Back to Journals » Journal of Pain Research » Volume 15
Social Media and Professional Conduct (SMART): Best Practice Guidelines from the American Society of Pain and Neuroscience (ASPN)
Authors Desai MJ ![]() , Khatri N
, Khatri N ![]() , Hagedorn JM
, Hagedorn JM ![]() , Strand N
, Strand N ![]() , D'Souza RS
, D'Souza RS ![]() , Tieppo Francio V
, Tieppo Francio V ![]() , Abd-Elsayed A, Lee DW, Petersen E
, Abd-Elsayed A, Lee DW, Petersen E ![]() , Goree JH
, Goree JH ![]() , Weisbein JS
, Weisbein JS ![]() , Deer TR
, Deer TR ![]()
Received 19 March 2022
Accepted for publication 3 June 2022
Published 14 June 2022 Volume 2022:15 Pages 1669—1678
DOI https://doi.org/10.2147/JPR.S366978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Robert Twillman
Mehul J Desai,1,2 Nasir Khatri,3,4 Jonathan M Hagedorn,5 Natalie Strand,6 Ryan S D’Souza,7 Vinicius Tieppo Francio,8 Alaa Abd-Elsayed,9 David W Lee,10 Erika Petersen,11 Johnathan H Goree,12 Jacqueline S Weisbein,13 Timothy R Deer14
1International Spine, Pain & Performance Center, Washington, DC, USA; 2George Washington University, School of Medicine & Health Sciences, Washington, DC, USA; 3University of Kansas, Department of Anesthesiology, Kansas City, KS, USA; 4Novant Spine Specialists, Division of Interventional Pain Medicine, Charlotte, NC, USA; 5iSpine Pain Physicians, Maple Grove, MN, USA; 6Mayo Clinic, Division of Pain Medicine, Phoenix, AZ, USA; 7Mayo Clinic, Department of Anesthesiology, Rochester, MN, USA; 8University of Kansas, Department of Rehabilitation Medicine, Kansas City, KS, USA; 9University of Wisconsin, Department of Anesthesiology, Madison, WI, USA; 10Fullerton Orthopedic Surgery Medical Group, Fullerton, CA, USA; 11University of Arkansas, Department of Neurosurgery, Little Rock, AR, USA; 12University of Arkansas, Department of Anesthesiology, Little Rock, AR, USA; 13Interventional Pain Management, Napa Valley Orthopaedic Medical Group, Napa, CA, USA; 14Spine & Nerve Centers of the Virginias, Charleston, WV, USA
Correspondence: Mehul J Desai, International Spine, Pain & Performance Center, 2021 K St NW Suite 615, Washington, DC, 20006, USA, Email [email protected]
Abstract: Social media has revolutionized internet communication and become ubiquitous in modern life. Though it originated as a medium for friendship, social media has evolved into an ideal venue for professional networking, scientific exchange, and brand building. As such, it is a powerful tool with which interventional pain physicians should become familiar. However, given the permanence and visibility of online posts, it is prudent for interventional pain physicians to utilize social media in a manner that is consistent with the ethical and professionalism standards to which they are held by their patients, employers, peers, and state medical boards. While there are extensive publications of professional codes of conduct by medical societies, there is a paucity of literature regarding social media best practices guidelines. Further, to date there have been no social media best practices recommendations specific to interventional pain medicine physicians. While not exhaustive, the aim of this document is to provide recommendations to pain physicians on how to maintain an effective professional and ethical online presence. Specifically, we provide guidance on online persona and professional image, patient–physician interactions online, patient privacy, industry relations, patient education, and brand building.
Keywords: professionalism, social media, ethics, best practices, LinkedIn, Instagram, Twitter, Facebook
Introduction
Over the past two decades, social media has revolutionized communication and become a ubiquitous aspect of modern life. Social media platforms are powerful tools which allow users to create and share content to wide audiences, free from geographical and chronological boundaries. The use of social media in medicine has increased dramatically in recent years. While only 5% of American adults had an active social media account in 2005, that number had risen to 72% by 2021.1 This is especially relevant in our society as screentime for all age groups has risen sharply over the past two decades.2,3 Social media use is even more prevalent among healthcare professionals, with nearly 90% of all physicians maintaining a social media presence.1 While initially used for personal reasons, there is a large and growing community of physicians utilizing social media for professional purposes.4
These online platforms present a low-cost, low-barrier entry for physicians to network with one another in a manner that previously was only possible during annual society meetings.5 While physician engagement in social media may take many forms, interventional pain physicians most commonly use Facebook, Twitter, Instagram, and LinkedIn to build their personal brand, highlight their competitive advantage to patients, and disseminate medical literature.5 Further, there is data to suggest that physicians with a strong social media presence tend to have fewer negative reviews online and improved search engine optimization.6 Social media is also used by pharmaceutical and medical device companies to advertise their products, share research studies, and engage with physicians online.
