Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Social Support and Depression Among Pulmonary Tuberculosis Patients in Anhui, China
Authors Fang XH, Qian Wu, Tao SS, Xu ZW, Zou YF, Ma DC, Pan HF ![]() , Hu WB
, Hu WB ![]()
Received 28 December 2021
Accepted for publication 15 March 2022
Published 29 March 2022 Volume 2022:15 Pages 595—603
DOI https://doi.org/10.2147/JMDH.S356160
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xue-Hui Fang,1,2,* Qian Wu,3,* Sha-Sha Tao,4,* Zhi-Wei Xu,5 Yan-Feng Zou,4 Dong-Chun Ma,1,2 Hai-Feng Pan,4 Wen-Biao Hu6
1Anhui Provincial Chest Hospital (Anhui Institute of Tuberculosis Control), Hefei, Anhui, 230022, People’s Republic of China; 2Anhui Provincial Chest Hospital Affiliated to Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China; 3Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Epidemiology and Biostatistics, School of Public Health, Anhui Medical University, Hefei, Anhui, People’s Republic of China; 5School of Public Health, Faculty of Medicine, University of Queensland, Brisbane, QLD, 4006, Australia; 6School of Public Health and Social Work, Queensland University of Technology, Brisbane, QLD, Australia
*These authors contributed equally to this work
Correspondence: Hai-Feng Pan, Department of Epidemiology and Biostatistics, School of Public Health, Anhui Medical University, 81 Meishan Road, Hefei, Anhui, 230032, People’s Republic of China, Tel +86 551 65161165, Fax +86 551 65161171, Email [email protected] Wen-Biao Hu, School of Public Health and Social Work, Institute of Health and Biomedical Innovation, Queensland University of Technology, Brisbane, Queensland, Australia, Email [email protected]
Introduction: Pulmonary tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis affecting multiple tissues and organs. It is one of the leading causes of death and is a social disease in China. Increasing studies have revealed that the state of mental health and the social support are associated with the morbidity, mortality and community transmission of pulmonary TB patients. However, the previous global TB control and research strategy focused almost solely on the biomedical aspects. Therefore, in this study, we evaluated the level of depression and explored potential factors, including social support domains and socio-demographic characteristics in pulmonary TB patients to research the mental health state and the association between social support and pulmonary TB, ultimately implementing a multilevel intervene.
Methods: A cross-sectional study was carried out to describe the status of depression and social support, and explore related factors associated with depression among pulmonary TB patients in Anhui Province, China. Five counties (districts) in Anhui Province, China were selected by simple random sampling method. Patients diagnosed with pulmonary TB eligible to the study criteria were investigated. A structured questionnaire composed of information on socio-demographic characteristics, self-rating depression scale (SDS) and social support rating scale (SSRS) was used to collect the data.
Results: In this study, a total of 250 questionnaires were issued, and the effective questionnaires 237 were actually returned. Of the 237 patients with pulmonary TB, 71.3% of them were male and the mean age was 46.16 years (SD = 13.09). Depression symptoms were observed in 125 (52.7%) participants. Objective support (β = − 0.192, P=0.002) and subjective support (β = − 0.158, P = 0.015) had significantly negative effects on depression, while the effect of support utilization was not statistically significant. In contrast, being female (β = 0.119, P = 0.036) and patients with positive sputum smear results (β = 0.140, P = 0.014) were positively related to depression. Patients with monthly income between 500 and 999 were less likely to suffer from depression (β = − 0.134, P = 0.024) than those who were poorer. Additionally, both education level and marital status were found to be correlated with social support and depression state (all P< 0.05).
Discussion: In summary, the prevalence of depressive symptoms in pulmonary TB patients were high in Anhui Province, China. Low levels of social support can be an important predictor of depression symptoms. Therefore, screening for depression among pulmonary TB patients in the primary care setting is greatly warranted. Furthermore, psychological interventions should focus on providing available and adequate social support in order to improve mental health of them.
