Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Sinonasal Symptoms in COPD: Burden and Associations with Clinical Markers of Disease
Authors Øie MR ![]() , Helvik AS
, Helvik AS ![]() , Sue-Chu M
, Sue-Chu M ![]() , Steinsvåg SK, Thorstensen WM
, Steinsvåg SK, Thorstensen WM
Received 1 May 2022
Accepted for publication 22 August 2022
Published 7 September 2022 Volume 2022:17 Pages 2137—2147
DOI https://doi.org/10.2147/COPD.S372991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Marte Rystad Øie,1,2 Anne-Sofie Helvik,1,3 Malcolm Sue-Chu,4,5 Sverre Karmhus Steinsvåg,6,7 Wenche Moe Thorstensen1,2
1Department of Otolaryngology, Head and Neck Surgery, St. Olavs hospital, 7006 Trondheim University Hospital, Trondheim, Norway; 2Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology (NTNU), Trondheim, Norway; 3Department of Public Health and Nursing, Norwegian University of Science and Technology, Trondheim, Norway; 4Department of Circulation and Medical Imaging, Norwegian University of Science and Technology, Trondheim, Norway; 5Department of Thoracic Medicine, St. Olavs hospital, Trondheim University Hospital, Trondheim, Norway; 6Department of Otolaryngology, Head and Neck Surgery, Sørlandet Hospital, Kristiansand, 4604, Norway; 7Haukeland University Hospital, Bergen, Norway
Correspondence: Marte Rystad Øie, Department of Otolaryngology, Head and Neck Surgery, St. Olavs hospital, Trondheim University Hospital, 3250 Torgarden, Trondheim, NO-7006, Norway, Tel +47 926 42 329, Email [email protected]; [email protected]
Purpose: Sinonasal symptoms are prevalent in COPD, and knowledge of the relationship between these symptoms and clinical markers of COPD is limited. This study explores the associations between the burden of sinonasal symptoms and clinical markers and thresholds recommended for guiding treatment decisions in the GOLD guidelines.
Patients and Methods: Sinonasal symptoms were quantified with the rhinological subscale of the Sino-Nasal-Outcome-Test (SNOT-22) in 93 COPD patients characterized by the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) 2012 diagnostic criteria for rhinosinusitis without nasal polyps (RSsNP). Associations between a high burden, defined as a SNOT22_rhinological score of ≥ 11, and the following markers were assessed by adjusted multivariable linear regressions; severity of dyspnea [modified Medical Research Council (mMRC)] and cough [Visual Analogue Scale (VAS)], physical activity [6-minute walking distance (6MWD)], mortality risk (BODE index), and HRQoL [disease-specific COPD Assessment Test (CAT) and St. Georges Respiratory Questionnaire (SGRQ), and physical component summary, Short Form-36 version 2.0 (PCS SF-36v2)]. Odds ratios for the association of a high burden and threshold levels for regular treatment were estimated by adjusted binomial logistic regression models.
Results: A high burden was associated with greater severity of dyspnea and cough, lower 6MWD, higher BODE index and poorer HRQoL. The odds ratio of having CAT and SGRQ scores that are above the thresholds recommended for treatment was 5– 7-fold greater in the high burden group.
Conclusion: A high burden of sinonasal symptoms is positively associated with the clinical markers of symptom severity and mortality risk and is inversely associated with physical activity and HRQoL in COPD. These findings add further support that the UAD concept also applies to COPD. Enquiry about sinonasal symptoms in COPD patients should be incorporated into the clinical routine.
Keywords: united airways disease, chronic nasal symptoms, rhinosinusitis, HRQoL
Corrigendum for this paper has been published.
Introduction
Asthma, COPD, rhinitis and rhinosinusitis (RS) are chronic diseases of the respiratory tract with an estimated global prevalence of about 12%.1 Of these, COPD is the most prevalent and is characterized by symptoms, such as dyspnea initially on exertion, cough and sputum production, irreversible airflow limitation and acute exacerbations.2 In the 2022 GOLD report for COPD,3 clinical assessment of the disease is based on the frequency of acute exacerbations and the severity of airflow limitation and symptoms. The modified British Medical Research Council (mMRC) scale for dyspnea and the COPD assessment test (CAT) are specified as the clinical markers of symptom severity, and health-related quality of life (HRQoL) is assessed with the St. Georges Respiratory Questionnaire (SGRQ). Moreover, cut-points of ≥2, 10 and 25 for the mMRC dyspnea, CAT and SGRQ scores, respectively, have been recommended as thresholds for guiding treatment decisions.3 Additional clinical markers are the six-minute walking distance (6MWD) for physical activity and the BODE index, which is a composite index of the Body-mass index, airflow Obstruction, Dyspnea, and Exercise, for mortality risk.4
The concept of united airways diseases (UAD) was formulated on the initial observation of the coexistence of allergic rhinitis and chronic rhinosinusitis with asthma.5 Moreover, there is increasing evidence that the UAD concept also applies to other chronic diseases of the respiratory tract, such as COPD, bronchiectasis, cystic fibrosis, and nasal polyps.6 For COPD, the reported prevalence of sinonasal symptoms is 40–88%7–10 and the prevalence of rhinosinusitis without nasal polyps (RSsNP) is 3-fold greater than in controls.11 Associations with upper airway symptoms,8,10,12,13 rhinitis14 and chronic rhinosinusitis with and without nasal polyps have been observed,11,15,16 and the latter is associated with poorer HRQoL.17 However, knowledge about the relationships between sinonasal symptoms and clinical markers and thresholds for guiding treatment decisions is limited.
