Back to Journals » Journal of Pain Research » Volume 19
Smartphone-Based Acceptance and Commitment Therapy for Postmastectomy Pain Syndrome: A Pilot RCT Evaluating Feasibility, Acceptability, and Preliminary Clinical Outcomes
Authors Sakai M, Toyama T, Hashimoto H ![]() , Ueno T, Wanifuchi-Endo Y, Fujita T
, Ueno T, Wanifuchi-Endo Y, Fujita T ![]() , Asano T, Horisawa N, Uchida M
, Asano T, Horisawa N, Uchida M ![]() , Akechi T
, Akechi T
Received 25 November 2025
Accepted for publication 17 April 2026
Published 21 May 2026 Volume 2026:19 574843
DOI https://doi.org/10.2147/JPR.S574843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rocío de la Vega
Mie Sakai,1 Tatsuya Toyama,2 Hiroya Hashimoto,3 Taro Ueno,4 Yumi Wanifuchi-Endo,2 Takashi Fujita,2 Tomoko Asano,2 Nanae Horisawa,2 Megumi Uchida,1 Tatsuo Akechi1
1Department of Psychiatry and Cognitive-Behavioral Medicine, Nagoya City University Graduate School of Medical Sciences, Nagoya, Aichi, Japan; 2Department of Breast Surgery, Nagoya City University Graduate School of Medical Sciences, Nagoya, Aichi, Japan; 3Depatment of Biostatistics, Nagoya University Graduate School of Medicine, Nagoya, Aichi, Japan; 4SUSMED Inc, Chuo-ku, Tokyo, Japan
Correspondence: Tatsuo Akechi, Department of Psychiatry and Cognitive-Behavioral Medicine, Nagoya City University Graduate School of Medical Sciences, 1 Kawasumi, Mizuho-cho, Mizuho-ku, Nagoya, Aichi, 467-8601, Japan, Tel +81-52-851-5511, Fax +81-52-852-0837, Email [email protected]
Objective: This study examined the feasibility and potential acceptability, with exploratory assessment of its effects on pain interference and fear of recurrence, of a smartphone-based acceptance and commitment therapy (ACT) intervention to reduce pain interference and fear of recurrence in breast cancer survivors.
Methods: This single-center, parallel-group, randomized controlled pirot trial included breast cancer survivors with postmastectomy pain syndrome who were randomly allocated to an ACT intervention group or control group in a 1:1 ratio. Of the 57 patients screened, 45 were randomly assigned to the ACT group (n = 22) and the control group (n = 23). The ACT app offered an 8-week program with outcome measures for before and after the intervention. Primary outcomes were feasibility and adherence, assessed by intervention completion rate, participants’ perceived usefulness, and satisfaction. Secondary outcomes included exploratory clinical measures assessed before and after the intervention.
Results: The intervention completion rate for the ACT group was 100%, and the degree to which patients’ needs were met and their overall satisfaction was high (> 60%). One minor adverse event was reported, but the patient had already recovered by the time of the interview stage, and the event was considered minor. No significant improvements were observed in clinical outcomes.
Discussion: The results demonstrate the feasibility and acceptability of smartphone-based ACT interventions. Clinical efficacy was not demonstrated and should be evaluated in future trials with adequately powered samples and participants with higher levels of pain interference.
Keywords: postmastectomy pain syndrome, acceptance and commitment therapy, cancer survivor, mobile health, decentralized clinical trial
Introduction
Breast cancer is one of the most common cancers among women. Early detection and individualized medical treatment have improved survival rates. The 10-year survival rate for this demographic is now 79.3%, suggesting improvements.1 Despite progress in its treatment, patients experience various distressing symptoms post-treatment, including postoperative pain. Approximately 20%–50% of patients with breast cancer who have undergone surgery reported chronic, persistent pain, called post-mastectomy pain syndrome (PMPS), which negatively affects employment, causes fear of recurrence, and reduces quality of life (QOL).2 In a study of 305 breast cancer survivors (mean age, 52.5 years; mean duration of surgery, 67.1 months), 51% of outpatient recurrence-free survivors who were more than one year postoperative had PMPS, and 39% of these survivors needed treatment.3 Needs for PMPS treatment were present in 20% of outpatient, recurrence-free breast cancer survivors.3 Pain in two or more regions and a high fear of recurrence are predictors of a need for PMPS treatment; developing effective treatments will relieve both pain and psychiatric symptoms.3 Hence, a cross-diagnostic treatment for pain and psychological symptoms is necessary. Nerve blocks, antidepressants, physical therapy, and psychotherapy have been attempted, and multidisciplinary treatment notably improves PMPS management.4
Acceptance and commitment therapy (ACT) demonstrates multifaceted efficacy for chronic pain. Recent meta-analyses for chronic pain have shown the effects of ACT on pain acceptance, QOL, pain-related functioning, pain intensity, anxiety, and depression.5 Investigations regarding the prophylactic effect on PMPS6 show that ACT was administered two weeks post-surgery to determine whether prevention occurred. The results showed that a single ACT intervention session produced small positive effects on postoperative pain and anxiety. Regarding fear of recurrence, the three-arm pilot randomized controlled trial (RCT) survivorship education program enhanced care and ACT showed a significant reduction in fear of recurrence in the ACT group.7 ACT is thus a cross-diagnostic approach8 and an appropriate intervention for this study on multiple symptom clusters. We confirmed the effectiveness of ACT in a case study conducted in a face-to-face format for a patient presenting with multiple psychological and physical symptoms, including PMPS, fear of recurrence, and depression.9
One recent study demonstrated significant improvements in pain interference with smartphone-delivered ACT interventions.10 The study consisted of 34 adults with long-standing chronic pain treated over eight weeks, but did not establish a comparison group.10 A related study tested a smartphone-delivered ACT program for fibromyalgia management.11 Participants were randomly assigned to the ACT group (n = 140) and the active control group (n = 135), with treatment lasting 12 weeks. After the treatment, 71% of ACT participants reported improvement versus 22% of active control participants, corresponding to a difference in proportion of 48%.11 However, there is no smartphone-based intervention that targets multiple symptom clusters such as PMPS and fears of recurrence.
