Back to Journals » Advances in Medical Education and Practice » Volume 15
Simulation Use in Respiratory Therapy Programs in Saudi Arabia: Results of a National Survey
Authors Al-Otaibi HM ![]() , Al-Abdullah NA, Naqru AA
, Al-Abdullah NA, Naqru AA ![]() , Boukhari MA, Almohaimeed AM, Alzhrani AJ
, Boukhari MA, Almohaimeed AM, Alzhrani AJ
Received 7 November 2023
Accepted for publication 27 March 2024
Published 16 April 2024 Volume 2024:15 Pages 323—331
DOI https://doi.org/10.2147/AMEP.S445235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Hajed M Al-Otaibi,1,2 Nabeela Abdullah Al-Abdullah,3 Abdulrahman A Naqru,4 Mohammed A Boukhari,5 Ahmed M Almohaimeed,2 Abdulaziz J Alzhrani6
1Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia; 2Respiratory Therapy Unit, King Abdulaziz University Hospital, King Abdulaziz University, Jeddah, Saudi Arabia; 3Department of Public Health, Faculty of Nursing, King Abdulaziz University, Jeddah, Saudi Arabia; 4Respiratory Therapy Department, Dr. Soliman Fakeeh Hospital, Jeddah, Saudi Arabia; 5Respiratory Therapy Department, Andalusia Group Hospital, Jeddah, Saudi Arabia; 6Respiratory Therapy Department, Bugshan Hospital, Jeddah, Saudi Arabia
Correspondence: Hajed M Al-Otaibi, Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, P.O. Box 80200, Jeddah, 21589, Saudi Arabia, Email [email protected]
Background: The use of simulation-based methods for teaching and learning in the education of health professions is increasing, but its prevalence in Saudi Arabia among respiratory therapy programs has yet to be investigated. The purpose of this study is to identify the use of simulation-based learning (SBL) in respiratory therapy programs in Saudi Arabia.
Methods: A cross-sectional study was performed by sending Google forms survey via Email to directors of respiratory therapy programs in Saudi Arabia (N=16) to evaluate how each one used simulations as an educational tool.
Results: The survey was returned with a total response of 12 out of all 16 program that were initially contacted (75% response rate). Among the respondents, approximately 75% of the programs are using SBL, while high-fidelity simulation is used by all programs. The present data show that 67% of the respiratory therapy programs has a space for simulation within the department, while 33% utilizes institutional simulation centers. For short simulation scenarios, debriefing is not conducted in 67% of the programs. There is acceptance by program directors that simulation hours should be counted towards clinical hours. About 67% of respondent programs have mandatory simulation learning activities, and 100% agree that simulations should be used more. However, lack of training and shortage of staff are among barriers to increase the use of SBL.
Conclusion: SBL is commonly used and relatively varied among respiratory therapy programs. However, it requires some improvements in several aspects, including the use of debriefing and increasing the number of properly trained staff.
Keywords: respiratory therapy, simulation, debriefing, medical education, Saudi Arabia
Introduction
Simulation in clinical settings can be defined as tools, devices, or environment that help mimicking real situation.1 Simulation in general is considered to be safe and useful method for teaching and learning. It helps avoiding risks that might be encountered by instructors, students, and subjects involved in the training.2 Therefore, simulation is considered an excellent educational tool to gain and enhance clinical skills. It is well documented that use of simulation for clinical education has significant impact on the learning outcomes. It has considerable effect on knowledge acquisition, gaining and enhancing skills, and behaviors related factors.1 Moreover, Arias et al reported that simulation adds greater significant accuracy to the intended learning skills.3 However, others stated that it might not be necessary to cause significant improvement in performance.4
Simulation-based learning (SBL) is defined as active and immersive learning activity, which occur in virtual learning environment but resemble real-life situation.5 Over the last decades, SBL in healthcare has grown in popularity. As the demand for training grows, more universities, colleges, hospitals, and even standalone simulation centers were established around the world. In Saudi Arabia, SBL is rapidly developing due to the expansion of healthcare specialties, increased training needs, and the availability of resources across many healthcare professions, including respiratory therapy.6 Respiratory therapy programs are well established in Saudi Arabia,7,8 and their use of SBL is reported to be a suitable alternative to some of the bedside clinical practices where critical interventions are vital, especially in intensive care units for neonates, pediatrics, and adults. Therefore, there is need to use different simulation methods like high-fidelity task trainers, low-fidelity task trainers, and computer-based simulation to perform procedures like intubation, extubation, arterial puncture, and mechanical ventilation management. The learning outcomes of using different simulation methods particularly high fidelity versus low fidelity simulation were inconsistent. It was reported to be in favor of low fidelity simulation,9 While others showed it is in favor of high fidelity simulation.10
In Saudi Arabia, early clinical exposure for the majority of respiratory therapy programs is considered vital component of the programs’ learning objectives.11 Early exposure to clinical practice, if not properly managed, can negatively affect student’s experience, confidence, and learning outcomes.11 SBL was reported to enhance theoretical knowledge and clinical practice together.12 It also can improve student’s personal skills, such as leadership, communication, teamwork, decision-making skills13 and critical thinking.14 More importantly, students can be closely supervised, so their overall performance is fully monitored using realistic clinical scenarios without risks to the patient.15
Currently, SBL is utilized across many disciplines in the healthcare field as a tool for teaching and learning.16 In Saudi Arabia, several investigations have aimed to explore the utilization of simulation in teaching and learning in medical schools.17–20 The purpose of these studies ranged from identifying utilization of SBL to measuring satisfaction of learners and instructors. Also, in nursing programs, it was reported that SBL improve learners’ knowledge, confidence, and satisfaction.21 Similarly, in the United States (US), some healthcare specialties such as paramedics and nursing have utilized SBL on their educational programs. But in respiratory therapy profession, the utilization of SBL is less compared to these professions.22–24 While in Saudi Arabia, up to the authors’ knowledge, the utilization of SBL within the respiratory therapy programs was not investigated. Therefore, the aim of the present investigation is to identify utilization and efficiency of SBL in respiratory therapy programs in Saudi Arabia.