Thus, the aims of the present study were to explore the associations between the burden of sinonasal symptoms in COPD patients who are well characterized for RSsNP and clinical markers for COPD, such as the severity of symptoms, physical activity, mortality risk and HRQoL, and the recommended thresholds for guiding treatment decisions of the disease.
Materials and Methods
Study Participants
One hundred and three participants with a COPD diagnosis were recruited for the study from February 2016 to December 2017 at St. Olavs hospital, Trondheim University Hospital, Norway.11 All participants were between 40 and 80 years of age and did not have a history of upper- or lower respiratory tract infection within the previous two weeks, acute exacerbation of COPD within the previous six weeks, long-term oxygen therapy or current radio-chemotherapy, physician-diagnosed asthma, previous sinonasal surgery or underlying systemic diseases that could affect the nose, such as sarcoidosis, granulomatous polyangiitis, cystic fibrosis, and primary ciliary dyskinesia. Thirteen patients with reversibility of more than 200 mL and a 12% increase from baseline FEV1 after β2-agonist, restrictive spirometry or nasal polyps on endoscopy were excluded from the study. Of the final sample of 90 patients with COPD, RSsNP was diagnosed in 46 patients (Figure 1). Informed consent was obtained from all participants, approval was granted by the Regional Committee for Medical and Health Research Ethics, Central Norway, REC (reference number 2015/2017) and investigations were performed in accordance with the principles of the Declaration of Helsinki/Hong Kong.
 |
Figure 1 Flow chart of the study participants and the subjects excluded. Abbreviations: EPOS, European Position Paper on Rhinosinusitis and Nasal Polyps (2012); RSsNP, Rhinosinusitis sin Nasal Polyps. |
Measurements
Self-administered questionnaires were used to collect data on smoking habits and symptoms of allergies affecting the airways, symptoms from the upper airway [Sinonasal Outcome Test-22 (SNOT-22)] and generic [Short Form-36 version 2.0 (SF-36v2)] and disease-specific HRQoL (CAT, SGRQ). Height, weight, spirometry with reversibility test and skin-prick test were recorded by trained research nurses. An ENT examination with nasal endoscopy was performed by one of three otolaryngologists (M.R.Ø, S.B.D and W.M.T). Details on these measurements have been described previously.11 The grade of dyspnea (mMRC), severity of cough [Visual Analogue Scale (VAS)] and 6MWD were also recorded.
Diagnostic Criteria
The clinical diagnosis of RSsNP was made post-inclusion on the presence of the symptomatic criteria and a positive nasal endoscopy as outlined in the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS 2012).18 The symptomatic criteria for RS are defined as the presence of two or more sinonasal symptoms, one of which should be nasal obstruction and/or nasal discharge, and decreased sense of smell or facial pain/pressure. A positive nasal endoscopy is defined as the uni- or bilateral presence of oedema and/or mucopurulent discharge in the middle nasal cavity. The diagnosis of COPD was confirmed by the presence of irreversible airflow obstruction, defined as a post-bronchodilator FEV1/FVC ratio of <0.7.19 Severity of airflow obstruction was graded according to the GOLD criteria.3 Allergic rhinitis was defined as the presence of symptoms of rhinoconjunctivitis on exposure to the specific allergen(s) with a positive skin prick test.20
Sinonasal Symptoms
The SNOT-22 incorporates 22 items on nasal and non-nasal symptoms and is the most widely accepted patient-reported outcome measure of sinonasal disease.21 A rhinological subscale of the SNOT-22 (SNOT22_rhinological score) was constructed by summation of the responses to items 1–5 (need to blow nose, sneezing, runny nose, nasal obstruction, loss of taste and smell), and items 7 and 8 (post-nasal discharge and thick nasal discharge). The response to each item was scored on a Likert scale from 0 to 5, with 0 indicating “no problem” and 5 indicating “problem as bad as it could be”. The subscale has a range from 0 to 35 and has been validated for the measurement of the burden of sinonasal symptoms.21–23
Clinical Markers in COPD
Symptom Severity
Dyspnea was graded using the mMRC 5-point scale from “none” (grade 0) to “almost complete incapacity” (grade 4).24 Cough severity was measured on a VAS from 0 (cough not troublesome) to 100 mm (cough worst thinkable troublesome).25
Physical Activity
The 6MWD was measured in accordance with the standard protocol with modifications.26 The latter were a shorter walking lap of 50 m instead of 60 m and the Borgs scale for dyspnea and fatigue was not recorded. Participants rested for 10 min before the test and then followed a straight corridor with a length of 25 m which was marked every 5 m. The turnaround points were set up with a red cone, and the distance walked in 6 minutes was recorded. Standardized phrases of encouragement were given during the test.
Mortality Risk
The BODE index is a composite score from BMI, FEV1% predicted post-bronchodilator, severity of dyspnea (mMRC) and exercise capacity (6MWD) and has a range from 0 to 10.27 A high score indicates a higher risk of death from any cause.27
HRQoL
Disease-specific HRQoL for COPD was measured by the CAT and the SGRQ questionnaires. The range of the total score is from 0 to 40 for the former and from 0 to 100 for the latter questionnaire, and high scores are indicative of poorer HRQoL.28
Generic HRQoL was assessed by the SF-36v2.29 The physical component summary (PCS) measures self-perceived physical HRQoL and is derived from the scales for the domains of physical functioning (PF), role participation with physical health problems (RP), bodily pain (BP) and general health (GH). A high score is indicative of better self-perceived physical HRQoL.
