Back to Journals » Journal of Pain Research » Volume 15
Sex-Specific Associations Between Preoperative Chronic Pain and Moderate to Severe Chronic Postoperative Pain in Patients 2 Years After Cardiac Surgery
Authors Liu J, Wang C, Gao Y, Tian Y, Wang Y, Wang S
Received 17 August 2022
Accepted for publication 5 November 2022
Published 19 December 2022 Volume 2022:15 Pages 4007—4015
DOI https://doi.org/10.2147/JPR.S384463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Jia Liu,1 Chunrong Wang,1 Yuchen Gao,1 Yu Tian,1 Yuefu Wang,2 Sudena Wang1
1Department of Anesthesiology, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, National Center of Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of Anesthesiology and Surgical Intensive Care Unit, Beijing Shijitan Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Yuefu Wang, Department of Anesthesiology and Surgical Intensive Care Unit, Beijing Shijitan Hospital, Capital Medical University, 10 Tieyi Road, Haidian District, Beijing, People’s Republic of China, Tel +86-10-88398082, Email [email protected]
Background and Purpose: Chronic postoperative pain (CPSP) after cardiac surgery can cause severe health problems. As demonstrated in noncardiac surgeries, preoperative chronic pain can potentially lead to CPSP. However, the association between preoperative chronic pain and CPSP over follow-up in cardiac surgical settings in the context of sex differences is still lacking. This observational study aims to explore the role and sex differences of preoperative chronic pain in the occurrence and development of long-term CPSP and CPSP-related complications after cardiac surgery.
Patients and Methods: This observational study enrolled 495 patients (35.3% women) who underwent cardiac surgery via median sternotomy in March 2019. Validated questionnaires were delivered to assess preoperative chronic pain and moderate to severe CPSP at 3 and 24 months following surgical procedures. The secondary outcomes included the occurrence of moderate to severe chronic pruritus, sleep disturbance, and daily activities interference at follow-up. Multivariable logistic regression was employed.
Results: Of 495 patients analyzed, the incidences of preoperative chronic pain (29.7% versus 20.6%) and moderate to severe CPSP (14.8% versus 8.1%) were both higher in females than males. Female sex (P = 0.048) and preoperative chronic pain (P = 0.008) were identified as significant risk factors for CPSP occurrence. However, preoperative chronic pain contributed significantly to CPSP (P = 0.008), sleep disturbance (P =0.047), and daily activities interference (P =0.019) in females, but not in males.
Conclusion: The 2-year prevalence of moderate to severe CPSP after cardiac surgery was 10.5%. Compared to males, females are more susceptible to CPSP and pain-related outcomes in the long term. In addition, preoperative chronic pain was associated with a higher risk of CPSP in females but not in males.
Keywords: cardiac surgery, chronic postoperative pain, preoperative chronic pain, sex differences
Introduction
Chronic postoperative pain (CPSP) and its related negative complications (pruritus, sleep disturbance, daily activities interference) are common after cardiac surgery. The incidence of CPSP after cardiac surgery via sternotomy varies from 3.8% to 60%, depending on the follow-up window, research methods, and the study population, whereas it decreases obtrusively over the years.1–3 It adversely threatens the quality of life and places a heavy burden on patient kin and society.4–7 Considering its detrimental health impact on the individual, further studies are warranted.
Preexisting chronic pain affects more than 30% of people worldwide.8,9 Chronic pain that is stimulated before surgery can lead to chronic stress,10 increased opioid use11 and central sensitization,12 and has a tendency to increase the likelihood of CPSP. Specifically, females are susceptible to accompanying preoperative chronic pain.9 Whereas, we hypothesized that sex differences in the association between preoperative chronic pain and CPSP. Several studies reported that, in cardiac surgery, preoperative intrinsic pain was a vital contributor to the development of subsequent chronic pain,1,2,7,13,14 however, only two studies included follow up periods of more than two years.1,2 Of note, there was no study aimed at investigating whether the relationship between preoperative chronic pain and CPSP in cardiac surgery differed by sex.
Understanding the role of gender in the relationship between preoperative chronic pain and CPSP will help to better understand the mechanism behind CPSP, optimize perioperative management, and reduce the incidence of postoperative chronic pain. Therefore, the primary aim of this observational study is to identify the role of preoperative chronic pain in the development of long-term CPSP and CPSP-associated complications following cardiac surgery with the exploration of sex differences.
Methods
Study Population
This study included adults who underwent cardiac surgery via median sternotomy at Fuwai Hospital, Chinese Academy of Medical Sciences, Beijing, China, in March 2019. This was an observational, single-center cohort study that was approved by the Institutional Review Board with waived written consent. The exclusion criteria included (1) emergency surgery; (2) mental illness and inability to communicate; (3) chronic chest pain prior to cardiac surgery; (4) American Society of Anesthesiologists (ASA) physical status VI; and (6) heart transplant. The flow chart is shown in Figure 1.
