Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Sexual Adverse Effects and Erectile Dysfunction During Buprenorphine/Naloxone Combination Treatment for Opioid Use Disorders
Authors Bestepe EE, Tunali N, Sarıdoğan GE ![]()
Received 13 August 2020
Accepted for publication 15 October 2020
Published 12 November 2020 Volume 2020:16 Pages 2695—2705
DOI https://doi.org/10.2147/NDT.S276708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Engin Emrem Bestepe, Nazlı Tunali, Gökçe Elif Sarıdoğan
Department of Psychiatry, Erenkoy Mental Health and Neurological Diseases Training and Research Hospital, University of Health Sciences, Istanbul, Turkey
Correspondence: Gökçe Elif Sarıdoğan
Department of Psychiatry, Erenkoy Mental Health and Neurological Diseases Training and Research Hospital, University of Health Sciences, Sinan Ercan Cad. No: 23 Kazasker, Istanbul 34736, Turkey
Tel +90 532 503 27 97
Email [email protected]
Background and Objectives: Compliance and maintenance of abstinence is a major issue in substance use disorders. Adverse effects of opioid maintenance treatments (OMT) include sexual dysfunctions. There is a vast amount of studies regarding sexual adverse effects of conventional OMTs; however, information regarding buprenorphine/naloxone (Bup/Nal) combination is limited, mostly evaluated in western populations and controversial. In this study, we aimed to assess the sexual adversities of Bup/Nal treatment in a Turkish alcohol and substance use disorder treatment center sample.
Materials and Methods: We recruited 100 subjects continuing sublingual Bup/Nal combination and 35 control subjects. Subjects were evaluated via the the Golombok-Rust Inventory of Sexual Satisfaction (GRISS) for sexual dysfunction and for erectile dysfunction (ED) with the International Index of Erectile Function-5 (IIEF-5) as a comparison.
Results: The mean dose of our treatment was 9.05. Overall sexual dysfunction scores were not significantly different in between groups with GRISS. ED and noncommunication scores were significantly higher in the Bup/Nal treatment group than the control group (p = 0.002, p = 0.02, respectively). Along with the increased ED scores in GRISS, IIEF-5 total scores also revealed more significant severity of the ED in the Bup/Nal group (p = 0.001).
Conclusion: Buprenorphine/naloxone combination lead to a higher degree of ED severity than the non-treatment controls. Noncommunication seems to play a role as a risk factor for ED in patients with opioid use disorder. Thus, effective communication can be a key factor for sexual assertivity and disclosing the sexual adverse effects to the clinicians as well as staying in the treatment.
Keywords: buprenorphine maintenance, Turkey, substance-related disorders, men, methadone
Introduction
Buprenorphine/naloxone (Bup/Nal) is a semisynthetic opioid which was initially developed (Suboxone® [Reckitt Benckiser Pharmaceuticals Incorporation, Richmond, VA]) as an analgesic which has been effectively in use for OMT since 2003 after approval by the Food and Drug Administration (FDA) in 2002.1,2 In Turkey Bup/Nal was introduced as the first OMT in 2010 since methadone was not legally available.
Buprenorphine is a mu (µ) and a kappa (ƙ) partial agonist and an antagonist at the gamma (ɣ) opioid receptors possessing a greater margin of safety than conventional full agonists as well as yielding less severe withdrawal symptoms. Bup/Nal emerged in an attempt to reduce the addiction profile if injected or crushed by combining buprenorphine with naloxone in a 4/1 ratio.3,4 The maintenance dose of sublingual Bup/Nal ranges between 4/1 mg to 24/6 mg depending on the response of the patient, while the induction dose is initially between 4/1 mg to 8/2 mg with required increments at two-hour intervals.5 Recommended dose for Bup/Nal maintenance on average is 16/4 mg.6 Bup/Nal maintenance has mostly tolerable adverse effects including abdominal pain, constipation, changes in appetite, nausea, headaches, insomnia, anxiety, sweating, muscle pain.7 Opioid substitutes are also reported to cause loss of sexual desire and erectile dysfunction (ED).8,9 A wide range of sexual dysfunction rates, 14% to 81%, for the full µ opioid receptor agonist methadone, have been reported throughout different studies.10 Despite the widely reported sexual adverse effects of methadone maintenance treatment (MMT), data concerning Bup/Nal treatment is limited and controversial.11
The results of the studies comparing the sexual adverse effects of buprenorphine maintenance treatment (BMT) and MMT were found to be controversial as well.10 Considering the limitations in some of these studies (eg, small sample sizes, lack of control group) there is a need to perceive more on the subject.12–14
Erectile dysfunction (ED) is one of the most common adverse sexual effect of OMT. ED is known to cause a decrease in patients’ overall quality of life leading to treatment discontinuation and resuming substance use.15 Due to the fact that disclosure of sexual adverse effects are well-known to be challenging in the clinical settings, medication induced secondary sexual dysfunctions are among the frequent reasons of unreported spontaneous noncompliance. In addition, ED leads to decreased self-esteem and a gross obstacle to overall treatment success.16 Enhancing awareness of physicians about association of poor treatment compliance and unexpected relapses following medication induced sexual dysfunction in patients with substance use disorder is of major importance.17
The present study aimed to evaluate the sexual adverse effects of buprenorphine/naloxone combination in comparison with a control group in a Turkish sample. We conceive that it is essential to further address and abate the limitations of the existing literature and to draw the attention of clinicians to the extent of the sexual adverse effects of Bup/Nal treatment in opioid use disorder.
Materials and Methods
A cross-sectional, descriptive study was conducted among 135 participants who applied to Erenkoy Mental Health and Neurological Research Hospital, Alcohol and Substance Use Disorder Treatment Center, between 2014 to 2020. The hospital is a foremost tertiary institution on the Asian side of Istanbul and in the Marmara geopolitical zone which receives referrals from the other clinical units within the hospital and primary and secondary health care facilities, from within and outside the city borders.
Sampling
The sample size was calculated accordingly to meet the necessary requirements of a cross-sectional study. The participants in the study comprised of 100 patients on buprenorphine/naloxone monotherapy for at least one month and 35 individuals as control subjects in the study. Patients collected from the Alcohol and Substance Use Disorder Treatment Center outpatient clinic were involved in the Bup/Nal maintenance treatment program and were free from opioid use (confirmed by urine chromatographic immune assay). The individuals of the control group were nonblood-related caregivers/visitors of patients attending the hospital, who were not regular users of any psychoactive substance except tobacco and alcohol on social occasions. There was no alternative legally available other opioid maintenance pharmacological treatment option such as methadone before the onset of our study in Turkey. For ethical reasons, we recruited the control group among individuals who are not opioid treatment patients since it is not suitable to leave patients untreated. An initial interview was made by a psychiatrist in order to appropriately recruit the subjects to the study by the preformed criteria.
