Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Small Bowel Obstruction in Virgin Abdomen: Predictors of Surgical Intervention Need in Resource-Limited Setting
Authors Ghabisha S ![]() , Ahmed F
, Ahmed F ![]() , Altam A, Hassan F, Badheeb M
, Altam A, Hassan F, Badheeb M ![]()
Received 5 October 2023
Accepted for publication 11 December 2023
Published 12 December 2023 Volume 2023:16 Pages 4003—4014
DOI https://doi.org/10.2147/JMDH.S441958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saif Ghabisha,1 Faisal Ahmed,2 Abdulfattah Altam,3 Fouad Hassan,4 Mohamed Badheeb5
1Department of General Surgery, School of Medicine, Ibb University, Ibb, Yemen; 2Department of Urology, School of Medicine, Ibb University, Ibb, Yemen; 3Department of General Surgery, School of Medicine, 21 September University, Sana’a, Yemen; 4Department of Nutrition and Dietetics, School of Medicine, Ibb University, Ibb, Yemen; 5Department of Internal Medicine, Yale New-Haven Health/Bridgeport Hospital, Bridgeport, CT, USA
Correspondence: Faisal Ahmed, Department of Urology, School of Medicine, Ibb University of Medical Sciences, Ibb, Yemen, Tel/Fax +967 4428950, Email [email protected]
Background: Limited evidence is available regarding the management of small bowel obstruction in the virgin abdomen (SBO-VA), with most studies excluding this entity. This study aims to assess the available data on the treatment outcomes and predictors of surgical intervention in SBO-VA.
Methods: A retrospective cross-sectional study was conducted between 2015 and 2021, including all diagnosed and managed cases of SBO-VA at Al-Nasar Hospital. Patients were divided according to the treatment approach into surgical or conservative groups. Preoperative laboratory and radiologic data were gathered and compared between groups.
Results: During the study period, 67 cases, primarily males (58.2%), with an average age of 52.2± 14.4 years were assessed. Common comorbidities included diabetes (20.9%) and hypertension (16.4%). Key symptoms were rebound tenderness (82.1%) and abdominal tenderness (70.1%). The predominant etiology was adhesions (23.9%). About 46.2% received conservative treatment, 53.8% underwent urgent surgery. Conservative treatment failed in 9.4% of cases, and complications arose in 23.9%, with most being fever (17.9%). Factors necessitating surgical management included older age (58.8 ± 11.7 vs 44.9 ± 13.8 years, p< 0.001), previous hospital admission (p< 0.001), presence of abdominal tenderness (p=0.030), longer abdominal pain duration (4.0 ± 0.9 vs 2.1 ± 0.6 days, p< 0.001), higher C- reactive protein (p= 0.033), higher white blood cell (p= 0.006), longer time to hospital presentation (75.3 ± 17.2 vs 39.0 ± 22.8 days, p= < 0.001), small bowel thickness ≥ 3 cm (p=0.009), and reduced bowel enhancement (p < 0.001) on computed tomography imaging. In surgical group, the need for ICU admission was higher and hospital stays were shorter than in conservative group and were statistically significant (p< 0.05).
Conclusion: The main etiology of SBO-VA in our study was adhesions. Older age, previous hospital admission, longer abdominal pain duration, abdominal tenderness, increased inflammatory markers, and alarm signs on CT scans are the main factors for determining the need for urgent surgical exploration in patients with SBO-VA. To achieve prompt identification and intervention, it is crucial to maintain a high level of vigilance and awareness, even in individuals with no prior surgical history.
Plain Language Summary: here is limited evidence available regarding the management of small bowel obstruction in the virgin abdomen (SBO-VA), with most studies excluding this entity especially in resource-limited settings. In this study, we investigated the factors associated with the need for surgical interventions in 67 cases diagnosed with SBO-VA. Our result showed that the predominant etiology was adhesion. While 46.2% received conservative treatment, 53.8% underwent urgent surgery. Conservative treatment failed in 9.4% of cases. Factors associated with need for surgical management included older age, previous hospital admission, presence of abdominal tenderness, longer abdominal pain duration, higher C-reactive protein (CRP), higher white blood cell (WBC), longer time to hospital presentation, small bowel thickness ≥ 3 cm and reduced bowel enhancement on computed tomography imaging. In surgical group, the need for ICU admission was higher and hospital stays were shorter than in conservative group.
