Back to Journals » Journal of Inflammation Research » Volume 18
Significance of Residual Inflammatory Risk and Persistent Inflammation in Patients with Myocardial Infarction with Nonobstructive Coronary Arteries
Authors Gao S, Huang S, Liu X, Yu M, Li W
Received 17 June 2025
Accepted for publication 27 September 2025
Published 6 October 2025 Volume 2025:18 Pages 13855—13868
DOI https://doi.org/10.2147/JIR.S547594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Side Gao,1 Sizhuang Huang,2 Xinming Liu,1 Mengyue Yu,2 Weiming Li1
1Heart Center and Beijing Key Laboratory of Hypertension, Beijing Chaoyang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China; 2Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100037, People’s Republic of China
Correspondence: Weiming Li; Mengyue Yu, Email [email protected]; [email protected]
Background: Inflammation as assessed by high-sensitivity C-reactive protein (hs-CRP) predicts cardiovascular outcomes independently of low-density lipoprotein cholesterol (LDL-C) levels even in statin-treated patients with coronary artery disease. However, data regarding implications of residual inflammatory risk in patients with myocardial infarction with nonobstructive coronary arteries (MINOCA) are lacking.
Methods: The present single-center cohort study prospectively enrolled 1062 patients with MINOCA stratified by the baseline hs-CRP (≥ 2 vs < 2 mg/L) and LDL-C (≥ 70 vs < 70 mg/dL). Change patterns of hs-CRP were identified in 792 patients with available hs-CRP at baseline and within 6– 12 months after index MI. The primary endpoint was major adverse cardiovascular events (MACE), a composite of death, nonfatal MI, stroke, revascularization, and hospitalization for unstable angina or heart failure.
Results: During the median follow-up of 41.7 months, patients with isolated residual inflammatory risk had the highest rate of MACE, followed by patients with combined cholesterol and inflammatory risk. At multivariate Cox model, residual inflammatory risk but not cholesterol risk was associated with an increased risk of MACE compared to those with no residual risk [hazard ratio (HR) 1.51; 95% confidence interval (CI): 1.17– 1.97, p=0.002]. The prognostic impact of hs-CRP ≥ 2mg/L remained significant in subgroup analysis, and particularly, in patients with well-managed LDL-C levels. Patients with persistently higher hs-CRP had a significantly higher risk of MACE than those with persistently low hs-CRP (HR 1.28; 95% CI: 1.09– 1.50, p=0.020).
Conclusion: Residual inflammation but not cholesterol risk drives poorer outcomes after MINOCA in the statin era, highlighting inflammation as a pivotal risk predictor and the necessity for anti-inflammatory strategies alongside LDL-C lowering.
Keywords: residual risk, inflammation, hs-CRP, LDL-C, myocardial infarction with nonobstructive coronary arteries, cardiovascular outcomes
Graphical Abstract:

Introduction
Myocardial infarction with nonobstructive coronary arteries (MINOCA) refers to a distinct population who have an acute myocardial infarction (AMI) with evidence of myocardial ischemia, but coronary angiography shows no significant obstruction in major coronary arteries.1,2 Recently, it has been increasingly recognized and occurs in 5% to 10% of patients with AMI.3 Although patients with MINOCA are younger and have fewer comorbidities than those with AMI and obstructive coronary artery disease (CAD), they are still at considerable risks for long-term cardiovascular (CV) events even after optimal medical therapies.4–7 Thus, the intensified management of residual risk factors should be addressed for outcome improvement in this population.
Current evidence has solidly confirmed the essential role of low-density lipoprotein cholesterol (LDL-C) in the development of CAD.8 To date, the “lower is better for LDL-C and CV risk” concept has been widely applied in daily practice, and achieving sustained LDL-C reduction to guideline-recommended levels remains a cornerstone in the treatment of CAD.9 However, targeting LDL-C alone is unlikely to completely eliminate risk as nearly one-third of patients is still at high risk of future CV events despite intensified LDL-C lowering strategies with statin or combination therapy.10,11 Beyond LDL-C, growing data have demonstrated that inflammation is a key driver of atherogenesis, plaque vulnerability, and CV risk.12,13 Recent studies confirmed that residual inflammation assessed by high-sensitivity C-reactive protein (hs-CRP) was a more robust predictor of CV events than LDL-C levels in statin-treated patients with CAD.14,15 Targeted anti-inflammatory agents also showed significant benefits when added to statin therapy, leading to an additional reduction in CV risk.16–18
To date, data are scarce regarding the prognostic value of residual cholesterol and inflammatory risk in patients with MINOCA. To address this issue, we analyzed the impact of residual inflammation and cholesterol risk on long-term CV outcomes after MINOCA, and explored if elevated hs-CRP still served as a risk predictor in patients with well-managed metabolic profiles. We further evaluated the association between persistent inflammation and CV risk in a subset of patients.
Methods
Study Population
The present prospective cohort study enrolled patients with MINOCA at a national tertiary center (Fuwai hospital) from Jan. 2015 to Dec. 2019, as previously reported.7 MINOCA were diagnosed if patients met the 4th universal definition of AMI19 and had no obstructive CAD, as confirmed by angiography with coronary artery stenosis of less than 50%.1,2 In line with the updated evidence, we primarily enrolled MINOCA patients with coronary-related causes, of which atherosclerotic mechanisms constitute the majority of MINOCA etiologies as assessed by angiography with the presence of any coronary plaque (even with <50% stenosis). In some cases, plaque disruption was further identified by intravascular imaging such as optical coherence tomography (OCT). The prevailing atherosclerotic subtype in our cohort was consistent with prior studies showing that atherosclerosis is the major contributor to MINOCA pathogenesis.1–3 Individuals with symptoms resembling MI, myocardial injury of non-coronary origin, and no ischemic features (eg, acute heart failure or myocarditis) were excluded. Still, other coronary-related causes of MINOCA (eg, vasospasm, spontaneous dissection) may occur alongside the atherosclerotic subtype, though they constitutes only a small proportion. Due to limited availability of advanced multi-modal imaging in the study setting, the exact etiologies of MINOCA in each patient were not adequately captured.
