Back to Journals » Clinical Ophthalmology » Volume 20
Smoking and Risk of Vision Threatening Complications: A Global Database Analysis
Authors Gad El Sayed M, Vu Pham N, Bandaru D, Abboud I ![]() , Zakhary MB, Zakhary M, Bishay RGE
, Zakhary MB, Zakhary M, Bishay RGE ![]() , Rezaei K, Khaksar P, Enciso J, Tran K, Martinez SJ
, Rezaei K, Khaksar P, Enciso J, Tran K, Martinez SJ ![]() , Mikhail K
, Mikhail K ![]() , Glendrange RR, Fouad Y
, Glendrange RR, Fouad Y ![]()
Received 6 February 2026
Accepted for publication 27 March 2026
Published 2 April 2026 Volume 2026:20 596936
DOI https://doi.org/10.2147/OPTH.S596936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Sotiria Palioura
Marina Gad El Sayed,1 Nathan Vu Pham,2 Dhiresh Bandaru,1 Ibrahim Abboud,1 Maria Bahaa Zakhary,3 Michael Zakhary,3 Rose Gloriana Emad Bishay,1 Kimia Rezaei,1 Parsa Khaksar,4 Jonathan Enciso,1 Khanh Tran,5 Stephanie J Martinez,1 Kirellos Mikhail,6 Ray R Glendrange,1,7 Yousef Fouad8
1School of Medicine, University of California Riverside, Riverside, CA, USA; 2David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA, USA; 3Department of Biology, Chaffey College, Rancho Cucamonga, CA, USA; 4School of Medicine, Virginia Tech Carilion School of Medicine, Roanoke, VA, USA; 5School of Medicine, University of California, Irvine, CA, USA; 6Cardiology Department, UCLA Cardiac Arrhythmia Center, Los Angeles, CA, USA; 7Ophthalmology Department, Riverside Eye Specialists, Riverside, CA, USA; 8Department of Ophthalmology, Ain Shams University Hospitals, Cairo, Egypt
Correspondence: Yousef Fouad, Department of Ophthalmology, Ain Shams University Hospitals, Cairo, 11517, Egypt, Tel +201063781237, Email [email protected]
Purpose: To investigate the association between smoking and the incidence of vision-threatening conditions, including cataract, glaucoma, diabetic retinopathy (DR), age-related macular degeneration (AMD), retinal vascular occlusion, uveitis, and ischemic optic neuropathy (ION) in a large real-world database to provide quantitative risk estimates to inform smoking cessation counseling.
Methods: A retrospective cohort study was conducted using the TriNetX electronic health records platform, analyzing 12,183,254 patients. Patients were categorized into smokers (n = 304,823) and non-smokers (n = 11,878,431), and then a propensity score matching was utilized to balance both groups for demographic features and vascular risk factors. The incidence rates of the studied ocular conditions were then compared over a ten-year period using risk ratios (RR).
Results: Matched cohorts included 300,867 patients per group. Smokers exhibited a significantly higher 10-year risk for all studied ophthalmic outcomes (p < 0.0001). The strongest associations were observed for posterior subcapsular cataract (RR 2.60; 95% CI, 2.41– 2.82), uveitis (RR 2.43 [2.25– 2.63]), and retinal vascular occlusions (CRAO: RR 2.35; CRVO: RR 2.16). Increased risks were also consistent across glaucoma subtypes (RR 1.57– 2.47), AMD (RR 1.85), and diabetic retinopathy (RR 1.21).
Conclusion: Smoking is significantly associated with an increased risk of multiple vision-threatening ocular diseases. These findings highlight the need for ophthalmologists and public health professionals to incorporate smoking history into risk stratification and screening programs and to emphasize ocular health during smoking cessation counseling.
