")
Back to Journals » International Journal of General Medicine » Volume 16
Sexual Behaviors and Intimate Relationships of Sexual Partners of Young Patients with Early-Stage Cervical Cancer: A Qualitative Study
Authors Li M, Wang D , Huang J, Luan S, Wang Q
Received 5 September 2023
Accepted for publication 9 November 2023
Published 20 November 2023 Volume 2023:16 Pages 5377—5387
DOI https://doi.org/10.2147/IJGM.S437150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mingyue Li,1 Dongyang Wang,2 Jiaxiang Huang,3 Shunlian Luan,3 Qinghua Wang1
1School of Nursing, Binzhou Medical University, Binzhou, 256603, People’s Republic of China; 2Department of Nursing, the Third People’s Hospital of Henan Province, Zhengzhou, 450000, People’s Republic of China; 3Oncology Department, Binzhou Medical University Hospital, Binzhou, 256603, People’s Republic of China
Correspondence: Dongyang Wang, 450000, Tel +86-1566-057-7010, Email [email protected] Qinghua Wang, 256603, Tel +86-1875-359-6769, Email [email protected]
Purpose: This study aimed to explore the sexual behaviors and intimate relationships of sexual partners of young patients with cervical cancer.
Patients and Methods: This study employed a descriptive phenomenological research design, which falls within the realm of qualitative research methods. Qualitative research typically utilizes interview techniques for gathering participants’ experiences, perceptions, and behaviors. This study conduct face-to-face semi-structured interviews with the sexual partners of 15 young cervical cancer patients receiving cancer treatment to collect their experiences and perspectives on intimate relationships and sexual behavior with cervical cancer patients, and use the Colaizzi method for data analysis.
Results: Four themes were identified through the interview analysis: (1) reduction or absence of sexual behavior, (2) unpleasant sexual experiences, (3) adjustment of intimate relationships, and (4) lack of sexual health education.
Conclusion: The sexual partners of young cervical cancer patients have experienced significant shifts in their perspectives on sexual behavior and intimate relationships. These changes include reduction or absence of sexual behavior, unpleasant sexual experiences, adjustment of intimate relationships, and lack of sexual health education. Hospitals should pay more attention to the sexual behavior and intimate relationships of patients with cervical cancer and their sexual partners, and social support systems and psychological and emotional counselling services should be established for providing relevant knowledge and guidance.
Keywords: young age, cervical cancer, sexual partners, sexual behavior, intimacy, qualitative study
Introduction
Cervical cancer is a disease of the female reproductive system caused by human papillomavirus (HPV) infection and is one of the leading causes of mortality in women.1 It ranks first among the three major gynecological malignancies and fourth among the most common cancers in women worldwide.2–4 Studies have shown that approximately 604,000 women worldwide are diagnosed with cervical cancer annually, and low- and middle-income countries account for 88% of new cervical cancer cases and 91% of deaths worldwide.5,6 In addition, the incidence of young women is rising in related studies.7 In 2020, Cancer Research UK (2020) reported a 54% increase in cervical cancer incidence in women aged 25–29.8 China is currently one of the countries with the largest cervical cancer burden, with approximately 65,000 new cases of cervical cancer and 25,000 cervical cancer-related deaths annually.9,10
Treatments for cervical cancer include surgery or concurrent chemoradiation. The National Cancer Center provides recommendations for the treatment of cervical cancer based on the stage of the disease. For patients with IA1 cervical cancer, the recommended treatment options include cold knife conization or total hysterectomy, with or without bilateral salpingo-oophorectomy. Patients with IA2 cervical cancer are advised to undergo modified radical hysterectomy and lymphadenectomy. For patients with IB and IIA cervical cancer, the recommended treatment is radical hysterectomy or radical hysterectomy and pelvic lymphadenectomy, in addition to radiotherapy and chemotherapy, based on their reproductive needs. Patients with stage IIB, III, and IVA cervical cancer are recommended to undergo surgical resection of pelvic lymph nodes, followed by radiotherapy and chemotherapy. In the case of stage IVB cervical cancer, which is considered advanced, palliative therapy is recommended to manage symptoms and improve the quality of life.11 However, these treatments can also have side effects on patients, such as low levels of vaginal lubrication and vaginal stenosis (associated with brachytherapy), hair loss, urinary incontinence, skin lesions, lymphedema, insomnia, and hormonal and reproductive dysfunction.12 In addition, about 50% of gynecological cancer survivors have sexual dysfunction, which is one of the most troublesome painful symptoms among cervical cancer survivors.13 In a retrospective case-control study conducted between 2019 and 2022 by Membrilla-Beltran et al, it was discovered that a significant proportion of cervical cancer survivors faced challenges related to sexual dysfunction and impaired sexual satisfaction.14 Comparatively, these issues were found to be more prevalent among cervical cancer survivors when compared to healthy women without any underlying health conditions. The study further indicated that cervical cancer survivors experienced sexual dysfunction, dissatisfaction, and a lower overall quality of life.
