")
Back to Journals » OncoTargets and Therapy » Volume 16
Single-Center Retrospective Clinical Evaluation of Venetoclax Combined with HMAs and Half-Dose CAG for Unfit or Refractory/Relapsed AML
Authors Chen X, Zhao Y, Li Q, Fan S
Received 3 February 2023
Accepted for publication 18 May 2023
Published 13 June 2023 Volume 2023:16 Pages 409—419
DOI https://doi.org/10.2147/OTT.S405611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Xiaotong Chen, Yanqiu Zhao, Qi Li, Shengjin Fan
Department of Hematology, The First Affiliated Hospital of Harbin Medical University, Harbin, 150001, People’s Republic of China
Correspondence: Shengjin Fan, Tel +86-13304641978, Email [email protected]
Purpose: The prognosis of patients with unfit or relapsed/refractory (R/R) AML remains poor. Venetoclax (VEN) has been shown to exhibit anti-leukemia stem cell activity; however, few studies have been published on the efficacy and safety of VEN combined with both hypomethylating agents (HMAs) and low-dose chemotherapy for patients with unfit or R/R AML.
Methods: This study retrospectively analyzed the clinical characteristics, treatment details, safety profile and clinical outcomes of patients with unfit or R/R AML treated with VEN+ HMAs+ half-dose CAG (LDAC, aclarubicin and granulocyte colony-stimulating factor).
Results: A total of 24 AML patients were involved in the study, of whom 13 (54.2%) were in the unfit group, and 11 (45.8%) were in the R/R group. FLT3 and IDH (8/24, 33.3%) were the most common gene aberrations. Patients in the R/R group were found to be more likely to carry KIT (5/11, 45.5%) compared with the unfit group (0/13, 0%) (P = 0.006). The ORR observed during the study was 83.3% (20/24; 14 CR, 2CRi, 4PR). In the unfit group, 11/13 (84.6%) patients achieved cCR (10 CR and 1 CRi); while 5/11 (45.5%) R/R patients achieved response (4 CR and 1 CRi). CR was observed in all AML patients with TP53 (5/5), GATA2 (3/3), CEBPA (3/3) and ASXL1 (3/3). The most common adverse events (AEs) during VEN+ HMAs+ half-dose CAG therapy were persistent cytopenias and infections.
Conclusion: The results of this study confirm that VEN+ HMAs+ half-dose CAG is associated with promising efficacy (even high-risk molecular patterns) and tolerable safety profile in patients with unfit or R/R AML. Yet, the study involves only a small sample size, which should not be overlooked. As such, further studies on the efficacy of VEN combined with HMAs and half-dose CAG regimen in AML patients are essential.
Keywords: acute myeloid leukemia, BCL2 inhibitor, venetoclax, combined chemotherapy
Introduction
Acute myeloid leukemia (AML) is predominantly a disease of the elderly, with a median age of 68 at diagnosis.1,2 Advanced age, high frequency of unfavorable genomic features and less favorable clinical characteristics, including reduced biological function and more complex medical comorbidities, may contribute to the inability of older patients to tolerate high-dose chemotherapy.3,4 Also, refractory/relapsed (R/R) AML is associated with a poor prognosis.5 The treatment outcome for R/R AML patients are rather poor and characterised by low cure rate, poor outcome and high follow-up dropout.6,7
B-cell leukemia/lymphoma-2 (BCL2) family exerts a central effect in the regulation of cell survival and apoptosis.8 Moreover, AML stem cells express aberrantly high levels of anti-apoptotic gene BCL2 and rely on the expression of BCL2 for their survival.9 Upregulated expression of BCL-2 may be required to permit ongoing death signaling without a cellular response.10 Relevant studies have revealed that the overexpression of BCL2 has a significant impact on inferior chemotherapeutic response and unfavorable overall survival in AML patients.11 Therefore, antagonizing BCL-2 function may cause death in AML cells.
Venetoclax (VEN), an orally active and potent BCL-2 selective inhibitor, has been shown to exhibit anti-leukemic activity and to induce cancer cell death.12 Recently, several small retrospective studies have evaluated the efficacy and chemotherapy toxicity of VEN in combination with hypomethylating agents [HMAs, such as decitabine (DAC) or azacitidine (AZA)] or low-dose cytarabine (LDAC).4 Studies have demonstrated VEN combination therapy improves the response rate and survival rate in elderly patients with unfit or R/R AML,13 but as many as 30% to 45% of the patients with unfit or R/R AML still failed to experience complete remission through VEN-HMAs/LDAC therapy.14 Meanwhile, VEN-HMAs/LDAC typically result in profound and prolonged neutropenia, which substantially increases the risk of infections in AML patients. Importantly, it is found that HMAs combined with CAG regimen [LDAC, aclarubicin and granulocyte colony-stimulating factor (G-CSF)] appear to be associated with improved prognosis of AML patients.15,16 In order to increase response rate and overcome the toxicity of VEN-HMAs/LDAC, VEN is combined with low-dose chemotherapy and the treatment duration of it is also shortened.
According to our research, this is the first study to evaluate the efficacy and side effects of VEN combined with HMAs and half-dose CAG. The clinical characteristics, treatment details, clinical outcomes and safety profile of 24 consecutive patients with unfit or R/R AML treated with VEN+ HMAs+ half-dose CAG will be presented and described in this report.