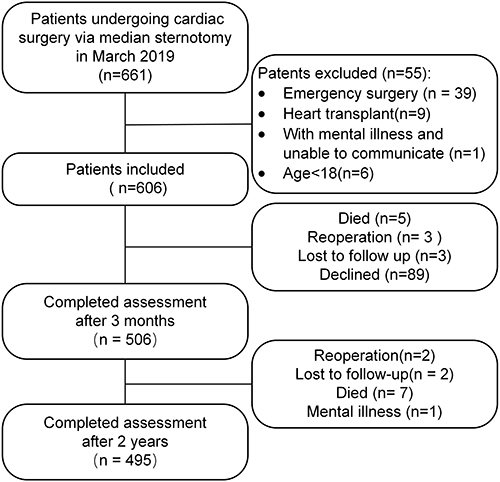 |
Figure 1 Participant flow through the study. |
Data Sources
Patient data were manually extracted from the electronic health records. Demographic characteristics (age, sex, body mass index, American Society of Anesthesiologists physical status, New York Heart Association), comorbidities (hypertension, diabetes mellitus), laboratory biomarkers (preoperative serum C-reactive protein, discharge white blood cell count), intraoperative information (the use of cardiopulmonary bypass, surgical time), and postoperative data (duration of mechanical ventilation, length of stay in hospital) were unanimously recorded in real time by medical personnel. Education level and employment status were collected via a demographic questionnaire. Other follow-up information (CPSP, postoperative chronic pruritus, sleep disturbance, and daily activities interference) was obtained via telephone interview.
Pain Assessment
Preoperative Chronic Pain
Information on preoperative chronic pain was obtained prospectively during the anesthesia consultation, regardless of the retrospective nature of this study. Chronic pain is defined as pain that persists or recurs for more than 3 months.5,15 Patients who completed psychosocial questionnaires prior to cardiac surgery (Supplementary Materials) and patients with chest pain or pain at the site of the proposed incision were excluded from the study.
Follow-Up CPSP and Pain-Related Complications
The International Association for the Study of Pain defines CPSP as pain that newly occurs or pain in which the extent increases after surgery and lasts for more than 3 months in the context of no other known causes of chronic pain.16 At both 3 and 24 months after cardiac surgery, the patients were contacted by telephone and asked to complete questionnaires regarding pain assessments. Pain intensity, pruritus degree, sleep interference, and daily activities interference were measured by the Numeric Rating Scale (NRS) (0–10),5,17–19 The participants were categorized as having no pain/pruritus/sleep interference/daily activities interference (NRS=0), light pain/pruritus/sleep interference/daily activities interference (NRS=1–3), moderate pain/pruritus/sleep interference/daily activities interference (NRS=4–7) or severe pain/pruritus/sleep interference/daily activities interference (NRS=8–10).5 In addition, pain-related complications such as pruritus, sleep interference and daily activities interference were followed up at 24 months. Detailed information on pain assessment is provided in the Supplementary Materials.
Statistical Analyses
Continuous variables are presented as the mean ± interquartile range (IQR) and were analyzed using the Mann–Whitney U-test or Student’s t-tests. Categorical variables were expressed as numbers and percentages (%) and compared by Pearson’s chi-square test or Fisher’s exact tests. Missing data were handled using multiple imputation techniques.
A multivariable logistic regression model was built to explore risk factors for the development of chronic pain over the follow-up period, and variables with a P value of 0.2 or less on individual univariate analysis were entered. The estimated odds ratios (OR) and 95% confidence intervals (95% CI) were reported. The associations between preoperative chronic pain and the primary outcome of moderate to severe CPSP and secondary outcomes, including moderate to severe chronic postoperative pruritus, daily activities interference and sleep disturbance were additionally assessed.
A two-tailed P value < 0.05 was considered statistically significant. The goodness of fit of the final model was excellent (P value by the Hosmer and Lemeshow test 0.11). The collinearity diagnostics suggested that there was no obvious multicollinearity among the variables, and a variance inflation factor (VIF) > 10 or tolerance < 0.1 was a criterion of severe collinearity. Statistical computations were performed in R version 4.1.3 (The R Foundation, Austria) and IBM SPSS Statistics 26.
Results
Among the 606 patients enrolled in this study, 495 patients were ultimately analyzed (Figure 1). The baseline demographics, comorbidities, intraoperative information, and postoperative outcomes are summarized in Table 1. Of the 495 patients, their median age was 62 (21–84) years old, and 175 (35.3%) were women. There were 118 (23.8%) patients who suffered from chronic pain preoperatively. In comparison with the patients without preexisting chronic pain, those with preexisting chronic pain were older, were more likely to be female and had a higher frequency of unemployment status.
