34(7):1707–1726. doi:10.1007/s12325-017-0573-0
82. Chang H-Y, Singh S, Mansour O, et al. Association between sodium-glucose cotransporter 2 inhibitors and lower extremity amputation among patients with type 2 diabetes. JAMA Intern Med. 2018;178(9):1190–1198. doi:10.1001/jamainternmed.2018.3034
83. Janghorbani M, Dam RMV, Willett WC, et al. Systematic review of type 1 and type 2 diabetes mellitus and risk of fracture. Am J Epidemiol. 2007;166(5):495–505. doi:10.1093/aje/kwm106
84. Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes—a meta-analysis. Osteoporosis Int. 2006;18(4):427–444. doi:10.1007/s00198-006-0253-4
85. Ma L, Oei L, Jiang L, et al. Association between bone mineral density and type 2 diabetes mellitus: a meta-analysis of observational studies. Eur J Epidemiol. 2012;27(5):319–332. doi:10.1007/s10654-012-9674-x
86. Thrailkill KM, Nyman JS, Bunn RC, et al. The impact of SGLT2 inhibitors, compared with insulin, on diabetic bone disease in a mouse model of type 1 diabetes. Bone. 2017;94:141–151. doi:10.1016/j.bone.2016.10.026
87. Thrailkill KM, Bunn RC, Nyman JS, et al. SGLT2 inhibitor therapy improves blood glucose but does not prevent diabetic bone disease in diabetic DBA/2J male mice. Bone. 2016;82:101–107. doi:10.1016/j.bone.2015.07.025
88. Bilezikian JP, Watts NB, Usiskin K, et al. Evaluation of bone mineral density and bone biomarkers in patients with type 2 diabetes treated with canagliflozin. J Clin Endocrinol Metab. 2016;101(1):44–51. doi:10.1210/jc.2015-1860
89. Kohan DE, Fioretto P, Tang W, et al. Long-term study of patients with type 2 diabetes and moderate renal impairment shows that dapagliflozin reduces weight and blood pressure but does not improve glycemic control. Kidney Int. 2014;85(4):962–971. doi:10.1038/ki.2013.356
90. Watts NB, Bilezikian JP, Usiskin K, et al. Effects of canagliflozin on fracture risk in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab. 2016;101(1):157–166. doi:10.1210/jc.2015-3167
91. Ruanpeng D, Ungprasert P, Sangtian J, et al. Sodium-glucose cotransporter 2 (SGLT2) inhibitors and fracture risk in patients with type 2 diabetes mellitus: a meta-analysis. Diabetes Metab Res Rev. 2017;33:6. doi:10.1002/dmrr.2903
92. Tang H, Zhang X, Zhang J, et al. Elevated serum magnesium associated with SGLT2 inhibitor use in type 2 diabetes patients: a meta-analysis of randomised controlled trials. Diabetologia. 2016;59(12):2546–2551. doi:10.1007/s00125-016-4101-6
93. Forst T, Guthrie R, Goldenberg R, et al. Efficacy and safety of canagliflozin over 52 weeks in patients with type 2 diabetes on background metformin and pioglitazone. Diabetes Obesity Metab. 2014;16(5):467–477. doi:10.1111/dom.12273
94. Weir MR, Kline I, Xie J, et al. Effect of canagliflozin on serum electrolytes in patients with type 2 diabetes in relation to estimated glomerular filtration rate (eGFR). Curr Med Res Opin. 2014;30(9):1759–1768. doi:10.1185/03007995.2014.919907
95. Taylor SI, Blau JE, Rother KI. Possible adverse effects of SGLT2 inhibitors on bone. Lancet Diabetes Endocrinol. 2015;3(1):8–10. doi:10.1016/s2213-8587(14)70227-x
96. Linfoot P, Bergstrom C, Ipp E. Pathophysiology of ketoacidosis in Type 2 diabetes mellitus. Diabetic Med. 2005;22(10):1414–1419. doi:10.1111/j.1464-5491.2005.01660.x
97. Daniele G, Xiong J, Solis-Herrera C, et al. Dapagliflozin enhances fat oxidation and ketone production in patients with type 2 diabetes. Diabetes Care. 2016;39(11):2036–2041. doi:10.2337/dc15-2688
98. Perry RJ, Rabin-Court A, Song JD, et al. Dehydration and insulinopenia are necessary and sufficient for euglycemic ketoacidosis in SGLT2 inhibitor-treated rats. Nat Commun. 2019;10:(1):548. doi:10.1038/s41467-019-08466-w