Materials and Methods
Study Design and Participants
Qualtrics survey was utilized with permission from previously published study.24 The development of the survey was explained on previous reports.24,25 It contains 23 item that involve multiple-choice, “select all that apply”, and free-text responses. The survey was divided into several categories including demographics, debriefing, modalities, accreditation, and recommendations for equivalent clinical time. The debriefing was defined as an organized meeting following the clinical simulation scenarios to discuss participants’ performance and promote the learning outcomes.26 It is interactive, reflective and bidirectional discussion between trainers and learners.27,28 The SBL activities were defined to include methods like high-fidelity simulation with a mannequin, task trainers simulations, and screen-based computer simulation. Some examples of these methods include arm simulator to extract arterial blood samples, adult and neonatal resuscitation-training mannequins, and airway mannequins for tracheal intubation. Box 1 shows definition of different types of simulation which were adapted from previous study.24 The simulation definitions were shown to participants at the top of the survey.
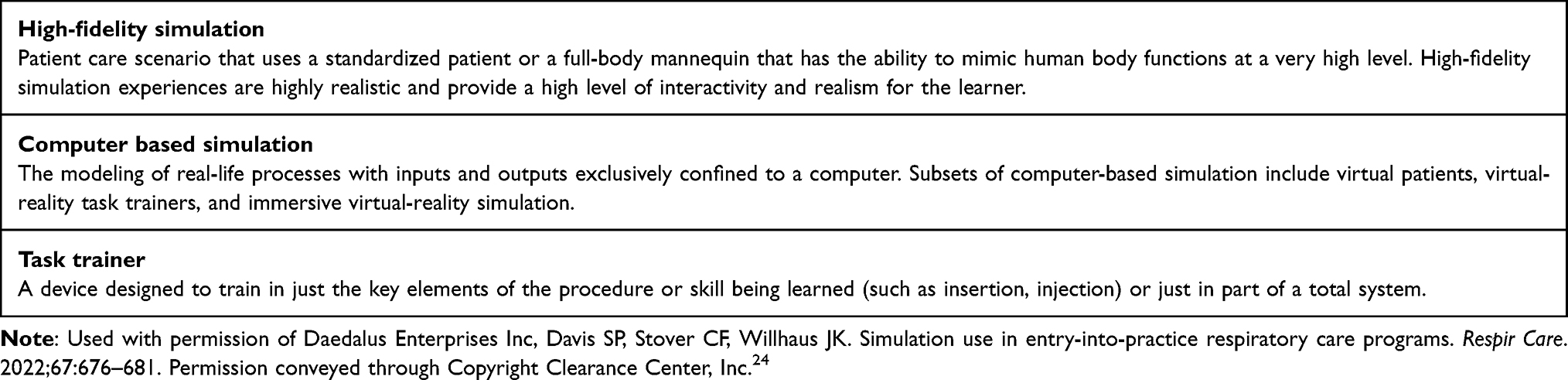 |
Box 1 Definition of Different Types of Simulation |
Data Collection
A report published in 2016 showed that there are 14 respiratory therapy program in Saudi Arabia.7 However, five of these programs were phased out. It is worth noting that one of the phased out programs was reactivated. But, this was not reflected on their official website. Therefore, it was missed out. Additionally, the official websites for colleges and universities were searched to identify active respiratory therapy programs. A total of 16 respiratory therapy programs were identified. The survey was sent using google form link through Email to each respiratory therapy program director in Saudi Arabia (N=16) in March 2022 and followed up until May 2022. Email contacts were obtained from the official websites of each institution. To exclude any repeated responses, the Email addresses of all institutions in Saudi Arabia were selected, and a restriction was activated to allow only one response per institution. Moreover, all respiratory therapy program directors were contacted through the phone and informed about the survey and the purpose of the study. A total of 12 non-duplicated surveys were received (75% response rate). Program directors give their consent to participate by their agreement to take part of this survey. Ethical approval was obtained from faculty of medical rehabilitation sciences’ ethics committee, King Abdulaziz University. Data were anonymized by removing any personal information for the purpose of confidentiality.
Statistical Analysis
For the descriptive analysis, categorical variables are presented as absolute numbers and percentages, and continuous variables are presented as mean and standard deviation. Statistical analysis was performed using Microsoft Excel® 2017 (Microsoft Corporation, Redmond, WA, USA).
Results
Table 1 presents the institutions’ demographic information. It shows that all programs were bachelor-of-science degree programs. All responses were obtained from universities or colleges. The majority of responses came from central and western regions of Saudi Arabia. The data show that 58% of the programs graduate at least 10 students. However, there were three programs from which no one had graduated. It should be noted that there were two programs, out of the 12, not operational: one had yet to start, and another was closed temporarily.
