Back to Journals » Open Access Journal of Contraception » Volume 14
Socio-Ecological Analysis of Barriers to Access and Utilization of Adolescent Sexual and Reproductive Health Services in Sub-Saharan Africa: A Qualitative Systematic Review
Authors Sidamo NB ![]() , Kerbo AA
, Kerbo AA ![]() , Gidebo KD
, Gidebo KD ![]() , Wado YD
, Wado YD
Received 5 April 2023
Accepted for publication 19 June 2023
Published 26 June 2023 Volume 2023:14 Pages 103—118
DOI https://doi.org/10.2147/OAJC.S411924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Negussie Boti Sidamo,1,2 Amene Abebe Kerbo,1 Kassa Daka Gidebo,1 Yohannes Dibaba Wado3
1School of Public Health, College of Health and Medicine Sciences, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3African Populations and Health Research Center, Nairobi, Kenya
Correspondence: Negussie Boti Sidamo, Email [email protected]
Background: In sub-Saharan African countries (SSA), despite the efforts to enable adolescents to access sexual and reproductive health (SRH) services, there are limited systematic review studies that comprehensively synthesize barriers to accessing services using a social-ecological model. Therefore, this review was conducted to fill this gap.
Methods: This study protocol was registered in the PROSPERO database (CRD42022259095). We followed PRISMA guideline to conduct this review. PubMed, Google Scholar, Embase and African Journal Online databases were used. Two authors individually screened articles. Only qualitative articles published in the English in last 10 years were included in this review.
Results: From the total of 4890 studies, 23 qualitative studies fulfilled the eligibility criteria. Those studies were from 11 SSA countries. This review finding revealed that inadequate information about the services, the incorrect perception about services, low self-esteem, fear of being noticed by family members, and financial constraints are barriers at the intrapersonal level. Unsupportive families and lack of open communication between adolescent-parent about sexuality issues were interpersonal barriers to access. Lack of provider competency, provider attitude, an unsupportive environment, physical inaccessibility of services, and shortage of medicine, and supplies were identified as institutional-level barriers. Moreover, community-level barriers like community stigma, social, religious, and gender norms within the society were identified as the main barriers to accessing services for adolescents.
Conclusion: This review finding reveals that the main barriers to access SRH services for adolescents living in SSA are misperception about services, low self-esteem to access services, financial constraints, unsupportive families, community stigma and social norms, unsupportive environments in health facilities, healthcare provider behavior, poor competency, being judgmental attitude, and breaking privacy and confidentiality. This study finding calls for new approach like a multi-pronged that works with service providers, with community, with families, and with adolescent to improve SRH services utilization of adolescent.
Keywords: adolescents, qualitative systematic review, sexual and reproductive health services, barriers, sub-Saharan Africa, socio-ecological model
Introduction
The World Health Organization (WHO) defines adolescent as an individual aged from 10 to 19 years.1 This age is the period in which most individuals become sexually active.2 It is also called the critical period for tackling trajectories of health inequities across the life course.2 The behavioral patterns develop at this age have an impact on their future life health status.3,4
Globally likewise in SSA countries, meeting the growing needs of adolescents and making SRH services accessible is one of the priority areas.5 Ensuring universal access to services is one of the focus targets of the SDG (target 3.7 and target 5.6).6 According to Guttmacher– Lancet Commission, SRH services package includes the widely known components of SRH, including maternal and newborn care, contraceptive services, and prevention and treatment of HIV/AIDS along with the less commonly recognized components of SRH like comprehensive sexuality education; care for STIs; safe abortion services; prevention, counseling and detection for gender-based violence; prevention, detection and treatment of infertility and cervical cancer; and counseling and care for sexual health and well-being.7 The Nairobi Summit (ICPD+25) also emphasized that the importance of these essential packages of SRH services packages should be provided across comprehensive life course approach to realizing choices and rights for all.8 Access and utilization of adolescent SRH services are essential to guarantee universal access to services.
Despite this, adolescents encounter different barriers to accessing SRH services.1,9,10 For instance, the finding of qualitative studies identified the attitude of healthcare providers,11,12 lack of confidentiality and privacy during services provision,13,14 negative cultural attitudes to premarital sex,15 social stigma towards the use of contraceptives before marriage,16 religious norms,16,17 and inadequate information about SRH services.14,18,19 However, there are limited published research evidences that comprehensively synthesized barriers adolescents faced to accessing SRH services using SEM.
In this study, the SEM was employed to systematically summarize barriers adolescents face to access and use SRH services. Using SEM is important to recognize multiple barriers, including barriers that operate at the individual, interpersonal, institutional, and community levels.20 Evidence shows that SEM has shown remarkable outcomes in attempting to prevent a range of public health issues.21 Thus, for a deeper understanding of persisting barriers to support efforts to ensure no adolescent is left behind, a qualitative systematic review using this SEM was required. It helps bring together research evidence to help inform our practice and help us understand what works.22,23 Therefore, this systematic review study aims to comprehensively synthesize the views and experiences of adolescents about barriers to accessing SRH services in SSA. Understanding these barriers can be useful to develop new strategies that can address those barriers and help bring SRH services closer to adolescents.
Research Question
What are the barriers reported by adolescents to access sexual and reproductive health services in SSA?
Objectives
The main objective of the current review was synthesises qualitative literatures to understand adolescents' perspectives and experiences regarding barriers to accessing SRH services in sub-Saharan Africa.
Methods
This study protocol was registered in the PROSPERO database (CRD42022259095). No prior studies were found on the topic of interest that has been registered in this database. Progress updates were documented periodically. This systematic review was done following PRISMA guideline for reporting systematic reviews.24 Following PRISMA guidelines, the selection of studies was systematically conducted and displayed using a PRISMA flow diagram (Figure 1).
 |
Figure 1 PRISMA flow diagram describes the selection of studies for a systematic review of barriers to access and utilization of adolescent sexual and reproductive health services in sub-Saharan Africa, 2023. Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–11. doi:10.1186/s13643-021-01626-4.24 |
Inclusion and Exclusion Criteria for Considering Studies for This Review
Types of Studies
All qualitative studies published in English within the last 10 years from December 2012 up to December 2022 were eligible for this systematic review. The inclusion of only qualitative studies was to generate evidence that is built on people’s views and experiences, acknowledging the rich context and different dimensions of the barriers from the participants’ perspective. This is important to inform and more effectively influence policy and practices on adolescent SRH services. The review included only peer-reviewed articles. Gray literature, systematic review studies, conference abstracts, and letters to editors, and the study protocol were excluded.