Keywords: pulmonary tuberculosis, mental health, depression, social support, epidemiology
Introduction
Pulmonary Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis affecting multiple tissues and organs. As reported in 2020, most TB cases were in the WHO regions of South-East Asia (43%) geographically. The 30 high TB burden countries accounted for 86% of all estimated incident cases worldwide, and eight of these countries accounted for two thirds of the global total, China ranked second accounting for 8.5% after India accounting for 26%.1 Pulmonary TB remains a social disease, inequitably affecting poor people especially in resource-constrained regions.2 Despite the progress it has made in pulmonary TB control, there are still considerable challenges in detection and treatment.3
Depression is the most prevalent mental disorder characterized by loss of interest, feelings of guilt or low self-worth.4 Several studies concur that the prevalence of depression is high among people with chronic diseases, including pulmonary TB.5,6 A cross-sectional study reported that patients with TB are often accompanied by pain, anxiety and depression, which all contribute to a lower Health-related quality of life (HRQoL).7 Social support is hypothesized to have positive effects on health outcomes both directly through the benefits of social relationships and indirectly as a buffer against stressful life events.8 There is an increasing body of evidence suggesting that pulmonary TB has a negative impact on social roles and exposes individuals at risk of social isolation, which may reduce confidence in the ability to self-manage their disease.9,10 It was also reported that depression may has negative influences on behaviors, including diet, seeking medical care, medication adherence, and/or treatment completion, which is highly detrimental to the global elimination of TB.11 Lack of adherence to anti-TB regimens may lead to higher risk for drug resistance, morbidity, mortality, as well as community transmission.12–15 Evidently, pulmonary TB patients with psychiatric disorders are more likely to have physical and social disability.16 In order to supplement biomedical work to control pulmonary TB, it is necessary to implement multi-level interventions. However, the previous global TB control and research strategy focused almost solely on the biomedical aspects. Little is known about the state of mental health and the association with social support among pulmonary TB patients.
Therefore, in this study, we evaluated the level of depression and explored potential factors, including social support domains and socio-demographic characteristics in pulmonary TB patients in Anhui province, aiming to investigate the association between social support, mental health disorders and pulmonary TB, which may help provide scientific basis for taking targeted measures, and improve the mental health of pulmonary TB patients, and ultimately to implement a multilevel intervene to control TB.
Materials and Methods
Study Design and Subjects
This was a cross-sectional study conducted in Anhui province, which consists of three regions (Jiangnan, Jianghuai and Huaibei) with a total of 106 counties (districts). The sample size was calculated by Power Analysis and Sample Size (PASS) software with the following assumptions: 17.73% prevalence rate of depression,10 95% confidence interval. Taking 5% as incomplete records, the minimum sample size was 243. From January 1, 2016 to June 30, 2016, five cities/counties (including Lixin county, Suixi county, Jinzhai county, Tongcheng city and Xi county) were randomly chosen as study sites. Finally, 250 patients were randomly selected from the Chinese Disease Prevention Control Information System, with 50 patients in each city/county. Inclusion criteria: 1. pulmonary TB cases with symptoms of tuberculosis infection, positive sputum smear, and imaging features suggestive of pulmonary TB were diagnosed by two professional physicians according to the Chinese “Pulmonary Tuberculosis Diagnosis (WS288–2008)”. 2. Cases who participated voluntarily and were able to complete the questionnaire independently. Exclusion criteria: 1. Cases with other extrapulmonary diseases and drug-resistant pulmonary TB; 2. Cases with HIV positive, malignant tumors and systemic infections; 3. Cases with severe heart, liver, and renal failure; 4. Cases who are unwilling to participate in this study. The informed consent agreements were obtained from all the participants. The study procedure complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Anhui Provincial Chest Hospital.
Measurement
Data were collected by trained interviewers. The structured questionnaire was designed to collect information regarding socio-demographic variables, including age, sex, education level, marital status, household monthly income, place of residence and sputum smear type. Meanwhile, depression symptoms and social support were assessed by Self-Rating Depression Scale (SDS) and Social Support Rating Scale (SSRS), respectively.
Self-Rating Depression Scale (SDS)
The scale consists of 20 items and each item includes 4 categories: always, often, sometimes, or rarely.17 The standardized score is equal to 1.25 times the raw score, and a score over 53 is considered to indicate the presence of depression. According to the results of the Chinese norm,18 a score of 53 to 62 indicates mild depression, and 63 to 72 is classified as moderate depression. Scores more than 72 are generally considered to reflect severe depression. This scale showed a fair internal consistency (Cronbach’s alpha = 0.862).