Considering that the survival rate of patients with cervical cancer has improved, sexual behavior and intimate relationships have become important issues for survivors.15 Intimacy refers to a person’s most intrinsic qualities and usually refers to the experience of a “strong sense of intimacy, connection, and bonding”.16 As the primary caregiver and the most important resource for supporting women diagnosed with gynecological cancer, spouses can help women meet their medical and non-medical needs and manage their conditions.17 Teskereci et al found that a substantial majority of caregivers for individuals with gynecological cancers were identified as their partners.18 It is suggested that sexual health and having a close relationship with a partner have been described as valuable “safe havens” that provide emotional support during the cancer experience. However, this psychological buffer can be disrupted as the disease progresses.19 Cancer affects not only patients’ physical health, but also their sexual behavior and intimate relationships with partners.20 There is still lack of consensus regarding the relationship between cancer and intimate behavior. Different studies have reported varying impacts of different types and stages of cancer on the level of intimate relationships.21,22
Most studies on sexual behavior and intimate relationships in patients with cervical cancer have adopted quantitative research methods, mainly focusing on the analysis of the status quo of sexual function and its influencing factors at different clinical stages,23,24 focusing on patients with cervical cancer and the disease itself. However, these studies did not analyze the real causes and experiences of changes in sexual behavior and intimate relationships between patients with cancer and their sexual partners. Therefore, qualitative research methods were used in this study to explore the views of sexual partners of young patients with cervical cancer on sexual behavior and intimate relationships.
Material and Methods
Study Design
This study employed a descriptive phenomenological research design, which falls within the realm of qualitative research methods. Qualitative research typically utilizes interview techniques for gathering participants’ experiences, perceptions, and behaviors.25 This study conduct face-to-face semi-structured interviews with the sexual partners of 15 young cervical cancer patients receiving cancer treatment to collect their experiences and perspectives on intimate relationships and sexual behavior with cervical cancer patients, and use the Colaizzi method for data analysis. The Colaizzi analysis method, also known as the Colaizzi seven step analysis method, is a commonly used analytical method for qualitative interview data. The detailed steps of the analysis are listed in Table 1.
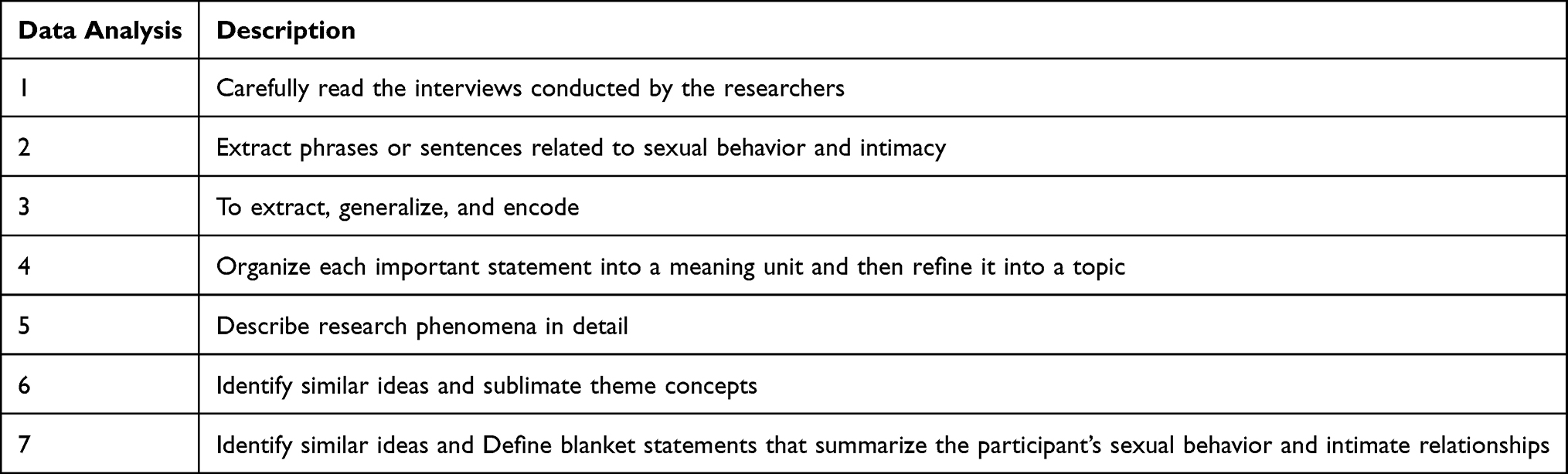 |
Table 1 Data Analysis Steps |
Patient and Public Involvement
Purposive sampling and maximum variation sampling were used to select 15 sexual partners of young patients with cervical cancer from 5 tertiary hospitals. A qualitative methodological approach is appropriate when researchers aim to understand and extract the meaning of phenomena by exploring participants’ perspectives and experiences.26 In the field of qualitative research, phenomenology seeks to understand how individuals construct their worldviews; The data obtained through qualitative research comes from data collection tools such as interviews, focus groups, and participant observations, as well as in the form of narrative transcriptions, images (paintings, photography), and documents (diaries, letters).27
Participants and Sampling
The inclusion criteria for the cervical cancer patients were: patients with a pathological diagnosis of cervical cancer; a diagnosis of stage 1, 2, 3 or 4 cervical cancer; age of 15–39 years old (the maximum age was determined based on previous literature regarding young people);28 having undergone hysterectomy and chemotherapy for ≥3 months; being sexually active (defined as having sexual activity until at least 6 months prior to surgery;29 and providing consent for participation in the study. The exclusion criteria were as follows: receiving intensive palliative care, severe mental or cognitive impairment, and other cancers.
The inclusion criteria for the patient’s partner were as follows: normal sexual function, age of < 60 years, and providing informed consent to participate in the study. The exclusion criteria were as follows: severe mental or cognitive impairment and no strenuous exercise.
Partners who met the inclusion criteria were informed of the purpose and design of the study by caregivers during the initial face-to-face contact during routine visits. The partners were then allowed to decide whether they wished to participate within a week. In the second face-to-face meeting, the partners were asked to provide written informed consent and permission for a recorded interview. All the selected partners agreed to participate in the study. There were no dropouts.
