Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Short- to Mid-Term Clinical Outcomes of Posterior-Stabilized Cementless Total Knee Arthroplasty with Trabecular Metal Components
Authors Momose T ![]() , Nakamura Y, Nakano M, Maeda T, Morioka S, Sobajima A
, Nakamura Y, Nakano M, Maeda T, Morioka S, Sobajima A ![]() , Nakatsuchi Y, Takahashi J
, Nakatsuchi Y, Takahashi J ![]() , Nawata M
, Nawata M
Received 19 May 2021
Accepted for publication 4 July 2021
Published 10 August 2021 Volume 2021:17 Pages 809—816
DOI https://doi.org/10.2147/TCRM.S320941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Takashige Momose,1 Yukio Nakamura,2 Masaki Nakano,2 Takashi Maeda,1 Susumu Morioka,3 Atsushi Sobajima,1 Yukio Nakatsuchi,1 Jun Takahashi,2 Masashi Nawata1
1Department of Orthopaedic Surgery, Marunouchi Hospital, Matsumoto, Nagano, 390-8601, Japan; 2Department of Orthopaedic Surgery, Shinshu University School of Medicine, Matsumoto, Nagano, 390-8621, Japan; 3Department of Orthopaedic Surgery, Chikuma Central Hospital, Chikuma, Nagano, 387– 8512, Japan
Correspondence: Yukio Nakamura
Department of Orthopaedic Surgery, Shinshu University School of Medicine, 3-1-1 Asahi, Matsumoto, Nagano, 390-8621, Japan
Tel +81-263-37-2659
Fax +81-263-35-8844
Email [email protected]
Objective: This study aimed to evaluate the short- to mid-term clinical results of posterior-stabilized trabecular metal total knee arthroplasty (TKA) with cementless fixation of all components and investigate the radiographic changes of tibial and patellar components and cut bone surfaces over time.
Methods: We retrospectively collected the data of 128 knees from 88 consecutive patients who had undergone initial TKA with NexGen LPS-Flex TM implants. A total of 66 knees from 45 patients (mean ± standard deviation age: 70.3 ± 7.5 years) met the selection criteria, which had been employed cementless fixation of all parts and at least 3 years of postoperative follow-up duration. Clinical evaluations included range of motion, conventional knee score, function score, postoperative complications, and revision. For radiological evaluations, the bone contact surface of each implant was divided into 7 zones for tibial component and 2 zones for patellar component. Each region was examined immediately after surgery, at 6 and 12 months, and then every year afterwards.
Results: The mean observation period of 45 subjects was 4.2 years. Adequate fixation of tibial components was maintained during follow-up, although the patellar components of 2 knees required revision after repeated falls. No loosening was observed in any implants. The initial gap in tibial components disappeared in all knees, and a reactive line remained in 4 knees. There were no revisions, except for 2 cases, which were ascribed to patellar component fracture caused by repeated falls.
Conclusion: Cementless posterior-stabilized trabecular metal TKA appears to be a good surgical option. Longer-term examination for revision cases is required to validate our results.
Keywords: cementless fixation, short- to mid-term clinical outcomes, total knee arthroplasty, trabecular metal components
Introduction
Biological reactions to insert particles are a common cause for revision in total knee arthroplasty (TKA). Implants have large metallic surfaces that may release wear products, such as metal ions and debris. Recent studies on material safety in total hip arthroplasty (THA) and TKA have led to concerns about the quality and reliability of joint arthroplasties.1–4 Thus, the optimal survival of knee implants is an important issue, which is reflected in the procedure revision rate.