Types of Population
We used the WHO definition of adolescents, those adolescent individuals aged 10 to 19 years as the target population. We also included studies that were conducted among young people (10–24), if the majority of participants are adolescents aged 10 to 19 years. However, those studies that were focused on the general or adult population were excluded from the study.
Types of Intervention
In the current review, adolescent SRH services are viewed as those services identified as essential packages of adolescents’ SRH services. This definition was adapted from ICPID+25 years.25 Specifically, those services include modern contraceptives, prevention and treatment of sexually transmitted infections (STIs) including HIV infection and safe abortion services.
Outcomes of Interest
The outcome of interest for this systematic review includes the actual and perceived barriers or challenges adolescents face in accessing SRH services.
Setting
Any qualitative studies are conducted in any country in SSA (according to the World Bank definition of SSA)26 and involving either male or female adolescents. However, those studies conducted in humanitarian settings were excluded from the study.
Search Strategy
To search literature, we used four online databases like PubMed, African Journal Online, Embase, and Google Scholar. Also, manual searching of references was done. Forward and backward citation of reference tracking was done to find any relevant studies not included in the databases. In addition, reference lists of highly relevant articles were checked, and snowballing of references was performed. The first author initially developed search strategy, then shared it to all research team. The search strategy was design using setting (SSA), perspective (adolescent 10–24 years of age), a phenomenon of interest (perceived or actual barriers to access SRH services) and evaluation (themes identified from original qualitative research). All research teams were meeting periodically, to develop the strategy iteratively. For each database, we used appropriate key terms, with the combination of MeSH terms using Boolean operators “AND” and “OR” running key search topics. The following keywords were used: ((Adolescents) AND (Sexual health services) OR (Reproductive health services)) OR (Adolescents friendly health services) OR (Sexual and reproductive health services) AND (construct* OR challenge* OR barrier OR Socio-ecological model OR Framework* OR qualitative study) AND (Sub-Saharan Africa). An updated search was performed in February 2023 to ensure the inclusion of relevant publications since the initial search Supplementary Tables 1–4.
Study Selection
After conducting comprehensive literature search, all eligible articles were exported into Endnote software and duplicate studies were removed before starting the review. A three-stage screening strategy was applied. The first stage was title screening. The second stage was abstract screening. An abstract screening was done for all potential studies. Evidence also shows that abstract screening helps to threaten the validity of the identified studies by reducing the potential bias.27 Once titles and abstracts have been screened, full‐text screening was followed. All potential studies were independently screened by research members (NBS and YDW). Discrepancies were resolved via discussion with the wider research teams.
Data Extraction
Standardized Joanna Briggs Institute (JBI) data extraction tool prepared in the Excel spreadsheet was used to extract the data from the included articles. The Excel spreadsheet was shared with all authors to determine the variables to extract and themes to be extracted to answer the research question and objective. The first author has undertaken data extraction. The third author (KDG) checks each day the extracted data. The other research team double-checked the extracted data subsample of papers to check the accuracy. To resolve discrepancies continuous discussions were done. The name of first authors with publication year, aim of study, study area, participants, data analysis approach, key finding, summary of quotations and author conclusions were extracted from each included study. Outcomes were perceived barriers or actual barriers to access SRH services. We further determined whether the outcomes assessed were intrapersonal, interpersonal, institutional, and community level barriers.
Quality Appraisal
The quality of all studies selected for the final synthesis was evaluated using JBI checklist for qualitative research appraisal tool.28 JBI checklist had 10 criteria,28 each study assessed by those criteria. Each questions a score one if it is evidenced in the paper and zero otherwise, producing a total score from 0 to 10. Then, the overall quality of the studies were classified as high quality study (scores of 8–10 out of 10); moderate quality study when scored (4–7 out of 10); and low quality study (0–3 out 10).28 Two reviewers (NBS and AAK) conducted quality assessment independently. Resolving disagreements between the reviewers was resolved through discussion.
Synthesised Findings
A deductive approach was used to systematically summarize the finding using a socio-ecological framework to guide synthesis. The priori-defined framework constructs were used to code data. A verbatim quotation from study participants as well as author interpretations on barriers to access services was extracted. The overall analysis process followed five steps: such as coding data from the selected articles, then categorizing the codes based on shared meaning. All codes that had similar meanings were rearranged and overlapping themes were merged. Then further categorize these groups and summarize them. Finally, the emerging themes in line with the research questions of the study were summarized using a socio-ecological framework. Participant quotations were included as a support for themes. The first author performed synthesis of the data; the reaming research team double-checked the final categories, sub-categories, and synthesis statements. Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) guidelines were used to report the synthesis of included studies.29
Results
Study Selection and Characteristics
A total of 4890 articles were identified (4854 articles were identified through a database search and an additional 36 articles were from other sources). At the screening stage, titles and abstracts were screened, and records are included or excluded according to the inclusion criteria. At the eligibility stage, full-text published articles were assessed to include in the review, and those with reason to be excluded are excluded. Inclusion stage of the remaining studies was included. After the full-text screening, 23 qualitative articles met the eligibility criteria and were included in the final review. The PRISMA flow diagram summarizes this process (Figure 1).
Characteristics of the Selected Studies
From the total identified studies, only 23 qualitative articles were included in this synthesis. Those studies were from 11 countries in SSA. Of those 23 articles, four of them were from South Africa, two of them from Ethiopia, three from Kenya, two from Tanzania, two from Nigeria, three from Ghana, two from Uganda, one from Malawi, two from Zambia, one from Guinea and one from Senegal. The characteristics of the articles are summarized in table (Supplementary Tables 1–4).
Quality Appraisal Results
The quality of each paper was evaluated using the 10 criteria of JBI Critical Appraisal checklist.28 From the total 23 articles, 21.74% (5 articles) rated as moderate quality articles and the remaining 78.26% (18 articles) rated as high quality articles. From the 10 domains, all 23 studies scored “Yes” (present) for six domains which covered issues linked to correct methodology employed; statements about research methodology and question; representation of data and analysis; interpretation of results; representation of participant voices; and conclusions flowing from data interpretation and analysis. From the total 23 research articles, 15 studies (not report the theoretical framework they used), five articles (not report statements that accounted for the influence of the authors on the research itself), and two articles (do not report evidence of ethical approval by an appropriate body).11,30 A philosophical perspective was not reported in all 23 studies. Critical appraisal in qualitative studies lacks agreement on exclusion of articles based on their quality and the potential impact of excluding eligible articles on review outcomes.31 So, no research articles were excepted from the review based on the quality of the articles. For these reasons, the team adopted an inclusive approach to critical appraisal, using the appraisal process to enable an in-depth understanding of each study. A summary of quality assessments is provided as (Supplementary Tables 1–4).