Keywords: smoking, counseling, vision loss, vision impairment
Introduction
Smoking exposes the body to over 4000 toxic compounds that induce oxidative stress and promote chronic inflammation in tissues, including ocular tissues, leading to degradation of their integrity. Smoking has been linked to increased retinal ischemia, microvascular dysfunction, and direct toxic effects to the optic nerve. The chemicals released by tobacco smoke inhalation may also damage mitochondrial DNA in the retinal cells contributing to the increased likelihood of their degeneration.1,2
Smoking has been strongly linked to the development of various ocular pathologies, including cataract, age-related macular degeneration (AMD), and thyroid eye disease. Other less-established associations include diabetic retinopathy (DR), ischemic optic neuropathy (ION), and retinal vascular occlusions.2,3 Fear of blindness has been found to be as strong a motivation for quitting among smokers, equivalent to the fear of stroke, lung cancer, and cardiac disorders.4 Nevertheless, most ophthalmologists do not ask patients about smoking status nor discuss motivation for smoking cessation, and there is a general lack of support at eye care centers for patients willing to quit.5
To provide proper counseling, ophthalmologists should be aware of the magnitude of increased risk for various eye disorders associated with smoking. Conflicting associations could be found in the literature, possibly due to different small sample sizes and population characteristics such as ethnic variation or confounding comorbidities.3 This study aims to explore the link between smoking and vision-threatening ocular conditions by analyzing the risk magnitude for the major ocular conditions, namely: cataract, glaucoma, AMD, DR uveitis, retinal vascular occlusion, and ION.
Methods
This retrospective multicentric cohort study was conducted using the TriNetX Global Federated Research Network, a large-scale real-world data platform aggregating de-identified electronic medical records (EMRs) from over 200 healthcare organizations across the United States and internationally. At the time of data extraction, the US Collaborative Network requested information from 68 HCOs, all of which responded with clinical data.
Ethical approval for this study was acquired from the University of California Riverside Office of Research Integrity (protocol approval number #30442). The research was classified as non-human subjects research with exemption from informed consent (anonymized retrospective database analysis with no intervention nor interaction with patients). The TriNetX network adheres to HIPAA regulations and is ISO 27001:2013 certified.
Patients who had at least one encounter with an ophthalmologist were categorized into two cohorts. Cohort A (non-smokers) consisted of 11,878,431 individuals with no recorded diagnosis, procedure, or laboratory result indicative of tobacco use, as verified through documentation (international classification of diseases [ICD]-10 codes) of general adult medical exams and absence of tobacco-related terms in their EMRs. Cohort B (Smokers) included 304,823 individuals with documented evidence of smoking or tobacco use based on clinical diagnoses (eg, nicotine dependence), or procedures (eg, smoking cessation counseling). Index events were defined as the earliest date on which patients met the inclusion criteria for each cohort. Patients whose index event occurred more than 20 years prior to the analysis were excluded to ensure temporal relevance, although no patients were excluded for this reason in the final cohort.
A 1:1 propensity score matching for age, sex, hypertension, and diabetes mellitus was utilized to create balanced cohorts (Table 1). The primary objective was to evaluate the incidence (new cases) of key vision-threatening ocular diseases over a 10-year observational period (3653 days) following the index event using the respective ICD-10 codes, including cataract (all types), glaucoma (ocular hypertension, open angle glaucoma [OAG], and primary angle closure glaucoma [PACG]), AMD (nonexudative and exudative), DR (non-proliferative [NPDR] and proliferative [PDR]), retinal vein occlusion (RVO, central [CRVO] and branch [BRVO]), retinal artery occlusion (RAO, central [CRAO] and branch [BRAO]), uveitis, and ION.
