Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Shortened questionnaires to assess anxiety and depression during in-hospital rehabilitation: clinical validation and cutoff scores
Authors Bertolotti G ![]() , Moroni L, Burro R
, Moroni L, Burro R ![]() , Spanevello A, Pedretti RFE, Giorgetti G
, Spanevello A, Pedretti RFE, Giorgetti G
Received 2 May 2016
Accepted for publication 17 June 2016
Published 12 October 2016 Volume 2016:12 Pages 2627—2633
DOI https://doi.org/10.2147/NDT.S111797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Giorgio Bertolotti,1 Loretta Moroni,1 Roberto Burro,2 Antonio Spanevello,3 Roberto FE Pedretti,4 Giandomenico Giorgetti5
1Psychology Unit, Salvatore Maugeri Foundation, IRCCS, Scientific Institute, Tradate, 2Department of Human Sciences – University of Verona, Verona, 3Department of Cardiology, 4Division of Pulmonary Disease, 5Department of Neuromotor Rehabilitation, Salvatore Maugeri Foundation, IRCCS, Scientific Institute of Tradate, Italy
Background: A postacute phase needs reliable routine screening instruments in order to identify the patients to be referred for a clinical interview with a psychologist. The aim of this study was to estimate the clinical cutoff scores of the anxiety and depression questionnaires and their clinical validity using a gold standard.
Methods: The study involved 177 patients with pulmonary, cardiac, or neurological disease undergoing in-hospital rehabilitation. Receiver operating characteristic curves were used to determine the best concordance between questionnaire’s scores and the gold standards.
Results: There was a significant difference (P<0.001) between clinically anxious and depressed patients and nonclinical subjects. The receiver operating characteristic curve for anxiety indicated that the best area under the curve for State Anxiety Inventory is obtained with a cutoff point of 21 for males and 25 for females; for depression scores, the highest area under the curve for Depression Questionnaire-Reduced Form is obtained with a cutoff point of six for males and eight for females.
Conclusion: Using appropriate cutoff values, the State Anxiety Inventory and Depression Questionnaire-Reduced Form allow psychologists to optimize early clinical intervention strategies selecting patients with significant needs.
Keywords: anxiety, depression, questionnaire, sensitivity and specificity, rehabilitation
Introduction
Many studies have established the presence of a high rate of psychological complaints among nonpsychiatric hospital patients.1 Symptoms of anxiety and depression may confuse a patient’s clinical image, reduce compliance with therapeutic programs and affect the medium- or long-term outcomes pursued during the course of hospitalization,2–4 predict health-related quality of life,5 and predict the influence of symptoms of anxiety and depression on medication noncompliance.6,7
The American Heart Association recently published a Science Advisory with the recommendation that patients with coronary heart disease (CHD) should be screened for depressive symptoms.8–10 Ziegelstein et al11 maintain that for routine screening of CHD patients for depression to be recommended, screening tests must be sufficiently sensitive, specific, and validated, because cutoff scores used in primary care may not work equivalently in patients with CHD.12 In a very recent review,13 it is noted that there are few examples of screening tools with high sensitivity and specificity using an a priori defined cutoff score in >1 CHD sample.
Mild-to-moderate symptoms of anxiety and/or depression have also been observed in patients with chronic obstructive pulmonary disease (COPD) and current recommendations indicate that they should not be ignored. Appropriate outcome measures for mental health are needed for this patient population.14 Similarly, depression and anxiety were significant for the outcomes regarding readmissions to hospital or death 6 months after a stroke. These are the reasons why clinicians need to identify specific patients with stroke with preexisting mental health conditions for which additional psychotherapy treatment may result in improved stroke outcomes.15
A Cochrane review16 indicated that psychological intervention in CHD patients did produce small to moderate improvements in depression and anxiety but there was no consistent evidence of a positive effect on health-related quality-of-life (HRQOL) or other psychological outcomes, including perceived stress, Type-A behavior, anger, and perceived exhaustion or Vital Exhaustion. All the aforementioned reasons and results support our search for clinical level of anxiety or depression in a rehabilitation setting and that both will be specific to the medical conditions of the patients concerned.
The aim of this study was to use receiver operating characteristic (ROC) curves to determine the best concordance between STAI-X3 and Depression Questionnaire-Reduced Form (acronym AD-R) scores using the opinion of a psychologist after a semi-structured clinical interview as gold standard.