The evolution of interventional pain medicine and the rapid development of new therapies provides rich fodder for social media content. Given the permanence and visibility of online posts, it is prudent for interventional pain physicians to utilize social media in a manner that is consistent with the ethical and professional standards to which they are held by their patients, employers, peers, and state medical boards. There is a lack of guidance regarding best practices for the use of social media by interventional pain physicians. While not exhaustive, the aim of this document is to provide recommendations to pain physicians on how to maintain an effective professional and ethical online presence.
Methods
Development Process
The American Society of Pain and Neuroscience (ASPN) performed a needs-based assessment of online professionalism and ethical codes of conduct published by medical societies and organizations. It was determined that there is sparsity in the literature regarding social media best practices guidelines. Previous social media guidelines published have focused on physicians in general or a society’s own subspecialists; however, there is a paucity of guidance for interventional pain physicians as there are certain aspects of our field which pose special challenges on social media. ASPN elected to address this by publishing a social media best practice review for interventional pain medicine physicians. A multi-disciplinary panel of pain medicine physicians was selected to create these guidelines. Selection was made based on consideration of experience with social media for personal and professional purposes, clinical experience, practice setting, and diversity. This study was exempt from IRB approval as it was only a literature review with no analysis of patient information.
Literature Search Method
A literature search was performed by the authors identifying webpages, guidelines, and publications relevant to social media use by physicians. Searches were completed using PubMed, Google Scholar, and Ovid MEDLINE. Keywords used were: “social media + physician,” “social media + patient physician,” “social media best practices + physician,” “code of conduct + physician.” Further, individual social media guidelines and recommendations were obtained from the websites of the American Medical Association, American College of Surgeons, American College of Obstetrics and Gynecology, Federation of State Medical Boards, American College of Physicians, and the American College of Cardiology.
Evidence Ranking and Consensus Development
Given the nature of the topic, traditional evidence ranking is not possible. Therefore, the ASPN social media working group opted to publish recommendations on which a consensus was reached by all members of the working group. For completeness, we have elected to assign a consensus-based United States Preventative Services Task Force (USPSTF) evidence ranking with letter grading for strength of recommendation (Table 1). In addition we have included both best practice recommendations under each section as well as consensus recommendations for each best practice (Table 2).
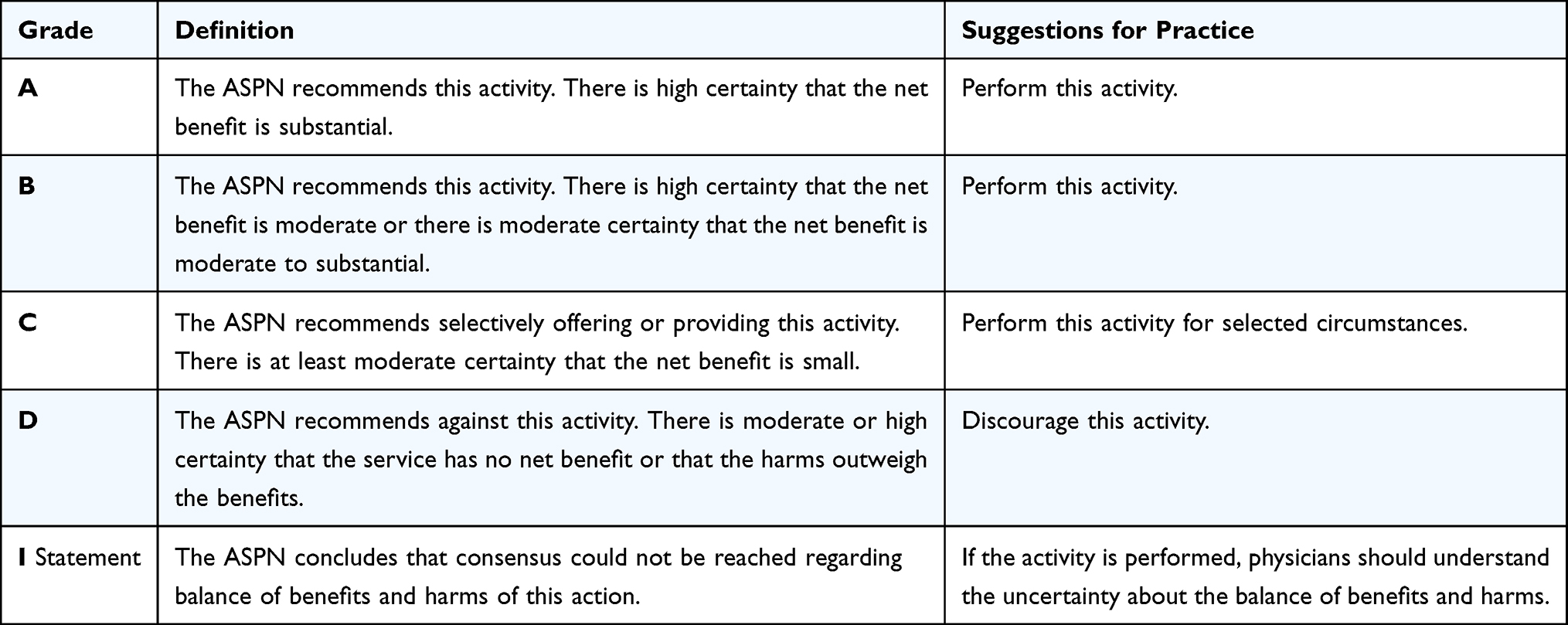 |
Table 1 Strength of Consensus Using United States Preventative Services Task Force Criteria Modified for Social Media Presence |
 |
Table 2 Consensus Recommendations for Each Best Practice Category Described in the Guidelines |
Best Practices
Online Persona and Professional Image
