Back to Journals » Journal of Pain Research » Volume 18
Sex-Specific Association Between Vitamin D Insufficiency and Burning Pain in Herpetic Neuralgia: A Prospective Cohort Study
Authors Zhao W ![]() , Li Z, Ju J, Liu J, Peng X, Chu T
, Li Z, Ju J, Liu J, Peng X, Chu T ![]() , Ren J, Tu Y, Gao F
, Ren J, Tu Y, Gao F
Received 20 July 2025
Accepted for publication 29 November 2025
Published 5 December 2025 Volume 2025:18 Pages 6515—6525
DOI https://doi.org/10.2147/JPR.S555071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor King Hei Stanley Lam
Wei Zhao, Zheng Li, Jie Ju, Jie Liu, Xiaoling Peng, Tiantian Chu, Jihao Ren, Ye Tu, Feng Gao
Department of Anesthesiology and Pain Medicine, Hubei Key Laboratory of Geriatric Anesthesia and Perioperative Brain Health, and Wuhan Clinical Research Center for Geriatric Anesthesia, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
Correspondence: Feng Gao, Department of Anesthesiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430000, People’s Republic of China, Tel +86 13971587381, Fax +86 27 83662853, Email [email protected]
Purpose: Vitamin D is important for host immunity and a large proportion of herpes zoster patients experience vitamin D insufficiency (VDI). However, the role of vitamin D in herpetic neuralgia (HN) remains controversial. This study aims to explore the potential relationship between vitamin D status and HN characteristics.
Patients and methods: This prospective observational cohort study was conducted from February 2024 to November 2024 with 160 HN patients within 12 weeks after rash onset. Demographic and clinical data of patients were collected. The serum 25-hydroxyvitamin D level, triglyceride and other laboratory parameters were measured at patients’ admission. Comprehensive pain evaluations including the Brief Pain Inventory (BPI), 11-point Numerical Rating Scale (NRS) and Douleur Neuropathique 4 questionnaires were performed at admission, as well as 1, 2, and 3 months after treatment.
Results: VDI was prevalent (121 VDI, 39 VDS) in the cohort. Although no significant correlation emerged between vitamin D levels and BPI or NRS scores, Female (n = 82, odds ratio [OR] 2.80, 95% CI 1.30– 6.33, P < 0.05) and high serum triglyceride level (OR 3.20, 95% CI 1.41– 8.86, P < 0.05) were identified as independent predictors of VDI. Female patients exhibited a significant negative correlation between vitamin D status and burning pain (Spearman’s ρ = − 0.347, P < 0.001) and a concomitantly lower early pain relief rate compared to males, in whom the correlation was non-significant (n = 78, ρ = 0.7, P > 0.05).
Conclusion: Low vitamin D levels are common in HN patients. The sex-specific association between VDI and burning pain, as well as short-term prognosis, Triglyceride levels served as a predictive indicator for VDI in HN patients. Future studies are needed to elucidate the underlying mechanisms of the pain-vitamin D association specifically in female patients.
Keywords: herpetic neuralgia, vitamin D, triglyceride, burning pain
Introduction
Herpetic neuralgia (HN) is a distinct neuropathic pain syndrome characterized by hyperalgesia and paresthesia following the reactivation of latent varicella-zoster virus in sensory ganglia.1 Pain persists for >3 months after the initial outbreak of herpes zoster (HZ) is classified as postherpetic neuralgia (PHN).2 Approximately 9% to 34% of HZ patients will progress to PHN, with the incidence increasing to 65% in patients aged >60 years.3 The pathogenic mechanism of HZ has not been completely understood, and current therapeutics for HN and PHN demonstrate limited efficacy in clinical practice.
Beyond its canonical effect in skeletal homeostasis, vitamin D functions as a pleiotropic neuroactive steroid in neuroinflammation and immune modulation.4 It exerts anti-inflammatory effect by suppressing pro-inflammatory cytokine cascades and enhancing the production of anti-inflammatory mediators. Furthermore, vitamin D exhibits notable antiviral properties by promoting antimicrobial peptide synthesis, potentially mitigating viral replication and reactivation.5 Vitamin D insufficiency (VDI) is highly prevalent among patients with chronic pain, with an incidence rate of averaging 50%.6 The mechanistic link between VDI and chronic pain potentially involves enhanced central sensitization in nociceptive pathways secondary to abnormal vitamin D level.7 Besides, Activation of the vitamin D receptor (VDR) inhibits PKCα/NOX4 signaling-mediated mitochondria-associated ferroptosis, thereby preserving spinal GABAergic interneurons and ultimately alleviating neuropathic pain.8 The specific mechanisms by which vitamin D influences pain perception remain elusive.