Methods
Patients
This retrospective study analyzed consecutive AML patients treated at the First Affiliated Hospital of Harbin Medical University from January 1, 2020 to June 1, 2022. Diagnostic procedures and genetic risk stratification were performed as per the recommendations of European Leukemia Net (ELN) 2017.3 The unfit group involved patients with newly diagnosed AML who were considered to be ineligible for high-dose chemotherapy if they were ≥60 years old, had an ECOG score≥3 or exhibited complex medical comorbidities. We included all patients who received the treatment of VEN+HMAs+half dose CAG, and the exclusion criteria were patients who did not receive the treatment of VEN+HMAs+half dose CAG. This study was approved by the institutional review board of the First Affiliated Hospital of Harbin Medical University, and the need for written informed consent was waived because of the retrospective nature of this study. The study was conducted in compliance with the Declaration of Helsinki and patient data were maintained with strict confidentiality. In our research, there was no overlap between the two groups. All patients in the unfit group were de novo AML patients, and all the RR patients were in RR group.
Treatment
VEN+ HMAs+ half-dose CAG regimens were implemented as follows: all patients received VEN once daily for 14 days. To prevent tumor lysis syndrome (TLS), the dose of VEN was 100mg on day 1 and 200mg on day 2; on day 3, to boost the concentration of VEN alongside routine antifungal prophylaxis, it was combined with CYP3A4 inhibitors fluconazole 400mg once a day.17 Plasma concentrations of VEN were measured after five days of VEN administration. HMA therapy included DAC 20 mg/m2/d intravenously for five days or AZA 75 mg/m2/d subcutaneously for seven days. Half-dose CAG regimen consisted of LDAC 10 mg/m2/12h subcutaneously for fourteen days, aclarubicin 8 mg/m2/d intravenously for four days and G-CSF 200 μg/m2/d subcutaneously for fourteen days. For patients with leukocytosis, whose white blood cell (WBC) count was greater than 10×109/L, hydroxyurea (1.0–3.0 g/day) was given orally until the WBC count dropped below 10×109/L, and then the chemotherapy was initiated. Notably, all patients did not receive other anti-leukemic agents (eg FLT3, IDH1, IDH2 inhibitors) during the same period.
Next‑generation Sequencing (NGS)
Bone marrow samples were collected from all the 24 AML patients. Next‑generation sequencing was performed by a third-party detection platform of Shanghai Yuanqi Biotechnology. Genomic DNA (gDNA) library for next-generation sequencing was prepared using a commercial kit (Shanghai Yuanqi Biotechnology). The sequencing was performed on a MiSeq instrument (Illumina) and all variants identified by NGS were confirmed by Sanger sequencing of individual mutations. The data generated in the present study are included in the figures or tables of this article.
Adverse Events Reporting
The severity of AEs was estimated according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.18 Clinical and laboratory data about AEs were collected from patients’ files.
Treatment Responses
Response to treatment was assessed by bone marrow (BM) evaluation at the time of hematological recovery and adjudicated in alignment with the recommendations of ELN 2017.18 All patients, including those with incomplete hematological recovery, were assessed for minimal residual disease (MRD). Complete response (CR) was defined as bone marrow blasts <5% with hematological recovery [absolute neutrophil count (ANC) ≥1.0×109/L and PLT ≥100×109/L].3 CR without minimal residual disease (CRMRD-) is referred to as CR with negativity for a genetic marker by RT-qPCR, or with negative MFC test.3 CRi means CR with incomplete hematological recovery and PR refers to bone marrow blast of 5% to 25% or at least 50%3 reduction in bone marrow blast compared to pre-treatment level. The overall response rate (ORR) is the sum of the CR, CRi, and PR and composite complete remission (cCR) is the composite of CR and CRi. Relapse occurs after CR with a greater than 5% recurrence of leukemic cells in bone marrow aspirates.3
Statistical Analysis
Patient characteristics were summarized based on descriptive statistics (medians or frequencies with ranges). For binary variable, Chi-squared or Fisher’s exact test were adopted to analyze the differences between the two subgroups. Time-to-event endpoints were measured through Kaplan–Meier method and the Log rank test was applied to compare the statistical differences between subgroups. Data were statistically analyzed with SPSS version 22.0 (IBM SPSS Statistics, IBM Corporation, Armonk, NY).
Results
Patients
From January 2020 to June 2022, a total of 24 AML patients were treated with VEN+ HMAs+ half-dose CAG regimens at our institution. A total of 13 patients (54.2%) were included in the unfit group and 11 patients (45.8%) in the R/R group (relapsed, n = 9; refractory, n = 2) (Table 1). The median age was 55 (range, 21–72), and 10/24 (41.7%) patients were ≥60 (Table 1). Table 1 summarizes the patient details upon initiation of VEN+ HMAs+ half-dose CAG treatment.
 |
Table 1 Clinical Characteristics of 21 AML Patients |
One patient in the R/R group had previously received allogeneic hematopoietic stem cell transplantation (HSCT) but experienced early recurrence after transplantation. In addition, nine patients had been previously treated with HMAs. The median number of prior therapies in the R/R group was 2 (range, 1–5), of whom 10 (90.9%) received VEN+ HMAs+ half-dose CAG therapy as the first salvage treatment.