Given the scarcity of specialized psychotherapy providers in Japan, a recent distributed clinical trial successfully utilized a cognitive-behavioral therapy application to address fears of cancer recurrence,12 while other digital ACT programs have been developed for chronic pain management.13 Furthermore, many survivors in the PMPS population are in the prime of their working lives or manage demanding roles in childcare and eldercare, making frequent hospital visits for in-person sessions physically and logistically challenging. For these individuals, physical pain is often inextricably linked to realistic anxieties regarding recurrence or metastasis. In such contexts, ACT may be uniquely effective compared to traditional CBT, which emphasizes reality testing of thought content. Rather than focusing on the validity of these realistic fears, ACT targets cognitive fusion and experiential avoidance, fostering the psychological flexibility necessary for patients to navigate health-related uncertainty and coexist with their anxieties. Accordingly, this randomized study examined the feasibility and potential acceptability of smartphone-based ACT interventions, with exploratory assessment of its effects on pain interference and fears of recurrence among breast cancer survivors in a pilot RCT.
Methods
Design
The study employed a single-center, two-armed, parallel-group, RCT. Participants were female breast cancer survivors with PMPS who were recruited through breast oncologists at Nagoya City University Hospital’s outpatient clinic in Nagoya, Japan. Ethical approval was granted by the Nagoya City University Graduate School of Medical Sciences Institutional Review Board (reference number: 46–22-0011). The trial was prospectively registered on the University Hospital Medical Information Network (Smartphone Acceptance and commitment therapy to Keep mind sUpple for Relief of post mAstectomy pain syndrome in breast cancer patients: A randomized controlled trial using an innovative decentralized platform (preliminary study); UMIN000051315).
Participants
Fifty-seven patients were screened. The inclusion criteria were: (1) patients must have been diagnosed with breast cancer; (2) patients had to be recurrence-free for at least one year post-mastectomy; (3) patients must 18 years or older at the time of obtaining consent; (4) patients had to have experienced PMPS (pain in the surgical site, axilla, or arm on the operated side since operation, in the back or abdomen following reconstruction, etc.) for at least one year since reconstruction; (5) patients had to be able to install the ACT app by themselves on an Android or iOS mobile device (Android 6.0 or higher, and iOS 13.0 or higher) and know how to use a smartphone.
The exclusion criteria for participation were: (1) patients who could not read or write Japanese; (2) patients who had pain for reasons other than cancer and were undergoing treatment for it; (3) patients who had pain in areas other than the wound, armpit, or arm and were being treated for it; (4) patients with psychiatric symptoms that the investigators considered inappropriate for participation, including dementia, cognitive dysfunction, severe depression with suicidal ideation, poorly-controlled schizophrenia, or schizoaffective disorder; (5) patients with serious a physical illness (eg, serious respiratory, cardiovascular, nervous system, or musculoskeletal illnesses) that could make psychotherapy difficult; (6) patients who had received ACT in the past; (7) other patients deemed inappropriate by the principal or co-principal investigator.
Procedures
This study was conducted in accordance with the principles of the Declaration of Helsinki. This study was conducted as a decentralized clinical trial (DCT), in which healthcare providers distribute leaflets to patients inviting them to participate in a clinical study and incorporating electronic informed consent (e-consent). Electronic informed consent (e-consent) was obtained through a secure web-based platform. Participants accessed detailed study information provided on a dedicated study website via their smartphones. Identity verification was performed by confirming patient identification using submitted images of their medical identification cards. Participants were provided with contact information for the study office and were able to ask questions via telephone or Email prior to providing consent. Informed consent was obtained electronically and recorded within the system. All data were handled securely to ensure confidentiality and privacy. All interventions and patient-reported outcomes (ePRO) can be performed via smartphones. DCTs are highly valued by patients because they reduce time costs, and they can significantly reduce the burden on physicians in terms of explanation time for clinical research. The investigators established a system of DCT in our previous studies12 with Accelight Inc., Japan, and utilized this system for the present study.
Collaborating breast oncologists were asked to distribute study leaflets to their patients with PMPS. Interested patients were invited to access the study website through the QR code on the leaflet. After providing e-consent and completing the baseline investigation at Week 0 through electronic patient-reported outcome, participants were randomly allocated to a smartphone-based ACT intervention and treatment as a trial group or to a waiting list control group that continued to receive treatment as usual. Participants were randomly assigned in a 1:1 ratio using a computer-generated randomization sequence implemented through an electronic data capture system at the data management center. The allocation sequence was automatically generated by the system. Allocation concealment was ensured through the centralized system. Participants were enrolled by research assistants, and group assignments were automatically generated by the system at the time of enrollment. Participants were fully informed about the purpose of the trial. Participants were offered Amazon gift certificates of up to 5000 yen as a reward, depending on the provision of their outcome measurements. In addition, exploratory feedback on the usability and improvement of the application was collected from participants through brief interviews. This was not conducted as a formal qualitative study. After the study was completed, participants who participated in interviews about their use of the application were rewarded an additional Amazon gift certificate of 2000 yen. The recruitment for the study began on 12th June 2023 and completed on 18th August 2023 based on completion of target sample size. The follow-up completed on 6th November 2023.
