")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Short-Term and Long-Term Impact of COVID-19 on Quality of Life and Psychological Outcomes in Saudi Arabia: A Comparative Cross-Sectional Study
Authors Althomali OW, Amin J , Shaik DH, Alghamdi W, Ibrahim AA , Hussein HM, Kanwal R
Received 13 November 2023
Accepted for publication 8 January 2024
Published 1 February 2024 Volume 2024:17 Pages 505—515
DOI https://doi.org/10.2147/JMDH.S449152
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Omar W Althomali,1,* Junaid Amin,1,* Daria Hussain Shaik,1 Wael Alghamdi,2 Ahmed Abdelmoniem Ibrahim,1,3 Hisham M Hussein,1,4 Raheela Kanwal1
1Department of Physical Therapy, College of Applied Medical Sciences, University of Ha’il, Ha’il, 2440, Saudi Arabia; 2Department of Nursing, College of Applied Medical Sciences, AlBaha University, AlBaha, 1988, Saudi Arabia; 3Department of Physical Therapy, Cairo University Hospitals, Giza, Egypt; 4Department of Basic Sciences for Physical Therapy, Faculty of Physical Therapy, Cairo University, Giza, Egypt
*These authors contributed equally to this work
Correspondence: Junaid Amin, Department of Physical Therapy, College of Applied Medical Sciences, University of Ha’il, Ha’il, 2440, Saudi Arabia, Tel +966-580931017, Email [email protected]
Background: Prior research has revealed notable declines in health-related quality of life (HRQoL) and substantial psychological impacts among individuals infected with COVID-19. However, there is a noticeable gap in studies addressing the enduring long-term effects of COVID-19 on HRQoL and psychological well-being.
Objective: The current study investigated and compared short and long-term effects of COVID-19 on HRQoL and psychological outcomes among the Saudi population.
Methods: The Arabic version of the SF-36 questionnaire was used to assess HRQoL while Anxiety and depression were evaluated by the Hamilton Anxiety (HAM-A) and Depression Scales (HDRS). Participants (n=292) were categorized into three groups: the “never-been-infected” group (n=134), the “one-year infected group” (n=43), and the “more than one year infected” group (n=115). Descriptive statistics were presented using numerical values and frequencies. To compare the groups, a one-way analysis of variance (ANOVA) test was used.
Results: Most SF-36 domains exhibited lower values while HAM-A and HDRS values were higher in individuals infected during last year compared to those who never infected. Social functioning subscale of the SF-36 showed a significant difference between the groups (F (2.289) = 6.094, p = 0.01) and the effect size was d = 0.95. Pairwise comparison showed a significant reduction in the social functioning component of SF-36 in “one-year group” compared to both groups “never-been-infected” group (mean difference − 13.58 (4.40– 22.76) p < 0.01) and “more than one year infected” group (mean difference − 10.80 (1.44– 20.16) p = 0.02). HAM-A and HDRS scores showed mild levels of anxiety (< 17 score) and depression (8 to 16 score) in all groups.
Conclusion: The influence of COVID-19 on psychological well-being and HRQoL is significant regardless of whether individuals infected with the virus. Overall, the consistent presence of mild anxiety and depression across all groups highlights the need for a holistic approach to mental health.
Plain Language Summary: In this study, we looked at how COVID-19 infection affected the quality of life and mental well-being of people in Saudi Arabia in both the short and long term. We used surveys to measure quality of life, anxiety, and depression among 292 participants, categorizing them based on whether they had never been infected, were infected within the last year, or were infected more than one year ago. The results showed that individuals who were infected in the last year had lower scores in various aspects of quality of life and higher levels of anxiety and depression compared to those who had never been infected.
Although mild levels of anxiety and depression were found in all groups. The study suggests that there is an impact on mental health in individuals even one year post-infection compared to never infected individuals. This highlights the importance of ongoing mental health support for individuals who have experienced the virus. Overall, the study emphasizes the need for a comprehensive approach to mental health care that considers both those who have been infected and those who have not.
Keywords: anxiety, COVID-19, depression, quality of life, SF-36
A Letter to the Editor has been published for this article.
