")
Back to Journals » International Journal of Women's Health » Volume 9
Sexual autonomy and contraceptive use among women in Nigeria: findings from the Demographic and Health Survey data
Authors Viswan SP, Ravindran TKS, Kandala NB, Petzold MG, Fonn S
Received 2 February 2017
Accepted for publication 29 April 2017
Published 23 August 2017 Volume 2017:9 Pages 581—590
DOI https://doi.org/10.2147/IJWH.S133760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Saritha P Viswan,1 T K Sundari Ravindran,1,2 Ngianga-Bakwin Kandala,1,3,4 Max G Petzold,1,5 Sharon Fonn1
1School of Public Health, University of the Witwatersrand, Johannesburg, South Africa; 2Achutha Menon Centre for Health Science Studies, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala, India; 3Division of Epidemiology and Biostatistics, School of Public Health, University of the Witwatersrand, Johannesburg, South Africa; 4Department of Mathematics, Physics and Electrical Engineering, Faculty of Engineering and Environment, Northumbria University, Newcastle upon Tyne, UK; 5Department of Public Health and Community Medicine, University of Gothenburg, Gothenburg, Sweden
Context: The persistent low contraceptive use and high fertility in Nigeria despite improvements in educational achievements calls for an examination of the role of factors, which may moderate the use of modern contraception. This article explores the influence of sexual autonomy on the use of modern contraceptive methods among women and its relative importance compared with other, more traditional, indicators of women’s autonomy such as education and occupation.
Data and methods: Data from two Demographic and Health Surveys (DHS), 2008 and 2013, were used in this study. An index of sexual autonomy was constructed by combining related DHS variables, and its association with current use of modern contraception was examined at each time point as well as over time using multivariate regression analysis.
Results: The observed prevalence for use of modern contraception was 2.8 and 2.6 times higher among women who had high sexual autonomy in 2008 and 2013, respectively. The corresponding figures for women with secondary or higher education were 8.2 and 11.8 times higher, respectively, compared with women with no education. But after controlling for wealth index, religion, place of residence, autonomy and experience of intimate partner violence (IPV), the likelihood of use of modern contraception was lowered to about 2.5 (from 8.2) and 2.8 (from 11.8) times during 2008 and 2013, respectively, among women with secondary or higher education. The likelihood of use of modern contraception lowered only to 1.6 (from 2.8) and 1.8 (from 2.6) times among women with high sexual autonomy after controlling for other covariates, respectively, during the same period.
Conclusion: Sexual autonomy seems to play an important role in women’s use of modern contraceptive methods independent of education and a number of other factors related to women’s status. Sexual autonomy needs to be simultaneously promoted alongside increasing educational opportunities to enhance women’s ability to use modern contraception.
Keywords: family planning, sexuality, decision making, education, empowerment, intimate partner violence
Introduction
Women’s contraceptive use is a function of many social, cultural and individual factors. These factors include education, occupation, economic status and autonomy or empowerment. A number of authors have reported that education has a strong influence on the use of contraception among women.1–6 Women with higher educational attainment were more likely to request their partners to use condoms.7 Studies have also found that occupation and wealth influence the use of modern contraception.3,8 For example, the use of contraception was higher among women who were engaged in skilled labour compared with those who were not engaged in remunerative employment.8–10 Increases in women’s general autonomy and greater use of contraception have been demonstrated in numerous studies. It was identified that in 8 of 19 sub-Saharan African countries, women with greater autonomy were more likely to use contraception.10 A similar result was also found in three of four sub-Saharan African countries using different methods,11 and similar results were also reported from Nigeria and Tanzania.5,7,12 This association has also been reported in many Asian countries.13–16
Measuring autonomy
Studies reporting women’s autonomy or empowerment have not been consistent in their use of terminologies. Alternate terms such as women’s position or role and gender inequality were frequently used interchangeably with autonomy in literature reviewed by us. Many studies have used one or more indicators from the Demographic and Health Surveys (DHS)13,17,18 to measure autonomy, for example, women’s involvement in household-level decision-making involving their own health care, large household purchases and ability to decide to visit family. Some researchers have elaborated autonomy as having the following three dimensions: economic autonomy, physical or movement autonomy and decision-making autonomy; these aspects are difficult to separate as they are interlinked. Other researchers incorporated the role of women in decisions regarding sexuality in constructing measures of autonomy/empowerment such as the role of women in controlling their sexual relations12 or reproductive decisions.9,14 Very few have constructed explicit measures for sexual autonomy.
Studies have used a range of sexual and reproductive variables in combination to describe measures of women’s sexual autonomy. For example, an Indian study among currently married women attending the gynecology and obstetrics outpatient services16 considered sexual and reproductive decisions such as when the couple would have sex and who made decisions about using contraception as indicating women’s autonomy. A study based on Reproductive Health and Family Planning Survey of Pakistan19 defined a woman as having reproductive autonomy if she had a role in deciding to have no more children, in delaying the next birth or in deciding to use a family planning method. There are also studies that included indicators from the DHS when constructing an index of autonomy as to whether a husband was justified in hitting or beating his wife if she refused to have sex with him.20,21
However, sexual autonomy has been addressed in a relatively small number of studies compared with the large body of literature on women’s general autonomy. In this article, sexual autonomy refers to the role of women in decisions related to when, with whom and how sexual relations were practiced and includes the idea that women must have freedom to decide on their sexual relations both within and out of wedlock. Intimate partner violence (IPV) on women – whether physical violence because of issues related to sex or sexual violence was viewed by us as an indicator of the absence of sexual autonomy.
