Back to Journals » Nature and Science of Sleep » Volume 18

Sleep Rhythmicity as a Core Domain of Multidimensional Sleep Health Associated with Cognitive Impairment in Older Men
Authors Chen C ![]() , Zhang M
, Zhang M ![]() , Wang Z
, Wang Z ![]() , Qu S
, Qu S ![]() , Liu X
, Liu X ![]() , Zhang C
, Zhang C ![]() , Deng J, Bao Y, Shi J, Li W, Lu L, Shi L
, Deng J, Bao Y, Shi J, Li W, Lu L, Shi L ![]()
Received 12 February 2026
Accepted for publication 14 May 2026
Published 9 July 2026 Volume 2026:18 598846
DOI https://doi.org/10.2147/NSS.S598846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Chunlin Chen,1,* Miaoyu Zhang,2,* Zhilin Wang,1 Shanshan Qu,1 Xinying Liu,1 Chi Zhang,2 Jiahui Deng,1 Yanping Bao,3 Jie Shi,3 Wenqiang Li,2 Lin Lu,1,3,4 Le Shi1
1Peking University Sixth Hospital, Peking University Institute of Mental Health, NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, 100191, People’s Republic of China; 2Henan Mental Hospital, The Second Affiliated Hospital of Xinxiang Medical University; Henan Key Laboratory of Biological Psychiatry, Henan Collaborative Innovation Center of Prevention and Treatment of Mental Disorder, Xinxiang Medical University, Xinxiang, 453003, People’s Republic of China; 3National Institute on Drug Dependence and Beijing Key Laboratory of Drug Dependence, Peking University, Beijing, 100191, People’s Republic of China; 4Peking-Tsinghua Center for Life Sciences and PKU-IDG/Mcgovern Institute for Brain Research, Peking University, Beijing, 100871, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Le Shi, Peking University Sixth Hospital, Peking University Institute of Mental Health, NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, 100191, People’s Republic of China, Tel +86-10-82803704, Fax +86-10-62032624, Email [email protected] Lin Lu, Peking University Sixth Hospital, Peking University Institute of Mental Health, NHC Key Laboratory of Mental Health (Peking University), National Clinical Research Center for Mental Disorders (Peking University Sixth Hospital), Beijing, 100191, People’s Republic of China, Tel +86-10-82803704, Fax +86-10-62032624, Email [email protected]
Purpose: Sleep encompasses multiple dimensions, each potentially involving distinct parameters that collectively capture the complex features of sleep health. However, limited studies focused on the construction of objective sleep multidimensions and its associations with cognitive impairment.
Patients and Methods: The study included 2670 community-dwelling older men from the Osteoporotic Fractures in Men study. Wrist actigraphy was used to collect sleep data. Latent sleep dimensions were identified from objectively measured sleep parameters using exploratory factor analysis without prespecified structures. Longitudinal associations between sleep domains and cognitive impairment were evaluated using Cox proportional hazards models over a mean follow-up of 7.4 years. XGBoost with SHapley Additive exPlanations (SHAP) was used to rank the predictive importance of each domain.
Results: Five dimensions of sleep health framework were identified: rhythmicity, quality, duration, regularity, and timing. Disrupted rhythmicity was significantly associated with an increased risk of cognitive impairment (HR = 1.21, 95% CI: 1.07– 1.37, p = 0.002). Longer duration (HR = 1.13, 95% CI: 1.00– 1.28, p = 0.043), poorer regularity (HR = 1.13, 95% CI: 1.00– 1.27, p = 0.046) and lower quality (HR = 1.13, 95% CI: 1.01– 1.27, p = 0.040) were also linked to elevated risk in fully adjusted model. No significant association was observed between timing and cognitive impairment. SHAP analysis indicated that rhythmicity ranked high in predictive importance compared with traditional risk factors and was the most influential domain among the sleep dimensions. After stratification, disrupted rhythmicity remained significantly associated with cognitive impairment in most demographic and lifestyle subgroups.
Conclusion: Our integrative modelling approach provides novel insights into the complex relationships between distinct sleep domains and cognitive impairment, highlighting rhythmicity as a key factor for preserving cognitive health in aging men. These findings suggest that sleep-related interventions, especially for management of rhythmicity, may be a promising approach for the prevention of cognitive impairment.
Keywords: sleep, cognitive impairment, rhythmicity, aging, actigraphy
Introduction
Cognitive impairment is a major health problem affecting older people worldwide, which not only leads to a serious decline in personal quality of life, but also brings a huge burden of care and economic costs to society.1 With the acceleration of the aging process of the population, finding modifiable factors to reduce the occurrence and development of cognitive impairment becomes a priority for public health and neuroscience research.2
Sleep is a complex and multidimensional physiological process essential for brain recovery and cognitive maintenance, and its relevance to cognitive impairment is well established.3,4 However, previous studies focused on individual sleep parameters in isolation, such as total sleep duration, sleep efficiency, and wake after sleep onset.5–9 This approach of using a single metric to represent domains of sleep health is inherently limited,10,11 for it does not capture the integrative physiological meaning of sleep as a unified construct, nor does it elucidate the underlying relationship among individual sleep parameters or the relative contributions of different sleep domains.
To address these limitations, recent research has moved toward constructing multidimensional sleep frameworks using data-driven approaches, allowing multiple sleep characteristics to be summarized into underlying domains.11,12 While these approaches provide a more comprehensive representation of sleep structure, their implications for clinically relevant outcomes, particularly cognitive impairment, remain less well understood. In this study, we applied a data-driven strategy using objective actigraphy data from the Osteoporotic Fractures in Men (MrOS) Sleep Study to construct a comprehensive sleep framework. We then examined their longitudinal associations with incident cognitive impairment using Cox proportional hazards models and further quantified their relative importance based on interpretable machine-learning approaches. We aimed to identify which objectively defined sleep domains are independently associated with cognitive impairment and to determine their relative contributions to cognitive outcomes in older men.
Methods
Study Population
The MrOS Sleep Study is an ancillary study of the parent MrOS cohort, a multicenter cohort study of community-dwelling older men (website: https://mrosonline.ucsf.edu).13 Between 2003 and 2005, a total of 3135 community-dwelling men aged 65 years or older were recruited from six US clinical centers (Birmingham, AL; Minneapolis, MN; Palo Alto, CA; Pittsburgh, PA; Portland, OR; and San Diego, CA). Cognitive assessments were subsequently administered at baseline and at four follow-up examinations (2005–2006 [mean follow-up 1.2 years], 2007–2009 [3.4 years], 2009–2012 [6.5 years], and 2014–2016 [10.8 years]). Among the 5994 men originally enrolled in the MrOS cohort, 3135 participated in the MrOS Sleep Study. Participants were excluded if they had cognitive impairment at baseline or lacked cognitive assessments (n = 143), had no actigraphy data (n = 77), had no follow-up cognitive evaluations (n = 138), or had missing information on sleep variables or covariates (n = 107). The final analytic sample consisted of individuals with complete data on sleep measures, covariates, and at least one cognitive assessment during follow-up (Supplementary Figure 1).