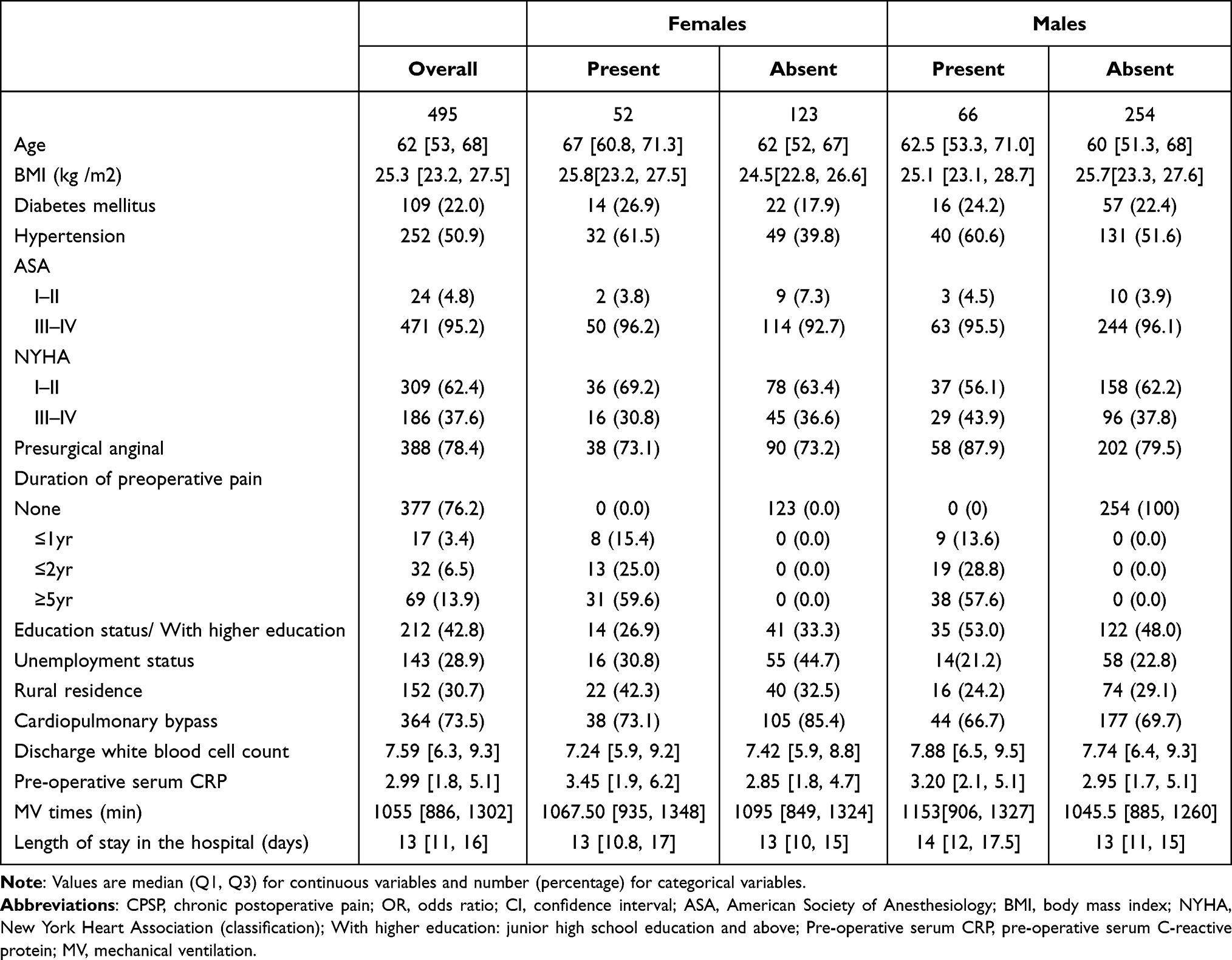 |
Table 1 The Characteristics of Patients with and without Presurgical Chronic Pain in Females and Males (n=495) |
Risk Factors for 24-Month CPSP
In our study, 10.5% of the participants (52/495) developed moderate to severe CPSP 2 years after surgery. As shown in Table 2, the patients who developed moderate to severe CPSP for 2 years had a higher incidence of preoperative chronic pain (P=0.001) and were more likely to be female (P=0.021). Age, a history of preoperative pain, female sex, and BMI were entered into the multivariate logistic regression analysis with stepwise backward elimination (Table 2). The female patients were more likely to develop moderate to severe CPSP at 2 years post-operation (adjusted OR 1.839 [1.014–3.334], P=0.048). Additionally, preoperative chronic pain contributed significantly to the risk of moderate to severe CPSP at 2 years after cardiac surgery (adjusted OR 2.352 [1.263–4.325], P=0.008).
