")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Socioeconomic and Behavioral Disparities Among Diabetics in Saudi Arabia: A Nation-Wide Descriptive Study
Authors Almubark RA , Althumairi NA, Alhamdan AA, AlNujaidi HY , Alzayer R, Almubark SA, BinDhim NF
Received 14 December 2021
Accepted for publication 29 July 2022
Published 2 September 2022 Volume 2022:15 Pages 2693—2703
DOI https://doi.org/10.2147/DMSO.S352769
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Rasha A Almubark,1,2 Nora A Althumairi,1 Adel A Alhamdan,3 Heba Y AlNujaidi,4 Reem Alzayer,5 Sarh A Almubark,6 Nasser F BinDhim1,7
1Scientific Department, Sharik Research Institution, Riyadh, Kingdom of Saudi Arabia; 2Department of Medical Sciences, Community College, Princess Nourah Bint Abdul Rahman University, Riyadh, Kingdom of Saudi Arabia; 3Community Health Sciences Department, College of Applied Medical Sciences, King Saud University, Riyadh, Kingdom of Saudi Arabia; 4College of Public Health, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia; 5Pharmacy Department, Mohammed Al-Mana College for Medical Sciences, Dammam, Kingdom of Saudi Arabia; 6Health Services Management Department, Faculty of public health, Umm Alqura University, Makkah, Kingdom of Saudi Arabia; 7College of Medicine, Alfaisal University, Riyadh, Kingdom of Saudi Arabia
Correspondence: Rasha A Almubark, Scientific Department, Sharik Research Institution, 6996 Abi baker Road, Alyasmin dis, Riyadh, 13326– 4549, Kingdom of Saudi Arabia, Tel +966 533 0000 43, Email [email protected]
Purpose: This study aims to explore sociodemographic, behavioral and clinical factors in adult participants with Diabetes in Saudi Arabia.
Methods: A population-based cross-sectional study of 20492 potential participants conducted in quarters 1 and 2 in 2021 from all 13 administrative regions of Saudi Arabia. A backward maximum likelihood logistic regression model, including all variables, was used to identify variables associated with participants living with Diabetes.
Results: A total of 14007 participants, aged ≥ 18 years, completed the interview, with a response rate of 68.3% and successful quota sampling. Fifty percent were male, the mean age was 36.7 (SD 13.7; range: 18– 90). Of the total sample, 1633, 11.7% had Diabetes. Seven percent only of diabetic patients (124 participants) had an acceptable level of fruit and vegetable intake. In addition, only (274, 16.8%) had an acceptable level of physical activity, compared to (2389, 19.3%) in the non-diabetic group. Daily smokers were slightly higher in the diabetic group compared to the non-diabetic group (13.2% vs 11.7%). Hypertension was reported mostly by the diabetic group (45.1% vs 8%). Overweight and Obesity were more prevalent in patients with Diabetes (72.50% vs 51.62%). The results of the logistic regression have shown that several sociodemographic, behavioral and intermediate risk factors were significantly associated with Diabetes.
Conclusion: The study found that the prevalence of Diabetes in Saudi Arabia is around 12%, which is lower than the previously reported prevalence of Diabetes in Saudi Arabia. Moreover, Diabetes was found to be associated with lower educational level, smoking, obesity and overweight, hypercholesterolemia and hypertension. These factors are essential to be identified and screened in the community at regular interval; furthermore, controlling these factors may improve their disease management and quality of life. Additionally, knowing these factors will assist policymakers to shape an effective practical approach to combat diabetes widespread.
Keywords: diabetes mellitus, diet, surveillance, epidemiology, Saudi Arabia
Introduction
Over the past 30-year period, Diabetes is still one of the top drivers for increasing global burden of disease. A systematic analysis for the Global Burden of Disease (GBD) from 1990 to 2019 across 204 countries has shown that age-standardized Disability-adjusted life-years (DALY) rates for Diabetes has increased by 24.4% (18·5–29·7).1 Despite the efforts made by the governments and medical staff to improve Diabetes management, Diabetes continues to place a significant burden on healthcare system, societies, and patients around the world. As well as, rising death rates due to poorly controlled Diabetes which is estimated to be responsible for 11.3% of fatalities worldwide.2
The International Diabetes Federation (IDF) reported that Middle East and North African (MENA) region has the world’s highest adult age adjusted Diabetes prevalence of 12.2%, which is expected to rise to 13.3% by 2030.3 The rates are ranging from 6.8% in Africa to 16.2% (highest) in the Middle East and North Africa.4 This high prevalence of Diabetes occurring in the Middle East and North Africa is due to the region’s rapid economic expansion, urbanization, and changes in lifestyle patterns.5
Three of the world’s top ten Diabetes-prevalence countries are in the Middle East: Kingdom of Saudi Arabia, Kuwait, and Qatar.3 The Kingdom of Saudi Arabia (KSA), specifically, is experiencing a high rate of Diabetes in a young population.6 Moreover, KSA rates of Diabetes have roughly reached a ten-fold increase in the past three eras.7
As reported by Institute for Health Metrics and Evaluation (IHME), Diabetes is ranked as the 8th top ten causes of deaths, which has increased death rate by 37.4% from 2009 to 2019.8 This will lead to a significant economic burden on individuals and national health-care systems. In fact, Diabetes-related health-care expenditures accounted for 11% of overall health-care expenditures worldwide in 2011. In KSA, the healthcare burden attributable to Diabetes is anticipated to surpass $0.87 billion.9
In addition, KSA has recently witnessed a decrease in fruit and vegetable consumption and physical activity, as well as considerable increases in e-cigarette use, occurrence of hypertension, and hypercholesterolemia, which may rise up the burden of chronic diseases in KSA.10
The healthcare system in Saudi Arabia is divided mainly into two parts: public and private. Both the Ministry of Health (MoH) and other government agencies administer public health-care facilities and delivery. The MoH oversees the network of community Primary Health Care Clinics (PHCCs) as well as larger public hospitals. Non-Saudis living in Saudi Arabia have access to the healthcare system; they can have private insurance and use private facilities, or they can use public facilities for free.