Sleep Variables Assessed by Actigraphy
In the MrOS Sleep Study, participants were instructed to wear an actigraphy device (Sleep-Watch-O, Ambulatory Monitoring, Inc., Ardsley, NY) on their non-dominant wrist for at least three consecutive 24-hour periods (mean ± SD: 5.13 ± 0.84 days). Activity data were recorded in 1-minute epochs. Sleep-wake states were derived from the actigraphy data using proportional integration mode with UCSD sleep-scoring algorithm.14 Actigraphy data were averaged across all valid nights for each participant to derive summary sleep parameters. Periods with excessive non-wear (defined as >2 hours during in-bed intervals or >10% of daytime intervals) were excluded to ensure data quality. Based on sleep data, we derived sleep variables and rest-activity rhythm metrics that met the following criteria:12,15 (1) obtained from actigraphy data related to sleep; (2) related to potential clinical and/or scientific relevance to cognitive impairment. Key sleep variables we focused on included sleep duration, sleep onset time, time in bed, midpoint of sleep, from sleep onset to wake, wake after sleep onset, sleep efficiency, and number of awakenings. Within rest-activity rhythm metrics, we included interdaily stability (IS), intradaily variability (IV), pseudo-F statistic (PsF), and acrophase,16 as they are closely related to sleep-wake patterns.17–20 IS quantifies the consistency of rest-activity rhythms across days, with higher values indicating greater sleep stability. IV reflects the degree of rhythm fragmentation, with higher values denoting more fragmented sleep. PsF represents the robustness or strength of the rhythmic pattern, where higher values suggest a stronger and more consolidated rhythm. Acrophase characterizes the timing of peak activity within the circadian cycle. Earlier acrophase values correspond to a tendency for earlier sleep preference, whereas later values indicate delayed sleep preference.
Cognitive Outcome
Cognitive assessments were conducted by trained staff during each clinic visit. The Modified Mini-Mental State (3MS) examination evaluated cognitive performance on a scale ranging from 0 to 100.21 Higher 3MS scores reflect better cognitive function, while declining scores indicate cognitive deterioration. Previous research has demonstrated that the 3MS provides high diagnostic accuracy for dementia using a cutoff score of 80.21,22 Cognitive impairment in this study was defined as (1) a 3MS score < 80 during follow-up visit; or (2) a self-reported physician diagnosis of dementia; or (3) use of medication for treating dementia. Participants with cognitive impairment at baseline were excluded. Follow-up duration was determined across four visits, and participants were censored at the occurrence of a cognitive event or at their last attended visit, whichever occurred first.
Covariates
Covariates were selected based on prior literature and established biological relevance to cognitive impairment. Demographic, lifestyle, and health-related factors included age at the sleep visit, race, body mass index (BMI), study site, marital status (married, widowed, separated/divorced or single), living arrangement (live alone or live with spouse, family or roommate), education level, smoking status, alcohol use, self-rated health condition, depressive symptoms assessed by the Geriatric Depression Scale, physical activity assessed by the Physical Activity Scale for the Elderly (PASE), sleep medications within the past 30 days (nonbenzodiazepines and nonbarbiturate sedative-hypnotics), caffeine intake, and tea consumption. Sleep apnea was defined as a self-reported physician diagnosis. Frailty at baseline was defined according to criteria established in previous MrOS studies:23 (1) shrinking, defined as unintentional weight loss of ≥5% since the baseline MrOS examination (mean ± SD years between examinations: 3.60 ± 0.49); (2) weakness, defined as grip strength in the lowest quintile within BMI quartiles or being unable to complete the grip strength test; (3) low energy, defined as a negative response to the item “Do you feel full of energy?” from the Geriatric Depression Scale; (4) slowness, defined as walking speed in the lowest height-stratified quintile or being unable to complete the walking test; and (5) low physical activity, defined as a PASE score in the lowest quintile. Frailty status was defined as follows: robust (0 components), intermediate stage (1–2 components), and frail (≥3 components). In addition, self-reported medical comorbidities, including hypertension, congestive heart failure, stroke, myocardial infarction, transient ischemic attack, angina, coronary heart disease, cerebrovascular disease, diabetes, cancer, cataracts, and hearing problems, were included to account for chronic conditions that may influence both sleep characteristics and cognitive outcomes.
Statistical Analysis
Exploratory factor analysis (EFA) was conducted to identify sleep domains based on the actigraphy-derived sleep variables.24 Prior to analysis, all sleep variables were standardized (mean = 0, SD = 1) to ensure comparability across measures and to improve model stability. To ensure the data sample was suitable for factor analysis, we performed Bartlett’s test of sphericity (p < 0.05) to confirm patterned relationships among variables, and computed the Kaiser-Meyer-Olkin measure of sampling adequacy, with values above 0.6 considered acceptable. In line with previous research, we applied a “quartimax” orthogonal rotation using the psych package in R to simplify the factor structure and enhance interpretability, allowing the data structure to emerge without predefined domains.12,25
Factors were extracted using maximum likelihood estimation. The number of factors was determined based on multiple criteria, including parallel analysis, eigenvalues, visual inspection of the scree plot, and theoretical interpretability. Parallel analysis compares observed eigenvalues with those obtained from randomly generated data, retaining factors with eigenvalues exceeding the corresponding random values. Variables were assigned to a factor if they had loadings greater than 0.6. When a variable loaded on multiple factors, it was assigned to the factor with the highest absolute loading. To maintain interpretive consistency, where higher factor scores indicate greater risk of cognitive impairment, certain sleep domain scores were reversed accordingly. Restricted cubic splines were employed to examine potential nonlinear relationships between sleep domains and the risk of cognitive impairment.26
The associations between sleep domains and cognitive impairment were examined using multivariable Cox proportional hazards regression models to calculate hazard ratios (HRs) and 95% confidence intervals (CIs). For covariates that violated the proportional hazards assumption, time-dependent effects were incorporated using an extended Cox regression model, allowing the effects of these variables to vary over time.27 Statistical significance was defined as P < 0.05. Three models were constructed: Model 1 adjusted for key demographic, lifestyle, and health-related factors, including age at the sleep visit, race, body mass index (BMI), study site, marital status (married, widowed, separated/divorced, or single), living arrangement (live alone or live with spouse, family or roommate), education level, smoking status, alcohol use, self-rated health condition, depressive symptoms and physical activity. Model 2 was further adjusted for major medical comorbidities, including hypertension, congestive heart failure, stroke, myocardial infarction, transient ischemic attack, angina, coronary heart disease, cerebrovascular disease, diabetes, cancer, cataracts, hearing problems and frailty. Based on model 2, model 3 further adjusted for sleep conditions, including sleep medications within the past 30 days (nonbenzodiazepines and nonbarbiturate sedative-hypnotics), caffeine intake, tea consumption, sleep apnea, and other sleep domains to account for their intercorrelations.
We applied the Extreme Gradient Boosting (XGBoost) algorithm with a Cox proportional hazards objective function to model the associations between sleep domains and the risk of cognitive impairment. To avoid overfitting and address potential multicollinearity, elastic net regression was first used for variable selection, incorporating the derived sleep domains, previously specified cognition‑related covariates, and baseline 3MS scores. The optimal penalty parameter (λ) was determined using 10-fold cross-validation, and variables with non-zero coefficients at the optimal λ were selected. After variable selection, the dataset was randomly divided into a training set (70%) and a testing set (30%). The model development and tuning were conducted on the training set, while model performance was independently evaluated on the testing set. A five-fold cross-validation framework was implemented within the training data to prevent overfitting and ensure model robustness. Model hyperparameters were optimized using Bayesian optimization with an expected improvement acquisition function. Early stopping rounds were applied to prevent overfitting during training. A complete list of hyperparameters is given in the supplementary. Feature importance and contribution were further interpreted using SHapley Additive exPlanations (SHAP) values, which quantify the marginal impact of each feature on model predictions. Analyses were performed using the glmnet, xgboost, rBayesianOptimization, and SHAPforxgboost packages in R (version 4.5.1).28–31
To minimize potential reverse causation, we conducted a sensitivity analysis excluding participants who developed the outcome within the first 2 years of follow-up in the Cox regression analysis. To more accurately define cognitive impairment, we excluded the 3MS component and restricted the outcome to self-reported dementia diagnoses only. We then examined the associations between sleep domains and the risk of dementia. Oblique rotations (oblimin and promax) were also applied in the EFA to allow for correlations between latent sleep domains and to assess the robustness of the identified factor structure. As cognitive impairment was assessed only at discrete follow-up visits, the exact onset time of the outcome was not directly observed. Therefore, we employed interval-censored Cox proportional hazards models. For each participant, the event interval was defined as the time between the last visit at which the participant was observed without evidence of cognitive impairment and the first visit at which cognitive impairment was identified. Participants who did not develop cognitive impairment during follow-up were treated as right-censored at their last available visit. These interval-censored data were analyzed using a semi-parametric proportional hazards model implemented in the icenReg R package.32
Results
Baseline Characteristics
Table 1 summarizes the demographic and clinical characteristics of the study participants according to cognitive outcomes. A total of 2670 participants were included in the analysis, among whom 285 (10.7%) developed cognitive impairment during a mean (SD) follow-up of 7.4 (3.7) years. The mean (SD) age at baseline was 76.0 (5.3) years, and most participants were White (91.6%). Compared with those who remained cognitively normal, participants who developed cognitive impairment were older, had a higher BMI, were less likely to be White, had lower educational attainment, reported more depressive symptoms, and exhibited more disrupted rhythm (reflected by lower IS and higher IV).