Interventions
Smartphone ACT
The treatment consisted of a smartphone-delivered ACT-based intervention. This intervention was based on the investigators’ empirically supported program, NOBIYAKA-Program (nobiyaka, のびやか, meaning peaceful and carefree), which was developed for chronic pain.13 Based on this program, the smartphone-based ACT program for PMPS, called SAKURA-App (sakura, 桜, meaning cherry blossom; SASUMED Inc, Japan), was developed for this study. SAKURA-App consisted of eight ACT sessions to be completed over eight weeks (one session per week). Each session was divided into three or four modules, each taking about 10 minutes to complete. The content was divided into three themes promoting psychological flexibility: openness, the present moment, and value. Each theme included multimedia content such as text, photos, video clips, and animations. Participants were also given mindfulness exercises and value-oriented behavior homework, which they were automatically prompted by the app to perform daily as much as possible. A summary of the contents of the app is shown in Table 1.
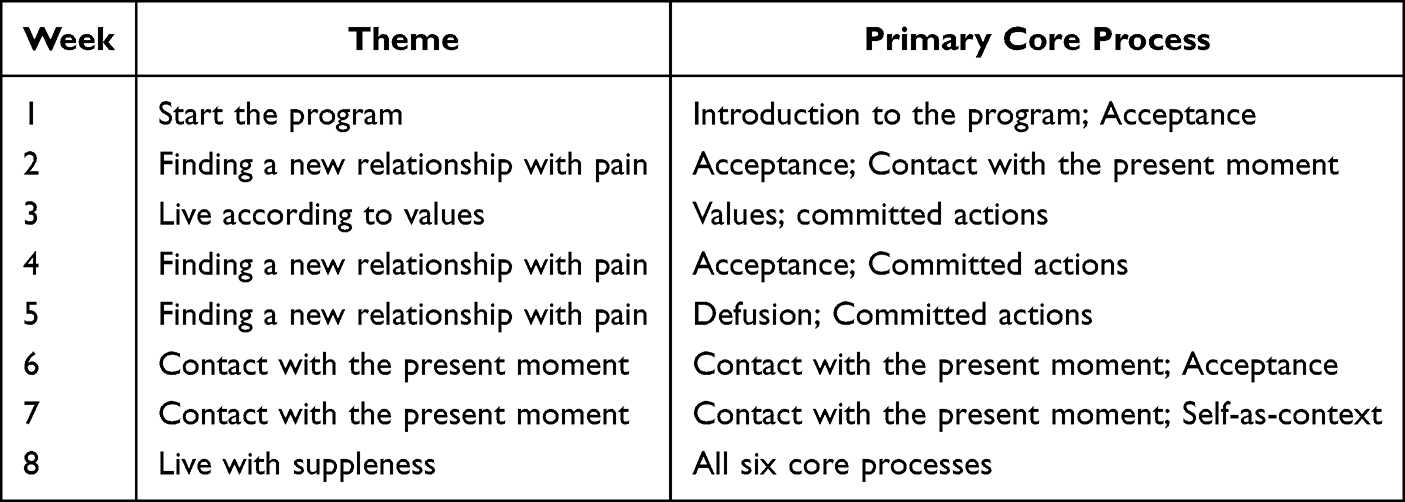 |
Table 1 SAKURA-App Contents |
Waiting List
Participants randomly assigned to the waiting list received treatment as usual during the study period. After the study period, participants were invited to use SAKURA-App.
Baseline Characteristics
The following data were collected: age, education, marital status, employment status, years since breast cancer surgery, years since reconstructive surgery, treatment history, and performance status.
Primary Outcomes: Feasibility, Acceptability, and Adherence
The primary outcomes were feasibility, acceptability, and adherence to the SAKURA-App intervention. Feasibility was assessed based on the extent to which the intervention met patients’ needs and their level of satisfaction. To evaluate feasibility, the level to which patients’ needs were met through the intervention and their reported satisfaction level were measured. The items were scored on a 100-point scale (response options ranged from 0 = “not helpful/satisfying at all” to 100 = “met all my needs”/“very satisfied”), where scores of 60 or higher were considered passing scores. Additionally, an item was included to measure whether there were any adverse or undesirable effects from participating. Acceptability was assessed by participants’ willingness to continue using the application, measured on a five-point scale (response options ranged from 1 = “not at all” to 5 = “very much”). Adherence was evaluated using the completion rate of the application.
Secondary Outcome Measure
Pain Interference
Pain interference was measured with a Brief Pain Inventory (BPI)14 interference subscale. This is a seven-item self-report questionnaire that measures the degree of pain interference with general activities, the ability to walk, work, mood, relationships, enjoyment of life, and sleep. The mean score of the BPI was calculated. The coefficient alpha was 0.81.
Pain Intensity
Pain intensity was assessed with a BPI14 intensity scale. This is a four-item self-report questionnaire that measures the degree of worst, least, and average during the past week and currently. The coefficient alpha was 0.81.
Fatigue and Numbness Intensity
Fatigue and numbness intensity were measured using the MD Anderson Symptom Inventory (MDASI).15 This is a 19-item self-report questionnaire that measures a patient’s symptoms and how many have interfered with various aspects of that patient’s life. In this study, two of these items (sluggishness and numbness) were measured on a scale of 0 to 10.
Pain Acceptance
Pain acceptance was assessed with the Chronic Pain Acceptance Questionnaire (CPAQ).16 This is a 20-item self-report questionnaire that measures patients’ acceptance of chronic pain. CPAQ consists of pain willingness and activity engagement subscales. The Cronbach’s alpha was 0.83 for the total, 0.83 for pain willingness, and 0.87 for activity engagement.
Fear of Cancer Recurrence
Fear of cancer recurrence was measured using the Fear of Cancer Recurrence Inventory-short form (FCRI-short form).17 This is a nine-item self-report questionnaire. The coefficient alpha was 0.89.
Work Productivity
Work productivity was assessed with the Work Productivity and Activity Impairment Questionnaire (WPAI).18 This is a six-item self-report questionnaire that measures the number of days and hours missed from work, days and hours worked, days in which working was difficult, and the extent to which the individual felt limited at work during the past seven days.