Studies from Ghana22 and Philippines23 have explicitly constructed an indicator of sexual autonomy The Philippines study considered, as a part of the sexual autonomy index, DHS questions on whether a wife was justified in refusing to have sex with her husband when a) she knows her husband had a sexually transmitted disease, b) she knows her husband had sex with other women, c) she had recently given birth or d) she was tired or not in the mood. The Ghanaian study considered DHS variables: can you say “no” to your husband/partner if you do not want to have sexual intercourse? In your opinion, is a husband justified in hitting or beating his wife if she refuses to have sex with him? Could you ask your husband/partner to use a condom if you wanted him to? If a wife knows her husband has a disease that she can contract during sexual intercourse, is she justified in asking him to use a condom when they have sex? Is a woman justified in refusing sex if she is tired/not in the mood? These studies found that the high sexual autonomy lowers the risk of unwanted pregnancy24 or increased the use of modern contraception.22 The Philippines study did not, however, examine the relationship of sexual autonomy to contraceptive use. Other studies have used one or two of the indicators used in constructing these sexual autonomies as an indicator of empowerment or autonomy and found empowerment to be related to the use of modern contraception.21 Associations have also been found between physical and sexual IPV and use of modern contraception, but the results have been equivocal, indicating that the relationship is possibly context specific and mediated by other factors.25,26
This article explores the role of sexual autonomy in use of modern contraception among currently married women in Nigeria, using data from DHS for 2008 and 2013, the 2 years for which variables for constructing a sexual autonomy index were available.
The Nigerian context
In Nigeria, the prevalence of contraceptive use, which was 9.8% among currently married women in 2013,27 continues to be much lower than the African average, despite the higher prevalence of family planning knowledge (85%).3 The proportion of women without education decreased from 62.2% in 1990 to 45.0% in 2013, and the labour force participation of females increased from 34.1% in 1990 to 42.4% in 2014. Even with these improvements, total fertility rate (TFR) declined only by about 0.5 births per women since the 1990s and was 5.25 in 2014.
Studies from Nigeria have reported the association of modern contraceptive use with educational status of the woman,24 women’s empowerment25 and decision-making26 regarding their own health care.27 However, very little is known about how women’s decision-making in matters related to sexuality influences their use of contraception.28,29
Our objective is to examine whether and how sexual autonomy or its absence, as indicated by experience of physical and/or sexual IPV, affects contraceptive use in Nigeria, the role of general (as distinct from sexual) autonomy (which was constructed using variables describing women’s ability to make decisions in her own household, about health care, regarding daily needs of the family or freedom of movement), and the relative importance of education in influencing modern contraceptive use. We have worked using DHS data obtained at two time points to confirm the direction and strength of association between sexual autonomy and use of modern contraception.
Data and methods
Data
The DHS provide information on demographic and health characteristics of a representative sample of the population for about 90 different countries of the world. In Nigeria, standard DHS data were collected during 1990, 1999, 2003, 2008 and 2013. The present study used DHS data from the 2008 and 2013 as these two surveys provide information on variables that we defined as indicators of sexual autonomy. The Nigerian Demographic and Health Survey (NDHS) collected data from a nationally representative sample of women aged 15–49 years. Women who were currently married or in union and for whom required data were complete were included in the analysis. The woman’s section of the DHS questionnaire collected information on background characteristics, reproductive history, childhood mortality, knowledge and use of family planning methods, fertility preferences, antenatal, delivery and postnatal care, female empowerment and a host of other health issues relating to specific diseases and disease-prevention programs/interventions. The details of sampling design, survey tools and data collection methods are provided in the DHS reports.22,30
Methods
The dependent or outcome variable used was dichotomous and assesses the current use of at least one of the modern methods of contraception before the survey by currently married or partnered women. Univariate statistics were used to describe the characteristics of the population and bivariate analysis carried out to understand the percentage distribution by the outcome variable. Chi-square tests were applied to understand the significance of the relationships found between variables. Predictor variables included in the analysis were women’s household decision-making index, sexual autonomy index, experience of sexual IPV index and experience of physical IPV index. Principal component analysis (PCA) was used to construct the indices of sexual autonomy, household decision-making autonomy, physical IPV and sexual IPV. All these indices were classified as low or high. Women’s household decision-making (her general autonomy) was based on women’s involvement in her own health care, large household purchases, freedom to embark on family visits and role in decision on husband’s earnings. Sexual autonomy was derived from three questions about whether women can ask husband/partner to use a condom if she wanted him to? If a wife knows her husband has a disease that she can contract during sexual intercourse, is she justified in asking him to use a condom when they have sex? Is a woman justified in refusing sex if she is tired/not in the mood? The experience of physical violence considered questions such as to whether she had ever been pushed, shook or had something thrown at her, ever been slapped, ever been punched with a fist or hit by something harmful, ever been kicked or dragged, ever had arm twisted or hair pulled by husband/partner, ever been strangled or burnt and ever been threatened with a knife/gun or other weapon. Similarly, experience of sexual IPV was measured through three questions in the DHS: as ever been physically forced into unwanted sex, ever been forced into other unwanted sexual acts and ever been physically forced to perform sexual acts the respondent didn’t want to perform. Other predictor variables considered were place of residence defined as rural or urban; educational background of women classified as illiterate, primary and secondary or higher educated; wealth index (a composite index based on the household’s ownership of a number of consumer items) classified as low, medium and high and religion.