Biological Characteristics
Molecular aberrations were identified with next-generation sequencing. All AML patients had cytogenetic and molecular aberration results, which are outlined in Figure 1, were available in all AML patients. In the 24 AML patients, the NGS panel showing a concordance rate of 100% with standard techniques. Ranging from 1 to 8 mutations, the average mutational burden was 4 (Figure 1). In this study, FLT3 and IDH (8/24, 33.3%) were the most common gene aberrations in all AML patients (Figure 1), followed by DNMT3A (7/24, 29.2%) (Figure 1). For the unfit group, FLT3 and IDH (6/13, 46.2%) were the most common gene aberrations. In addition, patients in the R/R group were found more likely to carry KIT (5/11, 45.5%) compared with the unfit group (0/13, 0%) (P = 0.006, Figure 1). In contrast, the distribution of other mutations did not reach a statistically significant difference.
 |
Figure 1 Distribution of mutated genes in patients with unfit or R/R AML. Each column represents a patient. The first line is the group of each AML patient, the second line shows the ELN genetic risk stratification, and the third line stands for the treatment response. In the fourth to the thirty-second line, each row represents a gene and each colored box indicates one mutated gene. |
Response
The median follow-up time for the 24 AML patients was 10.4 months (range, 0.8 to 23 months). A mean of 2 cycle (range, 1 to 4) of VEN+ HMAs+ half-dose CAG therapy was implemented, with a median response time (from the beginning of treatment to bone marrow blasts <5%) of 1.2 months (range, 0.6 to 2.2 months), or 1.4 cycles (range, 1 to 2). An ORR of 83.3% (20/24; 14 CR, 2CRi, 4PR) was observed, with 66.7% (16/24) of all the AML patients achieving cCR in the cohort (Figure 1 and Table 1). Twelve patients (8 in the unfit group and 4 in the R/R group) entered flow cytometry-assessed MRD-negative status. In the unfit group, 12/13 (92.3%) patients achieved response, of which, 10 CR (76.9%), 1 CRi (7.7%) and 1 PR (7.7%); while 8/11 (72.7%) R/R patients achieved response, of which, 4 CR (36.4%), 1 CRi (9.1%) and 3 PR (27.3%). Details of responders are presented in Table 2.
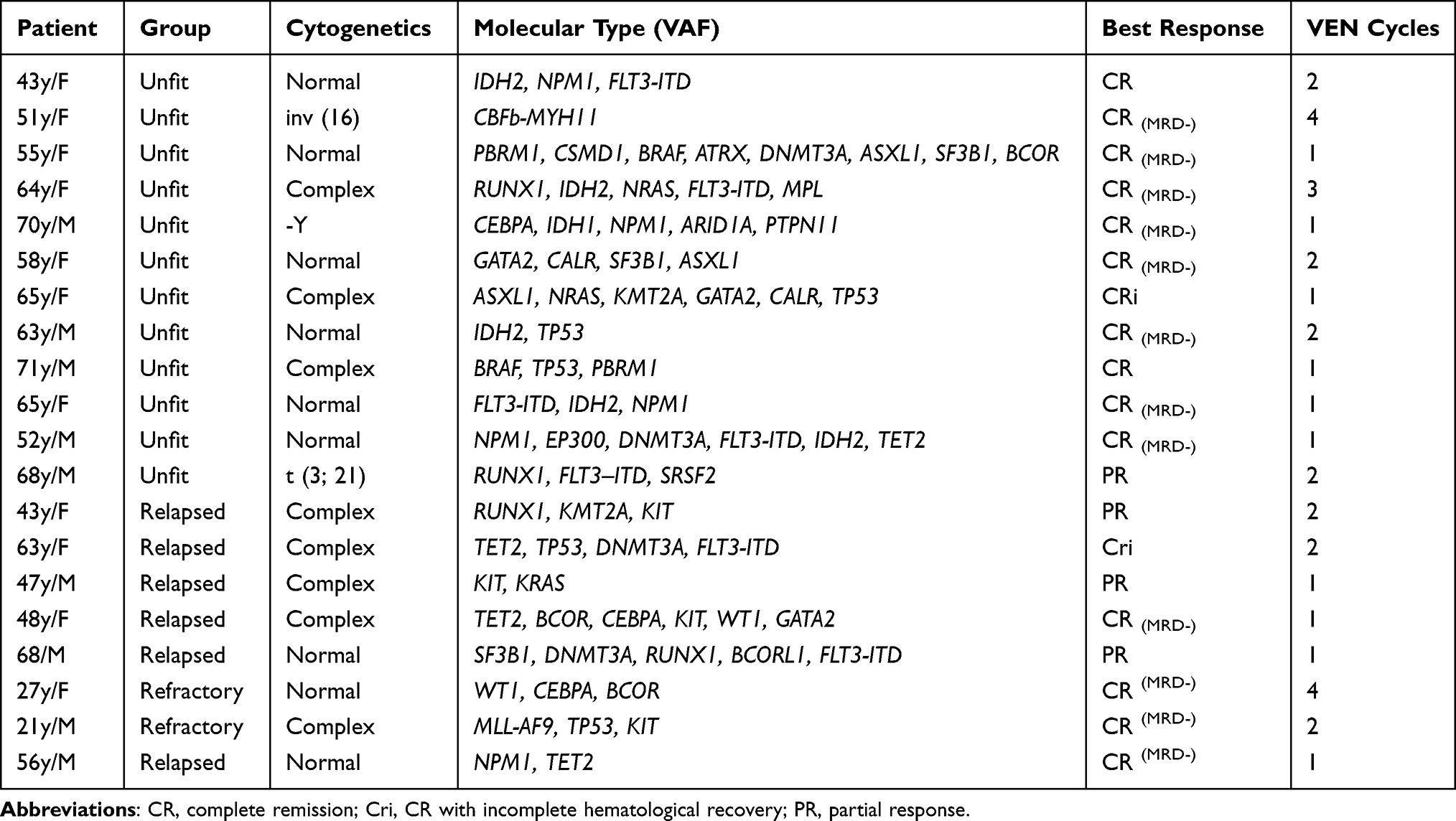 |
Table 2 Characteristics of Responding Patients (CR, CRi, PR) |
In this study, CR was observed in all AML patients with TP53 (5/5), GATA2 (3/3), CEBPA (3/3) and ASXL1 (3/3); 83.3% (5/6) of the AML patients with NPM1; 80% (4/5) of the AML patients with TET2; 75% of the AML patients with IDH (6/8) and BCOR (3/4); 66.7% of the AML patients with NRAS (2/3) and KMT2A (2/3); 62.5% (5/8) of the AML patients with FLT3; 42.9% (3/7) of the AML patients with DNMT3A; 40% (2/5) of the AML patients with KIT; 16.7% (1/6) of the AML patients with RUNX1; 0% (0/2) of the AML patients with RUNX1 (Figure 1).