Anxiety and Depression
Anxiety and depression were measured using the Hospital Anxiety and Depression Scale (HADS).19 This is a 14-item self-report questionnaire and consists of anxiety and depression subscales. The Cronbach’s alpha was 0.80 for anxiety and 0.50 for depression.
Psychological Flexibility
Psychological flexibility was assessed with the Acceptance and Action Questionnaire 2 (AAQ-2).20 This is a seven-item self-report questionnaire. The Cronbach’s alpha was 0.88.
Values-Aligned Behavior
Values-aligned behavior was measured using the Valuing Questionnaire (VQ).21 This is a 10-item self-report questionnaire. The VQ consists of progress and obstruction subscales. The Cronbach’s alpha was 0.82 for progress and 0.50 for obstruction.
QOL
QOL was assessed with the EuroQol-5-dimensions (EQ-5D).22 This is a five-item self-report questionnaire. EQ-5D is an instrument for obtaining QOL scores that are used to calculate the quality-adjusted life year.
Statistical Analysis
The sample size was determined for the purpose of examining feasibility and potential acceptability. The target sample size was set at 40 participants based on the study’s primary objectives of assessing feasibility and preliminary efficacy, as well as the practical recruitment capacity within the decentralized trial framework. As this is a pilot study, a formal power analysis was not performed. Instead, the sample size was determined to ensure a sufficient number of cases for qualitative evaluation and to provide reliable estimates of effect sizes and recruitment rates required to inform the design of a future full-scale trial. All statistical analyses were performed on all randomized participants according to the intention-to-treatment principle. The proportion of patients in the intervention group who completed the ACT app and its 95% confidence interval (CI) were estimated for the primary endpoint using the Clopper-Pearson method. Missing data were handled using the Mixed-effects Model for Repeated Measures (MMRM), which assumes data are missing at random (MAR) and utilizes all available data without formal imputation. For endpoints with three or more time points, The MMRM was used for group comparisons at each time point. The MMRM model included the treatment group, time point, and the interaction between the treatment group and the time point as a fixed effect. The participants were random effects and baseline values were covariates. For endpoints with two time points, an analysis of covariance with baseline values was used as a covariate to compare the treatment group. The number and percentage of adverse events were calculated.
All statistical tests were two-tailed, and p < 0.05 was considered statistically significant. The multiplicity of tests was not adjusted because this was a pilot study. All statistical analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Participant Characteristics
