Back to Journals » Nature and Science of Sleep » Volume 18

Sleep and Substance Use Among Firefighters: Associations with Alcohol, Caffeine, and Nicotine Use
Authors Reichenberger DA, Lee LJ ![]() , Hebl J
, Hebl J ![]() , Ayeni AO
, Ayeni AO ![]() , Robinson II LD, Watkins SL
, Robinson II LD, Watkins SL ![]() , Haswarey AH, Hurtado DA
, Haswarey AH, Hurtado DA ![]() , McHill AW
, McHill AW ![]() , Bodner T
, Bodner T ![]() , Shea SA
, Shea SA ![]() , Bowles NP
, Bowles NP ![]()
Received 25 February 2026
Accepted for publication 23 May 2026
Published 10 July 2026 Volume 2026:18 605149
DOI https://doi.org/10.2147/NSS.S605149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
David A Reichenberger,1,2 Lauren J Lee,1 Joey Hebl,1 Aanuoluwakiitan O Ayeni,1 LaTroy D Robinson II,1 Shelby L Watkins,1 Ayeisha H Haswarey,1 David A Hurtado,1,3 Andrew W McHill,1,4 Todd Bodner,5 Steven A Shea,1 Nicole P Bowles1
1Oregon Institute of Occupational Health Sciences, Oregon Health & Science University, Portland, OR, USA; 2Knight Cardiovascular Institute, Oregon Health & Science University, Portland, OR, USA; 3OHSU-PSU School of Public Health, Portland, OR, USA; 4School of Nursing, Oregon Health & Science University, Portland, OR, USA; 5Department of Psychology, Portland State University, Portland, OR, USA
Correspondence: David A Reichenberger, Oregon Institute of Occupational Health Sciences, Oregon Health & Science University, 3222 SW Research Drive, Portland, OR, 97239, USA, Email [email protected]
Purpose: Firefighters are at high risk for sleep disruption due to shift work. Use of alcohol, caffeine, and nicotine can also affect sleep. Thus, we evaluated daily, bidirectional associations between substance use and actigraphy-assessed sleep among firefighters.
Patients and methods: Micro-longitudinal data were drawn from 120 firefighters participating in the Shiftwork in Firefighters (SWIFT) Study. Participants completed surveys on daily alcohol and caffeine use, current and lifetime tobacco use, and wore actigraphy devices to assess sleep timing, duration, and quality (2,617 observations). Multilevel models were used to examine both between- and within-person associations between substance use and subsequent sleep, and between sleep and next-day substance use. Models were adjusted for covariates (shift schedule, on-shift status, nighttime call volume, and naps).
Results: Alcohol use demonstrated strong bidirectional associations with sleep. Greater within-person alcohol consumption predicted shorter sleep and earlier waketimes, while later sleep timing and shorter sleep predicted greater next-day alcohol use. Unexpectedly, greater caffeine consumption was associated with higher sleep efficiency and fewer nighttime awakenings at the between-person level and longer total sleep time at the within-person level. Current between-person use of smokeless tobacco was associated with approximately 30 minutes shorter total sleep time, whereas lifetime cigarette use showed no association with sleep outcomes.
Conclusion: Substance use among firefighters exhibited substance-specific and temporally dynamic relationships with sleep. Nicotine and caffeine effects were largely person-dependent, whereas daily alcohol showed consistent bidirectional effects on sleep. These findings highlight potential intervention targets aimed at improving sleep and reducing alcohol-related risk among firefighters.
Keywords: shift workers, actigraphy, multilevel, chewing tobacco, nicotine, caffeine, alcohol
Introduction
Across emergency response occupations, sleep disturbances are common due to irregular schedules and high operational demands, posing important risks to both worker health and public safety.1,2 Firefighters represent a distinct subgroup of shift workers characterized by unpredictable overnight call demands and extended duty periods often lasting 24 hours or more, albeit with the opportunity to obtain sleep in operational environments.3,4 Emergency response services frequently delay time in bed, interrupt sleep throughout the night, and precipitate early morning awakenings, all of which constrain sleep opportunity, shorten sleep duration, and degrade overall sleep quality.4–9 Moreover, firefighters are routinely exposed to intense psychosocial stressors, including traumatic events, unpredictable emergencies, and sustained demands for vigilance and rapid physical exertion.10–13 These exposures are closely intertwined with sleep, with evidence suggesting bidirectional relationships in which stress disrupts sleep and insufficient or fragmented sleep exacerbates emotional and physiological stress reactivity.14 Together, this dynamic interplay contributes to elevated risk for adverse mental health outcomes and highlights sleep as a central mechanism linking occupational stress to downstream health behaviors.15
In this context, substance use may emerge as a behavioral strategy to manage sleep disruption and operational demands. Firefighters frequently rely on substances such as caffeine, nicotine, and alcohol to combat fatigue, sustain performance, or facilitate psychological detachment from work.7,16,17 While stimulants may temporarily enhance alertness,7,18–20 they may interfere with subsequent sleep, whereas alcohol that is used to unwind or induce sleep may further degrade sleep quality.21,22 These coping behaviors highlight the potential for dynamic, bidirectional relationships between substance use and sleep among firefighters.
Alcohol use is widespread in the fire service, with estimates suggesting that 72–90% of firefighters report regular use23–25 and approximately half engage in binge drinking behaviors.7,21,24 Within the fire service, alcohol use is often embedded in social contexts for the expected purpose of fostering social cohesion and to facilitate unwinding after demanding shifts.7,21,23,24 Alcohol is also commonly used to promote sleep initiation.26 Although alcohol may initially shorten sleep onset latency through its sedative effects, these effects dissipate as alcohol is metabolized, leading to rebound sympathetic activation, light sleep, and increased awakenings during the second half of the night.8,23,26 Together, these patterns highlight the clinical relevance of alcohol use for sleep health in firefighters and underscore its potential role in contributing to disrupted and non-restorative sleep,8,23 although findings have been inconsistent across studies.7
Caffeine is another commonly used substance among firefighters, primarily for its stimulant properties that can improve daytime performance, vigilance, and mood regulation.17,27,28 Although the Food and Drug Administration recommends healthy adults limit daily consumption of caffeine to 400 mg,29 average daily caffeine consumption among firefighters may exceed 500 mg,30 with approximately 5% overconsuming caffeine (>700 mg/day).7 Consequently, mistimed or excessive caffeine consumption may disrupt sleep.17,31–33 Among Korean firefighters, consuming any caffeine was associated with lower odds of insomnia symptomatology34 but worse overall sleep quality.35 Among U.S. firefighters, caffeine overconsumption was associated with worse physical and mental health but was not associated with sleep.7 These inconsistent findings highlight the need to better understand how caffeine use and sleep interact within the unique occupational context of firefighting.
