Back to Journals » Cancer Management and Research » Volume 17

Skin Metastasis from Cervical Adenocarcinoma with Intrapulmonary Metastasis and Metachronous Ovarian Cancer Responding to Chemotherapy: A Case Report and Review
Authors Sutedja EK ![]() , Sutedja E
, Sutedja E ![]() , Ruchiatan K, Faldian Y
, Ruchiatan K, Faldian Y ![]() , Suwarsa O
, Suwarsa O ![]() , Anandita R
, Anandita R ![]() , Usman HA
, Usman HA ![]() , Ala NMI
, Ala NMI ![]()
Received 7 July 2025
Accepted for publication 2 December 2025
Published 16 December 2025 Volume 2025:17 Pages 3139—3147
DOI https://doi.org/10.2147/CMAR.S550834
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Eva Krishna Sutedja,1 Endang Sutedja,1 Kartika Ruchiatan,1 Yogi Faldian,1 Oki Suwarsa,1 Rafithia Anandita,1 Hermin Aminah Usman,2 Nur Mala Il Ala1
1Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung, Indonesia; 2Department of Anatomical Pathology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Bandung, Indonesia
Correspondence: Eva Krishna Sutedja, Department of Dermatology and Venereology, Faculty of Medicine, Universitas Padjadjaran - Dr. Hasan Sadikin Hospital, Jl. Pasteur 38, Bandung, West Java, 40161, Indonesia, Tel +62222551111, Email [email protected]
Abstract: Skin metastasis, a rare occurrence in cervical cancer, typically signifies advanced systemic disease with a poor prognosis. This case report presents a 55-year-old female with recurrent cervical adenocarcinoma, intrapulmonary metastasis, and metachronous mucinous ovarian cancer who developed skin metastasis. The patient presented with skin-colored and hyperpigmented plaques and papules on the lower abdomen. The histopathological examination of the skin lesion from the patient in this case report revealed subepithelial tumor masses composed of round to oval cells growing hyperplastically in compact clusters, with some forming glandular structures. The nuclei exhibited pleomorphism, ranging from hyperchromatic to vesicular, with clear nucleoli, and mitotic figures were observed. The fibrocollagenous stroma appeared partly edematous, while the skin adnexa, including the sweat and sebaceous glands, remained intact. Immunohistochemical staining for p16 in the skin lesion showed strong positivity in stromal tumor cell infiltrates and negativity in the papillary epithelium, supporting a metastatic origin from cervical adenocarcinoma, confirming the diagnosis of skin metastasis from adenocarcinoma. She was treated with three cycles of paclitaxel and carboplatin chemotherapy, resulting in thinning and a reduction in the size and number of plaques and papules. Despite the positive therapeutic response, the overall prognosis remains poor, and she passed away 16 months after the initial appearance of skin metastasis. This case underscores the importance of routine skin examination in cervical cancer patients, as skin metastasis often correlates with advanced disease and distant organ involvement. Early biopsy and prompt treatment may enhance progression-free survival in such cases.
Keywords: carboplatin, cutaneous malignancy, gynecologic malignancy, paclitaxel, p16 expression
Introduction
Skin metastasis refers to the spread of cancerous cells from a primary internal cancer to the skin and represents a manifestation of advanced systemic disease with poor prognosis.1,2 The presence of skin metastasis often indicates late-stage malignancy and is associated with a high mortality rate.2
Cervical cancer (CC) or carcinoma of the cervix is a cancer that has primary growth in the cervix.3 It remains one of the most prevalent malignancies among women globally, ranking as the fourth most common cancer overall. In Indonesia, CC is the second most common cancer in women and the third leading cause of cancer-related mortality.4
Skin metastasis from gynecologic cancers is rare, with skin involvement from cervical cancer being especially uncommon, even in the late stages of the disease.5 Imachi, et al6 reported that from 1190 cervical cancer patients, only 15 individuals (1.3%) were identified with skin metastasis during the follow-up period through biopsy, surgical specimen, or autopsy. When present, skin metastasis from cervical cancer is frequently accompanied by distant organ involvement, most commonly the lungs.7
The diagnosis of skin metastasis requires clinicopathologic correlation, as clinical manifestations are highly variable.1 Typical lesions appear as firm, painless nodules,7 but may also present as plaques or inflammatory telangiectatic lesions.8,9 The histopathological examination usually resembles the primary tumor.10 The histological subtype of CC has prognostic implications, with adenocarcinoma often demonstrating a more progressive course and poorer outcome.11
Currently, no standardized treatment guidelines exist for skin metastasis secondary to cervical cancer.7,12,13 Therapeutic approaches are largely palliative and include systemic chemotherapy, biological response modifiers, immunotherapy, external beam radiation therapy (EBRT), and electrochemotherapy.12 This case report aims to report a case of skin metastasis from cervical adenocarcinoma with intrapulmonary metastasis and metachronous mucinous ovarian cancer, which showed favorable clinical response to combination chemotherapy with paclitaxel and carboplatin. This case contributes to the limited literature on concurrent secondary malignancies and highlights the therapeutic potential of platinum-taxane regimens in managing skin metastasis form cervical cancer.