Inclusion and Exclusion Criteria for Inclusion
Males who are sexually active, aged between 18 and 45, diagnosed with substance use disorder according to DSM-5, currently on Bup/Nal monotherapy and fluent in speaking and writing the Turkish language were included; whereas subjects who had ongoing psychotic symptoms, intellectual disability, cognitive dysfunction, and severe medical illness preventing the patient from participating in the interview were excluded. Also excluded were those with regular use of medications to treat sexual dysfunctions (such as phosphodiesterase inhibitors).
Ethical Considerations
All participants were informed about the study and that participation in this study was voluntary and their information would be kept confidential.
The study was approved by the Local Ethics Committee of Erenkoy Mental Health and Neurological Research Hospital and voluntary and informed consent was obtained from each participant before the study was conducted and complete privacy was assured. Our study was conducted in accordance with Declaration of Helsinki.
Measures
A demographic data form was given to each participant. Questions included general socio-demographic data, sexual and relationship information and treatment and clinical variables. All questionnaires were self-administered. We assessed the sexual dysfunction with two cross-culturally validated instruments: Golombok Rust Inventory of Sexual Satisfaction (GRISS) and International Index of Erectile Function-5 (IIEF-5).
The Golombok-Rust Inventory of Sexual Satisfaction (GRISS) male version is a five-choice (Likert type) scale that has 28-items for assessing the existence and severity of sexual problems in men.18 It provides total scores, as well as subscale scores. The subscales consist of infrequency, nonsensuality, avoidance, dissatisfaction, noncommunication, impotence, and premature ejaculation. Both the total and subscale scores can be used for evaluation and the high scores on a particular item or subscale show the deterioration in the quality of the sexual relationship and in sexual functioning. GRISS was standardized and shown to be a reliable and a valid tool for assessing sexual dysfunction in the Turkish population.19 The International Index of Erectile Function (IIEF-5) is a scale for evaluating the presence and the severity of ED in men.20 Turkish validation is done by Turunc et al.21