Nicotine is a different stimulant used within the fire service,7,16 delivered through a range of tobacco products, particularly among male firefighters.36 Although overall tobacco use has declined in recent decades, primarily due to decreasing use of combustible tobacco products,37 current, estimates suggest that approximately 10–12% of firefighters smoke cigarettes,7,16 down from nearly 25% in the early 1990s.37 Conversely, use of noncombustible, smokeless tobacco products has increased37 to approximately 14%.16 Evidence suggest that entry into the fire service is associated with increased use of smokeless tobacco.38 Tobacco use also clusters with other health-risk behaviors, as firefighters who use tobacco products are more likely to engage in heavy or binge consumption of alcohol.16,36,39 Regarding sleep, the stimulating properties of nicotine can increase arousal and delay sleep onset, while overnight withdrawal may contribute to increased wake after sleep onset and early morning awakenings.40–42 However, findings in firefighters are limited with some studies reporting no association between current use of tobacco products on sleep patterns or quality.7,35
Overall, the majority of studies examining substance use and sleep among firefighters have relied on cross-sectional analyses of self-reported sleep. While prior studies have demonstrated that there may be a relationship between substance use and sleep among firefighters, these studies cannot report on the dynamics of any such relationship. For example, among this unique population, poor sleep may precede the total daily use of stimulants or alcohol, or vice versa. Alternatively, the relationship may be bidirectional, with poor sleep preceding substance use, which then undermines subsequent sleep. Thus, this study aims to determine any systematic bidirectional associations between substance use and sleep health among firefighters. It also leverages objectively assessed sleep health compared to relying on self-report. We hypothesized that firefighters who used nicotine products would have worse sleep on average. We also hypothesized that sleep would be worse after days of greater caffeine and alcohol use, which in turn would be associated with greater next-day caffeine and alcohol use. To that end, we leveraged multilevel modeling to investigate both the between- and within-person micro-longitudinal associations of substance use on subsequent sleep, and of sleep on subsequent substance use.
Methods
Participants
Data were collected from 120 participants in the Shiftwork in Firefighters (SWIFT) Study43 across one to three repeated 14-day sampling periods between 2020 and 2024 from four Pacific Northwest regional fire districts. Recruitment strategy and other study procedures have been previously reported.43 This study was conducted according to the guidelines established in the Declaration of Helsinki of 1975 (revised 1983). All participants provided written informed consent to the protocol, which was approved by the Oregon Health & Science University Institutional Review Boards (IRB# 20553).
Measures
Substance Use Variables
Daily alcohol use was assessed once every evening by asking participants to report their total number of standard drinks consumed that day. Examples of standard drinks were provided, including 12 fl oz of regular beer (5% alcohol), 5 fl oz of wine (12% alcohol), and 1.5 fl oz of distilled spirits (40% alcohol). Daily alcohol use was calculated as the summed number of standard drinks consumed that day.
Daily caffeine consumption was assessed using the Caffeine Consumption Questionnaire-Revised.44 Participants reported their total caffeine intake from various food and beverage sources, including coffee, tea, soda, energy drinks, and chocolate. Daily caffeine use was determined by summing all caffeine sources from that day.
Tobacco use was assessed once at the start of the study using items from the Behavioral Risk Factor Surveillance System. Participants reported whether they had smoked at least 100 cigarettes in their lifetime (“yes”, “no”, or “don’t know/not sure”). Those responding “yes” were asked about current cigarette smoking (“every day”, “some days”, or “not at all”). Participants also reported current use of smokeless tobacco products, including chewing tobacco, snuff, or snus (“every day”, “some days”, or “not at all”). Responses of “every day” and “some days” were combined to indicate current use.44
Self-Reported Sleep Variables
Participants completed daily morning sleep diaries45 via Email or automated text across one to three 14-day sampling periods, reporting bedtimes, waketimes, sleep onset latency, sleep duration, sleep quality, and naps. Diary data were used to verify actigraphic sleep periods, helping to distinguish periods of inactivity from the actual initiation of sleep including naps or nighttime awakenings related to emergency events.46
Actigraphic Sleep Variables
Participants continuously wore an Actigraph GT3X actiwatch (Actigraph LLC, Pensacola, FL) on their non-dominant wrist throughout each 14-day sampling period (both on-shift and off-shift), except when showering or bathing. Times in and out of bed for sleep periods were automatically estimated using the Cole-Kripke and Tudor-Locke algorithms with default settings and 60-second epochs in the ActiLife software (Actigraph LLC, Pensacola, FL). Sleep periods were excluded from analysis if there were no sleep diaries to verify the software-detected sleep periods. Whenever a sleep period was not reliably detected by the software (eg, due to excessive light, movement, or short duration; ≤1 night/recording), the sleep period was manually adjusted using information from the sleep diary. Approximately 2,617 of the 3,198 provided actigraphic sleep periods were verified using participant sleep diaries. Assessed sleep variables include timing of sleep onset and waketime (midnight-centered minutes, reported as clocktime), total 24-hour sleep time (minutes scored as asleep), sleep efficiency (percentage of time scored as asleep versus time between self-reported bedtime and waketime), number of awakenings during sleep, and wakefulness after sleep onset (WASO; minutes scored as awake during nighttime sleep). All actigraphic sleep variables were treated as continuous outcomes.
Covariates
Time-varying occupational factors were included as covariates, including work schedule, whether they were on-shift or off-shift, and nighttime call volume (from 11pm to 6am). Participants reported the shift schedule in effect during data collection, defined as either “24/48” (24 hours on followed by 48 hours off) or “1/3/2/3” (1-day on/3-days off/2-days on/3-days off). Finally, whether the participant napped at least once in a 24-hour period (“yes”, “no”) was included as an additional time-varying covariate.47
Statistical Analysis
Multilevel models were used to examine the between- and within-person associations of substance use on subsequent nighttime sleep and nighttime sleep on next-day substance use, adjusted for covariates (schedule, shift, nighttime call count, and naps), which were treated as fixed effects. Because tobacco use was assessed once, multilevel models were used to examine only the between-person associations of lifetime cigarette use and current chewing tobacco use on sleep. The between-person component consisted of person mean responses to examine interindividual variability, and the within-person component consisted of person-mean-centered responses to examine intraindividual variability. For example, between-person associations show how greater average substance use is associated with worse average sleep; within-person associations show how greater than average daily substance use is associated with nightly changes in sleep. Survey and actigraphy data were merged based on the date when participants awoke from sleep; person-mean-centered substance use predictors were therefore lagged by one day to examine their effect on subsequent sleep.
All analyses were conducted in R (version 4.4.0) using the packages nlme (version 3.1.166)48 for sleep and caffeine use outcomes and glmmTMB (version 1.1.10)49 for the zero-inflated alcohol use outcome due to 65% of days on which no consumption of alcohol was reported. Multilevel linear models were estimated using restricted maximum likelihood, whereas multilevel negative binomial models were estimated using maximum likelihood. The intercept and slope of the within-person predictor were treated as random variables nested within each participant. The random slope was removed from models whenever model convergence failed. Statistical significance was interpreted when p<0.05.