Case Report
A 55-year-old Javanese female was referred from the Obstetrics and Gynecology Department at Hasan Sadikin General Hospital with a chief complaint of skin-colored and hyperpigmented plaques and papules on the lower abdomen that were not painful or itchy.
Ten years before consultation, the patient had been diagnosed with stage IIB cervical adenocarcinoma accompanied by ascites. Cytological analysis of the ascitic fluid revealed no malignant cells. She received 25 sessions of external beam radiation and 3 sessions of intracavitary radiation therapy, which resulted in a complete response. Six years before consultation, the patient developed intrapulmonary metastasis and underwent six cycles of combination chemotherapy with paclitaxel and carboplatin. Four years before consultation, the patient presented again with lower abdominal enlargement. Histopathological examination of specimens from both ovaries and adnexa revealed bilateral mucinous carcinoma, while the right fallopian tube was free of malignancy. Based on clinical and pathological findings, she was diagnosed with recurrent cervical adenocarcinoma and stage IIIC mucinous ovarian carcinoma. She underwent suboptimal debulking surgery followed by six additional cycles of paclitaxel and carboplatin chemotherapy. Two years before consultation, the patient developed hematometra secondary to vaginal adhesions, attributed to recurrent cervical adenocarcinoma and stage IIIC mucinous ovarian carcinoma. She was treated with hematometra evacuation. One year before consultation, the patient was diagnosed with pulmonary tuberculosis infection and completed a six-month course of antituberculosis therapy.
Six months before consultation, new skin lesions began to appear as pin-point, skin-colored papules located in the midline of the lower abdomen. Over time, these papules became hyperpigmented, some coalesced into plaques, and gradually increased in both size and number. Four months before consultation, the lesions had extended laterally across the lower abdomen and were accompanied by noticeable lower abdominal enlargement.
The patient experienced menarche at the age of 12, coitarche at 20, and her first pregnancy at 22. She denied a history of smoking, contraceptive use, or HPV vaccination. There were no symptoms suggestive of malignancy in other organs. The patient reported a family history of cervical cancer in her maternal aunt.
On physical examination, there were enlarged cervical lymph nodes and an enlarged lower abdomen. The patient presented with multiple skin-colored and hyperpigmented papules and hyperpigmented plaques with diffuse hyperpigmented macules on the lower abdomen, and the size of the largest lesion was 2.3×0.4 x 0.2 cm. There were some serous crusts and scales on top of some hyperpigmented plaques and papules (Figure 1). Direct microscopic examination with potassium hydroxide 10% from the hyperpigmented macules revealed no fungal element. The histopathological examination of the skin biopsy from the hyperpigmented papule revealed subepithelial tumor masses composed of round to oval cells growing hyperplastically in compact clusters, with some forming glandular structures. The nuclei exhibited pleomorphism, ranging from hyperchromatic to vesicular, with clear nucleoli, and mitotic figures were observed. The fibrocollagenous stroma appeared partly edematous, while the skin adnexa, including the sweat and sebaceous glands, remained intact. (Figure 2A and B). The p16 immunohistochemical examination showed a positive result in tumor cell infiltration in the stroma and negative result in papiliferum, supporting the diagnosis of metastasis from adenocarcinoma (Figure 2C). The hematology examination was within normal limits. Abdomen magnetic resonance imaging (MRI) showed recurrent ovarian mass. Therefore, the patient was diagnosed with skin metastasis of cervical adenocarcinoma on the lower abdomen, recurrent cervical adenocarcinoma, and recurrent mucinous ovarian mass.
 |
Figure 1 Clinical manifestation showed multiple skin-colored and hyperpigmented papules and hyperpigmented plaques with diffuse hyperpigmented macules on the base. There were some serous crusts and scales on top of some hyperpigmented plaques and papules: before the chemotherapy (A) and one month after the third cycle of paclitaxel-carboplatin chemotherapy (B). |
 |
Figure 2 Histological findings from the hyperpigmented papule revealed subepithelial tumor mass consisting of round oval cells that grow hyperplastically, compacted in groups, with a small part forming glandular structures (H&E staining, 10x) (A). There are mitosis cell ans the cell nuclei were pleomorphic (yellow arrow), partly hyperchromatic, partly vesicular with clear nucleoli (H&E staining, 100x) (B). The p16 immunohistochemical examination showed positive result in tumor cell infiltration in the stroma that support the diagnosis of metastasis of adenocarcinoma (p16 staining, 100x)(C). |
The patient was treated with three cycles of paclitaxel and carboplatin chemotherapy. The plaques and papules became thinner and decreased in size and number after one cycle of chemotherapy, with continued improvement within one month following the third cycle (Figure 1). The largest lesion reduced from 2.3×0.4 x 0.2 cm cm before treatment to 0.5×0.2 x 0.2 cm after one month following the third cycle of chemotherapy. The patient complained of nausea after every cycle of therapy, which subsided three days after the chemotherapy. Laboratory examination showed low hemoglobin and leukocyte levels after the last cycle of chemotherapy. Then the patient was treated with hematometra evacuation and another six cycles of paclitaxel and carboplatin chemotherapy, but the patient did not return for follow-up to Dermatology and Venereology Department. Unfortunately, the patient passed away due to respiratory distress, one month after the fifth cycle of chemotherapy or 16 months after the first skin lesion appeared.