Unfortunately, health-care services are concentrated in urban areas, making access to rural areas difficult. Private health services are growing and are expected to support public infrastructure under Vision 2030.
Quality Diabetes care necessitates a population-based, evidence-based, and patient-centered approach.11 Numerous studies have examined the prevalence and distribution of Diabetes in KSA, but very few have examined socioeconomic and clinical characteristics of diabetic patients in KSA.12 Additionally, KSA has gone through a major socio-economic changes in the past decades that led to lifestyle changes and habits alteration.5
Thus, this study aims to explore sociodemographic determinants, behavioral and clinical factors in adult participants with Diabetes in KSA and to compare these factors to non-diabetic participants.
Materials and Methods
Design
This project is generated from a secondary analysis of Sharik Health Indicators Surveillance System (SHISS) (first and second quarters of 2021). The survey was developed and collected using ZdataCloud® research data collection system,13 which had integrated eligibility and sampling modules, to control sample’s distribution and to prevent human-related sampling bias.13 SHISS consists of short cross-sectional phone-interviews conducted in all 13 administrative regions of Saudi Arabia on a quarterly basis.10 Each phone survey was approximately 4 minutes and was conducted by a trained data collector. All questions had to be answered for the questionnaire to be successfully submitted to the database. All data were coded and stored on the ZdataCloud® database.13
SHISS Sampling and Sample Size
To guarantee accurate representation of the population, SHISS applied proportional quota sampling method to obtain an equal distribution of participants, stratified by age and gender, within and across the 13 administrative regions of Saudi Arabia. SHISS uses in its quota sampling two age groups (18–36 and 37+) based on the Saudi Arabian median age of 36 years which generates 52 strata.
The sample size in the SHISS was calculated based on the medium effect size of approximately 0.25 with 80% power and a 95% confidence level to provide sufficient power for comparison between sampling quotas.14 Thus, each quota required at least 135 participants, and a total sample of 540 per region, to form a grand total of 7020 participants/wave. Once the quota sample was reached, participants with similar characteristics were not eligible to participate in the study. The quota sampling is an automated process with no human interference, as the sampling process is controlled automatically by the ZdataCloud®.13
SHISS Participants and Recruitment
The participants were included in the study if they met the following inclusion criteria: 1) they were a resident of Saudi Arabia, 2) they were aged ≥18 years at the time of survey, and 3) they were fluent in spoken Arabic. Respondents were contacted by phone, and were first asked demographic questions (including region of residence and age). Respondents were excluded if quotas for cell in which the participant fell were full. A random phone number list was generated from Sharik Research Institution to identify potential participants.15 The Sharik database is composed of individuals who are interested in participating in future research projects, and contains a growing number of registered participants, having reached more than 200 000, distributed across the 13 regions of Saudi Arabia.15 SHISS integrates eligibility and sampling modules including three questions for verifying eligibility for sampling strata. Once these questions are answered, the SHISS blocks ineligible respondents from progressing with the interview. Participants were contacted by phone on up to three occasions. If they did not respond, a new number with similar demographics was generated from the database until the quota was completed and closed automatically. After obtaining consent to participate, the SHISS interviewer assessed the eligibility of the participant, based on the above-mentioned quota completion criteria.
SHISS Questionnaire Design
After providing verbal consent, participants were asked about their age to determine eligibility as this study is only targeting adults. Then the data collector would record the age, gender, and region of the participant. Thereafter, major chronic diseases and major behavioral and intermediate risk factors as suggested by the WHO and the CDC were collected.16,17 As shown in the HISS data model (Figure 1) the dataset included behavioral risk factors (diet, physical activity, and tobacco use including cigarette, waterpipe, and e-cigarette), diagnosed on-treatment intermediate risk factors (hypertension and hypercholesterolemia) and obesity. Finally, diagnosed major chronic diseases for participants currently receiving treatment for, Diabetes, hypercholesterolemia, hypertension, heart disease, stroke, cancer, and chronic respiratory disease. Moreover, the existence of diagnosed genetic diseases was also recorded as a non-modifiable risk factor. In 2021, SHISS introduced new variables including income and education level and depression screening using Patient Health Questionnaire-2 (PHQ-2).18
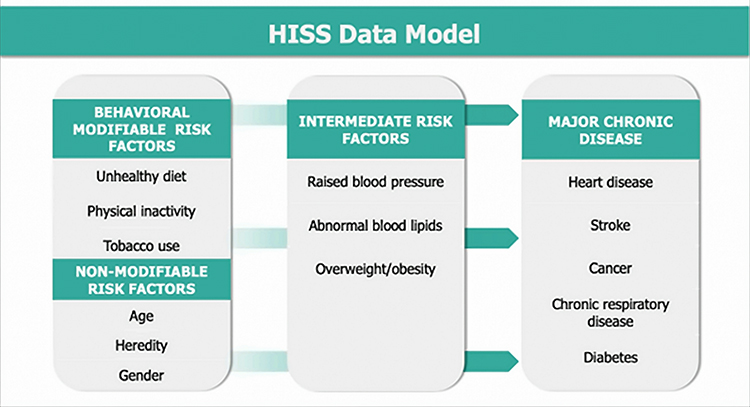 |
Figure 1 Health Indicators Surveillance System (HISS) data model. |
Participants were asked to provide their height in cm and weight in kg, and then body mass index (BMI) was calculated, using the following formula:
BMI = (Weights (kg))/(Height(m))2.7
The Center for Disease Control and Prevention (CDC) BMI category status was used (Underweight: Below 18.5, Normal or Healthy Weight: 18.5–24.9, Overweight: 25.0–29.9, Obese: 30.0 and Above) [20]. This study used the WHO’s global recommendations on physical activity for adults (18–64 years old): (1) vigorous intensity physical activity (VIPA), 75 min per week, or (2) moderate intensity physical activity MIPA, 150 min per week [21]. Based on participants’ self-reported responses to the interview questionnaire (ie, number of exercise minutes, frequency, and intensity level per week), two categorical outcome variables were created to reflect whether or not guidelines were met. Categories as: an acceptable level of physical activity (ALPA) (at least 150 min of MIPA per week and/or at least 75 min of VIPA per week) and a low level of physical activity (LLPA) (less than 150 min of MIPA and/or less than 75 min of VIPA).