Results
Participant demographics are shown in Table 1. Firefighters in the analytical sample (N=120) were predominantly male, younger than 45 years old, White, non-Hispanic/Latino, and married. Firefighters provided an average±SD of 21.8±11.2 days of daily survey and sleep data (2,617 diary-verified observations), with a median of 21.5 days. Firefighters reported consuming on average 1.4±1.3 alcoholic beverages on off-shift days and 228.0±118.2 mg of caffeine daily. 18% of firefighters reported smoking at least 100 cigarettes in their lifetime, while only 8% currently used chewing tobacco and only 1 firefighter currently smoked cigarettes. Mean sleep onset of the sample was 22:59±00:42, waketime was 06:41±00:36, and sleep duration was 7.0±0.8 hours.
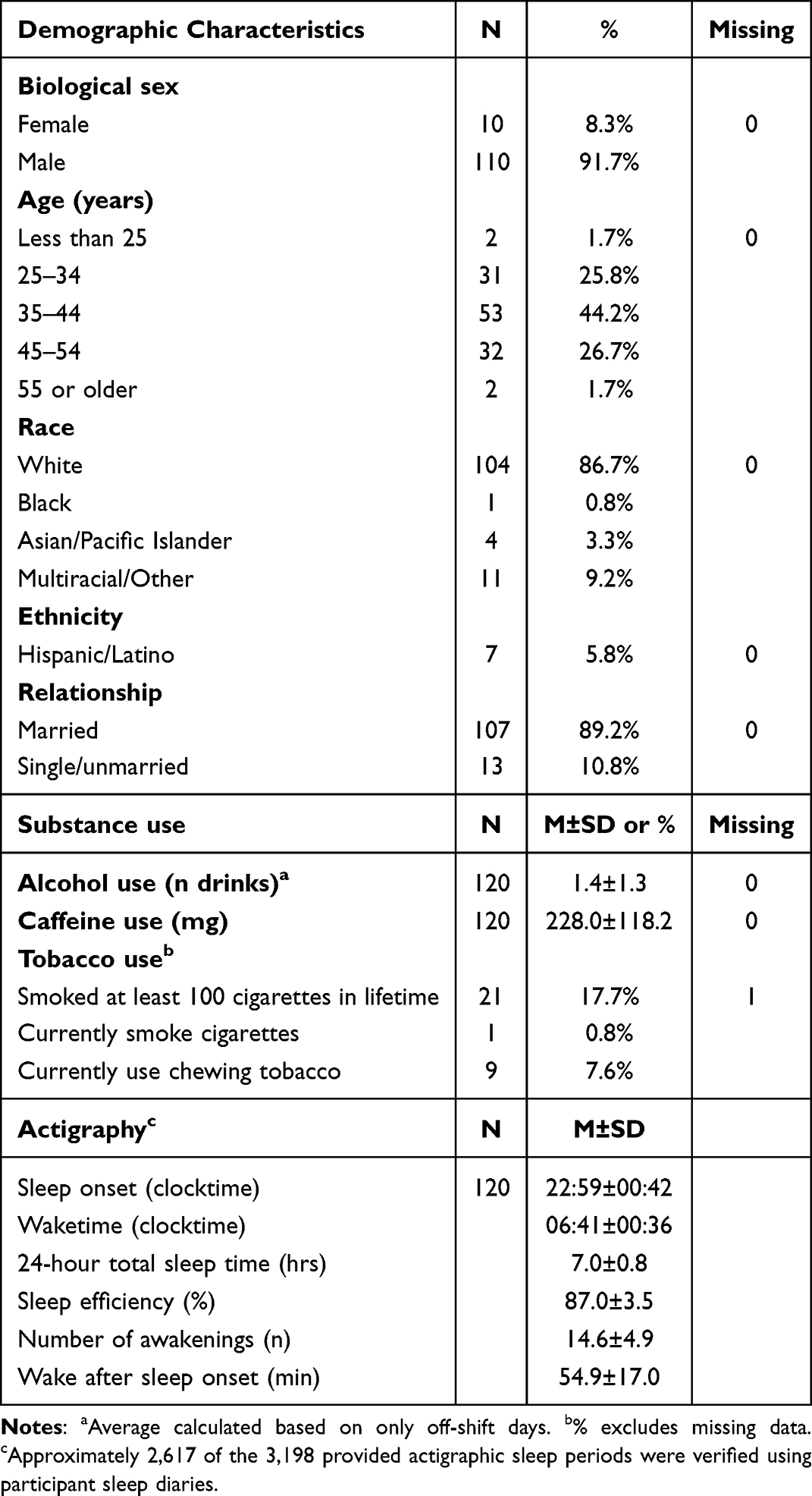 |
Table 1 Participant Demographics (N=120) |
Greater alcohol use was bidirectionally associated with worse sleep. Between-person findings in Table 2 showed that firefighters who consumed more drinks had on average 11±5 minutes later sleep onset (p=0.019). Within-person findings showed that waketime was 2±1 minutes earlier (p=0.009) and total sleep time was 3±1 minutes shorter (p=0.005) for each additional drink more than average consumed the prior day (see Figure 1). Conversely, within-person findings in Table 3 showed that poorer sleep also predicted greater next-day alcohol use, whereby firefighters consumed up to 33% more drinks the next day for each hour that sleep timing had been later than average (95% CI=1.05, 1.47), whereas each additional hour of sleep was associated with 8% fewer drinks the following day (95% CI=0.86, 0.98). There were no associations between alcohol use and actigraphic measures of sleep quality.