Discussion
Skin metastasis from internal malignancies is very rare with incidence ranging from 0.7% to 10%.14 It typically occurs in the advanced stages of internal cancers, spreading through hematogenous dissemination, lymphatic dissemination, direct invasion, or surgical implantation.15 In women, the most frequent primary cancers that lead to skin metastasis were breast cancer (69%), colorectal carcinoma (9%), melanoma (5%), and ovarian carcinoma (4%).2 Skin metastasis from CC is very rare, ranging from 0.1% to 2% of all reported events and the prognosis is typically unfavorable.5,7,12
According to GLOBOCAN 2020, there were an estimated 604,000 new cases of CC worldwide, leading to 342,000 deaths each year.4 In Indonesia, CC accounted for 17.2% of cancer cases and 8.8% of cancer-related deaths among women in 2018.16 According to data from the Indonesian Society of Gynecologic Oncology, histopathologically, the majority of cases were epidermoid carcinoma (59%), followed by adenosquamous carcinoma, and adenocarcinoma.17 The patient in this case was diagnosed with cervical adenocarcinoma, the third most common histologic type of CC in Indonesia.
Invasive CC extends directly to nearby structures such as the parametrium, vagina, uterus, and adjacent organs like the bladder and rectum. It also spreads through lymphatic dissemination to regional lymph nodes. Distant metastasis to the lungs, liver, and bones by the hematogenous dissemination typically occurs in the later stages.3 The anatomical regions affected by skin metastasis and the findings of tumor cells in lymphatic spaces suggest a lymphatic spread. Thus, it is thought to occur due to retrograde tumor spread secondary to lymphatic obstruction in most cases.18 However, several cases have been reported to develop at the sites of previous skin injuries, surgical incisions, drains, or radiation therapy needle insertions, raising the possibility of direct tumor cell implantation.5,19–23 Skin metastasis from cervical cancer is often associated with metastasis in other organs, with the lungs being the most commonly affected,7 which was also observed in this patient.
The time frame for the development of skin metastasis following cervical cancer treatment varies significantly. It can occur even before therapy is fully completed,12 while in some cases, it may take over a decade to manifest.24 The patient in this case report first presented with skin metastasis nine years after her initial cervical adenocarcinoma diagnosis and five years after she was diagnosed with intrapulmonary metastasis.
Skin metastasis from CC tends to affect the lower abdomen, vulva, lower extremities, and anterior chest wall more frequently. Typically, cutaneous lesions present as painless nodules,7 but can also appear as plaques or inflammatory telangiectatic lesions.8,9 The lesions may be single or multiple.12 In 2019, Katiyar, et al9 reported a case of skin metastasis as pearly hyperpigmented, dry papules on the lower abdomen and thighs in a patient with asymptomatic local recurrence of adenosquamous cervical carcinoma. The skin biopsy showed a poorly differentiated tumor similar to the previous cervical primary carcinoma. The patient received chemotherapy, and the skin lesion was completely resolved. The cutaneous lesions in our patient presented as asymptomatic, with multiple skin-colored and hyperpigmented papules and plaques with crust and scales on the lower abdomen, which are rare.
Based on the histopathological examinations, the World Health Organization Classification of Female Genital Tumours classified cervical cancer as squamous epithelial tumors (squamous cell carcinoma with HPV-associated, HPV-independent, or not otherwise specified/NOS), glandular tumors (adenocarcinoma NOS, HPV-associated, HPV-independent gastric type, HPV-independent clear cell type, HPV-independent mesonephric type, HPV-independent NOS, endometrioid adenocarcinoma NOS, carcinosarcoma NOS, adenosquamous carcinoma, mucoepidermoid carcinoma, adenoid basal carcinoma, and carcinoma undifferentiated NOS), mixed epithelial and mesenchymal tumors (adenosarcoma), and germ cell tumors (endodermal sinus tumor, yolk sac tumor NOS, and choriocarcinoma NOS).25 The incidence of skin metastasis is higher in adenocarcinoma compared to squamous cell carcinoma.6 It remains uncertain whether adenocarcinoma predicts a greater likelihood of distant metastasis.26 The patient, in this case report, also was diagnosed with cervical adenocarcinoma with skin metastasis and had intrapulmonary metastasis as the distant metastasis.