Materials and methods
Patient population and data collection
The present observational study involved consecutively enrolled patients with pulmonary, cardiac, or neurological and neuromuscular disease undergoing in-hospital rehabilitation at the Salvatore Maugeri Foundation, IRCCS, Scientific Institute Division of Respiratory, Cardiac, and Neuromotor Rehabilitation during a period of 6 months in 2010. As a rule, the subjects completed the AD-R within the second to third day from the hospital admission. On the same day, a psychologist independently assessed their anxiety and depression status using a semistructured interview17,18 and decided the appropriate psychological support needed. The psychologist was blinded to the AD-R scores. Exclusion criteria were as follows: the inability to complete questionnaires and a history of a severe psychiatric disease. The protocol was reviewed and approved by an internal review board for ethical protection of subjects (Comitato Tecnico Scientifico), and written informed consent of all the participants was obtained.
Measures
With the aim of making the screening process more rapid and accurate, we developed the ten-item version of the State Anxiety Inventory (STAI-X3)19–21 and the 15-item QD-R both with validated and reliable criteria (concurrent and predictive content).22,23 The reduced form of STAI-X3, consists of 10 items asking the subjects how they feel “right now” that are scored using a 4-point Likert scale (total score 10–40). The QD-R measures depressive symptoms and was originally constructed with reference to Diagnostic and Statistical Manual of Mental Disorders (DSM)-III and meets all of the DSM-IV Revised24 criteria for major depressive disorder (depressed mood; loss of interest or pleasure; variations in appetite and weight; insomnia/hypersomnia; psychomotor agitation/slowing; fatigability; self-depreciation; poor concentration; recurrent thoughts of death). For more details on the reduction methods, see Vidotto et al.22 The two questionnaires in the reduced form take ~5 minutes to complete.
It simplifies screening of patients in hospital settings as it is suitable for subjects with mild/moderate or subclinical depression.22,23 The QD-R has 15 items, each consisting of a statement (eg, “The future looks very bleak”) to be answered “yes” or “no” (total score 0–15) and excludes somatic symptoms, thereby avoiding potential confounding by the somatic symptoms in hospitalized patients. The instructions ask that the questions should be answered “thinking about how you feel at this moment”, with the subject being asked to ponder the time span corresponding to that required to complete the survey.
Using Cronbach’s alpha score, the internal consistency of the QD-R is 0.77; any value between 0.7 and 0.8 is considered satisfactory for comparing groups.25 STAI-X3 showed an internal consistency assessed with Cronbach’s alpha of 0.90 in healthy subjects.20
Semistructured clinical interview: gold standard
In order to structure and maintain a single criterion for defining the gold standard, we used a “semistructured clinical interview” form based on and in respect of the DSM-IV anxiety and depression (DSM code 300.4) criteria. Inter-rater agreement with the psychological judgment for anxiety state (Cohen’s K =3.60; concordance 76%) and for depressive reaction (Cohen’s K =2.39; concordance =86%) has been found in a previously published study.17 The “semistructured clinical interview” form is divided into three sections: anxiety, depression, and an area in which the diagnostic criteria for such disturbances overlap.
The interview began with a series of unstructured questions with the aim of establishing a cooperative relationship between the patient and the psychologist, and acquiring diagnostically useful information. At the end of the interview, the clinical psychologist had to judge whether the subject showed no anxiety/depression or one or both of these characteristics. If this was the case, the subject was invited to attend further sessions for clinical psychological support.
Statistical analysis
R software 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria. URL https://www.R-project.org/.; language and environment for statistical computing and graphics)26 was used to analyze the data sample and analysis of variance to verify the significance of the differences in mean QD-R and STAI-X3 scores between males and females and between the disease groups. The construct validity of the AD-R schedule as a measure of depression and anxiety was assessed by examining the differences in mean value between the clinical groups as classified by the psychologist. Bonferroni’s correction was applied for the type I error inflation due to multiple comparisons.