In addition, participants were asked about their daily fruit and vegetable intake. If a participant’s daily food intake included at least one portion of fruit and one portion of vegetables, they were categorized as having an acceptable level of fruit and vegetable intake (AFVI). If not, they were categorized as having a low level of fruit and vegetable intake (LFVI). For depression screening, PHQ-2 with a cut-off score of ≥3 was used [19].
Statistical Analysis
Descriptive statistics were used to describe prevalence. Quantitative variables are presented herein by mean and SD values if they have a normal distribution, or median and range, as appropriate, and are compared using the t-test. Categorical variables are presented as Frequency (n) and percentages (%). Bivariate analysis was conducted using a chi- square test of association between the presence of Diabetes and respondent socio-characteristic. A backward maximum likelihood logistic regression model including all the variables was used to identify variables that are currently associated with Diabetes status. As this study used automated electronic data collection, there were no missing values; the ZdataCloud® also includes a data integrity check to prevent users from entering invalid data (eg, the maximum age is between 18 and 99).13 The results have been reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for cross-sectional studies.19
Ethical Considerations
Because data collection was done by phone interviews in this study, participant consent was obtained verbally. Trained data collectors used participants information sheet, as a guide for the verbal explanation of the study by providing all relevant information (purpose, process, risks, benefits, alternatives to participation), and allowed the potential participant sufficient time to ask questions or to voice concerns.
After obtaining verbal consent, their response was recorded in the data collection system. Without verbal consent from potential participants, no survey would show or be submitted.
Because this research poses no more than minimal risk of harm to subjects and involves no procedures for which written consent is normally required. The local ethics committee of Sharik Research Institution approved this research project (Approval no. 2021–2), in accordance with national research ethics regulations. The authors declare that the study complies with the Declaration of Helsinki.
Results
Out of 20492 potential participants contacted in quarter 1 and 2 in 2021, 14007 participants completed the questionnaire from all the13 administrative regions of Saudi Arabia, with a response rate of 68.3% and successful quota sampling. Out of the total participants, 50.1% were male. The mean age was 36.7 (SD 13.7; range: 18–90). Table 1 shows the sociodemographic characteristics by Diabetes status.
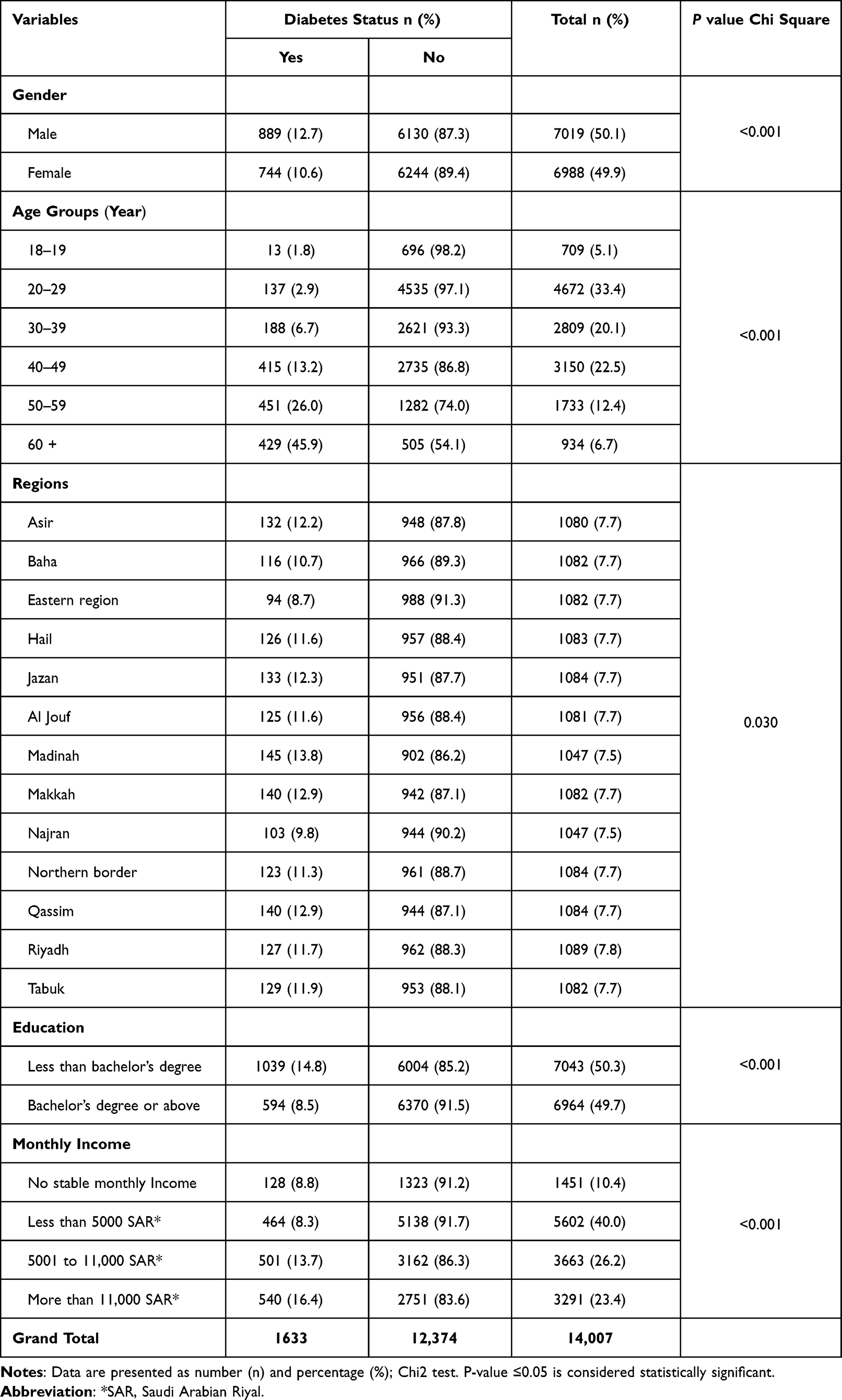 |
Table 1 Comparison of Sociodemographic Characteristics of Saudi Adults with and without Diabetes(n = 14,007) |
The overall prevalence of Diabetes in the sample is 11.7%. Table 2 shows the prevalence of chronic diseases and behavioral risk factors in the sample by Diabetes status.