The Social Support Rating Scale (SSRS)
The Social Support Rating Scale (SSRS) is a self-report inventory in Chinese. It was used to assess the social support status of individuals, which has been widely applied in Chinese populations due to its high reliability and validity.19,20 This scale consists of three dimensions, namely subjective support (items 1, 3, 4 and 6 of the questionnaire), objective support (items 2, 6 and 7 of the questionnaire) and support utilization (items 8, 9 and 10 of the questionnaire). The total score ranged from 12 to 66, with higher score indicating greater social support and more diverse social networks. The Cronbach’s alpha for each subscale ranged from 0.89 to 0.94.
Statistical Analysis
The Statistical Package for Social Science (SPSS) version 23.0 for Windows and PASS (version 11) was used for data analysis. Socio-demographic characteristics were described using frequencies for categorical variables, mean and standard deviation (SD) for continuous variables. The difference between continuous variables in groups was tested by Student’s t-test or One-way analysis of variance. Pearson correlations were performed to examine bivariate associations between social support and depression. Multiple linear regression analysis was conducted to determine factors independently associated with depression. The significance tests are two-sided, with a P value ≤0.05 considered statistically significant.
Results
Socio-Demographic Characteristics of Participants
In this study, a total of 250 questionnaires were issued, and the effective questionnaires 237 were actually returned, with an effective rate of 94.8%. The mean age of the patients was 46.16 years (SD = 13.09). Among the patients, 73.8% of them were married and 90.3% of them lived in rural area. The majority of them were male (71.3%). More than half of the pulmonary TB patients were graduates of primary school or junior high school (58.6%). The socio-demographic characteristics of all patients were shown in Table 1.
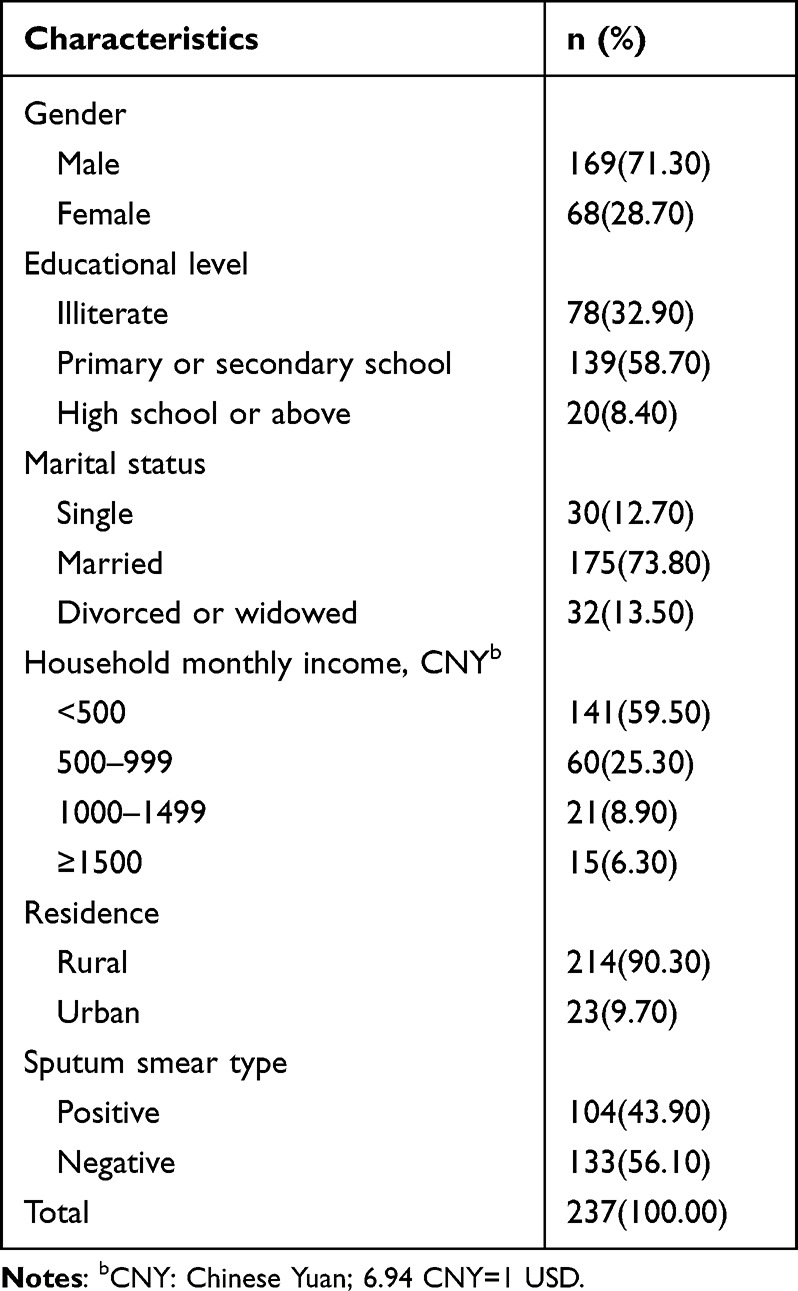 |
Table 1 The Socio-Demographic Characteristics of Study Subjects |
Prevalence of Depression
Of the 237 patients with pulmonary TB included in this study, depression was found in 125 participants with the use of the self-rating depression scale, accounting for 52.7%. The prevalence of mild, moderate and severe depression was 31.6%, 15.2% and 5.9%, respectively.
Comparison of Scores Among Pulmonary TB Patients with Different Characteristics