The reported incidence of secondary primary malignancy ranges from 1.33% to 5.8%.27 The two tumors can be diagnosed simultaneously (synchronous) or more than six months afterward (metachronous).28 The cases of cervical and ovarian cancer that occur in one patient have been rarely reported.29 Matsuo, et al30 reported that 0.3% of stage I cervical cancer patients developed metachronous ovarian cancer during approximately 10 years of follow-up. The median time to develop metachronous ovarian cancer was 5.4 years. Patients with adenocarcinoma or adenosquamous cervical carcinoma had a significantly higher risk of developing metachronous ovarian cancer. The patient in this case was diagnosed with metachronous mucinous ovarian carcinoma six years after the first initial cervical adenocarcinoma diagnosis.
Ovarian cancer is the second most prevalent gynecological cancer and has the highest mortality rate.31 Mucinous ovarian cancer (MOC) is a rare subtype of epithelial ovarian carcinoma.32 Skin metastasis from ovarian cancer are also uncommon with the incidence ranging from 0.9% to 5.8%. It can occur as nodules in the umbilicus (Sister Joseph nodules/SJN) or non-SJN metastasis that can occur in the abdominal wall, groin, external genitalia, and chest wall.33 Non-SJN metastasis may present as a cutaneous nodule, cicatricial plaque, multiple small papules, and inflammatory metastasis as pitting edema with erythematous skin that resembles lymphangitis and cellulitis.2,34 However, skin metastasis from the mucinous ovarian carcinoma have not been reported.33
The histopathological examination of skin metastasis is similar to the primary tumor.10 The histopathological examination of the skin lesion from the patient in this case report revealed subepithelial tumor masses composed of round to oval cells growing hyperplastically in compact clusters, with some forming glandular structures. The nuclei exhibited pleomorphism, ranging from hyperchromatic to vesicular, with clear nucleoli, and mitotic figures were observed. The fibrocollagenous stroma appeared partly edematous, while the skin adnexa, including the sweat and sebaceous glands, remained intact. These findings closely resemble the histopathologic characteristic of cervical adenocarcinoma.35 In contrast, mucinous ovarian cancer typically demonstrates multilocular cysts, structures lined by mucin-containing columnar epithelium, showing proliferation of anaplastic cells with pleomorphic nuclei, coarse chromatin, and areas of acinar or papillary formation, features that were not present in this case.36
The additional p16 examination demonstrates oncogenic activity in cervical carcinoma cell lines and is closely linked to the grade of cervical intraepithelial neoplasia, as well as the prognosis of cervical cancer.37,38 Immunohistochemical staining for p16 in the skin lesion showed strong positivity in stromal tumor cell infiltrates and negativity in the papillary epithelium, supporting a metastatic origin from cervical adenocarcinoma. Although additional immunohistochemical markers such as CK7, CK20, PAX8, ER, PR, or HPV RNA ISH were not available due to resource limitations, the overall clinicopathologic correlation strongly supports the diagnosis of skin metastasis from cervical adenocarcinoma.
Skin metastasis is often indicative of a pre-terminal stage and is commonly associated with local recurrence and distant metastasis, leading the focus of treatment becomes palliative. Currently, there is no established effective treatment, and no clear guidelines exist for managing skin metastasis.7,12,13 Available treatment options include chemotherapy, biological response modifiers, immunotherapy, EBRT, and electrochemotherapy.12 The treatment choice is influenced by several factors, such as the patient’s general condition, symptoms, visceral involvement, and financial circumstances. Most patients underwent palliative chemotherapy, with taxane-platinum (TC) combinations being commonly used.7 Cis-platinum alone is the most effective single agent for symptom management and paclitaxel has also been demonstrated to induce a complete response.5,39 This combination has also been studied as cervical cancer chemotherapy and ovarian cancer adjuvant therapy.40,41 If the patient’s condition is favorable, palliative chemotherapy using a single-agent cisplatin or a combination of cisplatin and paclitaxel may be considered to enhance progression-free survival.42
Paclitaxel is a broad-spectrum anticancer agent primarily derived from the bark of the yew tree Taxus brevifolia Nutt. It belongs to the class of diterpene taxanes and is one of the most commonly used chemotherapeutic agents for treating various types of cancer. Paclitaxel works as an anticancer drug by stabilizing microtubules, preventing their disassembly, and disrupting cell division. It also induces apoptosis through activation of p53 and Raf-1 and reduces tumor angiogenesis.43 Paclitaxel was administered at a dose of 175 mg/m2 (234.5 mg) and administered by intravenous (IV) infusion over 3 hours.41 Carboplatin is a main platinum-based antitumor drug. It binds with deoxyribonucleic acid (DNA), blocking replication and transcription, leading to cell death and triggering apoptosis.44,45 Carboplatin was given with the dosage of 5 area under the curve (AUC) and administered by IV infusion over 30 to 60 minutes.41
The TC regimen is expected to cause acute emesis in 30% to 90% of patients. It can also cause anemia, leukopenia, neutropenia, and thrombocytopenia, as well as hepatotoxicity and nephrotoxicity.41 The patient was treated with three cycles of paclitaxel and carboplatin chemotherapy. Progressive improvement was observed, as the plaques and papules became thinner and smaller after one cycle of chemotherapy, with further reduction within one month after the third cycle. The largest lesion decreased in size from 2.3×0.4 x 0.2 cm cm before treatment to 0.5×0.2 x 0.2 cm after one month following the third cycle of chemotherapy. The patient complained of nausea after each chemotherapy cycle, which subsided three days post-treatment. Laboratory examination showed low hemoglobin and leukocyte levels after the final cycle.