Individuals with missing data of LDL-C at baseline and those lacking hs-CRP level tests within 1–3 months after MI were excluded. Patients with recent infection, sepsis, markedly elevated hs-CRP (≥20mg/L) and long-term use of anti-inflammatory agents were also excluded. After screening, a total of 1062 eligible MINOCA patients with or without ST-segment elevation (STEMI or NSTEMI) were finally included in the analysis (Figure 1). Patients were separated into 4 groups based on their baseline LDL-C (tested during hospitalization) and hs-CRP levels (measured within 1–3 months after MI) as follows: no residual risk (LDL-C <70 mg/dL + hs-CRP <2 mg/L), residual cholesterol risk (RCR, LDL-C ≥70 mg/dL + hs-CRP <2 mg/L), residual inflammatory risk (RIR, LDL-C <70 mg/dL + hs-CRP ≥2 mg/L), and combined residual cholesterol and inflammatory risk (RCIR, LDL-C ≥70 mg/dL + hs-CRP ≥2 mg/L). The present classification aligned with the approaches used in previous studies.10–15 There were 792 patients who had available hs-CRP tests both at baseline and within 6–12 months after index MI. The change patterns of hs-CRP were classified in this sub-cohort as follows: persistently low hs-CRP (hs-CRP <2 mg/L both at baseline and follow-up), elevated hs-CRP (hs-CRP <2 mg/L at baseline and ≥2 mg/L at follow-up), reduced hs-CRP (hs-CRP ≥2 mg/L at baseline and <2 mg/L at follow-up), and persistently high hs-CRP (hs-CRP ≥2 mg/L both at baseline and follow-up). All the patients were prescribed guideline-directed medical therapies unless contraindicated, including dual anti-platelet therapy (DAPT), statins, β-blockers, and angiotensin-converting enzyme inhibitor/angiotensin receptor blocker. This observational study was approved by the Institutional Review Board of Fuwai hospital and performed in compliance with the Declaration of Helsinki. All patients provided written informed consent to participate.
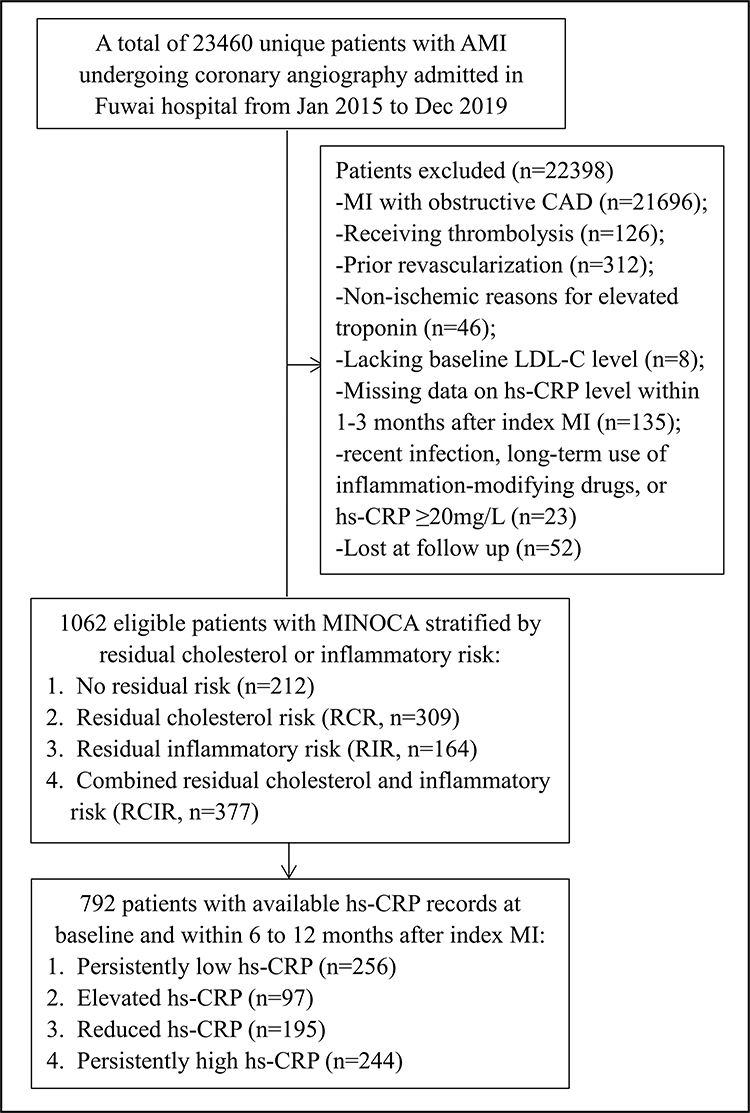 |
Figure 1 Study flowchart. |
Data Collection and Definitions
Data on the baseline characteristics and medications were obtained from electronic medical records. Blood samples for biochemical tests were collected after 12 hours of overnight fasting. Blood glucose and lipid parameters such as triglyceride (TG), total cholesterol, LDL-C, high-density lipoprotein cholesterol (HDL-C) and lipoprotein(a) were tested using an automatic biochemistry analyzer, with a coefficient of variation of <5% and a total imprecision of <10%. LDL-C was calculated using the Friedewald formula, and hs-CRP was tested by Beckman Assay 360 clinical chemistry analyzer (Beckman Coulter, Brea, CA) with a detection limit of 0.1 mg/L and an intra-assay coefficient of variation of ≤6%. Peak troponin I (TnI) level and N-terminal pro-B-type natriuretic peptide (NT-proBNP) values at admission were recorded. Left ventricular ejection fraction (LVEF) was measured by echocardiography. The comorbidities (eg hypertension, diabetes, dyslipidemia) were ascertained according to current guidelines via medical documentation, laboratory tests, and use of medications. The multi-modal imaging (eg, OCT or cardiac magnetic resonance [CMR]) and invasive measurement of index of microcirculatory resistance (IMR) were performed in only a small subset of selected patients, which might compromise the accuracy of etiology identification and plaque detection. Despite this, we relied on routinely accessible approaches (eg, echocardiography, re-evaluation of angiograms, ventriculography for identifying left ventricular motion abnormalities, and coagulation tests in suspicious cases to rule out thrombophilia) to clarify the underlying causes of MINOCA as accurately as possible.