Keywords: Small bowel obstruction, virgin abdomen, laparotomy, conservative management, Etiology
Introduction
Small bowel obstruction (SBO) is more accurately described as a clinical syndrome than a distinct disease. Indeed, it stands as one of the most frequent surgical emergencies, accounting for up to 15% of hospital admissions.1 Despite its significant incidence, SBO continues to pose diagnostic and therapeutic challenges. Contemporary clinical and diagnostic tools, while advanced, sometimes fall short of conclusively differentiating or detecting severe complications, such as ischemia which may results in gangrenous bowel necrosis.2
Several studies have highlighted adhesions as a predominant cause of SBO. In certain reports, adhesions have been implicated in up to two-thirds of cases.3 Besides adhesions, other causative factors may include hernias, neoplasms, intussusception, volvulus, and a myriad of intrinsic and extrinsic obstructive causes. Notably, the prevalence of these factors has considerable variation based on geographic regions.4,5 The adhesive type of SBO is typically associated with prior surgical interventions, occurring in 80–97% of such cases6 Nonetheless, SBO has been reported, albeit less frequently, in patients with no preceding surgeries, who have been classically referred to as a “virgin abdomen (VA)”.7
Recent trends indicate a marked shift towards non-operative management of SBO. This change, however, has been met with challenges, especially in SBO-VA cases. The inherent uncertainty surrounding SBO-VA etiology often necessitates surgical approaches, which is largely driven by concerns over potential non-adhesive causes, such as malignancies.8 Nevertheless, retrospective studies have revealed that even in SBO-VA contexts, adhesions remain the predominant cause, and this understanding has further shifted the emphases towards non-operative approaches in managing SBO-VA.6,9
While non-operative management of SBO offers advantages like reduced mortality and diminished hospital stays, it has been associated with increased recurrence rates.10 Therein lies a delicate equilibrium of avoiding unnecessary surgical procedures with their associated risks, while also ensuring that no critical treatment delays transpire. Determining the need for surgical intervention remains a point of debate, even among highly experienced surgeons.11 This is attributed to the absence of definitive clinical guidelines or consensus. While predictive scoring indices for surgical interventions in adhesive SBO exist, they primarily encompass patients with prior surgeries or excluded SBO-VA cases, casting doubt on their utility and relevance in such cases.12,13 Thus, this study seeks to evaluate the causes, outcomes, and predictors of surgical intervention among SBO-VA patients.
Materials and Methods
Study Setting and Design
Between January 2015 and December 2021, cases of SBO-VA treated at Al-Nasar Hospital (Ibb, Yemen) were retrospectively reviewed and analyzed. The study was adherent to the Helsinki Declaration’s principles, and Ibb University’s ethics board approved this research (Code number: IBBUNI.AC.YEM.2023.102). Participating patients were briefed about the research objectives, and written consent was obtained before inclusion in this study.
Inclusion Criteria
Patients aged ≥ 16 years, who presented with symptoms suggestive of small bowel obstruction were included.
Exclusion Criteria
Patients with a history of prior abdominopelvic surgeries, those manifesting symptoms or imaging characteristic of large bowel obstruction or functional SBO, and patients with strangulated external abdominal hernias.
Study Protocol
SBO was determined by the presence of suggestive clinical symptoms, including the classical cardinal symptoms of abdominal pain, nausea and/or vomiting, abdominal distention, and constipation/obstipation. These symptoms were supplemented by supportive or confirming radiological findings, such as small bowel dilatation proximal to the obstruction, collapsed distal intestine, and air-fluid levels (indicative of ascites) on plain film. Patients were managed either conservatively—with nil per mouth, fluid resuscitation, and gastric decompression—or through surgical interventions, primarily dictated by the clinical acumen of the consultant surgeons. Indeed, overt clinical signs, such as peritonitis, or compelling evidence of ischemia or strangulation, warranted an immediate surgical intervention. However, it’s noteworthy that some rationales for surgical intervention remained ambiguous due to the retrospective nature of our study. In both groups, medical management of electrolyte disturbances, potential underlying infections, and other chronic medical conditions (eg, hypertension, diabetes) was implemented.
The underlying etiology of SBO-VA was discerned via intra-operative observations or post-operative histopathological diagnoses in patients who underwent surgery. For those managed conservatively, the diagnosis was established through clinical and radiological evaluations, further supplemented by the exclusion of any overt etiological factors. The onset of flatus and feces, accompanied by the resolution of the presenting symptoms, signaled the resolution of the SBO.9
Data Collection
Patient demographic characteristics include age, gender, residency, education level, history of Khat chewing, and previous hospital admission for the same problem. Comorbidities include history of diabetes mellitus, hypertension, cardiovascular disease, malignancy, and neurologic disease. The main symptoms include abdominal pain, abdominal pain duration (day), time from symptoms starting to hospital presentation (day), vomiting, constipation, history of unintentional weight loss (loss of > 10% of body weight over 3 months), abdominal distension, melena or hematochezia. The physical examination findings include bowel movement in auscultation, abdominal tenderness, and rebound tenderness. The laboratory findings include Hemoglobin (g/dL), White Blood Cell (WBC) (/µL), C-reactive protein (CRP) (mg/dL), Blood Urea Nitrogen (BUN) (mg/dL), and Creatinine (Cr) (mg/dL). The computed tomography findings include small bowel thickness (≥3 Cm or < 3 cm), reduced bowel enhancement (yes or no), and fluid in the mesentery and/or peritoneal cavity (yes or no). The data on hospital admission include the need for intensive care unit (ICU) admission, hospital stays (day), outcome, and postoperative complications.
Study Outcome
The main outcome was to compare surgical and conservative treatment groups and find the factors that predicate the need for urgent surgical intervention.
Statistical Analysis
For numerical data, we utilized mean ± SD representations, and for categorical ones, we opted for frequency (percentage) portrayals. We determined statistical variances for numeric data via the Mann–Whitney U-test and used the χ2 test alongside Fisher’s exact test for category-based data. Statistical significance was considered with a P-value under 0.05. The data was processed using the software SPSS (IBM SPSS, version 18, Armonk, New York: IBM Corp).