Statistical analyses were performed using the SPSS v23.0 statistical software package. Continuous data are expressed as mean ± standard deviation while categorical data are presented as number and percentage of patients. The χ2 test and the Fisher exact test were used for the comparison of categorical variables while the Student t-test was used to compare parametric variables and nonparametric with the Mann–Whitney U-test, respectively. The homogeneity of variances was analyzed with the Levene’s test. One-way Mancova was used to perform multiple covariates analysis. Pillal’s trace was used for the multivariate tests. Correlation analysis was performed using the Spearman’s p correlation coefficient. A value of p<0.05 was considered statistically significant.
Results
A total of 135 questionnaires were administered and retrieved. None of the questionnaires were rejected because of bad filling. Opioid use patients, constituting a total of 100 subjects who are not using heroin for at least one month and on Bup/Nal treatment, were recruited for the study group and 35 controls who had never used opioids and were not on Bup/Nal treatment were analyzed in comparison. In the Bup/Nal group 47% (N = 47) were workers, 38% (N = 38) were self-employed, 1% (N = 1) were students and none were civil servants. In the control group, 54.3% (N = 19) were workers, 5.7% (N = 2) were self-employed, 37.1% (N = 13) were civil servant, and none were students. Patient characteristics by sociodemographic variables are shown in Table 1.
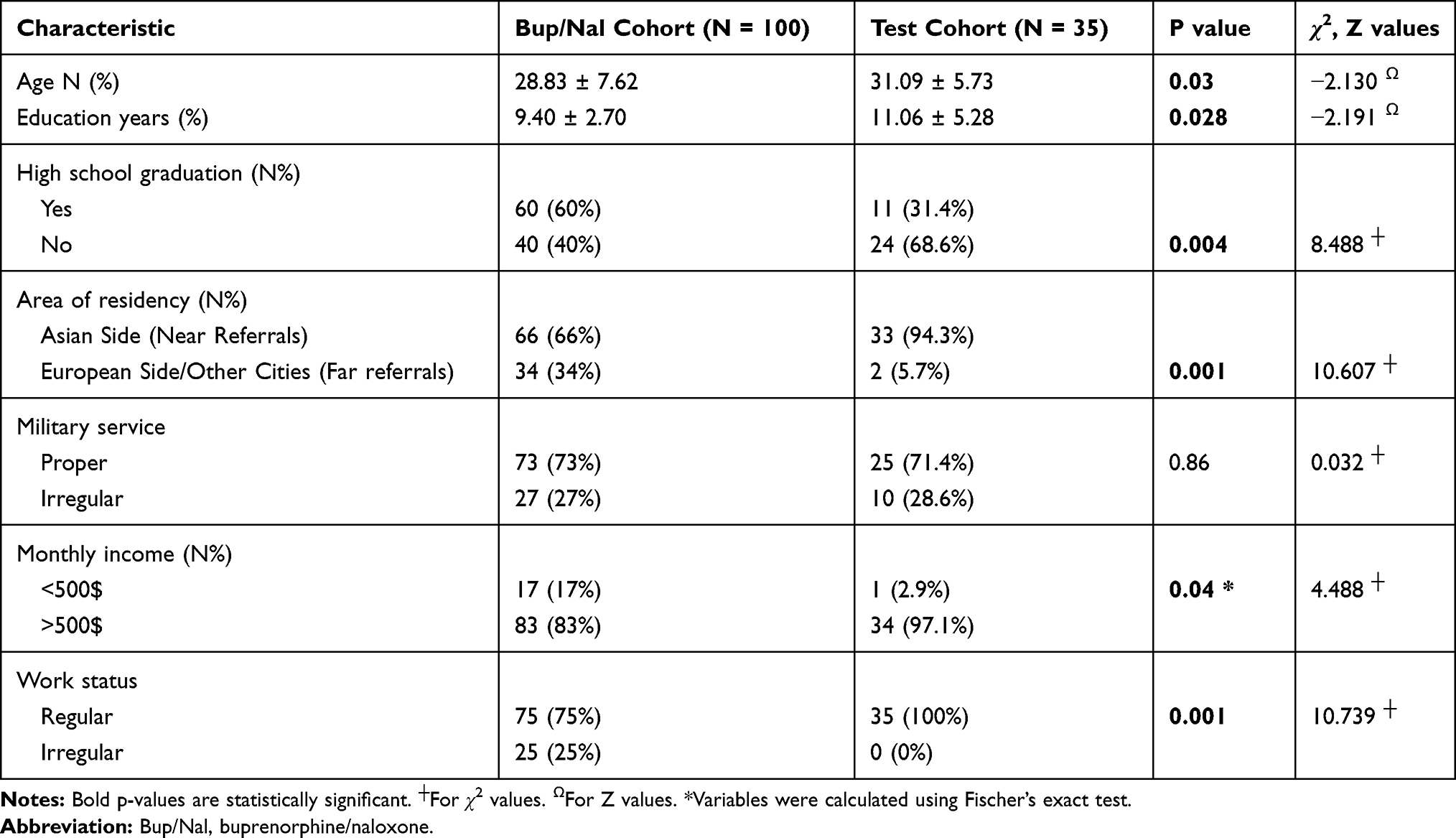 |
Table 1 Patient Characteristics by Sociodemographic Variables |
In our Bup/Nal group, distribution of the initial substance that was used was found to be 73%(N = 73) cannabis and cannabinoids, 13% (N = 13) heroin, 6% (N = 6) inhalants, 4% (N = 4) stimulants, 2% (N = 2) benzodiazepines, 1% (N = 1) alcohol and 1% (N = 1) medical drug use. The distribution of the psychiatric diagnoses were as follows; 16% (N = 16), 4% (N = 4), 4% (N = 4), 3% (N = 3) of the Bup/Nal group had major depressive disorder, anxiety disorder, personality disorder, and other unspecified psychiatric disorders, respectively. While 2.9% (N = 1), 2.9% (N = 1), 0% (N = 0), 0% (N = 0) had major depressive disorder, anxiety disorder, personality disorder, other unspecified psychiatric disorders, respectively, in the control group. In the Bup/Nal group 11%(N = 11) of the participants had been admitted to inpatient clinic. This ratio was 0%(N = 0) in the control group (Table 2).
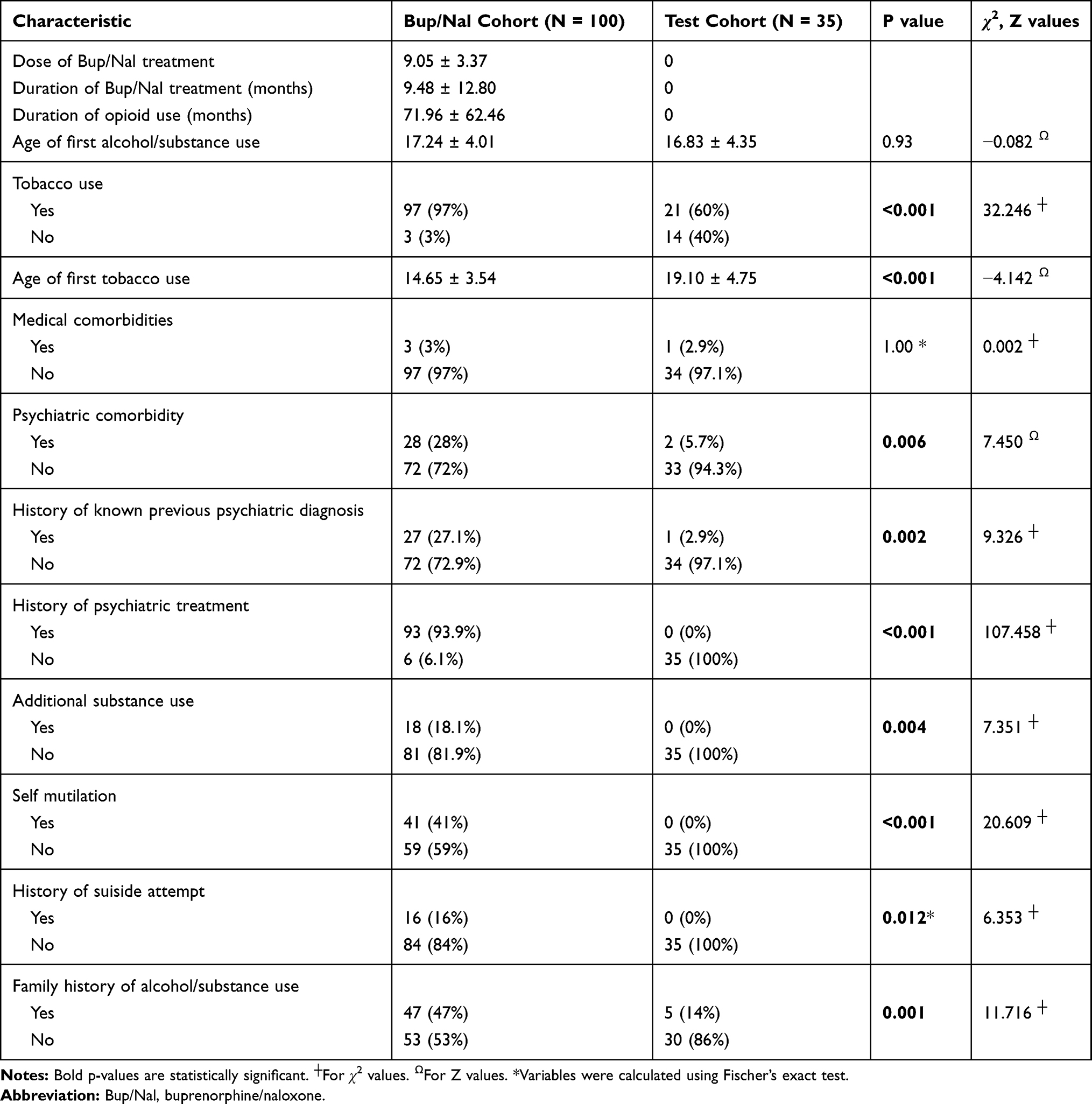 |
Table 2 Patient Characteristics by Opioid/Treatment and Medical Variables |
In our Bup/Nal group the history of sexually transmitted diseases (STD) are as follows; HBV 4% (N = 4), HCV 8% (N = 8), gonorrhea 3% (N = 3), other STDs 2% (N = 2). None of the participants had HIV. We also assessed same sexual behavior under substance influence and found that only nonheterosexual participants were involved in same sex behavior under the influence of a substance (Table 3).