Multivariate logistic regression analysis was used to study the potential association between contraceptive use, sexual autonomy and other explanatory variables. Four models were constructed to understand the unadjusted and adjusted association of sexual autonomy and education with the use of modern contraception. Models 1 and 2 were the unadjusted relationships of sexual autonomy and education to current use of modern contraception, respectively. In model 3, we studied the effect of sexual autonomy or education on current use of modern contraception while controlling the effect of other variables. Model 4 described the effect of each independent variable on use of modern contraception while controlling all other covariates. Generalized linear model (GLM) with the binomial link function was used to construct the graph describing trend over time. The graphs were plotted by the estimated marginal means computed for sexual decision-making autonomy and use of modern contraception. Data were analyzed using SPSS version 20.0 (IBM Corporation, Armonk, NY, USA).
Results
Table 1 presents the distribution of the population according to the dependent and predictor variables. From the 2008 and 2013 DHS, 23,954 and 27,274 women who were currently married or in a union constituted the study sample. Approximately 9% in 2008 and 10% in 2013 reported that they currently used any method of modern contraception. The mean age of the respondents was about 31 years with a standard deviation of about 9 during both the surveys. The percentage of the population with no education decreased from 51.3% in 2008 and to 45.9% in 2013. The proportion of women with secondary or more education increased over the period. More than 40% of women were in the lowest wealth quintile at both time points. The religious composition was almost stable from 2008 to 2013. More than half of the women reported that they were Muslim and about 42% were Christians. Experience of physical violence from an intimate partner decreased between 2008 and 2013, but sexual violence increased over the same period. An overall increase in women’s role in decision-making was observed between 2008 and 2013 except for decisions about large household purchases.
 | Table 1 Demographic, socioeconomic, reproductive and autonomy characteristics of women for 2013 and 2008 Nigeria DHS |
