")
Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Skin-to-Skin Care Practice and Its Associated Factors Among Postpartum Mothers in Gurage Zone, Southern Ethiopia: A Cross-Sectional Study
Authors Mose A , Adane D, Abebe H
Received 16 February 2021
Accepted for publication 7 June 2021
Published 16 June 2021 Volume 2021:12 Pages 289—297
DOI https://doi.org/10.2147/PHMT.S306411
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Ayenew Mose,1 Daniel Adane,1 Haimanot Abebe2
1Department of Midwifery, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 2Department of Public Health, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
Correspondence: Ayenew Mose Tel +251913634706
Email [email protected]
Background: Skin-to-skin care is placing an unclothed or diaper-only newborn baby on the mother’s bare chest, covered with a warm blanket. The World Health Organization recommends immediate, uninterrupted, and continuous mother–newborn skin-to-skin care practice almost immediately after birth. Despite this recommendation, separation of the newborn from the mother is common in many public health institutions. There was a limited study that examined the prevalence of skin-to-skin care practice and associated factors in Ethiopia. Therefore, the main aim of this study was to assess the prevalence of skin-to-skin care practice and its associated factors among postpartum mothers in Gurage Zone public health centers, Southern Ethiopia, 2020.
Methods: An institution-based cross-sectional study was conducted in twenty-two public health centers of Gurage Zone from January 1st up to 30th, 2020. A total of 382 postpartum mothers were selected using a systematic sampling technique. Data were collected using structured and pre-tested interviewer-administered questionnaires. Data were entered into EpiData version 3.1.0 and exported to SPSS version 23 for analysis. Both bivariable and multivariable logistic regression analyses were used to identify significant factors associated with skin-to-skin care practice. Statistical significance was declared at a P-value of < 0.05 with a 95% confidence level.
Results: About 35.3% (95% CI; 31.3%– 40.4%) of new-borns were received skin-to-skin care practice. Being urban residence [AOR=2.23, (95% CI; 1.17– 4.23)], normal newborn birth weight (≥ 2500gm) [AOR=3.1, (95% CI; 2.15– 3.89)], early initiation of breastfeeding [AOR=2.93, (95% CI; 1.29– 6.64)], colostrum feeding [AOR=4.19, (95% CI; 2.01– 8.73)], and having mothers good knowledge on skin-to-skin care practice [AOR=8.51, (95% CI; 4.32– 16.75)] were some of factors associated with mother to newborn skin-to-skin care practice.
Conclusion: The proportion of mother newborn skin-to-skin care practice was low in the study area. Mothers resided in the urban areas, normal newborn birth weight, early initiation of breastfeeding, colostrum feeding, and having good knowledge of the mothers about skin-to-skin care were factors associated with skin-to-skin care practice. Therefore, health care workers should counsel mothers on optimal breastfeeding practice and enhance maternal awareness regarding the merits of skin-to-skin care practice before discharge from the health facilities are recommended.
Keywords: skin-to-skin care, colostrum, breastfeeding, mother, newborn
Introduction
Maternal and child health can be improved through skin-to-skin care practice, which involves placing an unclothed or diaper only newborn baby on the mother’s bare chest immediately (within 10 minutes after birth) or early (any time after birth up to 23 hours) after delivery and keeping them together continuously for at least 1 hour regardless of the mode of delivery, birth setting, and infant feeding method.1
Skin-to-skin care (SSC) has tremendous benefits for both newborn and maternal health. For newborn, it stabilizes cardiovascular system and blood glucose level in preterm neonates, prevents hypothermia, enhances bonding, and reduce neonatal crying.2,3 For mothers, it is used to reduce maternal stress, postpartum depression, improved maternal attachment behaviour, and increases oxytocin level through an enhancement of early breastfeeding initiation, which in turn reduces postpartum hemorrhage the primary cause of maternal mortality in developing countries.4
World Health Organization, United Nation International Children Emergency Fund, Baby-Friendly Hospital Initiative,1 and American Academy of Pediatrics5,6 recommend SSC practice soon after birth. Despite this recommendation, separation of the newborn from the mother immediately following delivery is a common practice in many public health institutions.7
Worldwide, approximately 2.5 million newborns died per year.8 In Ethiopia, neonatal mortality increases from 29 in 2016 to 30 per 1000 live births in 2019, which indicates neonatal mortality is still stagnant and unacceptably high.9,10 By the end of 2030, Ethiopia has promised to reduce neonatal mortality to 12 deaths per 1000 live births.8,11 To achieve this ambition, continuous provision of safe and effective maternal-newborn SSC practice is crucial, particularly for developing countries that did not have adequate medical equipment such as infant radiant warmer to prevent neonatal hypothermia.1
The prevalence of SSC practice varies from 1% in Tanzania12 to 96% in Denmark.7 In Ethiopia, there are only a few studies conducted to assess SSC practice. For instance, the study conducted by Bedaso et al found that 28.1% of mothers were practiced SSC.13 Similarly, Abebe et al were found that 34.4% of mothers practiced SSC.14 Maternal education, antenatal care visits, and mode of delivery (vaginal delivery) were some of the factors associated with SSC practice in the previous study. Lack of standardized definition of SSC practice and inconsistency of findings was the limitation of previous studies.