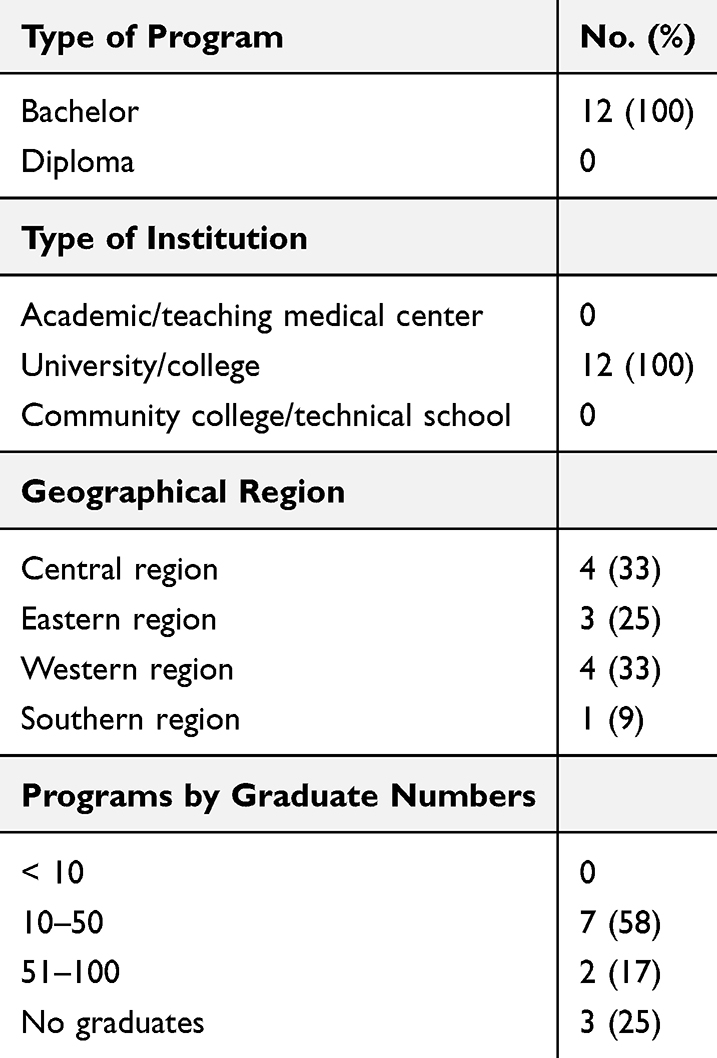 |
Table 1 Demographic Information |
Table 2 presents the utilization of SBL among respiratory therapy programs. It shows that 75% of the programs used at least one type of simulation, while 100% of them used high-fidelity simulation. It also shows that high-fidelity and task-trainer simulations were the most common types utilized within the respiratory therapy curricula. The present data show that 67% of the respiratory therapy programs has a space for simulation within the department, while 33% utilize institutional simulation centers. The institutional simulation center is multidisciplinary simulation center. It is independent and commonly utilized by other programs.
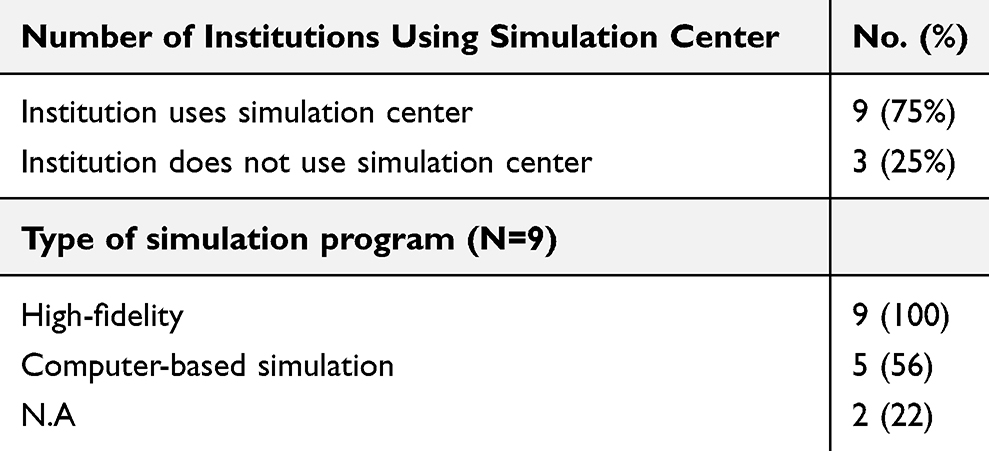 |
Table 2 Utilization of Simulations |
Table 3 presents the type of simulation in relation to the respiratory therapy courses. It shows that high fidelity simulator and task trainer are the most common types. It also shows more utilization of high fidelity and task trainer simulators in adult critical care courses and neonatal/pediatric courses; but less utilization of computer-based simulators. While utilization of computer-based simulator is more frequent in pulmonary function testing, foundation of adult therapeutics, and patient assessment courses.
