Back to Journals » Degenerative Neurological and Neuromuscular Disease » Volume 13
Sexual Motivation in Persons with Multiple Sclerosis: A Controlled Cross-Sectional Study
Authors Prinssen P, Jongen PJ ![]() , Heerings M, Wyverkens E, T'Sjoen G, Deschepper E, Dewitte M
, Heerings M, Wyverkens E, T'Sjoen G, Deschepper E, Dewitte M
Received 10 January 2023
Accepted for publication 10 June 2023
Published 28 June 2023 Volume 2023:13 Pages 33—44
DOI https://doi.org/10.2147/DNND.S401457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Thomas Müller
Petra Prinssen,1,2 Peter Joseph Jongen,3,4 Marco Heerings,5 Elia Wyverkens,6 Guy T’Sjoen,6 Ellen Deschepper,7 Marieke Dewitte8
1Praktijk Seksualiteit en welzijn, Roermond, 6045 GL, the Netherlands; 2Department of Public Health and Primary Care, Ghent University, Ghent, 9000, Belgium; 3MS4 Research Institute, Nijmegen, 6522 KJ, the Netherlands; 4Department of Community and Occupational Medicine, University Medical Centre Groningen, Groningen, 9713 AV, the Netherlands; 5Dutch National MS Foundation, Rotterdam, 3044 AT, the Netherlands; 6Department of Endocrinology, Center for Sexology and Gender, Ghent University Hospital, Ghent, 9000, Belgium; 7Biostatistics Unit, Department of Public Health and Primary Care, Ghent University, Ghent, 9000, Belgium; 8Department of Clinical Psychological Science, Faculty of Psychology and Neurosciences, Maastricht University, Maastricht, 6229 ER, the Netherlands
Correspondence: Peter Joseph Jongen, MS4 Research Institute, Ubbergseweg 34, Nijmegen, 6522 KJ, the Netherlands, Tel +31243239146 ; +31614037368, Email [email protected]
Purpose: Sexual motives are major determinants of sexual behaviour. It has been known that sexual motives may vary according to circumstances. Multiple sclerosis (MS) is a chronic disease causing a broad range of symptoms and disabilities, that often interfere with sexual activities. We aimed to investigate the sexual motives in persons with MS.
Patients and Methods: Cross-sectional study in 157 persons with MS and 157 controls matched for age, gender, relationship, duration of relationship and educational status via propensity score matching. The Reasons for Having Sex (YSEX) questionnaire assessed the proportion with which a person had engaged in sexual intercourse for each of 140 distinct motives to have sex. Estimated mean differences in scores for four primary factors (Physical, Goal attainment, Emotional, Insecurity) and 13 sub-factors, and sexual satisfaction and importance of sex were calculated as Average Treatment Effect of the Treated using 99% confidence intervals.
Results: Persons with MS reported a lower proportion of engaging in sex compared with the controls for the factors Physical (− 0.29), Emotional (− 0.23) and Insecurity (− 0.10); and for the physical sub-factors Pleasure (− 0.48), Experience seeking (− 0.32), Stress reduction (− 0.24), and Physical desirability (− 0.16), the emotional sub-factors Love and commitment (− 0.27) and Expression (− 0.17), and the insecurity sub-factor Self-esteem boost (− 0.23). In the control group seven of the top 10 sexual motives were physical versus five in the MS group. The importance of sex was lower in the MS group (− 0.68).
Conclusion: Findings of this controlled cross-sectional study suggest a reduction in the number of sexual motives in persons with MS, especially of physical motives related to pleasure and experience seeking. Health care professionals may consider assessing sexual motivation when dealing with persons with MS who suffer from decreased sexual desire or another sexual dysfunction.
Keywords: sexual motivation, reasons to have sex, importance of sex, YSEX questionnaire, sexual motive, multiple sclerosis
Introduction
Multiple sclerosis (MS) is a chronic demyelinating and degenerative disease of the central nervous system (CNS) that mainly affects persons between 20 and 45 years of age.1,2 The multi-focal and diffuse distribution of pathological changes in white and gray matter accounts for the wide range of symptoms and disabilities that may develop over time.1,2 The main clinical changes include motor disturbances, coordination problems, impaired vision, cognitive deficits, fatigue, sensory symptoms, and bladder and bowel dysfunction.1,2 In approximately 50–60% of the persons with MS the CNS pathology leads to profound and disabling changes in sexual functions and experiences.3–7 The most common complaints of sexual dysfunction in MS include reduced libido, difficulty in achieving an orgasm, decreased vaginal lubrication, erectile dysfunction, and ejaculatory dysfunction.8
Sexual desire or libido may be defined as the broad interest in sexual objects or experiences.9 It involves both physiological and psychological processes.10,11 In persons with MS a decreased sexual desire occurs in about 30–50% of the cases.6,7,10,12,13 Loss of sexual desire may be caused by CNS pathology – notably the limbic system and brain stem nuclei -, or by psychological mechanisms in response to MS symptoms’ interference with sexual activities.9
The construct of global sexual desire, however, has rather limited utility, both conceptually and in terms of accurately predicting behaviour.14–16 The multidimensional perspective of sexual motives, in contrast, has been shown to provide a more inclusive and accurate characterization of the various motivational functions regarding sex.14–17 Notably, sexual motives are more specific in their focus than the construct of global sexual desire,14,15 and study data indicate that sexual motives can be distinguished from global desire.14,15 Moreover, there is a distinctive relationship between specific sexual motives and sexual behaviour, controlling for the influence of global desire,14,15 and reactions to incentive-specific sexual situations are more strongly related to relevant sexual motives than to global sexual desire.15
Motives are directly related to sexual behaviour by preparing the person to approach versus to avoid sexual stimulation and thus engage or not engage in sexual activity. In fact, the motives with which people enter a sexual situation may determine whether they will open themselves to and accept sexual stimulation or not.18 Importantly, a wide variety of sexual motives may influence sexual behaviour,16,17,19 and an individual may experience various reasons or motives for interest in sex. Moreover, individual sexual motives may be uniquely correlated with sexual behaviour in situations specifically affording motive-related incentives.15,16
The study and knowledge of people’s sexual motivations are of interest to health and health promotion.16,20 Eg it has been shown that motives for sex can predict behaviour patterns, that can have negative consequences for health and well-being.21 As to MS, in view of the broad range of symptoms that may interfere with sexual activities, it is expected that what motivates persons with MS to engage in sex may change over time and becomes different from the motivation in persons without MS. Because a change in sexual motives is likely to affect sexual behaviour, it is important to explore in people with MS the reasons for having sex. Actually, knowledge of the diverse sexual motives can have profound implications for our comprehension of the causes, correlates, and consequences of sexual behaviour in persons with MS.22 More insight into the impact of MS on sexual motivation may help professional caregivers to better understand the underlying mechanisms and meaning of sexual problems in individual patients, eg to differentiate a motivation-related change in sexual behaviour versus a change resulting from a sexual dysfunction. As yet, however, there are no studies available that provide a comprehensive and detailed analysis of sexual motives in persons with MS.