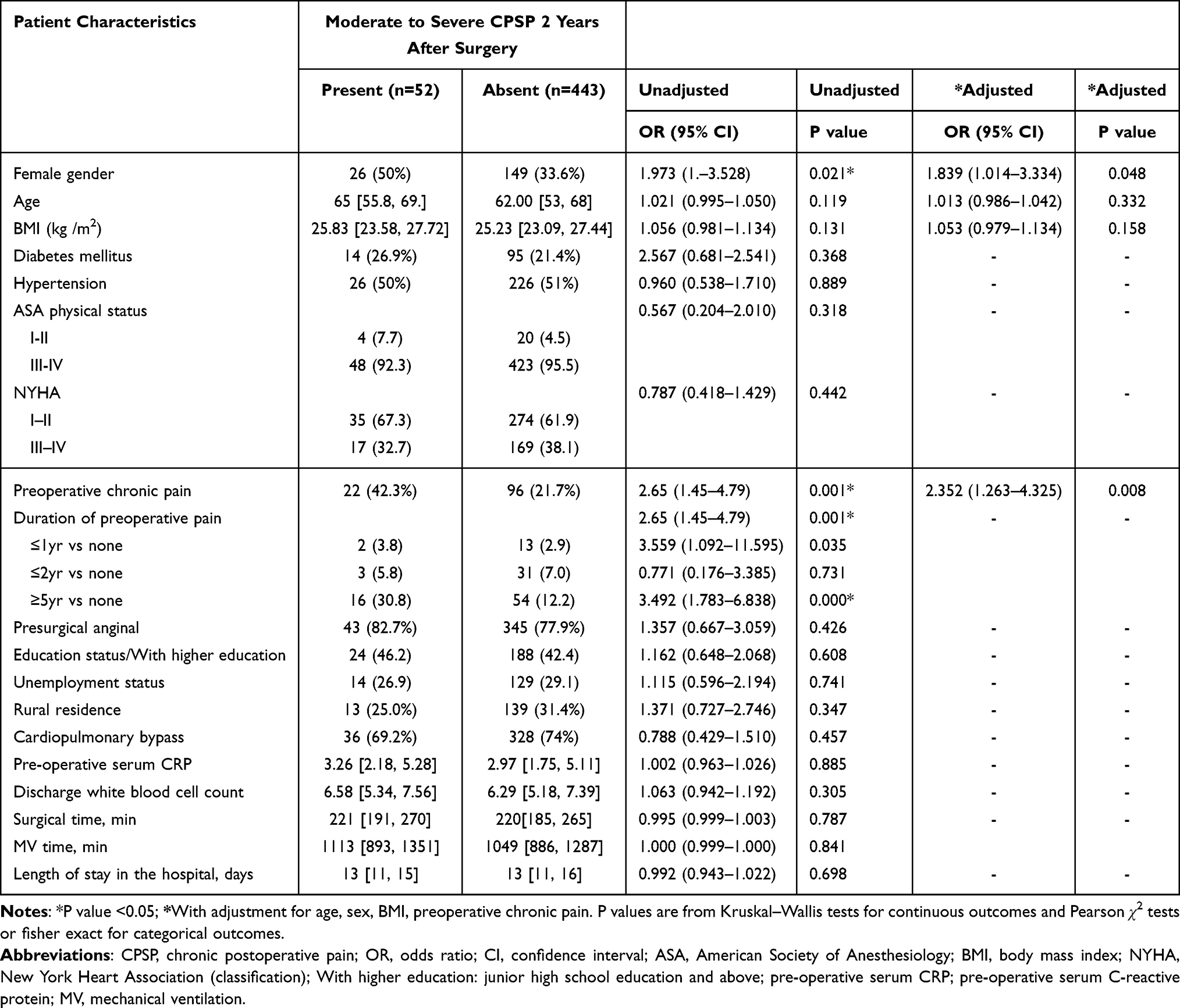 |
Table 2 The Characteristics of Patients Developing and Not Developing Moderate to Severe CPSP 2 Years After Cardiac Surgery (n=495) |
The Development of CPSP Stratified by Sex
The distributions of preoperative chronic pain, CPSP and other pain-related outcomes consisting of moderate to severe chronic postoperative pruritus, sleep disturbance and daily activities interference after cardiac surgery in the male and female patients are presented in Table 3. Relative to males, females were more likely to experience presurgical chronic pain (29.7% versus 20.6%; P=0.030) and gained higher incidences of moderate to severe CPSP at 3 months (41.1% versus 30.3%; P=0.020) and 24 months (14.8% versus 8.1%; P=0.029) after cardiac surgery. In addition, the odds of pain-related complications such as postoperative pruritus (13.4% versus 6.5%; P=0.013) and daily activities interference (9.6% vs 4.3%; P=0.032) among males were greater in comparison with females, however, a gender-specific analysis revealed no significant difference for sleep disturbance (p = 0.495).