Result
Sixty-seven cases were included during the study period. The mean age was 52.2 ±14.4 years. Most of the patients were male and illiterate, with 39 (58.2%) and 35 (52.2%) cases respectively, and 30 (44.8%) were from rural areas. A history of Khat chewing was present in 60 (89.6%) cases, and previous hospital admission was noted in 24 (35.8%) cases. A history of diabetes, hypertension, cardiovascular disease, malignancy, and neurological disorders were present in 14 (20.9%), 11 (16.4%), 13 (19.4%), 6 (9.0%), and 6 (9.0%) cases, respectively (Table 1). The main symptoms were abdominal pain (82.1%) and abdominal distension (68.7%). The main physical exam findings were rebound tenderness (82.1%) and abdominal tenderness (70.1%). The main time to hospital presentation was 57.9 ±27.0 days. The main WBC was 12,128.1 ±5579.2 /µL (Table 2). The main etiologies were adhesions (23.9%), followed by closed loop obstruction (19.4%), and then internal hernia (16.4%). Abdominal tuberculosis was represented in 3 (4.5%) cases (Table 3) (Figures 1 and 2). The computed tomography (CT) scan findings were small bowel thickness ≥3 cm, reduced bowel enhancement, and ascites in 31 (46.3%), 23 (34.3%), and 45 (67.2%) cases respectively. Urgent surgical management was performed in 35 (52.2%) cases while conservative treatment was performed in 32 (47.8%) cases. Conservative treatment failed in 3 (9.4%) cases. ICU admission was required for 31 (46.3%) cases. Complications occurred in 16 (23.9%) cases, and most of these complications were fever, accounting for 12 (17.9%) cases (Table 4).
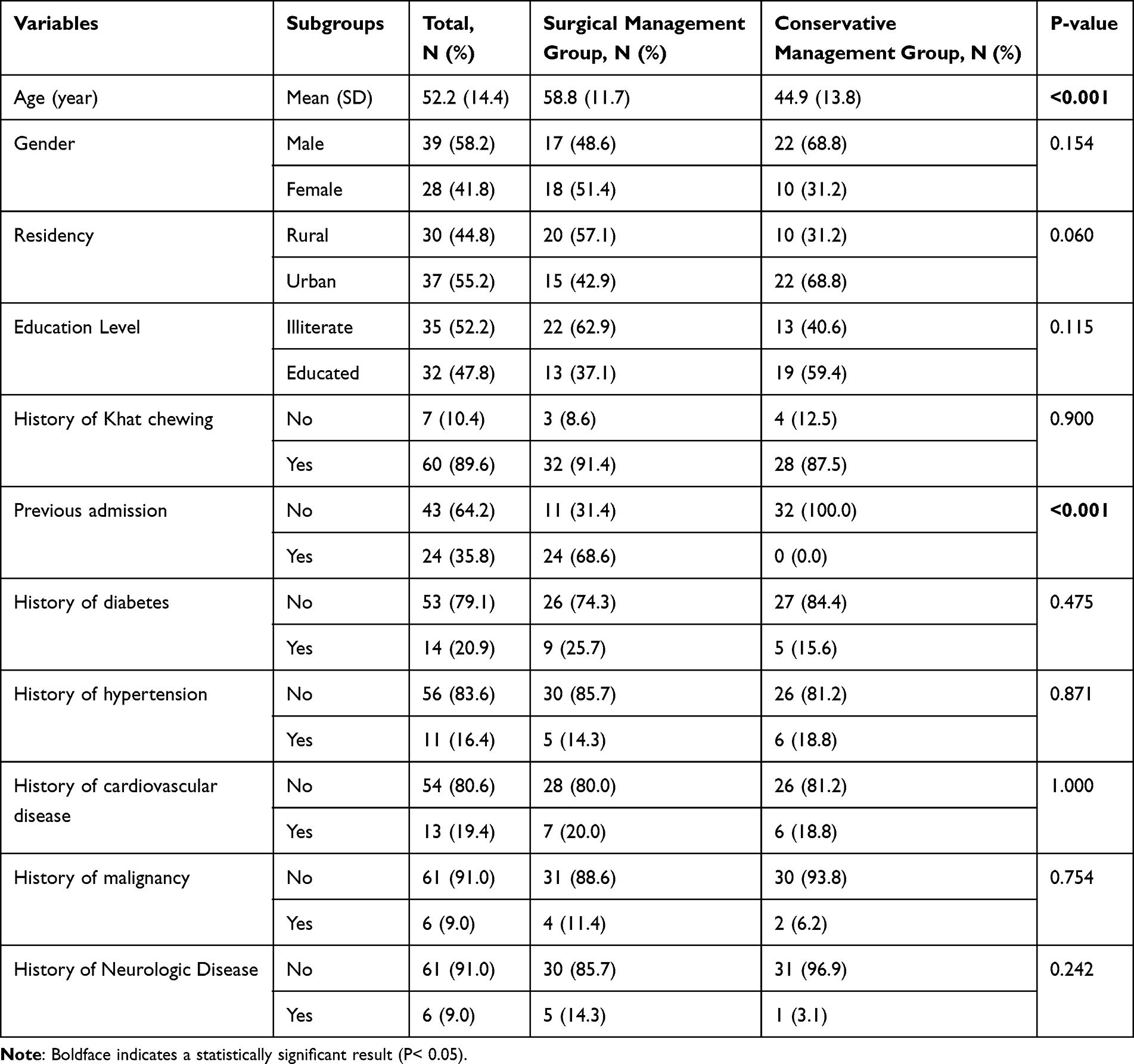 |
Table 1 Demographic Characteristics of Patients with Virgin Abdomen and Small Bowel Obstruction |
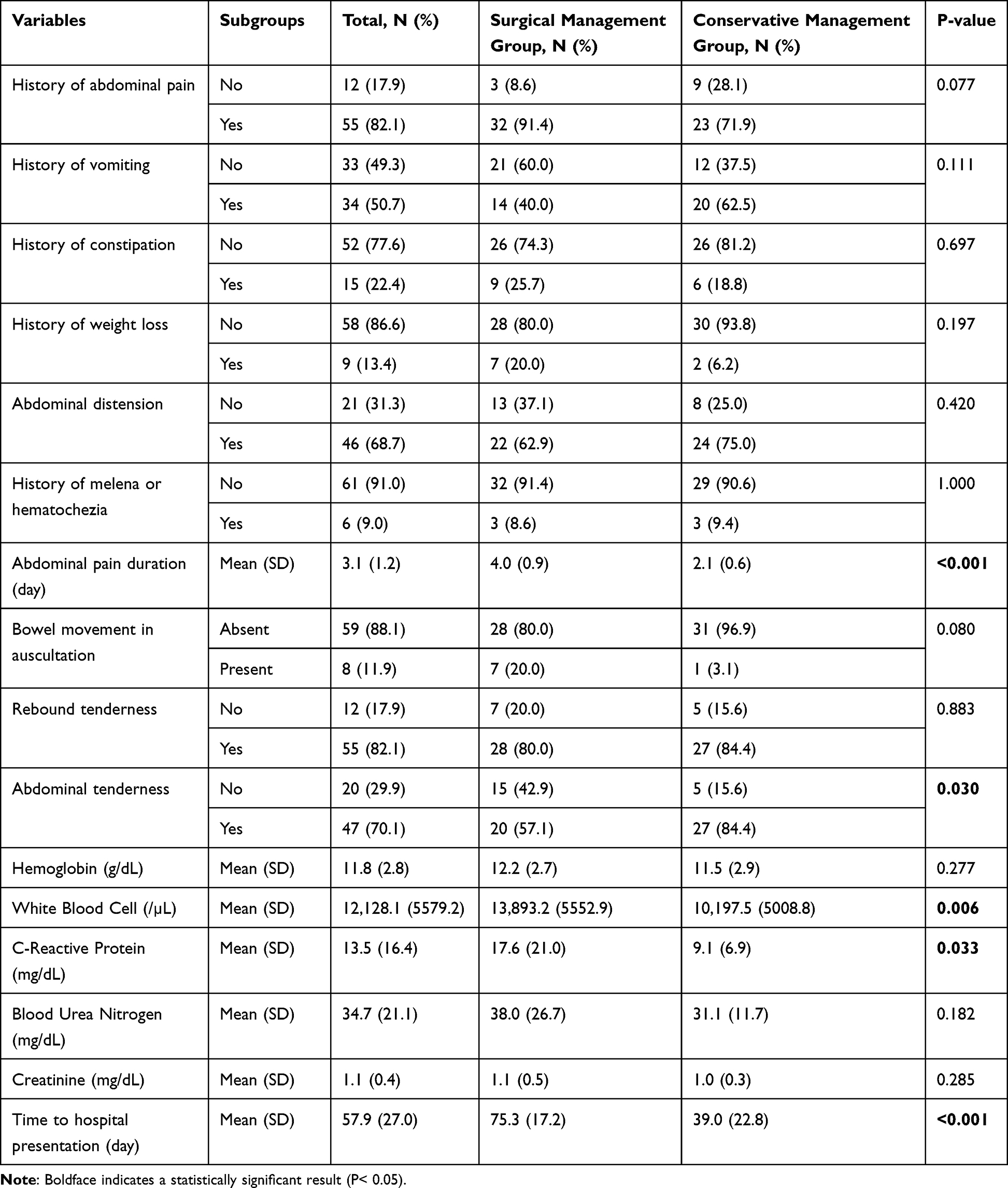 |
Table 2 History, Physical Exam Findings, and Laboratory Data of Patients with Virgin Abdomen and Small Bowel Obstruction |
 |
Table 3 The Main Etiology of Patients with Virgin Abdomen and Small Bowel Obstruction |
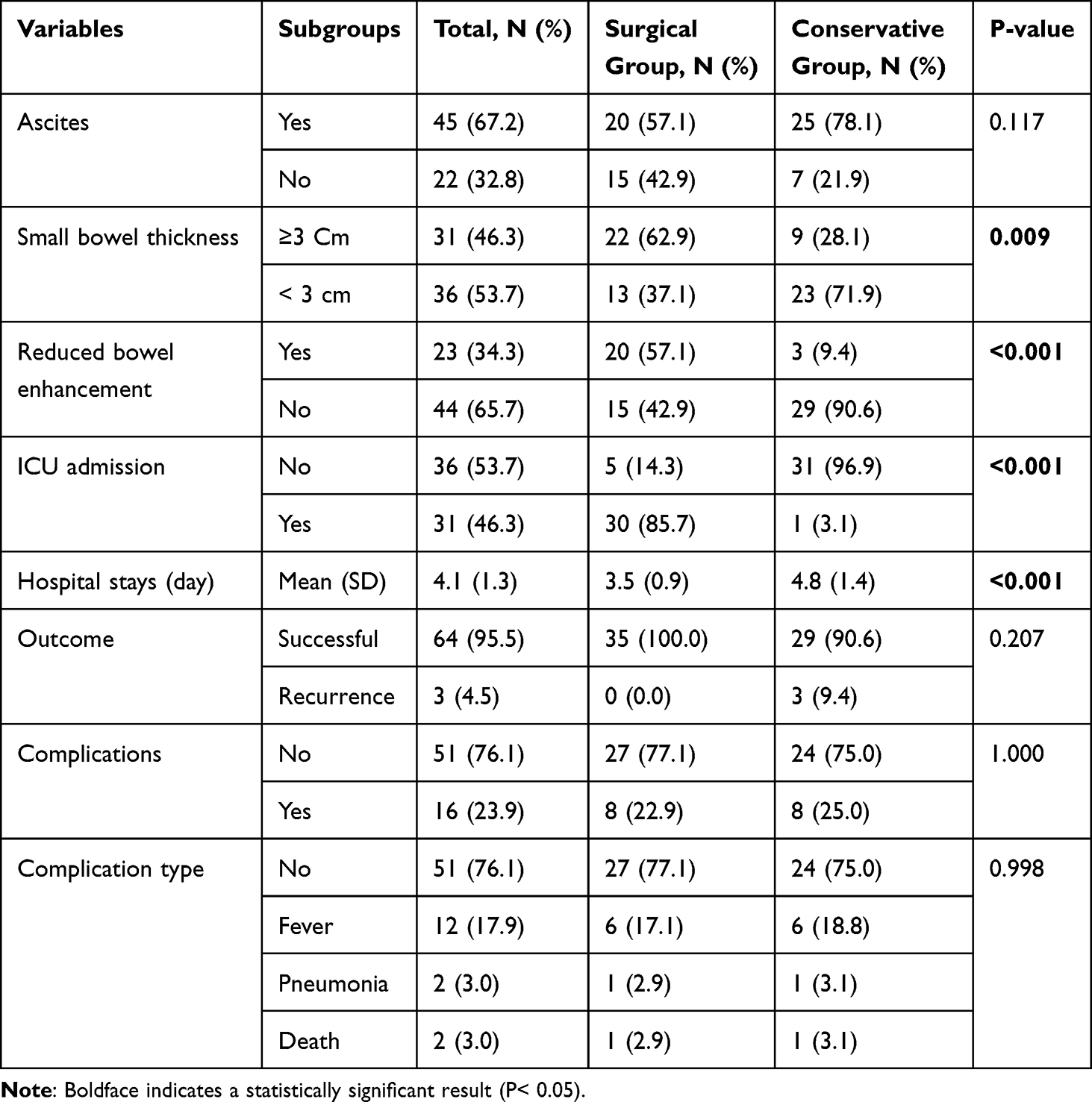 |