Trabecular metal (TM) is a new type of three-dimensional implant that consists of tantalum, a transition metal with high porosity. The surface of TM is similar to that of cancellous bone, with high frictional coefficiency for excellent initial fixation, resulting in effective bone ingrowth in femoral, tibial, and patellar cut areas and biological fixation as compared with conventional cementless components. TM also has a low modulus of elasticity and near-bone extensibility, which makes it easier to deflect in bone contact surfaces than such metals as cobalt-chrome and titanium.5
To date, few reports have addressed the clinical outcomes of posterior-stabilized (PS) cementless TKA, while results of conventional PS TKA remain less favorable due to lift-off from mechanical stress in the post-cam mechanism and premature loosening of the tibial component. However, Dunbar et al showed good short-term clinical results with PS TM cementless TKA and stated that TM might be more tolerant to mechanical stress owing to its low modulus of elasticity.6 Moreover, there was a report that the implants promoted rapid osteogenesis and bone growth from internally connected pores, and were expected to achieve stable, long-term fixation.5
Although there have been some reports on the long term follow-up investigation of uncemented cruciate-retaining (CR) TKA,7 there exist no studies of mid- to long-term results regarding the PS-type cementless TKA. Thus, we are now following the clinical outcomes of PS TM cementless TKA procedure. Despite multiple attempts to enhance fixation with cementless technology, cemented TKA continues to be the gold standard. We have been using TM patellar components in PS TKA since their introduction in Japan. The present study aimed to evaluate the short- to mid-term clinical results of PS-type TM TKA with cementless fixation of all parts and examine the radiographic changes of tibial and patellar components and cut bone surfaces over time.
Patients and Methods
This study was approved by the Institutional Review Board of Marunouchi Hospital and Shinshu University School of Medicine, Japan, prior to its commencement. The research procedure was conducted in accordance with the ethical guidelines of the 2013 Declaration of Helsinki. Informed consent for research and publication was obtained in a form of opt-out on the website.
Patient Data