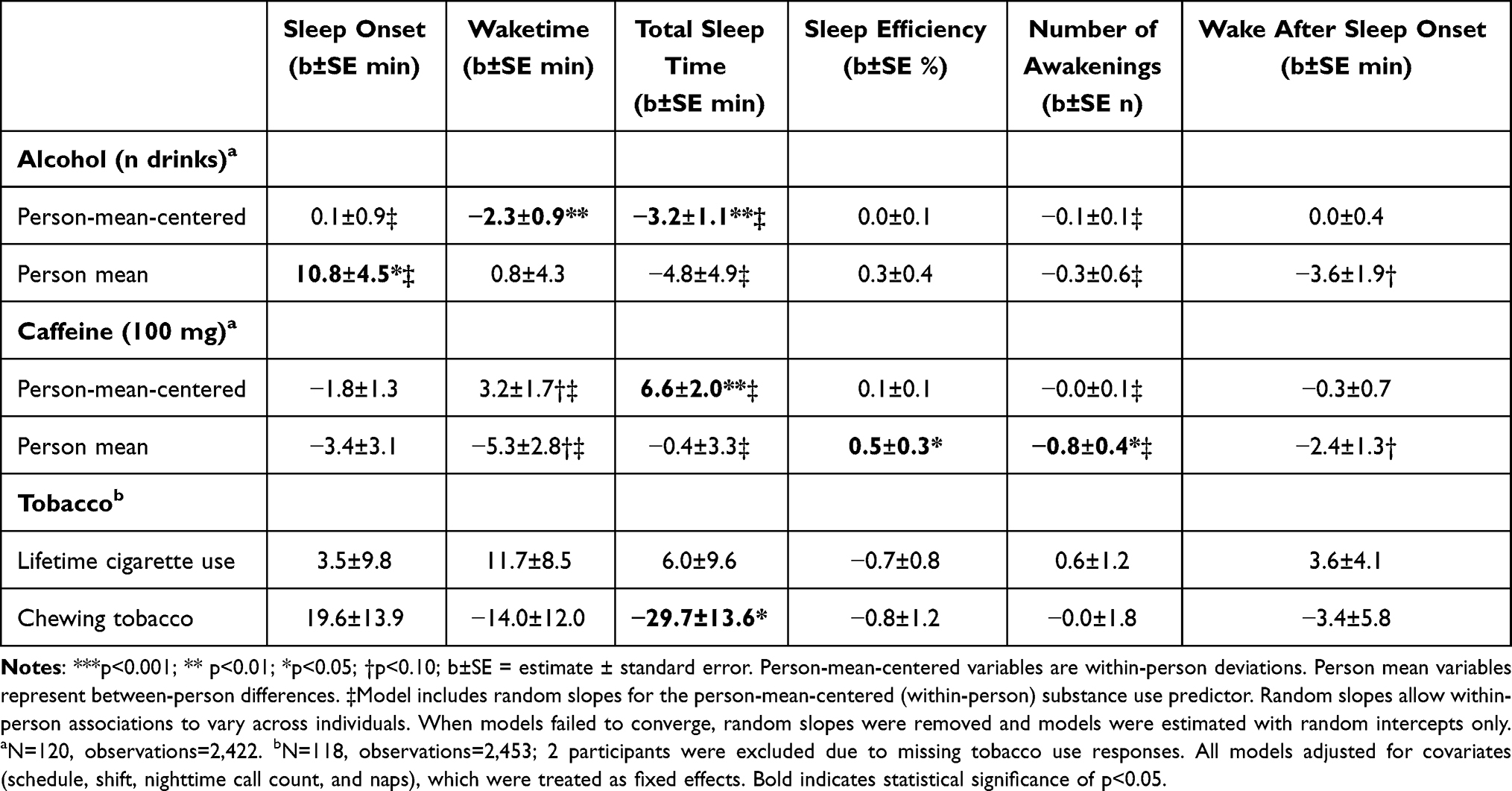 |
Table 2 Adjusted Multilevel Models of Associations Between Substance Use Predictors and Sleep Outcomes |
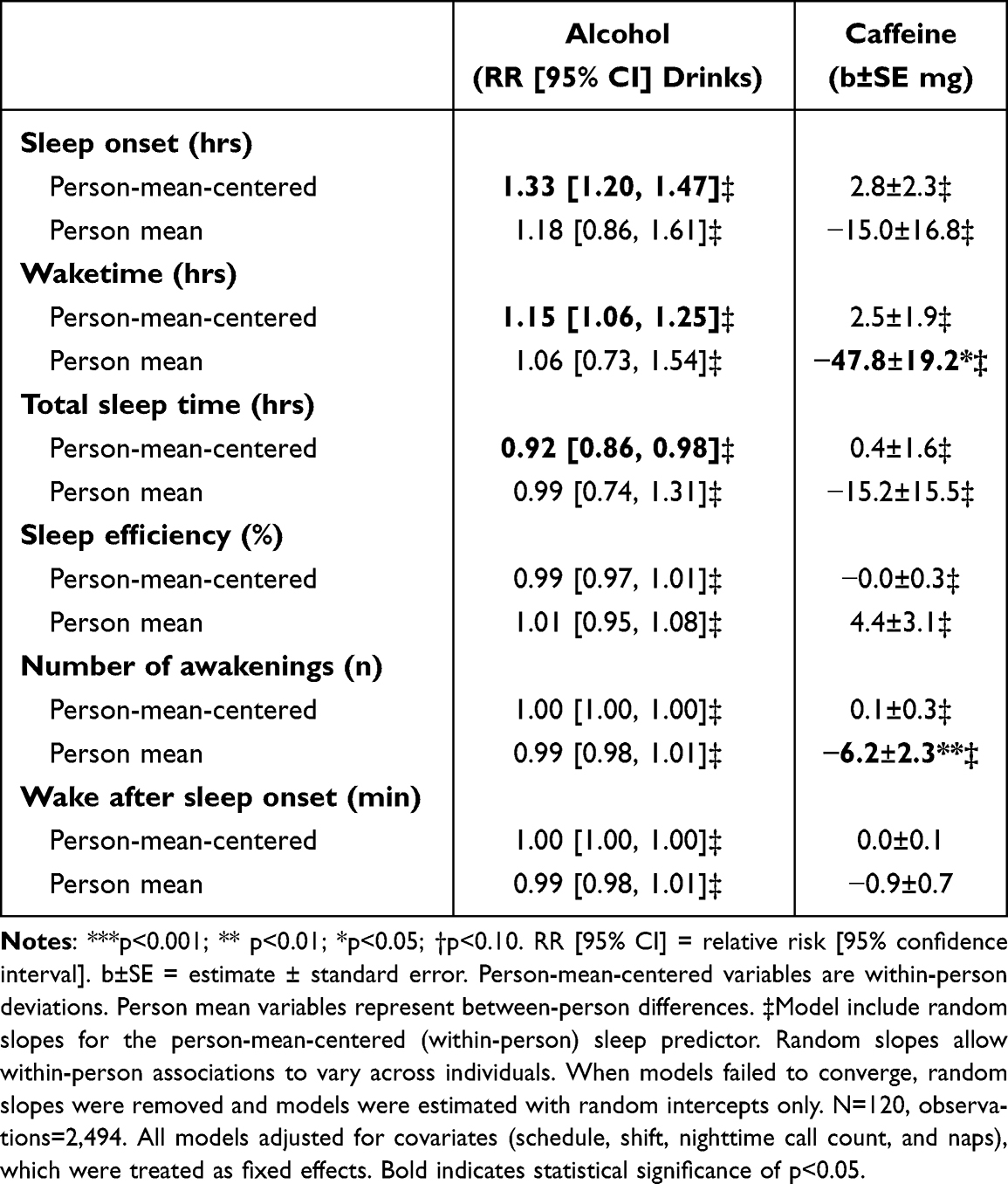 |
Table 3 Adjusted Multilevel Models of Associations Between Sleep Predictors and Substance Use Outcomes |
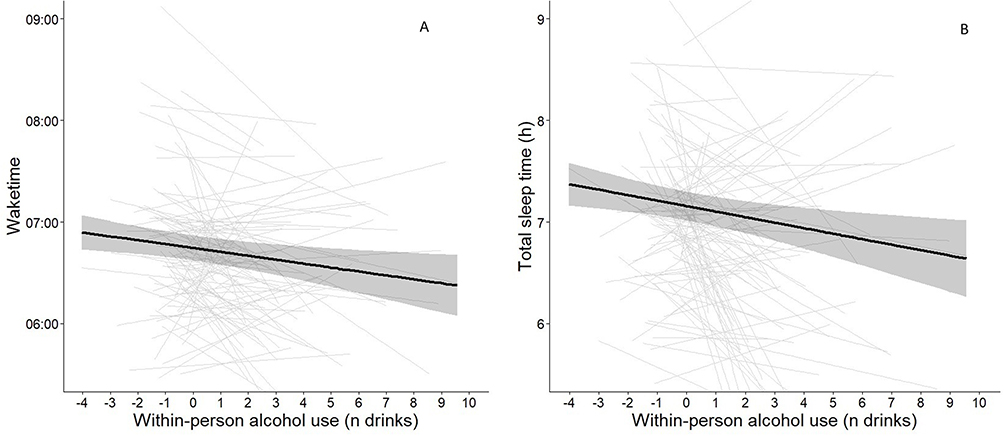 |
Figure 1 Within-person associations of alcohol use (n drinks) with A) waketime (clocktime) and B) total sleep time (h) from Table 2. On the X-axis, zero denotes the person mean number of drinks, and other values indicate daily deviation (person-mean-centered) from that person mean. All multilevel models adjusted for covariates (shift, schedule, nighttime call count, and naps). Shaded bands show 95% confidence interval of sleep outcome predicted across daily deviations of alcohol use; grey lines in the background depict individual firefighter slopes across repeated within-person observations. Note: N=120, observations=2,422. |
Associations between caffeine use and sleep were observed. Between-person findings in Table 2 showed that firefighters who consumed more daily caffeine had slightly higher sleep efficiency (p=0.031) and fewer awakenings at night (p=0.030). Between-person findings in Table 3 showed that firefighters who woke up later (p=0.014) or had more nighttime awakenings consumed fewer mg of caffeine (p=0.009). Within-person findings revealed that firefighters’ total sleep time was longer (p=0.001) for every additional 100 mg of caffeine (approximately one 8 fl oz cup of home brewed coffee) consumed the prior day (see Table 2).
There was no association between lifetime cigarette use and sleep (p≥0.172). Compared to firefighters who do not currently use chewing tobacco, between-person findings in Table 2 showed that firefighters who did use chewing tobacco had on average±SE 30±14 minutes shorter total sleep time (p=0.031), after adjusting for covariates. Current use of chewing tobacco was otherwise not associated with any sleep outcomes.
Discussion
This study aimed to examine daily bidirectional associations between substance use and actigraphically assessed sleep in this micro-longitudinal study of firefighters. Several key findings emerged. First, alcohol use demonstrated consistent bidirectional associations with sleep. Second, greater caffeine consumption was unexpectedly associated with slightly better sleep at the between-person level, and total sleep time was longer after days of greater caffeine use. Third, current use of smokeless tobacco was associated with shorter total sleep time, whereas lifetime cigarette use was not associated with sleep outcomes. Greater alcohol consumption predicted shorter subsequent sleep and earlier morning waketimes, while later sleep timing and shorter total sleep time predicted greater next-day alcohol use. Together, these findings underscore a complex and substance-specific relationship with sleep among firefighters.