The mean scores for depression and social support based on the categorical items are listed in Table 2. On univariate analysis, all pulmonary TB related variables except place of residence were associated with SDS scores (all P<0.05). It also reported a significant relationship between social support scores, except for support utilization scores, and the following variables: educational level (all P<0.05), marital status (all P<0.001) and household monthly income (all P<0.001).
 |
Table 2 The Distribution of SSRS Score Among Pulmonary TB Patients with Different Characteristics |
Correlation Analysis of Depression and Social Support
Table 3 presents the correlation coefficients between depression, social support. The results indicated that social support (r=−0.358), objective support (r=−0.357) and subjective support (r=−0.317) were negatively correlated with depression (all P<0.001), except for that between support utilization and depression (r=−0.090, P>0.05). However, a significantly positive correlation existed between social support and its three dimensions.
 |
Table 3 Correlation Analysis of Depression and Social Support |
Multiple Linear Regression Analysis for Depression
For the analysis of the predictors that influence depression state, a multiple regression analysis was performed. As the model shown in Table 4, objective support (β =−0.192, P=0.002), subjective support (β = −0.158, P=0.015) had significantly negative effects on depression, while the effect of support utilization was not statistically significant (P>0.05). In contrast, being female (β =0.119, P=0.036) and have positive sputum smear result (β =0.140, P=0.014) were positively related to SDS scores. Compared to patients with monthly income of less than 500, those with monthly income between 500 and 999 were less likely to suffer from depression (β = −0.134, P = 0.024). Additionally, illiterate patients were more prone to depressive symptoms than those who had received primary or junior high school (β = −0.179, P = 0.005) and high school or above education (β = −0.148, P = 0.033). Similarly, poor marital status was also found to be independently associated with depression state, it means that divorced or widowed patients were more likely to feel depressed than single (β = −0.201, P=0.006) or married (β = −0.162, P = 0.028) patients. Above all, a total of 31.1% of the variance was explained by this regression model.