Finding
The finding of this qualitative review synthesis is summarized and presented by the level of the socio-ecological framework (intrapersonal or individual, interpersonal, community, and institutional level barriers) and supported with participants’ quotations as well as authors’ interpretations from included references (reference, country, and population). Participants’ direct quotations were presented in statements (quotes) that appear in italics to easily distinguish them from the authors’ interpretations. To enrich readability, any words removed from a quote are shown by ellipses (…), and added words are provided in square brackets.
Barriers at the Intrapersonal (Individual) Level
Lack of Information About Sexual and Reproductive Health Services
Out of 23 studies, 6 studies report that lack of information about SRH services is the main barrier to accessing SRH services.13,17,18,32–36 A respondent from one Nigeria study noted,
Some of them (adolescents) are not aware of contraceptives and those aware don’t know where to get it from or which one will be good for them.13
Similarly, respondents from one Ethiopia study describe that
I don’t know which health facilities provide SRH service. No one informs [tell] us what SRH service is being provided at the different health facilities. For instance, I want to know my HIV status. But, I don’t know whether health facilities provide the service without special reason e.g. blood transfusion or as a precondition for marriage.32
Adolescent Low Self-Esteem
Findings from studies identified that certain behaviors of the adolescents like low self-esteem and lack of confidence to seek adolescent SRH services were among the barriers to seeking SRH services. They were also perceived to be too shy to openly discuss contraception with health workers.13,17,18 A respondent from one Ghana study noted
Before I visited the adolescent clinic, I was afraid that the nurses would not be comfortable discussing sex-related issues with me. But after visiting the adolescent clinic that negative thinking disappeared. There are ‘young’ people like me in the community who have similar perceptions.18
Adolescent Perception Towards Sexual and Reproductive Health Services
The finding of the study conducted in Rwanda, Ethiopia, South Africa, and Malawi also shows that adolescents’ perceptions are among the identified barriers to accessing the SRH services.16,37 Authors from one of the study conducted in Rwanda also confirm that most adolescents perceived that only adults are supposed to use the SRH services.16
Fear of Been Seen by Family or Relatives
Most studies commonly reported fear of adolescents being seen in the clinic for SRH services as a barrier for adolescents’ SRH services use.18,30,32,38,39 They would be able to visit SRH services without being seen by family relatives or other adults or by neighbors or teachers who would most likely tell their parents. A respondent from one South African study noted
… if anyone sees you in SRH clinic means they think that you have boyfriends or something like that.40
Another respondent from one Ghana study noted
Maybe when you go to the hospital, you know that somebody from your clan is there. So, you fear going there because they might find out and tell your parents.41
Financial Constraints
Qualitative study findings conducted in Ghana, Ethiopia (Southern), Nigeria (South East), Uganda (Kampala), and Kenya commonly identified direct and indirect costs like lunch or tea costs while spending for a day and transportation costs to come to the health facility for SRH services were also identified as barrier to access SRH services for adolescents.13,18,35,41,42 A respondent from one Nigeria study noted,
Adolescents may not have the fund for his/her medical expenses … … Most of the communities are far from health facilities.13
Similarly, respondent from one of the Guinea study noted,
… The financial problem of [young people’s] was a main barrier to access to modern contraceptive methods since these [modern contraceptive] methods are not free of charge. From condoms. implants cost more than 100,000 GNF ($10), the IUD is more expensive. you see they can’t afford it [buy].35
Barriers at the Interpersonal Level
Lack of Parental Support
Studies show that parents were reported to serve as truthful sources of information about SRH issues for adolescents.30,43 In most cases parents are a primary source of logistical and financial support to access SRH services by adolescents.30 However, the finding of studies conducted in Kenya (Kisumu and Kakamega), Ghana (Accra and Kumasi), Ethiopia (Southern), Nigeria (north-western), Ghana (Metropolitan Kumasi), Kenya (Homa Bay and Narok) shows that lack of parental support was the main barrier that affect access to SRH services by adolescents17,18,38,39,41,44 A respondent from one Kenya study noted,
Parents do not want to give their adolescents time to access this information, maybe because they feel it is not the right time.41
Another respondent from one Nigeria study mentioned,
I always want to come to the adolescent [SRH]clinic but if my parents find out that I[adolescent] come to the[SRH] clinic, they will beat me[adolescent] and warn me[adolescent] not to step foot here[SRH clinic] again. Because of that am always afraid to come to the adolescent clinic.17
Similarly, one parent from a Kenya study describes that
We tell them; sex is not for children. We tell them that there is a time for it, and this is not the time to have sex.44
One parent from Ethiopia study explained that:
… we (parents of adolescents) are advising them [adolescents] what is better for them [adolescents] was abstinence until them marriage…which is the only option to remain healthy for both males and females. The use of FP [family planning] is against our religion and culture that values abstinence and virginity. In our community[Ethiopia], no one advises his/her children [adolescents] to utilized SRH services. We [community members] have been advising this [abstinence] and will continue[advising abstinence] in the future.39
Poor Parent-to-Adolescent Communication About SRH Issues
Poor parent-to-adolescent communication of SRH issues was one of the interpersonal barriers to access and use of adolescent SRH services.32,35,39,41,45 In majority of SSA countries, SRH issues were rarely discussed at home due to social norm of the community, and they perceived that adolescents are as children and not as young adults.41 A respondent from one Ethiopia study noted,
My mother sometimes talks to me[adolescent girls] about menstrual hygiene; but, she [my mother] has never discussed to me birth control methods, sexually transmitted disease and other things that we are talking about now, but warning me not to get involved in sexual activity.32
Another respondent from Kenya study describes that,
she [my mother] only tells me to abstain to avoid all those, ‘I cannot take you for family planning because after I take you, you will know that you are protected from pregnancy but you won’t be safe, so you will be sure you cannot get pregnant and so you will not fear the diseases as well’. So they tell me to abstain.44
Barriers at Institutional Level
Barriers at institutional level are further classified into facility-related barriers and provider-related barriers. Facility-related barriers include an unsupportive environment, shortage of medicines and supplies, and inaccessibility of services, whereas the provider-related barriers include healthcare provider behaviors, poor provider competency, and attitude of the providers for adolescents.