The multiple properties of vitamin D indicate its potential involvement in attenuating varicella-zoster virus reactivation and subsequent development of HN through disrupting persistent neuroinflammatory process.6 Moreover, the crucial role of vitamin D in calcium homeostasis warrants particular consideration9 as dysregulation of calcium signaling is significantly correlated with both HN severity and clinical outcomes10 and the independent regulatory role of estrogen in calcium transport, as well as its synergistic effects with the vitamin D system.11 So sex also influencing vitamin D levels. Existing literature indicates that women in China are more susceptible to vitamin D deficiency than men,12 An Italian cohort study on vitamin D conducted between 2005 and 2016 demonstrated a higher prevalence of vitamin D insufficiency in women compared to men.13 On the other hand, It may regulate microsomal triglyceride transfer protein (MTP) by modulating calcium metabolism, thereby reducing triglyceride synthesis and secretion.14 However, previous studies yielded contradictory findings about the role of vitamin D in HN. VDI was identified as an independent predictor of HN development in a previous study,15 whereas others found no significant association between reduced vitamin D level and neuropathic pain syndrome.16 Due to the complexity of the pathophysiology of HN, more investigations are needed to explore the role of vitamin D in HN.
In this study, we aimed to determine the relationships among serum vitamin D level, characteristics of HN in acute/subacute phase (within 12 weeks from rash onset), and therapeutic responsiveness in a cohort of acute and subacute HN patients who were hospitalized in a university-affiliated teaching hospital.
Methods
Study Design and Participants
This prospective observational cohort study was conducted from February 2024 to November 2024 at Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China. The study protocol was approved by the Ethics Committee of Tongji Hospital (TJ-IRB20231251) on December 7, 2023, and registered at ClinicalTrials.gov (NCT06232486) on December 25, 2023. The first patient was enrolled on February 5, 2024, and the last interview of follow-up was finished on November 7, 2024, Written informed consent was obtained from all patients. The study was conducted in accordance with the Declaration of Helsinki and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline.
Inclusion and Exclusion Criteria
This study comprised HN patients who visited our outpatient pain clinic and hospitalized for treatment. The diagnosis of HZ and HN was performed according to Chinese version of the 10th International Classification of Disease (ICD-10-CM: B02. 9).17 The inclusion criteria were as follows: (1) age ≥18 years; (2) patients diagnosed as HN with a disease course from rash onset of ≤ 3 months; and (3) patients who cooperated with completing the inquiry and scale evaluation. The exclusion criteria were factors may affect vitamin levels, function and metabolism below: (1) severe spinal disease (fracture, malignancy, acute or chronic infection) confirmed by previous spinal surgery or imaging;18 (2) presence of autoimmune diseases (systemic lupus erythematosus, rheumatoid arthritis, auto thrombocytopenia);19 (3) presence of mental disorders, intellectual disability, epilepsy;20 (4) history of substance, drug, or alcohol abuse; (5) pregnant or breastfeeding women;21 and (6) recent participation in other clinical studies.
Data Collection
Patients’ demographic data were collected from the electronic medical database. Pain assessments, including the Brief Pain Inventory (BPI), 11-point Numerical Rating Scale (NRS), and Douleur Neuropathique 4 (DN4) questionnaires, were performed at patients’ admission to the ward through in-person interview, and 1, 2, and 3 months after standardized treatment by telephone consultation.
Plasma Sample Collection and Measurements
Blood samples were collected on day 2 after admission at 08:00–09:00 (fasting, 5 mL, EDTA) for the measurements of 25-hydroxyvitamin D [25(OH)D], immune indicators (C3, C4, CD4+ and CD8+ T cells), inflammatory factors [interleukin (IL)-6, IL-8, tumor necrosis factor-alpha (TNF-α), and IL-10], triglyceride (TG), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), blood uric acid (UA), mean cell volume (MCV), and serum electrolytes Ca2+ with clinical conventional laboratory tests. All indicators were measured in the hospital’s clinical laboratory following standard operating procedures on weekdays. The details of all testing assays, instruments, and major reagents are summarized in Supplementary Table 1.
Treatments
The standardized treatment protocol for HN patients with a disease course of ≤ 3 months included nerve block, pulse radiation frequency (PRF), and spinal cord stimulation (SCS). Treatments were administered based on pain intensity and treatment history: nerve block for mild pain, pulsed radiofrequency (PRF) for moderate to severe pain, and spinal cord stimulation (SCS) for cases of recurrence or refractory pain. All patients provided informed consent before treatment.
Vitamin D Status
Vitamin D status was classified according to the consensus from the First International Conference on Controversies in Vitamin D. Serum 25(OH)D levels below 12 ng/mL (30 nmol/L) were classified as deficient and associated with increased disease risk, while levels of 20–50 ng/mL (50–125 nmol/L) were considered as sufficient for optimal health.22 According to previous study,23 HN patients in this study were stratified into vitamin D insufficient (<20 ng/mL) and vitamin D sufficient (≥20 ng/mL) groups. A 25OHD level of 20 ng/mL is recommended for adults aged 18–70 and those over 71.24
Sample Size
Sample size calculation was performed using (PASS software, version 15, NCSS, LLC). And based on the reported VDI prevalence of 73.9% in the PHN group and 47.0% in the control group.15 To detect this difference with 90% power at a two-sided significance level a = 0.05, 130 participants were required. After inflating the sample size by 20% to account for potential loss to follow-up, a final sample of 152 was planned for recruitment. The final sample size for this study was 162 individuals.