Setting
All the interviews were conducted in a ward instruction classroom.
Data Collection
This study uses individual in-depth interview technology as a data collection method. This is a data collection technique that provides detailed information about the true causes and structural determinants of personal feelings, thoughts, beliefs, experiences, and observations. All researchers are all registered nurses who have participated in qualitative research related training and are certified to read the medical history of all patients in detail, in order to understand the situation of each participant before the interview. After the pre-interviews with two participants, the interview outline was adjusted. Complete verbatim records of each interview, field notes, and letters were produced, and the text was collated for qualitative analysis. We asked the following questions:
Please recall your sexual behavior and intimate relationships.
What do you think of your sexual behavior and intimacy with your partner?
What do you think has changed in your sexual behavior and intimacy after the partner got sick?
How have these changes affected you?
All interviews were completed by (LM) Mingyue Li and (HJ) Jiaxiang Huang. The interview lasted about 45–80 min for each participant until no new information was extracted. Determining sample size based on data saturation points is a commonly used method in qualitative research. When the themes and subtopics obtained from participants start to repeat, it is decided to reach data saturation. A total of 25 semi-structured interviews were conducted. The researchers’ field notes provided a rich source of information as participants described their personal experiences and behaviors during the data collection process and enabled them to note their reflections on aspects of the data collection methodology. No other participants were present during data collection.
Data Analysis
The interview data was imported into NVivo. Colaizzi’s method of analysis was used to analyze the data. Two researchers independently analyzed the interview data and identified the initial codes, categories, and subcategories to form four themes. We shared the final analysis results with the participants and sought their feedback. Additionally, we considered the availability of audio recordings during the interview process. This allowed us to verify the accuracy of the transcribed interview content by cross-referencing it with the recorded material.
Rigor
This study was conducted following according to the guidelines developed by the Consolidates Criteria for Reporting Qualitative Research and the Standards for Reporting Qualitative Research.30,31 The execution techniques and applications for controlling confidence are presented in Table 2.
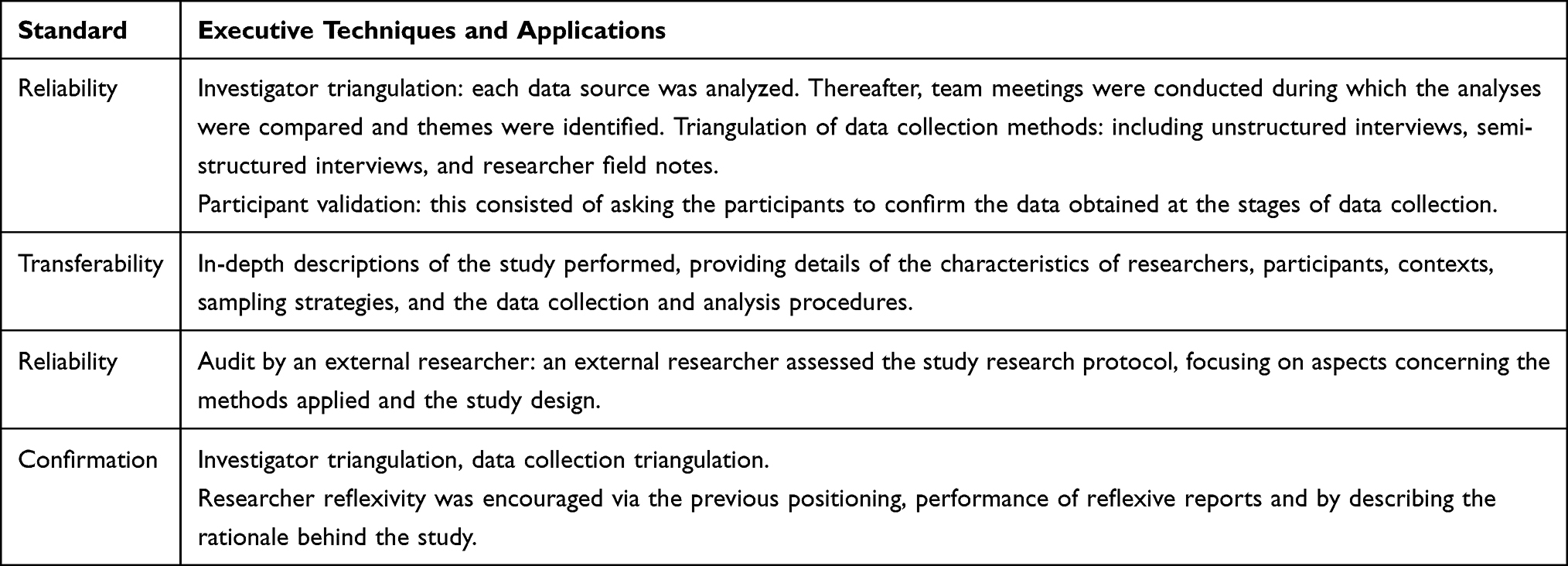 |
Table 2 Executive Techniques and Applications |
Results
Participant Characteristics
Fifteen sexual partners of young patients with cervical cancer were recruited. The mean age of the participants was 34.67 years (standard deviation, SD:2.74). The data are shown in Table 2.
Patients’ demographics, and diseases were extracted from electronic medical record reviews by the investigators. The mean age of the patients was 35.00 years (standard deviation, SD:2.65). The data are shown in Table 3.