ROC curves were used to identify the AD-R cutoff points. ROC analysis quantifies the accuracy of diagnostic tests (or further appraisal types) used to discriminate between two states or conditions. The discriminatory accuracy of a diagnostic test is quantified by its ability to suitably classify between subjects with and without disease.27 A ROC plot displays the performance of a dichotomous classification procedure with continuous or discrete ordinal outcome. In the ROC space, the area under the curve (AUC) measures the performance of a classifying variable and is frequently applied for method comparison. A higher AUC means a better classification.28 AUCs are computed with trapezoids.29 In our case, ROC curves were used to identify the AD-R cutoff points. This technique is commonly used in medical decision-making research in order to determine how well a potential classifier discriminates two classes.27–32 In the context of this study, the potential classifying variables were the total AD-R scores, and the two classes were the binary classification of the presence/absence of the clinically relevant psychological variables (anxiety and depression).
The confidence intervals (CIs) were computed with bootstrap for AUCs.33 The 95% CIs of the AD-R cutoff points and the sensitivity and specificity values were computed with bootstrap resampling (stratified manner), and the averaging methods described by Fawcett.32 In all bootstrap CIs, the subjects were resampled and the modified curve was built before the statistics of interest were computed.
Results
One hundred and seventy-seven subjects (101 males and 76 females) completed the AD-R schedule and the interview with the psychologist at the beginning of their in-hospital rehabilitation period. Tables 1 and 2 show their characteristics. The main pulmonary diseases were asthma, COPD, and respiratory failure; the main cardiac diseases were coronary artery disease (myocardial infarction, angina pectoris), congestive heart failure, and valvular heart disease; and the main neurological or neuromuscular diseases were stroke and myopathy.
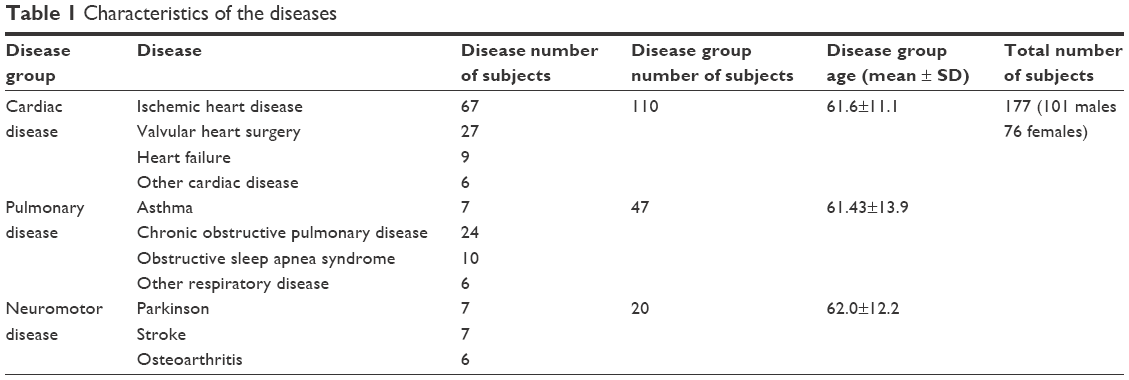 | Table 1 Characteristics of the diseases |
 | Table 2 Characteristics of the sample |
Comparing the three disease groups, no significant differences were found either for STAI-X3 scores (F(2,174)=0.252, P=0.778) or for QD-R scores (F(2,174))=0.186, P=0.830).
Table 3 shows the distribution of the AD-R scores on the basis of the psychologist’s diagnosis of depression and anxiety. Based on the psychologist’s judgment, 53 subjects were “possible case for anxiety” (prevalence =29.9%) and 42 were “possible case for depression” (prevalence =23.7%). There was a significant difference in mean STAI-X3 scores between the subjects with and without clinically relevant anxiety (t(175)=14.813, P<0.001), and in mean QD-R scores between the subjects with and without clinically relevant depression (t(175)=12.864, P<0.001).
 | Table 3 Construct validity of the AD-R schedule |
Cutoff scores
The best AUC for STAI-X3 was obtained with a cutoff point of 21.0 for males and 25.0 for females (Figure 1). CI of AUC for STAI-X3 sample of males (equal to 95.5%) was 92.0%–99.0%, whereas CI of AUC for STAI-X3 sample of females (equal to 92.9%) was 86.5%–99.4%.