Statistical Analysis
Statistical analysis was performed using SPSS software (IBM SPSS Statistics version 27). Statistical significance was established at P <0.05. Variables with >10% missing data were excluded from statistical analyses, including ESR and CRP, and outliers were treated as missing data to be deleted.
Categorical variables were expressed as frequencies and percentages, while continuous variables as means with standard deviations for normally distributed data or medians with interquartile ranges for non-normally distributed data. Kolmogorov–Smirnov test was used to assess the normality of continuous variables. Group differences in categorical variables were analyzed using appropriate chi-square or Fisher’s exact tests. For continuous variables, comparisons between groups were conducted using either Student’s t-test or two-way ANOVA, followed by Dunn’s multiple comparison test with Bonferroni correction for post hoc analysis, Comparisons between sex groups on the 11 pain indicators were performed using Bonferroni correction was applied by setting the significance level at α = 0.05/11 = 0.005. Variables at different time points were analyzed using repeated measures ANOVA. Mann–Whitney test was used for continuous variables that were not normally distributed.
The associations between serum 25(OH)D levels and pain severity metrics were assessed using Spearman’s rank correlation analysis. Multivariate logistic regression model was used to identify independent risk factors for VDI, This process entailed first conducting univariate analyses, followed by the entry of variables demonstrating preliminary significance (P < 0.1) into a multivariate model using stepwise regression to screen for the final predictive factors. Since most patients in our cohort underwent PRF therapy, their data were used to analyze the relationship between VD level and therapeutic outcome. The pain relief was defined as NRS score was reduced by at least 30% after treatment. Time-to-event analyses for pain relief were conducted with stratification by sex and vitamin D status. Kaplan-Meier survival curves were compared using Breslow test to determine the significant differences in therapeutic effect rates between groups.
Results
A total of 162 HN patients were assessed for eligibility. Two patients were excluded due to autoimmune disease and accepting orthopaedic surgery, respectively. Of 160 patients, most of them (66.3%) completed 12-week follow-up (Figure 1).
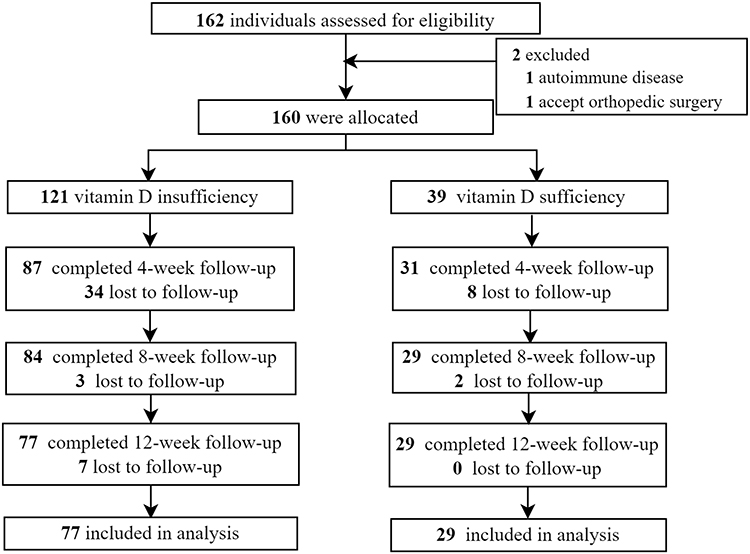 |
Figure 1 Flow diagram of the study. Bolded black labels shows the number of subjects included. |
Demographic and Clinical Characteristics of Patients
Of all the 160 patients, the median (interquartile range) age was 65 (59–71) years and 121 (75.6%) presented with VDI. The clinical characteristics of the patients are presented in Table 1. Although the proportions of the males and females were comparable in all patients, VDI was significantly more prevalent among females than males (P = 0.006). No significant differences were observed between groups in terms of BPI or NRS scores at admission and the prevalence of neuropathic pain characteristics, such as numbness, acid pain, burning pain, swelling sensations, sharp pain, electric shock-like sensations, or allodynia (P >0.05, Table 2). VDI patients had high serum triglyceride levels than those without VDI (P = 0.015, Table 3).