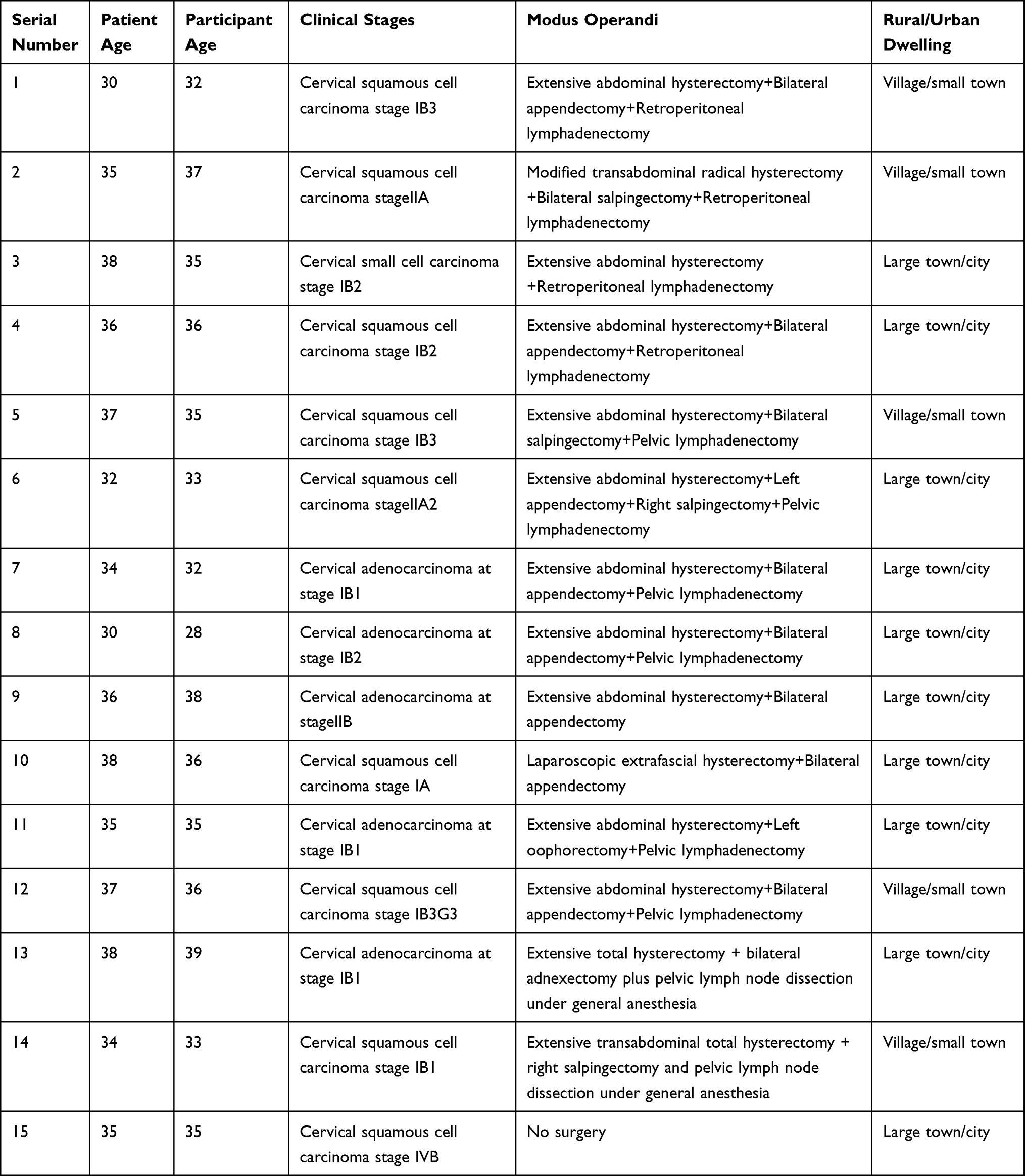 |
Table 3 Participant Characteristics and the Clinical and Demographic Characteristics of the Patients |
Qualitative Results—Thematic Findings
Four specific themes emerged from the analysis: reduced or absent sexual activity, unpleasant sexual experiences, adjustment of intimate relationships, and lack of sexual health education.