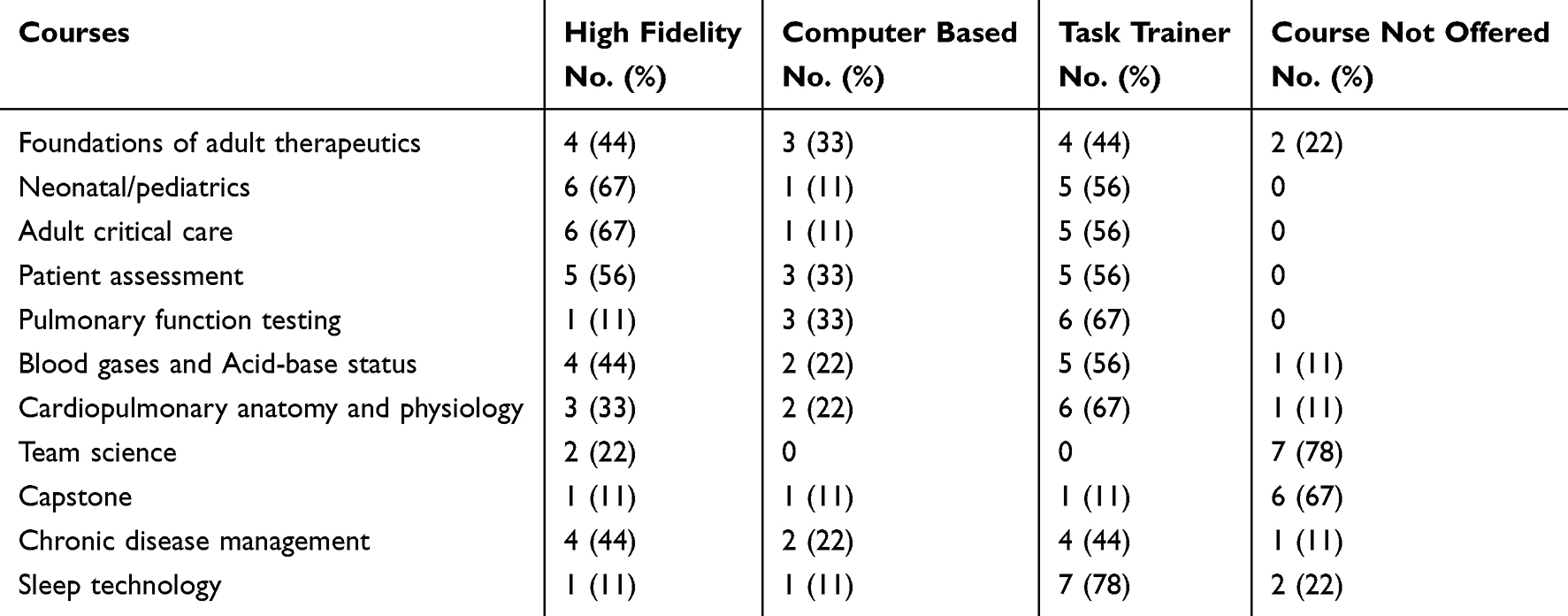 |
Table 3 Type and Amount of Simulation Uses in Courses (N=9) |
Table 4 presents the different types of simulations utilized by respiratory therapy programs. It shows that standardized patients and advanced breathing simulators were the most common types.
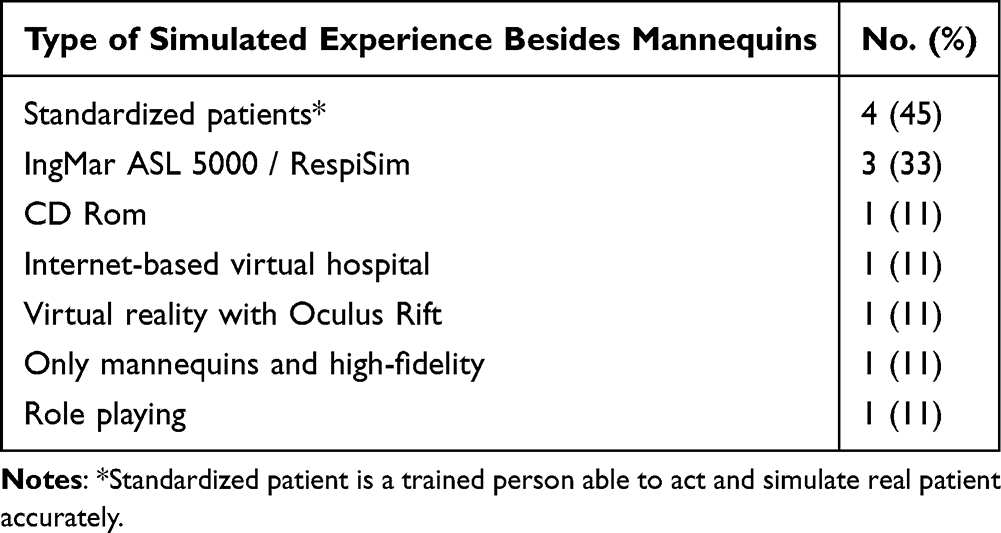 |
Table 4 Methods of Simulation |
Table 5 presents the variability of debriefing times among the respiratory therapy programs. It shows that 67% of the programs had no debriefing for simulation scenarios of less than 30 minute. On simulation scenarios longer than 30 minute, there is a debriefing on 67% of the respiratory therapy programs but the debriefing time is less than the scenario time on almost 50% of the programs.
 |
Table 5 Debriefing Time by Simulation Scenario Duration |
Table 6 presents the utilization of simulation training as a form of clinical training. The vast majority of the respondents (78%) believe that the simulation hours should be counted towards clinical hours. Some of the respondents agree that the number of simulation hours is equivalent to clinical practice, while others indicate that there should be more clinical practice than simulation. Respiratory therapy programs considerably differ in how they count the ratio of simulation hours to clinical hours.