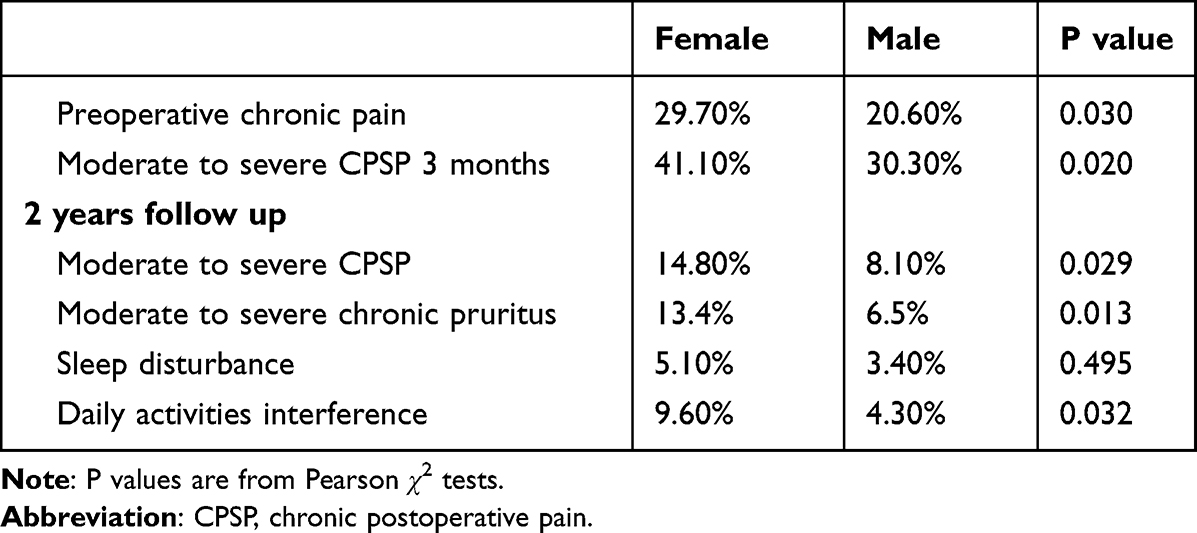 |
Table 3 Sex-Differences Regarding Preoperative and Postoperative Clinical Characteristics |
The associations between preoperative chronic pain and outcomes in the populations of males and females are presented in Table 4. In the female patients, preoperative chronic pain was associated with increased odds of moderate to severe CPSP (adjusted OR 3.377[1.375–8.501]; P =0.008), sleep disturbance (adjusted OR 5.022[1.068–28.893]; P =0.047) and daily activities interference (adjusted OR 3.378[1.246–11.284]; P =0.019) but not with moderate to severe chronic pruritus (adjusted OR 3.378[0.303–2.447]; P=0.856). However, in the male patients, preoperative chronic pain was not associated with any of the following outcomes: moderate to severe CPSP (P=0.425), sleep disturbance (P=0.261), daily activities interference (P=0.441) and moderate to severe chronic pruritus (P=0.864).
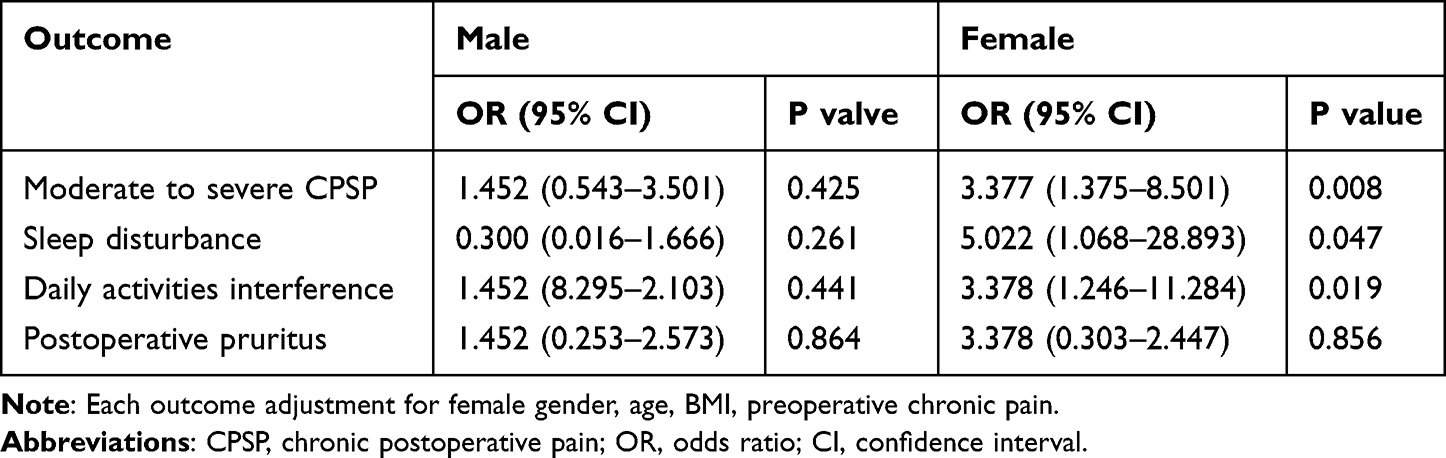 |
Table 4 Associations Between Preoperative Chronic Pain and Chronic Postoperative Pain Outcomes According to Sex |
Discussion
In this study, 23.8% of the patients reported preoperative chronic pain, and 10.5% of the participants experienced moderate to severe chronic pain 24 months after cardiac surgery. The results from the total sample indicated that female sex and preoperative chronic pain were significantly associated with chronic postoperative pain after cardiac surgery. However, according to gender analysis of the relationship between preoperative chronic pain and CPSP, preoperative chronic pain was only statistically significant in women.