Reduced or Absent Sexual Behavior
In this study, the majority of participants perceived no significant change in their sexual behavior, although they acknowledged a decrease. The long treatment cycle and cancer-related side effects imposed emotional and physical strain on both patients and participants. The participants reported the following:
Following my wife’s surgery, we did engage in sexual intimacy, albeit less frequently than before. Our encounters became occasional, happening only once or twice, and I sensed that both of us were guarded and less open. We were both preoccupied with concerns about her health worsening, which made me hesitant to express my desires due to the fear of adding further distress to her already challenging situation. The medication and radiation treatment had taken a toll on her emotional well-being, leaving her feeling deeply saddened and distressed. (Participant 2)
Well, I don’t feel like that I can think about that anymore. My wife was ill and had surgery which really affected her health. At first she had to have chemo and then she had to go back to therapy every month or so and it was really hard on her. She was exhausted. (Participant 6)
We haven’t had sex, and I would love to have sex with my wife. But she has HPV, which is sexually transmitted. She hasn’t said she wants to have sex with me since she got sick, so we haven’t had sex since she got sick. I hope to have sex when my wife’s health improves. (Participant 7)
We haven’t done much since my wife got sick. I don’t think I have this kind of idea, especially since my health is not good. In addition, I feel that my wife’s needs in this area have decreased. My wife is very tired during treatment, and when I administer a dozen chemotherapy drugs, my wife becomes very weak. She doesn’t miss me very much and she doesn’t miss it very much. (Participant 10)
I haven’t had sex with my wife since she got sick. I’m afraid that this kind of sex will do some harm to my wife’s health, so I don’t dare to have sex with my wife. She actually gave birth to three children for me, and now she has cancer. We can only give it a hug. (Participant 11)
We haven’t had sex for a long time and I’m worried that my wife’s cancer cells will transfer to me through sex. (Participant 13)
Unpleasant Sexual Experiences
Body scarring and urinary incontinence, among other factors, can have an impact on the patient’s and partner’s sexual behavior and intimacy, often leading to unpleasant sexual experiences. Some examples of participants’ opinions in this respect are provided below:
When my wife undresses, I notice a prominent scar on her body, which makes me reluctant to engage in sexual activity. The scar is quite significant, located right in the middle of her lower abdomen. (Participant 1)
My wife had a piece of her vagina cut after the surgery. I was afraid that she would suffer a second injury when I had sex with her. In addition, the decrease of vaginal fluid made me feel uncomfortable and unable to let go. (Participant 5)
As soon as I put it in, my wife said it hurts. When I tried again, my wife pushed me away. I felt that there was no mouth in her place and no fluid secretion. After trying several times, I didn’t want to do it, and I was busy with work and taking care of her and the children. (Participant 8)
After several cycles of treatment, my wife lost all her hair. I can’t accept this change in my wife, especially at night. I feel like an old lady is sleeping next to me.(Participant 12)
In addition, some participants claim that due to the effects of targeted drugs, the patient’s body undergoes significant changes, including development of rashes, ulcers, and a foul odor which greatly discourages them from attempting sexual activity.
I don’t know why, but there’s this weird stench coming from underneath my wife, like rotting meat, and when I smell it, I can’t go on. Some time ago, my wife received targeted therapy, and the side effects are very serious, hands and feet are broken, I don’t think we can continue to have sex. (Participant 15)
Adjustment of Intimate Relationships
An intimate relationship is not only an important indicator for evaluating patients’ subjective well-being and quality of life, but also an important predictor of disease prognosis. A good intimate relationship is an important factor influencing disease recovery. Most of the participants said they were more intimate and got better along, while some said they had “qualitatively changed”.
Since my wife’s illness, I feel closer to her, and she is more dependent on me. We have been together every day, we do not fight, and we have not been apart since we got married. I was sick four years ago. My wife always took care of me. I am very grateful to my wife. My wife have no one else to rely on, so she depends on me. (Participant 2)
There is an emotional basis to having sex with your wife, and I feel that our relationship has changed; that it is more of a husband’s responsibility for his wife, and that we communicate less. I even thought about getting divorced because cervical cancer is usually associated with unclean sexual behavior, and I have not had sexual intercourse with other women. (Participant 1)
Since my wife fell ill, I have noticed a shift in our relationship that has transformed us into more of a brother and sister dynamic. While we share the same family and maintain a strong bond, the romantic and intimate connection that typically exists between husband and wife seems to have diminished. (Participant 3)
I feel very distant from my wife. When she needs to undergo several rounds of chemotherapy, I feel very tired. Long hospital stays and illness are very stressful for both of us. The economic pressure and psychological stress brought by cancer treatment bored me (Participant 12)
Lack of Sexual Health Education
Participants expressed a prevailing sentiment that they were inadequately informed about sexual health matters both during and after treatment. The aftermath of treatment left them with scarce opportunities to openly discuss with medical professionals regarding sexual issues or potential sexual rehabilitation options. Below, several statements encapsulate their sentiments:
During my wife’s post-surgery period, I found myself uncertain about her condition and whether it was safe for us to engage in sexual activity. The medical professionals attending to her didn’t provide clear guidance on this matter. It was only through researching on my phone that I discovered the potential transmission of viruses through sexual contact. As a result, I have refrained from engaging in sexual intercourse with my wife for an extended period of time, as I wanted to prioritize her health and well-being. (Participant 4)
I did not go to a doctor. I did not need to go to a doctor. After she healed, we had sex. My wife made a request to me, but I hesitated, but still agreed to her request. I do not know if this is the right thing to do. (Participant 8)
I am not sure if my wife’s HPV infection will be transmitted to me. The doctor has not mentioned it to me, and I have not asked the doctor. I am afraid that the doctor or nurse may misunderstand me and say that I despise my wife. (Participant 14)
In addition, some participants expressed their desire for a offspring, but lacked corresponding reproductive guidance, which hindered them.
Is birth control or other protective measures necessary during the treatment period? Do you still need contraception after being cured? How long can I have a child after being cured? (Participant 2)
I don’t know what measures I can take to save my wife, because I still want one of our children. Should I avoid any type of sexual activity? (Participant 5)
Discussion
Our findings reflect the changes in sexual behavior and intimate relationships within the context of young patients with cervical cancer and their partners. Different partners have positive or negative experiences and perspectives regarding sexual behavior and intimate relationships among cervical cancer patients.