We retrospectively collected the data on 128 knees from 88 consecutive patients who had undergone initial TKA with NexGen LPS-Flex TM implants (Zimmer Biomet Holdings, Inc., Warsaw, IN) from April 2011 to March 2016. The analyzed subjects of the present investigation were 66 knees from 45 patients meeting the following selection criteria. Patients complicated with other diseases that might have an influence on knee motion postoperatively were excluded. This study included the patients who had completed at least 3 years of follow-up after surgeries with full outcome examinations. The demographic data of the patients in this study are presented in Table 1.
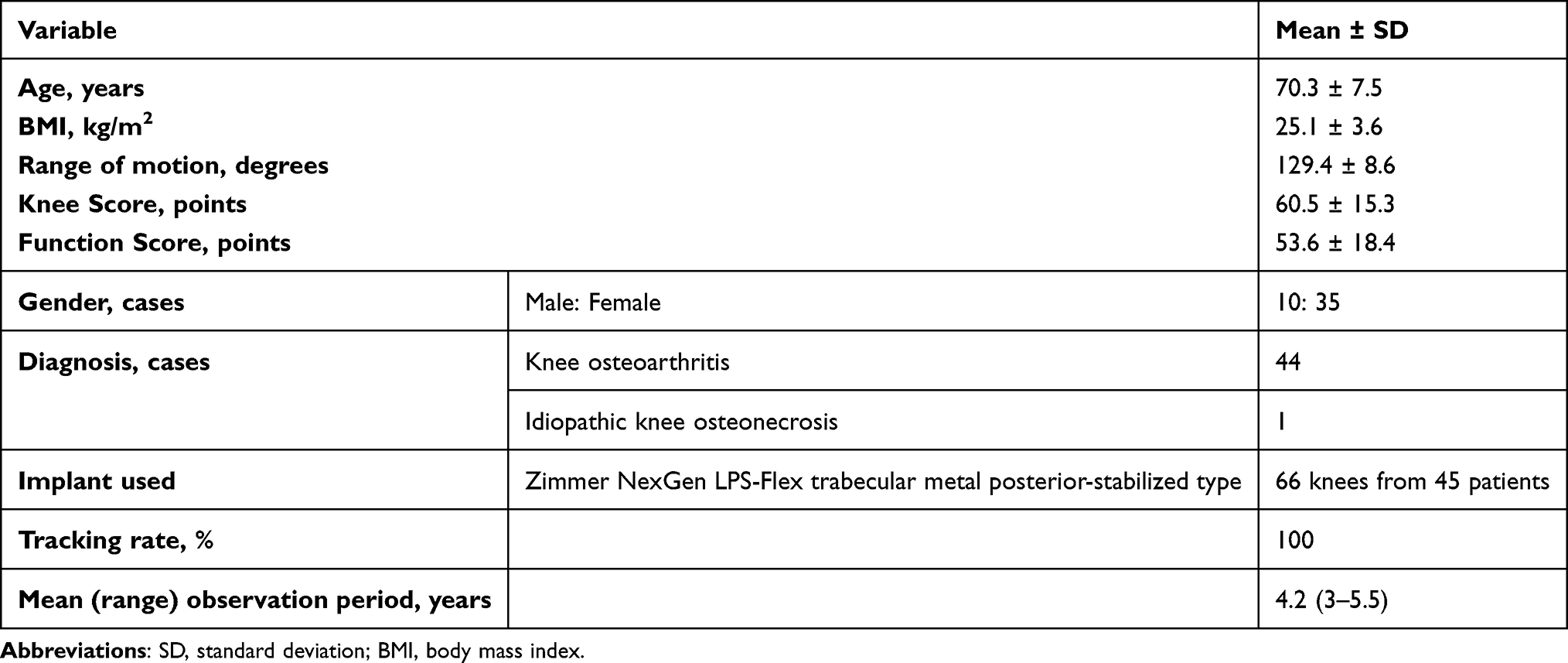 |
Table 1 Baseline Cohort Data |
Clinical Evaluation and Statistical Analysis
Clinical evaluations included range of motion (ROM), conventional (1989 version) Knee Score (KS) and Function Score (FS), postoperative complications, and revision. Imaging examinations were based on plain radiographs. The bone contact surface of each implant was divided into 7 zones for tibial component (A to G) and 2 zones for patellar component (pA and pB) (Figure 1). Each region was evaluated every 6 months from immediately postoperative and every year after 12 months of surgery. Since the femoral component had been fixed rigidly with its U-shaped design, a loosening was considered to hardly occur. Thus, the detailed assessment of femoral component was not made.
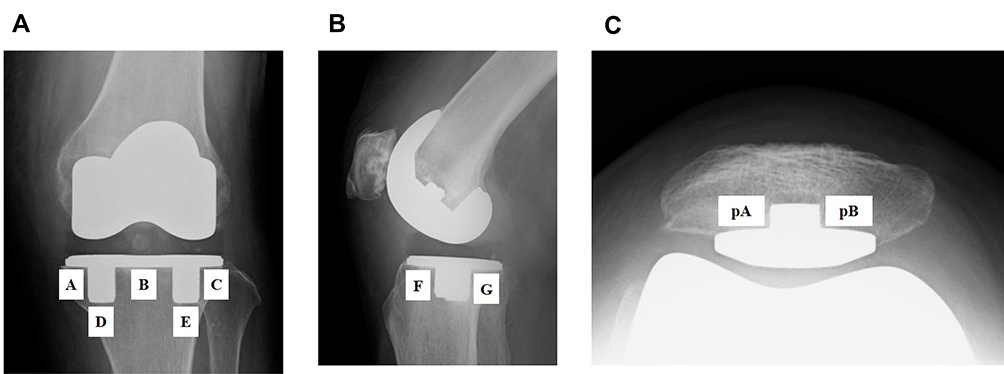 |
Figure 1 Radiographic division of (A and B) the tibial component into 7 zones (A–G) and (C) the patellar component into 2 zones (pA and pB). |
As for the fractured patellar component, we performed pathological examinations. Briefly, the excised peg and baseplate regions were fixed and embedded with polyester resin, and the center of each component was cut to create the specimens. Invaded connective tissue and bone ingrowth at contact regions were histologically examined by toluidine blue and alizarin red staining, respectively.
Statistical analysis of the clinical evaluations was performed by means of Kruskal–Wallis testing. A two-tailed p-value of < 0.05 was considered to be statistically significant.
Results
Immediately postoperative ROM was comparable to preoperative levels and was well maintained during the observation period (Figure 2). KS was significantly improved at 6 months postoperatively from mean preoperative scores (97.6 vs 60.5; p < 0.05), which was maintained throughout the follow-up period (Figure 3). A similar trend was observed for FS (80.7 at 6 months vs 53.6 at preoperative; p < 0.05) (Figure 4).