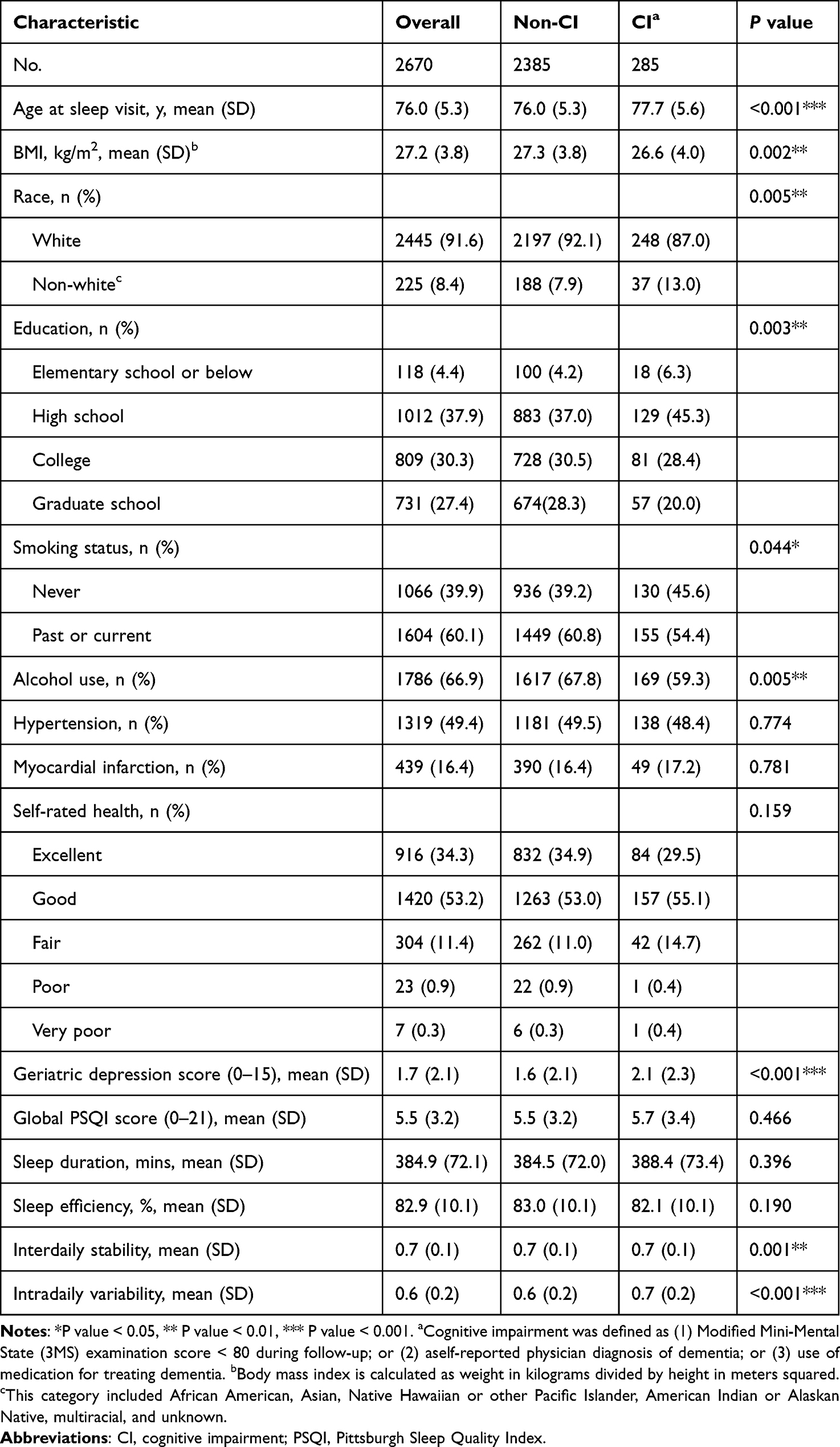 |
Table 1 Demographic Characteristics Stratified by Cognitive Outcome |
Construction of Sleep Domains
Using EFA, we established a multidimensional sleep framework from 15 sleep-related variables (Figure 1 and Supplementary Table 1). The number of domains was determined based on parallel analysis and visual inspection of the scree plot (Supplementary Figure 2). In accordance with previously proposed sleep health frameworks,11,12 five latent domains were identified, each representing distinct dimensions of sleep behavior: rhythmicity (sleep-wake pattern), timing (sleep preference for chronotype), regularity (deviation of sleep patterns across days), quality (sleep continuity and efficiency), and duration. This model accounted for 81.9% of the total variance, with strong intercorrelations observed among variables within each domain (Supplementary Figure 3).
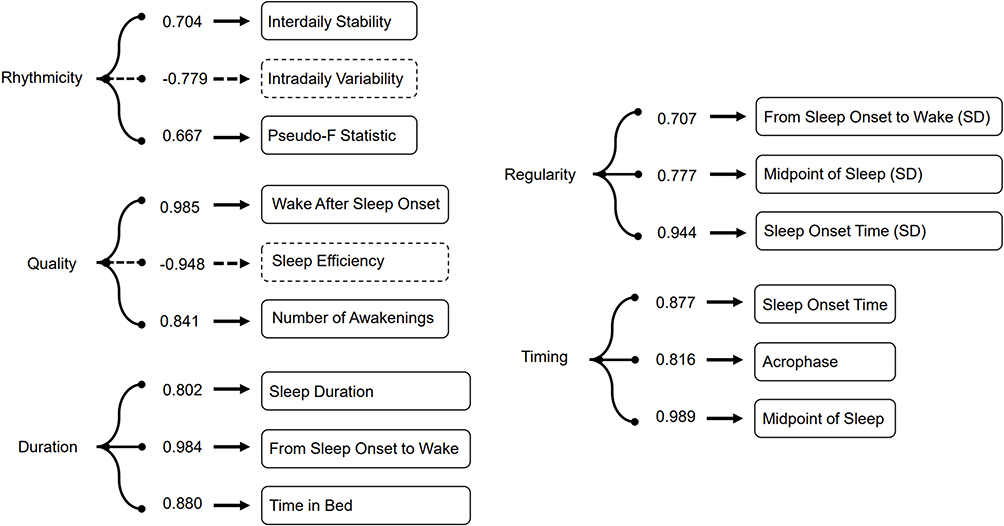 |
Figure 1 Exploratory factor analysis identified a five-factor model representing rhythmicity, quality, duration, regularity, and timing. Numbers indicate factor loadings for objective sleep variables; dashed line denotes negative associations between latent factors and their respective sleep variables. To maintain interpretive consistency, where higher factor scores indicate greater risk of cognitive impairment, rhythmicity was reversed in the following analysis. Abbreviation: SD, standard deviation. |
Associations of Sleep Domains and Risk of Cognitive Impairment
The Cox regression was used to examine the association of sleep domains and risk of cognitive impairment (Table 2). After adjusting for basic health-related factors and major medical comorbidities (Model 2), disrupted rhythmicity was significantly associated with a higher risk of cognitive impairment (HR = 1.20, 95% CI = 1.06–1.36, p = 0.003). Longer duration (HR = 1.14, 95% CI = 1.01–1.29, p = 0.033), and poorer regularity (HR = 1.13, 95% CI = 1.00–1.27, p = 0.046) were also significantly associated with greater cognitive impairment risk. No significant association was observed for quality (HR = 1.12, 95% CI = 0.99–1.26, p = 0.07) and timing (HR = 1.00, 95% CI = 0.88–1.13, p = 0.987). After mutual adjustment for all sleep domains and other sleep conditions (Model 3), rhythmicity (HR = 1.21, 95% CI: 1.07–1.37, p = 0.002), regularity (HR = 1.13, 95% CI = 1.00–1.27, p = 0.046), and duration (HR = 1.13, 95% CI = 1.00–1.28, p = 0.043) remained robustly associated with cognitive impairment. Sleep quality was not significant in Models 1 and 2 but became significantly associated with cognitive impairment after full adjustment for sleep conditions (HR = 1.13, 95% CI: 1.01–1.27, p = 0.040). No evidence of nonlinear association was observed between sleep domains and the risk of cognitive impairment (Supplementary Figure 4).