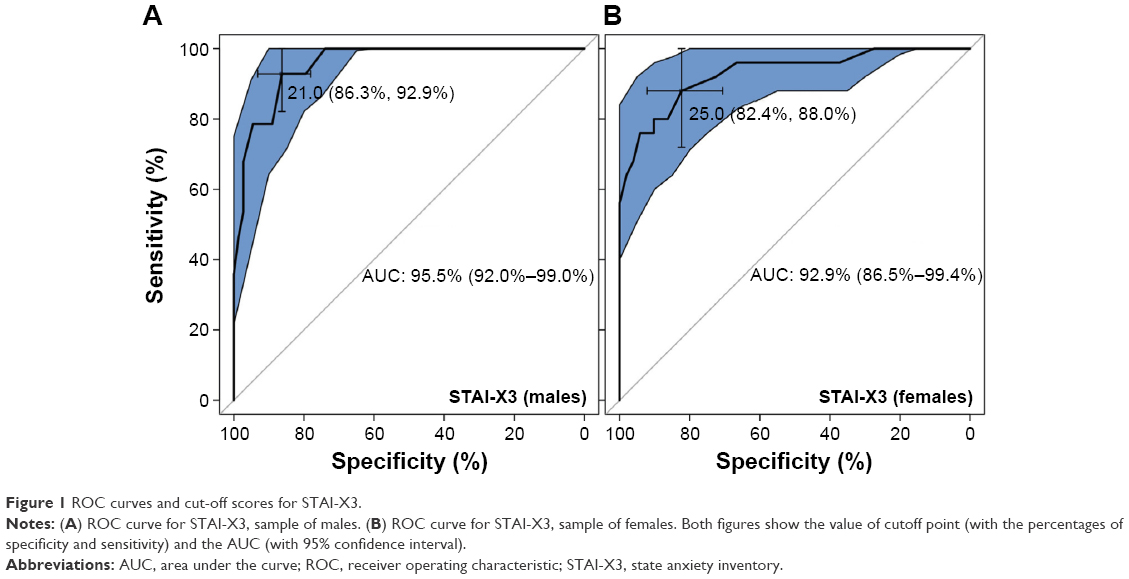 | Figure 1 ROC curves and cut-off scores for STAI-X3. |
The best AUC for QD-R was obtained with a cutoff point of 6.0 for males and 8.0 for females (Figure 2). CI of AUC for QD-R sample of males (equal to 94.9%) was 90.4%–99.4%, whereas CI of AUC for QD-R sample of females (equal to 96.7%) was 92.8%–100.0%.
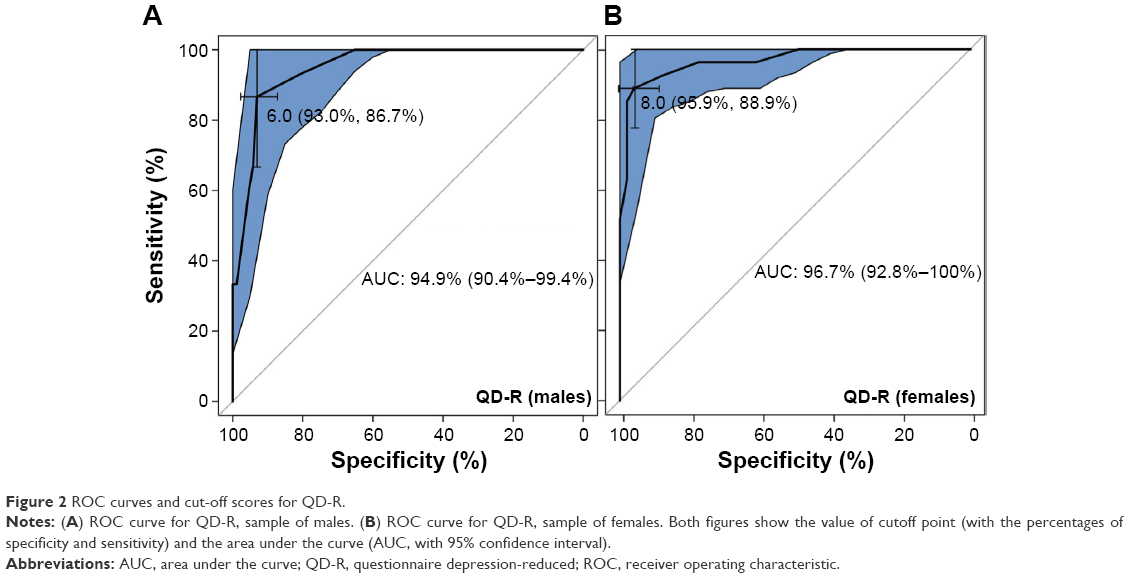 | Figure 2 ROC curves and cut-off scores for QD-R. |
Table 4 shows the CIs of cutoff points of STAI-X3 and QD-R in male and female samples. The table also shows the sensitivity, specificity, positive predictive value (what is the probability that the disease is present when the test is positive) and negative predictive value (what is the probability that the disease is not present when the test is negative), positive likelihood ratio (what is the ratio between the probability of a positive test result given the presence of the disease and the probability of a positive test result given the absence of the disease) and negative likelihood ratio (what is the ratio between the probability of a negative test result given the presence of the disease and the probability of a negative test result given the absence of the disease); 95% CIs for each index are also reported.