In their pioneering study “Why humans have sex” Meston and Buss identified 140 different reasons for having sex, and developed a questionnaire (YSEX) in which these motives are categorized into four primary factors that were equivalent in men and women: physical reasons, goal attainment reasons, emotional reasons and insecurity reasons, while discerning two to four sub-factors for each of the primary factors.17,19 To replicate the Meston and Buss results and to broaden its scope the Waarom seks? (Why sex?) study was performed in a community-based sample in Belgium and the Netherlands, and in specific patient groups.23 The present Waarom seks en MS? (Why sex and MS?) study focused specifically on people with MS, which were compared with healthy controls obtained from the larger Waarom seks? cohort.23 By documenting whether sexual motives in persons with MS are different from those without MS, the present study can be important for developing more targeted and personalized interventions in persons with MS and sexual dysfunction, and may also serve as a basis for future studies into the interrelations between sexual motivation, sexual dysfunction and MS.17 We hypothesized that people with MS would report different motives to have sex, were less motivated to have sex, were less satisfied with their sexual life, and considered sex less important.
Materials and Methods
Web-based questionnaires were used to assess the motives why people had sex in the past year, their sexual satisfaction and the importance of sex. Sex was defined as sexual intercourse meaning entering the penis or other object into the vagina or anus.
Procedures
Recruitment
Waarom seks? study participants were recruited via press releases in Belgian and Dutch media, including newspapers (De Gazet van Antwerpen, Metro, De Morgen, De Standaard, De Telegraaf, Het Nieuwsblad), magazines (Flair, MS-Link) and websites (www.knack.be, www.mensenkennis.be). The Belgian TV Networks VTM and Canvas broadcasted information about the study. To recruit people with MS for the Waarom seks en MS? study we collaborated with the Dutch National MS Foundation (Rotterdam) and the MS4 Research Institute (Nijmegen) by using their research databases and online research facilities; with the Belgian National Multiple Sclerosis Centre (Melsbroek), the Multiple Sclerose Liga (Overpelt), the Charcot Foundation (Leuven); with the neurology departments of the Belgian hospitals Jessa Ziekenhuis (Hasselt), Universitair Ziekenhuis Ghent (Ghent), Academisch Ziekenhuis Sint-Jan (Brugge-Oostende) and the Dutch hospitals Laurentius Ziekenhuis (Roermond), Medisch Centrum Leeuwarden (Leeuwarden) and Catharina Ziekenhuis (Eindhoven); and with MS nurses in Belgium and the Netherlands (Network of the Dutch National MS Foundation). We focused on web-based recruitment by using websites of the organisations mentioned above, of the Ghent University, Facebook pages and personal Linked-in sites and e-mail contacts of the researchers.
Inclusion Criteria and Period
Any person who was sexually active, regardless of age, could participate in the Waarom seks? study and give her or his consent via www.waaromseks.be. Persons who had been diagnosed with MS could participate in the present Waarom seks en MS? study. There were no MS-specific inclusion or exclusion criteria. Data were acquired from January 27, 2014 to March 31, 2014.