Introduction
COVID-19 was originally discovered in December 2019, the disease quickly expanded over all of China, and by February 2020, COVID-19 had spread to a large number of different nations.1–3 In March 2020, the World Health Organization (WHO) declared COVID-19 to be a pandemic.4,5 The first case of COVID-19 in Saudi Arabia was reported in March 2020. At this time, there are 841,469 COVID-19 cases in the kingdom. COVID-19 cases have a wide range of documented symptoms including fever, cough, dyspnea, fatigue, muscle aches, headache, loss of taste or smell, sore throat, congestion or runny nose, nausea or vomiting, and diarrhea.6,7 According to COVID-19 longitudinal studies, prolonged bed rest may be the cause of several pathological changes, such as lung fibrosis, atelectasis, muscle weakening, and mental health problems. COVID-19 patients were under exposure to long-term corticosteroid therapy, which led to common problems like musculoskeletal pain, decreased range of motion, neuropathy, and myopathy, as well as pulmonary dysfunction, dyspnea, disorientation, and difficulty performing everyday tasks.8,9 Persistent symptoms and prolonged symptoms from COVID-19 not only affect those with chronic conditions or the elderly but also young and healthy individuals can be affected.10 Therefore, COVID-19 may lead to long- and short-term reductions in health-related quality of life (HRQoL).11
HRQoL is an individual’s perception of their overall well-being and incorporates a multi-dimensional concept including several domains such as mental, physical, emotional, and social functioning.11 To control the spread of the disease several countries used restrictive public health control which may have further impacted the HRQoL of the patients infected with COVID-19 and the healthy as well.12 For example, forcing infected people to stay at home alone can affect their mental health due to social isolation.13 Other restricted measures such as leisure, work, and travel may also impact such outcomes.12 In addition, social media may also raise fear, anxiety, and depression among the population14 which may impact their HRQoL. There are several tools to be used to measure HRQoL some of them are disease-specific and some are generic. Generic tools such as SF-36 (36-item Short-Form Health Survey) are widely used in research to evaluate multi-dimension measures in a different population.15
Previous research showed significant impairment in HRQoL among COVID-19 patients within the first months after the infection.16–19 Only a small number of studies have examined the long-term effect of COVID-19 on HRQoL within 12 months and beyond. Furthermore, mixed results were found where some studies found good functional and physical recovery,20,21 while others have reported impaired HRQoL.22–25 Interestingly, previous research highlighted that symptoms and characteristics of the disease may vary from nation to nation.26 Therefore, the current study compared the short- and long-term impact of COVID-19 on HRQoL and psychological outcomes among the Saudi population.
The findings of this study would provide valuable insights into the long-term effects of the pandemic that can be helpful to develop effective intervention strategies and healthcare policies in Saudi Arabia and other countries, to improve the mental health and quality of life of individuals affected by the pandemic. Furthermore, it can also help to explore access to mental care including telemedicine as a means of providing mental health support during and after the pandemic, especially for individuals who may face barriers to in-person care.
Materials and Methods
The findings were reported following the guidelines outlined by the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) recommendations.27
Study Design, Sampling, and Participants