Although SSC is a safe and effective approach to prevent neonatal mortality, particularly in low resource income settings and has widely promoted in the delivery ward; yet, data on SSC practice followed the delivery of the newborn in the study setting was limited. Therefore, the main aim of this study was to assess the prevalence of SSC practice and its associated factors among mothers who gave birth in Gurage Zone public health centers.
Methods and Materials
Study Setting, Design and Period
An institution-based cross-sectional study design was conducted in the Gurage Zone, Southern Ethiopia from January 1st up to 30th, 2020. Gurage Zone is found 153 kilometers southwest of Addis Ababa, the capital city of Ethiopia. Wolkite is the administrative center of the Zone. According to the Central Statistical Agency of Ethiopia (CSA) in 2007, this Zone has a total population of 1,279,646, of whom 622,078 were men and 657,568 were women. The distributions of health centers in the Gurage Zone were 72 health centers and 402 health posts. All public health centers were providing maternal health care services for antenatal care, labor and delivery, and postpartum care service to mothers without any charges (free service).
Populations
The source populations were all postnatal mothers who had alive neonates in Gurage Zone public health centers whereas all postnatal mothers with alive/healthy newborns and admitted to the postnatal ward during the study period were taken as the study populations.
Inclusion and Exclusion Criteria
All postnatal mothers who had a healthy newborn were included. All postnatal mothers who had unable to respond, having childbirth complications, and newborn with congenital malformations were excluded.
Sample Size Determination
The minimum sample size for this study was determined using a single population proportion formula based on the following assumptions. The proportion of mothers who had skin-to-skin care practice (P=34.4%),14 95% confidence level (z=1.96), and a margin error to be 5% (d=0.05) and 10% non-response rate. The final sample size was therefore calculated to be 382 post-natal mothers.
Sampling Procedures
From seventy-two public health centers, twenty-two health centers were selected randomly. Initially, the calculated sample size was proportionally allocated to population size in each health center. Then, each postnatal mother was selected by using a systematic random sampling method (every third postnatal mother was selected) based on the allocated proportion.
Data Collection Tools
A structured interviewer-administered questionnaire was used to collect data. The tool was prepared after reviewing different works of relevant literatures.10,13,14 Seven experienced diploma holder midwives and two BSc holder midwives were recruited and trained for data collection and supervision, respectively. The tool contains socio-demographic characteristics, maternal health care service utilization related, mother–newborn SSC practice-related, knowledge, and attitude related items.
Operational Definition
Skin-to-Skin Care Practice
The World Health Organization (WHO) defined SSC as placing an unclothed or diaper only newborn baby on the mother’s bare chest or abdomen soon after birth and keeping them together continuously for at least 1 hour regardless of the mode of delivery (ie, cesarean section or vaginal delivery), birth setting (ie, health institution or home) and feeding method (ie, breastfeeding or formula feeding).1 In this study, skin-to-skin care practice was measured dichotomously as “Yes” (Practiced mother–newborn SSC) coded and “No” (did not practice mother–newborn SSC).15
Immediate Skin-to-Skin Care
Mothers who had initiated skin-to-skin care practice within 10 minutes after delivery of the newborn.1
Early Skin-to-Skin Care
Mothers who had initiated skin-to-skin care practice at any time after birth and continue up to the first 23 hours.1
Knowledge of Mothers About SSC
Those mothers who were responded greater than or equal to 50% of skin-to-skin care-related questions were considered as having good knowledge and those who responded less than 50% were considered as poor knowledge.16
The Attitude of Mothers Towards SSC
Those mothers who scored ≥ mean value on attitude-related questions were considered as having good attitude whereas those mothers who scored below the mean score of attitude-related questions were considered as having a poor attitude.
Data Quality Control
To ensure quality, the questionnaire was translated into the local language (Amharic) by experts. Finally, before data collection, it was re-translated back to English language to verify consistency. Before starting the actual data collection, two days (one day theoretical and one day practical) of extensive training was given for the data collectors and supervisors. A pre-test for appropriateness and feasibility of the tool was conducted and all necessary modifications and amendments were done accordingly. The reliability of the questionnaires was checked through SPSS by reliability index measurement for SSC practice (Cronbach’s alpha correlation coefficient was 0.75). The data collection team were communicated and discussed with principal investigators if they face any challenges during the data collection period daily. After data collection before analysis, all collected data were checked for completeness.