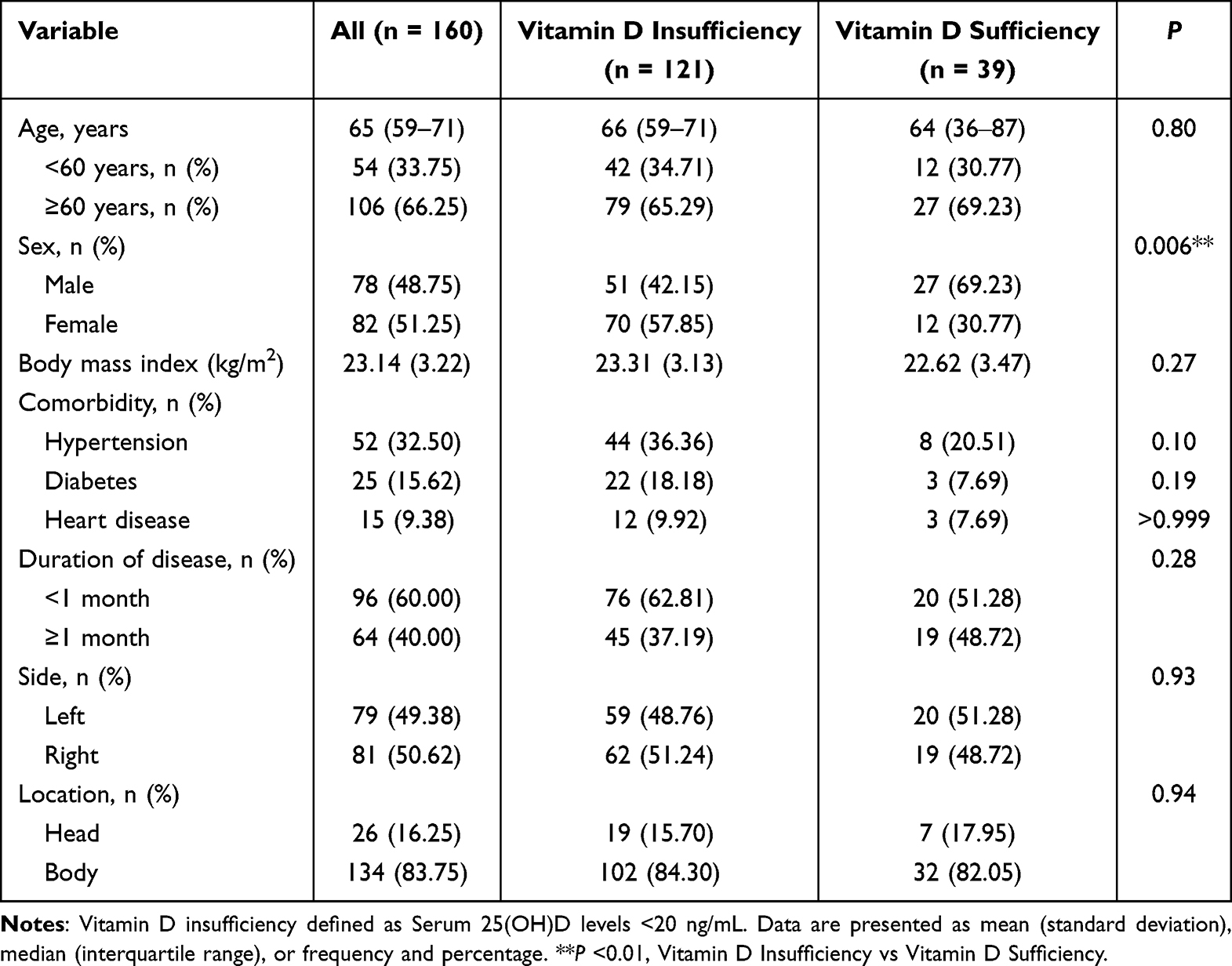 |
Table 1 Demographic and Clinical Characteristics Between Groups Based on Vitamin D Status |
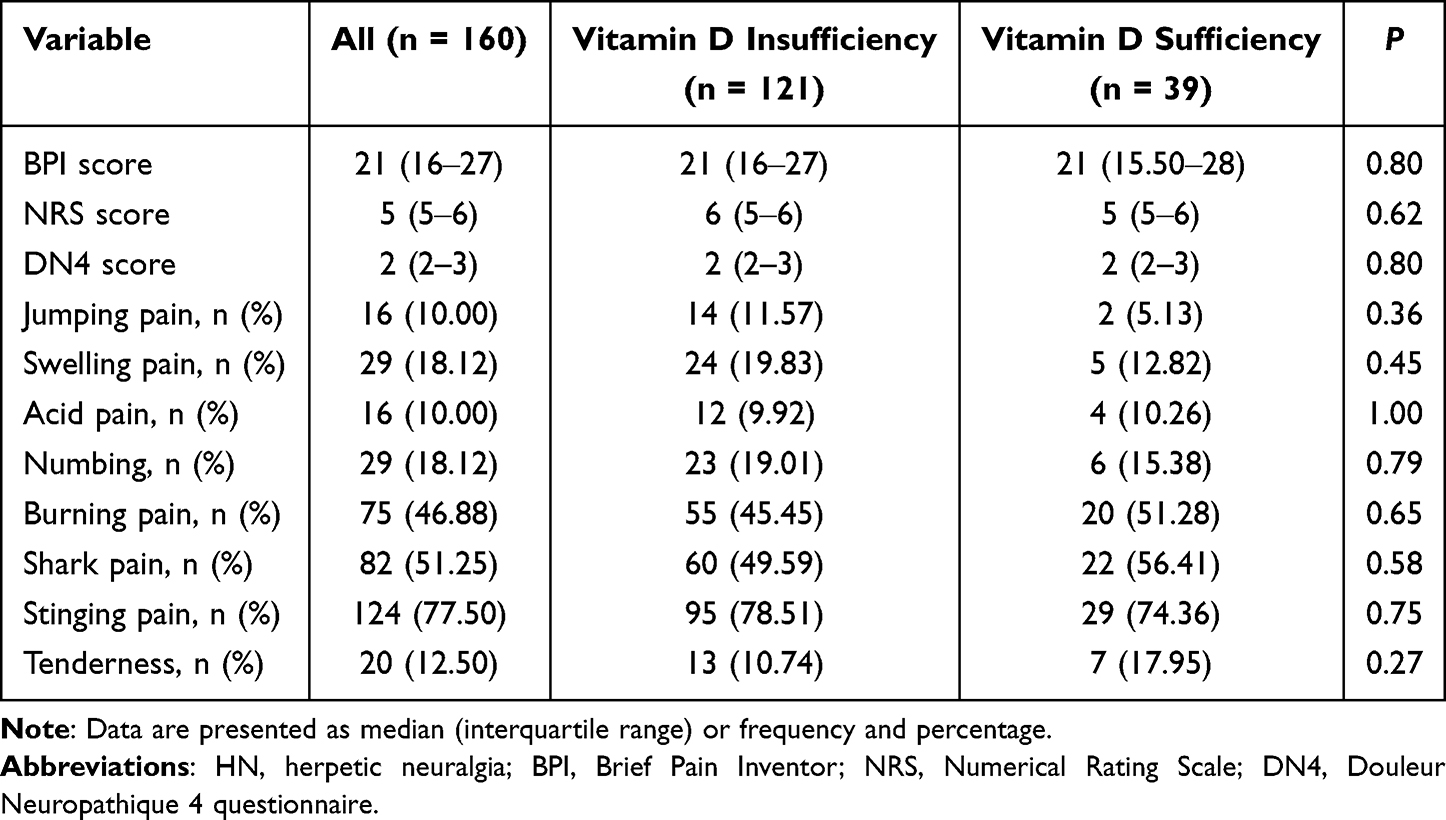 |
Table 2 Proportions of Items in the DN4 Questionnaire of HN Patients at Admission |
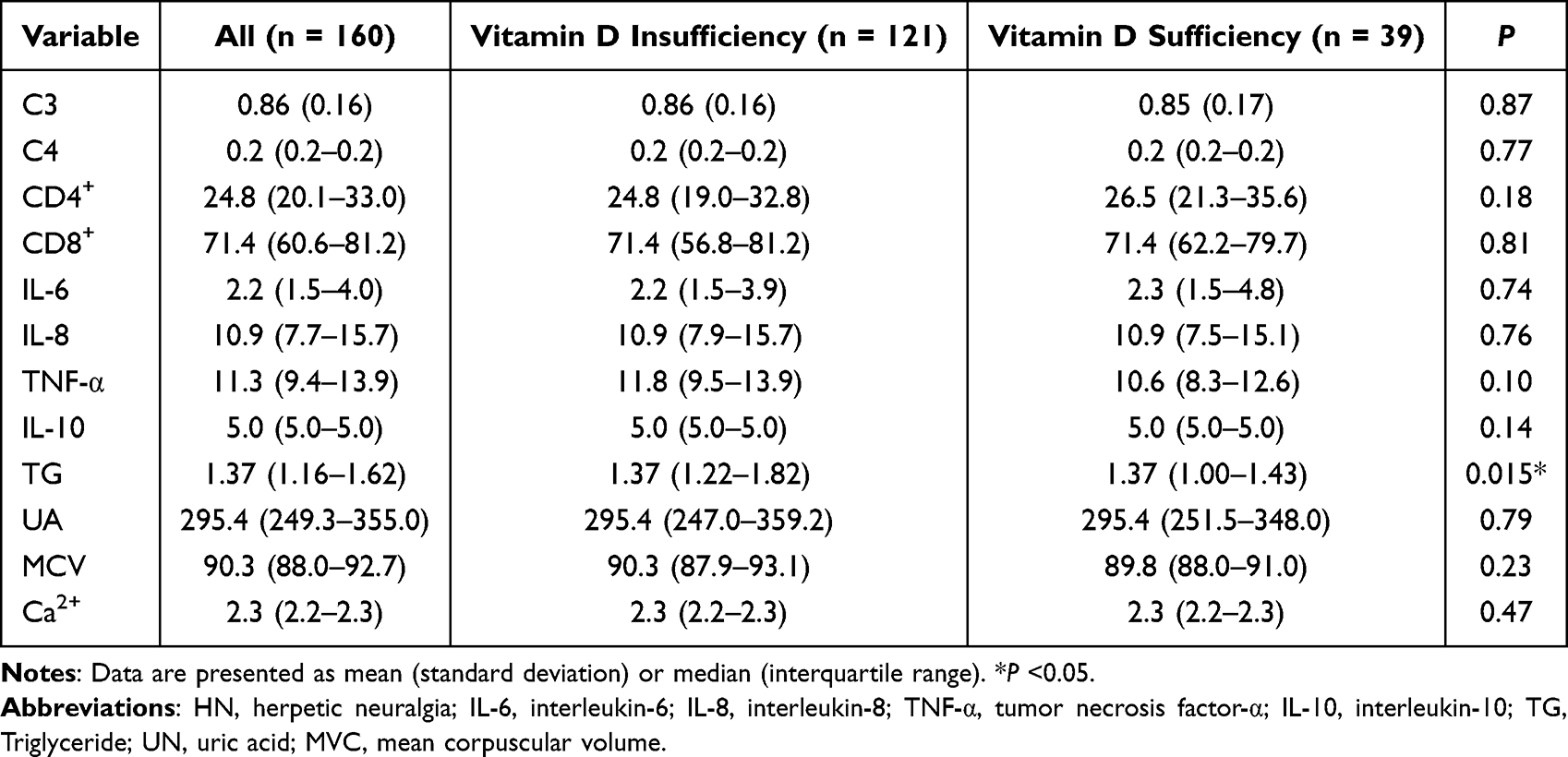 |
Table 3 Results of Clinical Laboratory Tests of HN Patients at Admission |
Risk Factors for Vitamin D Insufficiency in HN Patients
The incorporating variables included in multivariate logistic regression analysis were sex, hypertension and serum TG level, which demonstrated P <0.1 in univariate analysis. Female was identified as an independent risk factor for VDI, with male patients demonstrating a 64.3% lower probability of VDI (P = 0.011; OR = 0.357; 95% CI, 0.157–0.772). Additionally, TG levels were significantly associated with vitamin D status, with each 1 mmol/L increase in TG level conferring a 3.203-fold higher risk of VDI (P = 0.014; OR = 0.312; 95% CI, 0.112–0.710) (Table 4). Both TG levels and female sex were significantly associated with VDI in patients with HN.