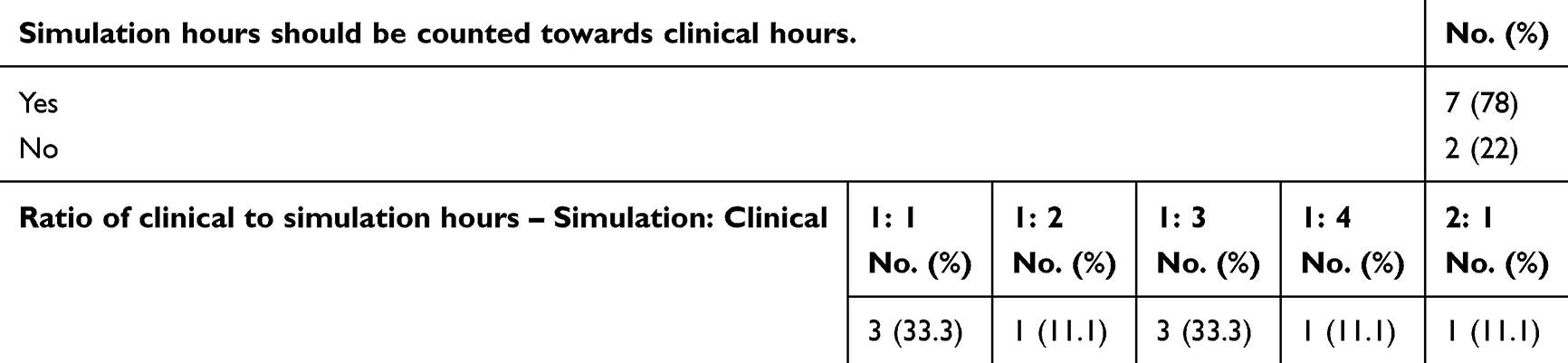 |
Table 6 The Ratio of Simulation Hours to Clinical Hours |
Table 7 presents the learning scenarios opportunities. It shows that simulations are used in all common types of learning scenarios. They are most commonly used to train students to master routine daily tasks such as routine respiratory therapy procedures and patient assessments.
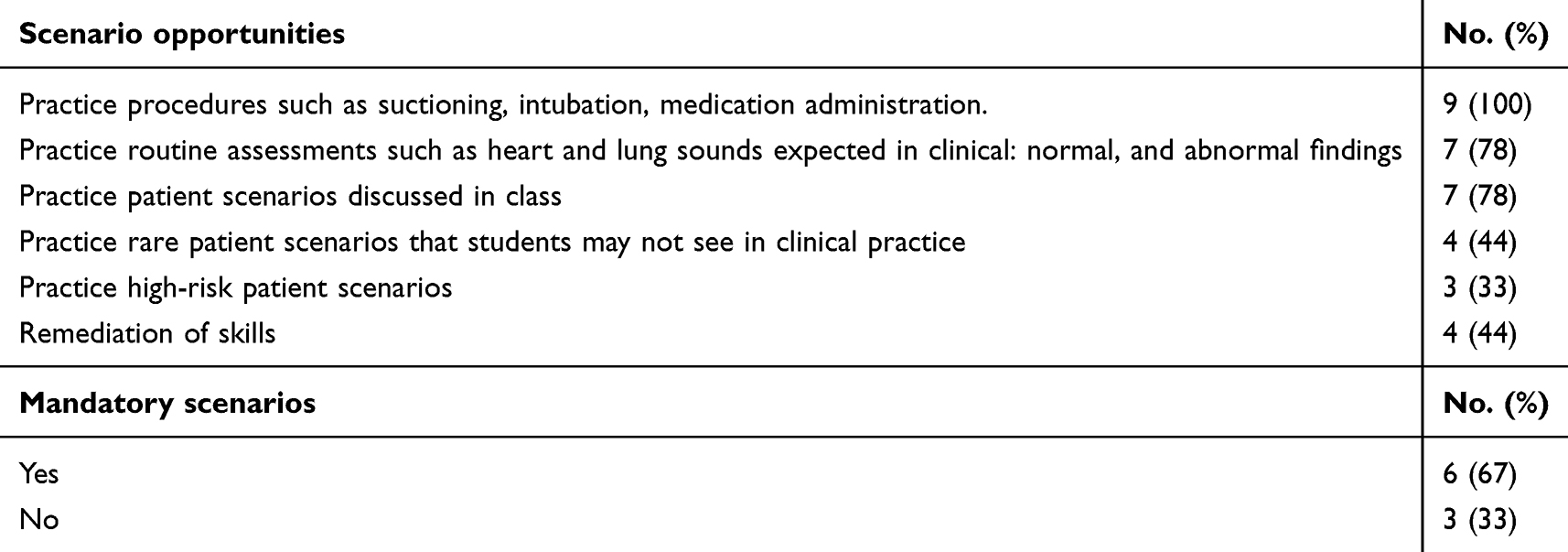 |
Table 7 Learning Scenarios |
Table 8 presents the opinions of respiratory therapy program directors about the need for simulation training within their teaching and learning activities. It also shows barriers that preclude more SBL utilization. All program directors agree to invest in simulation training. However, they state that shortage of staffing and lack of training are the most common barriers to increase simulation utilization.