Table 4 Radiologic Findings, Operative and Postoperative Outcome of Patients with Virgin Abdomen and Small Bowel Obstruction |
 |
Figure 1 Intraoperative photos showing: (A) Small bowel tumor with adhesion in a 55-year-old male who underwent resection and anastomosis. (B) adhesion in a 30-year-old male who underwent adhesiolysis. (C) Mesenteric ischemia in a 62-year-old male due to superior mesenteric thrombosis that underwent open and closed surgery. (D) Tuberculosis in a 21-year-old female who underwent a biopsy. |
 |
Figure 2 Intraoperative photos showing: (A and B) ileocecal intussusception in a 19-year-old female who underwent surgical exploration. (C and D) Volvulus of small intestinal in a 49-year-old male who underwent resection and anastomosis. (E) Closed Loop Obstruction in a 36-year-old male who underwent release and external (serosal) anastomosis. (F) Peritoneal carcinomatosis (mesenteric lymphoma) in a 66-year-old male who underwent a biopsy. |
Factors Associated with Urgent Surgical Management
Factors associated with surgical management were older age (58.8 ±11.7 vs 44.9 ±13.8 years, p<0.001), previous hospital admission (p<0.001), presence of abdominal tenderness (p=0.030), longer abdominal pain duration (4.0 ±0.9 vs 2.1 ±0.6 days, p<0.001), higher CRP (p= 0.033), higher WBC (p= 0.006), longer time to hospital presentation (75.3 ±17.2 vs 39.0 ±22.8 days, p= <0.001), small bowel thickness on CT scan image (p=0.009), reduced bowel enhancement on CT scan (p <0.001). Additionally, in surgical group, the need for ICU admission was higher and hospital stays were shorter than in conservative group (3.5 ±0.9 vs 4.8 ±1.4 days) and were statistically significant (p< 0.05).
Discussion
The complexity of SBO arises from the absence of distinct clinical findings that can pinpoint its etiology.14 Furthermore, when compared with adhesive SBO in patients with previous surgeries, there is a notable dearth of guidelines, protocols and consensus in the literature regarding the optimal diagnostic or therapeutic approaches.15