The major study exposure was residual cholesterol or inflammatory risk as assessed by LDL-C or hs-CRP levels at baseline. In our cohort, LDL-C values obtained during hospitalization were considered the baseline level, and hs-CRP levels were measured dynamically during hospitalization and after discharge as a routine clinical practice. Previous studies often used a single value of hs-CRP to define inflammation; however, hs-CRP levels often fluctuate in response to MI or such stress conditions and then be stable over time after 4–6 weeks post MI. Given the variability of hs-CRP in the acute phase of MI, the hs-CRP levels at a later phase (1–3 months after the index MI) rather than hs-CRP levels at admission were collected and regarded as the baseline level. To minimize the confounding of elevated hs-CRP caused by acute infection, we excluded patients with infective diseases, sepsis, hs-CRP ≥20mg/L, and long-term use of drugs that modify systemic inflammation (eg, antibiotics, non-steroidal anti-inflammatory drugs, corticosteroids, or immunosuppressive drugs). In addition, approximately 74% of patients had available hs-CRP tests within 6–12 months after MI, and the changing patterns of hs-CRP were identified in this sub-cohort. Although the optimal definition of residual inflammatory risk in post-MI patients has not been established in current guidelines, we chose the well-recognized cutoff of hs-CRP ≥2 mg/L as this threshold has been widely used in both observational studies and randomized controlled trials.
Endpoints and Follow-up
The primary endpoint was defined as a composite of major adverse cardiovascular events (MACE), including all-cause death, nonfatal spontaneous MI, nonfatal stroke, ischemia-driven unplanned revascularization, and hospitalization for unstable angina (UA) or heart failure (HF). The MACE was assessed in a time-to-first-event analysis. The secondary endpoints included each component of MACE and the composite hard endpoint of death, reinfarction, stroke or revascularization. Recurrent MI was defined according to the fourth universal definition of MI.19 Stroke was diagnosed as loss of neurological dysfunction caused by an ischemic or hemorrhagic event with symptoms lasting ≥24h.20 Revascularization was carried out at the discretion of the operators if patients had ischemia and obstructive coronary arteries. Hospitalization for UA with objective evidence of ischemia indicated a high risk of plaque instability and a threat to patients’ CV health. Hospitalization for HF, to some extent, reflected deterioration of cardiac function and life quality after MI. Patients were followed up through clinic visits or via telephone contact at 6 months, 1 year, and yearly thereafter until the end of observation period using a pre-designed structured questionnaire. Information from additional clinic visits or unplanned hospital admissions were recorded as appropriate. Incident events outside of Fuwai hospital were gathered via telephone interviews and verified with medical records from external providers. All the follow-up information were cross-checked and confirmed by a team of trained and independent researchers. The expert cardiologists and statisticians who were blinded to the study design would adjudicate all the adverse events to ensure data accuracy and reliability.
Statistical Analysis
Baseline profiles were reported as mean and standard deviation (SD) or median and interquartile range for continuous variables and percentages for categorical variables. Comparisons were performed using the analysis of variance, Kruskal–Wallis H-test, Pearson’s χ2 or Fisher’s test as appropriate. The cumulative incidence of MACE was analyzed using Kaplan–Meier curves, and comparisons were assessed by Log rank test. The univariable and multivariable Cox regression models were constructed to analyze the impact of residual inflammatory or cholesterol risk and persistent inflammation on the risk of MACE. The hazard ratio (HR) and its 95% confidence interval (CI) were calculated. The subgroup of patients with no residual inflammatory or cholesterol risk and the subset of patients with persistently low hs-CRP served as references. Several clinically relevant and unevenly distributed covariates were parsimoniously enrolled in multivariable Cox model, including age, sex, BMI, MI type (STEMI or NSTEMI), LVEF, hypertension, and diabetes. The other covariates such as fasting glucose, peak TnI, NT-proBNP and medications were comparable among the groups and were not included. Potential confounders, including lifestyles and the intensity and adherence to lipid-lowering therapy, were unmeasured. The prognostic impact of hs-CRP ≥2mg/L was further analyzed in subgroup analysis. Restricted cubic splines (RCS) were used to show a dose-response relationship between baseline hs-CRP and risk of MACE, in which the reference value (HR=1) was defined at the median level of hs-CRP and the four knots were set at the 5th, 35th, 65th, and 95th percentiles. All the analyses were performed by the SPSS (version 22.0) and R Software (version 4.0.2), and statistical significance was considered if two-tailed P < 0.05.
Results
Baseline Characteristics
The mean age of the cohort was 55.7±11.8 years and 74.0% were men. Coronary atherosclerosis appeared to be the leading cause of MINOCA in our cohort. Findings of multi-modal imaging and other diagnostic tests performed in a small proportion of patients were shown in Table S1. The median hs-CRP and LDL-C levels were 2.2 mg/L (IQR: 1.0–5.7) and 85.1 mg/dL (68.8–104.9), respectively. The distribution of baseline hs-CRP and the temporal changes in hs-CRP from baseline to follow-up were depicted (Figures S1 and S2). In total, 50.9% of patients had baseline hs-CRP ≥2 mg/L and 64.5% had LDL-C ≥70 mg/dL. Patients were further classified as no residual risk (19.9%), RCR (29.0%), RIR (15.4%) and RCIR (35.4%) groups (Figure 1). The baseline characteristics of these groups were presented in Table 1. As shown, the BMI, LVEF, hs-CRP and lipid levels were different among the 4 groups, while the demographics, presence of STEMI, comorbidities and medications did not differ significantly. The profiles and CV outcomes in patients stratified solely by baseline hs-CRP levels were shown in Supplementary Materials (Tables S2 and S3).