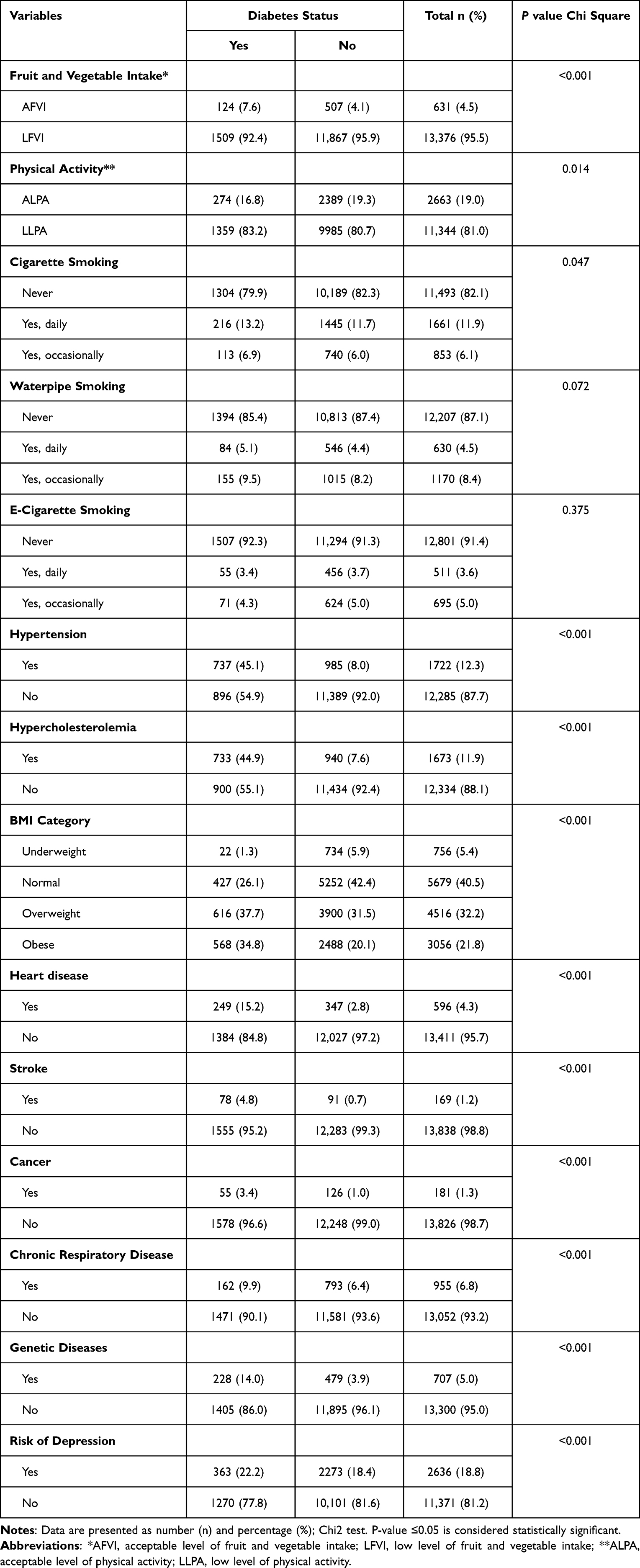 |
Table 2 Comparison of Behavioral and Intermediate Risk Factors Between Diabetic and Non-Diabetic Groups (n = 14,007) |
The regression model revealed that participants with Diabetes are associated with more likelihood of having lower educational level, living in regional regions, having overweight, obesity, hypercholesterolemia, hypertension, genetic diseases, risk of depression, and smoking waterpipe occasionally. However, sex and fruit and vegetable intake were eliminated from the model. Table 3: shows the results of the regression model.