Data Processing and Analysis
Data were coded, cleaned, edited, and entered into EpiData version 3.1.0 and exported to SPSS version 23 for statistical analysis. Descriptive analysis was done by computing proportions and summary statistics. The presence of an association between explanatory and outcome variables was ascertained using binary logistic regression analysis. The goodness of fit was tested by the log-likelihood ratio (LR). To control all possible confounders all variables with P<0.25 in the bivariable analysis were included in the final model of multivariable analysis. In a multivariable model adjusted odds ratio determined with a 95% confidence level was used to assess the strength of association. In this study P-value <0.05 was deemed to declare statistical significance. Then, the finding was presented by using simple frequencies, summary measures, tables, texts, and figures.
Results
Socio-Demographic Characteristics
In this study, a total of 382 postpartum mothers having newborns participated with a response rate of 100%. The mean age of the study participants was 27.06 years (SD ± 4.845). Nearly one-third (36.9%) of mothers were found in the age group of 25–29 years. Three hundred forty-six (90.6%) were from the Gurage ethnic group, and 180 (47%) of mothers were orthodox religion followers. Three hundred thirty-four of the study participants (87.4%) were married in marital status. Two hundred ten (55%) of the study participants had completed primary educational level, and 128 (33.5%) of the participants were housewives (Table 1).
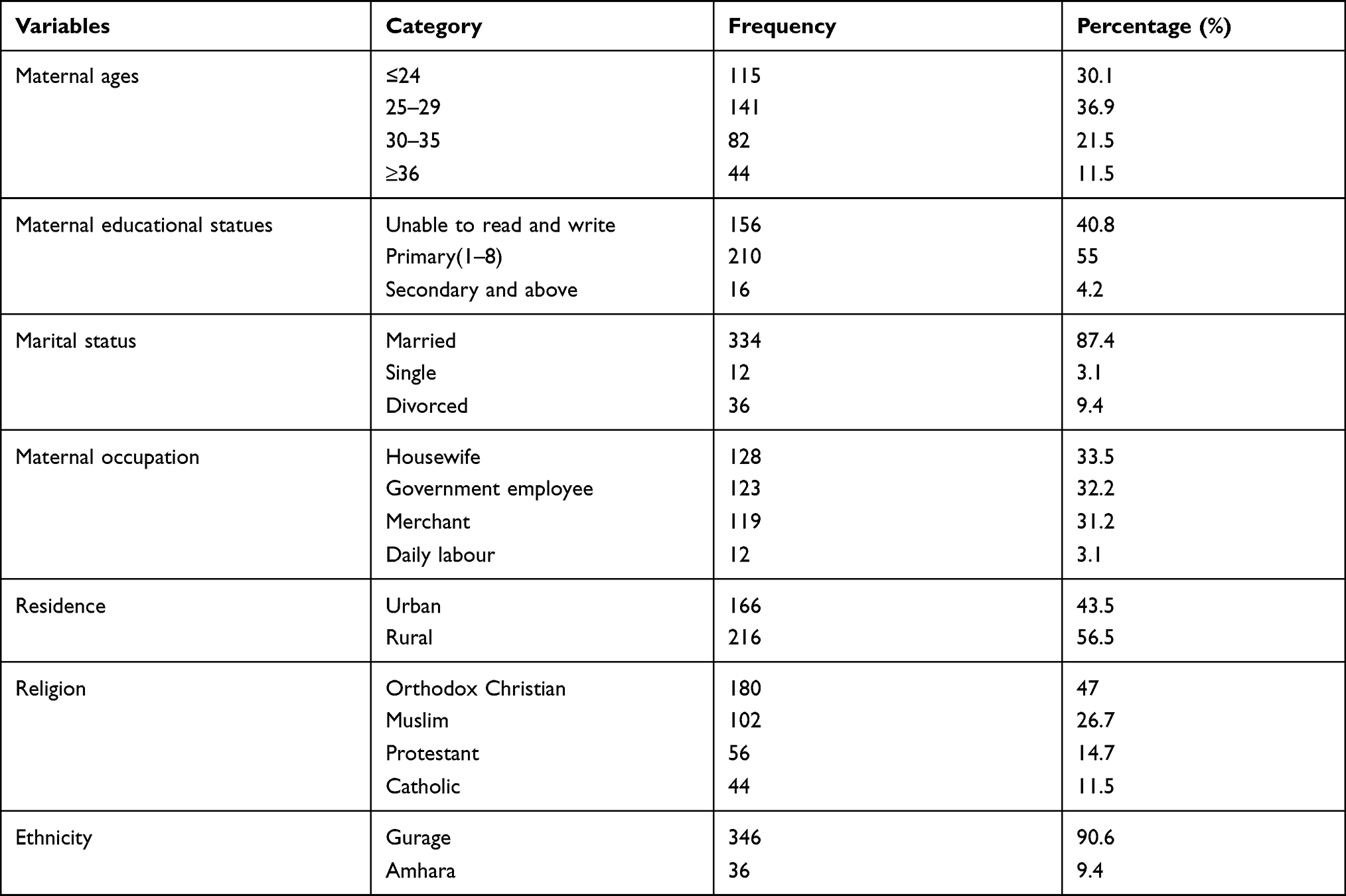 |
Table 1 Socio-Demographic Characteristics of Postpartum Mothers Attending Gurage Zone Public Health Centers, Southern Ethiopia 2020 |
Maternal Health Care Service Utilization
About three hundred five (79.8%) of mothers were multiparous. The majority 330 (86.4%) of mothers had a history of antenatal care (ANC) follow-up. One-fourth (25%) of mothers were completed ANC follow-up more than or equal to four times. The majority, 90.8% of mothers received counseling on immediate newborn care practice, 228 (59.7%) of mothers were not practiced colostrum feeding (Table 2).