We studied 67 patients with SBO-VA, among whom adhesions emerged as the predominant cause, accounting for 23.9%, followed by closed loop obstruction (19.4%) and internal hernia (16.4%). Neoplasm or metastasis constituted roughly 7.5% of the cases. These data challenge the prevailing perception that mandates surgical exploration in VA-SBO due to potential hidden malignancies.8 Numerous prior studies had echoed our findings. For instance, Beardsley et al underscored adhesions as the principal cause of SBO-VA,6 a sentiment endorsed by subsequent studies thereafter.16,17 Adhesions are traditionally seen as consequences of intra-peritoneal inflammation from surgical trauma, which results in fibrinogen deposition with reduced metalloproteinase activity with the resultant formation of adhesive bands, it can also be induced by infections, radiation, neoplasia, or endometriosis.6,9,18,19
The inclination towards surgical intervention in SBO-VA has predominantly been driven by the perceived risk of underlying malignancy, even in the absence of compelling evidence indicating superior outcomes or mortality benefits.6 This approach has been adopted at high institutional level.20,21 Past retrospective analyses have highlighted a commendable success rate for non-operative management of SBO-VA, approximating 86%.16,22 However, these data points are not uniform. For example, Collom et al reported a failure rate of 17% for SBO-VA patients treated conservatively using water-soluble contrast agents. The scenario becomes more intricate when noting that this failure rate climbs to 50% in patients who did not receive the oral contrast.22 Furthermore, a recent systematic review, incorporating two cohort studies and four case reports, posited the success rate of conservative management to lie between 50 and 70% for SBO-VA.23 In comparison to these findings, our research reported a success rate of 90.6% for non-operative strategies in the context of SBO-VA.