As social media posts are widely visible to a large audience, it is important to create boundaries separating one’s personal profile from one’s professional online persona.7 All content, regardless of whether it is posted on a personal or professional account, should be regarded as publicly visible.7 As physicians, our patients and society at large view our actions as representative of our profession and hold us to a high standard. Thus, healthcare professionals should adhere to professionalism standards expected by our employers, specialty societies, peers, and state medical boards.
In today’s world, political discourse is becoming commonplace. However, as it always has been, political conversations evoke strong and polarizing emotions among individuals. Posting political content, especially if done on a professional account, can affect a physician’s ability to establish a non-judgmental environment and trusting relationship with their patients, create an uncomfortable environment for trainees, and at its extreme can tarnish one’s reputation in a community. As an illustrative example related to the field of pain medicine, proponents for medical marijuana have supported the use of medical marijuana based on its effectiveness in managing debilitating pain. However, objections to the use of medical marijuana among the medical, legal, and ethical communities persist and are partly attributable to the national policy of the federal government of supporting a zero-tolerance approach toward illicit substances.8 Similarly, the opioid epidemic has also involved significant debate on the political arena. The opioid crisis has highlighted that opioid analgesics are causative agents for patient harm, with physicians as conduits and pharmaceutical companies as promoters of the crisis.9 This perspective has often overlooked the increasing prevalence of chronic pain in the general population due to musculoskeletal disease in an aging population, increasing survivorship after injury and cancer, increasing volume and complexity of surgery, and greater patient expectations for optimal analgesia.9 We recommend that healthcare professionals refrain from engaging in political, polarizing, or highly controversial topics. If a healthcare professional offers their perspective on a political topic, it should be handled with a prudent evidence-based approach.
In addition to maintaining professionalism and remaining vigilant when posting prospective content on social media platforms, healthcare professionals should also spend time to police and monitor what has already been posted to support their online professional persona.10 For instance, previous neglected social media profiles that are not actively managed may be prone to being unknowingly and unintentionally tagged and associated with unprofessional situations. Old content that is forgotten may still be accessed in the future and may potentially reveal past indiscretions. Images of intoxicated or impaired physicians, or involvement with explicit content, while seemingly innocent within proper context, may create distrust in the patient–physician relationship.11 For example, a study of Facebook posts among surgical residents revealed that 12.2% of posts contained unprofessional content that included HIPAA violations, drug use, binge drinking, and sexist or racist content.12 Exceptionally concerning images have even led to formal reprimands by medical boards and employers.7
Best Practice Recommendation #1: It is our recommendation to refrain from posting political content on your professional account. If this an important position for you, then consider a private personal account. Despite a private account there is no guarantee that posts on private social media will not be shared to a broader public view.