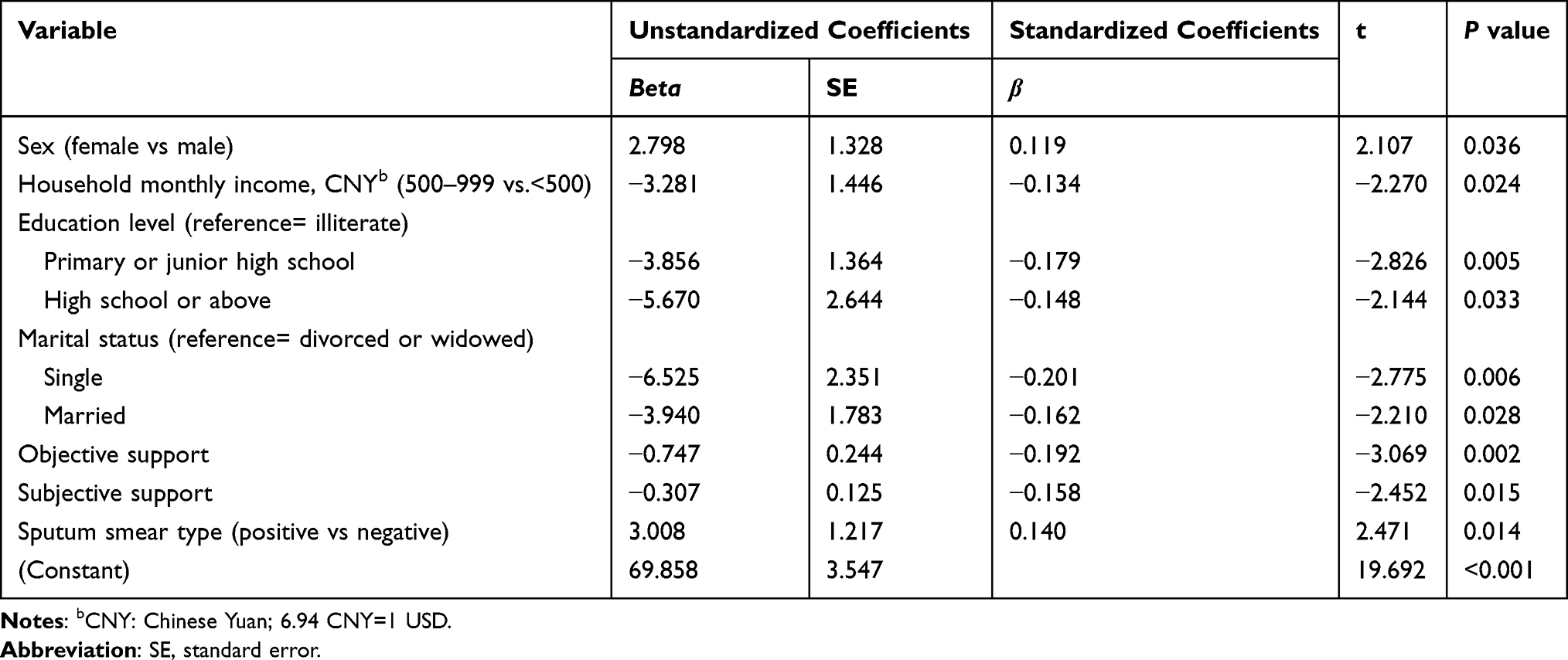 |
Table 4 Multiple Linear Regression Models for Predictors of Depression |
Discussion
Although most pulmonary TB patients can be fully cured after a six-month period of standard treatment, relapse or drug resistance may be caused by long-term treatment or drug side effects. Therefore, patients were often under too much psychological distress and low perceived social support.21,22 In this cross-sectional study, we examined the relationship between social support and depression in the patients with pulmonary TB to help to provide scientific basis for taking targeted measures, to improve the mental health of pulmonary TB patients, and ultimately to implement a multilevel intervene to control TB.
A database-based cohort study conducted in noted that overall incidence of pulmonary TB was 1.16-fold greater in the depression group than those without depression.23 In our study, the prevalence of depression symptoms in patients with pulmonary TB was 52.7%. Similar high rates have been reported in Nigeria, Ethiopia and Cameroon with prevalence rates ranging from 45.5% to 61.1%.4,24,25 However, lower prevalence rate were also observed in Peru and Nigeria.26,27 On the one hand, the differences may be partly explained by the fact that our study evaluated only depressive symptoms rather than major depression.28 On the other hand, this result can be attributed to the differences in scales selection, the characteristics of the subjects and study region.