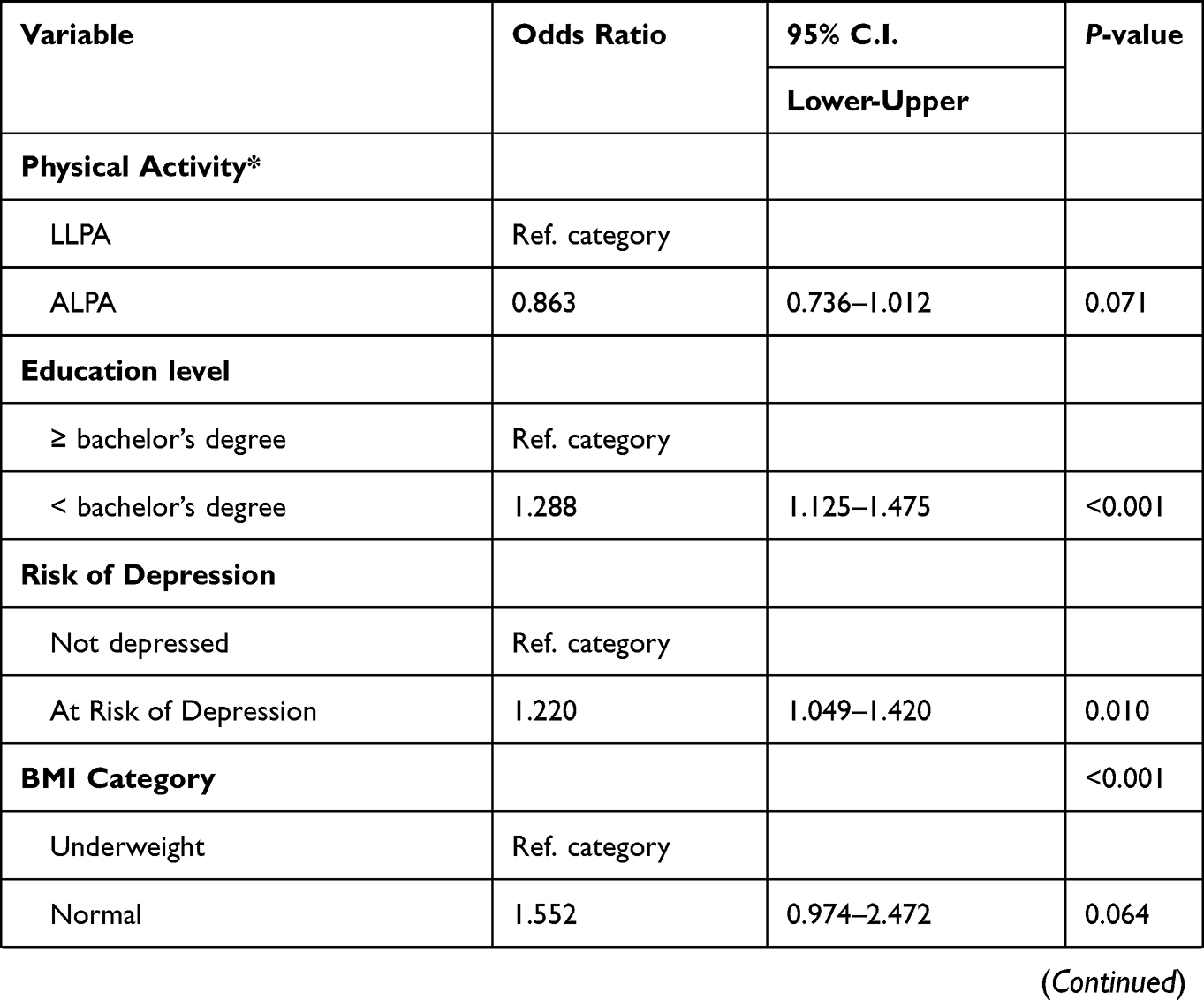 | 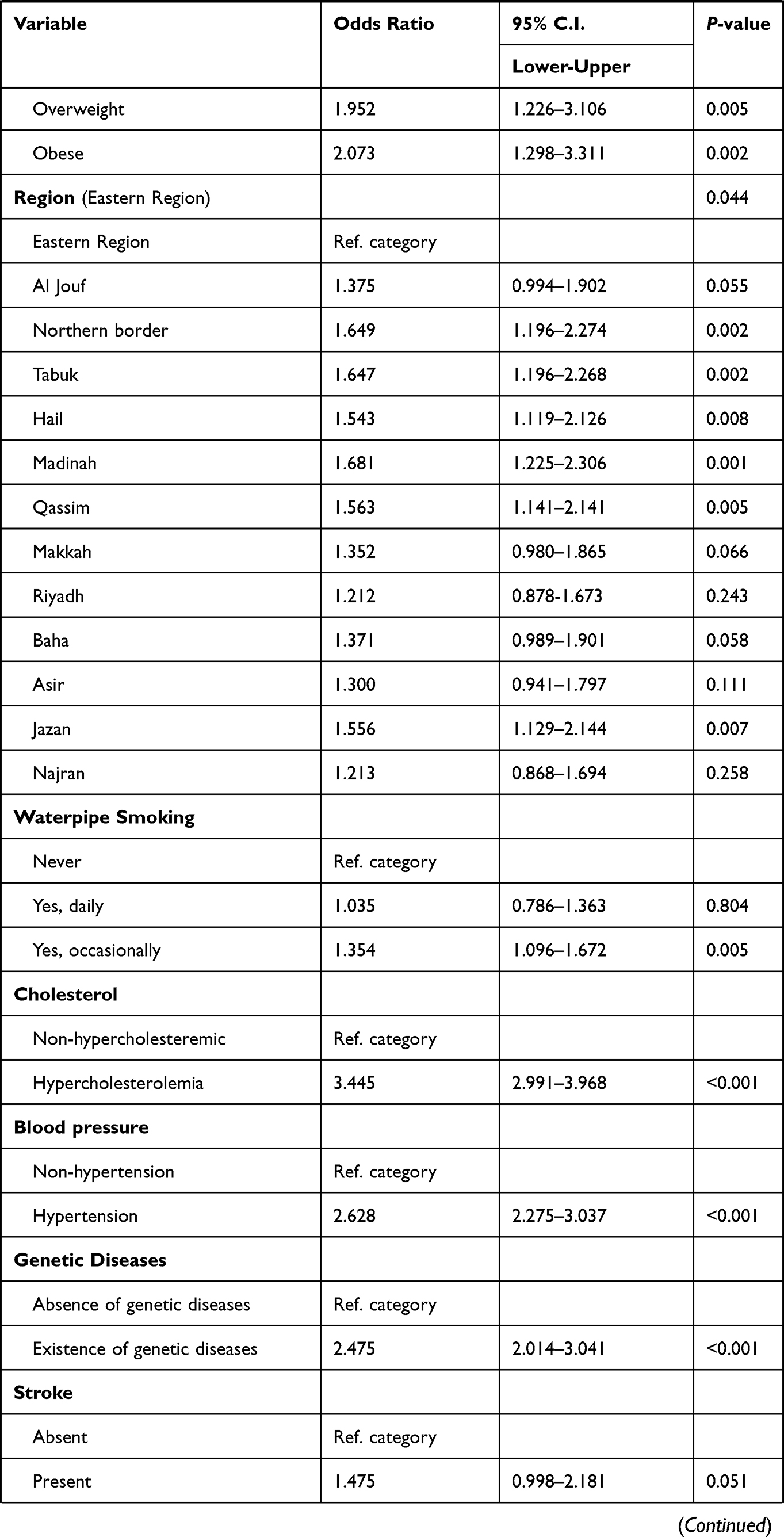 | 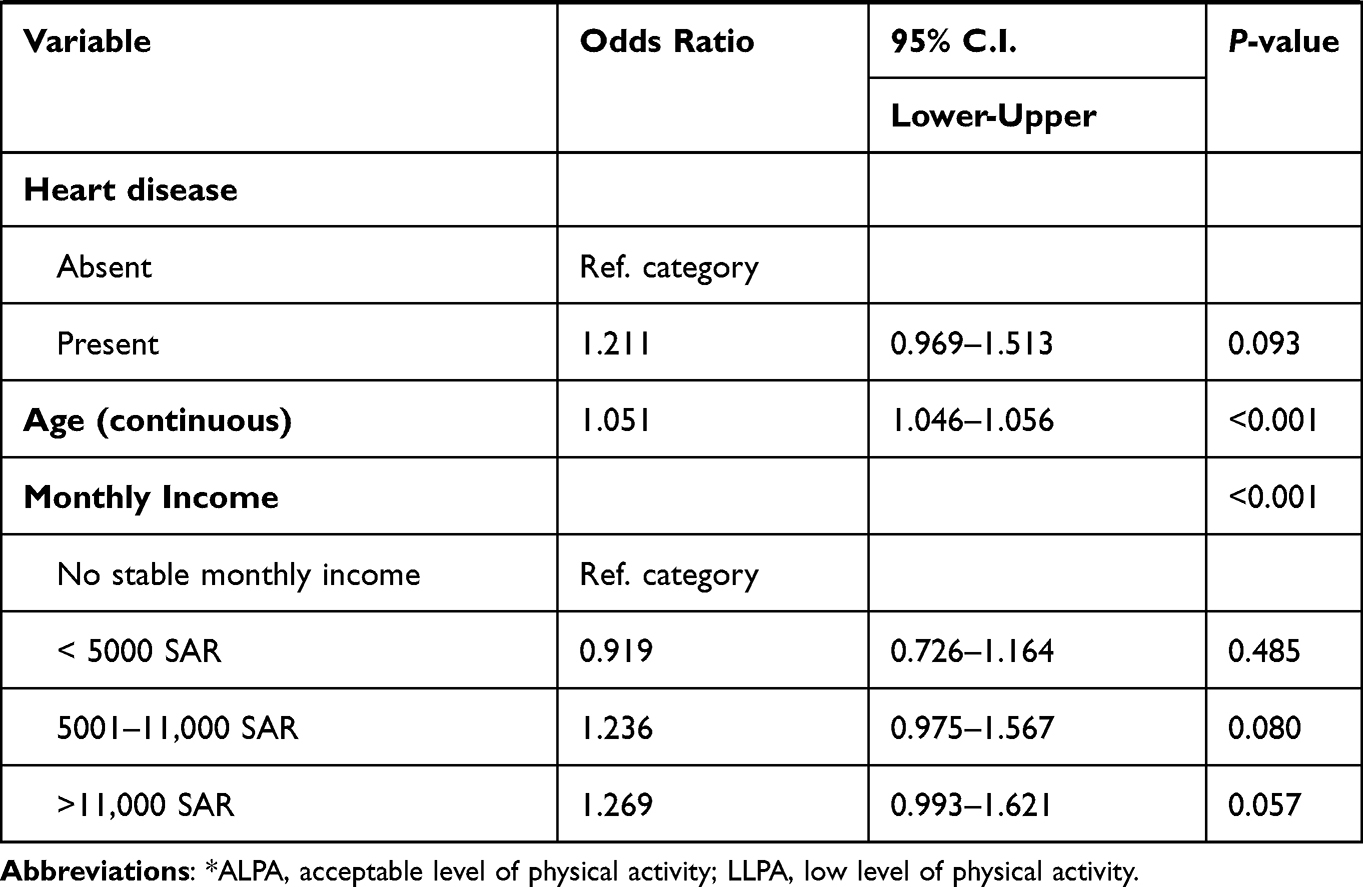 |
Table 3 Variables Associated with Diabetes in Saudi Arabia (n = 14,007) |
Discussion
The primary purpose of this study was to determine the prevalence of Diabetes and its association with sociodemographic status, behavioral and intermediate risk factors. This was a national study of adult participants in KSA aged 18 years and above. In this study, the prevalence of Diabetes was 11.7% (12.7% in male and 10.6% in female). The prevalence was lower than previously reported Nationwide prevalence rate of type 2 Diabetes in Saudi Arabia that was range from 23.7% in Saudi adults in the age group of 30–70-years (26.2% in male and 21.5% in female)20 to 25.4% in adults aged ≥30 years (29.1% in male and 21.9% in female).21 However, it confirms the lower rates of diabetes (between 8% and 13.5%) found in more recent studies.10,22
This study supports evidence from previous observations that males have a higher prevalence of Diabetes compared to females.7,21,23 A substantial proportion of diabetic participants suffered from overweight and obesity (37.7% and 34.8% respectively). These results are likely to be related to several initiatives aiming to decrease the rate of obesity that were implemented in KSA by different governmental organizations, such as the Obesity Control Program (OCP) by the Saudi Ministry of Health (MoH),24 and the Sports Boulevard Project, introduced by the local Riyadh municipal authority.25 However, even with the application of these interventions, the rates of Diabetes, and its associated factors such as obesity, were considered high.