The prognosis for cervical adenocarcinoma with skin metastasis is generally poor, with a median survival of 12 months and survival for more than 1 year seen in only 20% of patients. Furthermore, cervical adenocarcinoma is associated with a higher mortality rate than squamous cell carcinoma.7,11,12 In this case report, the patient passed away 16 months after the first lesion of skin metastasis appeared, confirming that skin metastasis signifies advanced systemic disease with a poor prognosis and chemotherapy may offer temporary clinical improvement.
Given the rarity of skin metastasis in cervical adenocarcinoma, a literature review was performed to compare previously reported cases over the period of 2015–2025 with the present patient (Table 1). Compared to previous reports, the present case is unique for its concurrent mucinous ovarian carcinoma and pulmonary metastasis, along with a favorable cutaneous response following paclitaxel–carboplatin chemotherapy.
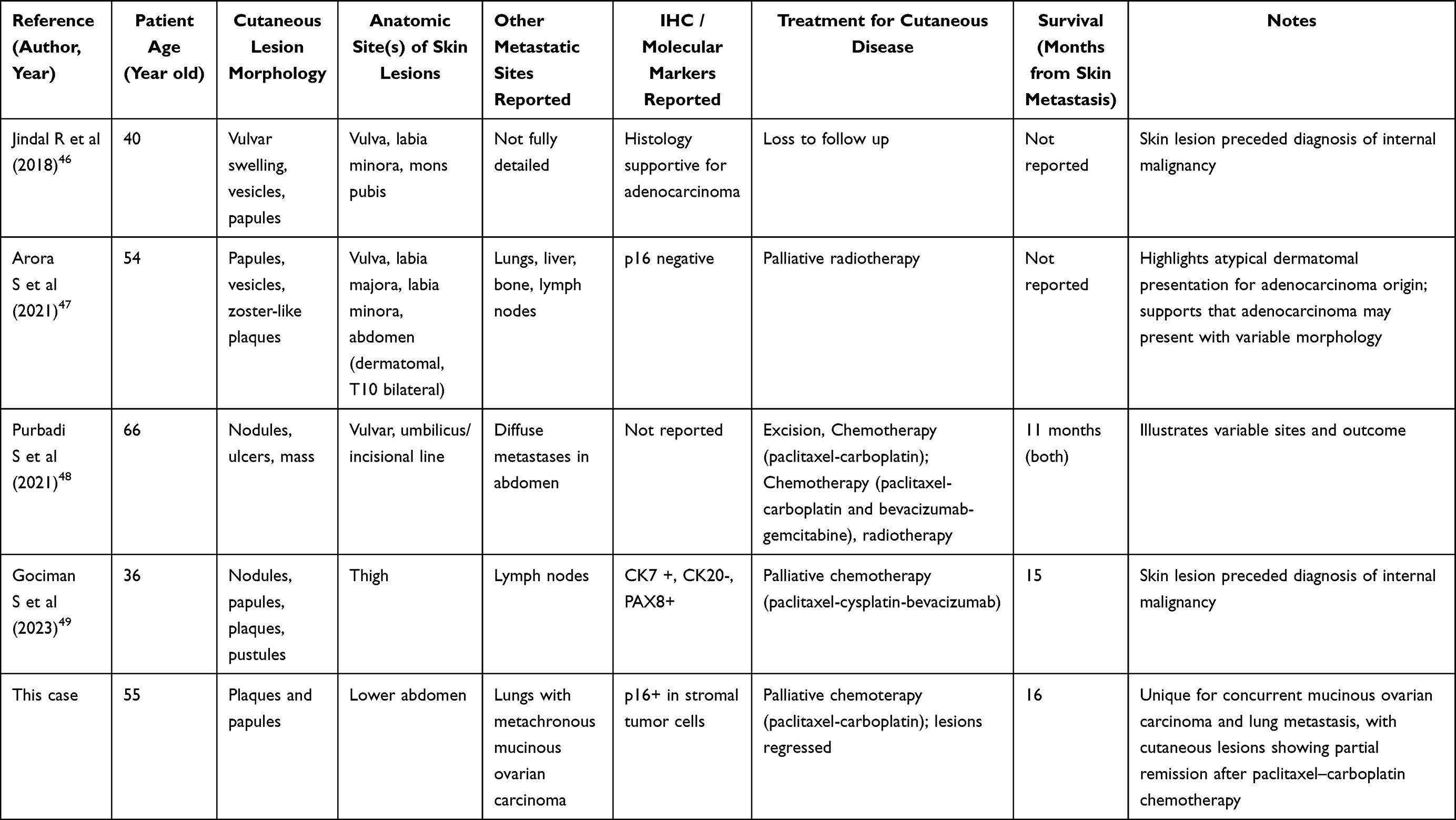 |
Table 1 Summary of Reported Cases of Skin Metastasis From Cervical Adenocarcinoma (2015–2025) |
Conclusion
In conclusion, although skin metastasis from cervical cancer is uncommon, a comprehensive skin examination should be conducted during routine visits for all patients. Any sudden skin lesions in patients with cervical cancer should prompt immediate biopsy to exclude metastasis, as it is often linked to advanced disease and organ metastasis. While there are no established guidelines for the treatment of skin metastasis in cervical cancer, systemic chemotherapy using paclitaxel-carboplatin regimen may offer temporary clinical improvement. This case report demonstrates a case of skin metastasis from cervical adenocarcinoma with recurrent cervical adenocarcinoma, recurrent mucinous ovarian cancer, and intrapulmonary metastasis which responded to combination chemotherapy with paclitaxel and carboplatin.
Abbreviations
AUC, area under the curve; CC, cervical cancer; DNA, deoxyribonucleic acid; EBRT, external beam radiation therapy; HPV, human papillomavirus; IV, intravenous; MOC, mucinous ovarian cancer; MRI, magnetic resonance imaging; NOS, not otherwise specified; SJN, Sister Joseph nodules; TC, taxane-platinum.
Ethics Statement
The publication of images was included in the patient’s consent for the publication of the case. Institutional approval was obtained to publish the case details from Dr. Hasan Sadikin Hospital Ethical Committee with ethical approval number DP.04.03/D.XIV.6.5/167/2025.