Questionnaires
A URL (www.waaromseks.be) provided access to the study questionnaires which were presented via Lime Survey, an open-source web application for developing online surveys (www.limesurvey.org). First, a general questionnaire assessed, amongst others, gender, nationality, age, education level, employment status, sexual orientation, having a relationship, duration of relationship, number of years since MS diagnosis, disease modifying treatment, MS symptoms interfering with sexual activity, impact of MS on sexual life (What is the impact of MS on your sexual life? [very negative, negative, somewhat negative, no impact, positive, very positive, do not know]), overall quality of life (Overall, how would you rate your own quality of life? [0, worst possible – 10, best possible]),24 and feeling about life as a whole (Which best describes how you feel about your life as a whole? [terrible, unhappy, mostly dissatisfied, about equally satisfied and dissatisfied, mostly satisfied, pleased, delighted]).24
Then, the 140-item YSEX questionnaire assessed the various reasons why participants had engaged in sexual intercourse during the past year.17,19 The respondents were asked to indicate the proportion of how frequently they had sex for each of the 140 reasons on a 5-point Likert scale: None of my sexual experiences (1), A few of my sexual experiences (2), Some of my sexual experiences (3), Many of my sexual experiences (4), and All of my sexual experiences (5).19 The 140 items fell into four categories analytically derived as primary motives (physical, goal attainment, emotional, insecurity) and 13 sub-factors. The physical reasons sub-factors included stress reduction, pleasure, physical desirability, and experience seeking. The goal attainment sub-factors included resources, social status, revenge, and utilitarian. The emotional sub-factors included love and commitment, and expression. The insecurity sub-factors included self-esteem boost, duty/pressure, and mate guarding.17,19 The YSEX questionnaire has been shown to be internally reliable with sub-factor α coefficients ranging from 0.70 to 0.89.17,19
A validated Dutch version of the YSEX questionnaire was available.25 A previous study had found that the Dutch version had a high internal consistency, ranging from 0.79 to 0.97 for physical reasons and sub-factors, 0.81 to 0.97 for the emotional factor and sub-factors, and 0.83 to 0.97 for the insecurity factor and sub-factors. For the goal attainment factor and sub-factors, the α values ranged from 0.71 to 0.97, except for the sub-factors resources, revenge, and utilitarian.23 In all, the YSEX inventory was considered a reliable measure.23
Finally, the sexual satisfaction (Overall, how satisfied were you with your sexual function during the past four weeks?)24 and the importance of sex (How important is sex for you?) were assessed using a 5-point Likert scale (0, very dissatisfied / very unimportant – 5, very satisfied / very important).