The bivariate relationship between use of modern contraception and other independent variables is shown in Table 2. Current use of contraception was higher among women with higher education (P<0.001). Among women who were illiterate, the use of contraception reduced between 2008 and 2013. Among those women who had primary or secondary education, the use of modern contraception increased between 2008 and 2013 (P<0.001). Compared to urban women, the proportion of use of modern contraception was very low in rural areas and also no increase occurred between 2008 and 2013 (P<0.001). Use of modern contraception increased with increasing wealth (P<0.001). However, among the poor, the use of modern contraception decreased from 2008 to 2013 (P<0.001). The proportion of women using modern contraception was about four times higher among those who described themselves as Christians compared to Muslims (P<0.001).
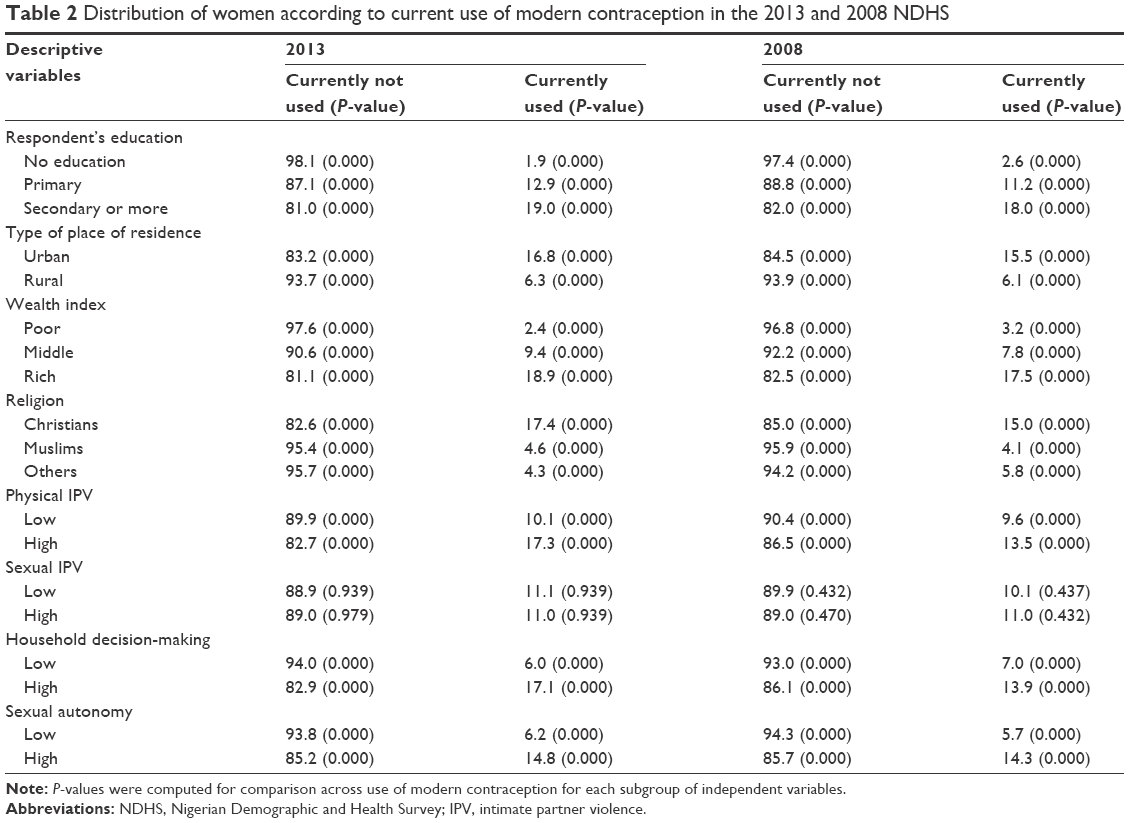 | Table 2 Distribution of women according to current use of modern contraception in the 2013 and 2008 NDHS |
A higher proportion of women experiencing high physical IPV reported use of modern contraception compared to those experiencing low physical IPV (P<0.001). Women with high household decision-making or with high sexual autonomy used modern contraception more (P<0.001). The chi-square significance test showed that all bivariate relations were significant for use of modern contraception except for sexual IPV.
From models 1 and 2 in Table 3, it seems that the unadjusted effect of education on use of modern contraception was very high compared to the role of sexual autonomy. The use of modern contraception was higher for both years (OR 2.771 and 2.625, 95% CI 2.451–3.132 and 2.363–2.916 for 2008 and 2013, respectively) among those who had high sexual autonomy compared with those with low sexual autonomy. But those with secondary or higher education had an 8–12 times higher (OR 8.254 and 11.783, 95% CI 7.262–9.380 and 10.274–13.514 for 2008 and 2013, respectively) chance of using modern contraception than those with no education.
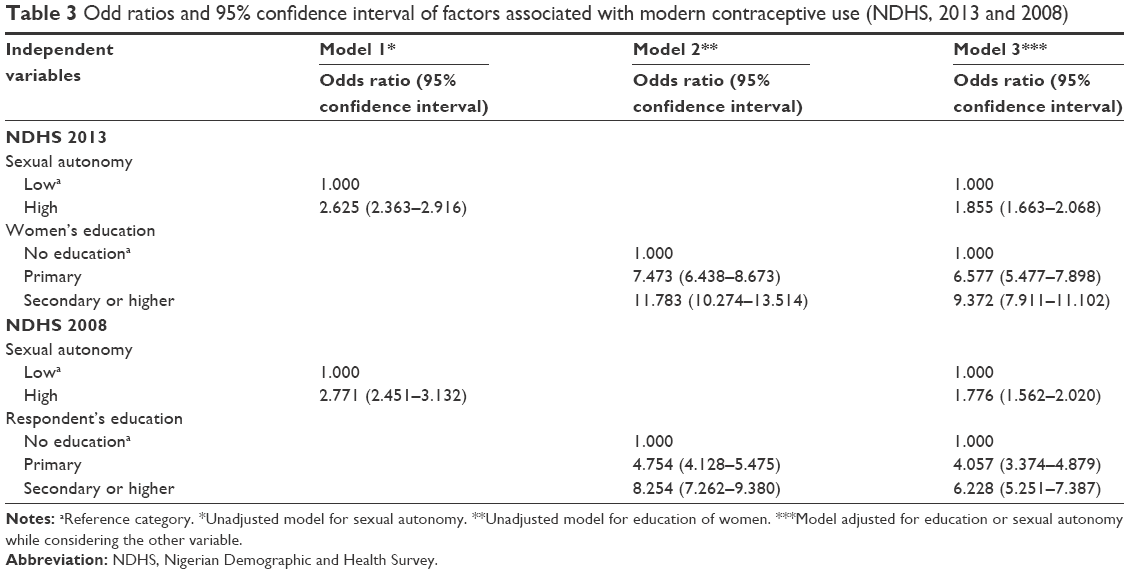 | Table 3 Odd ratios and 95% confidence interval of factors associated with modern contraceptive use (NDHS, 2013 and 2008) |
From model 3 in Table 3, we observe that, when controlling for the effect of sexual autonomy, those with secondary or higher education were nine times (OR 9.372, 95% CI 7.911–11.102) more likely to use modern contraception and seven times (OR 6.577, 95% CI 5.477–7.898) more likely if they had primary education during 2013. However, women with high sexual autonomy, irrespective of their education, had 1.8 times (OR 1.855, 95% CI 1.663–2.068) higher chance of using modern contraception in 2013.