The majority of participants showed a decrease in or loss of sexual activity and unpleasant sexual experiences. Firstly, this trend can be attributed, in part, to the physical conditions of the patients themselves. Engaging in sexual behavior requires the joint cooperation of both men and women. According to the World Health Organization (WHO), sexuality, together with sex, sexual identity, orientation, eroticism, pleasure, intimacy and reproduction, is one of the central aspects of human lives. Sex includes six aspects: thoughts, fantasies, attitudes, roles, behaviors, and desires, depending on biological, psychological, social, cultural, historical, and legal factors.32 However, in this study, most patients have undergone Hysterectomy (the removal of the uterus and its accessories), radiotherapy, chemotherapy, etc. to ensure the maintenance of life. The patients were exhausted during the treatment phase. In fact, these treatments usually lead to intestinal dysfunction and bladder dysfunction such as Urinary incontinence and Bowel obstruction, which indirectly affect the occurrence of sexual behavior,33,34 which is consistent with the findings of a previous study.35 Despite these challenges, most participants’ primary concern was survival, outweighing sexual health concerns. In addition, the smell and feeling during sexual intercourse will affect the sexual behavior of the Sexual partner. Research shows that Hysterectomy is usually associated with oophorectomy. Ovaries are very important for premenopausal and postmenopausal women to produce steroid hormones, which can regulate the central response to sexual stimulation and the sensitivity of genital tissue to tactile stimulation, thus ensuring the comfort of both men and women.36
It is worth noting that some partners indicated that changes in the patient’s body form can also lead to unpleasant sexual experiences. Body image is an important multi-dimensional and complex concept. Body image involves the positive and negative perception, thought, feeling and behavior of the whole body and its functions.37 In fact, most sexual partners in this study admitted that biological changes in patients had dampened their sexual behavior and overall interest in maintaining sexual relationships.
Furthermore, the participants’ personality traits emerged as an influencing factor in sexual behavior. During the treatment process of patients, sympathy and caregiving often took precedence over initiating or participating in sexual intimacy. This dynamic shifted as the patients’ health improved. When the patient’s health condition improves, they are more willing to engage in sexual behavior. Cultural norms, especially in China, place a strong emphasis on the role of men as caregivers within the family unit. Thus, when a wife falls ill, the husband’s focus shifts from personal needs to the welfare of the family, reflecting the traditional husband-wife dynamic. Some partners also voiced concerns about contracting HPV infection, a primary cause of cervical cancer as males act as both virus carriers and vectors and this is an important component of the epidemiological chain for HPV.38 This further hindered sexual intimacy due to the fear of transmission.
Adjustment of intimate relationships is one of the critical findings of this study. Intimacy is an important factor in the recovery phase, with social interactions and close relationships bolstering well-being and serving as vital coping mechanisms.39 Studies have shown that men influence women’s reproductive health through their roles as sexual partners, fathers, and healthcare providers.40 In addition, psychological status such as attachment, basic utility, and self are generated by intimate behaviors such as sexual activities.41 In this study, while most participants reported strengthened intimate bonds, a subset expressed negative shifts due to factors like postoperative scarring, high medical costs, and prolonged illness. Some relationships even transformed from spousal to sibling-like due to the enduring nature of cancer treatment and caregiving. Cancer is a chronic disease that requires long-term hospital treatment, and the long-term companionship and care of the partner as the first caregiver gradually deepens kinship. It is worth noting that some partners reported diminished communication or contemplated divorce due to misconceptions associating cervical cancer with “unclean” sexual behavior. This may be related to their erroneous belief that the onset of cervical cancer is related to unclean sexual behavior. Research shows that cervical cancer is caused by cervical infection of high-risk human papillomavirus (hrHPV) genotype. In addition to being associated with multiple sexual partners and HIV co infection, oral contraceptives, smoking, etc. are recognized as epidemiological risk factors of cervical hrHPV infection.42 In addition, the results of this study indicate that the economic toxicity of cancer treatment to families can also disrupt the intimate relationship between young partners and patients. The National Cancer Institute of the United States broadly defines financial toxicity as “problems related to cancer patients and treatment costs”. Economic toxicity occurs more frequently among young people than among elderly survivors, and younger age and lower income are identified as risk factors for financial distress.43
Another issue expressed by sexual partners was the lack of sexual health education. Sexual health remains important to many partners, despite advanced stages of cervical cancer. Fertility is a major issue for young cancer survivors and their caregivers, especially after completing their cancer treatment plans.44 Due to partners being of childbearing age, there may be sexual and reproductive health related issues and unmet needs between them and patients. In addition, research has shown that the major source of HPV awareness among the young population may be social media and some web blogs.45 Most husbands lack basic knowledge and even have negative views about female hysterectomies, making them unable to provide effective emotional support to their wives.46
We acknowledge limitations to the study.This study included few participants to obtain more comprehensive information. More prospective and temporal cohort studies are needed to obtain data on sexual behavior and intimacy in young patients with cervical cancer and their sexual partners.
Conclusion
The disease itself and the side effects of treatment of cervical cancer had an impact on young cervical cancer patients and their partners’ sexual behavior and intimate relationships. Given that cervical cancer is a chronic ailment, it becomes imperative not only for patients but also for their partners to be prepared, both mentally and physically. In addition, hospitals should pay more attention to the sexual behavior and intimate relationships of patients with cervical cancer and their sexual partners, and social support systems and psychological and emotional counselling services should be established for providing relevant knowledge and guidance.
Ethics Approval and Consent to Participate
This study was approved by the Clinical Research Ethics Committee of Binzhou Medical University (code: 2023-002). Informed consent and permission to record the interviews were obtained for each participant, and the study was conducted in accordance with the principles of the Declaration of Helsinki. In addition, no participant files or personal information were shared with anyone other than the research team.