Median OS of all patients was 8.5 months [95% confidence interval (CI) 3.6 to 15.4] (Figure 2A) when the VEN+ HMAs+ half-dose CAG therapy initiated, compared with 9 and 4.5 months for the unfit and the R/R AML patients (P= 0.020) (Figure 2B). Among all patients, OS was better in responders (CR, CRi, PR) than in non-responders, with medians of 9 and 4 months, respectively (hazard ratio, 0.28; 95% CI, 0.14–1.59; P=0.000) (Figure 2C).
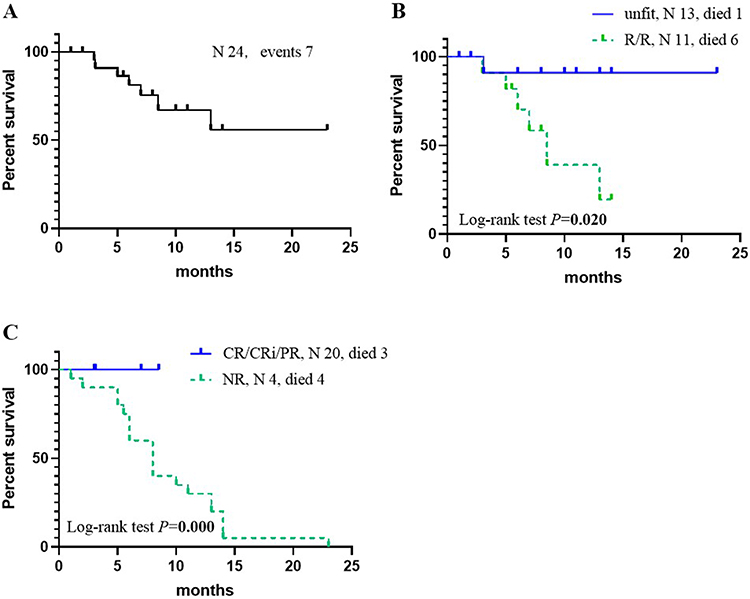 |
Figure 2 Kaplan–Meier survival curves for the survival rate of AML patients treated with VEN+ HMAs+ half-dose CAG therapy. (A) Data given for all patients; (B) Unfit vs R/R patients (P=0.020); (C) Responders vs Nonresponders (P=0.000). |
Adverse Events
The most common AEs during VEN+ HMAs+ half-dose CAG therapy were persistent cytopenia and infection. Our study suggested that 21 (87.5%) of the AML patients developed febrile neutropenia, transfusion-dependent anemia and thrombocytopenia (Table 3) and 10 (41.7%) of the AML patients experienced prolonged pancytopenia (requiring a treatment delay of more than 14 days). However, recovery of blood counts was observed only in patients who responded to chemotherapy. Among these patients, 24 days (range, 15 to 36 days) was the median time for neutrophil recovery (ANC >1.0×109/L), while PLT recovery (PLT >100× 109 /L) took 32 days (range, 22–58 days). Moreover, 21 (87.5%) of the AML patients presented with Grade 3 or higher neutropenia.