 |
Table 1 Baseline Characteristics in Patients Stratified by Residual Cholesterol or Inflammatory Risk |
Residual Cholesterol or Inflammatory Risk and Clinical Outcomes
Over the median follow-up of 41.7 months, 162 patients developed MACE (18 died, 40 suffered reinfarction, 12 had stroke, 44 had revascularization, 66 were hospitalized for UA and 45 for HF). Individuals with RIR had the highest rate of MACE (22.5%), followed by patients with RCIR (18.0%), RCR (11.0%) and no residual risk (10.8%) (Table 2). The Kaplan–Meier curves further showed a higher cumulative incidence of MACE in patients with hs-CRP ≥2 mg/L and in RIR group (Figure 2). At multivariable Cox analysis, elevated hs-CRP was independently associated with an increased risk of MACE (for 1 unit increase in hs-CRP, HR 1.06; 95% CI: 1.02–1.11, p=0.001; hs-CRP ≥2 mg/L vs <2 mg/L: HR 1.77; 95% CI: 1.29–2.43, p<0.001). Also, the adjusted risk of MACE was significantly higher in patients with RIR (HR 1.51; 95% CI: 1.17–1.97, p=0.002) and RCIR (HR 1.19; 95% CI: 1.01–1.39, p=0.030) than in patients with no residual risk; yet isolated RCR was not associated with the outcomes (Table 3). The impact of hs-CRP ≥2 mg/L on MACE risk remained significant in subgroup analysis (Figure 3). The RCS model showed a near-linear relationship between baseline hs-CRP level and risk of MACE (Figure S3), and analyses on the composite hard endpoints were consistent with the primary analysis of MACE (Table S4). Notably, among patients with traditional risk factors below the target level (eg, TG<150mg/dL, lipoprotein(a) <30mg/dL, LDL-C <70mg/dL, HbA1c <7% in diabetes or <5.7% in non-diabetes), residual inflammation defined by hs-CRP ≥2 mg/L still predicted MACE risk (Figure S4). These data indicated a robust association of residual inflammatory risk with MACE in MINOCA population, irrespective of LDL-C level and the other known risk factors.
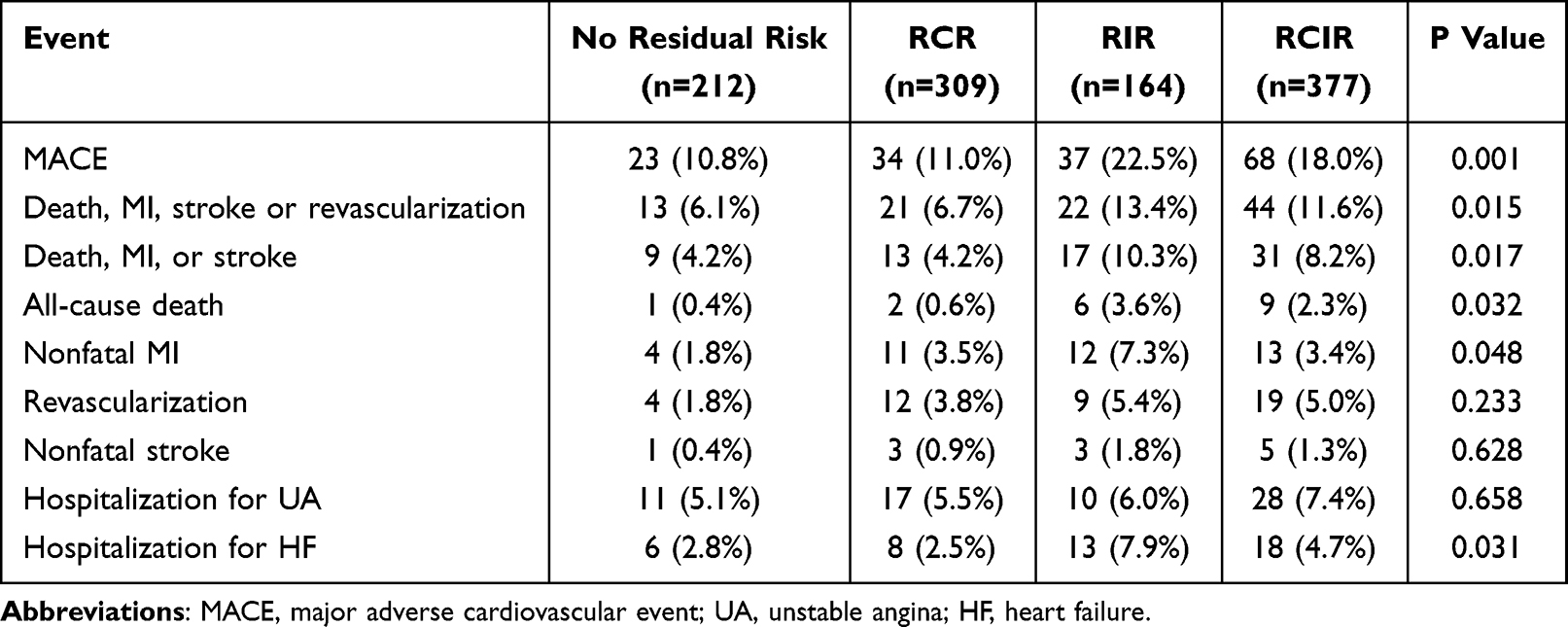 |
Table 2 Clinical Outcomes in Patients Stratified by Residual Cholesterol or Inflammatory Risk |
 |
Table 3 Relation Between Hs-CRP Levels at Admission and Risk of MACE |
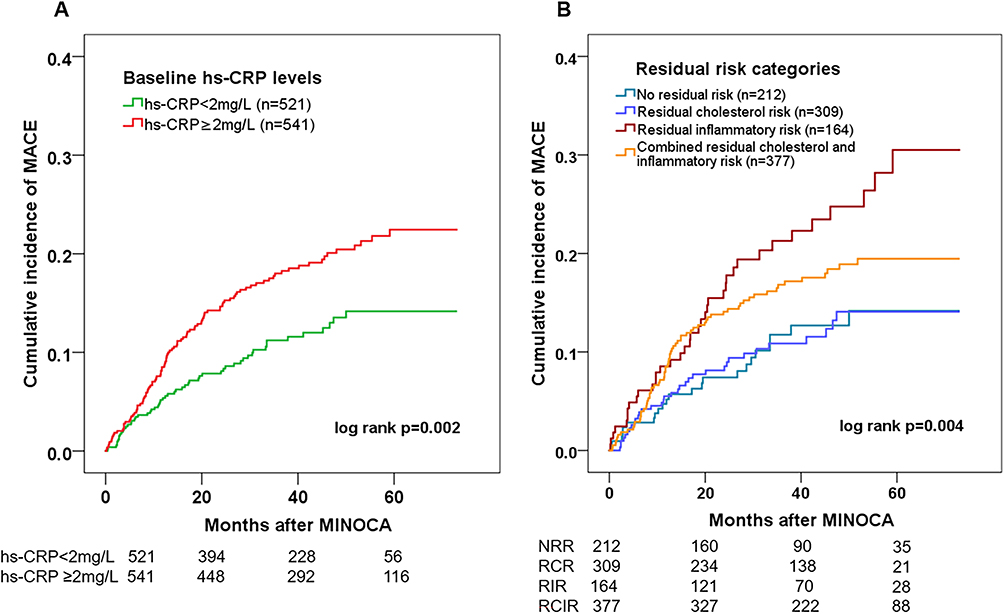 |
Figure 2 Incidence of MACE in patients stratified by residual inflammatory and cholesterol risk. Kaplan–Meier curves showing cumulative incidence of MACE in patients stratified by baseline hs-CRP levels at the cutoff of 2mg/L (A) and by residual inflammatory and cholesterol risk at the cutoff of 2mg/L for hs-CRP and of 70mg/dL for LDL-C (B). |