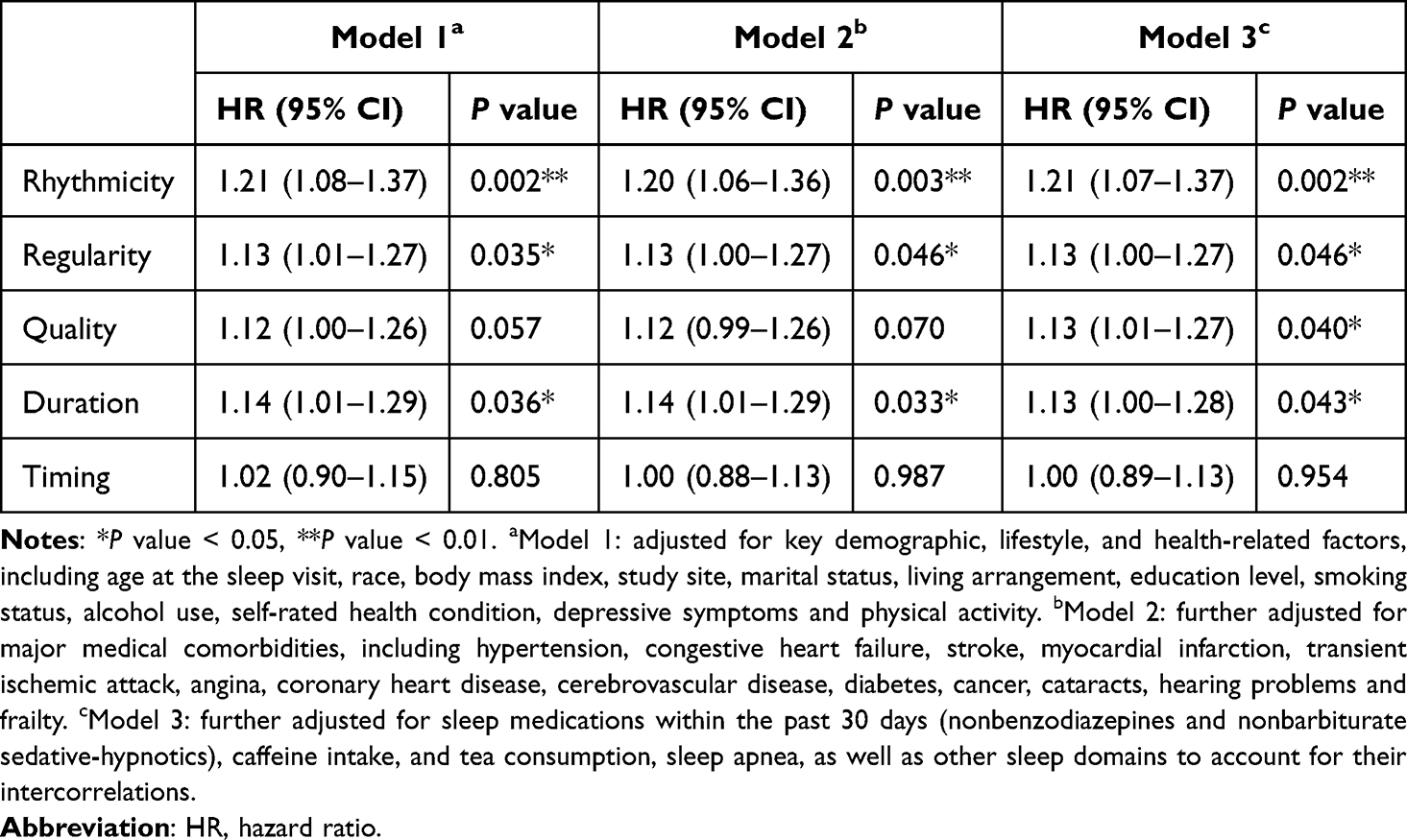 |
Table 2 Cox Regression Analysis of Sleep Domains and Risk of Cognitive Impairment |
Predictive Performance and Relative Importance of Sleep Domains in Cognitive Impairment
After variable selection, a total of 14 variables were included for subsequent analysis (Supplementary Table 2). In the best-performing XGBoost model, the concordance index (C-index) was 0.84 (95% CI: 0.80–0.89) for the training set and 0.74 (95% CI: 0.67–0.80) for the test set, indicating strong discriminative ability and good generalizability across datasets. Model hyperparameters are provided in Supplementary Table 3.
SHAP analysis was used to assess the relative importance of each predictor to the model output for cognitive impairment. As shown in Figure 2, baseline 3MS score was the most impactful factor (mean absolute SHAP value = 0.401), followed by frailty (0.297). Among sleep-related domains, rhythmicity ranked third overall (0.216), reflecting a consistent and substantial contribution to cognitive impairment. Regularity (0.172), quality (0.145) and duration (0.115) followed closely, each demonstrating comparable importance to conventional risk factors (Supplementary Table 4). Consistent with the Cox regression findings, the distribution of SHAP values across individuals suggested that lower rhythmicity, poorer sleep quality, longer sleep duration, and greater irregularity were associated with a higher predicted risk of cognitive impairment.
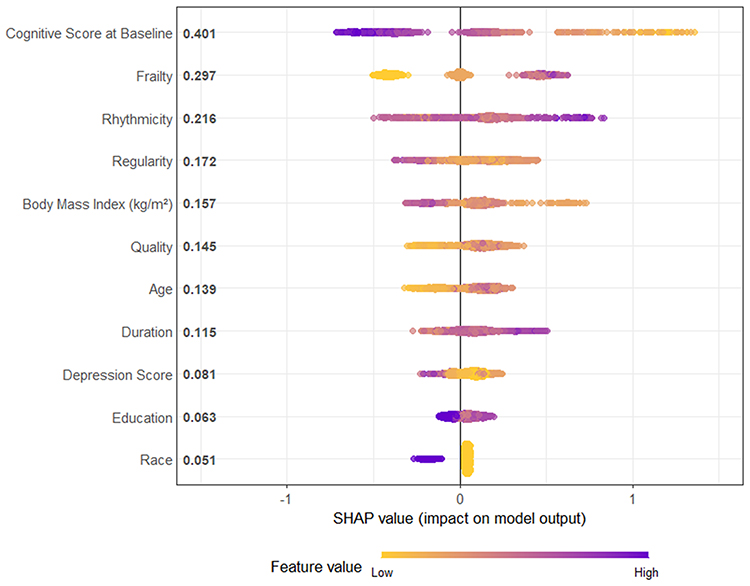 |
Figure 2 Shapley bee swarm plot for sleep domains and risk factors of cognitive impairment. Features are ranked on the y-axis according to their global importance, defined by the mean absolute SHAP value in descending order. Each point represents an individual observation. SHAP values indicate the contribution of each feature to the predicted risk of cognitive impairment, with positive values (to the right of the vertical line) indicating increased risk and negative values (to the left) indicating decreased risk. Color gradients from yellow to purple represent increasing raw values of each feature. For frailty, higher values indicate a greater number of frailty components. For education level, higher values indicate higher educational attainment. For race, purple represents White ethnicity and yellow represents other ethnic groups. |
Subgroup Analysis
To evaluate the robustness of associations between sleep domains and cognitive impairment, we conducted stratified Cox regression analyses across key demographic and lifestyle subgroups, including age, BMI, education level, smoking status, and alcohol consumption with fully adjusted models (Figure 3 and Supplementary Table 5).