Threshold Levels
A CAT score ≥10 and a SGRQ score ≥25 are the thresholds recommended by GOLD for considering regular treatment of symptoms.3,30 An mMRC of ≥2 is often used as the threshold for clinically significant dyspnea or moderate-severe dyspnea and is incorporated in the ABCD assessment tool in guiding treatment decisions.3,31 A BODE index ≥3 has been suggested as a cut-point associated with higher mortality risk.32–34
Statistical Analysis
Statistical analyses were performed using SPSS Statistics 27 (Statistical Packages for the Social Sciences, IBM Corporation, USA). Statistical significance was set at a p value of 0.05. A SNOT22_rhinological score of ≥11 was defined as a high burden of sinonasal symptoms. This cut-off was based on the results of a receiver operating characteristic (ROC) curve of SNOT22_rhinological score; the AUC was 0.87 (95% confidence interval 0.79–0.94, p < 0.001) and the sensitivity and specificity of the cut-off for a diagnosis of RSsNP were 72% and 82%, respectively. The dataset was analysed by the burden of sinonasal symptoms. Categorical data are presented as frequencies and proportions and compared using the chi square test. Continuous data were inspected for normality by use of histograms with normality curve and presented as means and standard deviations (SD) and compared by the Student t test. The mMRC dyspnea grade and BODE index were handled as continuous variables.27 Multivariable linear regression models were used to explore the associations between a high burden of sinonasal symptoms and the clinical markers for severity of symptoms, physical activity, mortality risk and HRQoL scores. Potential covariates were age, sex, FEV1% predicted, BMI, smoking and allergy. The latter two were excluded from the regression models; smoking pack-years was not significantly associated with any clinical marker in unadjusted regression analysis (data not shown), and the prevalence of allergic rhinitis was not significantly different between high and low burden groups (Table 1). Age and FEV1% predicted were modelled as continuous variables, and BMI was modelled as a categorical variable. FEV1% predicted and BMI were omitted from the regression model for the BODE index as these variables are included in the latter. The assumptions of linear regression were verified using residual plots and tests of normality for the distribution of residuals.
 |
Table 1 Subject Characteristics for COPD Patients and by Burden of Sinonasal Symptoms |
Binomial logistic regression models were performed to estimate the odds ratios (OR) for the association between a high burden of sinonasal symptoms, adjusted for the same covariates as in the multivariable linear regression models, and the likelihood of requiring regular treatment of COPD (SGRQ ≥25 and CAT ≥10), having clinically significant dyspnea/moderate-severe dyspnea (mMRC of ≥2) and higher risk of mortality (BODE index ≥3). The adjusted regression model for BODE index was performed with age and sex as covariates.
Results
Of 90 patients with COPD, 41 (45.6%) had a high burden of sinonasal symptoms. In this group, the SNOT22_rhinological score was 3-fold greater (p < 0.001), 81% had a positive nasal endoscopy for rhinosinusitis (p = 0.047) and FEV1% predicted was significantly lower (p = 0.049) than in the low burden group. Other subject characteristics were not significantly different between the groups (Table 1).
Symptom Severity, Physical Activity and Mortality Risk in COPD
The grade of dyspnea was 1.7-fold and the severity of cough was 2.5-fold greater, the 6MWD was lower and the BODE index was 1.5-fold greater in the high burden than in the low burden group (Figure 2).
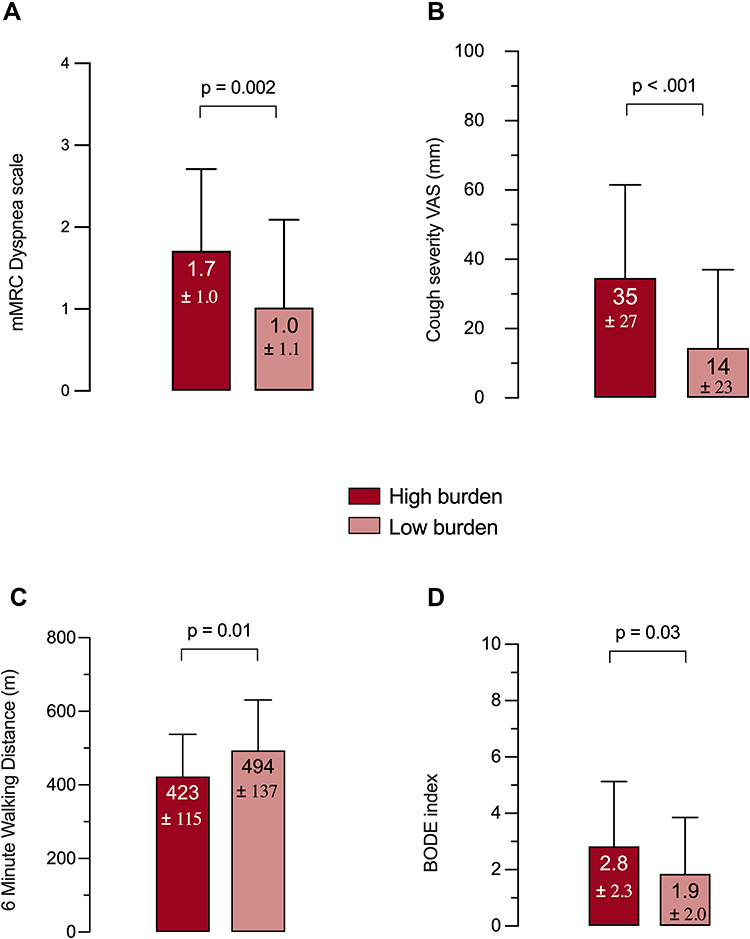 |
Figure 2 Clinical markers for Symptom severity [dyspnea (A), cough (B)], Physical activity (C) and Mortality risk (D) in patients by burden of sinonasal symptoms. Abbreviations: mMRC, modified Medical Research Council; VAS, Visual Analogue Scale; BODE, body mass index, airflow obstruction, dyspnea, exercise capacity. Notes: Data presented as mean ±SD. p-values are calculated using the Student t test. High burden: SNOT22_rhinological score ≥11; Low burden: SNOT22_rhinological score <11. Missing 6MWD data for 2 subjects in low burden group. |
In adjusted multivariable regression analysis, a high burden of sinonasal symptoms was significantly associated with greater severity of dyspnea (β 0.5; 95% CI 0.15 to 0.86, p = 0.006) and cough (β 20.9; 95% CI 9.7 to 32.0, p < 0.001), lower 6MWD (β −59; 95% CI −102 to −15.6, p = 0.008) and higher score of the BODE index (β 0.96; 95% CI 0.07 to 1.86, p = 0.08) (Table 2).