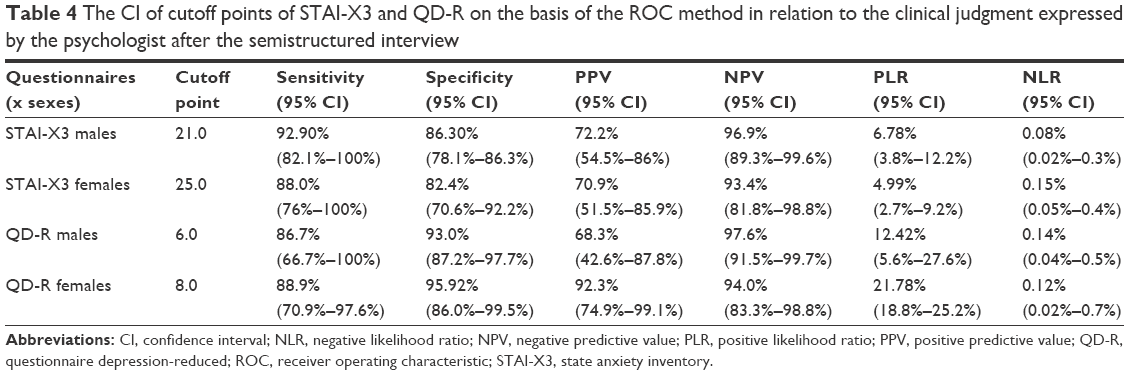 | Table 4 The CI of cutoff points of STAI-X3 and QD-R on the basis of the ROC method in relation to the clinical judgment expressed by the psychologist after the semistructured interview |
The difference between sexes in STAI-X3 scores was not significant (t(175)=−0.952, P=0.342), whereas female showed higher (t(175)=−2.415, P=0.017) QD-R scores (5.51±3.4) than male (4.37±3.2). The bootstrap test for ROCs (2,000 resampling) indicates that the differences between curves for males and females were not significant both for STAI X-3 (D =0.679, P-value =0.497), and QD-R (D =0.356, P-value =0.721).
Discussion
Granted that assessing depression and anxiety in patients undergoing rehabilitation in a hospital is of major importance, it is necessary to devise an efficient way of completing such assessments.34–38 In this study, we searched the cutoff score of the STAI-X3 and QD-R not referring particularly to the specific disease (ie, CHD, COPD), but to the hospitalized condition in general, considering that DSM criteria suggest to pay attention to symptoms that are clearly due to a general medical condition, not to a specific medical condition.24 When identifying a cutoff score for a routine screening, we also found that the QD-R was sensible and specific for a clinically relevant state of depression worthy of a deeper psychological examination, not to identify a major depressive disorder to be treated with antidepressants. This avoids the risk suggested by some authors11 that antidepressant medications may be initiated merely based on a positive depression screen.