Alcohol use showed the most consistent pattern with sleep. Firefighters who consumed more alcohol on average had later sleep onset, and days of greater alcohol consumption were associated with 2–3 minutes earlier waketimes and shorter sleep per each additional drink more than average. These results are consistent with extensive literature demonstrating that alcohol may have initial sedating effects but otherwise disrupts and limits sleep.41 Mechanistically, alcohol acutely enhances GABAergic inhibition, promoting sedation and facilitating sleep onset; however, as alcohol is metabolized, this effect wanes and is followed by increased arousal and awakenings, particularly in the second half of the night.50 Meta-analytic evidence further indicates does-dependent suppression of REM sleep with overall reductions in REM duration, despite possible rebound later in the sleep opportunity.26 As shown in Figure 1, days of heavier drinking may considerably curtail subsequent sleep51 and influence next-day vigilance and behaviors. Indeed, we also observed evidence of reverse directionality. Nights with later sleep timing and shorter sleep predicted greater next-day alcohol consumption, possibly due to sleep-attenuated prefrontal cortex activity impairing decision-making or increasing impulsivity.52,53 This bidirectionality reinforces earlier cross-sectional findings among firefighters that link alcohol use severity with worse sleep quality and greater sleep disturbances.8,23 Furthermore, the dynamics of these relationships suggest a potentially reinforcing cycle of sleep disruption and alcohol use.
Contrary to our hypothesis, greater caffeine consumption was associated with slightly better actigraphic sleep outcomes, including higher sleep efficiency and fewer nighttime awakenings at the between-person level and longer sleep at the within-person level. These findings run counter to laboratory and epidemiological studies of the general population that demonstrate how caffeine disrupts sleep,31,32 likely through adenosine receptor antagonism that reduces sleep pressure and can delay sleep onset depending on dose and timing.54–56 However, these findings are partially consistent with studies of firefighters. Among Korean firefighters, caffeine consumption was associated with lower odds of insomnia symptoms despite worse overall sleep quality,34,35 whereas caffeine overconsumption was associated with worse health but not sleep among U.S. firefighters.7 Regardless, because the time of day when caffeine was ingested was not assessed in this study, these reported findings should be interpreted with skepticism. Future studies should query when during the day caffeine or any other substance is consumed.