Physical Inaccessibility of Sexual and Reproductive Health Services
Qualitative study findings conducted in Ethiopia (Southern and Southwest), Zambia (Kabwe District), Uganda (Kampala), and Kenya (Kisumu and Kakamega) reveal that physical inaccessibility of SRH services was identified as one of the barriers for adolescents to access SRH services.32,33,41,42 One adolescent from one Ethiopia study noted,
Even the nearest health facility is far from my home, I found it[accessing the health facility] tough to travel a longer distance and get SRH information and service. Imagine[severity of issues] what it meant spending several hours out of home for a girl living with her distant relatives.32
Shortage of Medicines and Supplies
The main health facility level barrier that was identified in many studies was stock-outs of preferred methods, shortage of medicine, and supplies like equipment and educational materials.13,17,18,33,34 One adolescent from one Ghana study noted,
The nurses tell me not to have sex without a condom. But sometimes, I …request condoms and the nurses will tell me that it is finished. I do not feel happy to hear that, especially when I want to have sex.18
Similarly, a respondent from one Zambia study noted,
The pills should always be available at the clinic, not whereby whenever you go there, they tell you that they are not available now and then. In the end, they even become rude to you and you also lose interest in going there.33
Unsupportive Environment
Most studies identified that an unsupportive environment like inconvenient operating hours, long waiting, inadequate physical space, and lack of separate rooms were a serious institutional level barrier.13,16–18,42,46 A respondent from one Ghana study noted,
….adolescent [SRH] clinic was open in the morning, but …… close in the afternoon. The adolescent [SRH] clinic is not open on holidays and weekends. ….I am a student and cannot leave my classes to visit[access] the adolescent[SRH] clinic.18
Similarly, a respondent from one Nigeria study noted,
Waiting for a long time in health center because of coming late of a doctor, I believed is a big challenge to get treatment. I[respondent] for one do not like it [staying for a long time]. I am sure most people do not also like it [coming late of a doctor] like me. If we keep experiencing this, it will make us not use the clinic. This one is a big problem.47
Authors from one Ghana study also confirm that, for multiple purposes, they used single rooms for instance they often used as a library and for consultation due to this reason inconveniences such as overcrowding, inadequate privacy, and poor ventilation were commonly observed.18 Another author from a study from Rwanda also shows that the lack of separate rooms for delivering SRH services to adolescents is barriers that influence access to adolescents’ SRH services.16
Healthcare Provider Behaviors
The main barrier identified by the majority of studies was unfriendly behaviors of healthcare providers and mistreatment.13,17,18,32–34,38,41,42,47 A respondent from one Zambia study noted,
To be frank [truthful] some healthcare providers are rude, very rude. That is the major complaint of adolescents. That is why even most women not go to health facilities [shun away], they prefer buying from drug stores in town instead of going to clinics.33
Another respondent from one Nigeria study noted,
Most medical providers are full of themselves. You can imagine my own experience. After I wait for over two hours, he only took 5 minutes to talk to me and call in the next person without doing a proper examination of me. This is what happens all the time you visit for consultations.47
Poor Provider Competency
Poor healthcare providers’ competency prevents adolescents from using SRH services.13,18,32–34,46,47 Scolding (reprimand) and excessive questioning of adolescents by a healthcare provider are indicators of poor provider competency. Findings of qualitative studies conducted in Tanzania (North-Western) and Zambia (Kabwe District) also describe that adolescents who ask for contraception or other SRH services would be met with rude treatment and healthcare providers’ reluctance to offer services related to “promiscuous” behavior’.33,46
Judgmental Attitude of the Provider
The finding of the studies shows that healthcare provider attitude towards adolescent who is seeking SRH services, besides the atmosphere at the healthcare facility is an important factor affecting adolescents’ access to and utilization of sexual and reproductive healthcare services.13,17,18,32,33,38,41,42,46,47 A respondent from one North-Western Tanzania study noted
She would be asked some questions … because she would be asked as she is too young to have those contraceptive pills …. If she says that she doesn’t have any child, she wouldn’t be given.46
Similarly, a respondent from one Ethiopia study noted
Let me share with you what my friend experienced when visiting SRH service. She went to a health care facility to take a modern contraceptive; but, the healthcare provider assigned at the time was emotional even unwilling to provide the contraceptive for her, criticizing that she was too young to have sex by that time.32
Lack of Privacy and Confidentiality
The commonly identified barrier related to healthcare providers was confidentiality breaches disrespect and discrimination of adolescents, which prevented adolescents from accessing SRH services.13,18,32,36,41,47 A respondent from one Nigeria study noted,
If my health situation is exposed to anybody including my parents, I will not be using such health personnel because I desire some privacy in my life. Nobody is supposed to know what my health condition is unless I volunteered to make it so.47
Similarly, a respondent from one Kenya study noted
The doctor reads your name out loudly in public and what you are suffering from. This may make you even leave and go back home.41
Barriers at the Community Level
Community Stigma
Qualitative study findings conducted in Ethiopia (Southwest), Ghana, Nigeria (north-western), central Uganda, and Kenya (Kisumu and Kakamega) identified the stigma from healthcare providers, community, and family as a constraint to accessing SRH services.30,32,36,41,46 In addition, negative name-calling, particularly for girls who are pregnant before marriage, was harsh.30,32,46 A respondent from one Ethiopia study noted,
When I think of visiting a health care facility for SRH reasons, the thing that comes into my mind is what the community talk behind me. …. once the community defames[libel] you; it is really difficult to convince people who you are.32
Similarly, a respondent from one Kenya study noted,
if you are seen going to the hospital, it’s like you’re engaging in sex. So, society will have a particular perception of you.41
Community Attitude