99. Peters AL, Buschur EO, Buse JB, et al. Euglycemic diabetic ketoacidosis: a potential complication of treatment with sodium–glucose cotransporter 2 inhibition. Diabetes Care. 2015;38(9):1687–1693. doi:10.2337/dc15-0843
100. Fralick M, Schneeweiss S, Patorno E. Risk of diabetic ketoacidosis after initiation of an SGLT2 inhibitor. N Engl J Med. 2017;376(23):2300–2302. doi:10.1056/nejmc1701990
101. Donnan JR, Grandy CA, Chibrikov E, et al. Comparative safety of the sodium glucose co-transporter 2 (SGLT2) inhibitors: a systematic review and meta-analysis. BMJ Open. 2019;9:1. doi:10.1136/bmjopen-2018-022577
102. Saad M, Mahmoud AN, Elgendy IY, et al. Cardiovascular outcomes with sodium–glucose cotransporter-2 inhibitors in patients with type II diabetes mellitus: a meta-analysis of placebo-controlled randomized trials. Int J Cardiol. 2017;228:352–358. doi:10.1016/j.ijcard.2016.11.181
103. Häring H-U, Merker L, Seewaldt-Becker E, et al. Empagliflozin as add-on to metformin in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care. 2014;37(6):1650–1659. doi:10.2337/dc13-2105
104. Kovacs CS, Seshiah V, Swallow R, et al. Empagliflozin improves glycaemic and weight control as add-on therapy to pioglitazone or pioglitazone plus metformin in patients with type 2 diabetes: a 24-week, randomized, placebo-controlled trial. Diabetes Obesity Metab. 2013;16(2):147–158. doi:10.1111/dom.12188
105. Storgaard H, Gluud LL, Bennett C, et al. Benefits and harms of sodium-glucose co-transporter 2 inhibitors in patients with type 2 diabetes: a systematic review and meta-analysis. PLoS One. 2016;11:11. doi:10.1371/journal.pone.0166125
106. Hayashi T, Fukui T, Nakanishi N, et al. Dapagliflozin decreases small dense low-density lipoprotein-cholesterol and increases high-density lipoprotein 2-cholesterol in patients with type 2 diabetes: comparison with sitagliptin. Cardiovasc Diabetol. 2017;16:1. doi:10.1186/s12933-016-0491-5
107. Pieber TR, Famulla S, Eilbracht J, et al. Empagliflozin as adjunct to insulin in patients with type 1 diabetes: a 4-week, randomized, placebo-controlled trial (EASE-1). Diabetes Obesity Metab. 2015;17(10):928–935. doi:10.1111/dom.12494
108. Briand F, Mayoux E, Brousseau E, et al. Empagliflozin, via switching metabolism toward lipid utilization, moderately increases LDL cholesterol levels through reduced LDL catabolism. Diabetes. 2016;65(7):2032–2038. doi:10.2337/db16-0049
109. Zoppini G, Targher G, Chonchol M, et al. Serum uric acid levels and incident chronic kidney disease in patients with type 2 diabetes and preserved kidney function. Diabetes Care. 2011;35(1):99–104. doi:10.2337/dc11-1346
110. Chang Y-H, Lei -C-C, Lin K-C, et al. Serum uric acid level as an indicator for CKD regression and progression in patients with type 2 diabetes mellitus-a 4.6-year cohort study. Diabetes Metab Res Rev. 2015;32(6):557–564. doi:10.1002/dmrr.2768
111. Zhou Y, Fang L, Jiang L, et al. Uric acid induces renal inflammation via activating tubular NF-κB signaling pathway. PLoS One. 2012;7:6. doi:10.1371/journal.pone.0039738
112. Dekkers CCJ, Petrykiv S, Laverman GD, et al. Effects of the SGLT-2 inhibitor dapagliflozin on glomerular and tubular injury markers. Diabetes Obesity Metab. 2018;20(8):1988–1993. doi:10.1111/dom.13301
113. Jabbour SA, Hardy E, Sugg J, et al. Dapagliflozin is effective as add-on therapy to sitagliptin with or without metformin: a 24-week, multicenter, randomized, double-blind, placebo-controlled study. Diabetes Care. 2013;37(3):740–750. doi:10.2337/dc13-0467
114. Bailey CJ, Gross JL, Hennicken D, et al. Dapagliflozin add-on to metformin in type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled 102-week trial. BMC Med. 2013;11:1. doi:10.1186/1741-7015-11-43