The effect of each variable, when controlling for other covariates, on modern contraceptive use is described in Table 4. In this table, when considering the effect of one variable on the outcome variable, the effect of all other variables are adjusted for the presence or absence of other covariates, which makes no change in the relation between dependent and the one independent variable considered. Here, the most influential variable was education of the respondent. After education, high wealth index and high sexual autonomy had the second and third most important influence on use of modern contraception. Experience of high physical IPV seemed to be promoting the use of modern contraception compared with those who had low physical IPV, while there is no difference in use of modern contraception observed between women who experienced low or high sexual violence from intimate partner. Household decision-making had lesser influence on use of modern contraception (1.32 times [OR 1.322, 95% CI 1.170–1.493] in 2008 and 1.68 times [OR 1.688, 95% CI 1.514–1.881] in 2013) than sexual autonomy.
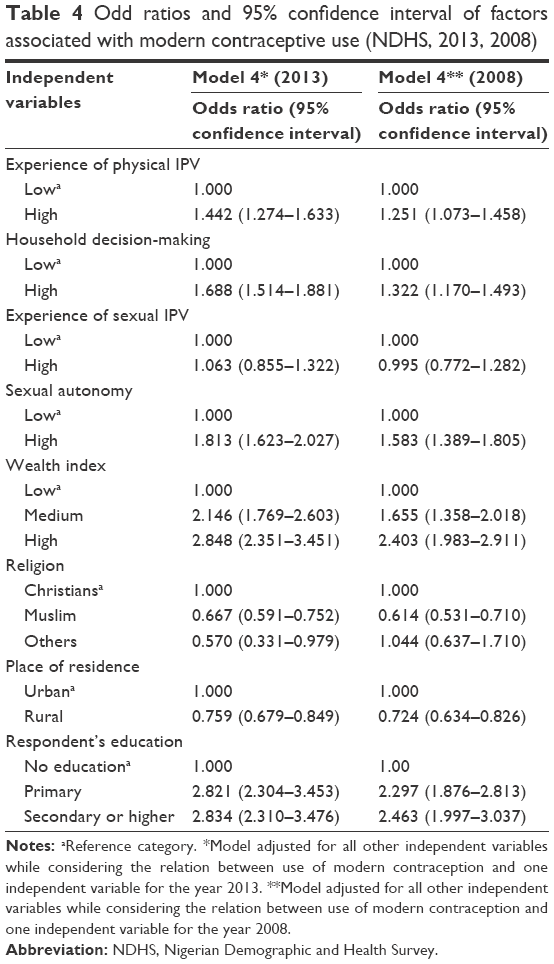 | Table 4 Odd ratios and 95% confidence interval of factors associated with modern contraceptive use (NDHS, 2013, 2008) |
What emerges as significant from Table 4 is that when adjusted for other covariates, the influence of higher education on current use of modern contraception reduces drastically (OR 2.834 in adjusted model from OR 11.783 in unadjusted model). This shows that the effect of education on modern contraceptive use is diminished when the other covariates are considered. In other words, the effect of education is modified by other factors. In the adjusted models, sexual autonomy has about 60% or higher chance of influencing the use of modern contraception (OR 1.813 and 1.583, 95% CI 1.623–2.027 and 1.389–1.805). The relationship between sexual autonomy and current use of modern contraception however remains more stable (OR 1.813 and 1.583 in adjusted models from OR 2.625 and 2.771 in unadjusted models in 2013 and 2008) even after adjusting for other covariates.
The estimated marginal mean of sexual autonomy and current use of modern contraception are shown in Figure 1, depicting the trend in the use of modern contraception over time. We can observe that the marginal means of sexual autonomy had increased from 2008 to 2013 among users of modern contraception. The mean values for sexual autonomy were 2.255 and 2.322 for 2008 and 2013, respectively. In Figure 2, we included education as a covariate, which raised the mean value for using modern contraception to 2.501 in 2008 and 2.521 in 2013. This indicates that education is an influential intermediary variable in enhancing the role of sexual autonomy in increasing modern contraceptive use.
 | Figure 1 Sexual decision-making and contraceptive use. |
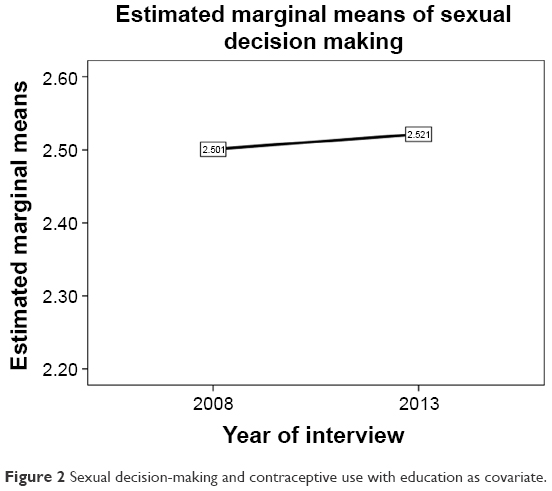 | Figure 2 Sexual decision-making and contraceptive use with education as covariate. |
Figure 3 depicts the graphical representation of the combined effect of education and sexual autonomy on modern contraceptive use. Compared to women with very low sexual autonomy, a higher proportion of those with high levels of autonomy were currently using modern contraception. At all education levels, women with higher sexual autonomy had higher odds of currently using modern contraception than those with lower sexual autonomy.