Community attitudes, such as rumors of prostitution, for adolescents who access sexual health services also hinder adolescents from accessing SRH services.13,18,39,46 For instance, most community members believed that SRH services was for married and young adults and it was unacceptable, and the behavior of bad girls if unmarried access the services. This kind of community attitude further challenges access to adolescent SRH services. Due to this reason, most adolescents did not want … to be seen around SRH clinics due to the association of adolescents’ SRH services with sexual activities, which were sometimes labeled as “bad manners.”41 A respondent from one Ghana study noted,
People in this [the place they live] community think negatively of adolescents who visit the [SRH Clinic]. They think we [adolescents] come here [health facility] to do abortions or collect condoms. Because of that I do not want people to see me[adolescent] when am coming to the SRH clinic. They[community members] may think am coming for a pregnancy test or an abortion and may call me a bad girl18
Adolescent from Ethiopia study explained that
I had sexual intercourse while I was in grade eight. I did not expect that I would be pregnant. … I went to a nearby town for pregnancy confirmation in a private SRH clinic. I was told that it was pregnancy and it is late for termination [to do safe abortion] so that I should give birth. When my belly [abdomen] grows, people began to whisper at me, thus, I dropped out of school. … When my mom noticed my status, she shouted at me. All family members felt sad and ignored me. … that was unforgettable bad event in my life.39
Religious Norms
Findings from the study conducted in Ethiopia (Southwest) reveal that adolescents’ SRH service utilization behavior is heavily influenced by the cultural and religious norms of the community they [adolescent] live in.32,35,39 Other study findings conducted in Nigeria (north-western) and Zambia (Kabwe District) also reveal that religious norms as the most significant barriers that affected adolescents’ access to and utilization of SRH services as well as the main barrier to the provision of adolescents’ SRH information and services.17,33 One adolescent from one Ethiopia study describes,
I am[respondent] an orthodox Christian, according to our faith, the use of artificial birth control method is considered as sinning the law of ….God.32
Another adolescent from one Nigeria study mention,
Like cases like contraceptives, the religion [Islam] does not allow it [the use of contraceptives], … or as an adolescent, you[healthcare provider] bring up the issue of contraceptives, and they will say you are spoilt [immoral], where did you learn it from?17
Social Norms
The finding of studies conducted in Nigeria (north-western), Ethiopia (Southwest), Zambia (Kabwe District), Rwanda, Ghana, and Kenya describes the social norm related to premarital sex as a constraint to accessing SRH services by adolescents.16,17,32,33,35,38,41 Most studies show that using adolescent SRH services, premarital sex, and childbirth are socially unacceptable for unmarried adolescents. This leads to serious challenges for adolescents as it leads to stigma and embarrassment due to community condemnation of premarital sex.30,32 One study finding from Rwanda and Ethiopia found that marriage was considered a prerequisite to accessing and utilizing SRH services and married adolescents were seen as young adults.45 Another study finding from a study conducted in Ghana describes that marriage was considered a prerequisite to access and utilize SRH services.30 Adolescents from Ethiopia study explained that:
As premarital sex is taboo in the locality, pregnancy/STIs keep secret. Because the prevailing norm does not accept this behavior. … there are instances that some girls had unwanted delivery while SRH services are available in the locality.39
Gender Norms
Findings from Tanzania (North-Western) show that adolescent girls who experienced unplanned pregnancies will be socially as well as physically isolated from their peers.46 The study from Uganda explained that men do not want to marry women who have already given birth. Most adolescents explain that they would be more comfortable sharing their SRH issues with a young and female healthcare provider.13,32,41
Theoretical Framework
Social-ecological model was used as a theoretical framework to guide data synthesis. This is due to its holistic future that helps to guide the overall structure of evidence in the existing literature. This framework provides the opportunity to address the dynamic and complex nature of human development during adolescence, and the dynamic interrelationship between adolescents and their environment. This framework helps to recognize the influences of multiple barriers that influence adolescents’ health behaviors and outcomes including barriers that operate at the individual (intrapersonal), community, interpersonal, and institutional levels. The interaction between adolescents with the environment which takes place at the individual, interpersonal, institutional or community levels of this framework helps to identify the interacting effect of different barriers which may be a source of weakness and strength in accessing SRH services. Evidence generated using this holistic model like SEM may help to design interventions and strategies that address barriers at multiple levels may be more effective than those that address only one level which is curial to improve adolescents’ access and utilization of SRH services for future interventions. We used the Blum et al48 conceptual framework for early adolescence,48 which is building on Bronfen brenner’s SEM.20 This theoretical framework illustrates that personal behaviors and attitudes are influenced by different barriers across different interacting domains at different levels: community, institutional, interpersonal, and intrapersonal level.49 The finding of this systematic review is summarized by using an adapted version of SEM (Figure 2).
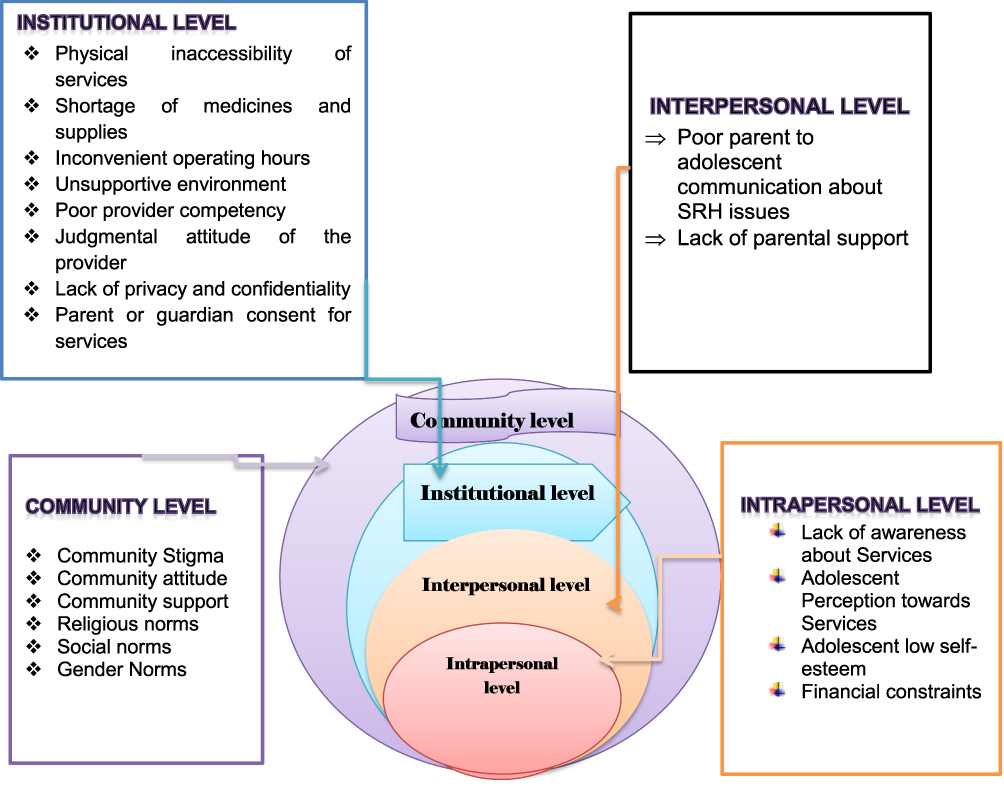 |
Figure 2 Summary of the finding using socio-ecological framework for a systematic review of barriers to access and utilization of adolescent sexual and reproductive health services in sub-Saharan Africa, 2023. |
Discussion
This systematic review finding highlights how barriers at intrapersonal level, interpersonal level, institutional level and community level interact to influence adolescents’ experiences to access services. At the individual or intrapersonal level, inadequate information about SRH services, fear of being seen by other family members, adolescents’ perception towards SRH services, adolescents’ low self-esteem, and financial constraints are the main barriers that affect access to adolescent SRH services in SSA. The findings of this review were consistent with previous review studies50–52 and qualitative studies conducted outside SSA.4,53 The implication of this finding is the need to address these types of barriers urgently.