Unlike SBO cases in patients with prior surgical interventions, clear indicators or predictors of surgical exploration in SBO-VA are not well-studied in the literature. Moreover, the frequently ambiguous rationale behind the surgical intervention in SBO-VA—attributable to the retrospective nature of most studies and the inherent subjectivity when deciding on surgical intervention—complicates the formulation of definitive assessments or preliminary conclusions. This complexity resonates with findings from various studies, including our own.17 It’s worth noting that while the avoidance of unnecessary intervention is crucial, it should not inadvertently lead to undue delays in required procedures.
In our study, we identified older age, prior hospital admissions, extended duration of abdominal pain, abdominal tenderness, elevated inflammatory markers, and specific CT scan alarm signs predominantly influenced the decision for urgent surgical exploration in SBO-VA patients, all of which bore statistical significance. There is a paucity of data constrains a comprehensive comparative analysis of these findings. From available literature, earlier studies have pointed to a more pronounced incidence of SBO-VA stemming from malignancies in older populations.24,25 Notably, within this older demographic, there appears to be a significant bias against the success of conservative management, often leading to surgical interventions. However, the actual benefits of these surgical procedures, especially in terms of reducing mortality, remain unclear. For instance, a study by Springer et al disclosed a 3% mortality rate among elderly patients who opted for early surgical exploration, in contrast to a 14% rate in the conservative group—findings that lacked statistical significance.26,27 Furthermore, our study also highlighted abdominal tenderness and elevated inflammatory markers as vital indicators suggesting the need for surgical intervention, which may indicate potential peritonitis.15 However, clinicians must approach these markers with caution due to their limited sensitivity and specificity, understanding that their absence does not rule out potential peritoneal involvement.28,29
Our research also highlighted certain Computed Tomography (CT) scan findings, such as mesenteric fat-stranding or edema, and the absence of small bowel fecal signs, as potential indicators for surgical intervention, a conclusion mirrored in earlier reports.30,31 These findings should not endorse the mere reliance on CT imaging to establish the etiology, or predicting the necessity of surgical intervention; as the utility of CT scan in diagnosing SBO-VA is limited, with a reported accuracy of less than 53%.32 This underlines the importance of a holistic clinical evaluation encompassing both clinical presentation and auxiliary laboratory and imaging findings.
Various studies have reported a number of factors potentially predicting the need for surgical intervention. For instance, the notable O’Leary et al study had flagged chronic abdominal pain, distention persisting beyond 48 hours, and pronounced SBO obstruction evident in CT scans as predictors of surgical exploration.33 These findings may not apply to SBO-VA scenarios, as these cases compromised the minority or were completely excluded from the studied populations, as evident in Table 5.12,13,19,33–36 A recent report by Blich et al, focusing exclusively on SBO-VA cases, could not conclusively correlate any clinical, laboratory, or imaging findings with the imperative for surgical intervention.19 However, there was no observed difference in outcome between the two treatment groups. In addition, the reasoning behind surgical intervention was not identified in the majority of SBO-VA retrospective studies. This recurrent predicament accentuates the inherent limitations of retrospective studies, advocating for more expansive, prospective studies.
 |
Table 5 Predictors for Surgical Intervention of Patients with Virgin Abdomen and Small Bowel Obstruction in Previously Reported Articles |
In our study, three patients who received conservative management experienced recurrence, necessitating subsequent surgical intervention. Such recurrences, based on previous studies, seem to be infrequent. For instance, Tavangari et al noted a recurrence in 5 out of 63 patients who had opted for conservative treatment.34 While long-term follow-up remains a recognized limitation in SBO-VAstudies, a review by Strajina et al, with a median follow-up of 34 ± 28 months, indicated a recurrence rate of 15% among patients managed conservatively, in contrast to a 7% rate in those who underwent surgical procedures.37 Another study reported even lower recurrence rates of 3.5% and 2.3% for conservative and operative groups, respectively.9 A notable limitation of these studies is the relatively small sample sizes, coupled with a lack of stratification based on underlying etiology (Other reported underlying etiology for bowel obstruction such as transient small bowel intussusception, gallstone ileus, and Meckel’s diverticulum have been reported in previous studies).38,39 Moreover, the rationale behind choosing either conservative or surgical management remains unclear in these studies. We believe that there is a pressing need for prospective studies to yield more precise and relevant data.
Surgical site infection (SSI) is the most common postoperative complication after colorectal surgery for bowel obstruction with a reported incidence ranging from 3% to 30%, causing pain and suffering to patients.40 In addition, this complication has been associated with negative economic impact, increased morbidity, extended postoperative hospital stay, readmission, sepsis, and death. In this study, the complications occurred in 23.9%, and the most common postoperative complication was fever in 17.9%.