In total, 57 patients were assessed for eligibility and 45 patients were randomly assigned; of these patients, 22 and 23 were allocated to the intervention and control groups, respectively (Figure 1). The baseline demographic and clinical characteristics for each group were well balanced (Table 2). Both groups had mean ages in the 50s (51.1 years (SD = 8.7) in the ACT group and 53.8 years (SD = 7.6) in the waiting list group). Over 70% of the participants had full- or part-time jobs. The baseline pain interference was low: 1.4 in the ACT group and 1.5 in the waiting list group.
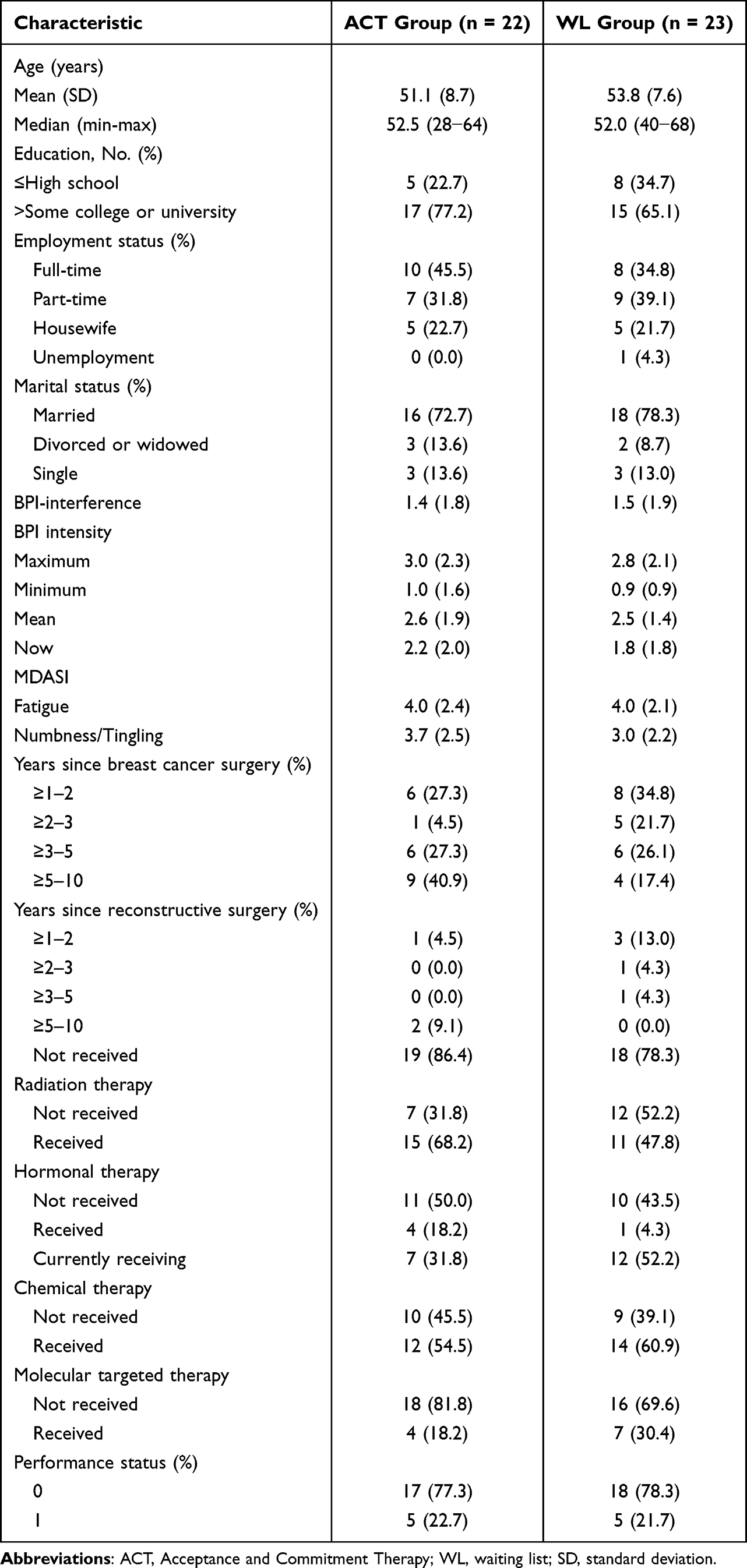 |
Table 2 Participant Characteristics at Baseline |
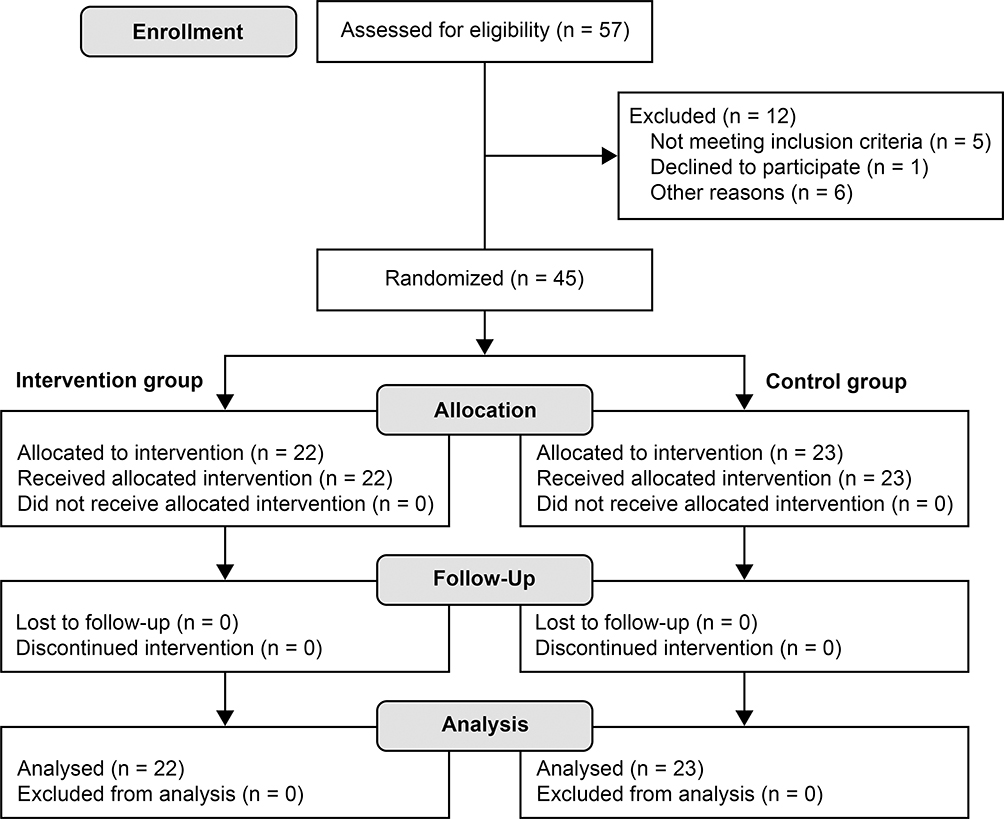 |
Figure 1 CONSORT Flowchart of Participants. |
Primary Outcomes: Feasibility, Acceptability, and Adherence
Feasibility: The mean score for the extent to which the patients’ needs were met by the intervention was 67.95 (SD = 15.17), and the mean overall satisfaction score was 69.32 (SD = 15.30). One adverse effect of participating in the study was reported: patients became bitter when recalling family members’ cancer experiences. However, this effect was reported as “Mild”.
Acceptability and Exploratory Feedback: Responses to the question of whether participants would like to continue using the SAKURA-App were as follows: “neutral” (n = 14), “agree” (n = 4), “not so much” (n = 2), and “not at all” (n = 2). Among the intervention group who completed the Week 8 follow-up (n = 22), 17 participants provided exploratory feedback via telephone interviews regarding product usability. Participants suggested several areas for improvement, including app functionality, content difficulty, and task volume Detailed qualitative feedback and a summary of suggested improvements for the SAKURA-App are provided in Supplementary Box 1.
Adherence: All 22 participants in the ACT group completed the eight-week SAKURA-App program, resulting in a completion rate of 100%. There were no missing responses at baseline and Week 8, one missing response at Week 2, and three missing responses at Week 4.
Secondary Clinical Outcomes
Table 3 presents the outcomes for each group. There were no significant differences in the ACT group outcomes at Week 8 in terms of BPI-interference (pain interference) (Figure 2) or between the two groups for BPI intensity (pain intensity), MDASI fatigue (fatigue intensity), and CPAQ (pain acceptance). At Week 8, participants in the ACT group showed a numerical improvement in MDASI-numbness (numbness intensity) compared to the control group; however, this finding was not statistically significant and should be considered exploratory (difference −0.81, 95% CI, −1.77 to −0.16, p = 0.09).