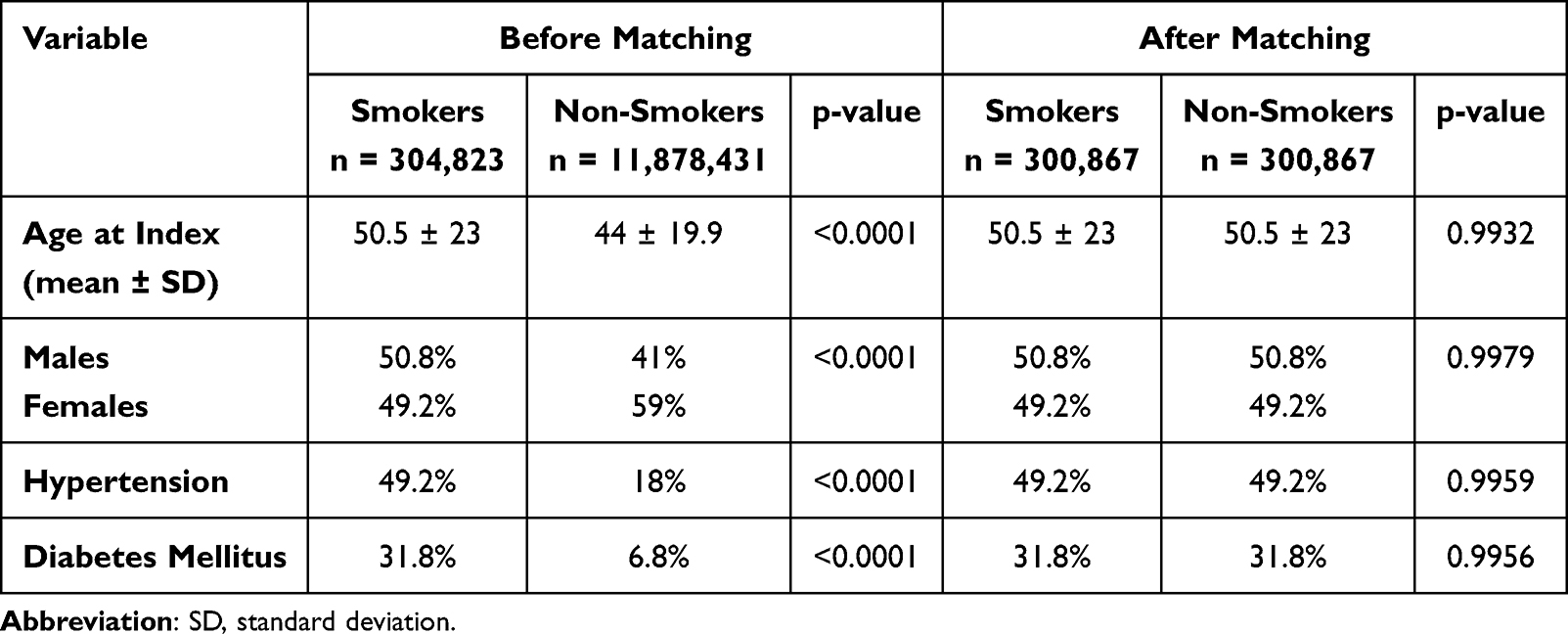 |
Table 1 Propensity Score Matching to Balance Both Cohorts |
TriNetX’s built-in analytics suite was used for statistical analysis. Risk ratios (RR) and odds ratios (OR) were computed for each outcome. These values were visualized using bar charts comparing disease incidence across cohorts. Confidence intervals (95% CI) and p-values were reported, and significance was determined at a two-sided threshold of p < 0.001 for all major outcomes.
Results
A total of 12,183,254 patients were included for 1:1 propensity score matching on demographic features and cardiac risk factors, yielding balanced cohorts of 300,867 individuals each for smoking and non-smoking status across all analyses. The risk and odds ratio for the different outcomes are given in Table 2.