Previous studies have demonstrated that females suffer more pain from chronic postoperative pain.11,20 In agreement with earlier research, females were associated with CPSP after cardiac surgery in our study.1,3,21 Additionally, whether pre- or postoperatively, more women reported chronic pain than men. Gene expression profiling studies have shown significant differences in the expression of genes associated with chronic pain between the sexes.22,23 Simultaneously, gender differences may exist in the neural and neural-immune mediation of pain.24 Calcitonin gene-related peptide (GCR P) can produce mechanical pain hypersensitivity and priming in female, but not male rats and mice.25 The spinal Toll-like receptor 4 is the critical receptor for microglial activation and controls pain allergy and allodynia caused by inflammation or nerve injury, but only in male mice.26 However, O’ Alabas et al believe that stereotypes of gender differences in pain were responsible for differences in pain expression.27
It has been confirmed that preoperative chronic pain is a risk factor for postoperative chronic pain in many surgeries,6,28,29 the mechanism of preoperative chronic pain leading to CPSP has not been clarified, pain sensitization and genetic factors are considered critical factors.30 However, little attention has been given to describing the relationship between preoperative chronic pain and CPSP after cardiac surgery with studies that include over two years of follow-up. In our research, 30% of patients with preoperative chronic pain had CPSP. Importantly, our study analyzed preoperative chronic pain and CPSP by sex and found that preoperative chronic pain was significantly associated with CPSP in women but not in men. Furthermore, we analyzed the relationship between preoperative chronic pain and pain-related outcomes, we obtained similar results. In women, preoperative chronic pain was significantly associated with pain-related complications, including sleep disturbance, and daily activities interference, but no significant association was found in the male population. This suggests that women might be more susceptible than men to the preoperative chronic pain effects on CPSP after cardiac surgery. On the one hand, long-term chronic pain forms chronic psychological stress, which exacerbates the development of postoperative chronic pain.31 Dawn K. Prusator et al reported that unpredictable early life stress produced visceral hypersensitivity and upregulation of stress-related genes in the central amygdala in female but not male rats.32 This finding demonstrates that there may be sex differences in stress as a risk factor for CPSP. On the other hand, there are sex differences in the effects of central sensitization and the genes associated with pain, which further explains the sex differences in preoperative chronic pain as a risk factor for CPSP. In addition, preoperative opioid use has also been found to exacerbate the development of CPSP in other studies.11 Patients with preoperative chronic pain were associated with an increased likelihood of preoperative opioid use. However, we were not able to obtain data on the preoperative opioid use by the patients in our study, and many of the participants could not recall opioid use. As early as 10 years ago, some researchers proposed using the preoperative pain questionnaire to determine the high-risk groups of postoperative chronic pain, but the previously formulated questionnaires were too complicated, making the clinical practicability not strong.33 Simpler tools may be considered in the future to identify high-risk patients preoperatively. In the future, we can divide preoperative chronic pain into specific subtypes and locations in a larger population, and explore which type of chronic pain is more likely to cause postoperative chronic pain.
Although younger age and higher BMI have been previously associated with CPSP after cardiac surgery,1,3,14,34 they were eventually not a predictor of CPSP in our study eventually. Additionally, we failed to find an association between other risk factors and CPSP other than gender and preoperative chronic pain. Regarding gender, more than half of the respondents were males. The main reason may be that cardiac surgery is more common in males according to statistics from the American Heart Association.35
Our research has many advantages, it was an observational study regarding CPSP after cardiac surgery with a low amount of missing data. The final model was tested using the Hosmer–Lemeshow goodness-of-fit test, and its results support the model. Notably, we are the first to attempt to elucidate sex differences in the relationship between preoperative chronic pain and postoperative chronic pain. Our study also has some limitations. First, our data only included patients from a single hospital, which may introduce some bias. Second, we did not measure the pain level of preoperative chronic pain, and different degrees of preoperative chronic pain may increase the risk of postoperative chronic pain differently. Third, In order to facilitate our research, we used the Numerical Rating Scale (NRS) assessment method for assessing our primary and secondary outcomes. Although this method has been used in many studies and demonstrated good reliability,5,17–19,36–38 it does not provide a comprehensive assessment. In the future, we can carry out multicenter studies in a larger population and provide a better assessment. Fourth, we focused on the long-term outcomes of postoperative chronic pain, therefore, we did not assess pain in acute phase patients. It is well known that the pain trajectory of patients in the acute phase is still an important clue to the occurrence of chronic postoperative pain in patients.