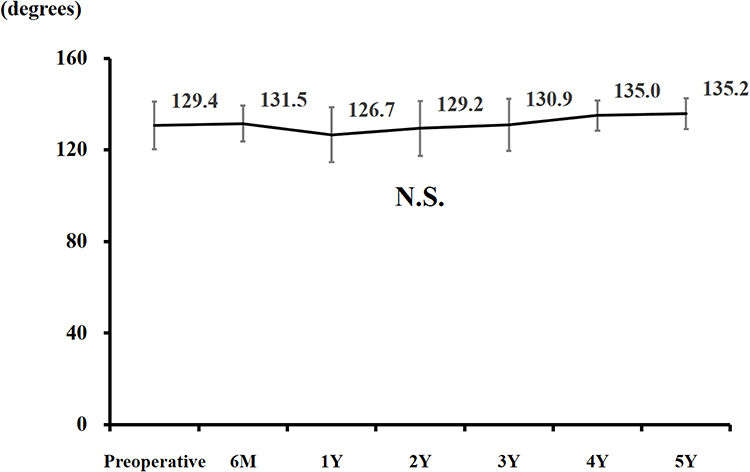 |
Figure 2 Changes in range of motion during the observation period. Statistical differences were assessed by the Kruskal–Wallis testing. Abbreviations: N.S., not significant; M, months; Y, years. |
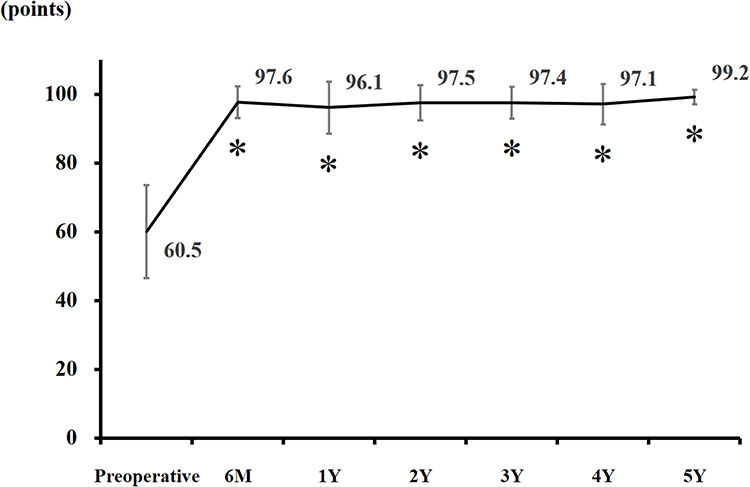 |
Figure 3 Changes in knee score during the observation period. Statistical differences were assessed by the Kruskal–Wallis testing (*p < 0.05 vs preoperative). Abbreviations: M, months; Y, years. |
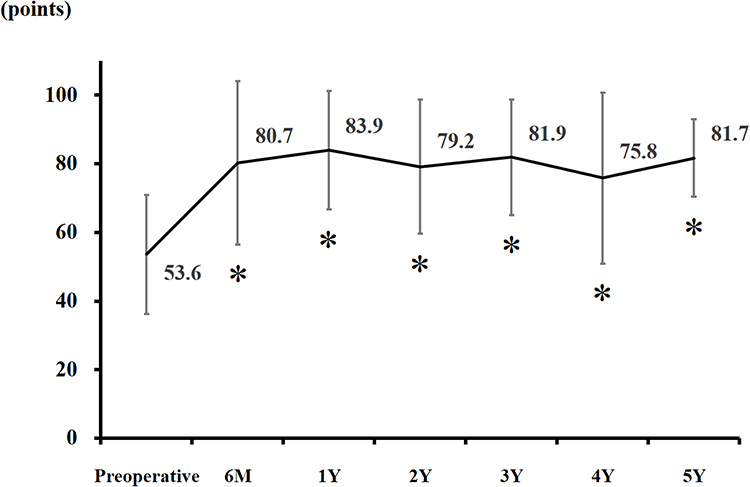 |
Figure 4 Changes in function score during the observation period. Statistical differences were assessed by the Kruskal–Wallis testing (*p < 0.05 vs preoperative). Abbreviations: M, months; Y, years. |
In imaging studies, immediately postoperative radiographic gaps on the tibial side were observed in 7 of 66 knees (10.6%). At 6 months postoperatively, they remained in 5 knees at zone A and 2 knees at zone C on the tibial side (Figure 5). The initial gaps had disappeared in all knees by 3 years of follow-up. Seven knees (10.6%) had an initial gap in the patellar component, 3 of which did not disappear during the observation period. Reactive lines were found predominantly in zone A (16 knees) of tibial components, appearing mainly on the base plate (Figure 6). In the tibial components, reactive lines were detectable in 27.3% of cases and tended to disappear over time. The lines had disappeared in 14 cases at the final observation. No clinical pain or other problems were recorded in the cohort subjects, and no cases of loosening occurred. On the patellar side, no problems were noted during the observation period.