 |
Figure 3 Subgroup analysis for the impact of elevated baseline hs-CRP. Impact of elevated baseline hs-CRP (≥2mg/L vs <2mg/L) in subgroups stratified by the sex, age, BMI, MI classification (NSTEMI or STEMI), history of hypertension, diabetes, and dyslipidemia. The risk of MACE in each subgroup was analyzed using univariable Cox regression analysis. The vertical dotted line indicated HR value of 1. |
The Impact of Persistent Inflammation on Clinical Outcomes
In a subset of 792 patients with available hs-CRP at baseline and 6–12 months after MINOCA, 32.3% of them had persistently low hs-CRP, 13.5% had increased hs-CRP, 23.3% had reduced hs-CRP, and 30.8% had persistently elevated hs-CRP (Figure 1). The highest rate of MACE was observed in those with persistently high hs-CRP (Figure 4A and Table S5). This subgroup had a significantly higher risk of MACE after multivariable adjustment (HR 1.28; 95% CI: 1.09–1.50, p=0.020), whereas those with increased or reduced hs-CRP had similar outcomes to those with persistently low hs-CRP (Figure 4B). These data highlighted the role of low-grade inflammation persisting in the late phase after AMI.
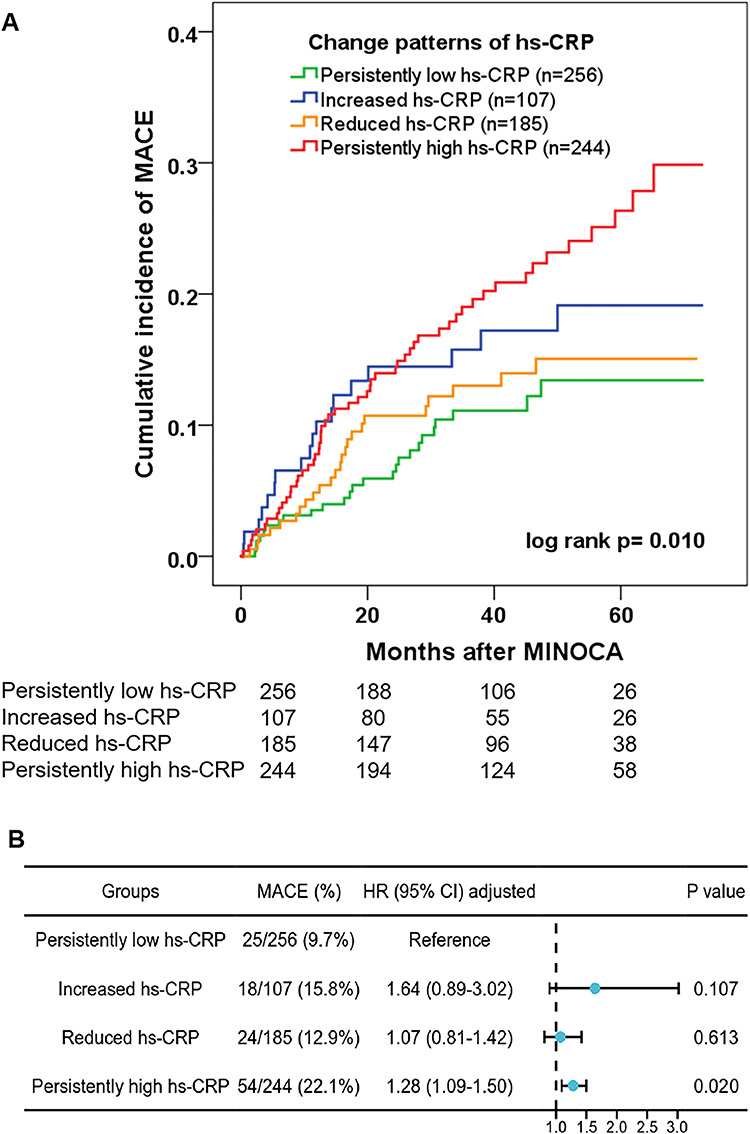 |
Figure 4 Relationship between change patterns of hs-CRP and risk of MACE. The change patterns of hs-CRP were identified as 4 types in a subset of 792 patients based on hs-CRP levels at baseline and follow-up (6–12 months after MI) at the cutoff of 2mg/L. Persistently high hs-CRP indicated hs-CRP ≥2 mg/L both at baseline and at follow-up. Cumulative incidence of MACE was shown by Kaplan–Meier curves (A). Associations between change patterns of hs-CRP and risk of MACE were assessed by multivariable Cox regression analysis (B). |
Discussion
In the present study, we found that residual inflammatory risk instead of cholesterol risk was significantly associated with an increased risk of MACE in a contemporary cohort of MINOCA despite the optimal medical therapies. The impact of hs-CRP was independent of LDL-C and known risk factors, and elevated hs-CRP still conferred a higher risk of MACE in statin-treated individuals with well-controlled lipid profiles. Further, patients with persistently high hs-CRP had a poorer prognosis as compared to those with persistently low hs-CRP. These results support previous findings regarding the deleterious effects of inflammation in CAD, and particularly underscore the value of residual inflammatory risk and persistent inflammation in MINOCA population.