Statistical Aspects
One person with MS was matched with one person from the control group, selected by means of a propensity scoring method based on a combination of the exact method for gender, education level and having a relationship, and a nearest neighbour method for age and duration of relationship, with caliper value set to 0.2. The balance between covariate distributions was assessed by means of balance diagnostics, and standardized means differences of 0.2 or less were considered to be acceptable. To analyze the sexual motivations in-depth we relied on the factor structure of Meston and Buss.17,19
Estimated mean differences in scores for factors, sub-factors, and sexual satisfaction and importance of sex are reported as Average Treatment Effect of the Treated (ATT).19 In this approach, a linear regression model adjusting for the confounders is fit to the matched data and predicted values of the dependent variables for the persons with MS are simulated as if they were controls, also known as counterfactual outcome values of the persons with MS. A 99% confidence interval (CI) was used to guard for multiple testing issues. All statistical analyses were performed in the statistical software package R (version 3.5.2).26 The MatchIt package was used for matching, together with the Zelig package to conduct the analyses after matching.27,28
Ethical Aspects
The study was approved by the Ethics Committee of the Ghent University Hospital, Ghent, Belgium. The study was performed in agreement with the Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects version 2013; 64th World Medical Association General Assembly, Fortaleza, Brazil, October 2013) (www.wma.net) and the Dutch Wet medisch-wetenschappelijk onderzoek met mensen (WMO).
Participants gave their informed consent via www.waaromseks.be. It took 35–45 minutes to complete the questionnaires. Confidentiality was protected by anonymous participation and data analysis. After having completed the questionnaires participants were given the option to submit their name and email address for a raffle for 100 euro’s. This latter information was disconnected from the answers and was not included in the information part of the informed consent.
Results
Participants
A total of 160 persons with MS were included in the Waarom seks en MS? study and 4655 persons in the Waarom seks? study. The demographic characteristics of the persons with MS are presented in Table 1, and the disease characteristics are presented in Table 2.
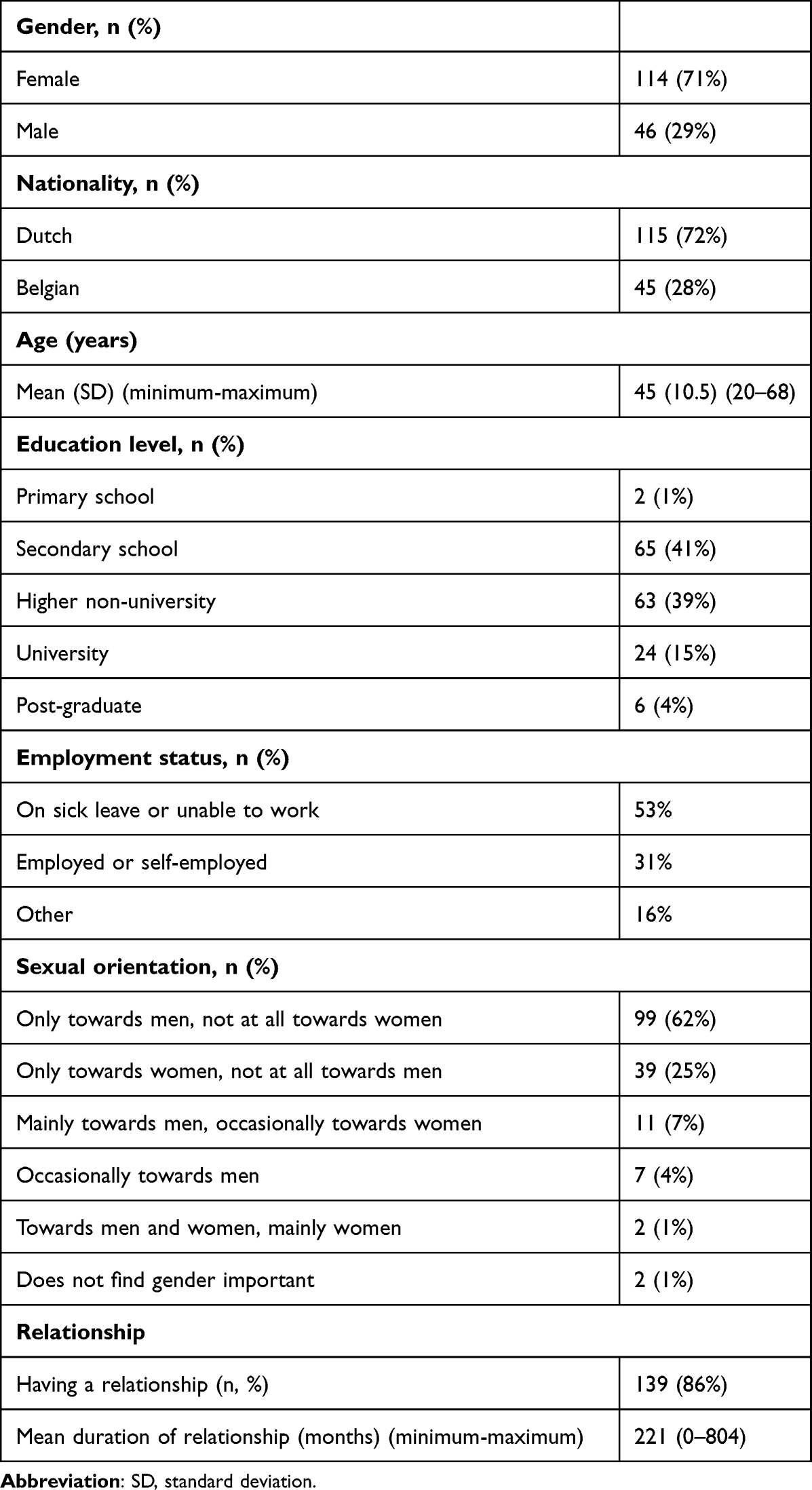 |
Table 1 Demographic Characteristics of Persons with MS (n=160) |
 |
Table 2 Disease Characteristics of Persons with MS (n=160) |