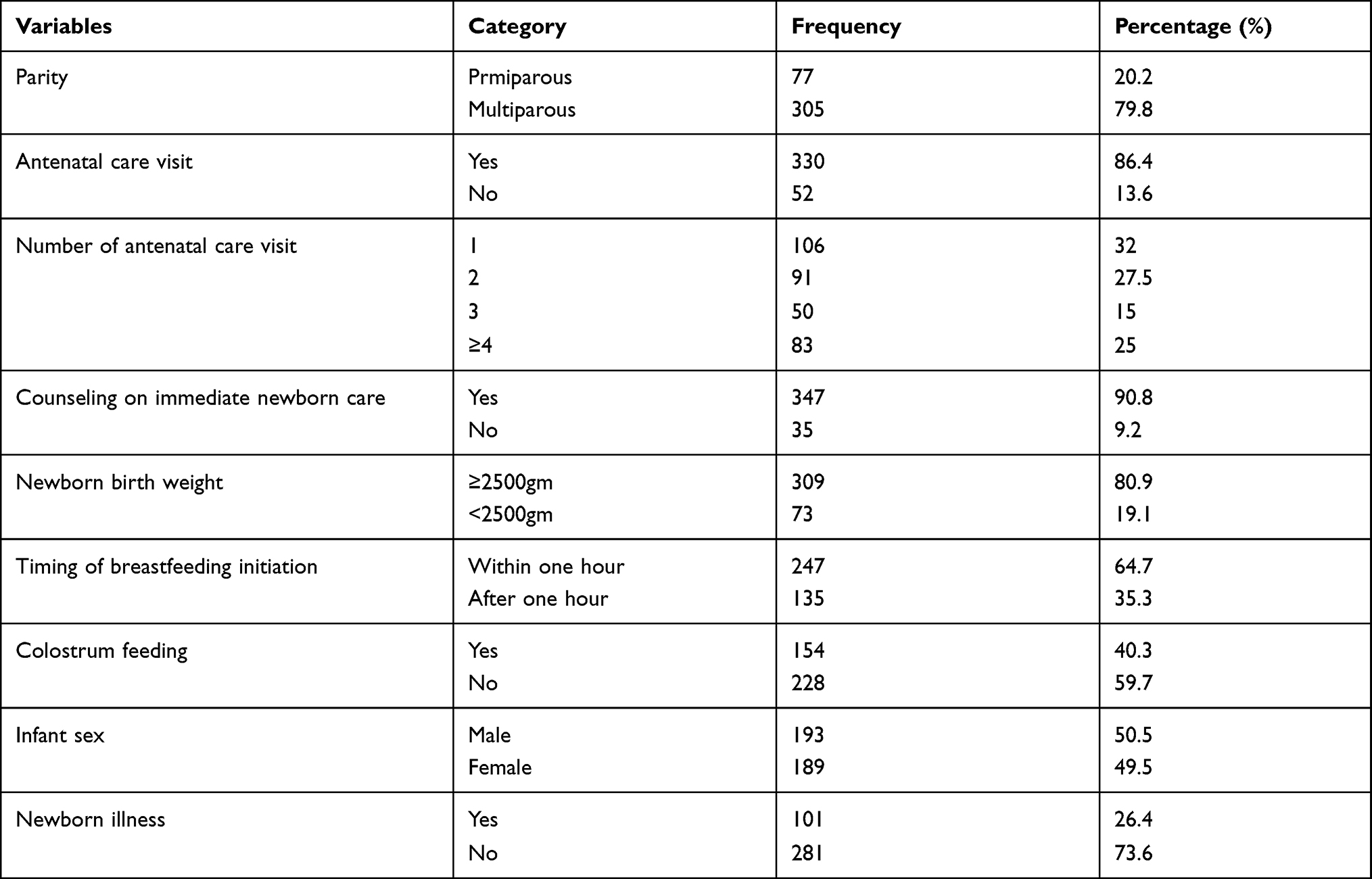 |
Table 2 Maternal Health Care Service Utilization of Postpartum Mothers Attending Gurage Zone Public Health Centers, Southern Ethiopia 2020 |
Prevalence of Skin-to-Skin Care Practice Among Respondents
This study revealed that the prevalence of skin-to-skin care practice among mothers was found to be 35.3% (95% CI; 31.3%–40.4%) (Figure 1).