MINOCA represents a heterogeneous clinical entity caused by diverse mechanisms, including plaque rupture, plaque erosion, coronary spasm, embolization, spontaneous dissection and microvascular dysfunction.1,2 It is crucial to conduct a comprehensive diagnostic workup to identify the underlying causes of MINOCA, as it facilitates risk stratification and tailored therapies. A multi-modal imaging study incorporating OCT and CMR found that the causes of MINOCA were often similar to mechanisms of MI with obstructive CAD, that is, atherosclerosis and plaque instability.21 Another OCT study reported the detection of plaque rupture, erosion, and calcified nodules in 44%, 31%, and 8% of cases, respectively.22 Other non-ischemic causes such as coronary artery spasm or dissection also contribute to the occurrence of MINOCA. Consistently, atherosclerotic subtype was observed in the majority of our cohort, of which only a minority of patients underwent multi-modal evaluations, including OCT, CMR, IMR, ventriculography, provocative spasm test, and thrombophilia screening. Such methods merit emphasis in refining etiological classification. In general, the optimal prevention medications for MINOCA were similar to those used in broader population with AMI. Even though, the etiology-driven personalized therapies should be noted. For instance, DAPT is indicated for most thrombotic MINOCA subtypes; however, it may not be suitable for patients without atherosclerosis or endothelial dysfunction. In some cases, DAPT was prescribed in high-risk patients before the cause is confirmed and served as a safe “bridge” during diagnostic uncertainty to address thrombotic risk in acute settings. The long-term outcomes of MINOCA are not necessarily benign and deserve more attention given a considerably high risk of adverse events in this population.4–7 Previous studies even showed that patients with MINOCA had a risk of death similar to or higher than those with MI and obstructive CAD.5,6 Here, 15.2% of patients in our cohort developed MACE despite the evidence-based optimal therapies. Nearly all the participants received statins, yet 64.5% of patients still had LDL-C levels higher than 70 mg/dL. Meanwhile, 50.9% of patients had elevated hs-CRP with the median hs-CRP level being 2.2 mg/L. Consistently, a Swedish study showed that hs-CRP ≥2 mg/L was seen in more than 60% of patients after 30 days of AMI.23 A large-scale analysis also revealed that more than half of statin-treated participants had hs-CRP ≥2 mg/L with the median hs-CRP levels ranging from 2.1 to 2.3 mg/L.14 In this context, residual inflammatory risk is highly prevalent in CAD populations and its role should be highlighted in the contemporary management of MINOCA patients.
Current evidence has clearly clarified the crucial role of LDL-C in the development of CAD and confirmed the dose-dependent relationship between LDL-C lowering and improved outcomes.8,9 However, even if very low LDL-C levels are achieved with intensive LDL-C lowering strategies using a combination of statins with ezetimibe or PCSK-9 inhibitors, a substantial residual risk for adverse events still persists.10,11 As reported in FOURIER trial, the composite of cardiac death, MI, or stroke occurred in 5.9% of patients during follow-up of 2.2 years in the evolocumab subgroup even after a significant reduction of LDL-C to a median of 30 mg/dL.24 More recently, research has found that inflammation should be responsible for this substantial residual risk. A collaborative analysis of three randomized trials reported that hs-CRP was a stronger indicator of adverse events than LDL-C levels in 31,245 patients receiving statins.14 Another analysis revealed that residual inflammatory risk but not cholesterol risk was associated with MACE risk in 15494 statin-treated patients undergoing percutaneous coronary intervention (PCI).15 Meanwhile, elevated hs-CRP predicted CV risk and death more strongly than LDL-C among high-risk patients with statin intolerance.25 Recent studies also demonstrated that hs-CRP was a more powerful predictor for CV events than LDL-C in various subpopulations with CAD, including stable CAD, acute coronary syndrome, and all-comers undergoing PCI.26–29 In line with prior findings, we found that residual inflammation defined by hs-CRP ≥2 mg/L rather than LDL-C was an independent driver of MACE in MINOCA. This effect was largely consistent in subgroup analysis, and hs-CRP remained a predictor of MACE in patients who had achieved the guideline-recommended targets for LDL-C and other risk determinants. A near-linear relationship between hs-CRP levels and risk of MACE was identified. These data addressed the role of residual inflammation as a key contributor to CV risk in MINOCA population. Despite the existing literature, our analysis has novel insights. First, a fundamentally different patient cohort was recruited, and so far, few data have addressed the impact of residual cholesterol and inflammatory risk in this population. Second, most studies reported hs-CRP using a single measurement at admission. Here, hs-CRP values recorded at a later phase (1–3 months post AMI) were defined as the baseline level considering the fluctuations of hs-CRP in acute settings and its stability 4–6 weeks after AMI. We further analyzed the temporal change of hs-CRP in a subset cohort and demonstrated a close association of persistently high hs-CRP with worse outcomes. This finding indicates the latent harm of persistent low-grade inflammation smouldering in the late phase of MINOCA and supports the concept that “the longer chronic inflammation persists, the higher the CV risk becomes”.30
Despite the solid evidence indicating inflammation as a key driver of residual risk, the importance of “lower is better” approach for LDL-C management should not be diminished given the fundamental role of lipid lowering in secondary prevention. The clinical trials and guidelines have recommended statin or adding other lipid-lowering medication such as ezetimibe, PCSK9 inhibitors, or bempedoic acid to further reduce LDL-C level and CV risk.8–10 Statins also have the ability to lower the inflammatory burden beyond the lipid-lowering properties.31 Therefore, LDL-C-targeted strategies should remain one of the cornerstones in the treatment of CAD. However, the existing CV risk in statin-treated patients highlights the role of residual inflammatory risk and provides a rationale for anti-inflammatory treatments in patients with CAD.