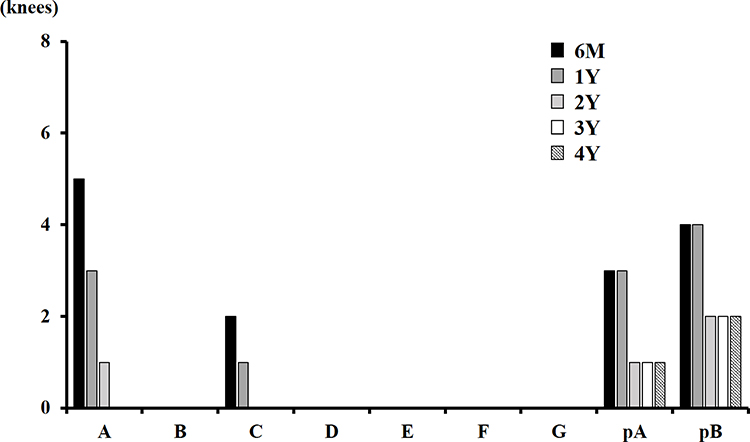 |
Figure 5 Number of knees with radiographic gaps during the observation period. Zones are as defined in Figure 1. Abbreviations: M, months; Y, years. |
 |
Figure 6 Number of knees with radiographic reactive lines during the observation period. Zones are as defined in Figure 1. Abbreviations: M, months; Y, years. |
A patellar component fracture at the base of the peg was observed in 2 knees (3.0%) and required revision. Both injuries were caused by repeated falls within 12 months after surgery. At the time of patellar revision surgery, the initial gaps had not disappeared. In the pathological examination of fractured patellar components, we observed the invasion of fibrous connective tissue and bone ingrowth into the porous regions in peg specimens (Figure 7), whereas baseplate region demonstrated insufficient early bone ingrowth. The survival rate of PS-type TM TKA with cementless fixation of all components was 97.0% over the mean observational period of 4.2 years.
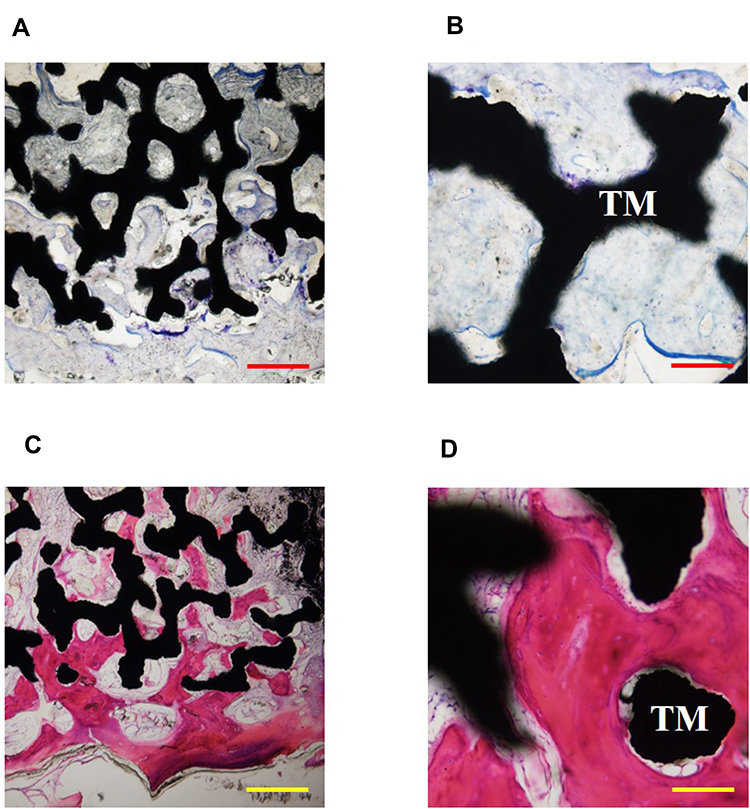 |
Figure 7 Pathological examination of the fractured patellar component peg region. (A and B) Toluidine blue and (C and D) alizarin red staining were performed to examine the invaded connective tissue and bone ingrowth, respectively. Respective bars indicate 500 µm (A and C) and 100 µm (B and D). Abbreviation: TM, trabecular metal. |
Discussion
In the present study, we observed significant improvements in KS and FS during 4.2 years of average follow-up period after PS-type TM TKA with cementless fixation of all parts. There recorded no clinical pain and other problems in the cohort subjects, and no cases of loosening occurred. Two cases of patellar component fracture caused by repeated falls were observed and required revision. The survival rate of this TKA procedure over the follow-up period was 97.0%. Since there have been no reports on the mid- to long-term clinical outcomes of PS cementless TKA, the present study would provide a new insight for this procedure.