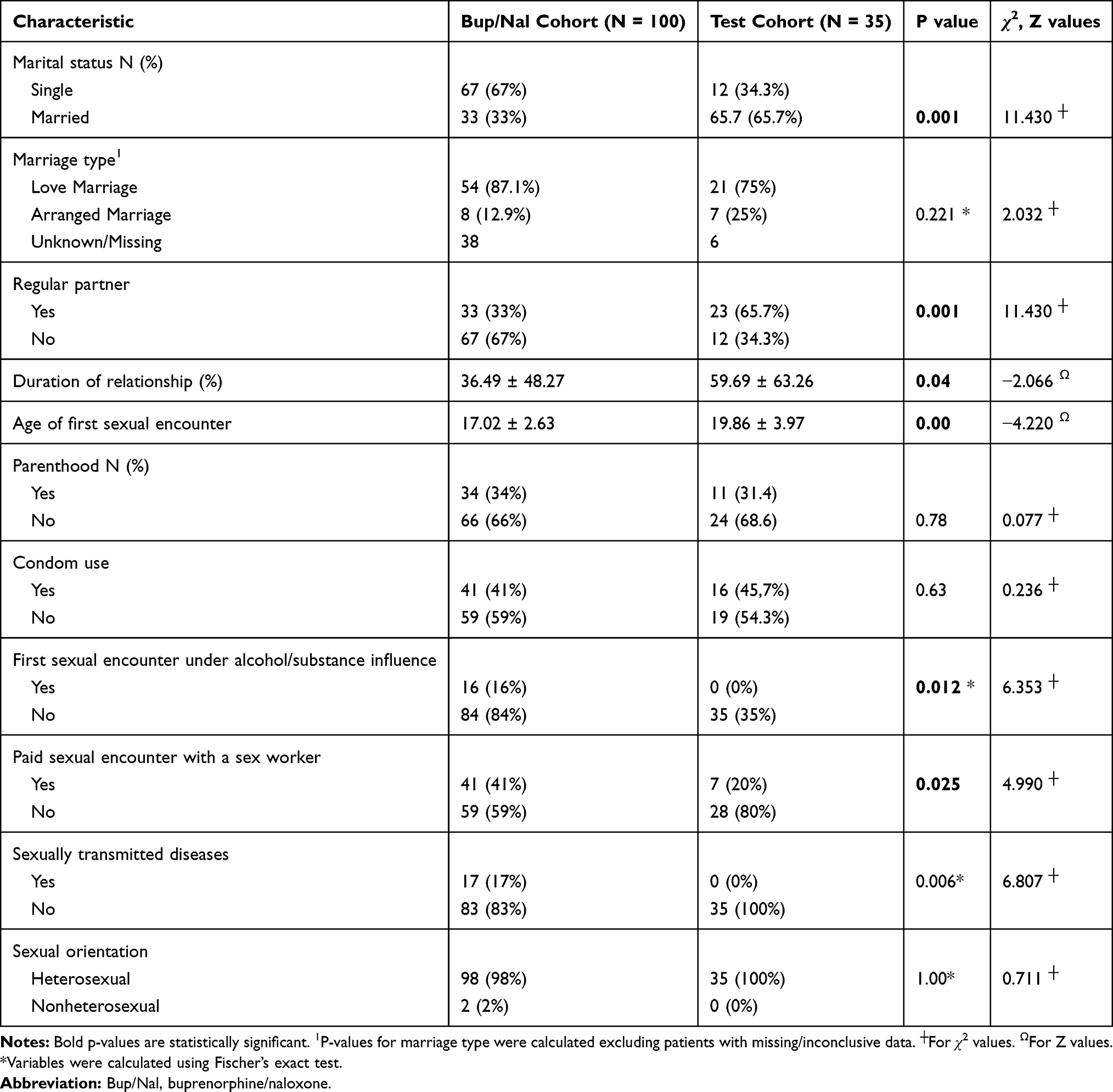 |
Table 3 Patient Characteristics by Relational Sexual/Relationship Variables |
The total and subscale scores of GRISS and IIEF-5 of the groups are shown in Table 4 and the correlations between GRISS subscales and IIEF-5 are shown in Table 5. When the sexual dysfunction measures were evaluated according to tobacco use, there was no significant difference in IIEF-5 and GRISS total scores and the subscales of the GRISS; apart from the noncommunication subscale of GRISS (p = 0.014, χ2= 6.030). According to the paid sexual encounter with sex worker parameter, there was no significant difference in IIEF-5 and GRISS total scores as well as GRISS subscales (p < 0.005 for all scales and subscales). When comparison was done according to medical comorbidities that might cause sexual dysfunction, there was no significant difference among the two groups in all scales and subscales (p > 0.05). When the same comparison was done for the additional psychiatric comorbidities there was no significant difference in the total scores of GRISS and its subscales; however, in the IIEF-5 total score, patients with additional psychiatric comorbidities were observed to score less and this finding was statistically significant indicating a statistically higher tendency to experience erectile problems (p = 0.02, Z = −2.346). We found no significant difference between the two groups according to marriage styles, parenthood, condom use, having a regular partner when IIEF-5 and GRISS total and subscales are analyzed (p < 0.05). When we compared the sexual functioning according to marriage status there was no significant difference in between all the sexual majors but the infrequency subscale (p = 0.004,Z = −2.865).