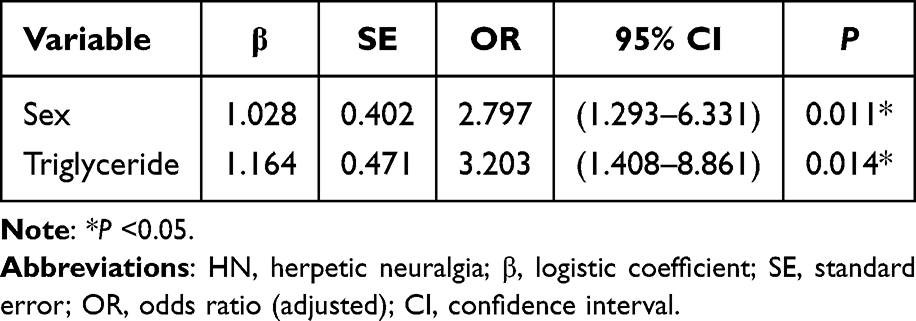 |
Table 4 Multivariable Logistic Regression Analysis of Risk Factors for Vitamin D Insufficiency in HN Patients |
Receiver operating characteristic curve analysis of TG level as a predictor of VDI yielded an area under the curve of 0.625 (95% CI, 0.535–0.723; P = 0.015), indicating moderate discriminating capacity (Figure 2). The optimal threshold value, determined by maximizing Youden’s index (sensitivity + specificity − 1), was 1.55 mmol/L, corresponding to a sensitivity of 94.87% and specificity of 33.06%. Notably, this threshold was lower than the established clinical reference value of 1.7 mmol/L for hypertriglyceridemia.
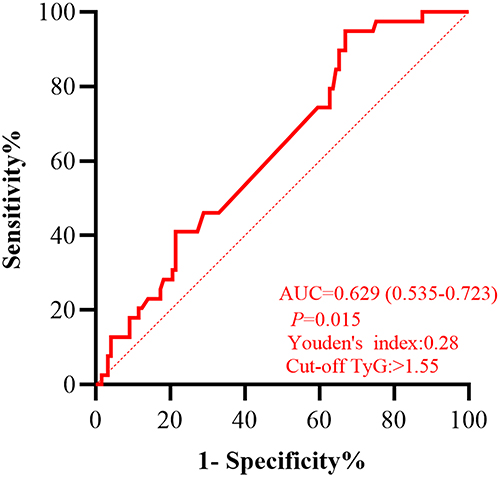 |
Figure 2 Receiver operating characteristic curve for triglyceride in vitamin D insufficiency. |
Association Between Vitamin D Status and Pain Characteristics Among Male and Female Patients
A significant negative correlation was observed between serum 25(OH)D levels and burning pain in female patients (P <0.001). No significant correlations were identified between serum 25(OH)D levels and BPI scores, NRS scores, DN4 composite scores, or other specific pain characteristics in either male or female patients (Table 5).