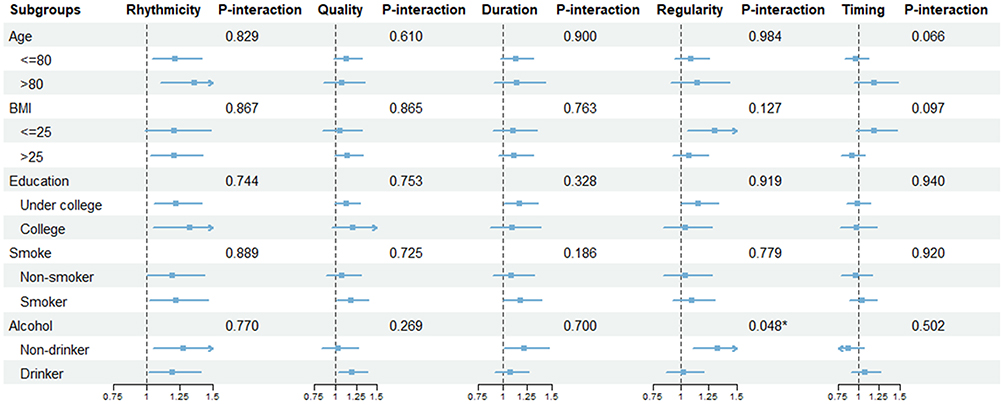 |
Figure 3 Subgroup analyses of associations between sleep domains and risk of cognitive impairment. Forest plots show hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations of five sleep domains (rhythmicity, quality, duration, regularity, and timing) with cognitive impairment across subgroups stratified by age, body mass index, education level, smoking status, and alcohol consumption. Smoker was defined as individuals who were past or current smokers, and non-drinker was defined as those reporting no alcohol consumption in the past 12 months. Estimates were obtained from fully adjusted Cox proportional hazards models (Model 3). |
Disrupted rhythmicity showed the most consistent association with increased risk of cognitive impairment across subgroup analyses, including participants aged ≤80 years (p = 0.034), >80 years (p <0.001), BMI >25 (p = 0.025), under-college education (p = 0.009), college education (p = 0.021), smokers (p = 0.030), non-drinkers (p = 0.016) and drinkers (p = 0.034). Although the association was not statistically significant in participants with BMI ≤25 or in non-smokers, the effect estimates remained in the same direction.
In contrast, the associations for other sleep domains were less consistent across subgroups. Quality was significantly associated with increased risk of cognitive impairment in smokers (p = 0.035), and drinkers (p = 0.018). Duration showed significant associations in the under-college subgroup (p = 0.031), non-drinker (p = 0.040) and smokers (p = 0.042). Regularity was positively associated with cognitive impairment risk in non-drinkers (p = 0.003) and those with BMI ≤25 (p = 0.014). A significant interaction between regularity and alcohol use was observed (p for interaction = 0.048). Timing did not show significant associations in any subgroup.
Sensitivity Analysis
After excluding participants who developed cognitive impairment within the first two years of follow-up, the overall pattern of results was similar to the primary analyses (Figure 4 and Supplementary Table 6). Rhythmicity and regularity remained associated with a higher risk of cognitive impairment across all models (Model 3: rhythmicity, HR = 1.21, 95% CI: 1.05–1.39, p = 0.008; regularity, HR = 1.18, 95% CI: 1.04–1.33, p = 0.013). Quality was not significantly associated with risk in Model 1 or Model 2, but became associated with a higher risk after further consideration for other sleep conditions (Model 3: HR = 1.16, 95% CI: 1.01–1.32, p = 0.036). Duration and timing were not associated with risk in all models after excluding early events.
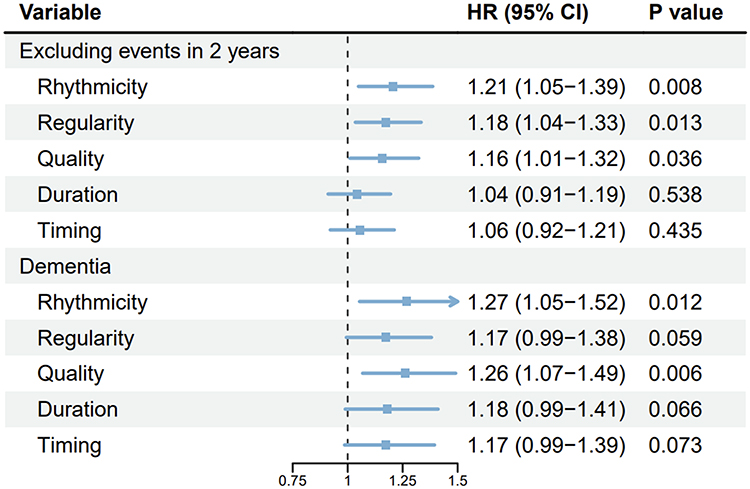 |
Figure 4 Sensitivity analyses of sleep domains and cognitive outcomes: cognitive impairment excluding early events and dementia diagnoses. Forest plots show hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations between sleep domains and cognitive outcomes. Analyses were conducted under two conditions: (1) excluding cognitive impairment events occurring within the first 2 years of follow-up, and (2) restricting the outcome to clinically diagnosed dementia. All estimates are derived from fully adjusted models (Model 3). |
When restricting the outcome to clinically diagnosed dementia (self-reported physician diagnosis), poorer rhythmicity and lower sleep quality were associated with increased dementia risk across all models. Although sleep duration and regularity did not reach statistical significance in the fully adjusted model, their effect estimates remained in the same direction (Figure 4 and Supplementary Table 6).
In sensitivity analyses using oblique rotations (oblimin and promax), the identified factor structure and subsequent associations were largely consistent with the primary analysis (Supplementary Tables 7 and 8). Rhythmicity remained significantly associated with cognitive impairment across all rotation methods in all models. Quality, duration, and regularity showed associations in each rotation method, although these were not consistent across models. No significant associations were observed for timing (Supplementary Tables 9 and 10). In the interval-censored models, the overall pattern of associations between sleep domains and cognitive impairment was broadly similar to the primary analysis. However, only rhythmicity demonstrated a statistically significant association with cognitive impairment in all models (Supplementary Table 11).
Discussion
Although prior studies primarily examined the relationships between individual sleep metrics and cognitive impairment, our study aimed to move beyond single sleep metric and evaluate associations of different sleep domains with cognitive outcomes in older men. Consistent with recent multidimensional sleep health frameworks,11,12 we constructed a five-domain structure encompassing rhythmicity, quality, duration, regularity, and timing. Our findings indicated that disrupted rhythmicity and poorer regularity were significantly associated with cognitive impairment. Longer duration and lower quality were associated with increased risk in certain conditions, whereas no association was observed for timing. Moreover, by systematically evaluating sleep domains and comparing their contributions with traditional risk factors, we provided an integrated perspective on the role of sleep in cognitive aging. Sleep domains remained among the strongest predictors even alongside established risk factors. Within sleep domains, rhythmicity emerged as most prominent predictor in the model. Taken together, these findings underscore the critical importance of multidimensional sleep health in cognitive decline, with sleep rhythmicity playing a particularly prominent role.