Strength of Consensus: A
Best Practice Recommendation #2: It is our recommendation to refrain from posting any image that could suggest intoxication, impairment, or explicit sexual content.
Strength of Consensus: A
Best Practice Recommendation #3: It is our recommendation to hold Best Practice Recommendations #1 and #2 as a rule when giving “likes and shares”, despite a disclaimer that these are not endorsements. Avoid sharing content that can compromise one’s professional image.
Strength of Consensus: A
Patient–Physician Relationship
With social media providing a medium through which people from all walks of life interact, it is not uncommon for physicians and their patients to cross paths online. The management of this interaction is complicated, however, and little guidance has been provided by professional medical societies on how to best proceed. As has been recommended by the American Medical Association and several specialty societies, it is critical for physicians to maintain a boundary between personal and professional relationships with their patients.13–15 Therefore, it is our recommendation that physicians do not solicit or accept “friend requests” on their private social media profiles, where personal information is shared.
If physicians do find it helpful to maintain a social media relationship with their patients for the purposes of disseminating medically related knowledge and marketing, strong consideration should be given to creating a professional social media account. However, it is prudent to remember that physician-patient communications on social media are not privacy-protected and the HIPAA Act of 1996 laws must be followed. Further, specific healthcare recommendations should not be expressed by a physician outside of a formal clinical encounter and certainly should be avoided during online interactions.
While statements such as “posts are not medical advice” are commonly used by physicians online, they provide neither legal nor ethical protection in the event that a patient misconstrues blanket medical advice as specifically targeted towards them without a consideration to their medical history.13,16
Best Practice Recommendation #4: If interacting on a social account with a patient be cautious of the Health Insurance Portability and Accountability Act (HIPAA) and assure you remain compliant with all privacy protection. If possible, limit social interaction with active or former patients, and avoid giving medical advice on these mediums. In addition, it should be noted that “posts do not equal medical advice” is not a legal contract and may not protect you if you make medical opinions in the social media arena.
Strength of Consensus: A
If physicians elect to establish a social media connection with their patients through their professional account, the patients themselves are still using their personal profiles. As such, the physician may have access to private information about patients which may have not been disclosed during clinical encounters.7 In the event that the information gathered will affect a patient’s treatment plan, the physician must approach the patient with honesty on how the information was obtained. This is a sensitive conversation and may negatively impact the physician-patient relationship.13 Thus, it is our strong recommendation that physicians not browse their patient’s social media profiles.
Best Practice Recommendation #5: Physicians should avoid accessing the patient’s social media profile and interacting on any issue that may be deemed personal, medical, or emotional in any way.
Strength of Consensus: A
Patient Privacy
Although HIPAA was passed prior to the advent of social media platforms and does not specifically comment on social media or provide online communication guidelines, its basic principles still apply to a patient’s right to privacy. The application of HIPAA to social media is the same as that of data within an electronic medical record system. Verbal consent is not sufficient and would not withstand medical-legal scrutiny. It is incumbent on the physician to obtain written consent prior to posting patient imaging or procedural photographs.9
If photographs are being used in a post, removing patient identifiers is the paramount. Further removing background items should be considered, particularly if they could be linked to patient. Examples of this may include the specific facility or staff involved, or the specific interventional tools used in the care of that patient. Special consideration should also be given to the fact that the metadata of an image may be enough to link to a specific patient. As such, steps to remove these identifying details should be considered. According to the Consumer Reports organization, “details about when, where, and how a photo was taken are captured automatically by smartphones and digital cameras, and stored as Exif (Exchangeable Image File Format) data”.17 While this information is not easily retrievable, there is certainly a risk of the data being leaked and patient confidentiality become breached.
When posting, consideration must be also taken in “tagging” certain individuals or “hashtagging” subject matter. Often “tagging” a patient, relative, or other involved providers may divulge the identity of a patient even if the post does not include this information explicitly. Using “hashtags” has similar implications and should be used judiciously.