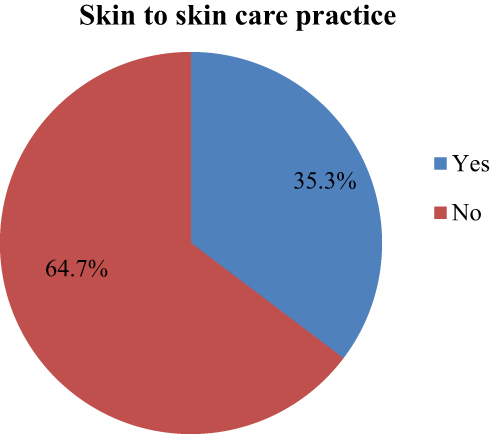 |
Figure 1 Prevalence of skin-to-skin care practices among postpartum mothers attending Gurage Zone public health centers, Southern Ethiopia, 2020. |
Source of Information Regarding Skin-to-Skin Care Practice
Only 44.5% of the study participants had heard about the skin-to-skin care practice. The main source of information for about 78.8% of the study participants was health professionals (Figure 2).
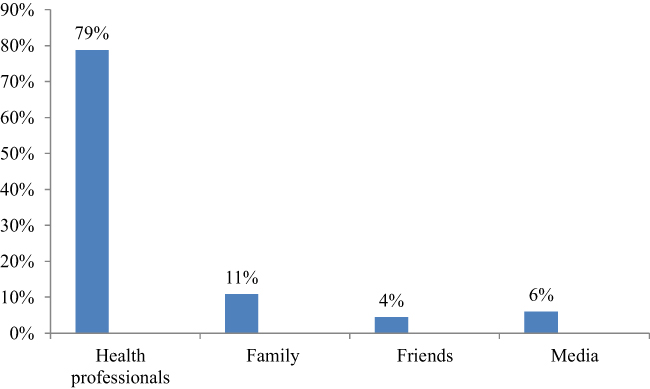 |
Figure 2 Maternal source of information regarding skin-to-skin care among postpartum mothers attending Gurage Zone public health centers, Southern Ethiopia, 2020. |
Knowledge and Attitude of Mothers Towards Skin-to-Skin Care Practice
The finding of this study showed that about 35.5% and 50.3% of mothers had good knowledge and a good attitude towards skin-to-skin care practice, respectively (Figure 3).
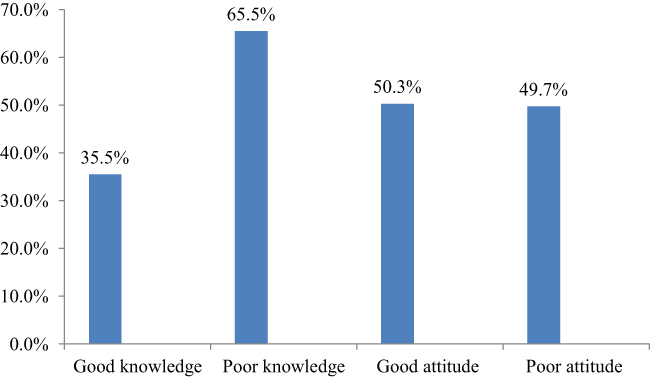 |
Figure 3 Maternal knowledge and attitude towards skin-to-skin care practice among postpartum mothers attending Gurage Zone public health centers, Southern Ethiopia, 2020. |
Factors Associated with Skin-to-Skin Care Practice
Both bivariable and multivariable logistic regression analyses were carried out to identify an association of maternal skin-to-skin care practice. The factors that showed a p-value of less than 0.25 were added to the multivariable regression model. The result of bivariable logistic regression analysis showed that mothers resided in the urban area, normal newborn birth weight (≥2500gm), multiparous mothers, early breastfeeding initiation, colostrum feeding, good attitude, and good knowledge of mothers towards skin-to-skin care were associated with SSC practice.
In multivariable logistic regression, all significant variables in binary logistic regression were adjusted. The result showed that mothers resided in the urban area; normal newborn birth weight, early breastfeeding initiation, colostrum feeding, and good knowledge of mothers were significantly associated with skin-to-skin care practice.