In brief, in the MS group, mean age was 45 years (median 46, 1st quartile [Q] 38, 3th Q 52, minimum 20, maximum 68); 115 (72%) persons were Dutch, 44 (28%) Dutch-speaking Belgian and 1 (1%) French-speaking Belgian; 114 (71%) were female and 46 (29%) male; and 139 (86%) had a relationship with a mean relationship duration of 221 months (median 298, 1st Q 76, 4th Q 358, minimum 0, maximum 804). The demographic characteristics of the Waarom seks? cohort have been reported elsewhere.23
Propensity Score Matching
In the MS group (n=160) there were missing values for age (n=1) and duration of relationship (n=1). In the Waarom seks? group (n=4655) there were missing values for sex (n=4), education level (n=2) and duration of relationship (n=16). As only complete cases can be used for propensity score matching the two persons with MS with missing values and one without match were not included in the analysis. Thus, for 157 persons with MS we obtained 157 matched controls.
YSEX Factors and Sub-Factors
The mean differences between the persons with MS and the controls for the YSEX factors and sub-factors are shown in Table 3. The physical, emotional, and insecurity factors were significantly lower in persons with MS than in the control group, with the physical factor showing the greatest difference. Likewise, the physical and emotional sub-factors were significantly lower in persons with MS than in controls, with the pleasure sub-factor showing the greatest difference. The goal attainment factor and sub-factors, and the insecurity sub-factors did not differ between the two groups, except for the self-esteem boost sub-factor which was lower in the MS group.
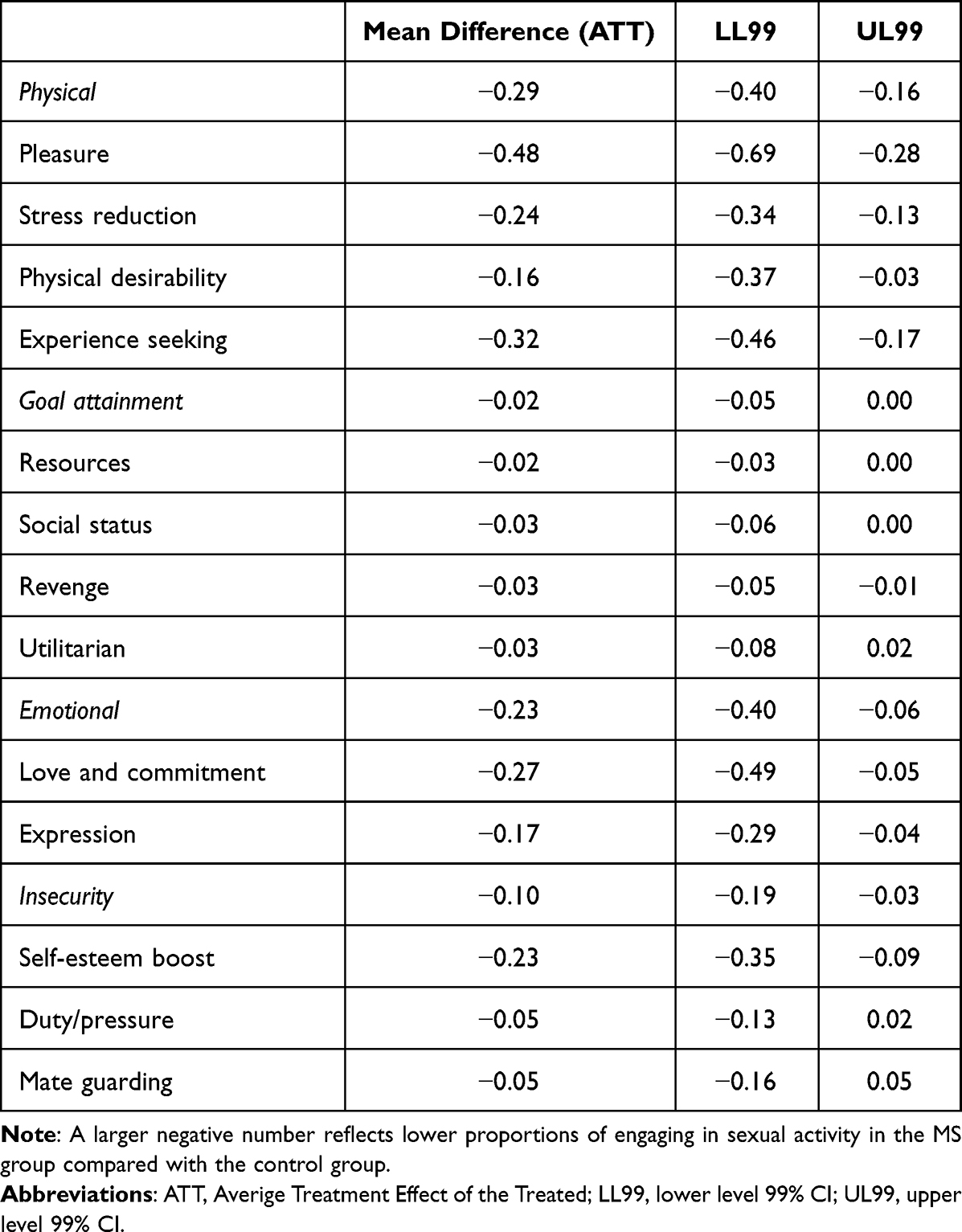 |
Table 3 YSEX Factors and Sub-Factors Mean Differences Between the MS Group and Controls |
Item Level Analysis
For descriptive purposes the top 10 reasons why persons with MS engaged in sex are listed in Table 4, and the top 10 reasons in the control persons are listed in Table 5.
 |
Table 4 The ten Highest-Scoring YSEX Items in the MS Group (n=157) |
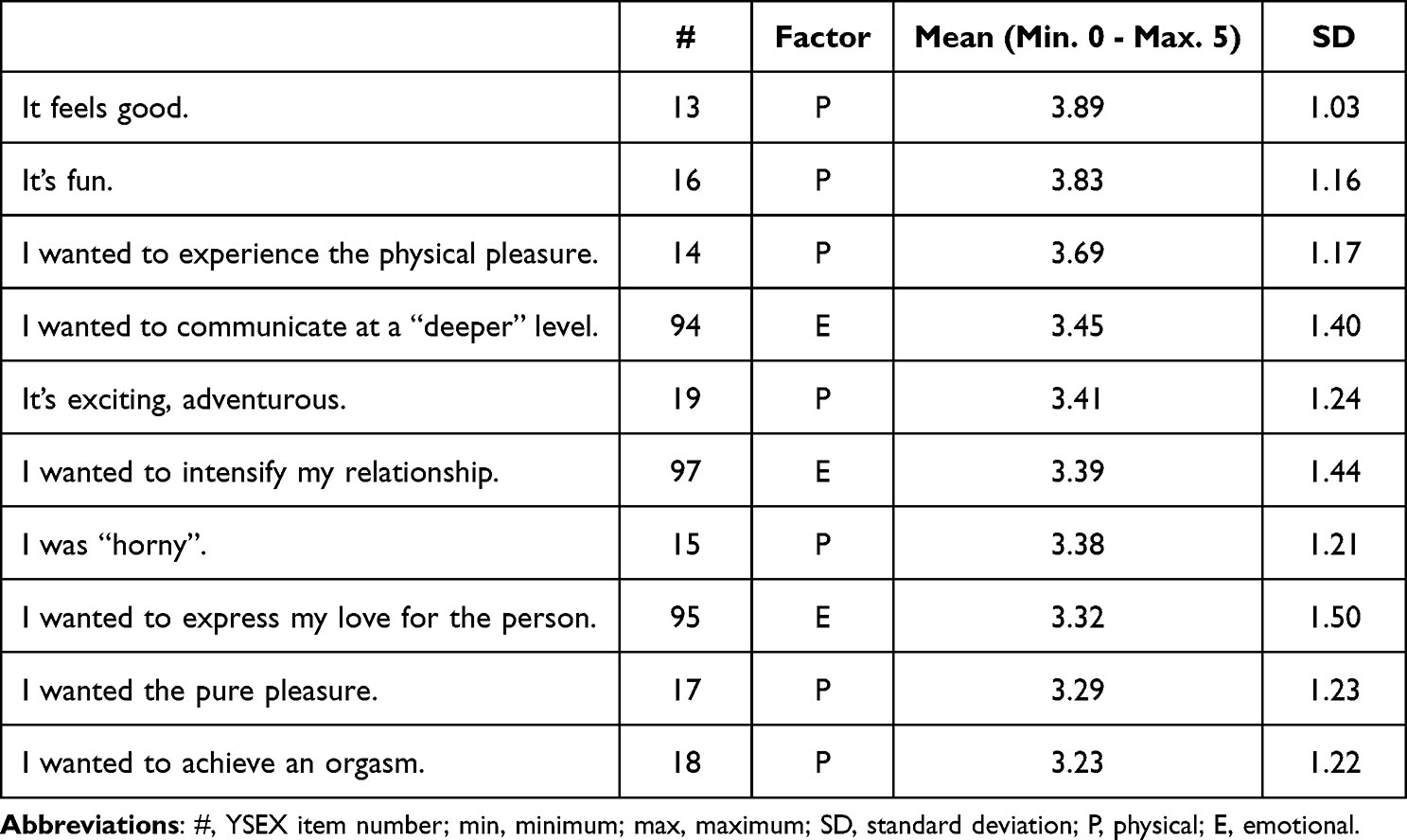 |
Table 5 The ten Highest-Scoring YSEX Items in the Control Group After Propensity Score Matching for Age, Sex, Relationship, Duration of Relationship, and Educational Level (n=157) |
Nine of the top 10 motives in the controls also occurred in the top 10 of the persons with MS. The two top reasons in both the control and MS group were “It feels good” and “It’s fun”. However, whereas in the control group seven of the top 10 items were physical, in the MS group five items were physical. On the other hand, five of the top 10 reasons in the MS group were emotional, as opposed to three in the controls. Interestingly, the persons with MS mentioned “I wanted to show my affection to the person” and “I desired emotional closeness (ie intimacy)” as a top 10 motive, whereas the controls did not; and “I wanted the pure pleasure” and “I wanted to achieve an orgasm” were mentioned by the controls, and not by the persons with MS.