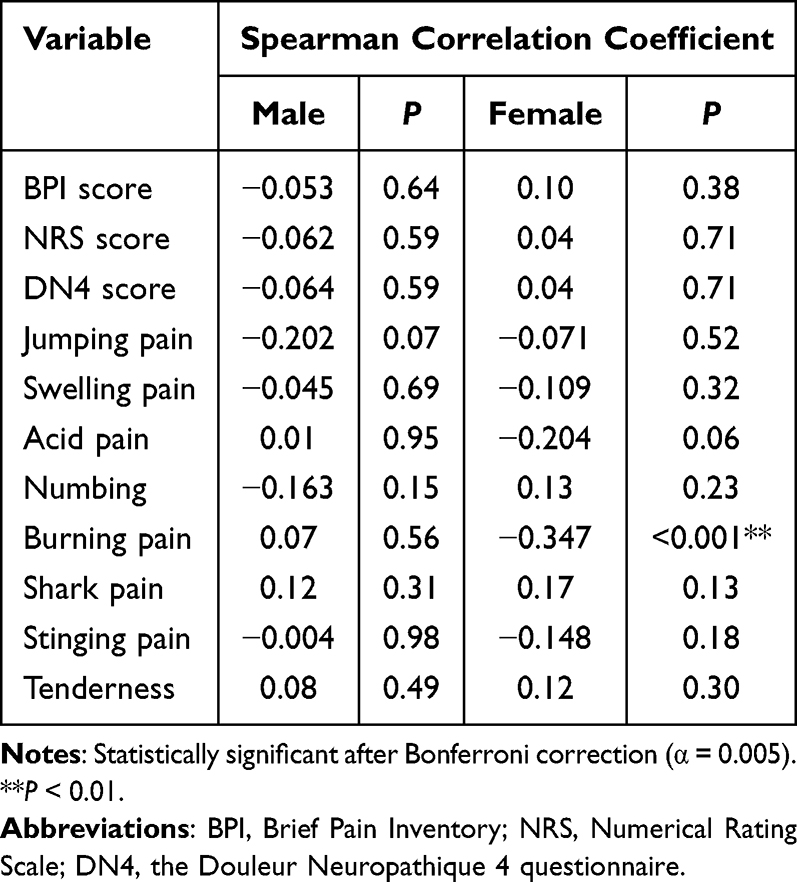 |
Table 5 Correlations Between Vitamin D Status and Pain Characteristics with Respect to Sex |
Prediction of Treatment Outcomes
Among all patients, 69.4% (111/160) received PRF (VDI group: 71.8%; vitamin D sufficiency group: 61.5%)) and 83.3% of them experienced pain relief at discharge, 21.3% (34/160) received SCS with 94.1% of pain relief, 3.8% (6/160) received nerve block with 66.7% of pain relief, and 5.6% (9/160) received drug therapy only with 11.1% of pain relieve.
The following analysis was restricted solely to the PRF treatment regimen. The NRS scores at 1, 2, and 3 months after discharge had no significant difference between patients with and without VDI (Figure 3). The Kaplan Meier curves in Figure 4 showed the pain relief of males (50/111) and females (61/111) after PRF treatment, as well as its distribution in patients with (87/111) and without VDI (24/111). Breslow test showed a significant difference in early survival between male and female patients (95% CI, 0.37–1.10; P <0.05). Survival analysis during follow-up period of less than 60 days indicated the poor pain relief effect after PRF therapy in female patients (HR = 0.38; 95% CI, 0.20–0.74; P <0.01).
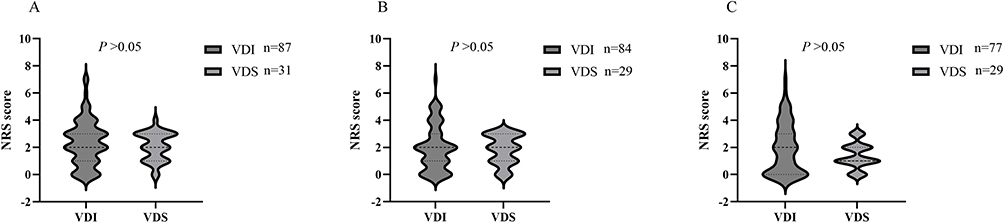 |
Figure 3 The NRS scores between VDI and VDS groups during 3-month follow-up. (A) During 1 month, VDI vs VDS, P > 0.05; (B) During 2 month, VDI vs VDS, P > 0.05; (C) During 3 month, VDI vs VDS, P > 0.05. Abbreviations: VDI, vitamin D Insufficiency; VDS, vitamin D sufficiency. |
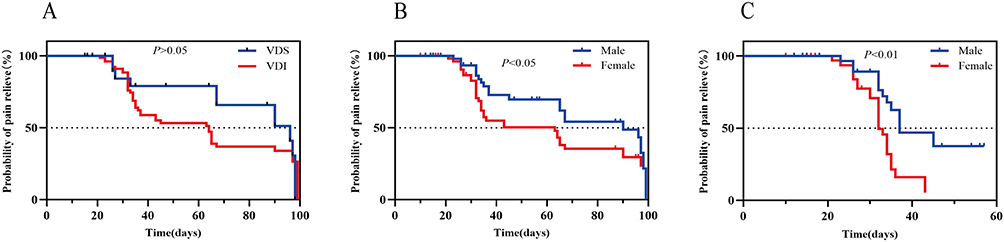 |
Figure 4 Probability of pain alleviation during 3-month follow-up. (A) VDI vs VDS, P > 0.05; (B) Male vs Female, P < 0.05; (C) Male vs Female, P < 0.01. Abbreviations: VDI, vitamin D Insufficiency; VDS, vitamin D sufficiency. |
Discussion
This study revealed a 75.6% prevalence of VDI in HN patients. Female and high serum triglyceride level were identified as the independent predictors of VDI. Although no global correlation emerged between serum 25(OH)D level and pain intensity, we identified a significant negative association between vitamin D status and burning pain in female patients. Additionally, female patients had a significant lower pain relief rate than male at early stage after PRF therapy.