115. Zhao Y, Xu L, Tian D, et al. Effects of sodium‐glucose co‐transporter 2 (SGLT2) inhibitors on serum uric acid level: a meta‐analysis of randomized controlled trials. Diabetes Obesity Metab. 2017;20(2):458–462. doi:10.1111/dom.13101
116. Rosenwasser R, Sultan S, Sutton D, et al. SGLT-2 inhibitors and their potential in the treatment of diabetes. Diabetes Metab Syndrome Obesity. 2013:453–467. doi:10.2147/dmso.s34416
117. Chino Y, Samukawa Y, Sakai S, et al. SGLT2 inhibitor lowers serum uric acid through alteration of uric acid transport activity in renal tubule by increased glycosuria. Biopharm Drug Dispos. 2014;35(7):391–404. doi:10.1002/bdd.1909
118. Wanner C, Inzucchi SE, Lachin JM, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323–334. doi:10.1056/NEJMoa1515920
119. Mosenzon O, Wiviott SD, Cahn A, et al. Effects of dapagliflozin on development and progression of kidney disease in patients with type 2 diabetes: an analysis from the DECLARE–TIMI 58 randomised trial. Lancet Diabetes Endocrinol. 2019;7(8):606–617. doi:10.1016/S2213-8587(19)30180-9
120. Perkovic V, Jardine MJ, Neal B, et al. Canagliflozin and Renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295–2306. doi:10.1056/NEJMoa1811744
121. Herrington WG, Preiss D, Haynes R, et al. The potential for improving cardio-renal outcomes by sodium-glucose co-transporter-2 inhibition in people with chronic kidney disease: a rationale for the EMPA-KIDNEY study. Clin Kidney J. 2018;11(6):749–761. doi:10.1093/ckj/sfy090
122. Ritesh J, U.S. Food and Drug Administration. Center for Drug Evaluation and Research. Dapagliflozin Clinical Pharmacology Review (Report No. 202293). Silver Spring, MD: Division of Drug Information.
123. Tang H, Dai Q, Shi W, Zhai S, Song Y, Han J. SGLT2 inhibitors and risk of cancer in type 2 diabetes: a systematic review and meta-analysis of randomised controlled trials. Diabetologia. 2017;60(10):1862–1872. doi:10.1007/s00125-017-4370-8
124. Shaikh A. SGLT2 inhibitors and cancer: why further evidence is required. Diabetologia. 2017;60(12):2536–2537. doi:10.1007/s00125-017-4434-9
125. Dicembrini I, Nreu B, Mannucci E, et al. Sodium‐glucose co‐transporter‐2 (SGLT‐2) inhibitors and cancer: a meta‐analysis of randomized controlled trials. Diabetes Obesity Metab. 2019. doi:10.1111/dom.13745
126. Washburn WN, Poucher SM. Differentiating sodium-glucose co-transporter-2 inhibitors in development for the treatment of type 2 diabetes mellitus. Expert Opin Investig Drugs. 2013;22(4):463–486. doi:10.1517/13543784.2013.774372
127. Cefalo CMA, Cinti F, Moffa S, et al. Sotagliflozin, the first dual SGLT inhibitor: current outlook and perspectives. Cardiovasc Diabetol. 2019;18:1. doi:10.1186/s12933-019-0828-y
128. Rieg JAD, Rieg T. What does sodium‐glucose co‐transporter 1 inhibition add: prospects for dual inhibition. Diabetes Obesity Metab. 2019;21(S2):43–52. doi:10.1111/dom.13630
129. Zambrowicz B, Freiman J, Brown PM, et al. LX4211, a dual SGLT1/SGLT2 inhibitor, improved glycemic control in patients with type 2 diabetes in a randomized, placebo-controlled trial. Clin Pharmacol Ther. 2012;92(2):158–169. doi:10.1038/clpt.2012.58
130. Zambrowicz B, Lapuerta P, Strumph P, et al. LX4211 therapy reduces postprandial glucose levels in patients with type 2 diabetes mellitus and renal impairment despite low urinary glucose excretion. Clin Ther. 2015;37:1. doi:10.1016/j.clinthera.2014.10.026
131. Garg SK, Henry RR, Banks P, et al. Effects of sotagliflozin added to insulin in patients with type 1 diabetes. N Engl J Med. 2017;377(24):2337–2348. doi:10.1056/nejmoa1708337
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.