Study Limitations
The primary limitation of this study stems from its reliance on secondary data, which is susceptible to inconsistencies due to varied documentation, data integrity, and record-keeping practices. This issue is compounded by the study’s retrospective design, introducing potential biases that could influence results. Furthermore, the small sample size might not capture the broader nuances of the studied population, and there’s an observed lack of comprehensive data on certain preoperative factors. As highlighted in previous discussions, a notable limitation is the absence of long-term follow-up, a recognized challenge in VA-SBO studies. Additionally, ambiguous rationales for choosing between conservative and surgical management could influence the datasets used. To fortify the reliability and depth of findings, it would be advantageous to conduct a prospective study with a larger cohort and a more detailed exploration of preoperative factors.
Conclusion
The main etiologies for SBO-VA in our study were adhesions. Older age, previous hospital admission, longer abdominal pain duration, abdominal tenderness, increased inflammatory markers, and alarm signs on CT scans are the main factors for determining the need for urgent surgical exploration in patients with SBO-VA. To achieve prompt identification and intervention, it is crucial to maintain a high level of vigilance and awareness, even in individuals without any previous medical or surgical history.
Data Sharing Statement
All the data was included in this study.
Ethics Approval and Informed Consent
We declare that our study was approved by the ethical committee of Ibb University with code number: IBBUNI.AC.YEM.2023.102. The current study was performed according to the Institutional Committee for the Protection of Human Subjects, which was adopted by the 18th World Medical Assembly, Helsinki, Finland, and its later amendments. Written informed consent was obtained from the patients.
Consent for Publication
Written informed consent was obtained from the patients including the figures.
Acknowledgments
The authors would like to thank the general manager of Al-Thora General Hospital and Al-Nassar Hospital, Ibb, Yemen, Dr. Abdulghani Ghabisha, for editorial assistance.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Taylor MR, Lalani N. Adult small bowel obstruction. Acad Emerg Med. 2013;20(6):528–544. doi:10.1111/acem.12150
2. Gore RM, Silvers RI, Thakrar KH, et al. Bowel Obstruction. Radiol Clin North Am. 2015;53(6):1225–1240. doi:10.1016/j.rcl.2015.06.008
3. Li C, Pallas R, Frewer N, Cornish J, Ellis-Owen R. Can we detect fibrofatty band in patients with bowel obstruction on CT scan? BJR Case Rep. 2021;7(5):20210016. doi:10.1259/bjrcr.20210016
4. Mucha P Jr. Small intestinal obstruction. Surg Clin North Am. 1987;67(3):597–620. doi:10.1016/S0039-6109(16)44234-9
5. Holcombe C. Surgical emergencies in tropical gastroenterology. Gut. 1995;36(1):9–11. doi:10.1136/gut.36.1.9
6. Beardsley C, Furtado R, Mosse C, et al. Small bowel obstruction in the virgin abdomen: the need for a mandatory laparotomy explored. Am J Surg. 2014;208(2):243–248. doi:10.1016/j.amjsurg.2013.09.034
7. Bresler L, Braun E, Debs A, Boissel P, Grosdidier J. Emergency surgery in colonic obstructions. Retrospective study of 70 cases. J Chir. 1986;123(12):713–718.
8. Zielinski MD, Bannon MP. Current management of small bowel obstruction. Adv Surg. 2011;45(1):1–29. doi:10.1016/j.yasu.2011.03.017
9. Ng YY, Ngu JC, Wong AS. Small bowel obstruction in the virgin abdomen: time to challenge surgical dogma with evidence. ANZ J Surg. 2018;88(1–2):91–94. doi:10.1111/ans.13714
10. Matsushima K, Sabour A, Park C, Strumwasser A, Inaba K, Demetriades D. Management of adhesive small bowel obstruction: a distinct paradigm shift in the United States. J Trauma Acute Care Surg. 2019;86(3):383–391. doi:10.1097/TA.0000000000002150
11. Bickell NA, Federman AD, Aufses AH Jr. Influence of time on risk of bowel resection in complete small bowel obstruction. J Am Coll Surg. 2005;201(6):847–854. doi:10.1016/j.jamcollsurg.2005.07.005
12. Zielinski MD, Eiken PW, Bannon MP, et al. Small bowel obstruction-who needs an operation? A multivariate prediction model. World J Surg. 2010;34(5):910–919. doi:10.1007/s00268-010-0479-3
13. Ng ZQ, Hsu V, Tee WWH, Tan JH, Wijesuriya R. Predictors for success of non-operative management of adhesive small bowel obstruction. World J Gastrointest Surg. 2023;15(6):1116–1124. doi:10.4240/wjgs.v15.i6.1116
14. Rubesin SE, Gore RM. 46 - Small Bowel Obstruction. In: Gore RM, Levine MS, editors. Textbook of Gastrointestinal Radiology.
15. ten Broek RPG, Krielen P, Di Saverio S, et al. Bologna guidelines for diagnosis and management of adhesive small bowel obstruction (ASBO): 2017 update of the evidence-based guidelines from the world society of emergency surgery ASBO working group. World J Emerg Surg. 2018;13(1):24. doi:10.1186/s13017-018-0185-2
16. Skeie E, Koch AM, Harthug S, et al. A positive association between nutritional risk and the incidence of surgical site infections: a hospital-based register study. PLoS One. 2018;13:e0197344.