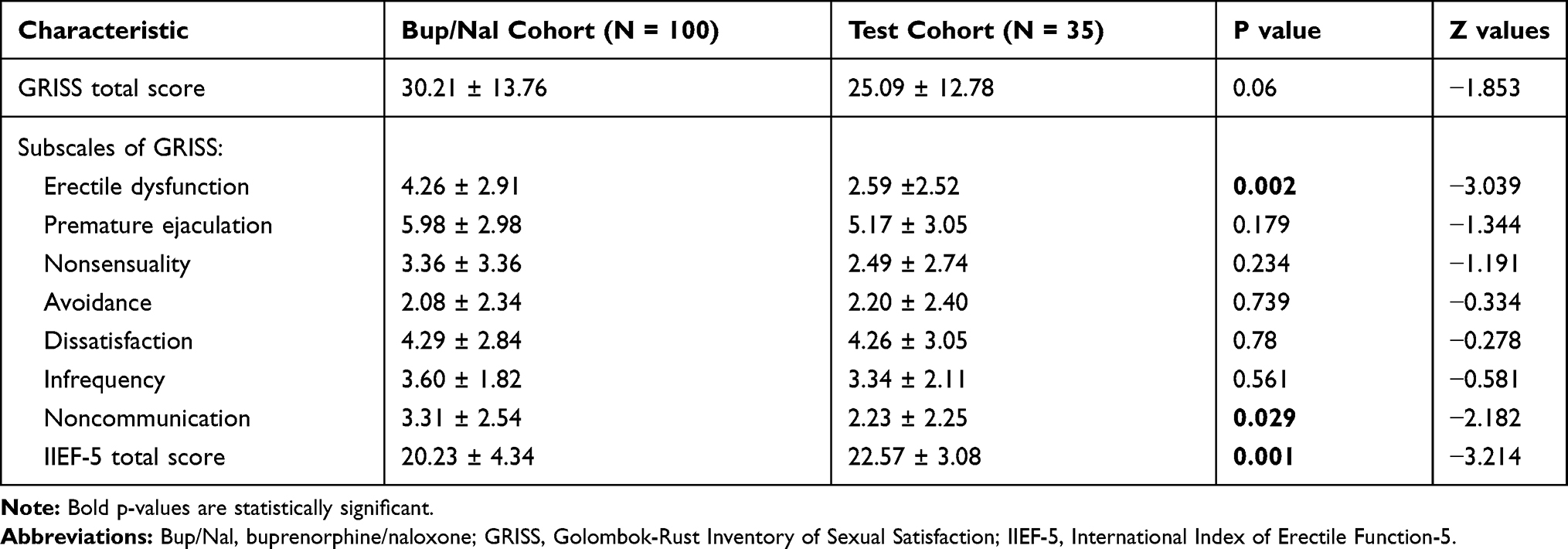 |
Table 4 GRISS and IIEF-5 Scores |
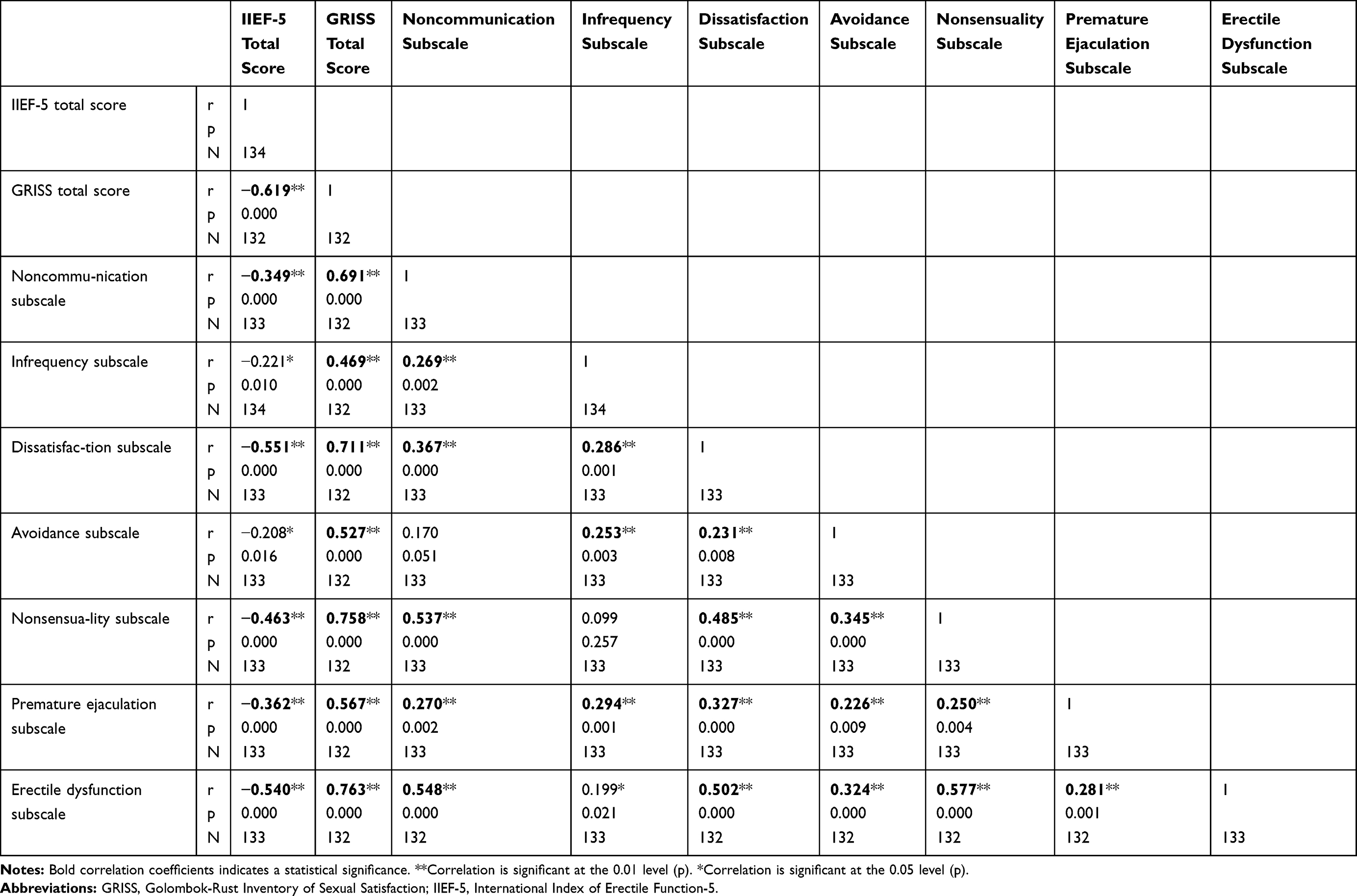 |
Table 5 Correlations |
After covariate analyses, having a regular partner was not significantly related to the IIEF-5, GRISS total, and GRISS subscales apart from infrequency subscale scores [F(1128) = 5.71, p = 0.018]. However, there was no significant effect of partner status on levels of infrequency subscale [F(1128) = 2.13, p = 0.15]. Having a regular partner was not significantly related to the GRISS erectile dysfunction subscale scores [F(1128) = 0.124, p = 0.73] and IIEF-5 total scores [F(1128) = 1.018, p = 0.315]. Bup/Nal treatment was found to be significantly related to significantly increased scores of erectile dysfunction subscale (p = 0.005) and significantly decreased IIEF-5 total scores (p = 0.005). No other significance was observed among the scales and subscales after controlling for partner status. After covariate analyses were done for medical comorbidities, there was significant effect for IIEF-5 total scores [F(1128) = 5.95, p = 0.016]. There was also a significant effect of medical comorbidities on levels of IIEF-5 total scores after controlling for the effect of comorbid medical illnesses [F(1128) = 8.507, p = 0.004]. However, IIEF-5 total scores showed a statistically significant decrease when compared to the control group after controlling for medical comorbidities. IIEF-5 total scores were decreased (p = 0.042), noncommunication (p = 0.014), and erectile dysfunction scores were increased (p = 0.002)
Discussion
Despite the widely researched sexually adverse effect of conventional opioid maintenance treatments there are a very limited number of studies regarding sexual dysfunction related to Bup/Nal treatment.12,14,22,23 Hence this study is one of the few studies related to the sexual effects of Bup/Nal combination in the field. In this context, previously two remarkable studies focused on the sexually adverse effects of Bup/Nal maintenance therapy. Dhawan et al, reported the mean dose of Bup/Nal in their study as 5.9±2.4.24 The study by Mattoo et al reported an average dose of 4.5±1.7.11 In our study, the average Bup/Nal dose in the treatment group was very close to the average of our clinic, which is approximately 10 mg.