Another critical modifiable risk factor associated with Diabetes is smoking which had been known to increase the risk of developing Diabetes and mortality. Various studies have established a causal relationship between cigarette smoking and chronic diseases.26 The risk is greater among current smokers than among former smokers. In addition, passive smoking is also a risk factor of Diabetes even in those who were not active smokers.27 Our data revealed that participants with Diabetes were associated with more likelihood to be occasional waterpipe smokers which could worsen their disease progression. A reasonable approach to tackle this issue could be by focusing on such behavior via physician advice and health promotion campaigns, targeting Diabetes patients in Saudi Arabia are particularly important to improve quality of life and disease management outcomes.
The most common cause of mortality and disability among diabetics is cardiovascular disease.5 High blood pressure, high cholesterol, and other risk factors contribute to an elevated risk of cardiovascular problems in patients with Diabetes. Our study found that Diabetes was associated with higher likelihood of having hypercholesterolemia, hypertension, genetic diseases, and risk of depression. All of which could play a vital role in reducing quality of life and worsening disease progression. More focus on multidisciplinary interventions and screening Diabetes patients in Saudi Arabia for such conditions, will provide more positive disease management outcomes.
Diabetes affects more people living in urban areas than in rural areas. The number of diabetic patients in low- and middle-income nations is 181 million in urban areas and 122 million in rural regions. The gap is anticipated to increase further by 2035, with 347 million people living in urban areas and 145 million in rural areas.5 In our study, people with lower educational level were more likely to suffer from Diabetes than others, which is consistent with what was found in literature.28–30 It has been reported that lower levels of education may increase the risk of Diabetes by 2 to 4 times compared to higher educational levels.28 Thus, it is important to customize health promotion campaigns related to Diabetes to be more understandable to a lower level of education.
A few articles have called for the need to implement a national prevention program for Diabetes in KSA.7,30 Due to Diabetes being a substantial economic burden, Diabetes could be diminished by implementing low-cost, easy-to-implement interventions. Even in developing countries, many of these interventions are cost effective and/or cost saving. Yet, these interventions are underutilized.31 The health burden due to Diabetes and its associated risk factors in KSA is expected to increase to tragic levels, unless a comprehensive epidemic management program is integrated.9
A limitation of this study is the way the data were collected through SHISS using Quota sampling rather than random probability sampling, which is associated with the risk of selection bias. This study, however, used a proportionally large sample size and fifty-two quotas to reduce sampling bias. In addition, the SHISS recruitment and sampling methods have been used successfully in several other national projects in KSA and it generated results that are consistent with other national surveys or records. The multi-wave design used in SHISS, as well as the systematic, high-quality data collection process and large sample size, make it an appropriate methodology for assessing the effects of large-scale events on general population health.
The data collection system used in this study “ZdataCloud®” has an integrated eligibility and sampling modules, allowing us to accurately represent the population. However, because more than one participant can pass the eligibility process at the exact time when ZdataCloud® closes the quota after completing the targeted sample, and because a group of phone call attempts is occurring at the same time, more than one participant can pass the eligibility process, and there may have been a very slight sample increase in some of the quotas above the targeted sample, resulting in a slightly larger sample size in some quotas. In addition, due to the nature of the study, the information provided by participants was self-reported. Unfortunately, this may have introduced bias into the study.
In conclusion, the study highlights the possible role of sociodemographic determinants, behavioral and clinical factors in adult participants with Diabetes in KSA. Extending the scope of Diabetes policies and regulations to include these data would improve clinicians’ and health systems’ ability to engage and treat patients with Diabetes and improve disease management outcomes, while also allowing policymakers to shape efforts to reduce such chronic conditions nationally.
Conclusion
The study revealed that the prevalence of diabetes in Saudi Arabia is 11.65%. Factors associated with diabetes in KSA participants include lower educational level, living in rural regions, obesity and overweight, chronic disease such as hypercholesterolemia, hypertension, and smoking. These factors are important to identify high risk groups in the community. Additionally, knowing these factors will assist policymakers to shape an effective approach to combat this widespread. Extending the scope of diabetes policies and regulations to include these data with such social determinants would improve clinicians’ and health systems’ ability to engage and treat patients with diabetes and improve disease management outcomes, while also allowing policymakers to shape efforts to reduce such chronic conditions nationally.
Disclosure
The authors report no conflicts of interest in this work.
References
1. GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Lond Engl. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Hwalla N, Jaafar Z, Sawaya S. Dietary management of type 2 diabetes in the MENA region: a review of the evidence. Nutrients. 2021;13(4):1060. doi:10.3390/nu13041060
3. International Diabetes Federation (IDF). IDF diabetes atlas; 2013. Available from: https://idf.org/e-library/epidemiology-research/diabetes-atlas.html.