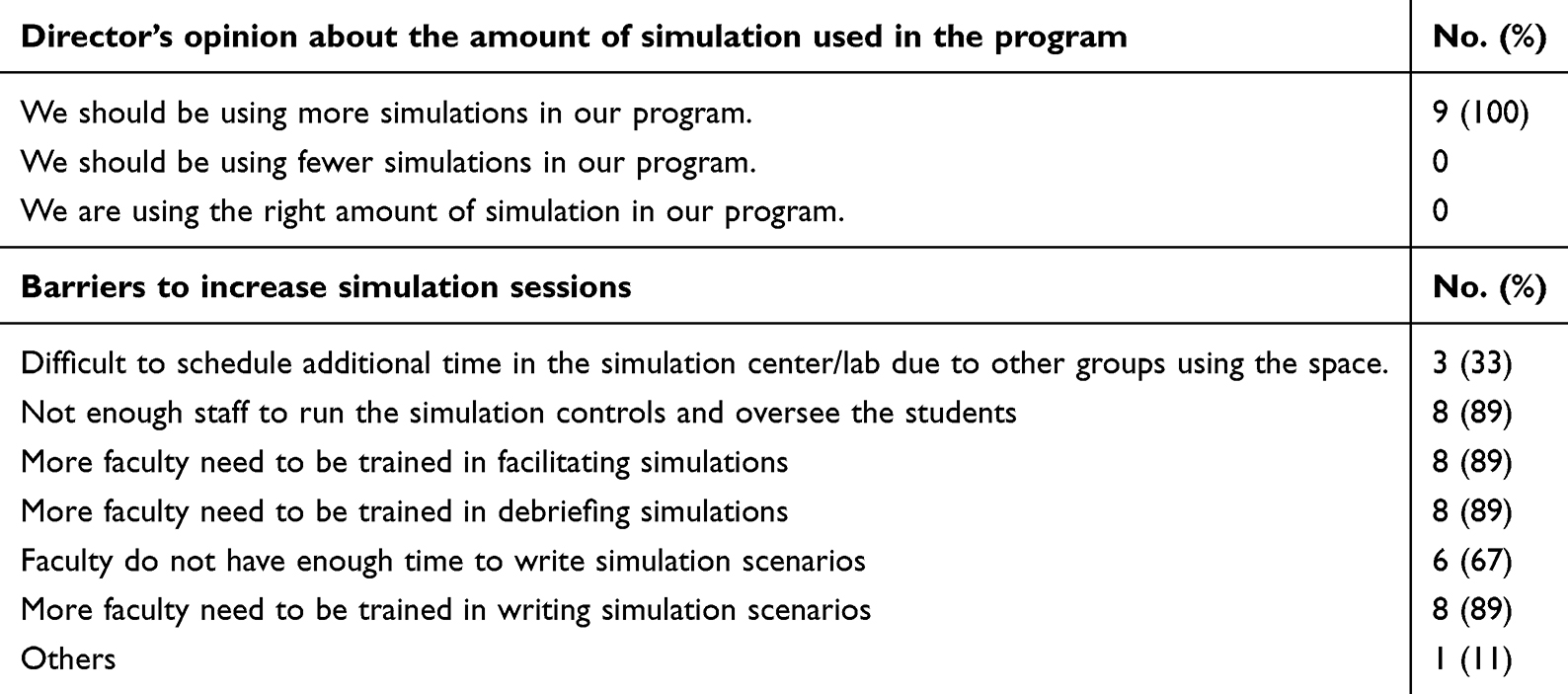 |
Table 8 Directors’ Opinions About the Amount of Simulation Needed and Barriers to Increase Simulation Sessions |
Table 9 shows there is a lack of knowledge about both the standards of healthcare simulation and the accreditation by the Society for Simulation in Healthcare. It also shows that majority of simulation centers are not accredited.
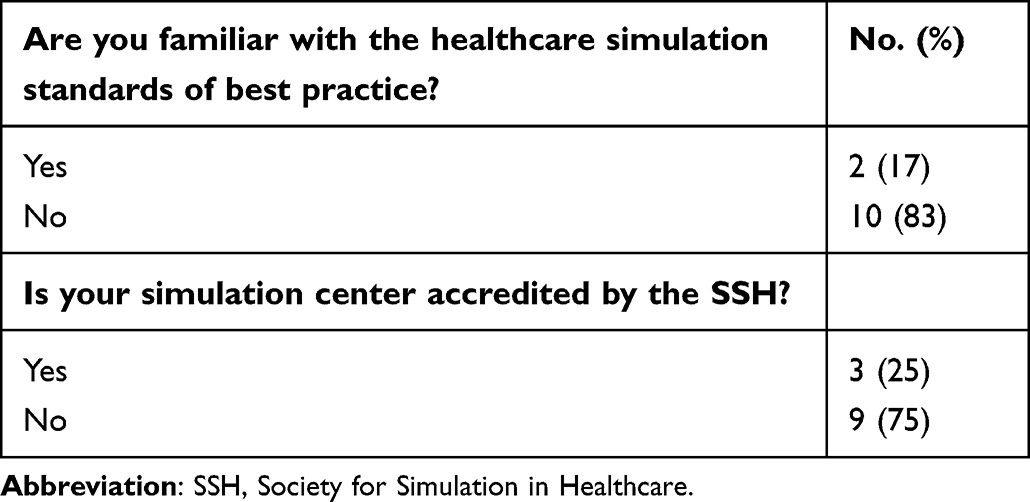 |
Table 9 SBL Guidelines and Accreditation |
Discussion
The present data show that majority of respiratory therapy programs in Saudi Arabia use at least one type of simulation, and high-fidelity simulation is the most predominant. High-fidelity simulation and task trainers are the most common types utilized within respiratory therapy curricula. Almost two-thirds of respiratory therapy programs utilize simulation within their departments. The present data imply that respiratory therapy programs’ directors and educators are investing in clinical simulation to improve clinical and nonclinical skills. Despite challenges and barriers that preclude maximum utilization of simulation, the present study offers evidence that some types of simulation is embedded within the respiratory therapy curriculums.
Debriefing is utilized by all respiratory therapy programs but considerably varied in time among these programs. Interestingly, the vast majority of respiratory therapy programs agree that simulation training hours should be counted toward clinical training. This would enable learners to enhance knowledge and master competencies with no risks to patients. It is well established that simulation is an excellent tool for learning and performance assessment.29–31 Therefore, more simulation training hours can safely replace clinical training hours. Also, directors of all respiratory therapy programs that utilize simulation in training agree that they need to invest more in simulation. They list shortage of staffing and lack of formal training among the most common barriers that preclude more utilization of simulation. Majority of programs’ directors state that faculty need to be trained in writing simulation scenarios, debriefing, and facilitating simulation.