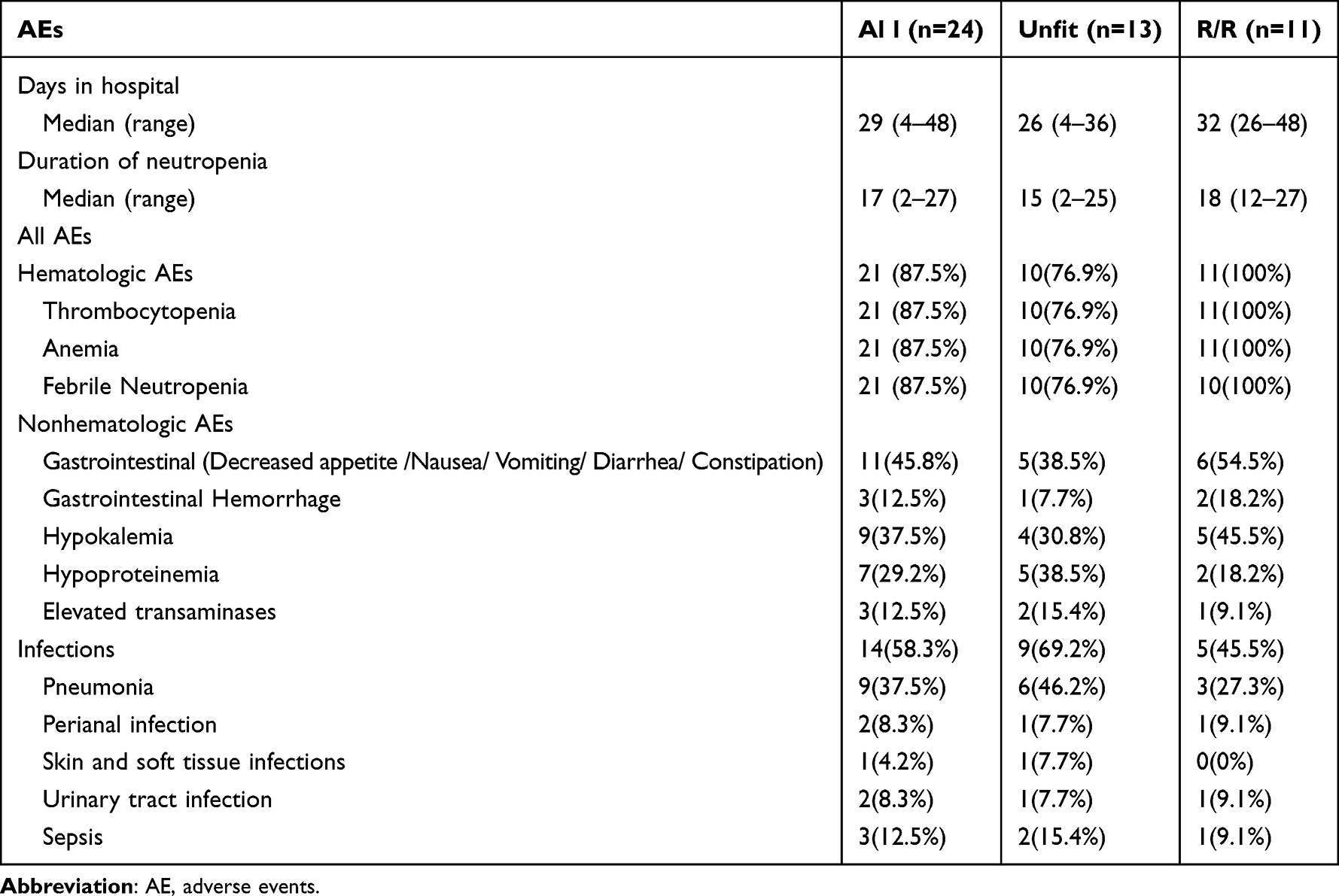 |
Table 3 The Most Notable AEs (Grade 3 or Higher) |
During the initial VEN cycle, 14 patients (58.3%) developed Grade 3 or higher infections, of which 9 had pneumonia, 3 suffered from sepsis, 2 experienced perianal infection, 2 had urinary tract infection and 1 developed skin infection. During VEN+ HMAs+ half-dose CAG therapy, 3 (12.5%) of the AML patients were treated with micafungin and 8 (33.3%) of them received voriconazole for prophylaxis. No patient experienced breakthrough fungal infection (BFI) and no patient suffered from tumor lysis syndrome (TLS). Three patients (12.5%) presented with hemorrhagic complications, including gastrointestinal hemorrhage and hematuria. The most common non-haematological AEs were gastrointestinal symptoms (decreased appetite, nausea, vomiting and diarrhea) (11/24, 45.8%). Early mortality (death within 30 days since the start of the therapy) occurred in 2 (8.3%) patients—one underwent a septic shock and acute left-heart failure followed by multi-organ dysfunction syndrome and DIC; the other patient developed severe pneumonia complicated with ARDS. Three other patients in the R/R group did not achieve any relief and a total of seven (29.2%) deaths were recorded. The most notable AEs are outlined in Table 3.
Discussion
Previous investigations have revealed a fact that both unfit and R/R AML are still associated with a dismal prognosis.3,19–22 Relevant studies have also reported that the remission rates of common chemotherapy regimens remain low in patients with unfit or R/R AML, with a CR rate of 32% for HD-Ara-C,23 46.5% for CAG regiment24,25 and 48% for FLAG.26 Recently, BCL-2 inhibitor VEN has been approved for use in AML patients in combination with hypomethylating agents (azacitidine or decitabine).27 Meanwhile, CAG regimen is widely applied in the treatment of MDS and AML in China. However, the remission rates of both VEN and CAG regimens are still unsatisfactory in patients with unfit or R/R AML.24,28 VEN combined with cytotoxic chemotherapy produces synergistic leukemic killing effects, and consequently improves clinical efficacy.29 The molecular mechanism is to increase DNA damage and decrease Mcl-1, which in turn increases the concentration of intracellular apoptosis activator Bim, leading to apoptosis.30,31 As the first study to evaluate the efficacy and side effects of VEN+ HMAs+ half-dose CAG in patients with unfit or R/R AML, this study identified VEN+ HMAs+ half-dose CAG therapy as the backbone of relevant therapies in which an improved clinical response in OS was noted in patients with unfit and R/R AML, but further randomized controlled trials and prospective cohort studies is needed.