Social support refers to subject and objective support, as well as support availability.29 In our study, the mean score for the total social support was 37.97 (SD = 8.20). Factors associated with social support domains, except for support utilization, were identified to be education level, household monthly income and marital status. Previous studies highlighted that social support can act as a potent buffer against the negative impacts of stressors.30 For people experiencing depression, they have less knowledge of the sources of beneficial social support.31 As important social determinants, objective support and subjective support were found to be inversely associated with the presence of depressive symptoms among patients suffering from TB. Therefore, considerable attention and adequate social support should be paid to these patients.
Consistent with prior studies conducted in both developing and developed countries,24,32,33 education level, household monthly income and marital status remained significant predictors of depression after controlling for all socio-demographic variables. Meanwhile, we confirmed that female patients were more likely to suffer from depression, which were also reported in previous researches34–37 and the etiology of the gender difference in depression is multifactorial.38,39 Although another cross-sectional survey conducted in hospitals found that young age (<30 years) may increase the risk of probable depression in TB patients, we did not find association between age and SDS scores among patients of different ages.10 In this study, a significant difference of depression was observed between the sputum smear-positive and negative group and the results of multiple regression analysis showed that positive sputum smear was positively related to SDS scores. All the above results suggested that there may be a link between depression and the severity of pulmonary TB, suggesting that we should pay more attention to the mental health of sputum smear-positive patients. However, there was no difference in the social support score between the sputum-smear-positive and negative groups, while the results of multiple regression analysis found a negative correlation between objective support, subjective support and depression, suggesting that the association between sputum-positive pulmonary TB and depression may not be through social support. It was also reported that 70% of mental disorders are diagnosed in tuberculosis patients and many medications used to treat TB and psychiatric conditions negatively affect each other.6 Moreover, it was revealed that mental illness may lead to low treatment-seeking and adherence among TB patients and contribute to high morbidity, mortality, transmission and drug resistance.40 In summary, the association between pulmonary TB and mental disorders may be bidirectional.41,42
However, several limitations to our findings should be taken into account. First of all, the conclusion in this study can only provide etiological clues for further research but not the directions of causality due to the cross-sectional design. Furthermore, due to the cases with HIV positive were excluded, there was a lack of available data on HIV to discuss the role of HIV played in the association between pulmonary TB, social isolation and depression, although it is well known that HIV-positive is associated with a higher risk for social isolation and depression. Therefore, the generalizability of our results may be restricted. In addition, the potential misclassification or unknown confounding factors may have led to underestimation of the link between pulmonary TB and depression. A comparison of our results to healthy controls was not possible due to the lack of a control group. Finally, the present study may be underpowered considering the small sample size, as only six cities/counties in Anhui Province were selected in this study. Therefore, further longitudinal studies with larger sample size are still awaited to assess the magnitude of depression, social support and associated factors among TB patients.
Conclusions
As we all know, mental illness may lead to low treatment-seeking and adherence among TB patients and contribute to high morbidity, mortality, transmission and drug resistance.40 Unfortunately, in this study we observed that there is a high prevalence of depressive symptom in pulmonary TB patients in Anhui Province, China. In addition, low levels of social support can be an important predictor of depression symptoms. However, mental health services and specialists are restricted in low-resource-constrained settings where the high burden of TB is located. Therefore, it is necessary to screen for and address depression in pulmonary TB patients and provide them with adequate social support, which will not only promote their mental health but also improve their compliance with treatments.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Acknowledgments
Xue-Hui Fang, Qian Wu, and Sha-Sha Tao are co-first authors for this study.
Funding
There is no funding to report.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. World Health Organization. Global tuberculosis report; 2021. Available from: https://apps.who.int/iris/bitstream/handle/10665/346387/9789240037021-eng.pdf?sequence=1&isAllowed=y.