17. Amara Y, Leppaniemi A, Catena F, et al. Diagnosis and management of small bowel obstruction in virgin abdomen: a WSES position paper. World J Emerg Surg. 2021;16(1):36. doi:10.1186/s13017-021-00379-8
18. Rajfer J. Role of fibrin in the development of surgical adhesions. Rev Urol. 2005;7(4):238–239.
19. Blich O, Nesher G, Tankel J, et al. Small Bowel Obstruction in Patients without Prior Abdominal Surgery: to Operate or Not? World J Surg. 2022;46(12):2919–2926. doi:10.1007/s00268-022-06719-2
20. Aquina CT, Becerra AZ, Probst CP, et al. Patients With Adhesive Small Bowel Obstruction Should Be Primarily Managed by a Surgical Team. Ann Surg. 2016;264(3):437–447. doi:10.1097/SLA.0000000000001861
21. McCloy C, Brown TC, Bolton JS, Bowen JC, Fuhrman GM. The etiology of intestinal obstruction in patients without prior laparotomy or hernia. Am Surg. 1998;64(1):19–22.
22. Fukami Y, Kaneoka Y, Maeda A, Takayama Y, Takahashi T, Uji M. Clinical Effect of Water-Soluble Contrast Agents for Small Bowel Obstruction in the Virgin Abdomen. World J Surg. 2018;42(1):88–92. doi:10.1007/s00268-017-4174-5
23. Bayat Z, Guttman MP, Shiroky J, Karanicolas PJ. Non-operative Management of Small Bowel Obstruction in Patients with No Previous Abdominal Surgery: a Systematic Review and Meta-analysis. World Journal of Surgery. 2021;45(7):2092–2099. doi:10.1007/s00268-021-06061-z
24. Quero G, Covino M, Laterza V, et al. Adhesive small bowel obstruction in elderly patients: a single-center analysis of treatment strategies and clinical outcomes. Scand J Gastroenterol. 2021;56(7):784–790. doi:10.1080/00365521.2021.1921256
25. Blair SL, Chu DZ, Schwarz RE. Outcome of palliative operations for malignant bowel obstruction in patients with peritoneal carcinomatosis from nongynecological cancer. Ann Surg Oncol. 2001;8(8):632–637. doi:10.1007/s10434-001-0632-1
26. Ozturk E, van Iersel M, Stommel MMWJ, Schoon Y, ten Broek RRPG, van Goor H. Small bowel obstruction in the elderly: a plea for comprehensive acute geriatric care. World J Emerg Surg. 2018;13(1):48. doi:10.1186/s13017-018-0208-z
27. Springer JE, Bailey JG, Davis PJ, Johnson PM. Management and outcomes of small bowel obstruction in older adult patients: a prospective cohort study. Can J Surg. 2014;57(6):379–384. doi:10.1503/cjs.029513
28. Sarr MG, Bulkley GB, Zuidema GD. Preoperative recognition of intestinal strangulation obstruction. Prospective evaluation of diagnostic capability. Am J Surg. 1983;145(1):176–182. doi:10.1016/0002-9610(83)90186-1
29. Loftus T, Moore F, VanZant E, et al. A protocol for the management of adhesive small bowel obstruction. J Trauma Acute Care Surg. 2015;78(1):13–19. doi:10.1097/TA.0000000000000491
30. Makar RA, Bashir MR, Haystead CM, et al. Diagnostic performance of MDCT in identifying closed loop small bowel obstruction. Abdom Radiol. 2016;41(7):1253–1260. doi:10.1007/s00261-016-0656-4
31. Zielinski MD, Eiken PW, Heller SF, et al. Prospective, observational validation of a multivariate small-bowel obstruction model to predict the need for operative intervention. J Am Coll Surg. 2011;212(6):1068–1076. doi:10.1016/j.jamcollsurg.2011.02.023
32. Desser TS, Gross M. Multidetector row computed tomography of small bowel obstruction. Semin Ultrasound CT MR. 2008;29(5):308–321. doi:10.1053/j.sult.2008.06.004
33. O’Leary EA, Desale SY, Yi WS, et al. Letting the sun set on small bowel obstruction: can a simple risk score tell us when nonoperative care is inappropriate? Am Surg. 2014;80(6):572–579. doi:10.1177/000313481408000621
34. Tavangari FR, Batech M, Collins JC, Tejirian T. Small Bowel Obstructions in a Virgin Abdomen: is an Operation Mandatory? Am Surg. 2016;82(10):1038–1042. doi:10.1177/000313481608201040
35. van Veen T, Ramanathan P, Ramsey L, Dort J, Tabello D. Predictive factors for operative intervention and ideal length of non-operative trial in adhesive small bowel obstruction. Surg Endosc. 2023;37(11):8628–8635. doi:10.1007/s00464-023-10282-9
36. Schwenter F, Poletti PA, Platon A, Perneger T, Morel P, Gervaz P. Clinicoradiological score for predicting the risk of strangulated small bowel obstruction. Br J Surg. 2010;97(7):1119–1125. doi:10.1002/bjs.7037
37. Strajina V, Kim BD, Zielinski MD. Small bowel obstruction in a virgin abdomen. Am J Surg. 2019;218(3):521–526. doi:10.1016/j.amjsurg.2019.02.011
38. Mulita F, Tchabashvili L, Liolis E, Maroulis I. Transient small bowel intussusception in a 30-year-old male. Prz Gastroenterol. 2021;16(3):252–253. doi:10.5114/pg.2021.108991
39. Mulita F, Tchabashvili L, Bousis D, et al. Gallstone ileus: a rare cause of small intestine obstruction. Clin Case Rep. 2021;9(11):e04924. doi:10.1002/ccr3.4924
40. Panos G, Mulita F, Akinosoglou K, et al. Risk of surgical site infections after colorectal surgery and the most frequent pathogens isolated: a prospective single-centre observational study. Med Glas. 2021;18(2):438–443. doi:10.17392/1348-21
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.