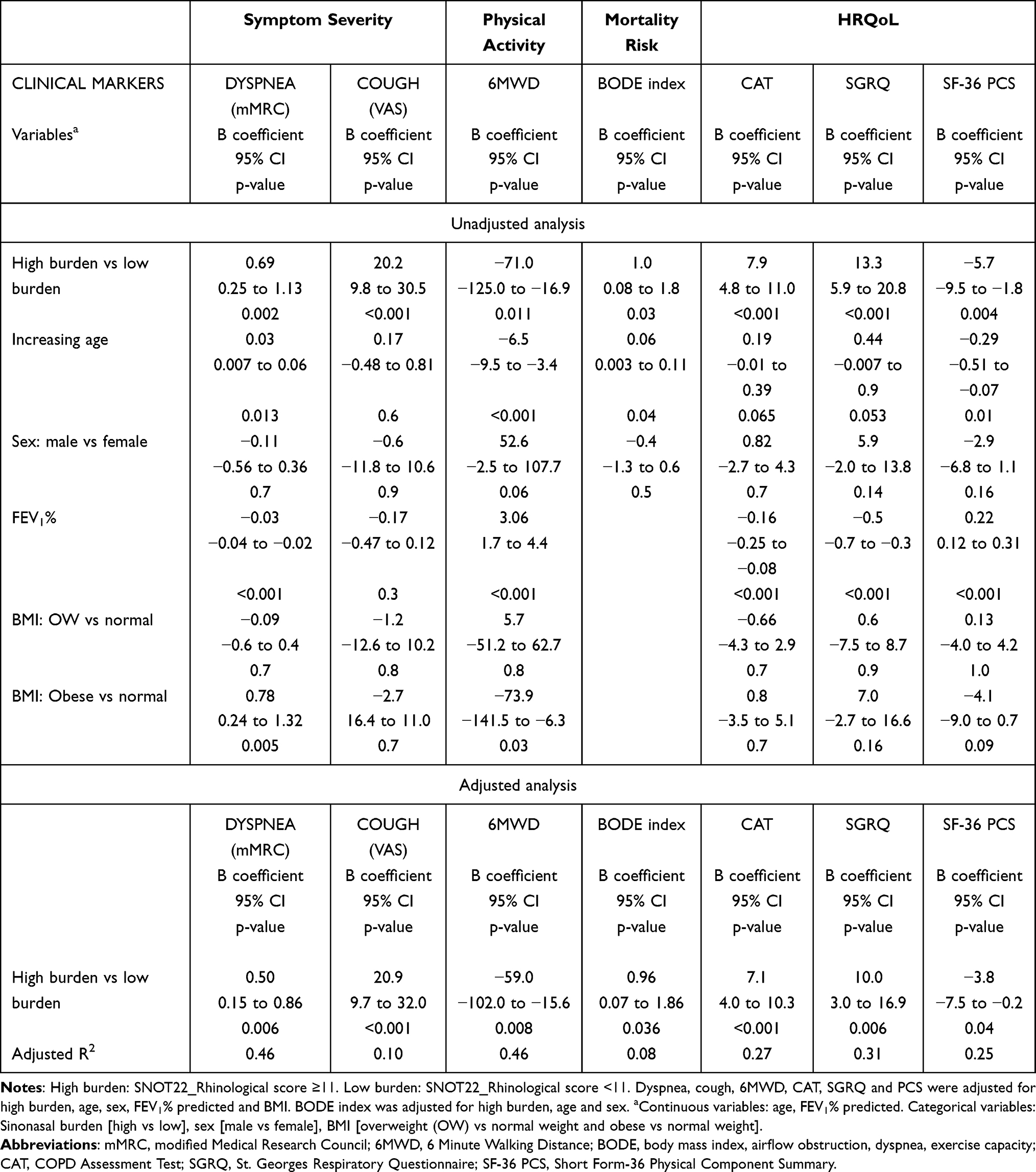 |
Table 2 Associations Between a High Burden of Sinonasal Symptoms and Clinical Markers for Symptoms, Physical Activity, Mortality Risk and HRQoL in COPD |
HRQoL
Disease-specific and generic physical HRQoL were significantly poorer in the group with a high burden than in the group with a low burden of sinonasal symptoms, with higher CAT and SGRQ and lower SF-36 PCS scores in the former group (Figure 3). In multivariable regression analysis, a high burden of sinonasal symptoms was significantly associated with higher disease-specific and lower generic HRQoL scores after adjusting for age, sex, FEV1% predicted and BMI (Table 2).