Those mothers who live in urban areas (AOR=2.23, 95% CI; 1.17–4.23), having normal birth weight newborn (≥2500gm) (AOR=3.1, 95% CI; 2.15–3.89), mothers who had initiated early breastfeeding (within one hour) (AOR=2.93, 95% CI; 1.29–6.64), mothers who gave colostrum feeding (AOR=4.19, 95% CI; 2.01–8.73), and mothers who had good knowledge (AOR=8.51, 95% CI; 4.32–16.75) were 2 times, 3 times, 2.9 times, 4 times and 8.5 times more likely to have practiced skin-to-skin care respectively (Table 3).
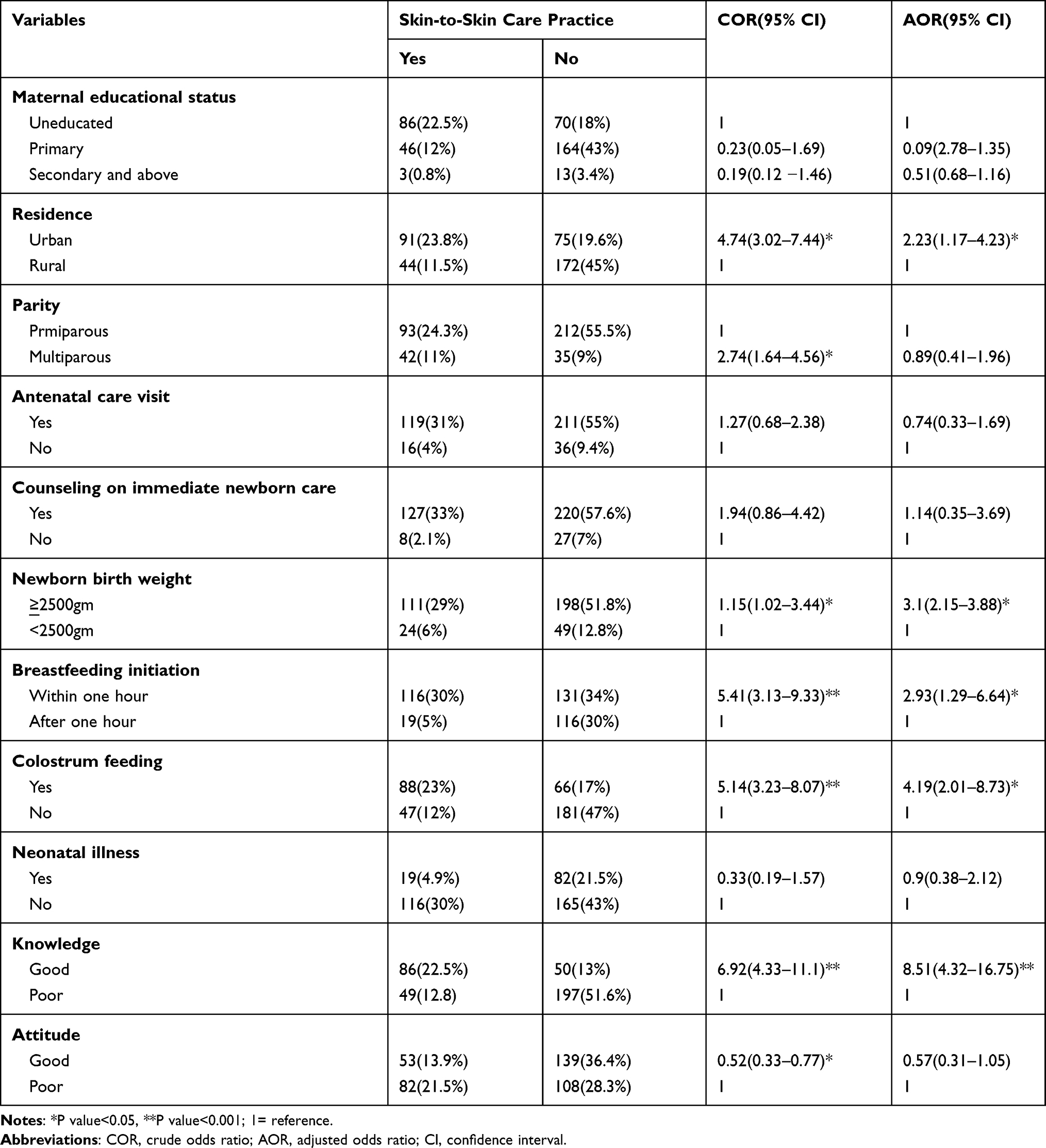 |
Table 3 Bivariate and Multivariate Logistic Regression Analyses of Skin-to-Skin Care Practice and Its Predictors Among Postpartum Mothers Attending in Gurage Zone Public Health Centers, Southern Ethiopia, 2020 |
Discussion
This study was conducted to assess skin-to-skin care practice and its associated factors among postnatal mothers who visit Gurage Zone public health centers; we found that 35.3% (95% CI; 31.3%–40.4%) of participants were practiced skin-to-skin care to their newborn. The finding of this study was comparable with the studies conducted in Harar city, eastern Ethiopia 34.4%,14 Gambia 35.7%,15 and Brazil 37.5%.17 The proportion of SSC practice in this study was higher than studies conducted in four regions of Ethiopia 25.8%,18 Eastern India 15%,7 and rural Ghana 10%.19 However, it was lower than a study conducted in Mekelle city, Tigray region 43.9%.20 The difference across the region might be due to the difference in access to health facilities, study population, sample size, and study area; for instance, Mekelle city is more urbanized compared to this study area.