This research represents an observational cross-sectional investigation carried out within the Hail, Saudi Arabian general population between May and July 2023. To participate in the study, individuals were required to meet certain criteria, including being 18 years or older, residing in Saudi Arabia, and expressing their willingness to take part. Notably, individuals with pre-existing psychiatric conditions predating the COVID-19 pandemic and those experiencing severe health problems were excluded from the study. A convenience sample of residents living in Hail, Saudi Arabia was assembled. The study’s anticipated sample size was calculated to be 280 using the Raosoft software (http://www.raosoft.com/samplesize.html), accessed on March 18, 2023, for estimation. Raosoft is a software platform that specializes in web-based data collection and analysis, offering a user-friendly interface for designing, administering, and analyzing surveys, enhancing its utility for researchers and professionals engaged in survey design and analysis. The participants were categorized into three distinct groups based on the various time intervals of COVID-19 infection: the “never-been-infected” group, the “one-year infected group”, (individuals infected within the last 12 months), and the ”more than one year infected” group (individuals infected more than 12 months ago) (Figure 1).
 |
Figure 1 Flow diagram of selection, data collection, and categorization of participants. |
Study Tools
A validated, self-administered questionnaire was used in this study. We employed a set of standardized assessment tools (SF-36 questionnaire, Hamilton Anxiety Rating Scale (HAM-A), and Hamilton depression rating scale (HDRS)) and collected the following: age, gender, smoking status, number of COVID-19 vaccination doses received, self-reported general health status and previous COVID-19 infection duration. SF-36 questionnaire and Hamilton Anxiety and Depression Scale which are reliable and valid outcome measures. We selected these questionnaires based on their ease of administration and alignment with our research goals and population characteristics. The SF-36 questionnaire, being the most popular and widely used tool for assessing health-related quality of life (HRQoL), was chosen for its relevance. Additionally, it has been extensively employed in evaluating the quality of life among individuals affected by COVID-19. Similarly, the Hamilton Anxiety and Depression Scales are among the foremost rating scales for assessing anxiety and depression, and they have been widely utilized to evaluate psychological outcomes in COVID-19 patients. To ensure consistency, electronic versions of the SF-36, HAM-A, and HDRS questionnaires were employed, and their validity and reliability were found to be comparable to the paper-based versions. SF-36 questionnaire and Hamilton Anxiety and Depression Scale have been validated in the Arabic language and adopted for use within the Saudi population.28–31
SF-36 Questionnaire
The quality of life was evaluated using the validated Arabic version for the Saudi population of the SF-36 questionnaire.32 The electronic administration of SF-36 demonstrated comparable performance to its paper-based version.33 This questionnaire is composed of 36 questions, categorized into eight distinct sections as follows; (1) physical functioning (10 questions), (2) role limitations due to physical health problems (4 questions), (3) role limitations due to personal or emotional problems (3 questions), (4) energy/fatigue (4 questions), (5) bodily pain (2 questions), (6) general health perceptions (5 questions), (7) social functioning (2 questions), and (8) emotional well-being (5 questions). A higher score on the SF-36 subscales, which range from 0 to 100, indicates greater health.34
Hamilton Anxiety Rating Scale (HAM-A)