Findings partially supported our hypothesis that use of nicotine products would be cross-sectionally associated with worse sleep. We observed null associations between combustible tobacco products and sleep outcomes, consistent with prior studies of firefighters.7,35 However, unlike prior studies, this study leveraged actigraphy to assess sleep. In the general population, nicotine use is more consistently associated with worse objective sleep than with self-reported sleep quality.40,41 Mechanistically, nicotine binds to nicotinic acetylcholine receptors, enhancing cholinergic signaling and downstream dopaminergic and serotonergic activity, all of which increases cortical arousal and promotes wakefulness.57 As a result, individuals may feel more alert following acute nicotine use;58 however, this increased arousal can delay sleep onset when used close to bedtime.57 As nicotine levels decline overnight, withdrawal-related increases in arousal may contribute to nighttime or early morning awakenings.42,57 The null findings for combustible tobacco products in the present study likely reflect limited variability and statistical power rather than a true absence of association. Measures of tobacco use were also coarse, and current smoking status identified only one participant, whose sleep outcomes were largely within one standard deviation of the sample mean (with the exception of sleep onset timing). Conversely, 8% of the sample currently used noncombustible, smokeless tobacco products. Smokeless tobacco use was associated with approximately half an hour of shorter sleep, a clinically meaningful difference consistent with findings in the general population,40,41 although estimates were imprecise due to the limited number of participants who used smokeless tobacco. Future studies should continue to explore the relationship between tobacco use and shorter sleep among firefighters, especially if the prevalence of smokeless tobacco use continues to increase in the fire service.16,37,38
Limitations
Several limitations should be considered when interpreting the findings of the present study. The sample was modestly sized and primarily derived from relatively healthy firefighters in Oregon. As such, the current sample may not represent other career or volunteer firefighters, other shift-working populations, or women firefighters. Substance use was assessed via self-report, which may have been subject to recall or social desirability bias, particularly in an occupational context where use of nicotine, caffeine, or especially alcohol is likely underreported. Nicotine use was operationalized using coarse indicators (ie, current or lifetime use), without any daily items that queried use of cigarettes or chewing tobacco. Consequently, only between-person, cross-sectional associations between nicotine use and sleep were assessed, precluding characterization of directionality, the dose-response relationship, or concurrent use of different nicotine products. Fortunately, there were daily items to assess approximate alcohol and caffeine use. However, these daily items did not capture the time of day of use, such as whether alcohol was primarily ingested in the evenings or caffeine in the mornings. Participants may have consumed additional alcohol or caffeine following completion of their evening survey, thereby underestimating their actual substance use. Moreover, total calculated caffeine use was based on assumed standard caffeine values,44 whereas actual caffeine content varies widely, particularly for energy drinks and specialty coffees. The sleep of firefighters in this study may have been overestimated, because actigraphy systematically misclassifies low-activity periods of wakefulness as sleep,59 and therefore should be interpreted with some reservation.60,61 We leveraged a micro-longitudinal design with multilevel modeling to disentangle the between- and within-person effects. This allowed the examination of directionality between substance use and sleep, yet analyses ultimately remain observational and causal inference cannot be drawn. Finally, other unassessed factors (eg, mental health, acute occupational stress, shift-specific workload, heterogeneity of emergency calls) may explain some observed associations. For example, post-traumatic stress experienced by firefighters has been linked to poorer sleep quality,62 including through pathways such as burnout and depressive symptomatology.63 Future studies of firefighters should consider the daily, time-varying experience of mental health symptoms on both sleep and substance use.
Conclusions
This study revealed how firefighters’ alcohol use and sleep temporally relate using micro-longitudinal study design, objective sleep assessment, and multilevel analyses. Based on between-person findings, the relationship between use of nicotine and caffeine with sleep seemed primarily person-dependent, with caffeine use being particularly nuanced. Conversely, alcohol use was strongly and bidirectionally tied to sleep. Taken together, these findings highlight potential targets for sleep health interventions among firefighters or within fire departments, pending confirmation from experimental and prospective studies. For example, interventions that promote healthier coping strategies for occupational health and trauma may have downstream benefits on both alcohol use and sleep health.
Data Sharing Statement
Data are available upon reasonable request from the corresponding author.
Ethics Approval
This study involved human participants. The study was approved by the Institutional Review Board at Oregon Health & Science University. All participants provided informed consent.
Acknowledgments
We would like to show our gratitude to the Portland Firefighters Association and Portland Fire & Rescue of Portland, OR for their support and participation in this study. The project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002369. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Author Contributions
David A. Reichenberger: Conceptualization, Data curation, Formal analysis, Methodology, Software, Writing – original draft, Writing – review and editing; Lauren Lee: Data curation, Investigation, Writing – original draft, Writing – review and editing; Joey Hebl: Data curation, Investigation, Writing – review and editing; Aanuoluwakiitan Ayeni: Data curation, Investigation, Project administration, Writing – review and editing; LaTroy D. Robinson: Data curation, Investigation, Writing – review and editing; Shelby L. Watkins: Data curation, Investigation, Project administration, Writing – review and editing; Ayeisha Haswarey: Data curation, Investigation, Writing – review and editing; David A. Hurtado: Investigation, Writing – review and editing; Andrew W. McHill: Investigation, Writing – review and editing; Todd Bodner: Conceptualization, Investigation, Methodology, Writing – review and editing; Steven A. Shea: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review and editing; Nicole P. Bowles: Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review and editing.
All authors made a significant contribution to the work reported; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Oregon Healthy Workforce Center, a National Institute for Occupational Safety and Health (NIOSH) Total Worker Health Center of Excellence (U19OH010154) and The Northwest Center for Occupational Health and Safety Professional Training Opportunities Program (PTOP) grant (T42OH008433-19-00). This work was also partly supported by the Oregon Institute of Occupational Health Sciences at Oregon Health & Science University via funds from the Division of Consumer and Business Services of the State of Oregon (ORS 656.630) and in part by NHLBI (R35HL155681) from the National Institutes of Health. DAR was supported by the Cardiovascular Research and Translational Science Fellowship (T32-HL166128). NIOSH was not involved in the design, data collection, analysis, or interpretation of the data of this study or in writing of this article.
Disclosure
DAR received a small honorarium from the National Sleep Foundation for participation in a consensus panel. AWM reports consulting for Pure Somni Inc and Portland Public Schools. NPB reports consulting with Mcgillivary Steele Elkin LLP, receiving grants from NIOSH and funding from the Division of Consumer and Business Services of the State of Oregon. SAA reports grants from NIH, and funding from the Division of Consumer and Business Services of the State of Oregon. The Authors confirm no further conflicts of interest in the reporting of this work.
References
1. Marvin G, Schram B, Orr R, Canetti EF. Occupation-induced fatigue and impacts on emergency first responders: a systematic review. Int J Environ Res Public Health. 2023;20(22):7055. doi:10.3390/ijerph20227055
2. Huang G, Lee TY, Banda KJ, et al. Prevalence of sleep disorders among first responders for medical emergencies: a meta-analysis. J Glob Health. 2022;12:04092. doi:10.7189/jogh.12.04092
3. Watkins SL, Shannon MA, Hurtado DA, Shea SA, Bowles NP. Interactions between home, work, and sleep among firefighters. Am J Ind Med. 2021;64(2):137–12. doi:10.1002/ajim.23194
4. Dzierzewski JM, Dautovich ND, Sabet SM, et al. Is healthy sleep possible for professional firefighters? A comparison of “On-Duty” and “Off-Duty” sleep. Sleep Health. 2025.