The present investigation has shown that majority of respiratory therapy programs in Saudi Arabia utilize SBL. Similarly, it was reported that more than three-quarters of respiratory therapy programs in US utilize SBL.24 In both countries, the most common courses utilizing SBL are foundations of adult therapeutics, patient assessment, adult critical care, and neonatal and pediatric respiratory care. However, utilization of computer-based programs is more prominent in respiratory therapy programs in US than in Saudi Arabia. In US, limited development of faculty in simulation use is reported to be one of the major barriers to implement SBL. Almost, half of the respondents did not receive any faculty development in designing simulations, programming, and debriefing.24 Similarly, in the present data, 90% of the respondents indicate that there is a need to train faculty in simulation utilization. Proper faculty training in simulation has the potential to improve their knowledge, skills, and confidence. This presumably would improve the quality of simulation application and expand its utilization. We agree with Davis et al24 that lack of faculty development programs can be attributed to shortage of financial resources, time, or lack of recommendations that support usage of SBL in respiratory therapy programs.
It is clear that respiratory therapy programs are behind medicine and nursing programs in terms of utilizing simulation on their educational training. This is supported by the present data. This is also evident in the absence of faculty development programs that enable them to utilize simulations efficiently. The present data are in line with other studies indicating that lack of knowledge in simulation design, implementation, and debriefing among faculty are barriers which preclude more utilization of simulation in respiratory therapy programs.24,32 Therefore, implementation of faculty development programs in simulation are required. These programs should aim to improve knowledge and enhance skills in facilitating SBL, writing simulation scenarios, and conducting debriefing.
The nature of the respiratory therapy profession can be considered similar to anesthesiology. Both can be considered as hands-on specialties. In these specialties, the best way to master a competency, cognitive, skill, behavior, and attitude, is to practice it repeatedly.32 Thus, the most appropriate way to achieve this would be through more utilization of simulation. Simulation would enable learners to repeat the procedure as many as they need. However, it is common within the anesthesiology profession for simulation trainers to attend certain number of courses under supervision of expert trainers. This would help to enhance skills and recruit more novice trainers to be involved in simulation.32 Thus, several mini-workshops for faculty members with certification could increase utilization of simulation within respiratory therapy programs. It would help recruiting more faculty members to be involved in simulation. The faculty could maintain their certification with evidence of running at least one simulation course annually.
The current data show that majority of respiratory therapy programs lack sufficient knowledge about the healthcare simulation standards of best practice. Davis et al reported similar results. Only 28% of respiratory therapy programs in US are familiar with healthcare simulation standards.24 The authors suggested that familiarity of the best practice standards would enhance simulation practice and integration in the respiratory therapy academic programs. Also, our data show that 75% of the simulation laboratories/ centers are not accredited. It is known that the fundamental purposes of accreditation is to ensure high quality of the program and maintain this quality overtime. Accredited centers commonly maintain good structure, sufficient resources, and standardized practice.33
The limitations of the present investigation include the single time point of data collection. More details about barriers and challenges of SBL implementation would be useful. Also, it would be more appropriate to collect data from all respiratory therapy programs in Saudi Arabia. Nevertheless, we believe that the sample is sufficiently representative of respiratory therapy programs in Saudi Arabia.
Conclusion
The present data show that SBL is commonly utilized and relatively varied among respiratory therapy programs in Saudi Arabia. Overall, respiratory therapy programs have a good basis for SBL. However, a lack of formal training and a shortage of faculty were reported to be the major barriers for more SBL utilization.
Acknowledgments
This manuscript has not been published in part or entirety, or submitted for publication elsewhere in the same form, in English or in any other language. The authors are grateful to all directors of respiratory therapy programs for their valuable contribution. The authors are also grateful for Samantha Davis for her unlimited support and cooperation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cook DA, Hatala R, Brydges R, et al. Technology-enhanced simulation for health professions education: a systematic review and meta-analysis. JAMA. 2011;306(9):978–988. doi:10.1001/jama.2011.1234
2. Aggarwal R, Mytton OT, Derbrew M, et al. Training and simulation for patient safety. Qual Saf Health Care. 2010;19(Suppl 2):i34–43. doi:10.1136/qshc.2009.038562
3. Arias T, Tran A, Breaud J, et al. A prospective study into the benefits of simulation training in teaching obstetric vaginal examination. Int J Gynaecol Obstet. 2016;133(3):380–384. doi:10.1016/j.ijgo.2015.08.028
4. Martins RS, Sabzwari SR, Iqbal M. Effectiveness of simulation-based clinical skills training for medical students in respiratory medicine: a Pilot Study. J Coll Physicians Surg Pak. 2021;31(12):1468–1472. doi:10.29271/jcpsp.2021.12.1468
5. Dai C-P, Ke F. Educational applications of artificial intelligence in simulation-based learning: a systematic mapping review. Comput Educ. 2022;2022:100087.
6. Lababidi H, Al‑jubran K, AlAhmari M, et al. Establishing a clinical simulation centre: recommendations from an expert panel from the International Conference on Advanced Clinical Simulation, Dhahran, Saudi Arabia. J Health Specialties. 2015;3:1.