Anxiety in study participants was assessed by the Hamilton Anxiety Scale.35,36 The level of anxiety was measured from the Hamilton Anxiety Rating Scale (HAM-A). The questionnaire is easy to use and contains 14 questions that measure both somatic anxiety (anxiety-related physical problems) and psychic anxiety (anxiety-related mental agitation and psychological issues). The score of each question ranged from 0 to 4 which provides a total with a maximum score of 56 and a minimum score of 0. A value <17 indicates mild severity, 18 to 24 is mild to moderate and from 25 to 30 indicates moderate to severe anxiety.37
Hamilton Depression Rating Scale (HDRS)
To measure the severity of depression the Hamilton depression rating scale (HDRS) was used. The questionnaire consists of 17 questions with a maximum score of 45 and a minimum score of 0. A score from 0 to 7 specifies no depression, 8 to 16 mild depression, 17 to 23 moderate depression, and above 24 severe depression.38
Data Collection
The data was collected using an online system using Google Forms. The electronic versions of SF-36, HAM-A, and HDRS questionnaires were used. Before the participants started filling out the questionnaires, an introductory part was prepared which contained the purpose of the study along with participant consent. After that, demographic data were collected as follows, age, gender, smoking, COVID-19 vaccination doses, and previous infection time with COVID-19. Participants were also asked to self-assess their general health, with responses categorized into excellent, very good, good, fair, and poor. Regarding the previous infection, multiple-choice questions were used. The questionnaire required 15 to 20 minutes to be collected. The survey link was shared with the Saudi population using social media platforms such as WhatsApp, Twitter, and Snapchat. Subsequent multiple reminders were sent to the potential participants to get a good response rate.
Ethical Considerations
Ethical approval was gained for the current study from the ethical committee of Hail University under the ethics number H-2021-236. Informed consent was obtained from every study participant before the commencement of data collection.
Statistical Analysis
After the responses were collected from the participants, the data were downloaded as an Excel sheet. The data was then coded and entered into the SPSS Version 28.0.1.1. Based on data availability, participants were divided into three groups (never been infected, infected in the last 12 months, infected more than 1 year ago). Descriptive statistics were communicated using numerical values and corresponding frequencies. To compare the groups, a one-way analysis of variance (ANOVA) test was used when the data met the assumption. If the data did not meet the assumption, the Kruskal–Wallis test was used. When the one-way ANOVA test was significant, a pairwise comparison was conducted using Tukey adjustment. To compare differences between the groups, which is considered as a nominal variable a chi-square test was used. The significant level was considered to be 0.05. Cohen’s d was calculated to estimate the effect size and interpreted as small = 0.2, medium = 0.5, and large = 0.8.
Results
Baseline Characteristics
In this study, we collected a total of 292 responses, which were subsequently categorized into three groups: the “never-been-infected” group (n = 134), the “one-year infected group” (n = 43), and the “more than one year infected” group (n = 115). The mean and standard deviation of the age for these groups was 34.7 (11.4) for the “never-been-infected” group, 33.4 (9.2) for the “one-year infected group”, and 33.8 (9.4) for those infected more than one year ago. Notably, a higher proportion of males was observed in both the never-infected group (62.7%) and the more than one-year-infected group (64.3%). One year Infected group demonstrated the highest percentage of non-smokers (86.0%). At least one dose of the COVID-19 vaccine was taken by each participant. Participants’ self-assessment of general health showed a prevalent perception of “excellent” and “very good”, with percentages ranging from 32.8% to 43.3% (Table 1).
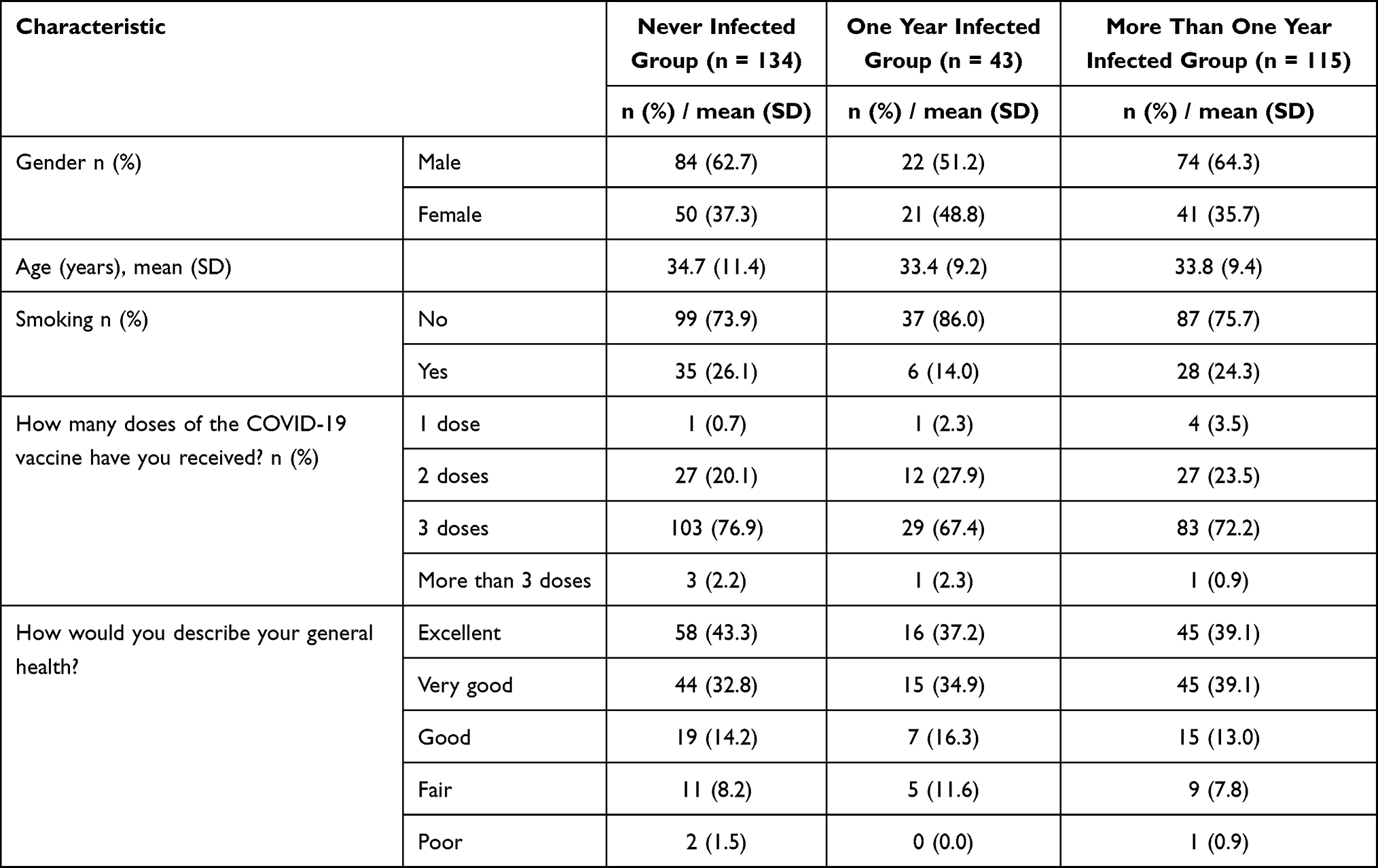 |
Table 1 Baseline Characteristics of Study Participants |
Quality of Life