To date, anti-inflammatory agents including canakinumab and colchicine have been demonstrated to decrease CV risk. The CANTOS trial first proved that the risk of CV events in patients with a history of MI and elevated hs-CRP was significantly lower in those who received interleukin-1β antibody (canakinumab) than in those without it.16 More recently, the COLCOT and LODOCO2 trials showed that low-dose colchicine safely lowered MACE rate by 31% among patients with stable CAD and by 23% after recent AMI.17,18 These magnitudes of benefit are larger than those in contemporary trials of adjunctive lipid-lowering agents.32,33 A meta-analysis reported a substantial reduction in adverse events by colchicine in patients with acute or chronic coronary syndrome.34 The individual lifetime benefits of colchicine in patients with chronic CAD even outperformed the intensified LDL-C reduction to 1.4 mmol/L and systolic blood pressure reduction to 130 mmHg.35 Yet, the CLEAR SYNERGY trial failed to show a reduction in MACE in AMI patients who received colchicine.36 Hence, the benefit of colchicine in AMI needs to be further validated by future trials. Currently, the most applicable anti-inflammatory agent for vascular protection is oral colchicine 0.5 mg daily.32 Newer agents like IL-6 inhibitors are being investigated by ongoing trials.37 Of note, inflammation inhibition and lipid lowering are not contradictory but are synergistic.33 The combined LDL-C lowering and anti-inflammatory treatments may become standard of care for most atherosclerotic patients in the future.38
Our study has several clinical implications. First, hs-CRP levels can be dynamically measured as a routine in patients with MINOCA for better risk stratification. A higher baseline hs-CRP and persistently elevated hs-CRP could indicate a greater likelihood of developing MACE. Yet, hs-CRP is a systemic biomarker and may be inadequate to capture the heterogeneous inflammatory profiles. Second, assessment of hs-CRP may facilitate pre-emptive decision-making and treatment strategies. For those with higher residual inflammatory risk, clinicians may consider a more tailored, biomarker-guided approach by combining anti-inflammatory and LDL-C-targeted agents. This approach is helpful for identifying MINOCA patients as a suitable target group who are likely to gain clinical benefits from the combination therapy. Third, our analysis showed an independent effect of hs-CRP, separate from with the other residual risk determinants such as LDL-C, TG, lipoprotein (a), and HbA1c. In patients who had well-controlled metabolic profiles but elevated hs-CRP levels, initiating anti-inflammatory therapy is reasonable and may confer additional CV benefits beyond the conventional secondary prevention therapies. Future research is warranted to elucidate the intricate interplay between inflammation, metabolic dysfunctions, and CV outcomes.
Limitation
Several limitations should be acknowledged. First, this was a single-center study with relatively small sample size and potential selection bias. Our results may not be representative and need to be validated and generalized in future nationwide studies. Second, we mainly studied the composite endpoint as MACE, and the limited number of each hard endpoint may not be sufficient for statistical significance. Third, detailed data on the intensity and duration of statins were not available. Newer lipid-lowering drugs and anti-inflammatory medications were not assessed as they became available during the latter part of the study period and were prescribed to only a few patients at the time of admission. Fourth, despite multivariable adjustment and subgroup analysis, potential unmeasured confounding factors may exist and thus bias the results because of the observational study design. Fifth, given the low usage of intravascular imaging and CMR, the exact causes of MINOCA in each patient were not adequately captured. This diagnostic limitation is inherent to our study design which relied on conventional diagnostic tools rather than comprehensive multi-modal approaches and may lead to under-diagnosis of subtle atherosclerosis and other mechanisms. Future research with multimodal imaging and functional assessment is needed to address this issue. Lastly, the change patterns of hs-CRP were identified based on available hs-CRP levels at two time periods, yet the real-time changes of hs-CRP and its cumulative levels were not recorded. Furthermore, inflammatory markers other than hs-CRP such as interleukin and cytokines were not measured, which may restrict a comprehensive understanding of the inflammatory profiles in this population.
Conclusions
Residual inflammatory risk quantified by hs-CRP ≥2mg/L was an independent risk factor of MACE in patients with MINOCA, irrespective of LDL-C levels. This effect was largely consistent in subgroup analysis, and particularly, in statin-treated patients with well-controlled lipid profile. Persistent post-MI inflammation defined by hs-CRP ≥2mg/L both at baseline and follow-up was a major driver for adverse outcomes after MINOCA even after adherence to guideline-directed secondary preventive measures.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Mengyue Yu) upon reasonable request.
Ethics Approval
This study was approved by the Ethics Committee of Fuwai hospital (No. 2014-617). Written informed consent was obtained from all patients.
Acknowledgments
We thank our team members for their invaluable contributions to this cohort study.
Funding
This study was supported by Beijing Chao-Yang Hospital Golden Seeds Foundation (CYJZ202210), and National Clinical Key Specialty Construction Project: Cardiology (Coronary Artery Disease) (“1+N” Discipline Cluster Model).
Disclosure
The authors declare that they have no competing interests that could influence the work in this paper.
References
1. Agewall S, Beltrame JF, Reynolds HR, et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. 2017;38(3):143–153. doi:10.1093/eurheartj/ehw149
2. Tamis-Holland JE, Jneid H, Reynolds HR, et al. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: a Scientific Statement From the American Heart Association. Circulation. 2019;139(18):e891–e908. doi:10.1161/CIR.0000000000000670
3. Pasupathy S, Air T, Dreyer RP, et al. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131(10):861–870. doi:10.1161/CIRCULATIONAHA.114.011201
4. Bainey KR, Welsh RC, Alemayehu W, et al. Population-level incidence and outcomes of myocardial infarction with non-obstructive coronary arteries (MINOCA): insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int J Cardiol. 2018;264:12–17. doi:10.1016/j.ijcard.2018.04.004
5. Andersson HB, Pedersen F, Engstrøm T, et al. Long-term survival and causes of death in patients with ST-elevation acute coronary syndrome without obstructive coronary artery disease. Eur Heart J. 2018;39(2):102–110. doi:10.1093/eurheartj/ehx491
6. Planer D, Mehran R, Ohman EM, et al. Prognosis of patients with non-ST-segment-elevation myocardial infarction and nonobstructive coronary artery disease: propensity-matched analysis from the Acute Catheterization and Urgent Intervention Triage Strategy trial. Circ Cardiovasc Interv. 2014;7(3):285–293. doi:10.1161/CIRCINTERVENTIONS.113.000606
7. Gao S, Xu H, Ma W, et al. Remnant Cholesterol Predicts Risk of Cardiovascular Events in Patients With Myocardial Infarction With Nonobstructive Coronary Arteries. J Am Heart Assoc. 2022;11(10):e024366. doi:10.1161/JAHA.121.024366
8. Borén J, Chapman MJ, Krauss RM, et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: pathophysiological, genetic, and therapeutic insights: a consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J. 2020;41(24):2313–2330. doi:10.1093/eurheartj/ehz962
9. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2020;41(1):111–188. doi:10.1093/eurheartj/ehz455
10. Tokgözoğlu L, Libby P. The Dawn of a new era of targeted lipid-lowering therapies. Eur Heart J. 2022;43(34):3198–3208. doi:10.1093/eurheartj/ehab841
11. Patel KV, Pandey A, de Lemos JA. Conceptual Framework for Addressing Residual Atherosclerotic Cardiovascular Disease Risk in the Era of Precision Medicine. Circulation. 2018;137(24):2551–2553. doi:10.1161/CIRCULATIONAHA.118.035289
12. Waksman R, Merdler I, Case BC, et al. Targeting inflammation in atherosclerosis: overview, strategy and directions. EuroIntervention. 2024;20(1):32–44. doi:10.4244/EIJ-D-23-00606
13. Bäck M, Yurdagul Jr A, Tabas I, et al. Inflammation and its resolution in atherosclerosis: mediators and therapeutic opportunities. Nat Rev Cardiol. 2019;16(7):389–406. doi:10.1038/s41569-019-0169-2
14. Ridker PM, Bhatt DL, Pradhan AD, et al. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. 2023;401(10384):1293–1301. doi:10.1016/S0140-6736(23)00215-5
15. Bay B, Tanner R, Gao M, et al. Residual cholesterol and inflammatory risk in statin-treated patients undergoing percutaneous coronary intervention. Eur Heart J. 2025:ehaf196. doi:10.1093/eurheartj/ehaf196.
16. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
17. Tardif JC, Kouz S, Waters DD, et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
18. Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020;383(19):1838–1847. doi:10.1056/NEJMoa2021372
19. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction. J Am Coll Cardiol. 2018;72(18):2231–2264. doi:10.1016/j.jacc.2018.08.1038
20. Hicks KA, Mahaffey KW, Mehran R, et al. Standardized Data Collection for Cardiovascular Trials Initiative (SCTI). 2017 Cardiovascular and Stroke Endpoint Definitions for Clinical Trials. J Am Coll Cardiol. 2018;71(9):1021–1034. doi:10.1016/j.jacc.2017.12.048
21. Reynolds HR, Maehara A, Kwong RY, et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women. Circulation. 2021;143(7):624–640. doi:10.1161/CIRCULATIONAHA.120.052008
22. Fluder-Wlodarczyk J, Milewski M, Roleder-Dylewska M, et al. Underlying Causes of Myocardial Infarction with Nonobstructive Coronary Arteries: optical Coherence Tomography and Cardiac Magnetic Resonance Imaging Pilot Study. J Clin Med. 2022;11(24):7495. doi:10.3390/jcm11247495
23. Carrero JJ, Andersson Franko M, Obergfell A, et al. hsCRP Level and the Risk of Death or Recurrent Cardiovascular Events in Patients With Myocardial Infarction: a Healthcare-Based Study. J Am Heart Assoc. 2019;8(11):e012638. doi:10.1161/JAHA.119.012638
24. Sabatine MS, Giugliano RP, Keech AC, et al. Fourier Steering Committee and Investigators. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664
25. Ridker PM, Lei L, Louie MJ, et al. Inflammation and Cholesterol as Predictors of Cardiovascular Events Among 13 970 Contemporary High-Risk Patients With Statin Intolerance. Circulation. 2024;149(1):28–35. doi:10.1161/CIRCULATIONAHA.123.066213
26. Kalkman DN, Aquino M, Claessen BE, et al. Residual inflammatory risk and the impact on clinical outcomes in patients after percutaneous coronary interventions. Eur Heart J. 2018;39(46):4101–4108. doi:10.1093/eurheartj/ehy633
27. Ahn JH, Tantry US, Kang MG, et al. Residual Inflammatory Risk and its Association With Events in East Asian Patients After Coronary Intervention. JACC Asia. 2022;2(3):323–337. doi:10.1016/j.jacasi.2021.11.014
28. Toso A, Leoncini M, Maioli M, et al. Biomarkers of residual risk and all-cause mortality after acute coronary syndrome. Am J Prev Cardiol. 2025;21:100934. doi:10.1016/j.ajpc.2025.100934
29. Iwata H, Miyauchi K, Naito R, et al. Significance of Persistent Inflammation in Patients With Chronic Coronary Syndrome: insights From the REAL-CAD Study. JACC Adv. 2024;3(7):100996. doi:10.1016/j.jacadv.2024.100996
30. Matter MA, Paneni F, Libby P, et al. Inflammation in acute myocardial infarction: the good, the bad and the ugly. Eur Heart J. 2024;45(2):89–103. doi:10.1093/eurheartj/ehad486
31. Taqueti VR, Ridker PM. Lipid-Lowering and Anti-Inflammatory Benefits of Statin Therapy: more Than Meets the Plaque. Circ Cardiovasc Imaging. 2017;10(7):e006676. doi:10.1161/CIRCIMAGING.117.006676
32. Deftereos SG, Beerkens FJ, Shah B, et al. Colchicine in Cardiovascular Disease: in-Depth Review. Circulation. 2022;145(1):61–78. doi:10.1161/CIRCULATIONAHA.121.056171
33. Nelson K, Fuster V, Ridker PM. Low-Dose Colchicine for Secondary Prevention of Coronary Artery Disease: JACC Review Topic of the Week. J Am Coll Cardiol. 2023;82(7):648–660. doi:10.1016/j.jacc.2023.05.055
34. Aimo A, Pascual Figal DA, Bayes-Genis A, et al. Effect of low-dose colchicine in acute and chronic coronary syndromes: a systematic review and meta-analysis. Eur J Clin Invest. 2021;51(4):e13464. doi:10.1111/eci.13464
35. Burger PM, Dorresteijn JAN, Fiolet ATL, et al. Individual lifetime benefit from low-dose colchicine in patients with chronic coronary artery disease. Eur J Prev Cardiol. 2023;30(18):1950–1962. doi:10.1093/eurjpc/zwad221
36. Jolly SS, d’Entremont MA, Lee SF, et al. Colchicine in Acute Myocardial Infarction. N Engl J Med. 2025;392(7):633–642. doi:10.1056/NEJMoa2405922
37. Ridker PM, Rane M. Interleukin-6 Signaling and Anti-Interleukin-6 Therapeutics in Cardiovascular Disease. Circ Res. 2021;128(11):1728–1746. doi:10.1161/CIRCRESAHA.121.319077
38. Ridker PM. From CANTOS to CIRT to COLCOT to Clinic: will All Atherosclerosis Patients Soon Be Treated With Combination Lipid-Lowering and Inflammation-Inhibiting Agents? Circulation. 2020;141(10):787–789. doi:10.1161/CIRCULATIONAHA.119.045256
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.