This study found that those mothers who lived in urban areas were approximately 2 times more likely to practice SSC than their counterparts. This is because mothers who lived in urban areas might have access to quality health care services and they might have better awareness regarding the merits of skin-to-skin care practices. The finding of this study was inconsistent with the previous study conducted in the Gambia. In Gambia mothers from rural areas were more likely to practiced skin-to-skin care. This difference was due to the difference in the distribution of health facilities where the distribution of health facilities in the study setting is found in urban areas whereas, in the Gambia, the health facilities are more distributed and found in rural area.15
Mothers who had normal birth weight newborns (≥ 2500gm) were 3 times more likely to practice skin-to-skin care than those mothers who had low birth weight newborns. This finding was consistent with the studies conducted in Gambia and Brazil.15,17 This is because a low birth weight baby has the probability of developing different neonatal complications such as neonatal sepsis, congenital anomalies, neonatal jaundice, and respiratory distress syndrome. Therefore, the newborn might separate from mothers to receive different medical treatments which in turn may reduce the mother’s no time to practice skin-to-skin care.
Those mothers who initiated early breastfeeding were 2.9 times more likely to practice skin-to-skin care compared to their counterparts. This might be due to mothers who had initiated early breastfeeding could have a higher chance of increased bonding and they will have a probability of practicing skin-to-skin care.
This study also found that the good knowledge of mothers about skin-to-skin care was 8.5 times more likely to practice skin-to-skin care compared to those mothers who had poor knowledge of SSC. The reason might be those mothers who had good knowledge of the benefits of skin-to-skin care (prevent hypothermia, maintain newborn clam, stabilize newborn blood glucose) will have a high tendency of practicing skin-to-skin care.
Limitation of the Study
This study was conducted in health centers that might not show the true prevalence of skin-to-skin care practice. Lack of qualitative data supplementations to explore the socio-cultural factors and also shares the limitation of cross-section study design.
Conclusion
The prevalence of skin-to-skin care practice in the study area was low. Being an urban residence, having normal newborn birth weight, early breastfeeding initiation, colostrum feeding, and having good knowledge towards SSC practice were some of the factors associated with skin-to-skin care practice. Therefore, health care workers should create strategies to increase maternal access to media, provide health education on optimal breastfeeding practice and enhance maternal awareness regarding the merits of skin-to-skin care practice before discharge from the health facilities are recommended.
Abbreviations
AAP, American Academy of Paediatrics; ANC, antenatal care; BFHI, Baby-Friendly Hospital Initiative; WHO, World Health Organization; UNICEF, United Nation International Children Emergency Fund.
Data Sharing Statement
All related data has been presented within the manuscript. The data set supporting the conclusions of this article is available from the authors on reasonable request.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. Before conducting the study, ethical clearance was also obtained from the Wolkite University ethical review committee (CMHS/12/2020). Explanation about the purpose of the study and a letter of support was given to administrative bodies of Gurage Zone health office. A cooperation letter was written for all selected public health centers. Written informed consent was obtained from each of the study participants after clearly describing the purpose, benefit, and risk of the study. Study participants were informed of their full right to withdraw their participation at any stage of the interviewee. Confidentiality was maintained by using anonymous questionnaires.
Acknowledgments
The authors would like to thank Wolkite University, supervisors, data collectors, and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was obtained.
Disclosure
The authors declare that no one has competing interests.
References
1. World Health Organization. Guideline: protecting, promoting, and supporting breastfeeding in facilities providing maternity and newborn services. World Health Organization; 2017. Available from: https://apps.who.int/iris/bitstream/handle/10665/259386/9789241550086-eng.pdf.