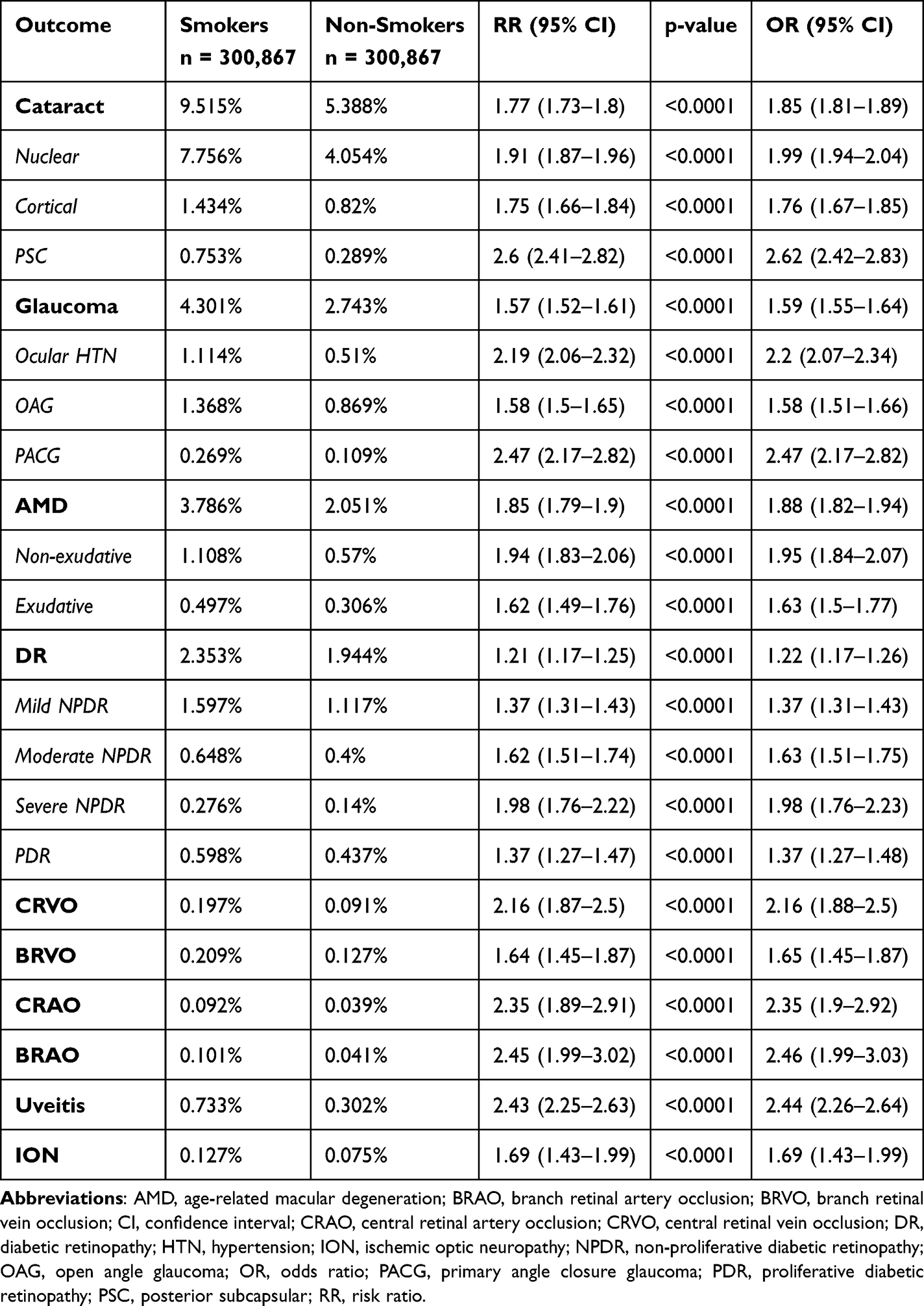 |
Table 2 Risk and Odds Ratio for Different Outcomes in the Smokers versus Non-Smokers Cohorts |
Cataract
Among patients without prior cataract, 9.5% of smokers compared to 5.4% of non-smokers developed new cataract during the 10-year follow-up (RR: 1.77, 95% CI: 1.73–1.8, p < 0.0001). The highest risk was observed for the posterior subcapsular type (RR: 2.6), followed by nuclear cataract (RR: 1.91) and cortical cataract (RR: 1.75).
Glaucoma
Overall incidence of glaucoma was 4.3% in smokers compared to 2.7% in non-smokers. The RR was 1.57 (95% CI: 1.52–1.61, p < 0.0001). The risk was highest for PACG (RR: 2.47), followed by ocular hypertension (RR: 2.19) and open angle glaucoma (RR: 1.58).