Consent Statement
The authors certify that they have obtained all appropriate patient consent forms. The patient signed a consent form for the publication of the case details and images during the course of her treatment. Following her death, we also obtained additional consent from her next of kin to ensure ethical compliance and respect for the patient’s legacy.
Acknowledgments
The authors would like to thank the patients, the staff of the Dermatology and Venereology Department and the Department of Anatomical Pathology, Faculty of Medicine, Universitas Padjadjaran – Dr. Hasan Sadikin General Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hussein MR. Skin metastasis: a pathologist’s perspective. J Cutan Pathol. 2010;37(9):e1–e20. doi:10.1111/j.1600-0560.2009.01469.x
2. Brownstein MH, Helwig EB. Patterns of cutaneous metastasis. Arch Dermatol. 1972;105(6):862. doi:10.1001/archderm.1972.01620090034008
3. Bhatla N, Aoki D, Sharma DN, et al. Cancer of the cervix uteri: 2021 update. Int J Gynecol Obstet. 2021;155(Suppl 1):28–44. doi:10.1002/ijgo.13865
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Behtash N, Ghaemmaghami F, Yarandi F, et al. Cutaneous metastasis from carcinoma of the cervix at the drain site. Gynecol Oncol. 2002;85(1):209–211. doi:10.1006/gyno.2001.6559
6. Imachi M, Tsukamoto N, Kinoshita S, et al. Skin metastasis from carcinoma of the uterine cervix. Gynecol Oncol. 1993;48(3):349–354. doi:10.1006/gyno.1993.1061
7. Mahapatra BR, Muraleedharan A, Badajena A, et al. Cutaneous metastasis in a treated case of cervical cancer with extraordinary response to chemotherapy: a case report of a rare event and review of the literature. Cureus. 2023;15(2):e35083. doi:10.7759/cureus.35083
8. Raj S, Kakkar N, Agrawal P, et al. Carcinoma cervix de novo with widespread cutaneous/subcutaneous metastasis: a rare case report. J Cancer Res Ther. 2019;15(6):1405. doi:10.4103/jcrt.JCRT_774_17
9. Katiyar V, Araujo T, Majeed N, et al. Multiple recurrences from cervical cancer presenting as skin metastasis of different morphologies. Gynecol Oncol Rep. 2019;28:61–64. doi:10.1016/j.gore.2019.02.008
10. Mandrekas DP, Dimopoulos AM, Moulopoulou D, et al. Distant cutaneous metastasis from carcinoma of the uterus. A case report. Eur J Gynaecol Oncol. 1999;20(3):212.