When comparing various SF-36 subscales using One-way ANOVA, including physical functioning, role limits brought on by physical health issues, role restrictions brought on by personal or emotional issues, energy/fatigue, and emotional well-being, no significant differences were observed between the three groups. Similarly, there were no significant differences in HAM-A and HDRS scores. However, the analysis revealed a noteworthy finding: the social functioning subscale of the SF-36 showed a significant difference between the groups (F (2, 289) = 6.094, p = 0.01) with an effect size of d = 0.95 as measured by Cohen’s d indicating a large effect (Table 2).
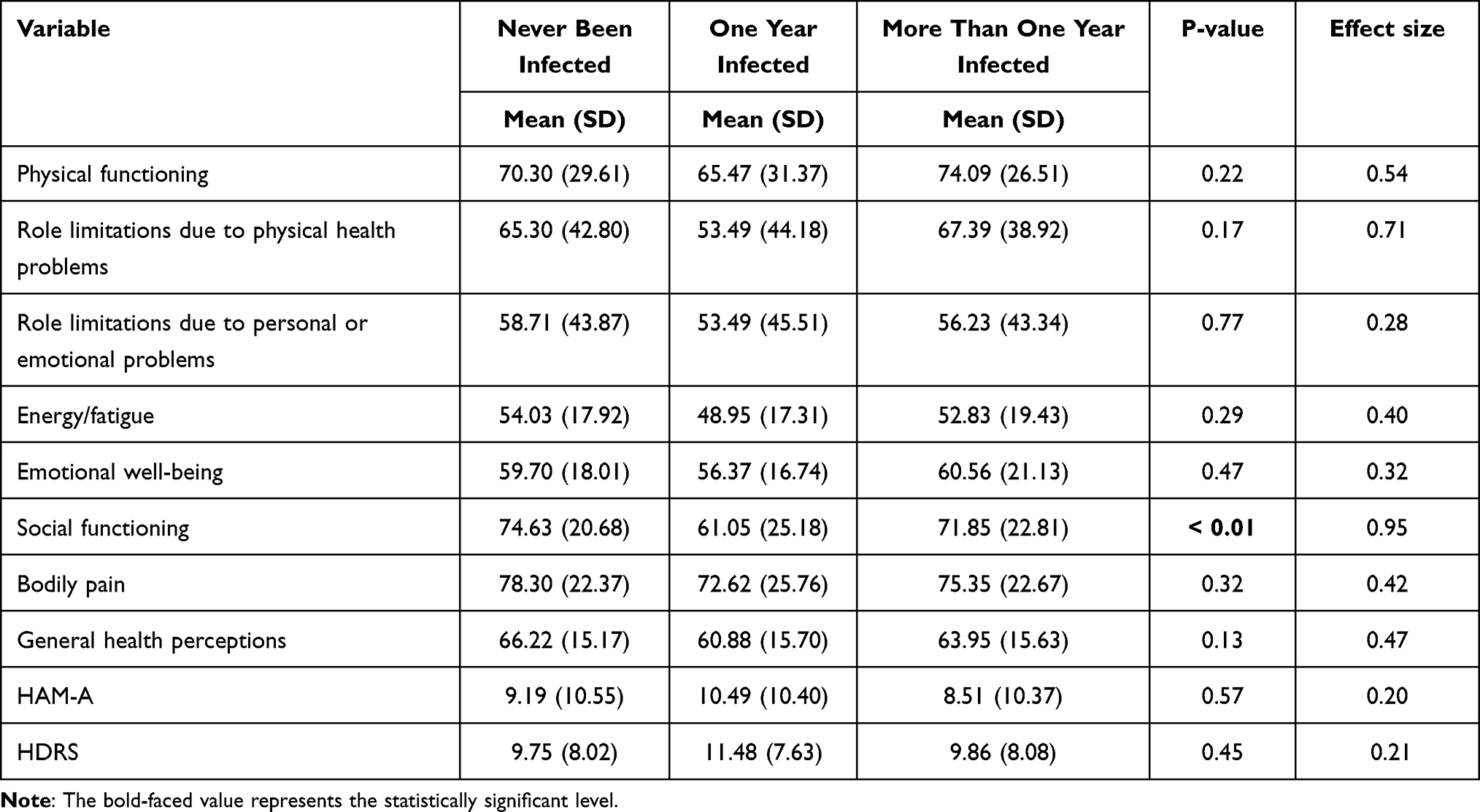 |
Table 2 SF-36, HAM-A, and HDRS Questionnaires Comparison Between the Groups |
Anxiety and Depression
The mean (M) and standard deviation (SD) for Hamilton Anxiety Rating Scale (HAM-A) scores were as follows: for the “never been infected” group, M = 9.19 (SD = 10.55); for the One year infected group, M = 10.49 (SD = 10.40); and for the More than one year infected group, M = 8.51 (SD = 10.37). There were no statistically significant differences between the groups for HAM-A scores, (F (2, 89) = 0.565, p = 0.57). Moreover, Cohen’s effect size value (d = 0.20) suggested a low practical significance (Table 2).
Similarly, for Hamilton Depression Rating Scale (HDRS) scores, the means and standard deviations were as follows: “Never been infected” group, M = 9.75 (SD = 8.02); “one-year infected” group, M = 11.48 (SD = 7.63); “more than one year infected” group, M = 9.86 (SD = 8.08). No significant differences were observed among the groups for HDRS scores, F (2, 288) = 0.797, p = 0.45). Moreover, Cohen’s effect size value (d = 0.21) suggested a low practical significance (Table 2).
While most variables did not exhibit significant differences, the bar charts showed an intriguing trend. Values across all variables were consistently worse in individuals who had been infected in the last year, compared to those who had never been infected. Notably, individuals with more than one year infection exhibited scores within the normal range compared to both the never-infected individuals and those who had experienced the infection for more than one year (Figures 2 and 3).
 |
Figure 2 Comparison of SF-36 scores between the groups. |
 |
Figure 3 Comparison of HAM-A and HDRS scores between the groups. |
Comparison Between Groups
Pairwise comparison showed that individuals who were infected in the last year showed a significant reduction in social functioning compared to both individuals who had never been infected (mean difference −13.58 (4.40–22.76) p < 0.01) and those infected more than one year ago (mean difference −10.80 (1.44–20.16) p = 0.02) (Tables 2 and 3).
 |
Table 3 Pairwise Comparison for Social Functioning |
Discussion
The present study aimed to explore the impact of COVID-19 on both short-term and long-term Health-Related Quality of Life (HRQoL) and psychological outcomes within the Saudi population. Through the assessment of HAM-A and HDRS scores, our investigation revealed noteworthy insights into the psychological implications of COVID-19 infection across different time frames. HAM-A and HDRS scores showed mild levels of anxiety and depression in all groups. Based on the scores of HAM-A and HDRS, our study found a slight increase in anxiety and depression in individuals infected one year ago compared to the never-infected individuals and the individuals with more than one year of infection. Additionally, we examined the broader dimensions of HRQoL using the SF-36 questionnaire, shedding light on the multifaceted consequences of the pandemic on individuals’ well-being. Likewise, the overall HRQoL was also lower in individuals infected one year ago compared to the never-infected individuals and the individuals with more than one year of infection. The score of the social functioning subscale of SF-36 showed a significant difference between the groups.