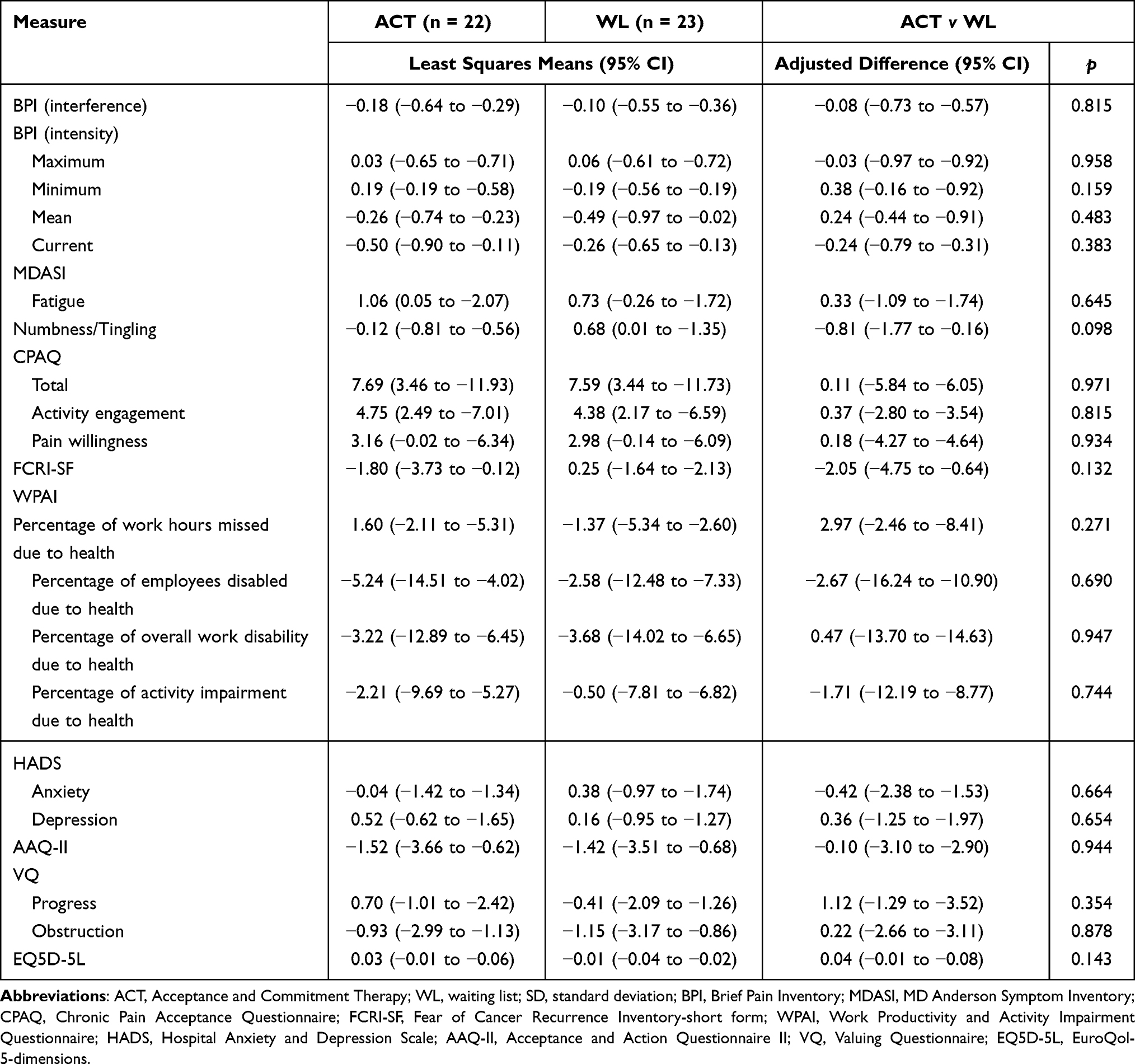 |
Table 3 Changes from Baseline at Week 8 in Secondary Outcomes |
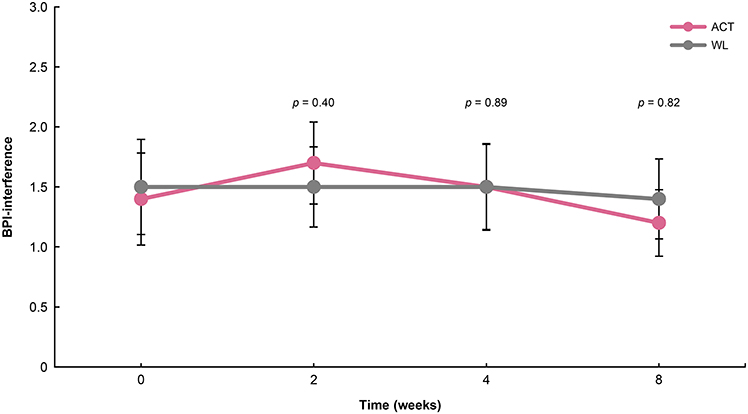 |
Figure 2 Changes from baseline in the overall BPI-interference scores. |
There were no significant differences between the two groups for WPAI (work productivity), HADS (anxiety and depression), AAQ-II (psychological flexibility), and VQ (values-aligned behavior). However, participants in the ACT group therefore demonstrated improvement at Week 8 compared with the control group in FCRI-SF (fear of cancer recurrence) (difference −2.05, 95% CI, −4.75 to −0.64, p = 0.13), and EQ5-D (QOL) (difference 0.04, 95% CI, −0.01 to −0.08, p = 0.14).
Discussion
To the investigators’ knowledge, this study is the first to examine the feasibility and acceptability of smartphone-based ACT interventions specifically targeting both PMPS and fear of recurrence, addressing a critical gap in cancer survivorship care. This pilot study demonstrated high feasibility with a decentralized trial format and provides a credible basis for future adequately powered trials.
This study demonstrated that the smartphone-based ACT intervention is feasible among breast cancer survivors with PMPS and fears of recurrence, as the mean scores for the extent to which patients’ needs were met and their satisfaction level were both above 60%, a predefined passing score. These results are highly plausible and consistent with outcomes from other well-designed digital health interventions. Regarding adverse events, one patient “recalled a family member’s experience with cancer” and felt bitter, but the patient had emotionally recovered by the time the interview occurred, and the event was considered minor.