Among the studies assessing the prevalence of sexual dysfunctions in patients who were treated with OMT, a previous study indicated that overall sexual dysfunction was differing between 30–100%.25 The average rate of prevalence among remarkable published studies changes between 16.0–83.6%.26–29 Conspicuously, many studies have reported ED as a more frequent adverse effect of those agents, with reported rates ranging between 16% to 83.6%.10,26,27 Ejaculatory difficulties, and decreased desire for sexual activity were observed in a considerable sample of men on MMT.23,29–33 Ramburg et al’s study, which is one of the limited number of buprenorphine studies, pointed out that buprenorphine was also related to at least one type of sexual dysfunction. In this study 83% of the participants reported premature ejaculation, 43% reported ED, and 33% reported decrease in sexual desire.23
On the other hand, not all studies report negatively correlated results and indicate controversial findings. A meta-analysis from 2014 showed that with partial agonist, BMT resulted in less sexual adverse effects in men when compared to the conventional MMT.10 There are other studies which concluded that partial agonist buprenorphine causes lower degrees of ED severity and a lower risk than the full agonist methadone.10,12–14 Cioe et al suggested that with buprenorphine treatment there was amelioration of ED symptoms in 3 months in previous opioid users, decreasing the adverse effect severity making buprenorphine a potential treatment option to decrease sexual adverse effects in opioid users who use full agonists.35 There are also publications that demonstrated no significant difference in sexual adverse events between methadone and buprenorphine maintenance treatments.14,35 However, the behavior of buprenorphine on sexual functioning still needs to be clarified in more detail.13,14
In our study ED was the most significantly affected dimension among the measured sexual dysfunctions. Previous studies reported different rates of particular sexual adverse effects due to Bup/Nal treatment. According to a recent study with opioid use disorder patients, ED was the third most common sexual dysfunction (77.5%), after hypoactive sexual desire (92.5%) and intercourse dissatisfaction (95%) in patients treated with Bup/Nal combination treatment.11 In meta-analysis comparing studies of methadone and buprenorphine-based treatments, hypoactive sexual desire was shown to be the most abundant symptom.10 Another meta-analysis confirmed that prevalence of ED was more common (relative risk = 1.96; 95% CI:1.66–2.32) in chronic treatment congruent with the past research findings.36
In the study of Mattoo et al, authors did not find any significance of sexual dysfunction with any of the clinical variables and the sociodemographic data.11 In our study, noncommunication subscale of GRISS was found to be associated with comorbid psychiatric illness and tobacco use disorder but not associated with medical comorbidities and condom use. Being single was found to be associated with higher infrequency scores among the GRISS subscales. Quaglio et al demonstrated that living together with a regular sexual partner was found to be a protective factor for ED, and not having a regular partner increased the likelihood of ED.14 In our study, we assessed marriage and having a regular sexual partner as two different dimensions. Neither having a regular sexual partner nor marriage status showed association with sexual dysfunction.
Donatucci and Lue demonstrated that substance use disorder in men before 40 years of age is one of the most common risk factors for ED.37 In our study we also assessed the sexual dysfunctions among younger men (<45 years old) in order to avoid the confounding comorbidity rates. It was also reported that over the age of 45, ED is found to be increased by 11.3% each year.38 Quaglio et al also reported in a cross-sectional study that 42% of male participants reported symptoms of ED when they were on OMT.14 Literature also indicates that ED severity increases with long-term treatment with an opioid agonist. In the mentioned study mean duration of opioid treatment use was 48.8 months.14,39 In our Bup/Nal group, the mean duration of opioid treatment was 9.48 months however there was a significant increase in ED despite the much shorter average duration of treatment in our study. On the other hand, opioid use duration in our treatment group was 71.96 months. This finding indicates a previous long-term opioid use despite of the cessation of heroin, in contrast to aforementioned studies.
Our findings indicated that degree of disturbed erectile functioning was higher in our treatment group by the GRISS erectile dysfunction subscale. This finding was also supported by the IIEF-5 as a significant decreased capacity in the erectile functioning. Evidence demonstrated that full opioid agonists (such as methadone) increase the prevalence of ED more significantly than the partial agonist buprenorphine.10 Despite the shorter duration but higher dose of Bup/Nal, our study indicates that Bup/Nal caused a respectable decrease in the erectile function, that could be classified as mild severity according to IIEF-5 classification compared to within normal mean erectile functioning in the control group. Another study by Gerra et al similarly demonstrated that ED is a consequence of long-term opioid receptor stimulation indicating a correlation between the opioid receptor and erectile functioning.40
We aimed to assess the severity of the sexual adversities in our study between the treatment and control groups. We did not use the GRISS pseudostanine conversion ratings as the system is based on evaluation of narrators as an alternative diagnostic tool. In addition, we found no significant difference among the treatment and control groups in terms of sexual dysfunction severity apart from ED. Thus, we evaluated the rising parameter, ED, with another detailed designed tool specifically for ED called IIEF-5.
We found that the noncommunication subscale of GRISS was also affected more in the Bup/Nal group than the control group. We also assessed if the comorbid disorders of the patients carry a potential risk for sexual dysfunctions. In our sample there was no significant difference between the treatment and control groups for the rates of comorbid physical health problems. We found no significant association of these physical health problems as well as tobacco use with sexual functioning in our comparison both by GRISS and IIEF-5 between the treatment and control groups. Nevertheless, we found a significant difference in noncommunication in our sample of patients with comorbid psychiatric disorder, as well as with tobacco use, hence asserting a communicative style might be both affected in opioid use disorder and mental health problems. Thus, noncommunication may constitute a common psychological risk factor or an etiological reason both for mental health problems, opioid use disorder, tobacco use disorder and problems in sexual functioning. Initiation sexual assertiveness, which is related to sexual functioning, was found to be impaired in drug users.41 Another comparative study by the same authors reported that opioid users had the worst sexual functioning among illicit drug users, supporting other previous research.42–44 Sexual communication, aspects of assertive communication, their correlation with opioid and drug use disorders and its effect on relapses are recommended to be further evaluated.