Our findings indicated higher levels of anxiety and depression among individuals who had contracted COVID-19 one year prior compared to both the never-infected individuals and those who had experienced the infection for more than one year. This elevation in psychological distress, although modest, underscores the potential persistence of mental health challenges even after the acute phase of the infection. These results align with emerging evidence that suggests the existence of post-acute psychological symptoms in a subset of individuals who have recovered from COVID-19.39,40
Intriguingly, when comparing individuals infected one year ago to both those who had never been infected and those with infections exceeding one year, we observed consistently lower HRQoL scores in individuals infected one year ago. The declined HRQoL may be linked with prolonged isolation, anxiety, and depression caused by viral infection.40 One plausible explanation is that survivors of COVID-19 exceeding one year may have developed a heightened sense of resilience and appreciation for life, leading to an improved subjective assessment of their overall well-being.41
The individuals infected one year ago showed lower scores in all domains of SF-36 and the energy/fatigue domain was recorded at the lowest level. This represents a compromised HRQoL in this group that may have extended beyond the acute phase of the disease. In line with our findings, previous studies reported that all domains of SF-36 of quality of life reduced after COVID-19 infection.11,42 The significant difference in the social functioning subscale of the SF-36 questionnaire among the studied groups is of particular importance. This difference underscores the intricate interplay between mental health and social interactions, indicating that individuals infected with COVID-19 more than one year ago might have adapted more effectively to the altered social landscape brought about by the pandemic. This finding is consistent with studies suggesting that individuals with prior exposure to stressors may develop coping strategies that facilitate better adaptation to subsequent challenges.43
The consistently mild level of anxiety and depression observed across all groups, as indicated by the HAM-A and HDRS scores, provides valuable context for understanding the psychological impact of COVID-19 within the Saudi population. However, the mean scores in the year-infected group were slightly higher than the other groups. This observation of mild anxiety and depression levels aligns with the findings of several international studies that have reported a general increase in psychological distress during the pandemic.39 This is in line with a study conducted in India by Kaur, Nimarpreet et al who also reported a mild level of psychological impact in the majority of the general population.44 The presence of mild anxiety and depression levels in both individuals infected and those never infected suggests a broader societal impact of the pandemic beyond the direct physiological effects of the virus. The reason for anxiety in the general population irrespective of infection can be due to anxiety and depression was associated with the fear of COVID-19 in previous studies.45 Moreover, the restricted leisure and social activities also imposed a psychosocial impact on the general population.12,13 This underscores the need for comprehensive mental health support for the entire population, irrespective of infection status.
The anxiety and depression symptoms were prevalent across different countries and populations, reflecting the shared global experience of uncertainty and disruption caused by COVID-19. This finding also echoes the broader recognition that the pandemic has had a widespread influence on mental health, irrespective of infection status.39,44 Our findings differ from studies from other authors in which they reported severe psychological impact and post-traumatic stress disorder symptoms.46
Interestingly, our study’s finding of a slight elevation in anxiety and depression among individuals infected one year ago compared to those with a longer infection duration of more than 12 months ago might indicate a potential trajectory of psychological adjustment over time. Individuals with longer infection duration could have adapted and developed coping mechanisms to better manage the psychological implications of the pandemic, leading to comparatively lower levels of anxiety and depression. On the other hand, those who were infected one year ago might still be navigating the transition from acute to post-acute phases of recovery, potentially contributing to the observed increase in symptoms.
Strengths and Limitations
Indeed, here are some potential strengths of the study on the short-term and long-term impact of COVID-19 on quality of life and psychological outcomes in Saudi Arabia. The study contributes to the growing body of knowledge regarding the multifaceted impact of COVID-19 on mental health and quality of life, particularly in the context of Saudi Arabia. The study utilized well established and validated assessment tools such as the SF-36, HAM-A, and HDRS, which enhanced the reliability and validity of the data collected. The study provides a temporal assessment of those who have been infected with COVID-19 at various time points to understand the evolving impact of the pandemic over time.
It is important to acknowledge the limitations of our study. Our analysis relied on self-reported measures, which could be influenced by recall bias and individual differences in reporting. Due to a lack of logistics support, we relied on non-probability sampling and findings may not be representative of the entire population, so researchers should be cautious when generalizing results. A cross-sectional design does not enable the exploration of causal relationships; to investigate deeper into causation longitudinal studies are imperative. We acknowledge the limitation of a relatively small sample size and the uneven distribution within the groups. Additionally, our study did not consider potential confounding variables such as access to healthcare, and social characteristics, which could affect our results.
Conclusions
In conclusion, the influence of COVID-19 on psychological well-being and Health-Related Quality of Life (HRQoL) outcomes within the Saudi population is significant, regardless of whether individuals have been infected with the virus. The observed increase in anxiety and depression among those infected, even one year after recovery, underscores the need for continued mental health support for individuals post-infection. The psychological and HRQoL impact of the pandemic extends beyond medical parameters and underscores the importance of addressing broader psychosocial factors that influence well-being. Further research is warranted to unravel the mechanisms underlying these patterns and to inform targeted interventions for those affected.
Abbreviations
SF-36, Short Form 36 Health Survey Questionnaire; HAM-A, Hamilton Anxiety Rating Scale; HDRS, Hamilton depression rating scale; HRQoL, Health-related quality of life; COVID-19, Coronavirus disease 2019; ANOVA, Analysis of variance; SPSS, Statistical Package for the Social Sciences.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. Ethical approval was gained for the current study from the ethical committee of Hail University under the ethics number H-2021-236. Informed consent was obtained from every study participant before the commencement of data collection.
Acknowledgments
We would like our thanks to the Scientific Research Deanship at the University of Ha’il - Saudi Arabia for supporting this project through project number RG-21058.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research has been funded by the Scientific Research Deanship at the University of Ha’il - Saudi Arabia through project number RG-21058.