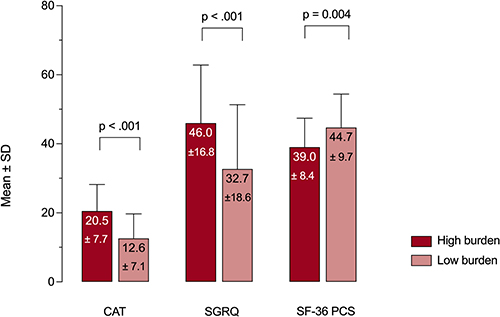 |
Figure 3 Scores for disease-specific (CAT, SGRQ) and generic physical (SF-36 PCS) HRQoL by burden of sinonasal symptoms. Abbreviations: CAT, COPD Assessment Test; SGRQ, St. Georges Respiratory Questionnaire; SF-36 PCS, Short-Form-36 Physical Component Summary. Note: p-values are calculated using the Student t test. High burden: SNOT22_rhinological score ≥11; Low burden: SNOT22_rhinological score <11. |
Threshold Levels
The proportion of patients with threshold scores for treatment indication, moderate-severe dyspnea and risk of mortality was greater in the high burden than in the low burden group; 93% vs 63% (p = 0.002) for the CAT ≥10, 90% vs 63% (p = 0.003) for the SGRQ ≥25, 51% vs 31% (p = 0.047) for the mMRC ≥2 and 54% vs 29% (p = 0.02) for the BODE index ≥3.
In adjusted logistic regression analyses, the high burden group was 7, 5 and 3 times more likely to have CAT, SGRQ and BODE index scores above the threshold levels. The association between a high symptom burden and a score for mMRC above the threshold level was not statistically significant (Figure 4).
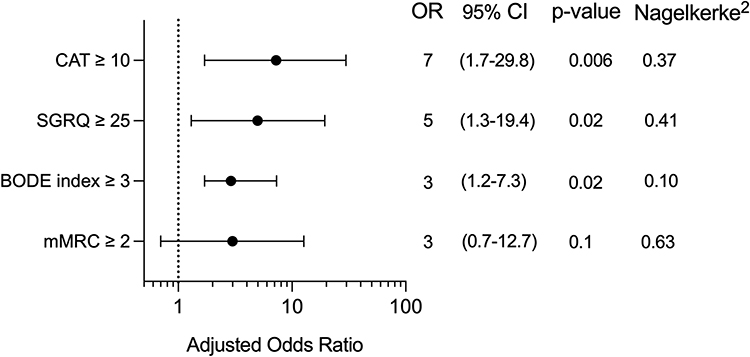 |
Figure 4 Adjusted odds ratios for high threshold levels in the group with high burden of sinonasal symptoms. Abbreviations: CAT, COPD Assessment Test; SGRQ, St. Georges Respiratory Questionnaire, BODE, body mass index, airflow obstruction, dyspnea, exercise capacity; mMRC, modified Medical Research Council. Notes: CAT ≥10, SGRQ ≥25 and mMRC ≥2 were adjusted for high burden (SNOT22_rhinological ≥11), age, sex, FEV1% predicted and BMI. BODE index was adjusted for high burden, age and sex. |
Discussion
This study shows an association between sinonasal symptoms and clinical markers of symptom severity, physical activity, mortality risk and HRQoL in COPD. The novel finding is that the burden of sinonasal symptoms is important for these associations. In adjusted multivariable regression analysis, a high burden of sinonasal symptoms was associated with greater severity of dyspnea and cough, lower 6MWD, higher BODE index and poorer disease-specific and generic physical HRQoL. Moreover, the high burden group had a 5–7-fold greater likelihood of having CAT and SGRQ scores that are above the thresholds recommended for treatment in the GOLD 2022 guideline.
The present study extends the findings of past studies on the association of nasal symptoms with clinical markers of symptom severity in COPD. Of those studies, nasal symptoms were not associated with dyspnea and cough in one study,10 but were associated with an increased grade of dyspnea on the mMRC scale and poorer HRQoL assessed by the SGRQ in the other study.7 Nasal symptoms were quantified as a nasal score derived by summation of the binary response to 5 symptoms (nasal obstruction, nasal discharge, post-nasal discharge, decreased sense of smell, sneezing) in the former study,10 and were defined as the presence of at least one of three symptoms (nasal obstruction, nasal discharge and decreased sense of smell) in the latter study.7 In contrast, the rhinological subscale of the SNOT-22 in the current study quantifies the presence as well as the subjective degree of severity of sinonasal symptoms and is validated for the measurement of symptom burden.21,22 Moreover, the present study shows that the association between sinonasal symptoms and clinical markers of symptom severity is dependent not only on the presence but also on the burden of these symptoms.
The association of a high burden of sinonasal symptoms with increased severity of dyspnea and cough may have pathophysiological and clinical relevance for COPD. An increase in upper airway resistance secondary to nasal obstruction may play a role in the pathogenesis of dyspnea.35,36 Post nasal discharge may lead to cough and is an added risk of instigating acute exacerbations.37–39 Conversely, population-based longitudinal studies over 5 years have suggested that COPD is a risk factor for developing nasal symptoms14 and chronic RSsNP.40 Furthermore, an increase in the prevalence of nasal symptoms over the course of 8 years has been reported in a cohort study.41 Moreover, nasal symptoms (SNOT items 1–8), degree of dyspnea (mMRC) and HRQoL (CAT score) were significantly improved after 8 weeks of daily anti-inflammatory treatment with nasal budesonide in a recent clinical trial in stable COPD patients.42 Thus, clinicians should be aware of the high prevalence of sinonasal symptoms in COPD, and enquiry about their presence in these patients should be a routine in clinical practice. Early recognition and treatment of sinonasal symptoms may contribute to optimising the management of COPD.