Sexual Satisfaction and Importance of Sex
In persons with MS the sexual satisfaction was not significantly lower than in controls: ATT −0.46 (lower level 99% CI −0.92, upper level 99% CI 0.02). The importance of sex was clearly lower in people with MS: ATT −0.68 (lower level 99% CI −1.14, upper level 99% CI −0.27).
Discussion
This controlled cross-sectional study examined potential differences in sexual motivation between persons with MS and those without MS using the YSEX questionnaire, that is composed of four primary sexual motivation factors and 13 sub-factors.17,19 To our knowledge this is the first report on sexual motivation in persons with MS.
We made some interesting observations. First, at a sub-factor level, the mean of eight of the 13 sub-factors showed significant differences between persons with MS and controls, in that persons with MS reported lower proportions of having sex for each of the eight sub-factor reasons than did the control group.17 One possible explanation for this finding is that, because of symptoms interfering with sexual activity, persons with MS may be less likely exposed to sexual scenarios within a breadth of different contexts.17 However, the YSEX questionnaire does not specifically ask the frequency of how often a person engages in sex but, rather, the proportion of one’s total sexual experiences for which each reason accounts.17,19 Therefore, a smaller number of sexual experiences cannot fully explain these findings.17,19 Instead, the fact that persons with MS, compared to controls, reported that fewer of the reasons for having sex represented many or all of their sexual experiences suggests that when persons with MS engaged in sexual activity, their underlying sexual motivation may be relatively smaller in quantity.17,19 Eg a person without MS might have sex because he or she wants to experience the physical pleasure, achieve an orgasm, and express love and commitment, whereas a person with MS - who knows being unable to have an orgasm or suffers from genital numbness - might have sex only to express love and commitment.
Several findings suggest that especially physical motives are less frequent in persons with MS. Namely, among the primary factors, the physical one showed the greatest difference with controls; and the two sub-factors showing the greatest difference were pleasure and experience seeking, both physical. Moreover, although the top 10 motives in persons with MS were quite similar to those in the controls, the preponderance of physical items was absent in the MS group. The two items that occurred in the top 10 of the controls but not in that of the MS group were physical as well: “I wanted the pure pleasure” and “I wanted to achieve an orgasm”. These findings suggest that the impact of MS is especially noticeable in the physical domain of sexual motivation. Conceivably, this may relate to the wide range of physical symptoms in MS. In our group, six of the nine symptoms that interfered with sexual activity - reported by 26–59% of the participants – can be considered to directly affect the physical aspect of sex, such as sensory disturbances, less feeling in genitals, and insecurity about one’s body (Table 2). Hence, it seems reasonable to suggest that the lower physical sexual motivation partly results from impairment of bodily functions. As to the motive “I wanted to achieve an orgasm”, having difficulty achieving an orgasm is a well-know symptom in MS, occurring in about 35–55% of the persons, and reported by 34% of our MS group.8 It seems plausible that over time this symptom may have a negative effect on orgasm-related motives.