At interpersonal level, poor adolescent to parental discussion about sexuality issues and lack of support from parents/caregivers were barriers identified at interpersonal level. The findings of this review were consistent with qualitative studies conducted outside SSA4,53 Another qualitative study finding, also show that lack of parental support to use modern contraceptive services has been a long-standing challenge to increase modern contraceptive uptake among adolescents.54 This study finding implies the need for parental or care givers of adolescent engagement in SRH services provision. Therefore, designing interventions focusing parental or caregiver support may be a promising approach.
At community level, community attitude and stigma, social and religious norms, and gender norms within the society were identified as the community level barriers to accessing services for adolescents. The findings of this review were consistent with previous research finding on the barriers to adolescent’s SRH services in other contexts outside of SSA.15 The finding of this study implies that the current SRH services provision is not in line with social and religious norms of most community. Making SRH services provision in line with social and religious norm by involving community elders, religious leaders, community leaders, community volunteers and parents or caregivers of adolescents, and teachers is urgently needed. Also, the finding implies that the need of identify available social and religious norms related to adolescent SRH services may be important.
Barriers at institutional level like unsupportive environment (inconvenient operating hours, inadequate physical space, long waiting times, long distances to reach healthcare facilities), and out-of-stock preferred methods were well-identified barriers in most included studies. Qualitative study findings conducted in high-income and middle-income countries support this study finding.4,15 Other systematic review studies also support our finding.55,56
Barriers at provider level were identified as hidden barriers to access SRH services for adolescents. Most included studies identified that healthcare provider behavior, poor provider competency, judgmental attitude of the provider, and breaking privacy and confidentiality were barriers that further discourage adolescents from accessing and utilization of SRH services. Previous systematic review studies were also supported this finding.55–57 This study finding implies that the need for urgent intervention to remove hidden barriers to access SRH services is needed.
In conclusion, the finding of this review shows that to access SRH services adolescents living in SSA faced a myriad of barriers at intrapersonal level (misperception about services, low self-esteem to access services and financial constraints), interpersonal level (unsupportive families), community level (community stigma and social norms), health facility level (unsupportive environments in health facilities), and provider level barriers (healthcare provider behavior, poor provider competency, judgmental attitude of the provider, and breaking privacy and confidentiality).
Strengths and Limitations of the Review
This review is not without limitations. First, limitation of the study, we did not differentiate the identified barriers between urban versus rural areas. Future study may consider to differentiate the barriers for urban versus rural areas. This review may have publication bias because we only included qualitative study publication on four databases in English language in the last 10 years. This may lead loose of essential data from unpublished sources and those not in English. Despite these limitations, we follow a rigorous and systematic approach like registered in the protocol in PROSPERO database, PRISMA guideline, PRISMA 2020 statement, standardized JBI data extraction tool and the use of a qualitative research appraisal checklist. We used conceptual thematic analysis to re-categories the barriers reported by the studies into major themes, sub-themes, and their respective codes. Two members of the research team who independently performed screening which will help to ensure the trustworthiness of the themes and sub-themes. The reviewers compared and decided upon the articles to be retained for final review after discussing and coming to a consensus. The finding from this review offers useful evidence to meet SDGs, as it highlights the positive aspects that can be further strengthened, as well as areas that need to be targeted and improved for better SRH services uptake. In most studies, researchers did not clearly state their influences in the study, and this may negatively influence the accuracy and rigor of the findings. The data drafting and synthesis of this paper are led by the first author, Ph.D. fellow, who may be influenced by interpretivism and realism. To maintain reflexivity, the team discussions were conducted at each step.
The Implication of the Finding of the Study
The finding of this study implies that barriers to access SRH services were beyond the adolescent, but their parents, community and institution play a great role. The finding calls for new approach like a multi-pronged that works with service providers, with community, with families, and with adolescent to improve SRH services utilization of adolescents. At individual levels, empowering adolescents to increase their self-esteem and their confidence to make decisions. At the interpersonal level, designing a parental center intervention to straighten parental support and promote communication about sexuality within their families. At the community level, a strong community-based movement brings together multiple stakeholders to support adolescent SRH services utilization and remove the social norms and stigma linked with adolescent SRH services uptake. To improve the institutional level barriers, making health facilities adolescents friendly by shorting waiting times, making operating hours convenient for adolescents, creating a safe space for adolescents, and available preferred SRH services types for adolescents. In addition, strengthening supportive supervision and providing training for service providers to provide SRH services based on adolescents’ needs and preferences, and without judgment. Also, more study that addresses the bottlenecks and innovative solutions to access and provision of SRH services focuses on interpersonal and policy-level barriers by including adolescents themselves, family members, and their immediate environment perspectives. For policy and practice, the finding of this study would help governmental organizations, non-governmental organizations, and international agencies to formulate and implementation of interventions to best address the SRH problems of adolescents. Specifically, the finding of this study helps to enhance service supply to adolescents. In sum, the results will help policymakers to assess acceptability and effectiveness of adolescent SRH services before any decision to scale it up or not. For future researchers, the finding of the study will contribute to knowledge on adolescent SRH services and serve as a guide for future researchers interested in adolescent health study.
Abbreviations
ENTREQ, Enhancing Transparency in Reporting the Synthesis of Qualitative Research; JBI, Joanna Briggs Institute; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; SDGs, Sustainable Development Goal; SEM, socio-ecological model; SRH, Sexual and Reproductive Health; SSA, Sub-Saharan Africa; STIs, Sexual Transmitted Infections; WHO, World Health Organization.
Data Sharing Statement
The data used to support the findings of this study are fully available without any restriction from the corresponding author.
Acknowledgments
The abstract for this paper was presented at the 33rd EPHA annual conference. The abstract is online: (https://etpha.org/conference/index.php/33rdConference/33rdConference/paper/view/3426). Both Wolaita Sodo University and Arba Minch University have no role in the design of the study, collection, analysis, and interpretation of the data, and in writing the manuscript.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. World Health Organization, WHO recommendations on adolescent sexual and reproductive health and rights; 2018.