Another novel finding of our study is that COPD patients with a high burden of sinonasal symptoms had significantly reduced 6MWD (Figure 2C) and poorer PCS-SF36 (Figure 3). The former is an objective assessment of physical activity, and the latter is a subjective assessment of generic physical HRQoL, and both markers were significantly associated with the burden of sinonasal symptoms after adjustments for lung function, age, sex and BMI. It can be speculated whether upper and lower airway symptoms have an additive or synergistic effect that may promote behavioural change into a more sedentary lifestyle to avoid exertional dyspnea.43,44 If this hypothesis is valid, the finding raises the intriguing question of whether awareness about and treatment of sinonasal symptoms may result in alleviation of dyspnea and thus increased physical activity. The latter has been reported to be the strongest predictor of all-cause mortality in a prospective cohort study of COPD patients.45 Improvement in the grade of dyspnea after 8 weeks of nasal corticosteroid therapy in a pilot study of COPD patients42 is a promising result that requires confirmation in a larger study.
We found a significant association between a high burden of sinonasal symptoms and higher scores for CAT and SGRQ and thus poorer disease-specific HRQoL. This is of significant interest as a recent review highlighted a knowledge gap regarding the impact of sinonasal symptoms on HRQoL in COPD.46 Past studies have used instruments such as the total SNOT-20,8,47 the SNAQ-11 score48 and the SNOT22-nasal symptom subscore15 to quantify sinonasal symptoms. The inclusion of cough, fatigue and sleep in those instruments is a limitation as these items are not specific for the nose and sinuses. In contrast, the rhinological subscale of the SNOT-22 in the present study does not include any of those items, and the cut-off for a high burden was based on an analysis of the ROC curve. Moreover, COPD patients with a high burden of sinonasal symptoms were 5–7 times more likely to have SGRQ and CAT scores that are above the threshold indicating the need for regular treatment of lower airway symptoms. These results suggest that sinonasal symptoms do contribute to poorer HRQoL, implying that diagnosis and treatment of concomitant rhinosinusitis may have clinical benefits in COPD.
In the present study, the cut-off value for a high burden of sinonasal symptoms was set at a rhinological subscale score of ≥11. With this cut-off, 46% of subjects had a high burden of sinonasal symptoms, which is comparable with the finding of 42% in the study by Obling et al.49 Although quantification of symptoms was similar, the rationale for the cut-off value was different for the two studies. The cut-off value in the present study was based on an analysis of a ROC curve for the diagnosis of RSsNP, whereas the cut-off value in that study was set at ≥6 to reflect the presence of mild symptoms in several items and/or moderate symptoms in a few items. In our opinion, the cut-off in that study is too low for a definition of a high burden of sinonasal symptoms, as a response of very mild (score of 1) to the 7 items in the subscale would give a total score of 7 and thus categorization as a high burden. The reliability and reproducibility of our cut-off value should be investigated in future research.
The choice of the rhinological subscale for the assessment of sinonasal symptoms is a strength of our study. This instrument does not assess cough and symptoms of fatigue and sleep and is validated for the assessment of sinonasal symptoms. Another strength is that the burden of sinonasal symptoms is not confounded by nasal polyps which is a different phenotype of chronic rhinosinusitis and known to be associated with sinonasal symptoms.50 Finally, blinding of the otolaryngologist for the presence of sinonasal symptoms and the severity of airflow limitation reduces the risk of bias concerning the outcome of the nasal endoscopic examination and hence the clinical diagnosis of RSsNP. Some limitations should also be addressed. The cross-sectional design precludes a conclusion on the causality of the association between sinonasal symptoms and COPD. However, causality has previously been suggested in a longitudinal follow-up study and two large population-based studies where COPD was associated with an increased risk of developing more nasal symptoms,41 non-infectious rhinitis14 and chronic RSsNP.40 Furthermore, we did not collect data on exacerbations, an important outcome in COPD, nor did we examine pathobiological mechanisms and the sample size was relatively small. Another limitation could be that we assessed cough using a simple VAS for cough severity. Despite being one of the most widely used tools in the clinic and in research,51,52 there are limited data for the generalizability of its validity.25
Conclusion
A high burden of sinonasal symptoms is positively associated with the clinical markers of symptom severity and mortality risk and is inversely associated with physical activity and HRQoL in COPD. These findings add further support that the UAD concept also applies to COPD. Enquiry about sinonasal symptoms in COPD patients should be incorporated into the clinical routine.
Acknowledgments
The authors thank Dr Sarah Bettina Dahlslett (S.B.D), research nurse Else Bartnes and the Clinical Research Facility, St. Olavs hospital, for their assistance and help with data collection. We would also like to thank all participants in the study. The study was supported by a PhD grant provided by the Liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology (NTNU).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, data design, execution, acquisition of data, analyses and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest relevant to this work.