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Holshue ML, DeBolt C, Lindquist S. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020;382(10):929–936. doi:10.1056/NEJMoa2001191
2. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109(102433):102433. doi:10.1016/j.jaut.2020.102433
3. Bassetti M, Vena A, Giacobbe DR. The novel Chinese coronavirus (2019-nCoV) infections: challenges for fighting the storm. Eur J Clin Invest. 2020;50(3):e13209. doi:10.1111/eci.13209
4. Covid ME. WHO declares pandemic because of ‘alarming levels’ of spread, severity, and inaction. BMJ. 2020;368:m1036. doi:10.1136/bmj.m1036
5. Siddiqui AA, Alshammary F, Amin J, et al. Knowledge and practice regarding prevention of COVID-19 among the Saudi Arabian population. Work. 2020;66(4):767–775. doi:10.3233/WOR-203223
6. Alshammary F, Siddiqui AA, Amin J, et al. Prevention knowledge and its practice towards COVID-19 among general population of Saudi Arabia: a gender-based perspective. Curr Pharm Des. 2021;27(13):1642–1648. doi:10.2174/1381612826666200818213558
7. Covid 19 dashboard: Saudi Arabia. Available from: https://covid19.moh.gov.sa/.
8. Kiekens C, Boldrini P, Andreoli A. Rehabilitation and respiratory management in the acute and early post-acute phase. ‘Instant paper from the field’ on rehabilitation answers to the COVID-19 emergency. Eur J Phys Rehabil Med. 2020;56(3):323–326. doi:10.23736/S1973-9087.20.06305-4
9. Chan MHM, Chan PKS, Griffith JF. Steroid-induced osteonecrosis in severe acute respiratory syndrome: a retrospective analysis of biochemical markers of bone metabolism and corticosteroid therapy. Pathology. 2006;38(3):229–235. doi:10.1080/00313020600696231
10. Tenforde MW, Kim SS, Lindsell CJ. Symptom duration and risk factors for delayed return to usual health among outpatients with COVID-19 in a multistate health care systems network - United States, March-June 2020. Morb Mortal Wkly Rep. 2020;69(30):993–998. doi:10.15585/mmwr.mm6930e1
11. Poudel AN, Zhu S, Cooper N. Impact of Covid-19 on health-related quality of life of patients: a structured review. PLoS One. 2021;16(10):e0259164. doi:10.1371/journal.pone.0259164
12. Verveen A, Wynberg E, Willigen HDG. Health-related quality of life among persons with initial mild, moderate, and severe or critical COVID-19 at 1 and 12 months after infection: a prospective cohort study. BMC Med. 2022;20(422). doi:10.1186/s12916-022-02615-7
13. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. 2021;8(2):141–149. doi:10.1016/S2215-0366(20)30482-X
14. Lee SA, Jobe MC, Mathis AA, Gibbons JA. Incremental validity of coronaphobia: coronavirus anxiety explains depression, generalized anxiety, and death anxiety. J Anxiety Disord. 2020;74(102268):102268. doi:10.1016/j.janxdis.2020.102268
15. Pequeno NPF, A CNL, Marchioni DM, Lima SCVC, Lyra CDO. Quality of life assessment instruments for adults: a systematic review of population-based studies. Health Qual Life Outcomes. 2020;18(208). doi:10.1186/s12955-020-01347-7
16. Chen KY, Li T, Gong FH, Zhang J-S, Li X-K. Predictors of health-related quality of life and influencing factors for COVID-19 patients, a follow-up at one month. Front Psychiatry. 2020;11(668). doi:10.3389/fpsyt.2020.00668
17. Talman S, Boonman-de Winter L, De Mol M, Hoefman E, Van Etten R, De Backer I. Pulmonary function and health-related quality of life after COVID-19 pneumonia. Respir Med. 2021;176(106272). doi:10.1016/j.rmed.2020.106272
18. Van den Borst B, Peters JB, Brink M, et al. Comprehensive health assessment 3 months after recovery from acute coronavirus disease 2019 (COVID-19. Clin Infect Dis an off Publ Infect Dis Soc Am. 2021;73(5):e1089–e1098. doi:10.1093/cid/ciaa1750
19. Jacobs LG, Gourna Paleoudis E, Lesky-di bari D. Persistence of symptoms and quality of life at 35 days after hospitalization for COVID-19 infection. PLoS One. 2020;15(12):e0243882. doi:10.1371/journal.pone.0243882
20. Tessitore E, Handgraaf S, Poncet A. Symptoms and quality of life at 1-year follow up of patients discharged after an acute COVID-19 episode. Swiss Med Wkly. 2021;151(4950):w30093. doi:10.4414/SMW.2021.w30093
21. Huang L, Yao Q, Gu X, et al. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. Lancet. 2021;398(10302):747–758. doi:10.1016/S0140-6736(21)01755-4
22. Betschart M, Rezek S, Unger I. One year follow-up of physical performance and quality of life in patients surviving COVID-19: a prospective cohort study. Swiss Med Wkly. 2021;151(4344):w30072. doi:10.4414/SMW.2021.w30072
23. Erber J, Wießner ZJR, Reiter S, Eli I, Winocur E, Sarig R. Longitudinal assessment of health and quality of life of COVID-19 patients requiring intensive care-an observational study. J Clin Med. 2021;11(1):10. doi:10.3390/jcm11010010
24. Gamberini L, Mazzoli CA, Prediletto I. Health-related quality of life profiles, trajectories, persistent symptoms and pulmonary function one year after ICU discharge in invasively ventilated COVID-19 patients, a prospective follow-up study. Respir Med. 2021;189(106665):106665. doi:10.1016/j.rmed.2021.106665
25. Seeßle J, Waterboer T, Hippchen T. Persistent symptoms in adult patients 1 year after coronavirus disease 2019 (COVID-19): a prospective cohort study. Clin Infect Dis an off Publ Infect Dis Soc Am. 2022;74(7):1191–1198. doi:10.1093/cid/ciab611
26. Kaidar E, Sk AT, Kassymova S. Assessment of quality of life one year after in COVID-19 cases using the SF-36. J Clin Med Kazakhstan. 2022;19(6):13–17. doi:10.23950/jcmk/12644
27. Cevallos M, Egger M STROBE (STrengthening the Reporting of OBservational studies in Epidemiology). Guidelines for reporting health research: a user’s manual; 2014:169–179.