Age-Related Macular Degeneration
The 10-year incidence of AMD was significantly higher among smokers (3.8%) compared to non-smokers (2.1%, RR: 1.85, 95% CI: 1.79–1.9, p < 0.0001). Risk was higher for developing non-exudative AMD (RR: 1.85) compared to exudative AMD (RR: 1.62).
Diabetic Retinopathy
Smokers had a significantly higher 10-year incidence of DR (2.4%) compared to non-smokers (1.9%, RR: 1.21, 95% CI: 1.17–1.25, p < 0.0001). Risk was significantly higher for all types of NPDR (mild [RR: 1.37], moderate [RR: 1.62], and severe [RR: 1.98]) and for PDR (RR: 1.37).
Retinal Vascular Occlusion
Smoking significantly increased the risk of all forms of retinal vascular occlusion (Figure 1). The highest risk was seen for BRAO (RR: 2.45, 95% CI: 1.99–3.02, p < 0.0001), followed by CRAO (RR: 2.35, 1.89–2.91, p < 0.0001), CRVO (RR: 2.16, 1.87–2.5, p < 0.0001), and BRVO (RR: 1.64, 1.45–1.87, p < 0.0001).
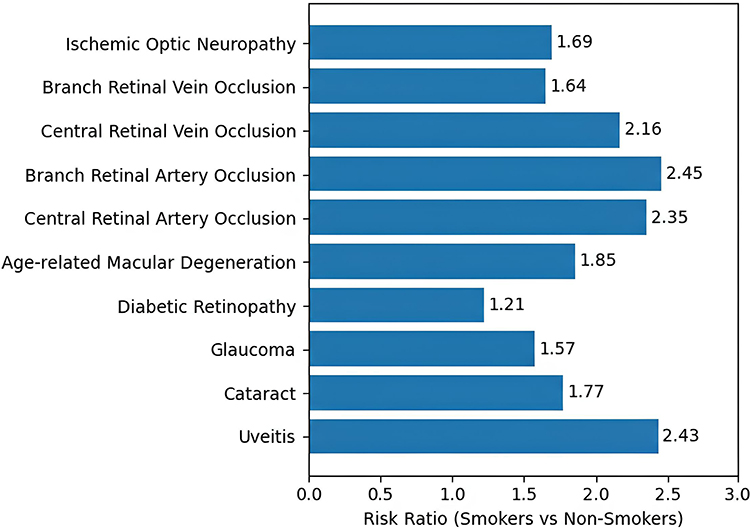 |
Figure 1 Diagram showing risk ratios for the main outcomes in the smokers group compared to the non-smokers group. |
Ischemic Optic Neuropathy
Incident ION was diagnosed in 0.13% of smokers versus 0.08% of non-smokers. The RR was 1.69 (95% CI: 1.43–1.99, p < 0.001).
Uveitis
Smokers had a significantly higher 10-year incidence rate of uveitis compared to non-smokers (0.7% vs. 0.3%, RR: 2.43, 95% CI: 2.25–2.63, p < 0.0001).
Discussion
In this large database analysis, we found that smoking was a significant risk factor for the development of the major vision-threatening ocular conditions over 10 years of follow-up, with more than a two-fold increased risk of posterior subcapsular cataract, PACG, ocular hypertension, CRVO, CRAO, BRAO, and uveitis and more than a 1.5-fold increased risk of nuclear and cortical cataract, AMD, OAG, and ION, and 1.2-fold the risk of developing DR. Our findings highlight the need for counseling of ophthalmology patients about smoking cessation and offer numbers that can help in such counseling.