2. Stierman EK, Kalbarczyk A, Oo HNL, et al. Assessing barriers to effective coverage of health services for adolescents in low-and middle-income countries: a scoping review. J Adolesc Health. 2021;69(4):541–548. doi:10.1016/j.jadohealth.2020.12.135
3. Napit K, Shrestha KB, Magar SA, et al. Factors associated with utilization of adolescent-friendly services in Bhaktapur district Nepal. J Health Popul Nutr. 2020;39(1):1–9. doi:10.1186/s41043-020-0212-2
4. Hayrumyan V, Grigoryan Z, Sargsyan Z, et al. Barriers to utilization of adolescent friendly health services in primary healthcare facilities in Armenia: a qualitative study. Int J Public Health. 2020;65(8):1247–1255. doi:10.1007/s00038-020-01499-9
5. Chandra-Mouli V, Neal S, Moller A-B. Adolescent Sexual and Reproductive Health for All in Sub-Saharan Africa: A Spotlight on Inequalities. Springer; 2021.
6. Sundewall J, Kaiser H. Sexual and reproductive health and rights:: an essential element of universal health coverage. Background document for the Nairobi Summit on ICPD25-accelerating the promise; 2019.
7. Starrs AM, Ezeh AC, Barker G, et al. Accelerate progress—sexual and reproductive health and rights for all: report of the Guttmacher–Lancet Commission. Lancet. 2018;391(10140):2642–2692.
8. UNFPA. Accelerating the promise: the report on the Nairobi Summit on ICPD25. New York: UNFPA; 2020.
9. World Health Organization. Handbook for conducting an adolescent health services barriers assessment (AHSBA) with a focus on disadvantaged adolescents: knowing which adolescents are being left behind on the path to universal health coverage, and why. World Health Organization; 2019.
10. World Health Organization. Leave no one behind: strengthening health systems for UHC and the SDGs in Africa; 2017.
11. Mbeba RM, Mkuye MS, Magembe GE, et al. Barriers to sexual reproductive health services and rights among young people in Mtwara district, Tanzania: a qualitative study. Pan Afr Med J. 2012;13(Suppl 1):1.
12. Manguro G, Mwaisaka J, Okoro D, et al. Failing the rights: sexual vulnerability, access to services and barriers to contraceptives among adolescents in Narok County, Kenya. Int J Hum Rights Healthc. 2021;14:374–386. doi:10.1108/IJHRH-11-2020-0099
13. Ezenwaka U, Mbachu C, Ezumah N, et al. Exploring factors constraining utilization of contraceptive services among adolescents in Southeast Nigeria: an application of the socio-ecological model. BMC Public Health. 2020;20(1):1–11. doi:10.1186/s12889-020-09276-2
14. Onasoga OA. Challenges and barriers to adolescents’ post-abortion care services: implications for reproductive health policy in Nigeria; 2017.
15. Thongmixay S, Essink DR, Greeuw TD, et al. Perceived barriers in accessing sexual and reproductive health services for youth in Lao People’s Democratic Republic. PLoS One. 2019;14(10):e0218296. doi:10.1371/journal.pone.0218296
16. Ndayishimiye P, Dine RD, Dukuze A, et al. Perceptions and barriers toward sexual reproductive health services accessibility, availability and quality among adolescents in selected cities of Rwanda; 2020.
17. Mohamed S, Nmadu AG, Usman NO. Barriers to adolescents’ access and utilisation of reproductive health services in a community in north-western Nigeria: a qualitative exploratory study in primary care. Afr J Prim Health Care Fam Med. 2020;12(1):1–8.
18. Abuosi AA, Anaba EA. Barriers on access to and use of adolescent health services in Ghana. J Health Res. 2019;33(3):197–207. doi:10.1108/JHR-10-2018-0119
19. Decker MJ, Atyam TV, Zárate CG, et al. Adolescents’ perceived barriers to accessing sexual and reproductive health services in California: a cross-sectional survey. BMC Health Serv Res. 2021;21(1):1–12. doi:10.1186/s12913-021-07278-3
20. McLeroy KR, Bibeau D, Steckler A, et al. An ecological perspective on health promotion programs. Health Educ Q. 1988;15(4):351–377. doi:10.1177/109019818801500401
21. Odimegwu CO, Ugwu NH. A multilevel mixed effect analysis of neighbourhood and individual level determinants of risky sexual behaviour among young people in South Africa. Reprod Health. 2022;19(1):119. doi:10.1186/s12978-022-01407-9
22. Seers K. Qualitative systematic reviews: their importance for our understanding of research relevant to pain. Br J Pain. 2015;9(1):36–40. doi:10.1177/2049463714549777
23. Butler A, Hall H, Copnell B. A guide to writing a qualitative systematic review protocol to enhance evidence‐based practice in nursing and health care. Worldviews Evid Based Nurs. 2016;13(3):241–249. doi:10.1111/wvn.12134
24. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):1–11. doi:10.1186/s13643-021-01626-4
25. Berhan Y, Ali M, Tassew A, et al. Universal health coverage policy and progress towards the attainment of universal sexual and reproductive health and rights services in Ethiopia. Ethiop J Health Sci. 2022;32(1):181–200. doi:10.4314/ejhs.v32i1.19
26. World Bank. World bank country and lending groups-2021; 2021.
27. Polanin JR, Pigott TD, Espelage DL, et al. Best practice guidelines for Abstract screening large‐evidence systematic reviews and meta‐analyses. Res Synth Methods. 2019;10(3):330–342. doi:10.1002/jrsm.1354
28. Lockwood C, Munn Z, Porritt K. Qualitative research synthesis: methodological guidance for systematic reviewers utilizing meta-aggregation. JBI Evid Implement. 2015;13(3):179–187.
29. Tong A, Flemming K, McInnes E, et al. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012;12:181. doi:10.1186/1471-2288-12-181
30. Challa S, Manu A, Morhe E, et al. Multiple levels of social influence on adolescent sexual and reproductive health decision-making and behaviors in Ghana. Women Health. 2018;58(4):434–450. doi:10.1080/03630242.2017.1306607
31. Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020;1(1):31–42. doi:10.1177/2632084320947559
32. Hailemariam S, Gutema L, Agegnehu W, et al. Challenges faced by female out-of-school adolescents in accessing and utilizing sexual and reproductive health service: a qualitative exploratory study in Southwest, Ethiopia. J Prim Care Community Health. 2021;12:21501327211018936. doi:10.1177/21501327211018936
33. Silumbwe A, Nkole T, Munakampe MN, et al. Community and health systems barriers and enablers to family planning and contraceptive services provision and use in Kabwe District, Zambia. BMC Health Serv Res. 2018;18(1):1–11. doi:10.1186/s12913-018-3136-4
34. Mukanga B, Nkonde H, Daka V. Exploring the multilevel factors influencing women’s choices and utilisation of family planning services in Mufulira district, Zambia: a socio-ecological perspective. Cogent Public Health. 2023;10(1):2168589. doi:10.1080/27707571.2023.2168589
35. Dioubaté N, Manet H, Bangoura C, et al. Barriers to contraceptive use among urban adolescents and youth in Conakry, in 2019, Guinea. Front Glob Womens Health. 2021;2021:42.