This study analyzed the genetic characteristics in both groups and only KIT mutation (P= 0.006) reached a statistical difference; patients in the R/R group were much more likely to carry KIT mutation. ELN risk stratification was the same in both groups (P= 0.657), and patients with unfit or R/R AML were more likely to assume a high-risk state of ELN risk stratification (17/24, 70.8%).
Biomarker analysis in our research demonstrated that VEN+ HMAs+ half-dose CAG was effective for most AML patients, even in those with a high-risk molecular profile. Previous studies have manifested that mutations such as TP5332 and FLT3-ITD33,34 are related to poor prognosis in AML patients. The CR rate of traditional chemotherapy in AML patients with TP53 mutant was as low as 28%. Kim et al reported an overall response rate of 66% in the treatment of AML patients with TP53 with VEN coupled with decitabine.35 Lower response rate and shorter survival rate with VEN are common in patients with TP53 AML, and it is disappointing to find that the addition of VEN to standard treatment regimens does not improve the prognosis of TP53 AML patients.35,36 Surprisingly, in the present study, patients with TP53 performed particularly well in all outcome indicators, achieving a CR/CRi rate of 100%. A study of 125 elderly AML patients treated with D-CAG illustrated that D-CAG tended to improve the prognosis of TP53 mutated patients.15 This result suggests that the VEN+ HMAs+ half-dose CAG regimen may be an effective rescue regimen for patients with TP53mut AML, but due to its small sample size, our studies may have some bias, and further expansion of the sample size is needed to verify this finding. Some studies have revealed that patients with IDH1/2 mutation exhibit a favorable prognosis.12,37 However, in other studies, the prognosis was poor or dependent on the type of IDH.38 In our study, CR rate is reported as 75% in AML patients with IDH1/2, which may indicate that AML patients with IDH mut are highly sensitive to VEN. Hence, the mechanism underlying this may be as follows: the accumulation of tumor metabolite 2-HG inhibits cytochrome C oxidase and effectively primes AML blasts to Bcl2 inhibition.39 In addition, AML patients with NPM1mut (CR rate of 83.3%) appear to have a relatively good prognosis under the treatment of VEN+ HMAs+ half-dose CAG.
With an ORR of 83.3% (20/24; 14 CR, 2 CRi, 4 PR) and the median duration of response was 8.5 months (95% CI 3.6 to 15.4) for VEN+HMAs+half-dose CAG therapy, the high CR rate of AML patients with high-risk mutations may demonstrate that VEN in combination with chemotherapy can overcome some of the mechanisms of conventional chemotherapy resistance.
Despite receiving a combination of chemotherapeutic agents, the side effects of VEN+ HMAs+ half-dose CAG are tolerable and mostly reversible. Most of the Grade 3/4 AEs are hematologic and are similar to those reported with VEN in combination with azacitidine or decitabine.40,41 Cytopenia improves mainly, although usually incompletely, at the beginning of the reaction. In subsequent VEN cycles, recurrent Grade 3/4 neutropenia was treated by suspending VEN, which shortened the application time of VEN and prolonged the treatment interval and using growth factor. Only one patient discontinued chemotherapy because of excessive myelosuppression and all patients received blood transfusion support. The type and interval of blood transfusion were evaluated in line with the blood cell count. Non-hematological toxicity was acceptable, and no significant end-organ damage events were noted. The low frequency of breakthrough invasive fungal infections could be attributed to the routine combination of CYP3A inhibitor azole antifungals, which reduced both VEN doses and the cost of treatment. Therefore, the toxicity associated with VEN+ HMAs+ half-dose CAG regimen is acceptable.
Limited by the relatively small sample size, too insufficient statistics were available for this study to draw definitive conclusions and further validation studies are therefore needed. Meanwhile, this study is a single-center retrospective study, and its results may be influenced by unrecognized bias.
In summary, this study has shown that the VEN combined with HMAs and half-dose CAG regimen has promising efficacy (even if the molecular pattern is high-risk) and a tolerable safety profile in patients with unfit or R/R AML is identified, whereas the VEN+ HMAs+ half-dose CAG regimen should and will be further evaluated prospectively in a larger AML population.
Abbreviations
AML, acute myeloid leukemia; BFI, breakthrough fungal infection; TLS, tumor lysis syndrome; VEN, venetoclax; AEs, adverse events; R/R, relapsed/refractory; HSCT, hematopoietic stem cell transplant; BCL2, B-cell leukemia/lymphoma-2; HMAs, hypomethylating agents; LDAC, low-dose cytarabine; HD, high-dose; DAC, decitabine; AZA, azacitidine; ELN, European Leukemia Net; WBC, white blood cell; PLT, platelet; CTCAE, Common Terminology Criteria for Adverse Events; MRD, minimal residual disease; CR, complete response; cCR, composite complete remission; PR, partial response; TF, treatment failure; ANC, absolute neutrophil cell; ORR, overall response rate; BM, bone marrow.
Data Sharing Statement
All data generated or analyzed during the research are included in this article. Further enquiries can be directed to the corresponding author.