5. Billings J, Focht W. Firefighter shift schedules affect sleep quality. J Occup Environ Med. 2016;58(3):294–298. doi:10.1097/JOM.0000000000000624
6. Barger LK, Rajaratnam SMW, Wang W, et al. Common sleep disorders increase risk of motor vehicle crashes and adverse health outcomes in firefighters. J Clin Sleep Med JCSM off Publ Am Acad Sleep Med. 2015;11(3):233–240. doi:10.5664/jcsm.4534
7. Carey MG, Al-Zaiti SS, Dean GE, Sessanna L, Finnell DS. Sleep problems, depression, substance use, social bonding, and quality of life in professional firefighters. J Occup Environ Med. 2011;53(8):928–933. doi:10.1097/JOM.0b013e318225898f
8. Vargas de Barros V, Martins LF, Saitz R, Bastos RR, Ronzani TM. Mental health conditions, individual and job characteristics and sleep disturbances among firefighters. J Health Psychol. 2013;18(3):350–358. doi:10.1177/1359105312443402
9. Hunnicutt LE, Corgan M, Brown SR, Nygaard A, Meares IVGL, Collier SR. Sleep differences in firefighters: barracks vs. home. Int J Environ Res Public Health. 2024;21(9):1155. doi:10.3390/ijerph21091155
10. Beaton R, Murphy S, Johnson C, Pike K, Corneil W. Exposure to duty-related incident stressors in urban firefighters and paramedics. J Trauma Stress Off Publ Int Soc Trauma Stress Stud. 1998;11(4):821–828. doi:10.1023/A:1024461920456
11. Beaton R, Murphy S, Johnson C, Pike K, Corneil W. Coping responses and posttraumatic stress symptomatology in urban fire service personnel. J Trauma Stress. 1999;12(2):293–308. doi:10.1023/A:1024776509667
12. Odes R, Hong O, Hong O. Job stress and sleep disturbances among career firefighters in Northern California. J Occup Environ Med. 2023;65(8):706–710. doi:10.1097/JOM.0000000000002901
13. Rajabi F, Molaeifar H, Jahangiri M, Taheri S, Banaee S, Farhadi P. Occupational stressors among firefighters: application of multi-criteria decision making (MCDM) techniques. Heliyon. 2020;6(4):e03820. doi:10.1016/j.heliyon.2020.e03820
14. Dyal MAA, Smith TD, DeJoy DM, Moore BA. Occupational stress and burnout in the fire service: examining the complex role and impact of sleep health. Behav Modif. 2022;46(2):374–394. doi:10.1177/01454455211040049
15. Wolkow AP, Barger LK, O’Brien CS, et al. Associations between sleep disturbances, mental health outcomes and burnout in firefighters, and the mediating role of sleep during overnight work: a cross-sectional study. J Sleep Res. 2019;28(6):e12869. doi:10.1111/jsr.12869
16. Jitnarin N, Poston WS, Haddock CK, Jahnke SA, Day RS. Tobacco Use Pattern Among a National Firefighter Cohort. Nicotine Tob Res. 2015;17(1):66–73. doi:10.1093/ntr/ntu131
17. Temple JL, Hostler D, Martin-Gill C, et al. Systematic review and meta-analysis of the effects of caffeine in fatigued shift workers: implications for emergency medical services personnel. Prehosp Emerg Care. 2018;22(sup1):37–46. doi:10.1080/10903127.2017.1382624
18. Buguet A, Montmayeur A, Pigeau R, Naitoh P. Modafinil, d-amphetamine and placebo during 64 hours of sustained mental work. II. Effects on two nights of recovery sleep. J Sleep Res. 1995;4(4):229–241. doi:10.1111/j.1365-2869.1995.tb00173.x
19. Pigeau R, Naitoh P, Buguet A, et al. Modafinil, d-amphetamine and placebo during 64 hours of sustained mental work. I. Effects on mood, fatigue, cognitive performance and body temperature. J Sleep Res. 1995;4(4):212–228. doi:10.1111/j.1365-2869.1995.tb00172.x
20. Haddock CK, Jitnarin N, Poston WS, Tuley B, Jahnke SA. Tobacco use among firefighters in the central United States. Am J Ind Med. 2011;54(9):697–706. doi:10.1002/ajim.20972
21. Haddock CK, Jahnke SA, Poston WSC, et al. Alcohol use among firefighters in the Central United States. Occup Med Oxf Engl. 2012;62(8):661–664. doi:10.1093/occmed/kqs162
22. Haddock CK, Poston WS, Jahnke SA, Jitnarin N. Alcohol use and problem drinking among women firefighters. Womens Health Issues. 2017;27(6):632–638. doi:10.1016/j.whi.2017.07.003
23. Smith LJ, Gallagher MW, Tran JK, Vujanovic AA. Posttraumatic stress, alcohol use, and alcohol use reasons in firefighters: the role of sleep disturbance. Compr Psychiatry. 2018;87:64–71. doi:10.1016/j.comppsych.2018.09.001
24. Haddock CK, Day RS, Poston WSC, Jahnke SA, Jitnarin N. Alcohol use and caloric intake from alcohol in a national cohort of U.S. career firefighters. J Stud Alcohol Drugs. 2015;76(3):360–366. doi:10.15288/jsad.2015.76.360
25. Rasmus P, Kocur J, Flirski M, Sobów T. Biopsychosocial correlates of psychoactive substance use in professional firefighters. J Med Sci Technol. 2013;54:70–75. doi:10.12659/MST.889093
26. Gardiner C, Weakley J, Burke LM, et al. The effect of alcohol on subsequent sleep in healthy adults: a systematic review and meta-analysis. Sleep Med Rev. 2025;80:102030. doi:10.1016/j.smrv.2024.102030
27. Astorino TA, Roberson DW. Efficacy of acute caffeine ingestion for short-term high-intensity exercise performance: a systematic review. J Strength Cond Res. 2010;24(1):257–265. doi:10.1519/JSC.0b013e3181c1f88a
28. Sünram-Lea SI, Owen-Lynch J, Robinson SJ, Jones E, Hu H. The effect of energy drinks on cortisol levels, cognition and mood during a fire-fighting exercise. Psychopharmacology. 2012;219(1):83–97. doi:10.1007/s00213-011-2379-0
29. Wikoff D, Welsh BT, Henderson R, et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem Toxicol. 2017;109:585–648. doi:10.1016/j.fct.2017.04.002
30. Berkowsky RS, Zaleski AL, Taylor BA, et al. Cardiometabolic biomarkers and habitual caffeine consumption associate with the adverse ambulatory blood pressure response to strenuous physical exertion among firefighters. Nutrients. 2022;14(19):4025. doi:10.3390/nu14194025
31. Drake C, Roehrs T, Shambroom J, Roth T. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J Clin Sleep Med JCSM off Publ Am Acad Sleep Med. 2013;9(11):1195–1200. doi:10.5664/jcsm.3170
32. Gardiner C, Weakley J, Burke LM, et al. The effect of caffeine on subsequent sleep: a systematic review and meta-analysis. Sleep Med Rev. 2023;69:101764. doi:10.1016/j.smrv.2023.101764