References
1. Valiulis A, Bousquet J, Veryga A, et al. Vilnius declaration on chronic respiratory diseases: multisectoral care pathways embedding guided self-management, mHealth and air pollution in chronic respiratory diseases. Clin Transl Allergy. 2019;9:7. doi:10.1186/s13601-019-0242-2
2. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
3. GOLD Reports. Global initiative for chronic obstructive lung disease; 2022. Available from: www.goldcopd.org.
4. Gonçalves I, Guimarães MJ, van Zeller M, Menezes F, Moita J, Simão P. Clinical and molecular markers in COPD. Pulmonology. 2018;24(4):250–259. doi:10.1016/j.pulmoe.2018.02.005
5. Passalacqua G, Ciprandi G, Canonica GW. United airways disease: therapeutic aspects. Thorax. 2000;55(Suppl2):S26–S27. doi:10.1136/thorax.55.suppl_2.s26
6. Tiotiu A, Novakova P, Baiardini I, et al. Manifesto on united airways diseases (UAD): an Interasma (global asthma association - GAA) document. J Asthma. 2021:1–16. doi:10.1080/02770903.2021.1879130
7. Caillaud D, Chanez P, Escamilla R, et al. Association of chronic nasal symptoms with dyspnoea and quality-of-life impairment in chronic obstructive pulmonary disease. Respirology. 2014;19(3):346–352. doi:10.1111/resp.12224
8. Hurst JR, Wilkinson TMA, Donaldson GC, Wedzicha JA. Upper airway symptoms and quality of life in chronic obstructive pulmonary disease (COPD). Article. Respir Med. 2004;98(8):767–770. doi:10.1016/j.rmed.2004.01.010
9. Montnemery P, Svensson C, Adelroth E, et al. Prevalence of nasal symptoms and their relation to self-reported asthma and chronic bronchitis/emphysema. Eur Respir J. 2001;17(4):596–603. doi:10.1183/09031936.01.17405960
10. Roberts NJ, Lloyd-Owen SJ, Rapado F, et al. Relationship between chronic nasal and respiratory symptoms in patients with COPD. Respir Med. 2003;97(8):909–914. doi:10.1016/S0954-6111(03)00114-8
11. Oie MR, Dahlslett SB, Sue-Chu M, Helvik AS, Steinsvag SK, Thorstensen WM. Rhinosinusitis without nasal polyps in COPD. ERJ Open Res. 2020;6(2):00015–2020. doi:10.1183/23120541.00015-2020
12. Luu K, Sutherland J, Crump T, Liu G, Janjua A. The impact of chronic airway disease on symptom severity and global suffering in Canadian rhinosinusitis patients. J Otolaryngol Head Neck Surg. 2018;47(1):40. doi:10.1186/s40463-018-0287-6
13. Hens G, Vanaudenaerde BM, Bullens DM, et al. Sinonasal pathology in nonallergic asthma and COPD: “united airway disease” beyond the scope of allergy. Allergy. 2008;63(3):261–267. doi:10.1111/j.1398-9995.2007.01545.x
14. Bergqvist J, Andersson A, Olin AC, et al. New evidence of increased risk of rhinitis in subjects with COPD: a longitudinal population study. Int J Chron Obstruct Pulmon Dis. 2016;11:2617–2623. doi:10.2147/copd.S115086
15. Arndal E, Sorensen AL, Lapperre TS, et al. Chronic rhinosinusitis in COPD: a prevalent but unrecognized comorbidity impacting health related quality of life. Respir Med. 2020;171:106092. doi:10.1016/j.rmed.2020.106092
16. Hansen AG, Helvik AS, Thorstensen WM, et al. Paranasal sinus opacification at MRI in lower airway disease (the HUNT study-MRI). Eur Arch Otorhinolaryngol. 2016;273(7):1761–1768. doi:10.1007/s00405-015-3790-7
17. Øie MR, Sue-Chu M, Helvik A-S, Steinsvåg SK, Steinsbekk S, Thorstensen WM. Rhinosinusitis without nasal polyps is associated with poorer health-related quality of life in COPD. Respir Med. 2021;189:106661. doi:10.1016/j.rmed.2021.106661
18. Fokkens WJ, Lund VJ, Mullol J, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl. 2012;23:1–298.
19. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
20. Bousquet J, Khaltaev N, Cruz AA, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy. 2008;63(Suppl 86):8–160. doi:10.1111/j.1398-9995.2007.01620.x
21. Erskine SE, Hopkins C, Clark A, et al. SNOT-22 in a control population. Clin Otolaryngol. 2017;42(1):81–85. doi:10.1111/coa.12667
22. Lange B, Thilsing T, Al-kalemji A, Baelum J, Martinussen T, Kjeldsen A. The Sino-Nasal outcome test 22 validated for Danish patients. Dan Med Bull. 2011;58(2):A4235.