2. Khadivzadeh T, Karimi FZ, Tara F, Bagheri S. The effect of postpartum mother-infant skin-to-skin contact on exclusive breastfeeding in the neonatal period: a randomized controlled trial. Int J Pediatr. 2017;5(7):5409–5417. doi:10.22038/ijp.2016.7522
3. Chwo MJ, Anderson GC, Good M, Dowling DA, Shiau SH, Chu DM. A randomized controlled trial of early kangaroo care for preterm infants: effects on temperature, weight, behavior, and acuity. J Nurs Res. 2002;10(2):129–142. doi:10.1097/01.JNR.0000347592.43768.46
4. Scime NV, Gavarkovs AG, Chaput KH. The effect of skin-to-skin care on postpartum depression among mothers of preterm or low birth weight infants: a systematic review and meta-analysis. J Affect Disord. 2019;253:376–384. doi:10.1016/j.jad.2019.04.101
5. Baley J. Skin-to-skin care for the term and preterm infants in the neonatal ICU. Pediatrics. 2015;136(3):596–599. doi:10.1542/peds.2015-2335
6. Feldman-Winter L, Goldsmith JP, Moon RY, et al. Safe sleep and skin-to-skin care in the neonatal period for healthy term newborns. Pediatrics. 2016;138:3. doi:10.1542/peds.2016-1889
7. Abdulghani N, Edvardsson K, Amir LH, van Wouwe JP. Worldwide prevalence of mother-infant skin-to-skin contact after vaginal birth: a systematic review. PLoS One. 2018;13(10):e0205696. doi:10.1371/journal.pone.0205696
8. Hug L, Alexander M, You D, Alkema L. National, regional, and global levels and trends in neonatal mortality between 1990 and 2017, with scenario-based projections to 2030: a systematic analysis. Lancet Glob Health. 2019;7(6):e710–e720. doi:10.1016/S2214-109X(19)30163-9
9. Ethiopia. Ethiopia demographic, and health survey, 2016: ICF International, central Statistical Agency. July, 2017.
10. Ethiopian Public Health Institute (EPHI)[Ethiopia] and ICF. Ethiopia mini demographic and health survey 2019: key indicators.
11. Ezbakhe F, Pérez foguet A. Child mortality levels and trends: a new compositional approach. Demogr Res. 2020;43:1263–1296. doi:10.4054/DemRes.2020.43.43
12. Penfold S, Hill Z, Mrisho M, et al. A large cross-sectional community-based study of newborn care practices in Southern Tanzania. PLoS One. 2010;5(12):1–6. doi:10.1371/journal.pone.0015593
13. Bedaso A, Kebede E, Adamu T. Assessment of skin-to-skin contact (SSC) during the postpartum stay and its determinant factors among mothers at public health institutions in Ethiopia. BMC Res Notes. 2019;12(1):1–7. doi:10.1186/s13104-019-4176-5
14. Abebe E, Bekele Z, Kedir Teji BG. The magnitude of early skin-to-skin care practice and associated factors among postnatal women in Harari Region Hospitals, Ethiopia. J Nurs Sci Pract. 2017;8(3). doi:10.37591/jonsp.v8i3.601
15. Ekholuenetale M, Onikan A, Ekholuenetale CE. Prevalence and determinants of mother and newborn skin-to-skin contact in The Gambia: a secondary data analysis. J Egypt Public Health Assoc. 2020;95(1):1–9. doi:10.1186/s42506-020-00050-1
16. Misgna HG, Gebru HB, Birhanu MM. Knowledge, practice and associated factors of essential newborn care at home among mothers in Gulomekada District, Eastern Tigray, Ethiopia, 2014. BMC Pregnancy Childbirth. 2016;16(1):1–8. doi:10.1186/s12884-016-0931-y
17. Saco MC, Coca KP, Marcacine KO, Abuchaim ÉD, Abrão AC. Contato pele a pele e mamada precoce: fatores associados e influência no aleitamento materno exclusivo. Texto contexto enferm. 2019;28(e20180260):1–12.
18. Callaghan-koru JA, Rawlins B, Callaghan-koru JA, et al. Newborn care practices at home and in health facilities in 4 regions of Ethiopia Newborn care practices at home and in health facilities in 4 regions of Ethiopia. BMC Pediatr. 2013;13(198):1–12. doi:10.1186/1471-2431-13-198
19. Hill Z, Tawiah-Agyemang C, Manu A, Okyere EKB, Kirkwood BR. Keeping newborns warm: beliefs, practices and potential for behaviour change in rural Ghana. Trop Med Int Health. 2010;15(10):1118–1124. doi:10.1111/j.1365-3156.2010.02593.x
20. Berhea TA, Belachew AB, Abreha GF, Biemba G. Knowledge and practice of essential newborn care among postnatal mothers in Mekelle City, North Ethiopia: a population-based survey. PLoS One. 2018;13(8):e0202542. doi:10.1371/journal.pone.0202542
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.