TKA and THA are very important techniques to improve mobility as well as quality of life in patients. TKA is one of the most frequent orthopaedic procedures and represents a very effective treatment option for advanced osteoarthritis of the knee for decreasing pain and ameliorating functions.8 As the number of younger and more active patients treated with TKA continues to increase, the consideration of better fixation as a means of improving implant longevity is required.9
There remains a certain percentage of TKA cases with poor postoperative outcomes that require revision surgery. The number of revision TKA procedures is rising in many countries, with 22,403 procedures in the United States10 and 15,232 in Australia.11 In Japan, the revision rate of knee arthroplasty is also on the rise.12 According to previous reports, polyethylene wear, aseptic loosening, and instability are common causes of TKA failure.13,14 Thus, to avoid revision, optimal techniques and implant materials for TKA should be explored.
A recent randomized trial reported no differences in any clinical outcomes from 1 month to an average of 2 years postoperatively between cemented and cementless TKA procedures.15 Moreover, no significant differences in the rate of revision between cemented (4.0%) and uncemented (4.9%) groups have been demonstrated in a meta-analysis.16 Regarding the contemporary cementless TKA, the revision incidence per 1000 person-years was shown to be 4.8 for all cementless TKA designs, and the mean postoperative KS and FS were 92 and 83, respectively.17
This study clarified the clinical outcomes of PS cementless TM TKA during an average of 4.2 years follow-up after surgery. KS and FS were successfully improved and maintained during the observation period, and the scores were comparable to contemporary cementless TKA designs.17 The short- to mid-term clinical results were good, the initial tibial component gaps disappeared in all cases over time, there was no implant loosening, and good fixation to each bone was maintained. Although reactive lines remained in 4 knees, there were no clinically problematic cases which indicated that the tibial component of TM had sufficient bone anchorage for PS cementless TKA and could be expected to remain stable longer than 4 years postoperatively. Radiographic gaps would imply the insufficient bone ingrowth, and thus the zones with gaps were inferred to be bonded with fibrous connective tissue alone. The gaps were characteristically observed in lateral sides of tibial component and baseplate of patellar component. The location of remaining gaps might reflect the difference in mechanical loading distributions.
On the other hand, the patellar component fractured in 2 knees (3.0%) in the early period after surgery due to repeated falls. We observed the invasion of fibrous connective tissue and bone ingrowth into the porous regions in peg, whereas baseplate region demonstrated insufficient early bone ingrowth after 12 months of surgery. Considering the histological findings, the patellar component could be fractured due to shear force since only peg region was fixed firmly. Careful attention to initial fixation of patellar components will be required for a better postoperative prognosis and an avoidance of revision surgeries. Clinically, it may be advisable to inform patients on the possibility of a patellar component fracture by falling in the year after TKA. The survival rate observed over the follow-up period in this study was 97.0%. No clinical pain and other problems including aseptic failure and loosening were recorded in the cohort. Since there were no revisions, except for two cases, which were ascribed to patellar component fracture caused by repeated falls, PS cementless TM procedure might be a good option for TKA.
The limitations of the current study were its retrospective design and relatively small number of subjects. Long term follow-up observation will be needed to confirm our novel findings.
Conclusion
This study clarified the short- to mid-term clinical outcomes of PS cementless TM TKA during a mean of 4.2 years of follow-up after surgeries. Adequate fixation of tibial components was maintained without any detectable loosening. The femoral components were stable without any radiographic loosening in all cases over the follow-up period, suggesting that it was rigidly fixed with its U-shaped design and associated with little mechanical stress. In patellar components, 2 knees (3.0%) showed premature failure after early repeated falls, potentially because the patellar component might be fixed firmly by peg region alone with insufficient early bone ingrowth at baseplate region. Cementless PS-type TM TKA appears to be an effective method of knee joint replacement that warrants validation in larger studies. Since there have been no reports on the mid- to long-term results of this procedure design, we continue to follow the clinical outcomes of the cohort.