23. Browne JP, Hopkins C, Slack R, Cano SJ. The Sino-Nasal Outcome Test (SNOT): can we make it more clinically meaningful? Otolaryngol Head Neck Surg. 2007;136(5):736–741. doi:10.1016/j.otohns.2007.01.024
24. Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93(3):580–586. doi:10.1378/chest.93.3.580
25. Martin Nguyen A, Bacci ED, Vernon M, et al. Validation of a visual analog scale for assessing cough severity in patients with chronic cough. Ther Adv Respir Dis. 2021;15:17534666211049743. doi:10.1177/17534666211049743
26. American Thoracic Society Committee. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
27. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
28. Jones PW, Quirk FH, Baveystock CM. The St George’s respiratory questionnaire. Respir Med. 1991;85(Suppl B):25–37. doi:10.1016/s0954-6111(06)80166-6
29. Ware JE
30. Jones PW, Tabberer M, Chen WH. Creating scenarios of the impact of COPD and their relationship to COPD Assessment Test (CAT) scores. BMC Pulm Med. 2011;11:42. doi:10.1186/1471-2466-11-42
31. Müllerová H, Lu C, Li H, Tabberer M. Prevalence and burden of breathlessness in patients with chronic obstructive pulmonary disease managed in primary care. PLoS One. 2014;9(1):e85540. doi:10.1371/journal.pone.0085540
32. Scarlata S, Finamore P, Laudisio A, et al. Association between frailty index, lung function, and major clinical determinants in chronic obstructive pulmonary disease. Aging Clin Exp Res. 2021;33(8):2165–2173. doi:10.1007/s40520-021-01878-z
33. Andrianopoulos V, Wouters EF, Pinto-Plata VM, et al. Prognostic value of variables derived from the six-minute walk test in patients with COPD: results from the ECLIPSE study. Respir Med. 2015;109(9):1138–1146. doi:10.1016/j.rmed.2015.06.013
34. Marin JM, Carrizo SJ, Casanova C, et al. Prediction of risk of COPD exacerbations by the BODE index. Respir Med. 2009;103(3):373–378. doi:10.1016/j.rmed.2008.10.004
35. Schumacher MJ. Nasal dyspnea: the place of rhinomanometry in its objective assessment. Am J Rhinol. 2004;18(1):41–46. doi:10.1177/194589240401800109
36. Hurst JR, Kuchai R, Michael P, Perera WR, Wilkinson TM, Wedzicha JA. Nasal symptoms, airway obstruction and disease severity in chronic obstructive pulmonary disease. Clin Physiol Funct Imaging. 2006;26(4):251–256. doi:10.1111/j.1475-097X.2006.00683.x
37. Koo HK, Park SW, Park JW, et al. Chronic cough as a novel phenotype of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2018;13:1793–1801. doi:10.2147/copd.S153821
38. Pratter MR. Chronic upper airway cough syndrome secondary to rhinosinus diseases (previously referred to as postnasal drip syndrome): ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1):63s–71s. doi:10.1378/chest.129.1_suppl.63S
39. Dąbrowska M, Arcimowicz M, Grabczak EM, et al. Chronic cough related to the upper airway cough syndrome: one entity but not always the same. Eur Arch Otorhinolaryngol. 2020;277(10):2753–2759. doi:10.1007/s00405-020-06071-y
40. Chien CY, Tai SY, Wang LF, Lee CT. Chronic obstructive pulmonary disease predicts chronic rhinosinusitis without nasal polyps: a population-based study. Am J Rhinol Allergy. 2015;29(3):e75–80. doi:10.2500/ajra.2015.29.4172
41. Huerta A, Donaldson GC, Singh R, et al. Upper respiratory symptoms worsen over time and relate to clinical phenotype in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2015;12(7):997–1004. doi:10.1513/AnnalsATS.201408-359OC
42. Calabrese C, Costigliola A, Maffei M, et al. Clinical impact of nasal budesonide treatment on COPD patients with coexistent rhinitis. Int J Chron Obstruct Pulmon Dis. 2018;13:2025–2032. doi:10.2147/copd.S165857
43. Hanania NA, O’Donnell DE. Activity-related dyspnea in chronic obstructive pulmonary disease: physical and psychological consequences, unmet needs, and future directions. Int J Chron Obstruct Pulmon Dis. 2019;14:1127–1138. doi:10.2147/copd.S188141
44. Polkey MI, Rabe KF. Chicken or egg: physical activity in COPD revisited. Eur Respir J. 2009;33(2):227–229. doi:10.1183/09031936.00176808
45. Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a Prospective Cohort Study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
46. Håkansson K, Konge L, Thomsen SF, Backer V, von Buchwald C. Sinonasal inflammation in COPD: a systematic review. Eur Respir J. 2013;42(5):1402–1411. doi:10.1183/09031936.00119712
47. Yang X, Xu Y, Jin J, Li R, Liu X, Sun Y. Chronic rhinosinusitis is associated with higher prevalence and severity of bronchiectasis in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:655–662. doi:10.2147/COPD.S124248
48. Piotrowska VM, Piotrowski WJ, Kurmanowska Z, Marczak J, Górski P, Antczak A. Rhinosinusitis in COPD: symptoms, mucosal changes, nasal lavage cells and eicosanoids. Int J Chron Obstruct Pulmon Dis. 2010;5:107–117. doi:10.2147/copd.s8862
49. Obling N, Backer V, Hurst JR, Bodtger U. Upper airway symptoms associate with the eosinophilic phenotype of COPD. ERJ Open Res. 2021;7(3):00184–2021. doi:10.1183/23120541.00184-2021
50. Gelardi M, Bocciolini C, Notargiacomo M, et al. Chronic rhinosinusitis with nasal polyps: how to identify eligible patients for biologics in clinical practice. Acta Otorhinolaryngol Ital. 2022;42(1):75–81. doi:10.14639/0392-100x-n1699
51. Brightling CE, Monterio W, Green RH, et al. Induced sputum and other outcome measures in chronic obstructive pulmonary disease: safety and repeatability. Respir Med. 2001;95(12):999–1002. doi:10.1053/rmed.2001.1195
52. Smith JA, Kitt MM, Butera P, et al. Gefapixant in two randomised dose-escalation studies in chronic cough. Eur Respir J. 2020;55(3):1901615. doi:10.1183/13993003.01615-2019
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.