Funding
This study was supported by the 2020 Medical Care and Health Industry Research Special Project of the Binzhou Medical University Social Science Development Fund (20SKYZ01) and the Graduate Scientific Research Innovation Plan of the Nursing University of Binzhou Medical University (2022-008).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tramacere F, Lancellotta V, Casà C, et al. Assessment of Sexual Dysfunction in Cervical Cancer Patients after Different Treatment Modality: a Systematic Review. Medicina. 2022;58(9):1223. doi:10.3390/medicina58091223
2. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. Cancer j Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Gavinski K, DiNardo D. Cervical Cancer Screening. Med Clin North Am. 2023;107(2):259–269. doi:10.1016/j.mcna.2022.10.006
4. Johnson CA, James D, Marzan A, et al. Cervical Cancer: an Overview of Pathophysiology and Management. Semin Oncol Nurs. 2019;35(2):166–174. doi:10.1016/j.soncn.2019.02.003
5. Drolet M, Laprise JF, Martin D, et al. Optimal human papillomavirus vaccination strategies to prevent cervical cancer in low-income and middle-income countries in the context of limited resources: a mathematical modelling analysis. Lancet Infect Dis. 2021;21(11):1598–1610. doi:10.1016/S1473-3099(20)30860-4
6. Wang H, Wang X, Chen P, et al. Factors influencing Chinese female college students’ willingness to receive human papillomavirus vaccine: a cross-sectional study based on information-motivation-behavioral skills model. Hum Vaccin Immunother. 2022;18(7):2140550. doi:10.1080/21645515.2022.2140550
7. Huang J, Deng Y, Boakye D, et al. Global distribution, risk factors, and recent trends for cervical cancer: a worldwide country-level analysis. Gynecol Oncol. 2022;164(1):85–92. doi:10.1016/j.ygyno.2021.11.005
8. Groves S, Brooks J. What do young women below national screening age in England think about cervical cancer and cervical screening? A qualitative study. J Clin Nurs. 2022;31(11–12):1588–1597. doi:10.1111/jocn.16012
9. Zhang BZ, Li Y, Xu L, et al. The relationship between the radiation dose of pelvic-bone marrow and lymphocytic toxicity in concurrent chemoradiotherapy for cervical cancer. Radiation Oncol. 2023;18(1):12. doi:10.1186/s13014-023-02205-8
10. Guo J, Guo S, Dong S. Efficacy, immunogenicity and safety of HPV vaccination in Chinese population: a meta-analysis. Front Public Health. 2023;11:1128717. doi:10.3389/fpubh.2023.1128717
11. Tsikouras P, Zervoudis S, Manav B, et al. Cervical cancer: screening, diagnosis and staging. J BUON Oncol. 2016;21(2):320–325.
12. Moysés R, Marques I, Santos BD, et al. Quality of Life in Amazonian Women during Cervical Cancer Treatment: the Moderating Role of Spirituality. Int J Environ Res Public Health. 2023;20(3):2487. doi:10.3390/ijerph20032487
13. Obora M, Onsongo L, Ogutu JO. Determinants of sexual function among survivors of gynaecological cancers in a tertiary hospital: a cross-sectional study. Ecancermedicalscience. 2022;16:1384. doi:10.3332/ecancer.2022.1384
14. Membrilla-Beltran L, Cardona D, Camara-Roca L, et al. Impact of Cervical Cancer on Quality of Life and Sexuality in Female Survivors. Int J Environ Res Public Health. 2023;20(4):3751. doi:10.3390/ijerph20043751
15. Lee Y, Lim MC, Kim SI, et al. Comparison of quality of life and sexuality between cervical cancer survivors and healthy women. Cancer Res Treatment. 2016;48(4):1321–1329. doi:10.4143/crt.2015.425
16. Wang T, Cheng HL, Wong PKK, et al. Men’s experiences of sex and intimacy after prostate cancer treatment in China: a qualitative study. Supportive Care in Cancer. 2022;30(4):3085–3092. doi:10.1007/s00520-021-06720-w
17. Zhou L, Hong J, Henricson M, et al. Factors associated with posttraumatic growth among spouses of women diagnosed with gynaecological cancer: a cross-sectional study. Nursing Open. 2023;10(2):630–640. doi:10.1002/nop2.1329
18. Teskereci G, Kulakaç O. Life experiences of caregivers of women with gynaecological cancer: a mixed-methods systematic review. Eur J Cancer Care (Engl). 2018;27(1):
19. Jonsdottir JI, Jonsdottir H, Klinke ME. A systematic review of characteristics of couple-based intervention studies addressing sexuality following cancer. J Adv Nurs. 2018;74(4):760–773. doi:10.1111/jan.13470
20. Li M, Chan CWH, Choi KC, et al. The Chinese version of the Revised Dyadic Adjustment Scale for gynaecological cancer patients and their partners: translation and psychometric evaluation. Asia-Pacific j Oncol Nursing. 2021;9(1):48–54. doi:10.1016/j.apjon.2021.12.004
21. Thompson T, Heiden-Rootes K, Joseph M, et al. The support that partners or caregivers provide sexual minority women who have cancer: a systematic review. Soc Sci Med. 2020;261:113214. doi:10.1016/j.socscimed.2020.113214
22. Chen X, Li Y, Sun H, et al. Dyadic communication quality and family resilience in gynecologic cancer survivors: a study on the mediating role of perceived spousal support. Support Care Cancer. 2022;31(1):68. doi:10.1007/s00520-022-07492-7