Rhythmicity is primarily characterized by sleep-related rest-activity rhythm patterns and captures the degree of rhythm fragmentation, day-to-day stability, and misalignment of circadian phase, reflecting disruption of the overall 24-hour sleep-wake cycle. Rhythmicity consistently emerged as the most consequential sleep domain, both in regression models and in importance rankings based on machine learning. Furthermore, in subgroup analyses, rhythmicity continued to show a protective association, suggesting that stable sleep-related rhythmicity may play a robust and generalizable role in preserving cognitive health across diverse population groups.
Disruption in rhythmicity reflects not only behavioral irregularities but also dysfunction of the endogenous central clock system, which becomes increasingly vulnerable with aging.33 Evidence from epidemiological studies shows that more disturbed rhythms are associated with faster cognitive decline, greater risk of Alzheimer’s disease, and accelerated cortical atrophy.34,35 In patients with established dementia, impaired rhythms further predict more rapid cognitive deterioration and disease progression.36,37 From a biological perspective, rhythmicity plays a central regulatory role in sleep architecture, metabolic homeostasis, and synaptic plasticity.38–40 Its disruption also impairs the glymphatic clearance pathway during sleep, thereby increasing β-amyloid burden and cerebrospinal fluid tau levels.41,42 Beyond neural mechanisms, disrupted rhythmicity is also linked to broader systemic disturbances, such as frailty, depressive symptoms, stroke, and chronic inflammation,43–46 each of which is independently associated with accelerated cognitive aging. Sleep rhythmicity appears to capture a multidimensional signal of physiological aging and neural vulnerability,47 and may represent a core mechanism underlying susceptibility to cognitive decline in later life.
Beyond rhythmicity, our study also validated associations between other sleep domains and cognitive impairment, further supporting the validity of our comprehensive framework. We found that poorer sleep quality, characterized by higher sleep fragmentation and lower sleep efficiency, was associated with an increased risk of cognitive impairment. This finding aligns with extensive previous research,48,49 as fragmented and inefficient sleep disrupts sleep microstructure and continuity, thereby compromising its core functions in memory consolidation and synaptic homeostasis.50,51 Sleep quality was not significantly associated with cognitive impairment in Models 1 and 2, but became significant only after further adjustment for other sleep-related factors (Model 3). Although the sleep domains were derived to be as independent as possible, this pattern suggests that sleep quality may not operate in isolation. Instead, its association with cognitive impairment may depend on the broader sleep context. Regarding duration, we observed that longer duration was associated with a higher risk of cognitive impairment. This finding may be related to the older average age of our study population and their generally shorter average sleep duration. In older adults, prolonged sleep duration often reflects compensatory responses to fragmented or poor-quality sleep, or diminished wake-maintenance capacity, rather than an increased physiological need for sleep. Extended sleep is also linked to broader physiological vulnerability and may further increase risk for cognitive decline in late life.52 When excluding early events, duration was no longer associated with cognitive impairment, suggesting that the observed association may be partly explained by reverse causation. Previous research also reported that longer sleep duration is connected to early or subclinical neurodegenerative changes in healthy adults.53 The association between long sleep duration and poorer cognitive function may reflect underlying pathological processes rather than a causal risk factor. Regularity was associated with cognitive impairment in both the primary analysis and the analysis excluding early events. Previous evidence has linked sleep irregularity to smaller gray matter and hippocampal volumes, which may provide a potential pathway connecting irregular sleep patterns with cognitive impairment.54 We also observed a significant interaction between sleep regularity and alcohol use, with the association between regularity and cognitive impairment evident only among non-drinkers. This finding suggests that the relevance of sleep regularity may differ across lifestyle subgroups and warrants further investigation. In contrast, timing was not associated with cognitive impairment in our study. This is consistent with previous reports,55 and is further supported by subsequent variable selection procedures, which did not identify timing as a predictor. The relationship between timing and cognitive impairment may be influenced by factors such as educational attainment, underlying health conditions, sleep quality, and depressive symptoms.56–58
The foremost strength of this study lies in the identification of multidimensional sleep domains, derived from multiple objective measures, without relying on predefined classifications. This approach enabled us to characterize both shared and distinct contributions of individual sleep features. In addition, by ranking the relative importance of sleep domains and risk factors associated with cognitive impairment, we provide an integrated perspective on sleep health and demonstrate that rhythmicity consistently emerged as one of the most influential determinants of cognitive impairment.
Several limitations should be acknowledged. First, the study population was restricted to older men, predominantly of White ethnicity, which may limit the generalizability of our findings. Second, our analyses focused exclusively on objective sleep measures, without incorporating additional subjective sleep domains that could yield further insights. Third, cognitive impairment was partly defined based on 3MS scores, which may be subject to educational level, measurement error and misclassification. Additionally, cognitive outcomes were assessed at different follow-up visits, and the exact time of cognitive impairment could not be precisely determined. Several covariates violated the proportional hazards assumption. We incorporated time-dependent effects, allowing for more flexible modeling of associations over follow-up. Finally, although we adjusted for a wide range of clinical confounders and dementia-related risk factors, the constraints of the available database meant that some potential confounding variables could not be accounted for.
Conclusion
In summary, this study establishes a multidimensional framework of sleep health and highlights its relevance to cognitive impairment. By integrating objective sleep measures with advanced machine-learning approaches, we demonstrated that disrupted rhythmicity was the predominant sleep domain associated with elevated risk of cognitive impairment in older men. Taken together, the results suggest that sleep-related monitoring and corresponding interventions for rhythmicity may contribute to the prevention of cognitive impairment. Future research should extend this framework to more diverse populations and further explore the mechanistic pathways and interventions of rhythmicity in preventing cognitive impairment.
Statement on the Use of Generative AI
We did not use generative AI in this study.
Data Sharing Statement
The MrOS data are available through the standard data access procedures described on the MrOS website (https://mrosonline.ucsf.edu/).
Ethics Approval and Consent to Participate
The MrOS Study was approved by the institutional review board at each participating clinical site and the study coordinating center, and written informed consent was obtained from all participants. Detailed information is available on the official MrOS website (https://mrosonline.ucsf.edu/). The current study protocol was reviewed and approved by the Ethics Committee of Peking University Sixth Hospital, Beijing, China (2025 Ethics Review No. 23). The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Acknowledgments
We would like to thank Dr. Qianwen Wang for helpful discussions and support for this work.