2. Wingfield T, Tovar MA, Huff D, et al. Beyond pills and tests: addressing the social determinants of tuberculosis. Clini Med. 2016;16(Suppl 6):s79–s91. doi:10.7861/clinmedicine.16-6-s79
3. Lin HH, Wang L, Zhang H, et al. Tuberculosis control in China: use of modelling to develop targets and policies. Bull World Health Organ. 2015;93(11):790–798. doi:10.2471/blt.15.154492
4. Kehbila J, Ekabe CJ, Aminde LN, et al. Prevalence and correlates of depressive symptoms in adult patients with pulmonary tuberculosis in the Southwest Region of Cameroon. Infec Dis Poverty. 2016;5(1):51. doi:10.1186/s40249-016-0145-6
5. Boing AF, Melo GR, Boing AC, et al. Association between depression and chronic diseases: results from a population-based study. Rev Saude Publica. 2012;46(4):617–623. doi:10.1590/S0034-89102012005000044
6. Doherty AM, Kelly J, McDonald C, et al. A review of the interplay between tuberculosis and mental health. Gen Hosp Psychiatry. 2013;35(4):398–406. doi:10.1016/j.genhosppsych.2013.03.018
7. Zarova C, Chiwaridzo M. The impact of social support on the health-related quality of life of adult patients with tuberculosis in Harare, Zimbabwe: a cross-sectional survey. BMC Res Notes. 2018;11(1):795. doi:10.1186/s13104-018-3904-6
8. Gariepy G, Honkaniemi H, Quesnel-Vallee A. Social support and protection from depression: systematic review of current findings in Western countries. J Ment Sci. 2016;209(4):284–293. doi:10.1192/bjp.bp.115.169094
9. Pachi A, Bratis D, Moussas G, et al. Psychiatric morbidity and other factors affecting treatment adherence in pulmonary tuberculosis patients. Tuberc Res Treat. 2013;2013:489865. doi:10.1155/2013/489865
10. Wang XB, Li XL, Zhang Q, et al. A survey of anxiety and depressive symptoms in pulmonary tuberculosis patients with and without Tracheobronchial Tuberculosis. Front Psychiatry. 2018;9:308. doi:10.3389/fpsyt.2018.00308
11. Sweetland AC, Kritski A, Oquendo MA, et al. Addressing the tuberculosis-depression syndemic to end the tuberculosis epidemic. Int J Tuberc Lung Dis. 2017;21(8):852–861. doi:10.5588/ijtld.16.0584
12. Acha J, Sweetland A, Guerra D, et al. Psychosocial support groups for patients with multidrug-resistant tuberculosis: five years of experience. Glob Public Health. 2007;2(4):404–417. doi:10.1080/17441690701191610
13. Husain MO, Dearman SP, Chaudhry IB, et al. The relationship between anxiety, depression and illness perception in tuberculosis patients in Pakistan. Clin Pract Epidemiol Ment Health. 2008;4(1):4. doi:10.1186/1745-0179-4-4
14. Sweetland A, Oquendo M, Wickramaratne P, et al. Depression: a silent driver of the global tuberculosis epidemic. World Psychiatry. 2014;13(3):325–326. doi:10.1002/wps.20134
15. Duarte EC, Bierrenbach AL, Barbosa da Silva J
16. Aydin IO, Ulusahin A. Depression, anxiety comorbidity, and disability in tuberculosis and chronic obstructive pulmonary disease patients: applicability of GHQ-12. Gen Hosp Psychiatry. 2001;23(2):77–83. doi:10.1016/S0163-8343(01)00116-5
17. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
18. Wang CF, Cai ZH, Xu Q. Evaluation of 1340 normal people by Self-rating Depression Scale-SDS. Chin J Nerv Ment Dis. 1986;14(5):267–268. Chinese.
19. Xiao SY. The theoretical base and research application of social support rating scale. J Clin Psychol Med. 1994;4(2):98–100. Chinese.
20. Lu CF, Jia CX, Zhang JY, et al. Reliability and validity of social support rating scale in rural suicides. Chin Ment Health J. 2011;25(3):218–222. Chinese.
21. Shen TC, Wang CY, Lin CL, et al. People with tuberculosis are associated with a subsequent risk of depression. Eur J Intern Med. 2014;25(10):936–940. doi:10.1016/j.ejim.2014.10.006
22. Yen YF, Chung MS, Hu HY, et al. Association of pulmonary tuberculosis and ethambutol with incident depressive disorder: a nationwide, population-based cohort study. J Clin Psychiatry. 2015;76(4):e505–511. doi:10.4088/JCP.14m09403
23. Cheng KC, Liao KF, Lin CL, et al. Increased risk of pulmonary tuberculosis in patients with depression: a cohort study in Taiwan. Front Psychiatry. 2017;8:235. doi:10.3389/fpsyt.2017.00235
24. Ige OM, Lasebikan VO. Prevalence of depression in tuberculosis patients in comparison with non-tuberculosis family contacts visiting the DOTS clinic in a Nigerian tertiary care hospital and its correlation with disease pattern. Ment Health Fam Med. 2011;8(4):235–541.