There are limitations of this study. First, our control group does not have opioid use disorder history. This might influence the relationship status and outcomes as well as marital status differences between the groups. The sample size of our control group is smaller than the treatment group because we had difficulty in recruiting the control group due to healthy controls’ reluctance to participate in the study because of social oppression and stigmatization over disclosure of male sexual problems in healthy men in Turkish culture. In addition, the patient characteristics differed most probably due to opioid use disorder history in the treatment group. Another limitation of our study is that this study does not discriminate between baseline pretreatment sexual dysfunctions with the posttreatment outcomes which can be further addressed in the future research. Both groups were informed that the study is designed to evaluate the sexual adverse effects. Additionally, we assessed sexual adverse effects only in men. Future studies are advised to be designed in order to evaluate both male and female counterparts. This study is advised to be conducted in older men to address their specific risks and needs. According to our findings noncommunication is a major issue for sexual functionality in the Bup/Nal treatment group who also have opioid use disorder history. This finding needs to be assessed further for the sexual functioning in opioid use disorder, other substance use disorders and its relevance with other psychiatric comorbidities. Assertiveness as a strong possible causality should be further addressed to clarify the etiological commonalities between substance use disorders, sexual dysfunction and relational difficulties.
Conclusion
Our findings indicate that participants who were treated with the Bup/Nal protocol had higher levels of ED as assessed by GRISS and IIEF-5. In our sample ED was the only significant sexual dysfunction under Bup/Nal treatment. On the other hand the GRISS subscale non-communication related to sexual communication and assertiveness were found to be impaired in the Bup/Nal group participants who had opioid use disorder as well as in participants with tobacco use disorder and psychiatric comorbidity underlining a possible common cognitive behavioral explanation for sexuality, substance use disorder and mental illness.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Chen KY, Chen L, Mao J. Buprenorphine-naloxone therapy in pain management. Anesthesiology. 2014;120(5):1262–1274. doi:10.1097/ALN.0000000000000170
2. Johnson RE, Strain EC, Amass L. Buprenorphine: how to use it right. Drug Alcohol Depend. 2003;70(2Suppl):S59–S77. doi:10.1016/s0376-8716(03)00060-7
3. Woody GE, Poole SA, Subramaniam G, et al. Extended vs short-term buprenorphine-naloxone for treatment of opioid-addicted youth: a randomized trial. JAMA. 2008;300(17):2003–2011. doi:10.1001/jama.2008.574
4. Yee A, Loh HS, Loh HH, Riahi S, Ng CG, Sulaiman AHB. A comparison of sexual desire in opiate-dependent men receiving methadone and buprenorphine maintenance treatment. Ann Gen Psychiatry. 2019;18(1):25. doi:10.1186/s12991-019-0249-z
5. Velander JR. Suboxone: rationale, science, misconceptions. Ochsner J. 2018;18(1):23–29.
6. Purdue Pharma, Inc. Prescribing information: BUTRANS (buprenorphine) transdermal system. [cited 2014, Jun 6]; Available from: http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/021306s001s003lbl.pdf, archived at http://www.webcitation.org/6VLVR73Qd.
7. Can Y, Mutlu E, Karabulut V, Demirci AÇ, Umut G, Çetin T. Maintanence treatment in opioid dependency. Dusunen Adam. 2012;25:90. doi:10.5350/DAJPN2011250114
8. Ajo R, Segura A, Inda MD, et al. Erectile dysfunction in patients with chronic pain treated with opioids. Disfunción eréctil en pacientes con dolor crónico tratados con opioides. Med Clin (Barc). 2017;149(2):49–54. doi:10.1016/j.medcli.2016.12.038
9. Baykara S, Alban K. The effects of buprenorphine/naloxone maintenance treatment on sexual dysfunction, sleep and weight in opioid use disorder patients. Psychiatry Res. 2019;272:450–453. doi:10.1016/j.psychres.2018.12.153
10. Yee A, Loh HS, Hisham Hashim HM, Ng CG. The prevalence of sexual dysfunction among male patients on methadone and buprenorphine treatments: a meta-analysis study. J Sex Med. 2014;11(1):22–32. doi:10.1111/jsm.12352
11. Mattoo SK, Ghosh A, Subodh BN, et al. Sexual dysfunction in men on buprenorphine - naloxone-based substitution therapy. Indian J Psychiatry. 2020;62(1):66–72. doi:10.4103/psychiatry.IndianJPsychiatry_195_19
12. Yee A, Danaee M, Loh HS, Sulaiman AH, Ng CG. Sexual dysfunction in heroin dependents: a comparison between methadone and buprenorphine maintenance treatment. PLoS One. 2016;11(1):e0147852. doi:10.1371/journal.pone.0147852
13. Hallinan R, Byrne A, Agho K, McMahon C, Tynan P, Attia J. Erectile dysfunction in men receiving methadone and buprenorphine maintenance treatment. J Sex Med. 2008;5(3):684–692. doi:10.1111/j.1743-6109.2007.00702.x
14. Quaglio G, Lugoboni F, Pattaro C, et al. Erectile dysfunction in male heroin users, receiving methadone and buprenorphine maintenance treatment. Drug Alcohol Depend. 2008;94(1–3):12–18. doi:10.1016/j.drugalcdep.2007.09.025
15. Chen W, Li X, Li X, et al. Erectile dysfunction among male heroin addicts receiving methadone maintenance treatment in Guangdong, China. J Addict Med. 2012;6(3):212–218. doi:10.1097/ADM.0b013e318259b2c4
16. Osasona SO, Ehimigbai M. Sexual dysfunction: prevalence and associated factors in patients with mental illness receiving psychotropic medication in Nigeria. Afr Health Sci. 2019;19(4):2973–2984. doi:10.4314/ahs.v19i4.18
17. Grover S, Mattoo SK, Pendharkar S, Kandappan V. Sexual dysfunction in patients with alcohol and opioid dependence. Indian J Psychol Med. 2014;36(4):355–365. doi:10.4103/0253-7176.140699
18. Rust J, Golombok S. The GRISS: a psychometric instrument for the assessment of sexual dysfunction. Arch Sex Behav. 1986;15(2):157–165. doi:10.1007/BF01542223
19. Tuğrul C, Öztan N, Kabakçı E. Golombok-Rust cinsel doyum ölçegi’nin standardizasyon çalışması. [Standardization of Golombok-Rust sexual satisfaction inventory]. Turk Psikiyatri Derg. 1993;4(2):83–89.
20. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM. Development and evaluation of an abridged, 5-item version of the international index of erectile function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11(6):319–326. doi:10.1038/sj.ijir.3900472
21. Turunç T, Deveci S, Güvel S, Peşkircioǧlu L. Uluslararası cinsel işlev indeksinin 5 soruluk versiyonunun (IIEF-5) türkçe geçerlilik çalışmasının değerlendirilmesi. [The assessment of Turkish validation with 5 question version of international index of erectile function (IIEF-5)]. Turk Uroloji Dergisi. 2007;33:45–49.
22. Cioe PA, Friedmann PD, Stein MD. Erectile dysfunction in opioid users: lack of association with serum testosterone. J Addict Dis. 2010;29(4):455–460. doi:10.1080/10550887.2010.509279
23. Ramdurg S, Ambekar A, Lal R. Sexual dysfunction among male patients receiving buprenorphine and naltrexone maintenance therapy for opioid dependence. J Sex Med. 2012;9:3198–3204.
24. Dhawan A, Chopra A. Does buprenorphine maintenance improve the quality of life of opioid users? Indian J Med Res. 2013;137(1):130–135.
25. Brown R, Balousek S, Mundt M, Fleming M. Methadone maintenance and male sexual dysfunction. J Addict Dis. 2005;24:91–106.
26. Déglon -J-J, Martin J-L, Imer RL. Methadone patients’ sexual dysfunctions: clinical and treatment issues. Heroin Addict Relat Clin Probl. 2004;6:17–26.
27. Bai XLN, Jia W, Zhang X. Study on sexual function of male MMT patients. Chin J Drug Abuse Prev Treat. 2009;15:158–160.
28. Teusch L, Scherbaum N, Böhme H, Bender S, Eschmann-Mehl G, Gastpar M. Different patterns of sexual dysfunctions associated with psychiatric disorders and psychopharmacological treatment. Results of an investigation by semistructured interview of schizophrenic and neurotic patients and methadone-substituted opiate addicts. Pharmacopsychiatry. 1995;28(3):84–92. doi:10.1055/s-2007-979596
29. Hanbury R, Cohen M, Stimmel B. Adequacy of sexual performance in men maintained on methadone. Am J Drug Alcohol Abuse. 1977;4(1):13–20. doi:10.3109/00952997709002743
30. Lafisca S, Bolelli G, Franceschetti F, Filicori M, Flamigni C, Marigo M. Hormone levels in methadone-treated drug addicts. Drug Alcohol Depend. 1981;8(3):229–234. doi:10.1016/0376-8716(81)90066-1
31. Daniell HW. Narcotic-induced hypogonadism during therapy for heroin addiction. J Addict Dis. 2002;21(4):47–53. doi:10.1300/J069v21n04_05
32. La Pera G, Carderi A, Marianantoni Z, Peris F, Lentini M, Taggi F. Sexual dysfunction prior to first drug use among former drug addicts and its possible causal meaning on drug addiction: preliminary results. J Sex Med. 2008;5(1):164–172. doi:10.1111/j.1743-6109.2007.00571.x
33. Xia Y, Zhang D, Li X, et al. Sexual dysfunction during methadone maintenance treatment and its influence on patient’s life and treatment: a qualitative study in South China. Psychol Health Med. 2013;18(3):321–329. doi:10.1080/13548506.2012.729845
34. Cioe PA, Anderson BJ, Stein MD. Change in symptoms of erectile dysfunction in depressed men initiating buprenorphine therapy. J Subst Abuse Treat. 2013;45(5):451–456. doi:10.1016/j.jsat.2013.06.004
35. Bliesener N, Albrecht S, Schwager A, Weckbecker K, Lichtermann D, Klingmüller D. Plasma testosterone and sexual function in men receiving buprenorphine maintenance for opioid dependence. J Clin Endocrinol Metab. 2005;90(1):203–206. doi:10.1210/jc.2004-0929
36. Zhao S, Deng T, Luo L, et al. Association between opioid use and risk of erectile dysfunction: a systematic review and meta-analysis. J Sex Med. 2017;14(10):1209–1219. doi:10.1016/j.jsxm.2017.08.010
37. Donatucci CF, Lue TF. Erectile dysfunction in men under 40: etiology and treatment choice. Int J Impot Res. 1993;5(2):97–103.
38. Weber MF, Smith DP, O’Connell DL, et al. Risk factors for erectile dysfunction in a cohort of 108 477 Australian men. Med J Aust. 2013;199(2):107–111. doi:10.5694/mja12.11548.
39. Teoh JB, Yee A, Danaee M, Ng CG, Sulaiman AH. Erectile dysfunction among patients on methadone maintenance therapy and its association with quality of life. J Addict Med. 2017;11(1):40–46. doi:10.1097/ADM.0000000000000267
40. Gerra G, Manfredini M, Somaini L, Maremmani I, Leonardi C, Donnini C. Sexual dysfunction in men receiving methadone maintenance treatment: clinical history and psychobiological correlates. Eur Addict Res. 2016;22(3):163–175. doi:10.1159/000441470
41. Santos-Iglesias P, Sierra JC, Vallejo-Medina P. Predictors of sexual assertiveness: the role of sexual desire, arousal, attitudes, and partner abuse. Arch Sex Behav. 2013;42(6):1043–1052. doi:10.1007/s10508-012-9998-3
42. Vallejo-Medina P, Sierra JC. Effect of drug use and influence of abstinence on sexual functioning in a Spanish male drug-dependent sample: a multisite study. J Sex Med. 2013;10(2):333–341. doi:10.1111/j.1743-6109.2012.02977.x
43. Bang-Ping J. Sexual dysfunction in men who abuse illicit drugs: a preliminary report. J Sex Med. 2009;6(4):1072–1080. doi:10.1111/j.1743-6109.2007.00707.
44. Aguilar de Arcos F, Verdejo-García A, Ceverino A, et al. Dysregulation of emotional response in current and abstinent heroin users: negative heightening and positive blunting. Psychopharmacology (Berl). 2008;198(2):159–166. doi:10.1007/s00213-008-1110-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.