Author Contributions
Chunlin Chen: Methodology, Writing – original draft, Visualization, Data curation, Formal analysis, Conceptualization, Software. Miaoyu Zhang: Writing – original draft, Methodology, Data curation, Software, Formal analysis. Zhilin Wang: Writing – original draft, Visualization. Shanshan Qu: Formal analysis, Validation, Writing – review & editing. Xinying Liu: Formal analysis, Validation, Writing – review & editing. Chi Zhang: Validation, Writing – review & editing. Jiahui Deng: Resources, Methodology, Writing – review & editing. Yanping Bao: Validation, Methodology, Writing – review & editing. Jie Shi: Validation, Resources, Writing – review & editing. Wenqiang Li: Validation, Supervision, Writing – review & editing. Lin Lu: Validation, Supervision, Funding acquisition, Writing – review & editing. Le Shi: Writing – review & editing, Funding acquisition, Project administration, Supervision, Methodology. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Brain Science and Brain-like Intelligence Technology — National Science and Technology Major Project (2025ZD0218200), the National Natural Science Foundation of China General Program (82271527), and the Beijing Nova Program (20230484320). The Osteoporotic Fractures in Men (MrOS) Study is supported by National Institutes of Health funding. The following institutes provide support: the National Institute on Aging (NIA), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS), the National Center for Advancing Translational Sciences (NCATS), and NIH Roadmap for Medical Research under the following grant numbers: U01 AG027810, U01 AG042124, U01 AG042139, U01 AG042140, U01 AG042143, U01 AG042145, U01 AG042168, U01 AR066160, R01 AG066671, and UL1 TR002369. The National Heart, Lung, and Blood Institute (NHLBI) provides funding for the MrOS Sleep ancillary study “Outcomes of Sleep Disorders in Older Men” under the following grant numbers: R01 HL071194, R01 HL070848, R01 HL070847, R01 HL070842, R01 HL070841, R01 HL070837, R01 HL070838, and R01 HL070839.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Aranda MP, Kremer IN, Hinton L, et al. Impact of dementia: health disparities, population trends, care interventions, and economic costs. J Am Geriatr Soc. 2021;69(7):1774–14. doi:10.1111/jgs.17345
2. Norton S, Matthews FE, Barnes DE, Yaffe K, Brayne C. Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data. Lancet Neurol. 2014;13(8):788–794. doi:10.1016/S1474-4422(14)70136-X
3. Shi L, Chen SJ, Ma MY, et al. Sleep disturbances increase the risk of dementia: a systematic review and meta-analysis. Sleep Med Rev. 2018;40:4–16. doi:10.1016/j.smrv.2017.06.010
4. You Y, Li J, Zhang Y, Li X, Li X, Ma X. Exploring the potential relationship between short sleep risks and cognitive function from the perspective of inflammatory biomarkers and cellular pathways: insights from population-based and mice studies. CNS Neurosci Ther. 2024;30(5):e14783. doi:10.1111/cns.14783
5. Bokenberger K, Strom P, Dahl Aslan AK, et al. Association between sleep characteristics and incident dementia accounting for baseline cognitive status: a prospective population-based study. J Gerontol a Biol Sci Med Sci. 2017;72(1):134–139. doi:10.1093/gerona/glw127
6. Xu W, Tan -C-C, Zou -J-J, Cao X-P, Tan L. Sleep problems and risk of all-cause cognitive decline or dementia: an updated systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2020;91(3):236–244. doi:10.1136/jnnp-2019-321896
7. Blackwell T, Yaffe K, Ancoli-Israel S, et al. Association of sleep characteristics and cognition in older community-dwelling men: the MrOS sleep study. Sleep. 2011;34(10):1347–1356. doi:10.5665/SLEEP.1276
8. Ma XQ, Jiang CQ, Xu L, et al. Sleep quality and cognitive impairment in older Chinese: guangzhou biobank cohort study. Age Ageing. 2019;49(1):119–124. doi:10.1093/ageing/afz120
9. You Y, Liu J, Li X, Wang P, Liu R, Ma X. Relationship between accelerometer-measured sleep duration and Stroop performance: a functional near-infrared spectroscopy study among young adults. PeerJ. 2024;12:e17057. doi:10.7717/peerj.17057
10. Lee S, Lawson KM. Beyond single sleep measures: a composite measure of sleep health and its associations with psychological and physical well-being in adulthood. Soc Sci Med. 2021;274:113800. doi:10.1016/j.socscimed.2021.113800
11. Wallace ML, Lee S, Stone KL, et al. Actigraphy-derived sleep health profiles and mortality in older men and women. Sleep. 2022;45(4). doi:10.1093/sleep/zsac015
12. Zhang S, Zhang M, Yuan Y, Li Z, Li X, Li X. Health risks and genetic architecture of objectively measured multidimensional sleep health. Nat Commun. 2025;16(1):7026. doi:10.1038/s41467-025-62338-0
13. Orwoll E, Blank JB, Barrett-Connor E, et al. Design and baseline characteristics of the osteoporotic fractures in men (MrOS) study--a large observational study of the determinants of fracture in older men. Contemp Clin Trials. 2005;26(5):569–585. doi:10.1016/j.cct.2005.05.006
14. Jean-Louis G, Kripke DF, Mason WJ, Elliott JA, Youngstedt SD. Sleep estimation from wrist movement quantified by different actigraphic modalities. J Neurosci Methods. 2001;105(2):185–191. doi:10.1016/s0165-0270(00)00364-2
15. Wallace ML, Yu L, Buysse DJ, et al. Multidimensional sleep health domains in older men and women: an actigraphy factor analysis. Sleep. 2021;44(2). doi:10.1093/sleep/zsaa181
16. Zhang L, Viola Lee KA, Stone K, et al. Metabolomic biomarkers of rest-activity rhythms in older men: results from the osteoporotic fractures in men study (MrOS) study. Sleep. 2025. doi:10.1093/sleep/zsaf319
17. Luik AI, Zuurbier LA, Hofman A, Van Someren EJ, Tiemeier H. Stability and fragmentation of the activity rhythm across the sleep-wake cycle: the importance of age, lifestyle, and mental health. Chronobiol Int. 2013;30(10):1223–1230. doi:10.3109/07420528.2013.813528
18. Makarem N, Zuraikat FM, Aggarwal B, Jelic S, St-Onge MP. Variability in sleep patterns: an emerging risk factor for hypertension. Curr Hypertens Rep. 2020;22(2):19. doi:10.1007/s11906-020-1025-9
19. Ganesan S, Magee M, Stone JE, et al. The impact of shift work on sleep, alertness and performance in healthcare workers. Sci Rep. 2019;9(1):4635. doi:10.1038/s41598-019-40914-x
20. Wallace ML, Stone K, Smagula SF, et al. Which sleep health characteristics predict all-cause mortality in older men? an application of flexible multivariable approaches. Sleep. 2018;41(1). doi:10.1093/sleep/zsx189
21. Teng EL, Chui HC. The modified mini-mental state (3MS) examination. J Clin Psychiatry. 1987;48(8):314–318.
22. McDowell I, Kristjansson B, Hill GB, Hebert R. Community screening for dementia: the mini mental state exam (MMSE) and modified mini-mental state exam (3MS) compared. J Clin Epidemiol. 1997;50(4):377–383. doi:10.1016/s0895-4356(97)00060-7
23. Adabag S, Vo TN, Langsetmo L, et al. Frailty as a risk factor for cardiovascular versus noncardiovascular mortality in older men: results from the MrOS Sleep (outcomes of sleep disorders in older men) study. J Am Heart Assoc. 2018;7(10). doi:10.1161/jaha.118.008974
24. Watkins MW. Exploratory factor analysis: a guide to best practice. J Black Psychol. 2018;44(3):219–246. doi:10.1177/0095798418771807
25. psych: procedures for psychological, psychometric, and personality research. Northwestern University; 2025. Available from: https://CRAN.R-project.org/package=psych.
26. Xu H, Chen C, Lu Z, Nie Z. rcssci: an R package for visualization of restricted cubic spline. Med Res. 2025;1(2):201–206. doi:10.1002/mdr2.70015
27. Zhang Z, Reinikainen J, Adeleke KA, Pieterse ME, Groothuis-Oudshoorn CGM. Time-varying covariates and coefficients in Cox regression models. Ann Transl Med. 2018;6(7):121. doi:10.21037/atm.2018.02.12
28. Chen T, Guestrin C. XGBoost: a scalable tree boosting system.
29. rBayesianOptimization: bayesian optimization of hyperparameters. 2024. Available from: https://github.com/yanyachen/rbayesianoptimization.