Timing of posts is also an important consideration. Posting on social media shortly after the date of service or visit may allow users to identify the patient involved. Delayed or random posting of work-related topics can allow for more ambiguity when it comes to those involved.
Responses and comments to posts on social media are not often thought of when posting on health related matters involving patients. However, a HIPAA violation may occur when replies or commentary reveal too much information. This may include discussion of involved facilities and offices, referencing specific details of treatment, or even in explaining details of a visit or procedure.
Even with proper consent and considerations, the use of a patient photo or information in a social media post should take into account grander implications. While information and photos can be later deleted from a provider’s account, the photo and information may not necessarily be deleted completely from the internet. Images or content may live on as a cached file or archived content on other website or search engines. The possibility of permanence on the internet should be disclosed to patients during the consenting process.
Best Practice Recommendation #6: Physicians should obtain written consent for use of patient images, photos, or patient testimonials as part of the consent process.
Strength of Consensus: A
Best Practice Recommendation #7: It is strongly recommended that physicians avoid posting procedural images or patient imaging without ensuring all identifying information is removed. When posting images, care must be taken to avoid patient faces and other identifiable features, as well as background persons or items related to the patient.
Strength of Consensus: A
Best Practice Recommendation #8: It is strongly recommended that physicians “pause before posting”. Consider waiting a period of time prior to posting images from recent procedures or surgery; patients browsing social media may be able to identify posts detailing their procedure or surgery in instances where posting occurred soon after their date of service.
Strength of Consensus: A
Industry Relations
One of the many challenges associated with social media specifically as it pertains to specific pharmaceutical agents or medical devices is conflict of interest. Often physicians post “testimonials” of specific devices as their implicit endorsement without disclosing any conflicts that may be present. Furthermore, this endorsement may be misconstrued as medical advice. Indeed, there have been a proliferation of posts offering implicit endorsement of various devices. This is a troubling development and particularly one that is not unique to interventional pain medicine. The absence of disclosures or the presentation of devices without data is particularly problematic, but no standards or policy currently exists.
Perhaps more troubling, is the recent trend where there has also been a proliferation of posts regarding devices or therapies without significant evidence for their support or use and promotion of one “brand” of device over another without any supporting data. In some settings, this has occurred where a method with no evidence is stated to be “just as efficacious” or “better” than a high-level supported method, where the person making the post has implicit conflicts.
Best Practice Recommendation #9: The need for specific guides for physician and industry social media is paramount to better allow for a balanced view of postings. There are several best practices that ASPN makes at the present time that will lead to new standards going forward.
9a. When a company posts an event with physician consultants, the event is obvious to the viewer as company sponsored. No further disclosure is needed by the physician, but the company should obtain physician permission before the posting.
9b. When a physician performs a new procedure, obtains new training, or reports new outcomes with a company sponsored device, it may not be possible to avoid branding. In these instances, if any claim is made as to efficacy, either disclosure or supporting literature should be included in the post.
9c. New innovations may lead to many off label uses, studies, and clinical applications of devices and medications. Company sponsored posts should always indicate if something is off label with appropriate warnings as driven by the respective nation’s regulatory body. Physicians do not have the same responsibility since in normal practice of medicine off label use is often appropriate. It is also not a reasonable expectation for physicians to know the labeling of every device or drug they utilize. If a post presents a new use of a product, with little or no research publications this lack of data should be discussed.
9d. Physicians may choose to disclose that they received fees from manufacturers mentioned in their postings. Since posts are not deemed Continuing Medical Education (CME) there are no disclosure rules that must apply to these actions, therefore the physician’s decision to follow these recommendations are at the discretion of judgement and not legally or professionally binding.
Strength of Consensus: A
Networking and Brand Building
Originating as a vehicle for connection and friendship, social media has evolved into an ideal venue for professional networking and brand building. As such, it is a powerful tool with which interventional pain physicians should become familiar. The large online footprint of sites such as Facebook, Twitter, and Instagram may be leveraged by physicians to become influential researchers, well-regarded clinicians, and to build one’s brand.16,18 In a field as rapidly evolving as pain medicine, it can also be used to keep abreast of the latest publications and advancements in therapies.