11. Galic V, Herzog TJ, Lewin SN, et al. Prognostic significance of adenocarcinoma histology in women with cervical cancer. Gynecol Oncol. 2012;125(2):287–291. doi:10.1016/j.ygyno.2012.01.012
12. Benoulaid M, Elkacemi H, Bourhafour I, et al. Skin metastases of cervical cancer: two case reports and review of the literature. J Med Case Rep. 2016;10(1):265. doi:10.1186/s13256-016-1042-0
13. Alrefaie S, Alshamrani H, Abduljabbar M, et al. Skin metastasis from squamous cell carcinoma of the cervix to the lower extremities: case report and review of the literature. J Fam Med Prim Care. 2019;8(10):3443–3446. doi:10.4103/jfmpc.jfmpc_541_19
14. Sariya D, Ruth K, Adams-McDonnell R, et al. Clinicopathologic correlation of cutaneous metastases: experience from a cancer center. Arch Dermatol. 2007;143(5):613–620. doi:10.1001/archderm.143.5.613
15. Lehman JS, Benacci JC. Cutaneous metastasis of invasive ductal carcinoma of the breast to an infusaport site. Cutis. 2008;81(3):223–226.
16. World Health Organization (WHO). Indonesia Fact Sheets: GLOBOCAN 2019. Int Agency Res Cancer Globocan. 2019;256:2018–2019.
17. Indonesian Society of Gynecologic Oncology (INASGO). National data report 2021. Jakarta: INASGO; 2021.
18. Burbano J, Salazar-González A, Echeverri C, et al. Cutaneous lymphangitic carcinomatosis: a rare metastasis from cervical cancer. Gynecol Oncol Rep. 2018;26(18):1–3. doi:10.1016/j.gore.2018.07.006
19. Pertzborn S, Buekers TE, Sood AK. Hematogenous skin metastases from cervical cancer at primary presentation. Gynecol Oncol. 2000;76(3):416–417. doi:10.1006/gyno.1999.5704
20. Srivastava K, Singh S, Srivastava M, Srivastava AN. Incisional skin metastasis of a squamous cell cervical carcinoma 3.5 years after radical treatment – a case report. Int J Gynecol Cancer. 2005;15(6):1183–1186. doi:10.1111/j.1525-1438.2005.00173.x
21. Yamashita H, Okuma K, Nakagawa K. Iatrogenic vulvar skin metastases after interstitial radiotherapy for recurrent cervical cancer. J Dermatol. 2009;36(12):663–665. doi:10.1111/j.1346-8138.2009.00729.x
22. Ozmen B, Sükür YE, Atabekoğlu C, Güngör M. Prolonged survival (>48 months) in a squamous cell carcinoma of the cervix after late skin metastasis (>5 year) to incision site: a case report. J Turk Ger Gynecol Assoc. 2009;10(3):175–177.
23. Basu B, Mukherjee S. Cutaneous metastasis in cancer of the uterine cervix: a case report and review of the literature. J Turk Ger Gynecol Assoc. 2013;14(3):174–177. doi:10.5152/jtgga.2013.62444
24. Khurana R, Singh S. Isolated cutaneous metastasis to thigh from cancer cervix – fourteen years after curative radiotherapy. Int J Gynaecol Obstet. 2008;11(1):1–3.