30. SHAPforxgboost: SHAP plots for ‘XGBoost. 2023. Available from: https://CRAN.R-project.org/package=SHAPforxgboost.
31. Friedman JH, Hastie T, Tibshirani R. Regularization paths for generalized linear models via coordinate descent. J Statistical Softw. 2010;33(1):1–22. doi:10.18637/jss.v033.i01
32. Anderson-Bergman C. icenReg: regression models for interval censored data in R. J Statistical Softw. 2017;81(12):1–23. doi:10.18637/jss.v081.i12
33. Kim JH, Elkhadem AR, Duffy JF. Circadian rhythm sleep-wake disorders in older adults. Sleep Med Clin. 2022;17(2):241–252. doi:10.1016/j.jsmc.2022.02.003
34. Espinosa N, Hoyos CM, McKinnon AC, Almgren H, Duffy SL, Naismith SL. Rest-activity rhythm fragmentation and synchronization are linked with reduced cortical thickness in older adults “at risk” for dementia. Sleep. 2025;48(5). doi:10.1093/sleep/zsaf017
35. Haghayegh S, Gao C, Sugg E, et al. Association of rest-activity rhythm and risk of developing dementia or mild cognitive impairment in the middle-aged and older population: prospective cohort study. JMIR Public Health Surveill. 2024;10:e55211. doi:10.2196/55211
36. Li P, Gao L, Gaba A, et al. Circadian disturbances in Alzheimer’s disease progression: a prospective observational cohort study of community-based older adults. Lancet Healthy Longev. 2020;1(3):e96–e105. doi:10.1016/s2666-7568(20)30015-5
37. Targa ADS, Benitez ID, Dakterzada F, et al. The circadian rest-activity pattern predicts cognitive decline among mild-moderate Alzheimer’s disease patients. Alzheimers Res Ther. 2021;13(1):161. doi:10.1186/s13195-021-00903-7
38. Franken P, Dijk DJ. Sleep and circadian rhythmicity as entangled processes serving homeostasis. Nat Rev Neurosci. 2024;25(1):43–59. doi:10.1038/s41583-023-00764-z
39. Frank MG. Circadian regulation of synaptic plasticity. Biology. 2016;5(3). doi:10.3390/biology5030031
40. Sato T, Sato S. Circadian regulation of metabolism: commitment to health and diseases. Endocrinology. 2023;164(7). doi:10.1210/endocr/bqad086
41. Nguyen Ho PT, Hoepel SJW, Rodriguez-Ayllon M, Luik AI, Vernooij MW, Neitzel J. Sleep, 24-hour activity rhythms, and subsequent amyloid-β pathology. Article. JAMA Neurol. 2024;81(8):824–834. doi:10.1001/jamaneurol.2024.1755
42. Eckhardt JL, Isenberg L, Aslanyan V, et al. Circadian rhythms are associated with higher amyloid-beta and tau and poorer cognition in older adults. Brain Commun. 2025;7(5):fcaf322. doi:10.1093/braincomms/fcaf322
43. Cai R, Gao L, Gao C, et al. Circadian disturbances and frailty risk in older adults. Nat Commun. 2023;14(1):7219. doi:10.1038/s41467-023-42727-z
44. Gao L, Zheng X, Baker SN, et al. Associations of rest-activity rhythm disturbances with stroke risk and poststroke adverse outcomes. J Am Heart Assoc. 2024;13(18):e032086. doi:10.1161/JAHA.123.032086
45. Liao Y, Zhang W, Chen S, et al. Associations between rest-activity/light-exposure rhythm characteristics and depression in United States adults: a population-based study. J Affect Disord. 2025;369:1004–1012. doi:10.1016/j.jad.2024.10.073
46. Wright KP, Drake AL, Frey DJ, et al. Influence of sleep deprivation and circadian misalignment on cortisol, inflammatory markers, and cytokine balance. Brain Behav Immun. 2015;47:24–34. doi:10.1016/j.bbi.2015.01.004
47. Nagayach A, Bhaskar R, Ghosh S, et al. Interplay between circadian rhythm, ageing and neurodegenerative disorder. Open Biol. 2025;15(7):240161. doi:10.1098/rsob.240161
48. Qin S, Leong RLF, Ong JL, Chee MWL. Associations between objectively measured sleep parameters and cognition in healthy older adults: a meta-analysis. Sleep Med Rev. 2023;67:101734. doi:10.1016/j.smrv.2022.101734
49. Carpi M, Fernandes M, Mercuri NB, Liguori C. Sleep biomarkers for predicting cognitive decline and Alzheimer’s disease: a systematic review of longitudinal studies. J Alzheimers Dis. 2024;97(1):121–143. doi:10.3233/JAD-230933
50. Tononi G, Cirelli C. Sleep function and synaptic homeostasis. Sleep Med Rev. 2006;10(1):49–62. doi:10.1016/j.smrv.2005.05.002
51. Hokett E, Arunmozhi A, Campbell J, Verhaeghen P, Duarte A. A systematic review and meta-analysis of individual differences in naturalistic sleep quality and episodic memory performance in young and older adults. Neurosci Biobehav Rev. 2021;127:675–688. doi:10.1016/j.neubiorev.2021.05.010
52. Jike M, Itani O, Watanabe N, Buysse DJ, Kaneita Y. Long sleep duration and health outcomes: a systematic review, meta-analysis and meta-regression. Sleep Med Rev. 2018;39:25–36. doi:10.1016/j.smrv.2017.06.011
53. Namsrai T, Northey JM, Ambikairajah A, et al. Sleep characteristics and brain structure: a systematic review with meta-analysis. Sleep Med. 2025;129:316–329. doi:10.1016/j.sleep.2025.02.028
54. Yiallourou SR, Cribb L, Cavuoto MG, et al. Association of the sleep regularity index with incident dementia and brain volume. Neurology. 2024;102(2):e208029. doi:10.1212/WNL.0000000000208029
55. Wang Q, Xu S, Liu F, et al. Causal relationship between sleep traits and cognitive impairment: a Mendelian randomization study. J Evid Based Med. 2023;16(4):485–494. doi:10.1111/jebm.12576
56. Wenzler AN, Liefbroer AC, Voshaar RCO, Smidt N. Chronotype as a potential risk factor for cognitive decline: the mediating role of sleep quality and health behaviours in a 10-year follow-up study. J Prev Alzheimers Dis. 2025;12(6):100168. doi:10.1016/j.tjpad.2025.100168
57. Sauers SC, Toedebusch CD, Richardson R, et al. Midpoint of sleep is associated with sleep quality in older adults with and without symptomatic Alzheimer’s disease. Sleep Adv. 2024;5(1):zpae023. doi:10.1093/sleepadvances/zpae023
58. Zou H, Zhou H, Yan R, Yao Z, Lu Q. Chronotype, circadian rhythm, and psychiatric disorders: recent evidence and potential mechanisms. Front Neurosci. 2022;16:811771. doi:10.3389/fnins.2022.811771
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
How Does Chronobiology Contribute to the Development of Diseases in Later Life
Stowe TA, McClung CA
Clinical Interventions in Aging 2023, 18:655-666
Published Date: 20 April 2023
Quantification of Differences in Sleep Measurement by a Wrist-Worn Consumer Wearable Compared to Research-Grade Accelerometry and Sleep Diaries of Female Adults in Free-Living Conditions
Hu CR, Delaney C, Chavarro JE, Laden F, Librett R, Katuska L, Kaplan ER, Yi L, Rueschman M, Kossowsky J, Onnela JP, Coull BA, Redline S, James P, Hart JE
Nature and Science of Sleep 2025, 17:1973-1983
Published Date: 27 August 2025
Recent Trends in Cannabis Use in Adults Ages 60 Years and Older
Thayer RE, Anquillare E, Coromac-Medrano J, Hardin EE, Hatcher K, Hermann GE
Substance Abuse and Rehabilitation 2026, 17:560360
Published Date: 13 February 2026