We found an increased risk of cataract among smokers compared to non-smokers (1.8 fold). This is consistent with prior literature supporting that smoking is a significant modifiable risk factor for cataract development, where the odds ratio ranged from 1.6 for posterior subcapsular cataract to 1.8 for nuclear cataract.1,6 In our analysis, however, the posterior subcapsular subtype had the highest risk. The pathogenesis is likely related to the accumulation of harmful ions like vanadium, aluminum, and cadmium, the increased reactive oxygen species in the lens, and reduced systemic antioxidants. These factors all contribute to opacification and lens protein degradation.7
We also found a significant risk of glaucoma among smokers compared to non-smokers (1.6 fold), particularly PACG (2.5 fold). Studies on association between smoking and the risk of glaucoma or ocular hypertension have yielded mixed results. While some studies found a significant positive association with primary OAG,8,9 other studies reported no association,10 or even a protective one.11,12 A recent systematic review and meta-analysis explored the association between smoking and primary OAG risk and found no significant association.13 However, most of the included studies did not achieve low bias risk, highlighting the need for further research on the topic. The association between smoking and PACG is less studied, and a lack of association between smoking and ACG severity has similarly been reported.14 Our study, thus, provides exploratory real-world data on a possible association.
Our results indicated a significant association between smoking and both forms of AMD. This aligns with the literature showing an established association between smoking and an increased risk of both the incidence of new AMD and the progression to advanced stages (exudative AMD and geographic atrophy).15–17 The pathogenesis is suggested to relate to an inflammatory microenvironment with reactive oxygen species, and mitochondrial DNA damage with accumulation of degradation products in the retinal pigment epithelial cells.18
The incidence of DR, both NPDR and PDR, was significantly higher among smokers, although the risk was lowest (1.21 fold) compared to other outcomes. Smoking has not been thoroughly investigated in association with DR, but some limited old studies seem to suggest no association.19–21 A more recent review concluded a significant association between smoking and DR in type 1 but not type 2 diabetes mellitus.22 The pathogenesis of vascular pathology may be related to the vasoconstrictive properties of nicotine and increased carboxyhemoglobin as a result of smoking cause a reduction in retinal blood flow which exacerbates retinal hypoxia.23 These effects may also explain the increased risk of retinal vascular occlusion (RVO and RAO) and ION in our study among smokers compared to non-smokers, which is consistent to prior literature reports.24–26
We also found that smokers had a significantly higher risk of developing uveitis compared to non-smokers (2.4 fold). This is consistent with findings from a recent meta-analysis that found nearly two-fold increased odds of uveitis among smokers.27 Taken together, this suggests that smoking is a key modifiable risk factor for uveitis development and carries implications to the counseling of patients suffering intraocular inflammation.
The strength of the study is the large sampling of real-world data that allows the exploration of the weight of each interplaying risk factor. However, the retrospective methodology of this study and the reliance on data from EMRs introduce several limitations. Calculating smoking status based on recorded diagnoses, procedures, or test data may underestimate the study population due to underreporting. Furthermore, stratified risk assessment among present versus former smokers was not possible due to the study’s lack of detail regarding smoking quantity, duration, type of tobacco used, and time since cessation. Even when major cardiovascular risk factors (hypertension and diabetes) were matched using a propensity score, other residual confounding remains a challenge. The smoker-dominated population was more likely to have obesity and dyslipidemia, and unmeasured factors such as alcohol intake, socioeconomic level, dietary intake, or access to eye care may have influenced the outcomes. Finally, given the observational nature of this study, these findings should be interpreted as associations rather than evidence of a direct causal relationship between smoking and the identified ophthalmic conditions.
In conclusion, smoking was significantly associated with an increased risk of multiple vision-threatening ocular diseases. These findings highlight the need for ophthalmologists and public health professionals to incorporate smoking history into risk stratification and screening programs and to emphasize ocular health during smoking cessation counseling.