7. Al-Otaibi HM, AlAhmari MD. The respiratory care profession in Saudi Arabia: past and present. Ann Thorac Med. 2016;11(4):237–242. doi:10.4103/1817-1737.191872
8. Alotaibi G. Status of respiratory care profession in Saudi Arabia: a national survey. Ann Thorac Med. 2015;10(1):55–60. doi:10.4103/1817-1737.146878
9. Massoth C, Röder H, Ohlenburg H, et al. High-fidelity is not superior to low-fidelity simulation but leads to overconfidence in medical students. BMC Med Educ. 2019;19(1):29. doi:10.1186/s12909-019-1464-7
10. Saad Shaaban S, Salah hassan M, Hamdy Mohamed A. Comparison between low and high-fidelity simulation regarding nursing students’ self-confidence, achievement and satisfaction. Egypt J Health Care. 2021;12(3):1529–1546. doi:10.21608/ejhc.2021.197206
11. Al Khathlan N, Al Adhab F, Al Jasim H, Al Furaish S, Al Mutairi W, Al Yami BH. Simulation-based clinical education versus early clinical exposure for developing clinical skills in respiratory care students. Saudi J Med Med Sci. 2022;10(1):36–41. doi:10.4103/sjmms.sjmms_839_20
12. Cant RP, Cooper SJ. The value of simulation-based learning in pre-licensure nurse education: a state-of-the-art review and meta-analysis. Nurse Educ Pract. 2017;27:45–62. doi:10.1016/j.nepr.2017.08.012
13. Akaike M, Fukutomi M, Nagamune M, et al. Simulation-based medical education in clinical skills laboratory. J Med Invest. 2012;59(1,2):28–35. doi:10.2152/jmi.59.28
14. Macauley K, Brudvig TJ, Kadakia M, Bonneville M. Systematic review of assessments that evaluate clinical decision making, clinical reasoning, and critical thinking changes after simulation participation. J Phys Ther Educ. 2017;31(4):64–75. doi:10.1097/JTE.0000000000000011
15. Kalaniti K, Campbell DM. Simulation-based medical education: time for a pedagogical shift. Indian Pediatr. 2015;52(1):41–45. doi:10.1007/s13312-015-0565-6
16. McGaghie WC, Issenberg SB, Cohen ER, Barsuk JH, Wayne DB. Does simulation-based medical education with deliberate practice yield better results than traditional clinical education? A meta-analytic comparative review of the evidence. Acad Med. 2011;86(6):706–711. doi:10.1097/ACM.0b013e318217e119
17. Al-Mously N, Baalash A, Salem R, Mukaddam S. The proper timing to introduce simulation-based education in internal medicine clerkship. J Contemp Med Educ. 2014;2:180–184. doi:10.5455/jcme.20141016021437
18. Nuzhat A, Salem RO, Al Shehri FN, Al Hamdan N. Role and challenges of simulation in undergraduate curriculum. Med Teach. 2014;36(Suppl 1):S69–73. doi:10.3109/0142159X.2014.886017
19. Agha S, Alhamrani AY, Khan MA. Satisfaction of medical students with simulation based learning. Saudi Med J. 2015;36:731–736. doi:10.15537/smj.2015.6.11501
20. Marei HF, Al-Jandan BA. Simulation-based local anaesthesia teaching enhances learning outcomes. Eur J Dent Educ. 2013;17:e44–8. doi:10.1111/j.1600-0579.2012.00760.x
21. Warren J, Luctkar-Flude M, Godfrey C, Lukewich J. A systematic review of the effectiveness of simulation-based education on satisfaction and learning outcomes in nurse practitioner programs. Nurse Educ Today. 2016;46:1.
22. McKenna KD, Carhart E, Bercher D, Spain A, Todaro J, Freel J. Simulation Use in Paramedic Education Research (SUPER): a Descriptive Study. Prehosp Emerg Care. 2015;19:432–440. doi:10.3109/10903127.2014.995845
23. Hayden JK, Smiley RA, Alexander M, Kardong-Edgren S, Jeffries PR. The NCSBN National Simulation Study: a longitudinal, randomized, controlled study replacing clinical hours with simulation in prelicensure nursing education. J Nurs Regul. 2014;5(2):S3–S40. doi:10.1016/S2155-8256(15)30062-4
24. S PD, C FS, Willhaus JK. Simulation use in entry-into-practice respiratory care programs. Respir Care. 2022;67:676–681. doi:10.4187/respcare.08673
25. Hayden J. Use of simulation in nursing education: national survey results. J Nurs Regul. 2010;1:52–57. doi:10.1016/S2155-8256(15)30335-5
26. Dieckmann P, Molin Friis S, Lippert A, Ostergaard D. The art and science of debriefing in simulation: ideal and practice. Med Teach. 2009;31(7):e287–94. doi:10.1080/01421590902866218
27. Meakim C, Boese T, Decker S, et al. Standards of best practice: simulation standard I: terminology. Clin Simul Nurs. 2013;9(6):S3–S11. doi:10.1016/j.ecns.2013.04.001
28. Eppich WJ, Hunt EA, Duval-Arnould JM, Siddall VJ, Cheng A. Structuring feedback and debriefing to achieve mastery learning goals. Acad Med. 2015;90(11):1501–1508. doi:10.1097/ACM.0000000000000934
29. Gaba DM, Howard SK, Flanagan B, et al. Assessment of clinical performance during simulated crises using both technical and behavioral ratings. Anesthesiology. 1998;89(1):8–18. doi:10.1097/00000542-199807000-00005
30. Gupta A, Peckler B, Schoken D. Introduction of hi-fidelity simulation techniques as an ideal teaching tool for upcoming emergency medicine and trauma residency programs in India. J Emerg Trauma Shock. 2008;1(1):15–18. doi:10.4103/0974-2700.41787
31. Lateef F. Simulation-based learning: just like the real thing. J Emerg Trauma Shock. 2010;3(4):348–352. doi:10.4103/0974-2700.70743
32. Arab A, Alatassi A, Alattas E, et al. Integration of simulation in postgraduate studies in Saudi Arabia: the current practice in anesthesia training program. Saudi J Anaesth. 2017;11(2):208–214. doi:10.4103/1658-354X.203059
33. Ahmed RA, Wong AH, Musits AN, et al. Accreditation of simulation fellowships and training programs: more checkboxes or elevating the field? Simul Healthc. 2022;17(2):120–130. doi:10.1097/SIH.0000000000000593
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.