Acknowledgments
The authors would like to thank Mr Trevor Ralph for his English editorial assistance. This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All of the authors have declared that there were no conflicts of interest in this study.
References
1. Godlee F. Serious risks from metal-on-metal hip implants. BMJ. 2012;344(mar01 1):e1539. doi:10.1136/bmj.e1539
2. Smith AJ, Dieppe P, Vernon K, Porter M, Blom AW. Failure rates of stemmed metal-on-metal hip replacements: analysis of data from the National Joint Registry of England and Wales. Lancet. 2012;379(9822):1199–1204. doi:10.1016/S0140-6736(12)60353-5
3. Labek G, Neumann D, Agreiter M, Schuh R, Böhler M. Impact of implant developers on published outcome and reproducibility of cohort-based clinical studies in arthroplasty. J Bone Joint Surg Am. 2011;93(Suppl 3):55–61. doi:10.2106/JBJS.K.01108
4. Pabinger C, Berghold A, Boehler N, Labek G. Revision rates after knee replacement. Cumulative results from worldwide clinical studies versus joint registers. Osteoarthritis Cartilage. 2013;21(2):263–268. doi:10.1016/j.joca.2012.11.014
5. Bobyn JD, Hacking SA, Chan SP, Toh KK, Krygier JJ, Tanzer M. Characterization of new porous tantalum biomaterial for reconstructive orthopaedics.
6. Dunbar MJ, Wilson DA, Hennigar AW, Amirault JD, Gross M, Reardon GP. Fixation of a trabecular metal knee arthroplasty component. A prospective randomized study. J Bone Joint Surg Am. 2009;91(7):1578–1586. doi:10.2106/JBJS.H.00282
7. Costales TG, Chapman DM, Dalury DF. The natural history of radiolucencies following uncemented total knee arthroplasty at 9 years. J Arthroplasty. 2020;35(1):127–131. doi:10.1016/j.arth.2019.08.032
8. Carr AJ, Robertsson O, Graves S, et al. Knee replacement. Lancet. 2012;379(9823):1331–1340. doi:10.1016/S0140-6736(11)60752-6
9. Dalury DF. Cementless total knee arthroplasty: current concepts review. Bone Joint J. 2016;98-B(7):867–873. doi:10.1302/0301-620X.98B7.37367
10. Registry AJR. American Joint Replacement Registry. ISSN 2375-9119 (online). Annual Report 2014; 2014. Available from: www.ajrr.net.
11. Australian Orthopaedic Association National Joint Replacement Registry. Annual report. Adelaide: AOA; 2015.
12. Analysis of cumulative revision rates in THA, TKA/UKA/PFA 2013–2017. Summary report. Tokyo, Japan:JSRA; 2020.
13. Sharkey PF, Hozack WJ, Rothman RH, Shastri S, Jacoby SM; Insall Award Paper. Why are total knee arthroplasties failing today? Clin Orthop Relat Res. 2002;404:7–13. doi:10.1097/00003086-200211000-00003
14. Kasahara Y, Majima T, Kimura S, Nishiike O, Uchida J. What are the causes of revision total knee arthroplasty in Japan? Clin Orthop Relat Res. 2013;471(5):1533–1538. doi:10.1007/s11999-013-2820-2
15. Nam D, Lawrie CM, Salih R, Nahhas CR, Barrack RL, Nunley RM. Cemented versus cementless total knee arthroplasty of the same modern design: a prospective, randomized trial. J Bone Joint Surg Am. 2019;101(13):1185–1192. doi:10.2106/JBJS.18.01162
16. Liu Y, Zeng Y, Wu Y, Li M, Xie H, Shen B. A comprehensive comparison between cementless and cemented fixation in the total knee arthroplasty: an updated systematic review and meta-analysis. J Orthop Surg Res. 2021;16(1):176. doi:10.1186/s13018-021-02299-4
17. Bingham JS, Salib CG, Hanssen AD, Taunton MJ, Pagnano MW, Abdel MP. Clinical outcomes and survivorship of contemporary cementless primary total knee arthroplasties. JBJS Rev. 2020;8(8):e2000026. doi:10.2106/JBJS.RVW.20.00026
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.