The high number of factors (three) and sub-factors (eight) that scored lower in the MS group indicates that the negative impact of MS on the various motives to have sex is clinically relevant. This would be in line with the strong influence of decreased sexual desire on quality of life that has been reported in women with MS.5 It might therefore be considered to analyse the sexual motivation in persons with MS who suffer from a decreased sexual desire.29 As the application of a range of scales may contribute to a more coherent management of sexual dysfunctions,30 the YSEX questionnaire could be used for this purpose, eg as an integrated part of web-based programs for multidisciplinary management of MS.31
Persons with MS considered sex less important than controls. It is conceivable that lower levels of sexual motivation, in combination with physical impairments interfering with sexual intercourse, may change the internal standards and values regarding sex.32 We suggest that persons with MS reappraise the value of sex and consider it less important because they experience more sexual problems. Thus, appraising sex as less important may be a cognitive means to lower the distress associated with dysfunctional or dissatisfying sexual activities. In general, persons with a chronic disease tend to adapt to their worsening condition, as is eg reflected by a slower decrease in quality of life than physical worsening would suggest (“response shift”).32
Sexual activities, sexual desire and sexual motives may vary according to age, gender, and relational status.15,21,33 Thus, with the use of the YSEX questionnaire it was found that, compared with younger women, those aged 31–45 years had a higher proportion of engaging in sex for the sub-factors stress reduction, physical desirability, experience seeking, resources, social status, revenge, expression, self-esteem boost, and mate guarding.17 In general, as people age sexual motives related to intimacy become more important.14,15 Relational status is also relevant with respect to the reasons for having sex.21 For instance, self-affirmation is less relevant as a sexual motivation for persons who are in a committed relationship,34 whereas discrepancies in desire between partners in a long-term relationship may also affect sexual motivation.35 A study in students aged 19–32 and living in a steady partnership reported a declined sexual desire in women, not in men; and the desire for tenderness had declined in men and risen in women.35
So, to correct for the confounding effects of age, gender, (not) having a relationship, duration of relationship and also educational status, we applied a controlled study design by using the statistical technique of propensity score matching.36 Thus, we constructed a control group by matching each person with MS with a participant of the main study cohort of similar age, gender, education level, (not) having a relationship, duration of relationship, and educational status.36 This enabled us to reliably assess the impact on sexual motivation of MS per se, irrespective of the effect of known confounding covariates.36
Our study has several strengths. First, we performed a detailed analysis of the various reasons to have sex by applying the validated YSEX questionnaire. Second, the study was controlled for the effects of gender, age, relationship, duration of relationship and educational status via propensity score matching, and the controls were obtained from a large cohort. Limitations of the study are that we did not analyse female and male persons separately and that, from a theoretical perspective, it can be argued that persons with MS – and persons with a chronic disease in general – may develop over time sexual motives that are different from those in healthy persons, and that therefore may not have been identified by Meston and Buss in their study in American college students.19
Further research, including qualitative and mixed method approaches, is needed to better understand the changes in sexual motivation in persons MS. Topics may include the associations between specific symptoms and YSEX factor and sub-factor scores, and the assessment of sexual motives conjointly with those of partners.37,38
Conclusion
This controlled cross-sectional study suggests a reduction in the number of sexual motives in persons with MS, especially of physical motives related to pleasure and experience seeking. Health care professionals should focus on changes in sexual motivation when dealing with persons with MS who suffer from a loss of sexual desire.
Ethics Statement
The study was approved by the Ethics Committee of the Ghent University Hospital, Ghent, Belgium. Participants gave their informed consent via www.waaromseks.be.
Acknowledgments
The statistical analyses and in part the preparation of the manuscript were funded by the Dutch National MS Foundation, Rotterdam, Netherlands. The funding source had a role in the collection of the data. We are grateful to the study participants and the persons who contributed to the recruitment process.
Funding
The statistical analyses, the open access publication costs, and in part the preparation of the manuscript were funded by the Dutch National MS Foundation, Rotterdam, Netherlands. The funding source had a role in the collection of the data.
Disclosure
Dr Peter Joseph Jongen reports he was a member of the Scientific Advisory Board of the Dutch National MS Foundation at the time of the study. Miss Petra Prinssen reports a grant from the Dutch National MS Foundation, during the conduct of the study. The authors have no other conflicting interests to declare that are relevant to this article.
References
1. Oh J, Vidal-Jordana A, Montalban X. Multiple sclerosis: clinical aspects. Curr Opin Neurol. 2018;31(6):752–759.
2. Dobson R, Giovannoni G. Multiple sclerosis - A review. Eur J Neurol. 2019;26(1):27–40. doi:10.1111/ene.13819
3. Nabavi SM, Dastoorpoor M, Majdinasab N, et al. Prevalence of sexual dysfunction and related risk factors in men with multiple sclerosis in Iran: a multicenter study. Neurol Therapy. 2021;10(2):711–726. doi:10.1007/s40120-021-00257-0
4. Domingo S, Kinzy T, Thompson N, Gales S, Stone L, Sullivan A. Factors associated with sexual dysfunction in individuals with multiple sclerosis: implications for assessment and treatment. Int J MS Care. 2018;20(4):191–197. doi:10.7224/1537-2073.2017-059