 | Figure 3 Current use of modern contraception by education and sexual decision-making. |
Discussion and conclusion
This article set out to explore whether and how sexual autonomy or its absence affects the use of modern contraception among women in Nigeria in recent years (2008–2013). We found that women with high sexual autonomy had about 60% of higher chance of using modern contraception than those with low sexual autonomy at both time points, even after controlling for other variables such as socioeconomic status. We found only one study examining the role of sexual autonomy and the use of modern contraception, which indicated increased use of modern contraception with high sexual autonomy in Ghana.22 In our study, we observed a strong relationship between sexual autonomy and contraceptive use, which was more stable than the relationship between education and use of modern contraception over time.
We considered prevalence of physical IPV and sexual IPV as proxies for the absence of sexual autonomy and explored how these affected the use of modern contraception. Women reporting high physical IPV had higher chance (25% in 2008, and 44% in 2013) of using modern contraception compared with those experiencing low levels of IPV. Sexual IPV, however, did not demonstrate any impact on the use of modern contraception.
In contrast to our findings, a study based on 2007 DHS of Jordan reported that women ever experiencing severe physical violence from their husband were significantly less likely to use contraception than women who did not report severe physical violence (OR 0.34).31 But, a study of a large sample of women from sub-Saharan African countries reported that women experiencing sexual violence had a 1.5 times higher odds of using a modern method of contraception.32 Others studies have corroborated the association of sexual violence with higher use of modern contraception41 and also reported that the frequency of use of contraception increased with multiplicity of violence subtypes (P>0.01).33 A slightly more nuanced finding from Nicaragua was34 that experiencing IPV was associated with a decrease in women’s use of partner-dependent methods and condom use by their male partners, rather than any method of contraception.
Thus, it would appear that sexual and physical IPV can affect the use of modern contraception in either direction. One explanation of the positive association of IPV with contraceptive use has been that it reflects the desire of women who experience IPV to avert pregnancy under unfavorable conditions.33 It may be that women who have the confidence to report IPV may also be more likely to use contraceptives. However, many explanations are possible: partners may prevent women’s use of contraception by threatening violence. Furthermore, even when one observes a positive association between IPV and use of modern contraception, it may not be possible to establish directionality because of the possibility that initiation of contraceptive use might make some women vulnerable to violence from their partner.9,33 The actual relationship between IPV and contraceptive use may depend on the way autonomy reinforces or undermines IPV.6,35,42
Our study also found that women with high household decision-making power had a 32%–69% higher chance of using modern contraception than their counterparts. Other studies too have found an association between various measures of decision-making and contraceptive use. Based on the Fertility and Family Planning Survey, a study from Pakistan similarly found that women with freedom of mobility and final say in household decisions, such as choices with regard to seeking health care for children and food purchase, were more likely to be current users of contraception.25 Other studies also found a positive association for use of modern contraception and women’s greater decision-making role in the household.6
While sexual autonomy, IPV and general autonomy were all significantly associated with use of modern contraception in our study, women’s educational status showed the strongest association of all. But the effect of education was moderated by other variables considered in this study. It raises the question as to whether education alone, without other interventions, is sufficient to improve contraceptive use. A study in 27 sub-Saharan African countries found that modern contraceptive prevalence is generally high among women with at least secondary education, but some studies have found that contraceptive prevalence did not increase significantly with increasing levels of education.36 For example, in some sub-Saharan African countries, Madagascar and Rwanda, prevalence of modern contraceptive use increased during 2003 to 2008 but only a marginal increase was observed among women with secondary or more education; and countries like Zimbabwe experienced a plateauing of contraceptive use even as the proportion of women with secondary education increased.36 The relationship between attending school and contraceptive use was mediated by other predictors such as approval of family planning, knowledge of contraceptive methods and visiting a health clinic.37,43,44 So access to care and ability to access care appear important in addition to education.
This study not only found that a greater proportion of women with high sexual autonomy (compared to low) used modern contraceptives, even after controlling for the effect of education and other covariates, but also that high sexual autonomy had a more consistent effect on contraceptive use and was less affected by other covariates compared with the educational status of women. Thus, we postulate that sexual autonomy can impart a direct effect on the use of modern contraceptive methods.
While it stands to reason that sexual autonomy may be expected to have an influence on use of modern contraception, studies seldom analyze the relationship between these variables. One of the reasons may be the unavailability of adequate explanatory variables. Even though DHS provide data on sexual decision-making, these are not available consistently for all time periods.