36. McGranahan M, Bruno-McClung E, Nakyeyune J, et al. Realising sexual and reproductive health and rights of adolescent girls and young women living in slums in Uganda: a qualitative study. Reprod Health. 2021;18(1):1–11. doi:10.1186/s12978-021-01174-z
37. Schriver B, Meagley K, Norris S, et al. Young people’s perceptions of youth-oriented health services in urban Soweto, South Africa: a qualitative investigation. BMC Health Serv Res. 2014;14(1):1–7. doi:10.1186/s12913-014-0625-y
38. Amankwaa G, Abass K, Gyasi RM. In-school adolescents’ knowledge, access to and use of sexual and reproductive health services in Metropolitan, GhanaKumasi. J Public Health. 2018;26(4):443–451. doi:10.1007/s10389-017-0883-3
39. Munea AM, Alene GD, Debelew GT, et al. Socio-cultural context of adolescent sexuality and youth friendly service intervention in West Gojjam Zone, Northwest Ethiopia: a qualitative study. BMC Public Health. 2022;22(1):1–11. doi:10.1186/s12889-022-12699-8
40. Jonas K, Roman N, Reddy P, et al. Nurses’ perceptions of adolescents accessing and utilizing sexual and reproductive healthcare services in Cape Town, South Africa: a qualitative study. Int J Nurs Stud. 2019;97:84–93. doi:10.1016/j.ijnurstu.2019.05.008
41. Mutea L, Ontiri S, Kadiri F, Michielesen K, Gichangi P. Access to information and use of adolescent sexual reproductive health services: qualitative exploration of barriers and facilitators in Kisumu and Kakamega, Kenya. PLoS One. 2020;15(11):e0241985. doi:10.1371/journal.pone.0241985
42. Ahumuza SE, Matovu JK, Ddamulira JB, et al. Challenges in accessing sexual and reproductive health services by people with physical disabilities in Kampala, Uganda. Reprod Health. 2014;11(1):1–9. doi:10.1186/1742-4755-11-59
43. Mehus CJ, Aldrin S, Steiner RJ, et al. Parents’ sources of adolescent sexual health information and their interest in resources from primary care. Acad Pediatr. 2022;22(3):396–401. doi:10.1016/j.acap.2021.09.007
44. Mwaisaka J, Wado YD, Ouedraogo R, et al. “Those are things for married people” exploring parents’/adults’ and adolescents’ perspectives on contraceptives in Narok and Homa Bay Counties, Kenya. Reprod Health. 2021;18(1):1–13. doi:10.1186/s12978-021-01107-w
45. Coast E, Jones N, Francoise UM, et al. Adolescent sexual and reproductive health in Ethiopia and Rwanda: a qualitative exploration of the role of social norms. SAGE Open. 2019;9(1):2158244019833587. doi:10.1177/2158244019833587
46. Nyblade L, Stockton M, Nyato D, et al. Perceived, anticipated and experienced stigma: exploring manifestations and implications for young people’s sexual and reproductive health and access to care in North-Western Tanzania. Cult Health Sex. 2017;19(10):1092–1107. doi:10.1080/13691058.2017.1293844
47. Onokerhoraye AG, Dudu JE. Perception of adolescents on the attitudes of providers on their access and use of reproductive health services in Delta State, Nigeria. Health. 2017;9(1):88.
48. Blum RW, Astone NM, Decker MR, et al. A conceptual framework for early adolescence: a platform for research. Int J Adolesc Med Health. 2014;26(3):321–331. doi:10.1515/ijamh-2013-0327
49. Kågesten A, Gibbs S, Blum RW, et al. Understanding factors that shape gender attitudes in early adolescence globally: a mixed-methods systematic review. PLoS One. 2016;11(6):e0157805. doi:10.1371/journal.pone.0157805
50. Shatilwe JT, Mashamba-Thompson TP. Mapping evidence on access to healthcare information by women of reproductive age in low-and-middle-income countries: scoping review protocol. Syst Rev. 2019;8(1):1–7. doi:10.1186/s13643-019-1203-5
51. Ganle JK, Baatiema L, Quansah R, et al. Barriers facing persons with disability in accessing sexual and reproductive health services in sub-Saharan Africa: a systematic review. PLoS One. 2020;15(10):e0238585. doi:10.1371/journal.pone.0238585
52. Rizvi F, Williams J, Maheen H, et al. Using social ecological theory to identify factors associated with risky sexual behavior in cambodian adolescent girls and young women aged 10 to 24 years: a systematic review. Asia Pac J Public Health. 2020;32(2–3):71–80. doi:10.1177/1010539520911493
53. Bhatt N, Bhatt B, Neupane B, et al. Perceptions of family planning services and its key barriers among adolescents and young people in Eastern Nepal: a qualitative study. PLoS One. 2021;16(5):e0252184. doi:10.1371/journal.pone.0252184
54. Jonas K, Duby Z, Maruping K, et al. Perceptions of contraception services among recipients of a combination HIV-prevention interventions for adolescent girls and young women in South Africa: a qualitative study. Reprod Health. 2020;17(1):1–14. doi:10.1186/s12978-020-00970-3
55. Garney W, Wilson K, Ajayi KV, et al. Social-ecological barriers to access to healthcare for adolescents: a scoping review. Int J Environ Res Public Health. 2021;18(8):4138. doi:10.3390/ijerph18084138
56. Aventin Á, Gordon S, Laurenzi C, et al. Adolescent condom use in Southern Africa: narrative systematic review and conceptual model of multilevel barriers and facilitators. BMC Public Health. 2021;21(1):1–22. doi:10.1186/s12889-021-11306-6
57. Alomair N, Alageel S, Davies N, Bailey JV. Factors influencing sexual and reproductive health of Muslim women: a systematic review. Reprod Health. 2020;17(1):1–15. doi:10.1186/s12978-020-0888-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.