From a clinical perspective, our findings support the use of AD-R cutoff scores as a means of screening psychological status in rehabilitation and hospital settings. Additionally, there were no differences between the disease groups. This would allow the multidisciplinary team to devise therapeutic interventions designed to improve both physical and psychological symptoms across disease conditions, which may be the best method to optimize functioning.39–44
The AD-R schedule is clearly subdivided in a solid measure of anxiety and another of depression, with different scores and cutoff points. Some questionnaires measuring depression focus narrowly on anhedonia, defined as a reduced ability to experience pleasure; it is too much to expect that ill patients will discriminate the intended meaning from their experience of not wanting to engage in previously pleasurable activities because of pain, fatigue, and other physical impairment.45
The use of ROC curves provide information concerning AD-R cutoff values, which allow psychologists to optimize early clinical interventions during rehabilitation or in the provision of secondary prevention by identifying a clinically relevant state of depression and/or anxiety worthy of a deeper examination. In our sample, we found a STAI-X3 cutoff point of 21 for males and 25 for females. This means that a score ≥21 for males and ≥25 for females is indicative of a clinical level of anxiety that needs to be evaluated further by a psychologist. For QD-R, we found a cutoff point of 6 for males and 8 for females. This means that a score ≥6 for males and ≥8 for females is indicative of a critical mood level suggestive of a level of depression that requires a more complete evaluation by a psychologist.
Regarding construct validity, we found higher cutoff scores in females compared to males, as has been reported.23 These results may be due to sex differences in illness perception: females, compared to males, are more likely to attribute cardiovascular disease (CVD) to causes beyond their control and perceive CVD as a chronic, untreatable condition.46 Screening, especially for depression, is strongly recommended even in primary care.47 Furthermore, in our previous paper, QD-R scores significantly correlated with meters walked in the 6-m walking test by 252 patients during cardiovascular rehabilitation, and patients with QD-R scores ranging from 0 to 5 showed a progressive reduction in the total distance walked during the test. In that study, a fall in walking distance corresponded to a value of 6 in the depression score as measured by QD-R.14 Further research could be performed to observe the trend of functional performance along clinical cutoff points and to evaluate the effectiveness of integrated and multidisciplinary stepped care,48,49 and studies with hospitalized subjects.50–53
Limitations
We collected a sample from a single hospital; our results essentially describe what was found in the sample, but the extent to which those results might generalize beyond the center where the study was conducted is unknown. We also studied patients with pulmonary, cardiac, or neurological and neuromuscular diseases with very heterogeneous characteristics. However, this situation reproduces the proportion of patients usually followed by a psychologist during the rehabilitation phase in our institute. Further study with a larger sample and with different diseases would be required to test the validity of the AD-R cutoff scores for the screening of hospitalized patients that need a specific psychological support.
Conclusion
Using these cutoff values, the STAI-X3 and QD-R allow psychologists to optimize early clinical intervention strategies.
Acknowledgments
The authors wish to thank and acknowledge Alessandra Ianni for her help in collecting and organizing the data set. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
Gilbody SM, House AO, Sheldon TA. Routinely administered questionnaires for depression and anxiety: systematic review. BMJ. 2001;322(7283):406–409. | ||
Balady GJ, Ades PA, Comoss P, et al. Core components of cardiac rehabilitation/secondary prevention programs: a statement for healthcare professionals from the American Heart Association and the American Association of Cardiovascular and Pulmonary Rehabilitation Writing Group. Circulation. 2000;102(9):1069–1073. | ||
British Thoracic Society Standards of Care Subcommittee on Pulmonary Rehabilitation. Pulmonary rehabilitation. Thorax. 2001;56(11):827–834. | ||