Data Sharing Statement
The data analyzed in this study are available from the TriNetX registry. Restrictions apply to the availability of these data, which were used under license from the University of California Riverside. Data are available from the authors with the permission of TriNetX.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kai JY, Zhou M, Li DL, et al. Smoking, dietary factors and major age-related eye disorders: an umbrella review of systematic reviews and meta-analyses. Br J Ophthalmol. 2022;108(1):51–7. doi:10.1136/bjo-2022-322325
2. Galor A, Lee DJ. Effects of smoking on ocular health. Curr Opinion Ophthalmol. 2011;22(6):477–482. doi:10.1097/icu.0b013e32834bbe7a
3. Asiamah R, Ampo E, Ampiah EE, et al. Impact of smoking on ocular health: a systematic review and meta-meta-analysis. Eur J Ophthalmol. 2025;16:11206721251334705. doi:10.1177/11206721251334705
4. Bidwell G, Sahu A, Edwards R, et al. Perceptions of blindness related to smoking: a hospital-based cross-sectional study. Eye. 2005;19(9):945–948. doi:10.1038/sj.eye.6701955
5. Sahu A, Edwards R, Harrison RA, Thornton J, Kelly SP. Attitudes and behaviour of ophthalmologists to smoking cessation. Eye. 2008;22(2):246–250. doi:10.1038/sj.eye.6702592
6. Ye J, He J, Wang C, et al. Smoking and risk of age-related cataract: a meta-analysis. Invest Ophthalmol Visual Sci. 2012;53(7):3885. doi:10.1167/iovs.12-9820
7. Langford-Smith A, Tilakaratna V, Lythgoe PR, et al. Age and smoking related changes in metal ion levels in human lens: implications for cataract formation. PLoS One. 2016;11(1):e0147576. doi:10.1371/journal.pone.0147576
8. Pérez-de-arcelus M, Toledo E, Martínez-González MÁ, Martín-Calvo N, Fernández-Montero A, Moreno-Montañés J. Smoking and incidence of glaucoma: the SUN cohort. Medicine. 2017;96(1):e5761. doi:10.1097/MD.0000000000005761
9. Mahmoudinezhad G, Nishida T, Weinreb RN, et al. Associations of smoking and alcohol consumption with the development of open angle glaucoma: a retrospective cohort study. BMJ open. 2023;13(10):e072163. doi:10.1136/bmjopen-2023-072163
10. Khalili AF, Razzaghi S, Motlagh BF, et al. Prevalence of primary open-angle glaucoma and its relationship with smoking in the population of the Azar cohort: a cross-sectional study. Middle East Afr J Ophthalmol. 2023;29(3):109–115. doi:10.4103/meajo.meajo_101_22
11. Kang JH, Pasquale LR, Rosner BA, et al. Prospective study of cigarette smoking and the risk of primary open-angle glaucoma. Arch Ophthalmol. 2003;121(12):1762–1768. doi:10.1001/archopht.121.12.1762
12. Law SM, Lu X, Yu F, et al. Cigarette smoking and glaucoma in the United States population. Eye. 2018;32(4):716–725. doi:10.1038/eye.2017.292
13. Niven TCS, Azhany Y, Rohana AJ, et al. Cigarette smoking on severity of primary angle closure glaucoma in Malay patients. J Glaucoma. 2019;28(1):7–13. doi:10.1097/IJG.0000000000001120
14. Yee H, Adkins S. Cigarette smoking and its association with primary open angle glaucoma: a systematic review and meta-analysis. Ophthalmic Epidemiol. 2025;32(4):361–373. doi:10.1080/09286586.2024.2391028
15. Klein R, Knudtson MD, Cruickshanks KJ, Klein BEK. Further observations on the association between smoking and the long-term incidence and progression of age-related macular degeneration: the beaver dam eye study. Arch Ophthalmol. 2008;126(1):115–121. doi:10.1001/archopht.126.1.115
16. Tan JSL, Mitchell P, Kifley A, et al. Smoking and the long-term incidence of age-related macular degeneration: the blue mountains eye study. Arch Ophthalmol. 2007;125(8):1089–1095. doi:10.1001/archopht.125.8.1089
17. Chakravarthy U, Augood C, Bentham GC, et al. Cigarette smoking and age-related macular degeneration in the EUREYE Study. Ophthalmology. 2007;114(6):1157–1163. doi:10.1016/j.ophtha.2006.09.022
18. Wang AL, Lukas TJ, Yuan M. Changes in retinal pigment epithelium related to cigarette smoke: possible relevance to smoking as a risk factor for age-related macular degeneration. PLoS One. 2009;4(4):e5304.