Ethical Approval
This study protocol was discussed and approved by the Medical Ethics Committee of the First Affiliated Hospital of Harbin Medical University, and the informed consent was approved to be waived in this retrospective analysis by the committee. The study was conducted in compliance with the Declaration of Helsinki, and patient data were maintained with strict confidentiality.
Funding
No funding was received.
Disclosure
There is no competing interest among the authors.
References
1. Siegel R, Jemal A, Ward E, et al. Cancer statistics. CA Cancer J Clin. 2020. doi:10.3322/caac.21590
2. Howlader N, Noone A, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2016. National Cancer Institute; 2019.
3. Döhner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
4. DiNardo CD, Pratz K, Pullarkat V. Venetoclax combined with decitabine or azacitidine in treatment-naive, elderly patients with acute myeloid leukemia. Blood. 2019;133(1):7–17. doi:10.1182/blood-2018-08-868752
5. Thein MS, Ershler WB, Jemal A, Yates JW, Baer,MR. Outcome of older patients with acute myeloid leukemia: an analysis of SEER data over 3 decades. Cancer. 2013;119(15):2720–2727. doi:10.1002/cncr.28129
6. Walter RBO, Othus M, Burnett AK, et al. Resistance prediction in AML: analysis of 4601 patients from MRC/NCRI, HOVON/SAKK, SWOG and MD Anderson cancer center. Leukemia. 2015;29(2):312–320. doi:10.1038/leu.2014.242
7. Shah AAT, Andersson TM-L, Rachet B, Björkholm M, Lambert,PC. Survival and cure of acute myeloid leukaemia in England, 1971–2006: a population-based study. Br J Haematol. 2013;162(4):509–516. doi:10.1111/bjh.12425
8. Adams CM, Clark-Garvey S, Porcu P, Eischen,CM. Targeting the Bcl-2 family in B cell lymphoma. Front Oncol. 2019;8:636. doi:10.3389/fonc.2018.00636
9. Campos LRJ, Rouault JP, Sabido O, et al. High expression of bcl-2 protein in acute myeloid leukemia cells is associated with poor response to chemotherapy. Blood. 1993;81(11):3091–3096. doi:10.1182/blood.V81.11.3091.3091
10. Del Gaizo Moore VLA. Rational design of therapeutics targeting the BCL-2 family: are some cancer cells primed for death but waiting for a final push? Adv Exp Med Biol. 2008;615:159–175. doi:10.1007/978-1-4020-6554-5_8
11. Mehta SV, Shukla SN, Vora HH. Overexpression of Bcl2 protein predicts chemoresistance in acute myeloid leukemia: its correlation with FLT3. Neoplasma. 2013;60(06):666–675. doi:10.4149/neo_2013_085
12. Konopleva M, Pollyea DA, Potluri J, et al. Efficacy and biological correlates of response in a Phase II study of venetoclax monotherapy in patients with acute myelogenous leukemia. Cancer Disc. 2016;6(10):1106–1117. doi:10.1158/2159-8290.CD-16-0313
13. DiNardo CD, Maiti A, Rausch,CR, et al. 10-day decitabine with venetoclax for newly diagnosed intensive chemotherapy ineligible, and relapsed or refractory acute myeloid leukaemia: a single-center, Phase 2 trial. Lancet Haematol. 2020;7(10):e724–e736. doi:10.1016/S2352-3026(20)30210-6
14. Wei AH, Montesinos P, Ivanov V. Venetoclax plus LDAC for newly diagnosed AML ineligible for intensive chemotherapy: a Phase III randomised placebo-controlled trial. Blood. 2020;135(24):2137–2145. doi:10.1182/blood.2020004856
15. Hong M, Zhu H, Sun Q. Decitabine in combination with low-dose cytarabine, aclarubicin and G-CSF tends to improve prognosis in elderly patients with high-risk AML. Aging. 2020;12(7):5792–5811. doi:10.18632/aging.102973
16. Qu Q, Liu L, Zhang Y, et al. Increasing aclarubicin dosage of the conventional CAG (low-dose cytarabine and aclarubicin in combination with granulocyte colony-stimulating factor) regimen is more efficacious as a salvage therapy than CAG for relapsed/refractory acute myeloid leukemia. Leuk Res. 2015;39(12):1353–1359. doi:10.1016/j.leukres.2015.09.014
17. Matthew Mei M, Aldoss I, Marcucci G, Pullarkat V. Hypomethylating agents in combination with venetoclax for acute myeloid leukemia: update on clinical trial data and practical considerations for use. Am J Hematol. 2019;94(3):358–362. doi:10.1002/ajh.25369
18. Institute. NIoHaNC. Common terminology criteria for adverseEvents (CTCAE), v5.0. Bethesda, MD, USA: National Institutes of Health and National Cancer Institute; 2017. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/ctcae_v5_quick_reference_5x7.pdf.