28. El Osta N, Kanso F, Saad R, Khabbaz LR, Fakhouri J, El Osta L. Validation of the Arabic version of the SF-36, generic questionnaire of quality of life related to health among the elderly in Lebanon. East Mediterr Heal J. 2019;25(10):706–714. doi:10.26719/emhj.19.041
29. AboAbat A, Qannam H, Bjorner JB, Al-Tannir M. Psychometric validation of a Saudi Arabian version of the sf-36v2 health survey and norm data for Saudi Arabia. J Patient-Reported Outcomes. 2020;4(67). doi:10.1186/s41687-020-00233-6
30. Sheikh K, Yagoub U, El-Setouhy M. Reliability and validity of the Arabic version of the SF-36 health survey questionnaire in population of khat chewers—Jazan Region-Kingdom of Saudi Arabia. Appl Res Qual Life. 2013;3:10.
31. Maier W, Buller R, Philipp M, Heuser I. The Hamilton Anxiety Scale: reliability, validity and sensitivity to change in anxiety and depressive disorders. J Affect Disord. 1988;14(1):61–68. doi:10.1016/0165-0327(88)90072-9
32. Sheikh KA, Yagoub U, Elsatouhy M, Al Sanosi R, Mohamud SA. Reliability and validity of the Arabic Version of the SF-36 health survey questionnaire in population of Khat Chewers—Jazan Region-Kingdom of Saudi Arabia. Appl Res Qual Life. 2015;10(1):1–13. doi:10.1007/s11482-013-9291-1
33. Ryan JM, Corry JR, Attewell R, Smithson MJ. A comparison of an electronic version of the SF-36 general health questionnaire to the standard paper version. Qual Life Res. 2002;11(1):19–26. doi:10.1023/A:1014415709997
34. Ware JEJ, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. doi:10.1097/00005650-199206000-00002
35. Hamilton M. Development of a rating scale for primary depressive illness. Br J Soc Clin Psychol. 1967;6(4):278–296. doi:10.1111/j.2044-8260.1967.tb00530.x
36. Alhadi AN, Alarabi MA, Alshomrani AT, Shuqdar RM, Alsuwaidan MT, McIntyre RS. Arabic translation, validation and cultural adaptation of the 7-item Hamilton Depression Rating Scale in two community samples. Sultan Qaboos Univ Med J. 2018;18(2):e167–72. doi:10.18295/squmj.2018.18.02.008
37. Shaddad AMAK, Hussein AARM, Tohamy AMA, Khaleel WGE. Cognitive impact on patients with COVID-19 infection. Egypt J Bronchol. 2023;17(38). doi:10.1186/s43168-023-00213-6
38. Rajewska-Rager A, Dmitrzak-Weglarz M, Lepczynska N, Vassilikos V. Dimensions of the Hamilton Depression Rating Scale correlate with impulsivity and personality traits among youth patients with depression. J Clin Med. 2023;13(1):12. doi:10.3390/jcm13010012
39. Rathore HA, Hassan I, Ilyas M, et al. Psychological impact of COVID-19 lockdown on general population of Hail, Saudi Arabia. Med Sci. 2020;24(106):4682–4688.
40. Baig AM, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host–virus interaction, and proposed neurotropic mechanisms. ACS Chem Neurosci. 2020;11(7):995–998. doi:10.1021/acschemneuro.0c00122
41. Zhou F, Tao M, Shang L, et al. Assessment of sequelae of COVID-19 nearly 1 year after diagnosis. Front Med. 2021;8:717194. doi:10.3389/fmed.2021.717194
42. De Matos DG, Aidar FJ, Almeida-Neto PF, et al. The impact of measures recommended by the government to limit the spread of coronavirus (COVID-19) on physical activity levels, quality of life, and mental health of Brazilians. Sustainability. 2020;12(21):9072. doi:10.3390/su12219072
43. Dyson R, Renk K. Freshmen adaptation to university life: depressive symptoms, stress, and coping. J Clin Psychol. 2006;62(10):1231–1244. doi:10.1002/jclp.20295
44. Singh RK, Bajpai R, Kaswan P. COVID-19 pandemic and psychological wellbeing among health care workers and general population: a systematic-review and meta-analysis of the current evidence from India. Clin Epidemiol Global Health. 2021;11:100737. doi:10.1016/j.cegh.2021.100737
45. Ahorsu DK, Lin C-Y, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. 2020;3:1–9.
46. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.