Conclusion
In this retrospective observational study, the prevalence of moderate to severe CPSP 24 months after cardiac surgery was 10.5%. We found that preoperative chronic pain is associated with postoperative chronic pain in the female population and that women are more susceptible to CPSP and pain-related complications in the long term than men. Preoperative and postoperative chronic pain is a serious problem, especially in women. Continued research is needed to examine how these sex differences may impact clinical treatment for opioid-related problems.
Acknowledgments
We thank all participants for their contribution to this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Choinière M, Watt-Watson J, Victor JC, et al. Prevalence of and risk factors for persistent postoperative nonanginal pain after cardiac surgery: a 2-year prospective multicentre study. Can Med Assoc J. 2014;186(7):E213–E223. doi:10.1503/cmaj.131012
2. Gjeilo KH, Stenseth R, Wahba A, Lydersen S, Klepstad P. Chronic postsurgical pain in patients 5 years after cardiac surgery: a prospective cohort study. Eur j Pain. 2017;21(3):425–433. doi:10.1002/ejp.918
3. Guimaraes-Pereira L, Farinha F, Azevedo L, Abelha F, Castro-Lopes J. Persistent postoperative pain after cardiac surgery: incidence, characterization, associated factors and its impact in quality of life. Eur J Pain. 2016;20(9):1433–1442. doi:10.1002/ejp.866
4. Hawash AA, Ingrasci G, Nouri K, Yosipovitch G. Pruritus in keloid scars: mechanisms and treatments. Acta Derm Venereol. 2021;101(10):adv00582. doi:10.2340/00015555-3923
5. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
6. Correll D. Chronic postoperative pain: recent findings in understanding and management. F1000Research. 2017;6:1054. doi:10.12688/f1000research.11101.1
7. Fletcher D, Stamer UM, Pogatzki-Zahn E, et al. Chronic postsurgical pain in Europe: an observational study. Eur J Anaesthesiol. 2015;32(10):725–734. doi:10.1097/EJA.0000000000000319
8. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
9. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
10. Timmers I, Quaedflieg C, Hsu C, Heathcote LC, Rovnaghi CR, Simons LE. The interaction between stress and chronic pain through the lens of threat learning. Neurosci Biobehav Rev. 2019;107:641–655. doi:10.1016/j.neubiorev.2019.10.007
11. Glare P, Aubrey KR, Myles PS. Transition from acute to chronic pain after surgery. Lancet. 2019;393(10180):1537–1546. doi:10.1016/S0140-6736(19)30352-6
12. Castellanos JP, Woolley C, Bruno KA, Zeidan F, Halberstadt A, Furnish T. Chronic pain and psychedelics: a review and proposed mechanism of action. Reg Anesth Pain Med. 2020;45(7):486–494. doi:10.1136/rapm-2020-101273
13. Veal FC, Bereznicki LR, Thompson AJ, Peterson GM, Orlikowski CE. Pain and functionality following sternotomy: a prospective 12-month observational study. Pain Med. 2016;17(6):1155–1162. doi:10.1093/pm/pnv066
14. Bjørnnes AK, Rustøen T, Lie I, Watt-Watson J, Leegaard M. Pain characteristics and analgesic intake before and following cardiac surgery. Eur J Cardiovasc Nurs. 2016;15(1):47–54. doi:10.1177/1474515114550441
15. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
16. Schug SA, Lavandhomme P, Barke A, Korwisi B, Rief W, Treede RD. The IASP classification of chronic pain for ICD-11: chronic postsurgical or posttraumatic pain. Pain. 2019;160(1):45–52. doi:10.1097/j.pain.0000000000001413
17. Pereira MP, Ständer S. Assessment of severity and burden of pruritus. Allergol Int. 2017;66(1):3–7. doi:10.1016/j.alit.2016.08.009
18. Kimel M, Zeidler C, Kwon P, Revicki D, Ständer S. Validation of psychometric properties of the itch numeric rating scale for pruritus associated with prurigo nodularis: a secondary analysis of a randomized clinical trial. JAMA Dermatol. 2020;156(12):1354–1358. doi:10.1001/jamadermatol.2020.3071
19. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152(10):2399–2404. doi:10.1016/j.pain.2011.07.005
20. Blichfeldt-Eckhardt MR. From acute to chronic postsurgical pain: the significance of the acute pain response. Dan Med J. 2018;65(3):B5326.