19. Ofran Y, Rowe JM. Treatment for relapsed acute myeloid leukemia: what is new? Opinion Hematol. 2012;19(2):89–94.
20. Shipley JL, Butera JN. Acute myelogenous leukemia. Exp Hematol. 2009;36(7):649–658.
21. Garciaz S, Hospital M-A, Alary A-S. Azacitidine plus venetoclax for the treatment of relapsed and newly diagnosed acute myeloid leukemia patients. Cancers. 2022;14(8):2025. doi:10.3390/cancers14082025
22. DiNardo CD, Lachowiez CA, Takahashi K. Venetoclax combined with FLAG-IDA induction and consolidation in newly diagnosed and relapsed or refractory acute myeloid leukemia. J Clin Oncol. 2021;39(25):2768–2778. doi:10.1200/JCO.20.03736
23. Karanes KJK C, Kopecky KJ, Head DR, et al. A phase III comparison of high dose ARA-C (HIDAC) versus HIDAC plus mitoxantrone in the treatment of first relapsed or refractory acute myeloid leukemia southwest oncology group study. Leukemia Res. 1999;23(9):787–794. doi:10.1016/S0145-2126(99)00087-9
24. Li YS JM, Wu DP, Liang H, et al. Aclarubicin and low-dose cytosine arabinoside in combination with granulocyte colony-stimulating factor in treating acute myeloid leukemia patients with relapsed or refractory disease and myelodysplastic syndrome: a multicenter study of 112 Chinese patients. Int J Hematol. 2005;82:48–54.
25. Liu YZ L, Si Y, Si Y, et al. Increasing the dose of aclarubicin in low-dose cytarabine and aclarubicin in combination with granulocyte colony-stimulating factor (CAG regimen) can safely and effectively treat relapsed or refractory acute myeloid leukemia. Int J Hematol. 2014;99(5):603–608. doi:10.1007/s12185-014-1528-8
26. Lee Dhy SR, Ahn JS, Kim YK, et al. The clinicaloutcome of FLAG chemotherapy without idarubicin in patients with relapsed or refractory acute myeloid leukemia. Korean Med. 2009;24(3):498–503.
27. Ganzel C, Ram R, Gural A. Venetoclax is safe and efficacious in relapsed/refractory AML. Leuk Lymphoma. 2020;61(9):2221–2225. doi:10.1080/10428194.2020.1761964
28. Mian M, Rinaldi A, Mensah AA. A meta-analysis of CAG (cytarabine, aclarubicin, G-CSF) regimen for the treatment of 1029 patients with acute myeloid leukemia and myelodysplastic syndrome. Hematol Oncol. 2011;30(1):46. doi:10.1002/hon.997
29. Pei S, Pollyea A, Gustafson A, et al. Monocytic subclones confer resistance to venetoclax-based therapy in patients with acute myeloid leukemia. Cancer Discov. 2020;10(4):536–551. doi:10.1158/2159-8290.CD-19-0710
30. Niu X, Zhao J, Ma J. Binding of released Bim to Mcl-1 is a mechanism of intrinsic resistance to ABT-199 which can be overcome by combination with daunorubicin or cytarabine in AML cells. Clin Cancer Res. 2016;22(17):4440–4451. doi:10.1158/1078-0432.CCR-15-3057
31. Bose P, Gandhi V, Konopleva M. Pathways and mechanisms of venetoclax resistance. Leuk Lymphoma. 2017;58(9):2026–2039. doi:10.1080/10428194.2017.1283032
32. Stirewalt DL, Kopecky KJ, Meshinchi S. FLT3, RAS, and TP53 mutations in elderly patients with acute myeloid leukemia. Blood. 2001;97(11):3589–3595. doi:10.1182/blood.V97.11.3589
33. Fathi AT, Chen Y-B. Treatment of FLT3-ITD acute myeloid leukemia. Am J Blood Res. 2011;1(2):175–189.
34. Lazenby M, Gilkes AF, Marrin C, Evans A, Hills RK, Burnett AK. The prognostic relevance of flt3 and npm1 mutations on older patients treated intensively or non-intensively: a study of 1312 patients in the UK NCRI AML16 trial. Leukemia. 2014;28(10):1953–1959. doi:10.1038/leu.2014.90
35. Kim KK, Maiti A, Loghavi S, et al. Outcomes of TP53 -mutant acute myeloid leukemia with decitabine and venetoclax. Cancer. 2021;127(20):3772–3781. doi:10.1002/cncr.33689
36. Venugopal SM, Shoukier M, Konopleva M, et al. Outcomes in patients with newly diagnosed TP53 -mutated acute myeloid leukemia with or without venetoclax-based therapy. Cancer. 2021;127(19):3541–3551. doi:10.1002/cncr.33675
37. Patel JP, Gönen M, Figueroa ME. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med. 2012;366(12):1079–1089. doi:10.1056/NEJMoa1112304
38. Green CL, Evans CM, Zhao L. The prognostic significance of IDH2 mutations in AML depends on the location of the mutation. Blood. 2011;118(2):409–412. doi:10.1182/blood-2010-12-322479
39. Venugopal S, Takahashi K, Daver N, et al. Efficacy and safety of enasidenib and azacitidine combination in patients with IDH2 mutated acute myeloid leukemia and not eligible for intensive chemotherapy. Blood Cancer J. 2022;12(1):10. doi:10.1038/s41408-021-00604-2
40. Dombret H, Butrym JF, Butrym A, et al. International Phase 3 study of azacitidine vs conventional care regimens in older patients with newly diagnosed AML with >30% blasts. Blood. 2015;126(3):291–299. doi:10.1182/blood-2015-01-621664
41. Kantarjian HM, Thomas XG, Dmoszynska A, et al. Multicenter, randomized, open-label, phase III trial of decitabine versus patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. J Clin Oncol. 2012;30(21):2670–2677. doi:10.1200/JCO.2011.38.9429
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.