Notably, this study demonstrated an exceptional level of adherence, with a completion rate of 100% for the intervention. In both groups, 70% of the participants had full- or part-time jobs, suggesting that this scalable intervention can be implemented even among busy patients, for example during breaks. However, when participants were asked whether they would like to continue using the app in the future, more than half of the ACT intervention group gave neutral responses, and some reported that daily use of the app felt burdensome. In interviews, improvements were suggested for the app, mainly related to its functionality, the difficulty of the content, and the number of tasks.
This study also examined the exploratory effects of smartphone-based ACT intervention on multiple symptom clusters, including pain interference, pain intensity, fatigue, and numbness/tingling. The analysis showed changes in the intensity of numbness/tingling; however, no statistically significant effects were observed, and no significant effects were found for the other indicators. As shown in Table 2, participants had a lower mean level of pain interference at baseline—1.4 (SD = 1.8) in the ACT group and 1.5 (SD = 1.9) in the waiting list control group—and a lower mean pain intensity—2.6 (SD = 1.9) in the ACT group and 2.5 (SD = 1.4) in the waiting list control group. These clinical characteristics likely resulted in a significant floor effect, which strictly limited the detectability of treatment efficacy in this sample.
In addition, this study examined exploratory effects on secondary clinical outcomes, including pain acceptance, fears of recurrence, work productivity, anxiety and depression, psychological flexibility, value-aligned behaviors, and QOL. Changes were observed in fears of recurrence; however, no statistically significant effects were found, and these findings should be interpreted as exploratory. The degree of pain acceptance at baseline for both the ACT group and waiting list group in this study was very high compared to values for chronic pain patients in a previous study.16 Moreover, both groups in this study were relatively healthy, with low levels of hindrance to work productivity at baseline and psychological flexibility and values-aligned behaviors comparable to the average for college students in previous studies.20,21 Both groups also had lower anxiety and depression and a higher QOL at baseline. Collectively, these findings must be interpreted with caution, as the baseline floor and ceiling effects across most measures indicate that the therapeutic efficacy of the intervention could not be properly tested within this specific population.
Limitations and Conclusion
This study had several limitations. First, the participants exhibited very low baseline pain interference, which likely resulted in a floor effect. According to the International Association for the Study of Pain (IASP), pain interference is classified as mild (1–3), moderate (4–6), or severe (7–10) on a NRS scale.23 Due to the inclusion of patients with only mild interference, efficacy could not be properly tested in this sample. This floor effect precluded the detection of clinically significant improvements and limits the generalizability of the findings to the broader PMPS population. Therefore, future research should evaluate the effectiveness of ACT apps in patients with moderate or greater pain disability to rigorously establish clinical utility.
Second, the 8-week intervention period, while appropriate for assessing feasibility in this pilot study, may have been insufficient to fully capture long-term behavioral changes compared to full-scale ACT trials. Future studies should employ extended intervention and follow-up periods to evaluate the sustained clinical efficacy and the trajectory of psychological flexibility over time.
Third, the use of a waitlist control, while acceptable for a pilot feasibility study, limits the ability to isolate the specific therapeutic effects of ACT from non-specific factors, such as digital placebo effects or the mere expectation of improvement. Ideally, a sham application—designed to mimic the digital engagement and interface of the SAKURA-App without its core therapeutic components—should be utilized as an active control.
Fourth, despite the high adherence rate within the trial, more than half of the ACT group gave neutral responses regarding future use, citing daily engagement as a burden. Such neutral feedback highlights a significant “engagement challenge” for real-world implementation. Future studies must address these usability concerns and investigate strategies to maintain long-term user involvement outside of a controlled research environment.
Overall, this pilot study demonstrates that the SAKURA-App is highly feasible and acceptable for patients with PMPS and fears of recurrence. The feedback provided by participants offers valuable insights into potential enhancements, which will inform the design of future verification testing. Thus, this study supports the integration of digital technology into the multimodal care of PMPS patients.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
Ethical approval was granted by the Nagoya City University Graduate School of Medical Sciences Institutional Review Board (reference number: 46-22-0011).
Acknowledgments
The authors especially thank the study participants. We also thank the project members, especially Shinji Ohno, Yosuke Uchitomi, Takanori Ishida, Toshinari Yamashita, Naomi Sakurai, Takeshi Sugiura, Naruto Taira, Yasuaki Sagara, Eriko Tokunaga, and Dr Naoto Kondo in the Department of Breast Surgery. Additionally, we thank Hiroshi Koyama and Takaaki Sano for their contributions to the production of the application.
We also thank our research assistants for this study, especially Akane Nomura, Kana Tojima, Ikuyo Sakakima, and Kaori Kobori in the Department of Psychiatry and Cognitive-Behavioral Medicine, Nagoya City University Graduate School of Medical Sciences.
Funding
This work was supported by a Practical Research for Innovative Cancer Control project grant (No. 22ck0106786h0001) from the Japan Agency for Medical Research, and by Japan Society for the Promotion of Science KAKENHI (Grant 23K25738).
Disclosure
Dr Mie Sakai reports personal fees from Meiji-Seika Pharma, Pfizer, AstraZeneca; also reports a pending patents ((2024-516288), outside the submitted work. Dr Hiroya Hashimoto reports personal fees from Chugai, outside the submitted work. Dr Taro Ueno is the CEO of SUSMED Inc. Professor Tatsuo Akechi reports personal fees from AstraZeneca, Chugai, Daiichi-Sankyo, Eisai, Eli-Lilly, Kowa, Lundbeck, MSD, Meiji-Seika Pharma, Merck, Otsuka, Pfizer, Shionogi, Sumitomo pharma, Takeda, Tsumura, UCB, and Viatris; grants from Shinogi, royalties from Igaku-Shoin; serves as the representative director of the General Incorporated Association NCU CRESS and receives compensation as an advisor to Snom Inc., outside the submitted work; In addition, Professor Tatsuo Akechi has patents 2020-135195 and 2024-516288 pending to Institute, a patent 7313617 issued to Institute. The authors declare no other conflicts of interest associated with this manuscript.