33. Bonnet MH, Arand D. Caffeine use as a model of acute and chronic insomnia. Sleep. 1992;15(6):526–536.
34. Jeong S, Kim J, Oh SS, Kang HT, Ahn YS, Jeong KS. The risk of insomnia by work schedule instability in Korean firefighters. Ann Occup Environ Med. 2024;36:e24. doi:10.35371/aoem.2024.36.e24
35. Lim M, Lee S, Seo K, et al. Psychosocial factors affecting sleep quality of pre-employed firefighters: a cross-sectional study. Ann Occup Environ Med. 2020;32:e12. doi:10.35371/aoem.2020.32.e12
36. Jitnarin N, Poston WSC, Haddock CK, Jahnke SA. Tobacco use among women firefighters. Womens Health Issues. 2019;29(5):432–439. doi:10.1016/j.whi.2019.05.006
37. Phan L, McNeel TS, Jewett B, Moose K, Choi K. Trends of cigarette smoking and smokeless tobacco use among U.S. firefighters and law enforcement personnel, 1992–2019. Am J Ind Med. 2022;65(1):72–77. doi:10.1002/ajim.23311
38. Jitnarin N, Poston WS, Haddock CK, Jahnke SA, Day RS, Severson HH. Prevalence and correlates of late initiation of smokeless tobacco in US firefighters. Nicotine Tob Res. 2017;20(1):130–134. doi:10.1093/ntr/ntw321
39. Gulliver SB, Zimering R, Knight J, et al. Tobacco and alcohol use among firefighters during their first 3 years of service. Psychol Addict Behav J Soc Psychol Addict Behav. 2018;32(3):255–263. doi:10.1037/adb0000366
40. Catoire S, Nourredine M, Lefebvre S, et al. Tobacco-induced sleep disturbances: a systematic review and meta-analysis. Sleep Med Rev. 2021;60:101544. doi:10.1016/j.smrv.2021.101544
41. Garcia AN, Salloum IM. Polysomnographic sleep disturbances in nicotine, caffeine, alcohol, cocaine, opioid, and cannabis use: a focused review. Am J Addict. 2015;24(7):590–598. doi:10.1111/ajad.12291
42. Branstetter SA, Horton WJ, Mercincavage M, Buxton OM. Severity of nicotine addiction and disruptions in sleep mediated by early awakenings. Nicotine Tob Res. 2016;18(12):2252–2259. doi:10.1093/ntr/ntw179
43. Abdelmoaty WF, Watkins SL, Ayeni A, et al. Impact of firefighters’ work schedule on cardiovascular disease risk, wellbeing and safety in firefighters: protocol for the SWIFT study, a multidisciplinary prospective and cross-sectional study. BMJ Public Health. 2025;3(2):e002427. doi:10.1136/bmjph-2024-002427
44. Irons JG, Bassett DT, Prendergast CO, Landrum RE, Heinz AJ. Development and initial validation of the caffeine consumption questionnaire-revised. J Caffeine Res. 2016;6(1):20–25. doi:10.1089/jcr.2015.0012
45. Carney CE, Buysse DJ, Ancoli-Israel S, et al. The consensus sleep diary: standardizing prospective sleep self-monitoring. Sleep. 2012;35(2):287–302. doi:10.5665/sleep.1642
46. Fekedulegn D, Andrew ME, Shi M, Violanti JM, Knox S, Innes KE. Actigraphy-based assessment of sleep parameters. Ann Work Expo Health. 2020;64(4):350–367. doi:10.1093/annweh/wxaa007
47. Mograss M, Abi-Jaoude J, Frimpong E, et al. The effects of napping on night-time sleep in healthy young adults. J Sleep Res. 2022;31(5):e13578. doi:10.1111/jsr.13578
48. Pinheiro J, Bates D, DebRoy S, Sarkar D. R Core team. nlme: linear and nonlinear mixed effects models; 2021. Available from: https://CRAN.R-project.org/package=nlme.
49. Brooks ME, Kristensen K, Van Benthem KJ, et al. glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. 2017.
50. Dharavath RN, Pina-Leblanc C, Tang VM, et al. GABAergic signaling in alcohol use disorder and withdrawal: pathological involvement and therapeutic potential. Front Neural Circuits. 2023;17:1218737.
51. St-Onge MP, Aggarwal B, Fernandez-Mendoza J, et al. Multidimensional sleep health: definitions and implications for cardiometabolic health: a scientific statement from the American Heart Association. Circ Cardiovasc Qual Outcomes. 2025;18(5):e000139. doi:10.1161/HCQ.0000000000000139
52. Zhao R, Zhang X, Fei N, et al. Decreased cortical and subcortical response to inhibition control after sleep deprivation. Brain Imaging Behav. 2019;13(3):638–650. doi:10.1007/s11682-018-9868-2
53. Thomas M, Sing H, Belenky G, et al. Neural basis of alertness and cognitive performance impairments during sleepiness. I. Effects of 24 h of sleep deprivation on waking human regional brain activity. J Sleep Res. 2000;9(4):335–352. doi:10.1046/j.1365-2869.2000.00225.x
54. Ribeiro JA, Sebastiao AM. Caffeine and adenosine. J Alzheimer’s Dis. 2010;20(s1):S3–S15. doi:10.3233/JAD-2010-1379
55. Reddy VS, Shiva S, Manikantan S, Ramakrishna S. Pharmacology of caffeine and its effects on the human body. Eur J Med Chem Rep. 2024;10:100138.
56. Gardiner CL, Weakley J, Burke LM, et al. Dose and timing effects of caffeine on subsequent sleep: a randomized clinical crossover trial. Sleep. 2025;48(4):zsae230. doi:10.1093/sleep/zsae230
57. Singh N, Wanjari A, Sinha AH. Effects of nicotine on the central nervous system and sleep quality in relation to other stimulants: a narrative review. Cureus. 2023;15(11):e49162. doi:10.7759/cureus.49162
58. Valentine G, Sofuoglu M. Cognitive effects of nicotine: recent progress. Curr Neuropharmacol. 2018;16(4):403–414. doi:10.2174/1570159X15666171103152136
59. Marino M, Li Y, Rueschman MN, et al. Measuring sleep: accuracy, sensitivity, and specificity of wrist actigraphy compared to polysomnography. Sleep. 2013;36(11):1747–1755. doi:10.5665/sleep.3142
60. Marmis R, McGoldrick-Ruth L, Kelly MR, Haynes PL. Comparing actigraphy and diary to measure daily and average sleep in firefighters: a bland–altman analysis. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2024;20(4):497–503. doi:10.5664/jcsm.10916
61. Billings JM. Firefighter sleep: a pilot study of the agreement between actigraphy and self-reported sleep measures. J Clin Sleep Med JCSM Off Publ Am Acad Sleep Med. 2022;18(1):109–117. doi:10.5664/jcsm.9566
62. Khumtong C, Taneepanichskul N. Posttraumatic stress disorder and sleep quality among urban firefighters in Thailand. Nat Sci Sleep. 2019;11:123–130. doi:10.2147/NSS.S207764
63. Khoshakhlagh AH, Sulaie SA, Cousins R, Yazdanirad S, Laal F. Understanding the effect of occupational stress on sleep quality in firefighters: the modulating role of depression and burnout. Int Arch Occup Environ Health. 2024;97(9):1007–1016. doi:10.1007/s00420-024-02104-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.