Pooler A, Beech R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: a systematic review. Int J Chron Obstruct Pulmon Dis. 2014;9:315–330. | ||
Blakemore A, Dickens C, Guthrie E, et al. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2014;9:501–512. | ||
Sundbom LT, Bingefors K. The influence of symptoms of anxiety and depression on medication nonadherence and its causes: a population based survey of prescription drug users in Sweden. Patient Prefer Adherence. 2013;7:805–811. | ||
DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for non-compliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–2107. | ||
Lichtman JH, Bigger JT Jr, Blumenthal JA, et al. AHA science advisory. Depression and coronary heart disease. Recommendations for screening, referral, and treatment. A science advisory from the American Heart Association Prevention Committee to the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiology and Prevention, and Interdisciplinary Council on Quality of Care Outcomes Research. Endorsed by the American Psychiatric Association. Prog Cardiovasc Nurs. 2009;24(1):19–26. | ||
Gallagher R, Trotter R, Donoghue J. Preprocedural concerns and anxiety assessment in patients undergoing coronary angiography and percutaneous coronary interventions. Eur J Cardiovasc Nurs. 2010;9(1):38–44. | ||
Iguchi A, Senjyu H, Hayashi Y, et al. Relationship between depression in patients with chronic obstructive pulmonary disease and the percent predicted FEV1, BODE index, and health-related QOL. Respir Care. 2013;58(2):334–339. | ||
Ziegelstein RC, Thombs BD, Coyne JC, de JongeP. Routine screening for depression in patients with coronary heart disease never mind. J Am Coll Cardiol. 2009;54(10):886–890. | ||
Williams JW Jr, Pignone M, Ramirez G, Perez Stellato C. Identifying depression in primary care: a literature synthesis of case-finding instruments. Gen Hosp Psychiatry. 2002;24(4):225–237. | ||
Thombs BD, Roseman M, Coyne JC, et al. Does Evidence Support the American Heart Association’s recommendation to screen patients for depression in cardiovascular care? An updated systematic review. PLoS One. 2013;8(1):e52654. | ||
Cafarella PA, Effing TW, Usmani ZA, Frith PA. Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: a literature review. Respirology. 2012;17(4):627–638. | ||
Dossa A, Glickman ME, Berlowitz D. Association between mental health conditions and rehospitalization, mortality, and functional outcomes in patients with stroke following inpatient rehabilitation. BMC Health Serv Res. 2011;11:311. | ||
Whalley B, Rees K, Davies P, et al. Psychological interventions for coronary heart disease. Cochrane Database Syst Rev. 2011;(8):CD002902. | ||
Zotti AM, Bertolotti G, Michielin P, Sanavio E, Vidotto G. – CBA-H. Cognitive Behavioural Assessment forma Hospital. Manuale. Firenze:Giunti OS; 2010. | ||
Vedana L, Baiardi P, Sommaruga M, et al. Clinical validation of an anxiety and depression screening test for intensive in-hospital rehabilitation. Monaldi Arch Chest Dis. 2002;58(2):101–106. | ||
Spielberger CD, Gorsuch RL, Lushene R, et al. Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press, 1983. | ||
Bertolotti G, Michielin P, Sanavio E, Vidotto G, Zotti AM. A computerized approach to cognitive behavioral assessment: an introduction to CBA-2.0 primary scales. J Behav Ther Exp Psychiatry. 1990;21(1):21–27. | ||
Vidotto G, Bertolotti G. Una valutazione base dell’ansia di stato. La versione ridotta dello STAI X-1. [A basic assessment of state anxiety. The STAI X – 1 reduced version]. Bollettino Psicologia Applicata. 1991;198:33–40. | ||
Vidotto G, Moroni L, Burro R, et al. A revised short version of the depression questionnaire. Eur J Cardiovasc Prev Rehabil. 2010;17(2):187–197. | ||
Moroni L, Bettinardi O, Vidotto G, et al. [Anxiety and Depression Short Scale: norms for its use in rehabilitation]. Monaldi Arch Chest Dis. 2006;66(4):255–263. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th-ed. Washington, D.C: American Psychiatric Press, 2000. | ||
Bland JM, Altman DG. Statistics notes. Cronbach’s alpha. BMJ. 1997;314(7080):572. | ||
R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing, 2016. Available from: http://www.R-project.org/. Accessed April 5, 2016. | ||
Pepe MS. The Statistical Evaluation of Medical Tests for Classification and Prediction. New York: Oxford University Press, 2003. | ||
Hanczar B, Hua J, Sima C, Weinstein J, Bittner M, Dougherty ER. Small-sample precision of ROC-related estimates. Bioinformatics. 2010;26(6):822–830. | ||