25. International Agency for Research on Cancer (IARC). WHO Classification of Female Genital Tumours.
26. Vinh-Hung V, Bourgain C, Vlastos G, et al. Prognostic value of histopathology and trends in cervical cancer: a SEER population study. BMC Cancer. 2007;7(1):164. doi:10.1186/1471-2407-7-164
27. Pan SY, Huang CP, Chen WC. Synchronous/metachronous multiple primary malignancies: review of associated risk factors. Diagnostics. 2022;12(8):1940. doi:10.3390/diagnostics12081940
28. Coyte A, Morrison DS, McLoone P. Second primary cancer risk – the impact of applying different definitions of multiple primaries: results from a retrospective population-based cancer registry study. BMC Cancer. 2014;14(1):272. doi:10.1186/1471-2407-14-272
29. Bacalbasa N, Balescu IC, Diaconu C, et al. Synchronous cervical adenocarcinoma and ovarian serous adenocarcinoma: a case report and literature review. Medicina. 2020;56(4):152. doi:10.3390/medicina56040152
30. Matsuo K, Machida H, Horowitz MP, et al. Risk of metachronous ovarian cancer after ovarian conservation in young women with stage I cervical cancer. Am J Obstet Gynecol. 2017;217(5):
31. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2019. CA Cancer J Clin. 2019;69(1):7–34. doi:10.3322/caac.21551
32. Seidman JD, Kurman RJ, Ronnett BM. Primary and metastatic mucinous adenocarcinomas in the ovaries: incidence in routine practice with a new approach to improve intraoperative diagnosis. Am J Surg Pathol. 2003;27(7):985–993. doi:10.1097/00000478-200307000-00014
33. Otsuka I. Cutaneous metastases in ovarian cancer. Cancers. 2019;11(9):1292. doi:10.3390/cancers11091292
34. Patsner B, Mann WJ, Chumas J, et al. Herpetiform cutaneous metastases following negative second look laparotomy for ovarian adenocarcinoma. Arch Gynecol Obstet. 1988;244(1):63–67. doi:10.1007/BF00931405
35. Stolnicu S, Park KJ, Kiyokawa T, et al. Tumor typing of endocervical adenocarcinoma: contemporary review and recommendations from the international society of gynecological pathologists. Int J Gynecol Pathol. 2021;40(Suppl 1):S75–S91. doi:10.1097/PGP.0000000000000751
36. Rahmalia K, Sudiarta KE, Setianingsih H, et al. The characteristics of sociodemography, histopathologic features, stage, and management of ovarian cancer in Dr. Ramelan Navy Hospital Surabaya. Indonesian J Cancer. 2024;18(2):131–137. doi:10.33371/ijoc.v18i2.1050
37. Huang K, Li LA, Meng YG, et al. p16 expression in patients with cervical cancer and its prognostic significance: meta-analysis of published literature. Eur J Obstet Gynecol Reprod Biol. 2014;183:64–69. doi:10.1016/j.ejogrb.2014.10.016
38. Liao GD, Sellors JW, Sun HK, et al. p16 INK4A immunohistochemical staining and predictive value for progression of cervical intraepithelial neoplasia grade 1: a prospective study in China. Int J Cancer. 2013;134(7):1715–1724. doi:10.1002/ijc.28485
39. Palaia I, Angioli R, Cutillo G, et al. Skin relapse from cervical cancer. Gynecol Oncol. 2002;87(1):155–156. doi:10.1006/gyno.2002.6808
40. Tinker AV, Bhagat K, Swenerton KD, et al. Carboplatin and paclitaxel for advanced and recurrent cervical carcinoma: the British Columbia cancer agency experience. Gynecol Oncol. 2005;98(1):54–58. doi:10.1016/j.ygyno.2005.03.037
41. Akin JM, Waddell JA, Solimando DA. Paclitaxel and Carboplatin (TC) regimen for ovarian cancer. Hosp Pharm. 2014;49(5):425–431. doi:10.1310/hpj4905-425
42. Moore DH, Blessing JA, McQuellon RP, et al. Phase III study of cisplatin with or without paclitaxel in stage IVB, recurrent, or persistent squamous cell carcinoma of the cervix: a gynecologic oncology group study. J Clin Oncol. 2004;22(15):3113–3119. doi:10.1200/JCO.2004.04.170
43. Sharifi-Rad J, Quispe C, Patra JK, et al. Paclitaxel: application in modern oncology and nanomedicine-based cancer therapy. Oxid Med Cell Longev. 2021;2021(1):3687700. doi:10.1155/2021/3687700
44. Brabec V, Kasparkova J. Modifications of DNA by platinum complexes. Relation to resistance of tumors to platinum antitumor drugs. Drug Resist Updat. 2005;8(3):131–146. doi:10.1016/j.drup.2005.04.006
45. Hah SS, Stivers KM, De Vere WRW, et al. Kinetics of carboplatin-DNA binding in genomic DNA and bladder cancer cells as determined by accelerator mass spectrometry. Chem Res Toxicol. 2006;19(5):622–626. doi:10.1021/tx060058c
46. Jindal R, Mittal A, Shirazi N, et al. Cutaneous metastasis from adenocarcinoma of cervix: a rare case report. Int J Res Dermatol. 2018;4(2):259–261. doi:10.18203/issn.2455-4529.IntJResDermatol20181831
47. Arora S, Dabas R, Ranjan E, et al. Cutaneous metastases in a case of adenocarcinoma cervix with atypical presentation. Indian J Dermatopathol Diagn Dermatol. 2021;8(1):17–19. doi:10.4103/ijdpdd.ijdpdd_76_20
48. Purbadi S, Rustamadji P, Purwoto G, et al. Skin metastases originated from cervical cancer: a rare case report. Ann Med Surg. 2021;66:102363. doi:10.1016/j.amsu.2021.102363
49. Gociman S, Florell SR, Clarke JT. Cutaneous metastasis as a first sign of adenocarcinoma of the cervix. Dermatol Online J. 2023;29(5). doi:10.5070/D329562409
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Outcome and Safety of the TCX Regimen for Advanced Gastric Cancer: A Prospective Cohort Study
Nguyen HT, Do KH, Le NB, Tran T
Cancer Management and Research 2022, 14:2825-2837
Published Date: 19 September 2022