23. Gough K, Bergin RJ, Drosdowsky A, et al. Women with gynaecological cancer awaiting radiotherapy: self-reported wellbeing, general psychological distress, symptom distress, sexual function, and supportive care needs. Gynecol Oncol. 2022;167(1):42–50. doi:10.1016/j.ygyno.2022.08.008
24. Froeding LP, Ottosen C, Rung-Hansen H, et al. Sexual functioning and vaginal changes after radical vaginal trachelectomy in early stage cervical cancer patients: a longitudinal study. J Sex Med. 2014;11(2):595–604. doi:10.1111/jsm.12399
25. Zhu P, Shi G, Wu Q, et al. Ethical challenges of death faced by nursing undergraduates in clinical practice: a qualitative study. Nurse Educ Today. 2022;118:105516. doi:10.1016/j.nedt.2022.105516
26. Stavropoulou A, Vlamakis D, Kaba E, et al. Living with a Stoma’: exploring the lived experience of patients with permanent colostomy. Int J Environ Res Public Health. 2021;18(16):8512. doi:10.3390/ijerph18168512
27. Álvarez-Villarreal M, Velarde-García JF, Chocarro-Gonzalez L, et al. Body changes and decreased sexual drive after dialysis: a qualitative study on the experiences of women at an Ambulatory Dialysis Unit in Spain. Int J Environ Res Public Health. 2019;16(17):3086. doi:10.3390/ijerph16173086
28. Miller KD, Fidler-Benaoudia M, Keegan TH, et al. Cancer statistics for adolescents and young adults. CA. 2020;70(6):443–459. doi:10.3322/caac.21637
29. Novackova M, Pastor Z, Chmel R, et al. Sexuality and quality of life after nerve-sparing radical hysterectomy for cervical cancer: prospective study. Taiwan J Obstet Gynecol. 2022;61(4):641–645. doi:10.1016/j.tjog.2021.10.006
30. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inf. 2004;22:63–75. doi:10.3233/EFI-2004-22201
31. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
32. Iżycki D, Woźniak K, Iżycka N. Consequences of gynecological cancer in patients and their partners from the sexual and psychological perspective. Prz Menopauzalny. 2016;15(2):112–116. doi:10.5114/pm.2016.61194
33. Cianci S, Tarascio M, Arcieri M, et al. Post Treatment Sexual Function and Quality of Life of Patients Affected by Cervical Cancer: a Systematic Review. Medicina. 2023;59(4):704. doi:10.3390/medicina59040704
34. Oldertrøen Solli K, de Boer M, Nyheim Solbraekke K, et al. Male partners’ experiences of caregiving for women with cervical cancer-A qualitative study. J Clin Nurs. 2019;28(5–6):987–996. doi:10.1111/jocn.14688
35. Osei Appiah E, Amertil NP, Oti-Boadi EE, et al. Impact of cervical cancer on the sexual and physical health of women diagnosed with cervical cancer in Ghana: a qualitative phenomenological study. Women’s Health. 2021;17:17455065211066075. doi:10.1177/17455065211066075
36. Dedden SJ, Werner MA, Steinweg J, et al. Hysterectomy and sexual function: a systematic review and meta-analysis. J Sex Med. 2023;20(4):447–466. doi:10.1093/jsxmed/qdac051
37. Saris LMH, Vlooswijk C, Kaal SEJ, et al. A Negative Body Image among Adolescent and Young Adult (AYA) Cancer Survivors: results from the Population-Based SURVAYA Study. Cancers. 2022;14(21):5243. doi:10.3390/cancers14215243
38. Zou K, Huang Y, Li Z. Prevention and treatment of human papillomavirus in men benefits both men and women. Front Cell Infect Microbiol. 2022;12:1077651. doi:10.3389/fcimb.2022.1077651
39. Löfgren C, Elmerstig E, Schröder J, et al. Changes in Intimacy and Sexuality During the COVID-19 Pandemic: a Qualitative Analysis of Data from a Survey on Partnered Individuals in Eight European Countries. Sex Cult. 2023;27(2):693–714. doi:10.1007/s12119-022-10035-1
40. Isabirye A. Individual and intimate-partner factors associated with cervical cancer screening in Central Uganda. PLoS One. 2022;17(9):e0274602. doi:10.1371/journal.pone.0274602
41. Du X, Wang D, Du H, et al. The correlation between intimate relationship, self-disclosure, and adaptability among colorectal cancer enterostomy patients. Medicine. 2021;100(19):e25904. doi:10.1097/MD.0000000000025904
42. Ezechi O, Akinsolu F, Salako A, et al. High-risk human papillomavirus infection among Nigerian women: a systematic review and meta-analysis. J Int Med Res. 2023;51(7):3000605231182884. doi:10.1177/03000605231182884
43. Thom B, Benedict C, Friedman DN, et al. Economic distress, financial toxicity, and medical cost-coping in young adult cancer survivors during the COVID-19 pandemic: findings from an online sample. Cancer. 2021;127(23):4481–4491. doi:10.1002/cncr.33823
44. Xie J, Sun Q, Duan Y, et al. Reproductive concerns among adolescent and young adult cancer survivors: a scoping review of current research situations. Cancer Med. 2022;11(18):3508–3517. doi:10.1002/cam4.4708
45. Honnavar P, Mansoor E, Tulloch C, et al. Cervical Cancer and Human Papillomavirus Awareness among Women in Antigua and Barbuda. Medicine. 2023;59(7):1230. doi:10.3390/medicina59071230
46. Li N, Shen C, Wang R, et al. The real experience with women’s hysterectomy: a meta-synthesis of qualitative research evidence. Nursing Open. 2023;10(2):435–449. doi:10.1002/nop2.1348
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.