25. Ambaw F, Mayston R, Hanlon C, et al. Burden and presentation of depression among newly diagnosed individuals with TB in primary care settings in Ethiopia. BMC Psychiatry. 2017;17(1):57. doi:10.1186/s12888-017-1231-4
26. Ugarte-Gil C, Ruiz P, Zamudio C, et al. Association of major depressive episode with negative outcomes of tuberculosis treatment. PLoS One. 2013;8(7):e69514. doi:10.1371/journal.pone.0069514
27. Issa BA, Yussuf AD, Kuranga SI. Depression comorbidity among patients with tuberculosis in a University teaching hospital outpatient clinic in Nigeria. Ment Health Fam Med. 2009;6(3):133–138.
28. Masumoto S, Yamamoto T, Ohkado A, et al. Prevalence and associated factors of depressive state among pulmonary tuberculosis patients in Manila, The Philippines. Int J Tuberc Lung Dis. 2014;18(2):174–179. doi:10.5588/ijtld.13.0335
29. McNally ST, Newman S. Objective and subjective conceptualizations of social support. J Psychosom Res. 1999;46(4):309–314. doi:10.1016/s0022-3999(98)00110-x
30. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
31. Smith L, Hill N, Kokanovic R. Experiences of depression, the role of social support and its impact on health outcomes. J Ment Health. 2015;24(6):342–346. doi:10.3109/09638237.2014.954693
32. Moussas G, Tselebis A, Karkanias A, et al. A comparative study of anxiety and depression in patients with bronchial asthma, chronic obstructive pulmonary disease and tuberculosis in a general hospital of chest diseases. Ann Gen Psychiatry. 2008;7:7. doi:10.1186/1744-859x-7-7
33. Guerra M, Prina AM, Ferri CP, et al. A comparative cross-cultural study of the prevalence of late life depression in low and middle income countries. J Affect Disord. 2016;190:362–368. doi:10.1016/j.jad.2015.09.004
34. Li D, Zhang DJ, Shao JJ, et al. A meta-analysis of the prevalence of depressive symptoms in Chinese older adults. Arch Gerontol Geriatr. 2014;58(1):1–9. doi:10.1016/j.archger.2013.07.016
35. Piccinelli M, Wilkinson G. Gender differences in depression Critical review. J Ment Sci. 2000;177:486–492. doi:10.1192/bjp.177.6.486
36. Bromet E, Andrade LH, Hwang I, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011;9:90. doi:10.1186/1741-7015-9-90
37. Salk RH, Hyde JS, Abramson LY. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull. 2017;143(8):783–822. doi:10.1037/bul0000102
38. Hyde JS, Lindberg SM, Linn MC, et al. Diversity Gender similarities characterize math performance. Science. 2008;321(5888):494–495. doi:10.1126/science.1160364
39. Cyranowski JM, Frank E, Young E, et al. Adolescent onset of the gender difference in lifetime rates of major depression: a theoretical model. Arch Gen Psychiatry. 2000;57(1):21–27. doi:10.1001/archpsyc.57.1.21
40. Ruiz-Grosso P, Cachay R, de la Flor A, et al. Association between tuberculosis and depression on negative outcomes of tuberculosis treatment: a systematic review and meta-analysis. PLoS One. 2020;15(1):e0227472. doi:10.1371/journal.pone.0227472
41. Oh KH, Choi H, Kim EJ, et al. Depression and risk of tuberculosis: a nationwide population-based cohort study. Int J Tuberc Lung Dis. 2017;21(7):804–809. doi:10.5588/ijtld.17.0038
42. Hayward SE, Deal A, Rustage K, et al. The relationship between mental health and risk of active tuberculosis: a systematic review. BMJ Open. 2022;12(1):e048945. doi:10.1136/bmjopen-2021-048945
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.