4. Saeedi P, Salpea P, Karuranga S, et al. Mortality attributable to diabetes in 20–79 years old adults, 2019 estimates: results from the International Diabetes Federation Diabetes Atlas. Diabetes Res Clin Pract. 2020;162:108086. doi:10.1016/j.diabres.2020.108086
5. Alotaibi A, Perry L, Gholizadeh L, Al-Ganmi A. Incidence and prevalence rates of diabetes mellitus in Saudi Arabia: an overview. J Epidemiol Glob Health. 2017;7(4):211–218. doi:10.1016/j.jegh.2017.10.001
6. El Bcheraoui C, Basulaiman M, Tuffaha M, et al. Status of the diabetes epidemic in the Kingdom of Saudi Arabia, 2013. Int J Public Health. 2014;59(6):1011–1021. doi:10.1007/s00038-014-0612-4
7. Al Dawish MA, Robert AA, Braham R, et al. Diabetes mellitus in Saudi Arabia: a review of the recent literature. Curr Diabetes Rev. 2016;12(4):359–368. doi:10.2174/1573399811666150724095130
8. Institute for Health Metrics and Evaluation. Saudi Arabia global burden of disease. IHME; 2015. Available from: http://www.healthdata.org/saudi-arabia.
9. Naeem Z. Burden of Diabetes Mellitus in Saudi Arabia. Int J Health Sci. 2015;9(3):V–VI.
10. BinDhim NF, Althumiri NA, Basyouni MH, et al. Exploring the impact of COVID-19 response on population health in Saudi Arabia: results from the “Sharik” health indicators surveillance system during 2020. Int J Environ Res Public Health. 2021;18(10):5291. doi:10.3390/ijerph18105291
11. Heng BH, Sun Y, Cheah JTS, Jong M. The Singapore National Healthcare Group Diabetes Registry–descriptive epidemiology of type 2 diabetes mellitus. Ann Acad Med Singapore. 2010;39(5):348–352.
12. Tourkmani AM, Alharbi TJ, Rsheed AB, Alotaibi YK. Utilizing diabetes registry for exploring sociodemographic and clinical characteristics of type II diabetic patients in Saudi Arabia. Saudi Med J. 2021;42(1):56–65. doi:10.15537/smj.2021.1.25629
13. Z-DataCloud. Available from: https://zdatacloud.com/.
14. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
15. Sharik Health; 2021. Available from: https://sharikhealth.com.
16. World Health Organization. Chronic diseases and their common risk factors; 2005. Available from: https://www.who.int/chp/chronic_disease_report/media/Factsheet1.pdf.
17. Centers for Disease Control and Prevention. About chronic diseases; 2021. Available from: https://www.cdc.gov/chronicdisease/about/index.htm.
18. Kroenke K, Spitzer RL, Williams JBW. The Patient Health Questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. doi:10.1097/01.MLR.0000093487.78664.3C
19. Von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg Lond Engl. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
20. Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25(11):1603–1610.
21. Al-Rubeaan K, Al-Manaa H, Khoja T, et al. The Saudi abnormal glucose metabolism and diabetes impact study (Saudi-DM). Ann Saudi Med. 2014;34(6):465–475. doi:10.5144/0256-4947.2014.465
22. Saudi Arabian Ministry of Health (MoH). World Health Survey Saudi Arabia (KSAWHS); 2019:192. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/Population-Health-Indicators/Documents/World-Health-Survey-Saudi-Arabia.pdf.
23. Alqurashi KA, Aljabri KS, Bokhari SA. Prevalence of diabetes mellitus in a Saudi community. Ann Saudi Med. 2011;31(1):19–23. doi:10.4103/0256-4947.75773
24. Al Eid AJ, Alahmed ZA, Al-Omary SA, Alharbi SM. RASHAKA Program: a collaborative initiative between Ministry of Health and Ministry of Education to control childhood obesity in Saudi Arabia. Saudi J Obes. 2017;5(1):22–27.
25. Abdelrahman. Sports boulevard project. الهيئة الملكية لمدينة الرياض; 2020. Available from: https://www.rcrc.gov.sa/en/projects/sports-boulevard-project.
26. Jee SH, Foong AW, Hur NW, Samet JM. Smoking and risk for diabetes incidence and mortality in Korean men and women. Diabetes Care. 2010;33(12):2567–2572. doi:10.2337/dc10-0261
27. Wei X, Yu S EM, Yu S. A meta-analysis of passive smoking and risk of developing type 2 diabetes mellitus. Diabetes Res Clin Pract. 2015;107(1):9–14. doi:10.1016/j.diabres.2014.09.019
28. Hill J, Nielsen M, Fox MH. Understanding the social factors that contribute to diabetes: a means to informing health care and social policies for the chronically Ill. Perm J. 2013;17(2):67–72. doi:10.7812/TPP/12-099
29. Agardh EE, Sidorchuk A, Hallqvist J, et al. Burden of type 2 diabetes attributed to lower educational levels in Sweden. Popul Health Metr. 2011;9(1):60. doi:10.1186/1478-7954-9-60
30. Sacerdote C, Ricceri F, Rolandsson O, et al. Lower educational level is a predictor of incident type 2 diabetes in European countries: the EPIC-InterAct study. Int J Epidemiol. 2012;41(4):1162–1173. doi:10.1093/ije/dys091
31. Ramachandran A, Snehalatha C, Yamuna A, Mary S, Ping Z. Cost-effectiveness of the interventions in the primary prevention of diabetes among asian Indians: within-trial results of the Indian diabetes prevention programme (IDPP). Diabetes Care. 2007;30(10):2548–2552. doi:10.2337/dc07-0150
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.