21. van Gulik L, Janssen LI, Ahlers SJ, et al. Risk factors for chronic thoracic pain after cardiac surgery via sternotomy. Eur J Cardiothorac Surg. 2011;40(6):1309–1313. doi:10.1016/j.ejcts.2011.03.039
22. Korczeniewska OA, Husain S, Khan J, Eliav E, Soteropoulos P, Benoliel R. Differential gene expression in trigeminal ganglia of male and female rats following chronic constriction of the infraorbital nerve. Eur J Pain. 2018;22(5):875–888. doi:10.1002/ejp.1174
23. Stephens KE, Zhou W, Ji Z, et al. Sex differences in gene regulation in the dorsal root ganglion after nerve injury. BMC Genom. 2019;20(1):147. doi:10.1186/s12864-019-5512-9
24. Gregus AM, Levine IS, Eddinger KA, Yaksh TL, Buczynski MW. Sex differences in neuroimmune and glial mechanisms of pain. Pain. 2021;162(8):2186–2200. doi:10.1097/j.pain.0000000000002215
25. Ceriani CEJ, Wilhour DA, Silberstein SD. Novel medications for the treatment of migraine. Headache. 2019;59(9):1597–1608. doi:10.1111/head.13661
26. Wang XY, Ma HJ, Xue M, et al. Anti-nociceptive effects of Sedum Lineare Thunb. On spared nerve injury-induced neuropathic pain by inhibiting TLR4/NF-κB signaling in the spinal cord in rats. Biomed Pharmacother. 2021;135:111215. doi:10.1016/j.biopha.2020.111215
27. Alabas OA, Tashani OA, Johnson MI. Effects of ethnicity and gender role expectations of pain on experimental pain: a cross-cultural study. Eur J Pain. 2013;17(5):776–786. doi:10.1002/j.1532-2149.2012.00229.x
28. Olsson A, Sandblom G, Fränneby U, Sondén A, Gunnarsson U, Dahlstrand U. Impact of postoperative complications on the risk for chronic groin pain after open inguinal hernia repair. Surgery. 2017;161(2):509–516. doi:10.1016/j.surg.2016.08.011
29. Lewis GN, Rice DA, McNair PJ, Kluger M. Predictors of persistent pain after total knee arthroplasty: a systematic review and meta-analysis. Br J Anaesth. 2015;114(4):551–561. doi:10.1093/bja/aeu441
30. Ji RR, Nackley A, Huh Y, Terrando N, Maixner W. Neuroinflammation and central sensitization in chronic and widespread pain. Anesthesiology. 2018;129(2):343–366. doi:10.1097/ALN.0000000000002130
31. Richebé P, Capdevila X, Rivat C. Persistent postsurgical pain: pathophysiology and preventative pharmacologic considerations. Anesthesiology. 2018;129(3):590–607. doi:10.1097/ALN.0000000000002238
32. Prusator DK, Greenwood-Van Meerveld B. Amygdala-mediated mechanisms regulate visceral hypersensitivity in adult females following early life stress: importance of the glucocorticoid receptor and corticotropin-releasing factor. Pain. 2017;158(2):296–305. doi:10.1097/j.pain.0000000000000759
33. Raja SN, Jensen TS. Predicting postoperative pain based on preoperative pain perception: are we doing better than the weatherman? Anesthesiology. 2010;112(6):1311–1312. doi:10.1097/ALN.0b013e3181dcd5cc
34. Harrogate SR, Cooper JA, Zawadka M, Anwar S. Seven-year follow-up of persistent postsurgical pain in cardiac surgery patients: a prospective observational study of prevalence and risk factors. Eur J Pain. 2021;25(8):1829–1838. doi:10.1002/ejp.1794
35. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American Heart Association. Circulation. 2021;143(8):e254–e743. doi:10.1161/CIR.0000000000000950
36. Puelles J, Fofana F, Rodriguez D, et al. Psychometric validation and responder definition of the sleep disturbance numerical rating scale in moderate-to-severe atopic dermatitis. Br J Dermatol. 2022;186(2):285–294. doi:10.1111/bjd.20783
37. Hayhurst CJ, Jackson JC, Archer KR, Thompson JL, Chandrasekhar R, Hughes CG. Pain and its long-term interference of daily life after critical illness. Anesth Analg. 2018;127(3):690–697. doi:10.1213/ANE.0000000000003358
38. Taguchi T, Nozawa K, Zeniya S, et al. Direct and indirect pathways for health-related quality of life change from pain improvement in neuropathic pain patients with spine diseases: path analysis with structural equation modeling using non-interventional study results of pregabalin. J Pain Res. 2021;14:1543–1551. doi:10.2147/JPR.S289396
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.