Choosing the right social medial platform may be challenging and there is limited data addressing which platform to utilize for which activity. For pain clinicians with an interest in starting a social media presence, a few questions are important to consider, such as who the target audience is and what are the goals of the social media activity. For example, Twitter offers a mean for physicians and scientists to stay connected, share their scholarly activities, engage with the public and advocate for a change with real time reactions. LinkedIn offers an opportunity to expand your network peers and with the medical industry in a professional manner. Meanwhile, a professional or business Instagram account can help optimize a social media presence with a younger generation and enhance business developmental and brand awareness expansion with audiovisual capabilities. A personal Facebook and Instagram account are commonly used to stay in contact with friends and family, but these must be distinguished from business related accounts.
Regardless of the social media platform utilized, building a professional online brand is a key first-step in harnessing the power of social media as a pain physician. Building a brand requires identifying one’s clinical or professional interests.16 It is important to maintain consistency of the brand across all social media platforms so that colleagues and patients can easily recognize and identify the user’s brand. This means that one should consider utilizing the same images, logos, or headshots for all social media services. After doing so, the user should “follow” and engage with established physicians in one’s field or who share similar interests. Posting one’s own content of substantive value is another key manner in which a physician may improve their social media visibility and build their brand. This also allows for engagement with potential patients and as such, informative videos explaining procedures may also be included for educational purposes.
A unique aspect of the field of interventional pain medicine is the volume of clinical research performed by physicians in non-academic settings. Prior to the COVID-19 pandemic, annual society meetings were one of the most common places for physicians to network with one another which would eventually lead to involvement in research projects. As such, many physicians who were not able to attend society meetings did not have opportunities to participate in clinical research projects. Social media has provided a democratic platform for pain medicine physicians of all backgrounds to network with one another and express interest in becoming involved in research studies, publications, society leadership, or to offer their expertise in a number of other ways. Further, it has provided an avenue for trainees who may not have the opportunity for mentorship at their home institutions to seek career guidance from a larger pool of mentors.
Patient Education
Over the past several years, social media has become an important medium through which physicians share health related messages with the public. Unfortunately, only a small percentage of these posts are by interventional pain medicine specialists. Platforms such as Twitter, Instagram, Facebook, and TikTok represent a low-cost and time efficient way for pain physicians to interact with the public. With nearly 65 million Americans classified as medically underserved, social media use is common and can serve as a launch pad for important health and quality of life conversations.19 As a result, studies have found that 34% of Americans turn to the internet to research medical questions they would otherwise have asked a healthcare provider.20 While there are undoubtedly benefits to patients utilizing their available resources, misinformation is rampant. For instance, studies appraising social media platforms regarding pain-related topics revealed widespread misinformation on spinal cord stimulation, epidural analgesia, and manifestations of pain during the COVID-19 pandemic.21–23 By utilizing social media, pain medicine physicians may educate patients directly about a variety of topics including common pain conditions, treatments, as well as new and emerging therapies.
Though marketing is an appropriate use of social media for pain physicians, honest and ethical advertising must be a priority. Anecdotal experiences should not be advertised as generalizable results. This may lead to misinformation and potential harm. Guidelines for appraising the quality and reliability of healthcare-related information have been reported previously and may be used to guide interpretation of healthcare-related social media content.24 This is an especially important consideration given the growing number of novel therapies in our field. At times in interventional pain medicine, the amount of growth is outpacing the data available for its support. While many patients may benefit from these therapies, setting unrealistic expectations may damage trust and decrease perceived effectiveness of a therapy. The pain physician thus has a responsibility to be transparent with the patient and set realistic expectations regarding interventional therapies, as has been further described in the Industry Relations subsection of this manuscript.
Best Practice Recommendation #10: When providing patient education via social media it is critical to offer balanced information concerning the product and appropriate patient selection. When possible, a link should be provided which offers a peer reviewed source or a balanced discussion of the risk-to-benefit ratio.
Strength of Consensus: A
Conclusion
Social media has revolutionized the way people interact with one another on both personal and professional levels. While social media platforms have become immense repositories of information, there are troubling elements regarding the validity of much of this information, in part due to the lack of regulatory guidance. More recently, social media has impacted the way physicians engage with each other, current patients, and potential patients online. While professionalism and ethics guidelines have long existed in the field of medicine, the use of social media mandates special considerations. Previous online and social media guidelines published by medical societies have addressed their specific practitioners, which left a paucity of guidance for interventional pain medicine physicians. In addition, there are aspects unique to our field which lend themselves to greater public scrutiny compared to other medical fields. ASPN supports the need for best practice recommendations in social media use by pain medicine physicians to guide responsible and ethical professional use.