While there is a paucity of studies documenting distribution of availability and accessibility to services providing modern contraception in Nigeria; the low contraceptive prevalence rate may be attributed to poorer access to contraceptive services at government health facilities compared with private clinics and the relative lack of access to private facilities for at least part of the population.38 Patent medical shops remain the main source of contraceptives in Nigeria.39 It was reported that a strong political will and prioritization of safe motherhood and contraception services is still required in Nigeria.40
Findings from this study have implications for both programs and research. In terms of programs, the findings indicate that creating conditions in which women are able to exercise sexual autonomy is likely to enhance their ability to use modern contraception, irrespective of their levels of education, and that education combined with increased sexual autonomy would produce better outcomes. Further research is needed to understand the pathways through which sexual autonomy, education and use of modern contraception act. However, in the meanwhile, programmatic interventions should not stop short by focusing only on women’s education; sexual autonomy needs to be simultaneously promoted.
Limitations of the study
Our study is limited to those variables available for analysis in DHS. The cross-sectional nature of these data can only demonstrate associations and can reveal no causal relationships between variables. Data on women’s use of modern contraception influenced by supply side factors, like access to services, distribution mechanisms, stock-outs, etc., were not available to us and we can only postulate on the effect of this. In addition, women with different social or cultural backgrounds may report their roles and experience of violence differently, which may also influence the results.
Acknowledgment
Saritha P Viswan was a postdoctoral student funded by the Gender and Health Unit in the School of Public Health, University of the Witwatersrand.
Disclosure
The authors report no conflicts of interest in this work.
References
Atteraya MS, Kimm H, Song IH. Women’s autonomy in negotiating safer sex to prevent HIV: findings from the 2011 Nepal Demographic and Health Survey. AIDS Educ Prev. 2014;26(1):1–12. | ||
Dwivedi LK, Sogarwal R. Understanding contraceptive adoption in India: does women’s autonomy matter? J Fam Welf. 2008;54(1):24–34. | ||
Kabir MA, Khan MMH, Kabir M, Rahman MM, Patwary MFK. Impact of woman’s status on fertility and contraceptive use in Bangladesh: evidence from Bangladesh Demographic and Health Survey, 1999–2000. J Fam Welf. 2005;51:1–10. | ||
Al Riyami A, Afifi M, Mabry RM. Women’s autonomy, education and employment in Oman and their influence on contraceptive use. Reprod Health Matters. 2004;12:144–154. | ||
Ayoub SA. Effects of Women’s schooling on contraceptive use and fertility in Tanzania. African Population Studies. 2004;19(2):139–157. | ||
Bawah AA, Akweongo P, Simmons R, Phillips JF. Women’s fears and men’s anxieties: the impact of family planning on gender relations in northern Ghana. Stud Fam Plann. 1999;30:54–66. | ||
Darteh EKM, Doku DT, Esia-Donkoh K. Reproductive health decision making among Ghanaian women. Reprod Health. 2014;11:23. | ||
Mason KO, Smith HL. Husbands’ versus wives’ fertility goals and use of contraception: the influence of gender context in five Asian countries. Demography. 2000;37:299–311. | ||
Kritz MM, Makinwa-Adebusoye P, Gurak DT. Wife’s Empowerment and Fertility in Nigeria: the Role of Context. Ithaca, NY: Cornell University, Department of Rural Sociology, Population and Development Program; 1997:13. Issue 5. (Population and Development Program Working Paper Series No. 97.05). | ||
Msuya SE, Adinan J, Mosha N. Intimate partner violence and empowerment among women in Tanzania: prevalence and effect on utilization of reproductive and maternal health services. Glob Health Action. 2015;7:22942. | ||
Patrikar SR, Basannar DR, Seema Sharma M. Women empowerment and use of contraception. Med J Armed Forces India. 2014;70(3):253–256. | ||
Moonzwe Davis L, Schensul SL, Schensul JJ, Verma RK, Nastasi BK, Singh R. Women’s empowerment and its differential impact on health in low-income communities in Mumbai, India. Glob Public Health. 2014;9:481–494. | ||
Deb S, Kabir A, Kawsar LA. Women’s empowerment and regional variation of contraceptive norms in Bangladesh. Int Q Community Health Educ. 2010;31(4):401–410. | ||
Castro R, Casique I, Brindis CD. Empowerment and physical violence throughout women’s reproductive life in Mexico. Violence Women. 2008;14:655–677. | ||
Do M, Kurimoto N. Women’s empowerment and choice of contraceptive methods in selected African countries. Int Perspect Sex Reprod Health. 2012;38:023–033. | ||
Nanda G, Schuler SR, Lenzi R. The influence of gender attitudes on contraceptive use in Tanzania: new evidence using husbands’ and wives’ survey data. J Biosoc Sci. 2013;45(3):331–344. | ||