References
1. Ito Y, Miyashiro I, Ito H, et al. Long-term survival and conditional survival of cancer patients in Japan using population-based cancer registry data. Cancer Sci. 2014;105(11):1480–12. doi:10.1111/cas.12525
2. Tait RC, Zoberi K, Ferguson M, et al. Persistent post-mastectomy pain: risk factors and current approaches to treatment. J Pain. 2018;19(12):1367–1383. doi:10.1016/j.jpain.2018.06.002
3. Uemoto Y, Uchida M, Kondo N, et al. Predictive factors for patients who need treatment for chronic post-surgical pain (CPSP) after breast cancer surgery. Breast Cancer. 2021;28(6):1346–1357. doi:10.1007/s12282-021-01275-4
4. Chappell AG, Yuksel S, Sasson DC, Wescott AB, Connor LM, Ellis MF. Post-Mastectomy pain syndrome: an up-to-date review of treatment outcomes. JPRAS Open. 2021;30:97–109. doi:10.1016/j.jpra.2021.07.006
5. Ma T-W, Yuen AS-K, Yang Z. The efficacy of acceptance and commitment therapy for chronic pain. Clin J Pain. 2023;39(3):147–157. doi:10.1097/AJP.0000000000001096
6. Hadlandsmyth K, Dindo LN, Wajid R, Sugg SL, Zimmerman MB, Rakel BA. A single-session acceptance and commitment therapy intervention among women undergoing surgery for breast cancer: a randomized pilot trial to reduce persistent postsurgical pain. Psycho-Oncology. 2019;28(11):2210–2217. doi:10.1002/pon.5209
7. Johns SA, Stutz PV, Talib TL, et al. Acceptance and commitment therapy for breast cancer survivors with fear of cancer recurrence: a 3-arm pilot randomized controlled trial. Cancer. 2020;126(1):211–218. doi:10.1002/cncr.32518
8. Gentili C, Zetterqvist V, Rickardsson J, Holmström L, Simons LE, Wicksell RK. ACTsmart: guided smartphone-delivered acceptance and commitment therapy for chronic Pain—A pilot trial. Pain Med. 2021;22(2):315–328. doi:10.1093/pm/pnaa360
9. Sakai M, Kondo M, Sugiura T, Akechi T. Acceptance and commitment therapy in the transdiagnostic treatment of a breast cancer survivor: a case study 1. Japanese Psychol Res. 2024;66(3):264–275. doi:10.1111/jpr.12422
10. Dindo L, Van Liew JR, Arch JJ. Acceptance and commitment therapy: a transdiagnostic behavioral intervention for mental health and medical conditions. Neurotherapeutics. 2017;14(3):546–553. doi:10.1007/s13311-017-0521-3
11. Gendreau RM, Mccracken LM, Williams DA, et al. Self-guided digital behavioural therapy versus active control for fibromyalgia (PROSPER-FM): a Phase 3, multicentre, randomised controlled trial. Lancet. 2024;404(10450):364–374. doi:10.1016/S0140-6736(24)00909-7
12. Akechi T, Yamaguchi T, Uchida M, et al. Smartphone psychotherapy reduces fear of cancer recurrence among breast cancer survivors: a fully decentralized randomized controlled clinical trial (J-SUPPORT 1703 Study). J Clin Oncol. 2023;41(5):1069–1078. doi:10.1200/JCO.22.00699
13. Sakai M, Kondo M, Muto T, Sugiura T, Akechi T. Preliminary utility of group acceptance and commitment therapy for patients with chronic pain. Jpn J Behav Cognit Ther. 2025;51(3):179–189. doi:10.24468/jjbct.24-003
14. Uki J, Mendoza T, Cleeland CS, Nakamura Y, Takeda F. A brief cancer pain assessment tool in Japanese. J Pain Symptom Manag. 1998;16(6):364–373. doi:10.1016/S0885-3924(98)00098-0
15. Okuyama T, Wang XS, Akechi T, et al. Japanese version of the M.D. anderson symptom inventory: a validation study. J Pain Symptom Manag. 2003;26(6):1093–1104. doi:10.1016/j.jpainsymman.2003.05.003
16. Anno K, Iwaki R, Murakami M, et al. Development, reliability, and validation of Japanese version of the chronic pain acceptance questionnaire (CPAQ-J). J Jpn Soc Study Chron Pain. 2022;41:83–90.
17. Simard S, Savard J. Screening and comorbidity of clinical levels of fear of cancer recurrence. J Cancer Surviv. 2015;9(3):481–491. doi:10.1007/s11764-015-0424-4
18. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. PharmacoEconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
19. Kugaya A, Akechi T, Okuyama T, Okamura H, Uchitomi Y. Screening for psychological distress in Japanese cancer patients. Jpn J Clin Oncol. 1998;28(5):333–338. doi:10.1093/jjco/28.5.333
20. Shima T, Yanagihara M, Kawai T, Kumano H. Validation of the Japanese version of the acceptance and action questionnaire-II. In
21. Doi S, Sakano A, Muto T, Sakano Y. Reliability and validity of A Japanese version of the valuing questionnaire (VQ). Jpn J Behav Ther. 2017;43:83–94.
22. Ikeda S, Shiroiwa T, Igarashi A, et al. Developing A Japanese version of the EQ-5D-5L value set. J Natl Inst Public Health. 2015;64:47–55.
23. Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.