Given the dynamic nature of social media and the rapidity with which it is evolving, we acknowledge that these guidelines are not fully comprehensive. Further innovations in social media may bring forth unprecedented challenges requiring new guidelines in the future. However, it is our hope that these best practice recommendations provide a framework through which interventional pain physicians may be able to interact with one another, and the broader public, so that we live up to the professionalism standards to which we are held by our patients, state medical boards, peers, and the general public.
Disclosure
Dr Mehul J Desai reports Stock Options from SPR Therapeutics, SynerFuse, and Virdio, personal fees, also reports Research Support to Institution from Avanos, Abbott, Averitas, Bioventus, Mainstay Medical, Nalu, Nature Cell, Seikagaku, and Vivex, outside the submitted work. Dr Jonathan M Hagedorn reports personal fees and research funds from Abbott, personal fees from Boston Scientific, personal fees and research funds from Medtronic, personal fees from Nevro, personal fees and research funds from Saluda Medical, outside the submitted work. Dr Erika Petersen reports personal fees from Abbott Neuromodulation, personal fees from Medtronic Neuromodulation, grants, personal fees from Nalu, grants from Nevro, personal fees from Presidio Medical, grants from Saluda, personal fees from Vertos, grants from SPR, also stock options from SynerFuse and neuro.42, personal fees from Biotronik, grants from ReNeuron, grants from Neuros Medical, outside the submitted work. Dr Johnathan H Goree reports personal fees from Abbott, personal fees from Stratus Medical, personal fees from Saluda Medical, outside the submitted work. Dr Jacqueline S Weisbein is consultant and/or researcher for Abbott, Medtronic, Biotronik, Saluda, SI Bone, Vertos, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Pew Research Center. Social media use in 2021; 2021.
2. García-Soidán JL, Leirós-Rodríguez R, Romo-Pérez V, Arufe-Giráldez V. Evolution of the habits of physical activity and television viewing in Spanish children and pre-adolescents between 1997 and 2017. Int J Environ Res Public Health. 2020;17(18):E6836. doi:10.3390/ijerph17186836
3. García-Soidán JL, Boente Antela B, Leirós Rodríguez R. Los menores españoles, en su tiempo libre, prefieren dispositivos electrónicos o actividad física?[Do Spanish minors, in their free time, prefer electronic devices or physical activity?] Sportis Sci J. 2020;6(2):347–364. doi:10.17979/sportis.2020.6.2.6160
4. Ventola CL. Social media and health care professionals: benefits, risks, and best practices. P T. 2014;39(7):491–520.
5. Arora Y, Llaneras N, Arora N, Carillo R. Social media in physician education. Cureus. 2021;13(10):e19081. doi:10.7759/cureus.19081
6. Widmer RJ, Shepard M, Aase LA, Wald JT, Pruthi S, Timimi FK. The impact of social media on negative online physician reviews: an observational study in a large, academic, multispecialty practice. J Gen Intern Med. 2019;34(1):98–101. doi:10.1007/s11606-018-4720-3
7. Statement on guidelines for the ethical use of social media by surgeons [Internet]; 2019 [
8. Clark PA, Capuzzi K, Fick C. Medical marijuana: medical necessity versus political agenda. Med Sci Monit. 2011;17(12):RA249–261. doi:10.12659/MSM.882116
9. Dasgupta N, Beletsky L, Ciccarone D. Opioid crisis: no easy fix to its social and economic determinants. Am J Public Health. 2018;108(2):182–186. doi:10.2105/AJPH.2017.304187
10. Langenfeld SJ, Batra R. How can social media get us in trouble? Clin Colon Rectal Surg. 2017;30(4):264–269. doi:10.1055/s-0037-1604255
11. Devon K, Ganai S. Online medical professionalism. Ann Intern Med. 2013;159(2):157–158. doi:10.7326/0003-4819-159-2-201307160-00019