19. Klein R, Klein BE, Davis MD. Is cigarette smoking associated with diabetic retinopathy? Am J Epidemiol. 1983;118(2):228–238. doi:10.1093/oxfordjournals.aje.a113630
20. Moss SE, Klein R, Klein BE. Cigarette smoking and ten-year progression of diabetic retinopathy. Ophthalmology. 1996;103(9):1438–1442. doi:10.1016/s0161-6420(96)30486-7
21. Gaedt Thorlund M, Borg Madsen M, Green A, Sjølie AK, Grauslund J. Is smoking a risk factor for proliferative diabetic retinopathy in type 1 diabetes? Ophthalmologica. 2013;230(1):50–54. doi:10.1159/000350813
22. Cai X, Chen Y, Yang W, et al. The association of smoking and risk of diabetic retinopathy in patients with type 1 and type 2 diabetes: a meta-analysis. Endocrine. 2018;62(2):299–306. doi:10.1007/s12020-018-1697-y
23. Morgado PB, Chen HC, Patel V, Herbert L, Kohner EM. The acute effect of smoking on retinal blood flow in subjects with and without diabetes. Ophthalmology. 1994;101(7):1220–1226. doi:10.1016/s0161-6420(94)31185-7
24. Kolar P. Risk factors for central and branch retinal vein occlusion: a meta-analysis of published clinical data. J Ophthalmol. 2014;2014(1):724780. doi:10.1155/2014/724780
25. Pothikamjorn T, Charnnarong C, Susantitaphong P, Jariyakosol S. Incidence and risk factors associated with ischemic cerebrovascular disease in patients with retinal artery occlusion: a systematic review and meta-analysis. Sci Rep. 2025;15(1):33244. doi:10.1038/s41598-025-18419-7
26. Kemchoknatee P, Tangon D, Srisombut T. Risk factors of developing non-arteric ischemic optic neuropathy in patients with type 2 diabetes mellitus: a single-center retrospective cohort study. Int J Ophthalmol. 2025;18(2):290–296. doi:10.18240/ijo.2025.02.13
27. Kuč S, Drent M, Erckens R, et al. Smoking and risk of uveitis: a systematic review and meta-analysis. Ocul Immunol Inflamm. 2025;24:1–8. doi:10.1080/09273948.2025.2574484
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Visual Outcomes, Spectacle Independence, and Patient-Reported Satisfaction of the Vivity Extended Range of Vision Intraocular Lens in Patients with Early Glaucoma: An Observational Comparative Study
Kerr NM, Moshegov S, Lim S, Simos M
Clinical Ophthalmology 2023, 17:1515-1523
Published Date: 30 May 2023
Demographic, Socioeconomic, and Clinical Factors Associated with Severe Vision Loss in Patients with Neovascular Glaucoma
Cotton CC, Goerl BA, Kaplan EF, Krause MA
Clinical Ophthalmology 2024, 18:2137-2145
Published Date: 19 July 2024
Bio-Interventional Cyclodialysis and Allograft Scleral Reinforcement for Uveoscleral Outflow Enhancement in Open-Angle Glaucoma Patients: One-Year Clinical Outcomes
Ianchulev T, Weinreb RN, Calvo EA, Lewis J, Kamthan G, Sheybani A, Rhee DJ, Ahmed IK
Clinical Ophthalmology 2024, 18:3605-3614
Published Date: 6 December 2024
Fear of Cataract Surgery and Vision Loss: The Effects of Health Literacy and Patient Comprehension at an Academic Hospital-Based Eye Clinic
Hu S, Wey S, Yano RA, Kelly LD
Clinical Ophthalmology 2025, 19:1103-1110
Published Date: 28 March 2025