Zweig MH, Campbell G. Receiver-operating characteristic (ROC) plots: a fundamental evaluation tool in clinical medicine. Clin Chem. 1993;39(4):561–577. | ||
Bartfay E, Bartfay WJ. Accuracy assessment of prediction in patient outcomes. J Eval Clin Pract. 2008;14(1):1–10. | ||
Linden A. Measuring diagnostic and predictive accuracy in disease management: an introduction to receiver operating characteristic (ROC) analysis. J Eval Clin Pract. 2006;12(2):132–139. | ||
Fawcett T. An introduction to ROC analysis. Pattern Recogn Lett. 2006;27:861–874. | ||
Carpenter J, Bithell J. Bootstrap confidence intervals: when, which, what? A practical guide for medical statisticians. Stat Med. 2000;19(9):1141–1164. | ||
Lou P, Zhu Y, Chen P, et al. Prevalence and correlations with depression, anxiety, and other features in outpatients with chronic obstructive pulmonary disease in China: a cross-sectional case control study. BMC Pulm Med. 2012;12:53. | ||
Kamphuis MH, Kalmijn S, Tijhuis MA, et al. Depressive symptoms as risk factor of cardiovascular mortality in older European men: the Finland, Italy and Netherlands Elderly (FINE) study. Eur J Cardiovasc Prev Rehabil. 2006;13(2):199–206. | ||
Schroeder V, Borner U, Gutknecht S, Schmid JP, Saner H, Kohler HP. Relation of depression to various markers of coagulation and fibrinolysis in patients with and without coronary artery disease. Eur J Cardiovasc Prev Rehabil. 2007;14(6):782–787. | ||
Putman-Casdorph H, McCrone S. Chronic obstructive pulmonary disease, anxiety, and depression: state of the science. Heart Lung. 2009;38(1):34–47. | ||
Coventry PA, Gemmell I, Todd CJ. Psychosocial risk factors for hospital readmission in COPD patients on early discharge services: a cohort study. BMC Pulm Med. 2011;11:49. | ||
Murphy BM, Elliott PC, Higgins RO, et al. Anxiety and depression after coronary artery bypass graft surgery: most get better, some get worse. Eur J Cardiovasc Prev Rehabil. 2008;15(4):434–440. | ||
Gary RA, Dunbar SB, Higgins MK, Musselman DL, Smith AL. Combined exercise and cognitive behavioral therapy improves outcomes in patients with heart failure. J Psychosom Res. 2010;69(2):119–131. | ||
Freedland KE, Skala JA, Carney RM, et al. Treatment of depression after coronary artery bypass surgery: a randomized controlled trial. Arch Gen Psychiatry. 2009;66(4):387–396. | ||
Tselebis A, Pachi A, Ilias I, Kosmas E, Bratis D, Moussas G, Tzanakis N. Strategies to improve anxiety and depression in patients with COPD: a mental health perspective. Neuropsychiatr Dis Treat. 2016;12:297–328. doi:10.2147/NDT.S79354. | ||
Hynninen MJ, Bjerke N, Pallesen S, Bakke PS, Nordhus IH. A randomized controlled trial of cognitive behavioral therapy for anxiety and depression in COPD. Respir Med. 2010;104(7):986–994. | ||
Braverman DL. Cardiac rehabilitation: a contemporary review. Am J Phys Med Rehabil. 2011;90(7):599–611. | ||
Coyne JC, van Sonderen E. No further research needed: abandoning the Hospital and Anxiety Depression Scale (HADS). J Psychosom Res. 2012;72(3):173–174. | ||
Grace SL, Krepostman S, Brooks D, et al. Illness perceptions among cardiac patients: relation to depressive symptomatology and sex. J Psychosom Res. 2005;59(3):153–160. | ||
Reynolds CF 3rd, Frank E. US Preventive Services Task Force Recommendation statement on screening for depression in adults: Not good enough. JAMA Psychiatry. 2016;73(3):189–190. | ||
Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2014;9:1289–1306. | ||
Tselebis A, Pachi A, Ilias I, et al. Strategies to improve anxiety and depression in patients with COPD: a mental health perspective. Neuropsychiatr Dis Treat. 2016;12:297–328. | ||
Wu YS, Lin PY, Chien CY, et al. Anxiety and depression in patients with head and neck cancer: 6-month follow-up study. Neuropsychiatr Dis Treat. 2016;12:1029–1036. | ||
Novick D, Montgomery W, Aguado J, Peng X, Haro JM. Impact of anxiety symptoms on outcomes of depression: an observational study in Asian patients. Neuropsychiatr Dis Treat. 2016;12:795–800. | ||
Yanartas O, Kani HT, Bicakci E, et al. The effects of psychiatric treatment on depression, anxiety, quality of life, and sexual dysfunction in patients with inflammatory bowel disease. Neuropsychiatr Dis Treat. 2016;12:673–683. | ||
Gerez M, Suárez E, Serrano C, Castanedo L, Tello A. The crossroads of anxiety: distinct neurophysiological maps for different symptomatic groups. Neuropsychiatr Dis Treat. 2016;12:159–175. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.