5. Lew-Starowicz M, Rola R. Correlates of sexual function in male and female patients with multiple sclerosis. J Sex Med. 2014;11(9):2172–2180. doi:10.1111/jsm.12622
6. Lew-Starowicz M, Rola R. Sexual dysfunctions and sexual quality of life in men with multiple sclerosis. J Sex Med. 2014;11(5):1294–1301. doi:10.1111/jsm.12474
7. Lew-Starowicz M, Rola R. Prevalence of sexual dysfunctions among women with multiple sclerosis. Sex Disabil. 2013;31(2):141–153. doi:10.1007/s11195-013-9293-9
8. Guo ZN, He SY, Zhang HL, Wu J, Yang Y. Multiple sclerosis and sexual dysfunction. Asian J Androl. 2012;14(4):530–535. doi:10.1038/aja.2011.110
9. Calabro RS, Cacciola A, Bruschetta D, et al. Neuroanatomy and function of human sexual behavior: a neglected or unknown issue? Brain Behav. 2019;9(12):e01389. doi:10.1002/brb3.1389
10. Holloway V, Wylie K. Sex drive and sexual desire. Curr Opin Psychiatry. 2015;28(6):424–429. doi:10.1097/YCO.0000000000000199
11. Regan PC, Atkins L. Sex differences and similarities in frequency and intensity of sexual desire. Soc Behav Person. 2006;34(1):95–102. doi:10.2224/sbp.2006.34.1.95
12. Orasanu B, Frasure H, Wyman A, Mahajan ST. Sexual dysfunction in patients with multiple sclerosis. Mult Scler Relat Disord. 2013;2(2):117–123. doi:10.1016/j.msard.2012.10.005
13. Pfaffenberger N, Gutweniger S, Kopp M, et al. Impaired body image in patients with multiple sclerosis. Acta Neurol Scand. 2011;124(3):165–170. doi:10.1111/j.1600-0404.2010.01460.x
14. Hill CA, Preston LK. Individual differences in the experience of sexual motivation: theory and measurement of dispositional sexual motives. J Sex Res. 1996;33:18. doi:10.1080/00224499609551812
15. Hill CA. The distinctiveness of sexual motives in relation to sexual desire and desirable partner attributes. J Sex Res. 1997;34(2):15. doi:10.1080/00224499709551878
16. Barrada JR, Castro A, Fernandez-Del-Rio E, Ramos-Villagrasa PJ. Motives to have sex: measurement and correlates with sociodemographic, sexual life, and psychosexual characteristics. Front Psychol. 2021;12:645493. doi:10.3389/fpsyg.2021.645493
17. Meston CM, Hamilton LD, Harte CB. Sexual motivation in women as a function of age. J Sex Med. 2009;6(12):3305–3319. doi:10.1111/j.1743-6109.2009.01489.x
18. Both S, Brauer M, Laan E. Classical conditioning of sexual response in women: a replication study. J Sex Med. 2011;8(11):3116–3131. doi:10.1111/j.1743-6109.2011.02453.x
19. Meston CM, Buss DM. Why humans have sex. Arch Sex Behav. 2007;36(4):477–507. doi:10.1007/s10508-007-9175-2
20. Hensel DJ, He F, Harezlak J, Fortenberry JD. Daily diary study of adult men’s and women’s event-level sexual motivations and sexual behaviour. Sex Health. 2017;14(2):147–154. doi:10.1071/SH16109
21. Cooper ML, Shapiro CM, Powers AM. Motivations for sex and risky sexual behavior among adolescents and young adults: a functional perspective. J Pers Soc Psychol. 1998;75(6):1528–1558. doi:10.1037/0022-3514.75.6.1528
22. Cooper ML, Barber LL, Zhaoyang R, Talley AE. Motivational pursuits in the context of human sexual relationships. J Pers. 2011;79(6):1333–1368. doi:10.1111/j.1467-6494.2010.00713.x
23. Wyverkens E, Dewitte M, Deschepper E, et al. YSEX? A replication study in different age groups. J Sex Med. 2018;15(4):492–501. doi:10.1016/j.jsxm.2018.02.012
24. Vickrey BG, Hays RD, Harooni R, Myers LW, Ellison GW. A health-related quality of life measure for multiple sclerosis. Qual Life Res. 1995;4(3):187–206. doi:10.1007/BF02260859
25. Brauer M, Lakeman M, van Lunsen R, Laan E. Predictors of task-persistent and fear-avoiding behaviors in women with sexual pain disorders. J Sex Med. 2014;11(12):3051–3063. doi:10.1111/jsm.12697
26. R Core Team V, Austria. R: a language and environment for statistical computing; 2018. Available from: https://www.R-project.org/.
27. Ho DE, King G, Stuart EA, Stuart EA. MatchIt: nonparametric preprocessing for parametric causal inference. J Stat Softw. 2011;42(8):28. doi:10.18637/jss.v042.i08
28. Imai K, Lau O. Toward A common framework for statistical analysis and development. J Compu Graph Stat. 2008;2008:21.
29. Meyers M, Margraf J, Velten J. A qualitative study of women’s experiences with cognitive-behavioral and mindfulness-based online interventions for low sexual desire. J Sex Res. 2022;2022:1–10.
30. Hatzichristou D, Kirana PS, Banner L, et al. Diagnosing sexual dysfunction in men and women: sexual history taking and the role of symptom scales and questionnaires. J Sex Med. 2016;13(8):1166–1182. doi:10.1016/j.jsxm.2016.05.017
31. Jongen PJ, Sinnige LG, van Geel BM, et al. The interactive web-based program MSmonitor for self-management and multidisciplinary care in multiple sclerosis: utilization and valuation by patients. Patient Prefer Adherence. 2016;10:243–250. doi:10.2147/PPA.S93786
32. Schwartz CE, Andresen EM, Nosek MA, Krahn GL; Measurement REPoHS. Response shift theory: important implications for measuring quality of life in people with disability. Arch Phys Med Rehabil. 2007;88(4):529–536. doi:10.1016/j.apmr.2006.12.032
33. Carvalheira A, Traeen B, Stulhofer A. Correlates of men’s sexual interest: a cross-cultural study. J Sex Med. 2014;11(1):154–164. doi:10.1111/jsm.12345
34. Gravel EEP, Pelletier LG, Reissing ED. ”Doing it” for the right reasons: validation of a measurement of intrinsic motivation, extrinsic motivation, and motivation for sexual relationships. Personal Individ Differ. 2016;92:9. doi:10.1016/j.paid.2015.12.015
35. Herbenick D, Mullinax M, Mark K. Sexual desire discrepancy as a feature, not a bug, of long-term relationships: women’s self-reported strategies for modulating sexual desire. J Sex Med. 2014;11(9):2196–2206. doi:10.1111/jsm.12625
36. Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res. 2011;46(3):399–424. doi:10.1080/00273171.2011.568786
37. Miller DD, Shaw L. Sex bias in the care of patients with cardiovascular disease? N Engl J Med. 1994;331(13):883. doi:10.1056/NEJM199409293311320
38. Blackmore DE, Hart SL, Albiani JJ, Mohr DC. Improvements in partner support predict sexual satisfaction among individuals with multiple sclerosis. Rehabil Psychol. 2011;56(2):117–122. doi:10.1037/a0023362
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.