Ahmed S, Creanga AA, Gillespie DG, Tsui AO. Economic status, education and empowerment: implications for maternal health service utilization in developing countries. PLoS One. 2010;5(6):e11190. | ||
Ung M, Boateng GO, Armah FA, Amoyaw JA, Luginaah I, Kuuire V. Negotiation for safer sex among married women in Cambodia: the role of women’s autonomy. J Biosoc Sci. 2014;46(1):90–106. | ||
Hakkim A, Salway S, Mumtaz Z. Women’s autonomy and uptake of contraception in Pakistan. Asia Pac Popul J. 2003;18(1):63–82. | ||
Kumar A, Fuloria K, Taunk A. A comparative study of tribal and non tribal women in the state of Uttarakhand (India) in the field of womenâ s autonomy contraceptive used and family planning. J Res Peace Gen Dev. 2012;2:156–161. | ||
Jesmin SS, Cready CM. Can a woman refuse sex if her husband has a sexually transmitted infection? Attitudes toward safer-sex negotiation among married women in Bangladesh. Cult Health Sex. 2014;16(6):666–682. | ||
Crissman HP, Adanu RM, Harlow SD. Women’s sexual empowerment and contraceptive use in Ghana. Stud Fam Plann. 2012;43(3):201–212. | ||
Saleem A, Pasha GR. Women’s reproductive autonomy and barriers to contraceptive use in Pakistan. Eur J Contracept Reprod Health Care. 2008;13:83–89. | ||
Abada T, Tenkorang EY. Women’s autonomy and unintended pregnancies in the Philippines. J Biosoc Sci. 2012;44(6):703–718. | ||
Maxwell L, Devries K, Zionts D, Alhusen JL, Campbell J. Estimating the effect of intimate partner violence on women’s use of contraception: a systematic review and meta-analysis. PLoS One. 2015;10:e0118234. | ||
Dalal K, Andrews J, Dawad S. Contraception use and associations with intimate partner violence among women in Bangladesh. J Biosoc Sci. 2012;44(1):83–94. | ||
National Population Commission and ICF International, Nigeria Demographic and Health Survey 2013. Abuja; Rockville, MD: National Population Commission; ICF International; 2014. | ||
Oye-Adeniran BA, Adewole IF, Umoh AV, et al. Community-based study of contraceptive behaviour in Nigeria. Afr J Reprod Health. 2006;10(2):90–104. | ||
Corroon M, Speizer IS, Fotso JC, et al. The role of gender empowerment on reproductive health outcomes in urban Nigeria. Matern Child Health J. 2014;18(1):307–315. | ||
OlaOlorun FM, Hindin MJ. Having a say matters: influence of decision-making power on contraceptive use among Nigerian women ages 35–49 years. PLoS One. 2014;9:e98702. | ||
Okenwa L, Lawoko S, Jansson B. Contraception, reproductive health and pregnancy outcomes among women exposed to intimate partner violence in Nigeria. Eur J Contracept Reprod Health Care. 2011;16(1):18–25. | ||
Austin A. Unmet contraceptive need among married Nigerian women: an examination of trends and drivers. Contraception. 2015;91(1):31–38. | ||
Haque SE, Rahman M, Mostofa MG, Zahan MS. Reproductive health care utilization among young mothers in Bangladesh: does autonomy matter? Womens Health Issues. 2012;22(2):e171–e180. | ||
Woldemicael G. Do women with higher autonomy seek more maternal health care? Evidence from Eritrea and Ethiopia. Health Care Women Int. 2010;31(7):599–620. | ||
Ogunjuyigbe PO, Akinlo A, Oni GO. Violence against women as a factor in unmet need for contraception in southwest Nigeria. J Fam Violence. 2009;25:123–130. | ||
National Population Commission, Nigeria and ICF Macro, Nigeria Demographic and Health Survey 2008. Abuja: National Population Commission and ICF Macro; 2009. | ||
O’Hara K, Tsai LC, Carlson CE, Haidar YM. Experiences of intimate-partner violence and contraception use among ever-married women in Jordan. East Mediterr Health J. 2013;19(10):876. | ||
Amazigo U, Silva N, Kaufman J, Obikeze DS. Sexual activity and contraceptive knowledge and use among in-school adolescents in Nigeria. Int Fam Plan Perspect. 1997;23:28. | ||
Monjok E. Contraceptive practices in Nigeria: literature review and recommendation for future policy decisions. Open Access J Contracept. 2010;2010(1):9–22. | ||
Adekunle AO, Otolorin EO. Evaluation of the Nigerian population policy – myth or reality? Afr J Med Med Sci. 2000;29:305–310. | ||
Alio AP, Daley EM, Nana PN, Duan J, Salihu HM. Intimate partner violence and contraception use among women in Sub-Saharan Africa. Int J Gynecol Obstet. 2009;107(1):35–38. | ||
Tuladhar S, Khanal KR, Lila KC, Ghimire PK, Onta K. Women’s Empowerment and Spousal Violence in Relation to Health Outcomes in Nepal: Further Analysis of the 2011 Nepal Demographic and Health Survey. Kathmandu: Ministry of Health and Population; 2013:59. | ||
Emina JBO, Chirwa T, Kandala N-B. Trend in the use of modern contraception in sub-Saharan Africa: does women’s education matter? Contraception. 2014;90(2):154–161. | ||
Gordon C, Sabates R, Bond R, Wubshet T. Women’s education and modern contraceptive use in Ethiopia. Int J Educ. 2011;3:E9. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.