12. Langenfeld SJ, Cook G, Sudbeck C, Luers T, Schenarts PJ. An assessment of unprofessional behavior among surgical residents on Facebook: a warning of the dangers of social media. J Surg Educ. 2014;71(6):e28–e32. doi:10.1016/j.jsurg.2014.05.013
13. Logghe HJ, Boeck MA, Gusani NJ, et al. Best practices for surgeons’ social media use: statement of the Resident and Associate Society of the American College of Surgeons. J Am Coll Surg. 2018;226(3):317–327. doi:10.1016/j.jamcollsurg.2017.11.022
14. Farnan JM, Snyder Sulmasy L, Worster BK, et al. Online medical professionalism: patient and public relationships: policy statement from the American College of Physicians and the Federation of State Medical Boards. Ann Intern Med. 2013;158(8):620–627. doi:10.7326/0003-4819-158-8-201304160-00100
15. American Medical Association. Professionalism in the use of social media [Internet]. [
16. Ladeiras-Lopes R, Baciu L, Grapsa J, et al. Social media in cardiovascular medicine: a contemporary review. Eur Heart J - Digital Health. 2020;1(1):10–19. doi:10.1093/ehjdh/ztaa004
17. Baker E. EXIF custom: automatic image metadata extraction for scratchpads and drupal. BDJ. 2013;1:e973. doi:10.3897/BDJ.1.e973
18. Goldsweig AM, Galper BZ, Alraies C, et al. Optimal use of social media in interventional cardiology. Catheter Cardiovasc Interv. 2021;98(1):97–106. doi:10.1002/ccd.29643
19. Wieland ML, Beckman TJ, Cha SS, Beebe TJ, McDonald FS. Resident physicians’ knowledge of underserved patients: a multi-institutional survey. Mayo Clin Proc. 2010;85(8):728–733. doi:10.4065/mcp.2009.0703
20. Chen YY, Li CM, Liang JC, Tsai CC. Health information obtained from the internet and changes in medical decision making: questionnaire development and cross-sectional survey. J Med Internet Res. 2018;20(2):e47. doi:10.2196/jmir.9370
21. Langford B, Hooten WM, D’Souza S, Moeschler S, D’Souza RS. YouTube as a source of medical information about spinal cord stimulation. Neuromodulation. 2021;24(1):156–161. doi:10.1111/ner.13303
22. D’Souza RS, D’Souza S, Sharpe EE. YouTube as a source of medical information about epidural analgesia for labor pain. Int J Obstet Anesth. 2021;45:133–137. doi:10.1016/j.ijoa.2020.11.005
23. D’Souza RS, Kilgore AE, D’Souza S. Manifestations of pain during the COVID-19 pandemic portrayed on social media: a cross-sectional study. Pain Med. 2022;23(2):229–233. doi:10.1093/pm/pnab305
24. D’Souza RS, Daraz L, Hooten WM, Guyatt G, Murad MH. Users’ guides to the medical literature series on social media (part 1): how to interpret healthcare information available on platforms. BMJ EBM. 2022;27(1):11–14. doi:10.1136/bmjebm-2021-111817
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Social Media Usage by Dental Practitioners of Pakistan for Professional Purposes – A Cross-Sectional Study
Ghandhi D, Bodani N, Lal A, Maqsood A, Ahmed N, Basha S, Assiry AA, Heboyan A, Karobari MI
Clinical, Cosmetic and Investigational Dentistry 2022, 14:245-252
Published Date: 10 August 2022
The Impact of Social Media Influencers on Food Consumption in Saudi Arabia, a Cross-Sectional Web-Based Survey
Alwafi H, Alwafi R, Naser AY, Samannodi M, Aboraya D, Salawati E, Alqurashi A, Ekram R, Alzahrani AR, Aldhahir AM, Assaggaf H, Almatrafi M
Journal of Multidisciplinary Healthcare 2022, 15:2129-2139
Published Date: 23 September 2022
Instagram and Aesthetic Dentistry: A Study of Content and Engagement Among Arabic Posts Related to Dental Smile
AlSheikh RN, Albalawi MA, AlHumaid GA, Alsahiem JK, Alotaibi DA, Al-Swuailem AS, Halawany HS, Al-Khalifa KS
Clinical, Cosmetic and Investigational Dentistry 2025, 17:135-146
Published Date: 19 February 2025
Content Analysis of a Congenital Cataract Social Media Support Group
Zhou A, Kraus CL
Clinical Ophthalmology 2025, 19:4099-4105
Published Date: 6 November 2025