The high prevalence of VDI observed in our cohort aligns with previous study.25 This phenomenon is typically the result of multiple contributing factors. The average age of the participants in this study is over 60 years old, and advanced age is closely related to the increased incidence of VDI and osteoporosis, not just HN.23 Increased comorbidity burden, such as diabetes, asthma, lymphoproliferative disorders, and Helicobacter pylori-associated peptic ulceration, may contribute to the onset of VDI.26–28 Through its modulation of innate and adaptive immunity, vitamin D may influence several aspects of herpes zoster, from susceptibility and clinical course to its outcomes. This influence potentially encompasses treatment complications, drug efficacy, and the risk of postherpetic neuralgia.29 However, the temporal relationship between suboptimal vitamin D status and HN needs to be determined. Whether VDI predates and potentially predisposes to HN development, or represents a consequence of pain-related behavioral changes or ongoing neuroinflammatory processes are still unclear.
We found serum vitamin D levels did not correlate with global pain severity metrics, which corresponds with the observation by Lin et al that neither VDI nor supplementation influenced HZ incidence.30 However, the results of Chen et al identified low vitamin D level as an independent predictor of post-HN development.15 These discrepancies might reflect the methodological heterogeneity in defining VDI, with threshold values ranging from 15 ng/mL to 30 ng/mL across the studies.30 Our classification adhered to the recently adopted European guidelines, including those from the European Calcified Tissue Society, which recommend a threshold of 20 ng/mL (50 nmol/L) to define vitamin D insufficiency or sufficiency.31
The negative correlation between serum 25(OH)D levels and burning dysesthesia, specifically in female patients with HN, indicates a novel finding of sex-specific pathogenetic mechanisms. HN typically manifests as multiple somatosensory abnormalities, including spontaneous lancinating pain, dysesthesia, and burning sensations within the affected dermatomal distribution.32 The burning component specifically implicates the spontaneous activation of intact C-fiber nociceptors.33 VDI may enhance spontaneous activity and prolong evoked responses in primary afferent neurons.34 Evidence suggests that estrogen acts via ERα to presynaptically suppress nociceptive transmission from Aδ- and C-fibers to spinal SG neurons, as blocking this receptor with MPP enhanced both synaptic excitation and behavioral responses.35 Vitamin D not only improve the bioavailability of estrogen, but also the latter can improve vitamin D absorption efficiency and affinity of transport system in women especially at autoimmune diseases.36 Following ovariectomy, the marked reduction in total VDR expression, largely due to a specific loss of cytoplasmic VDR in unmyelinated CGRP-positive neurons, implicates vitamin D signaling in a specialized, nociceptive-specific pathway.37 Based on these findings, we speculate that estrogen may impacts pain progression through VDR modulation C-fiber nociceptors, warranting further investigation into the specific processes of estrogen and VDR interplay in HN.
Identifying serum TG level as an independent predictor of VDI in HZ patients is a novel finding of this study. This aligns with the findings in type 2 diabetes mellitus, which showed a correlation between hypertriglyceridemia and vitamin D deficiency.38 These potentially reflect the fat-soluble properties of vitamin D and its regulatory effect in lipid metabolism,39 and the increased age is related to the incidence of hypertriglyceridemia.40 However, there is currently limited evidence about the relationship between TG and VDI in herpes zoster neuralgia. Emerging data indicate that vitamin D receptor polymorphism influences lipid homeostasis, with specific genetic variants associated with elevated triglyceride and cholesterol profiles.41–43 Furthermore, calcium and vitamin D co-supplementation effectively reduced total cholesterol and TG levels.44 The lower TG threshold (1.55 mmol/L) identified in our cohort compared with standard clinical reference (1.7 mmol/L) likely reflects the distinct demographic and metabolic characteristics of HN patients, highlighting the complex interrelationship between vitamin D homeostasis and lipid metabolism in neuroinflammatory condition, and it is a potential predictor of vitamin D deficiency in HN patients, useful for preliminary screening but not sufficient for diagnosis.
This study has several limitations. First, sun exposure, daily activity, and dietary intake were the potential influential factors for vitamin D status. Their relationships with HZ were not considered in our study. Second, A limitation of this prospective observational study is the loss of patients to follow-up, for whom treatment efficacy remains unknown. This may bias the outcome assessment. Therefore, the follow-up results are exploratory and not conclusive. Third, A limitation of this study is the absence of an a priori power calculation for subgroup analyses, including the sex-stratified correlation analyses. Last, The observational study prevents us from making causal inferences about the roles of the studied factors in the development of vitamin D deficiency. But the observed association is consistent with the known role of vitamin D in the disease. In addition, our recent results show that vitamin D correlates with burning pain in HN female patients, and that triglycerides and gender serve as predictive factors for VDI. There is a need for a prospective, randomized cohort study to determine the difference of vitamin D levels in HN patients exhibiting various pain characteristics.
Conclusion
A significant negative association exists between serum 25(OH)D levels and burning dysesthesia in female than male patients, VDI is highly prevalent among HN patients, but does not correlate with pain intensity. Sex and triglyceride are dependent predictors for VDI in HN. In addition, we identified poorer short-term functional recovery in female patients after PRF. Our findings provide guidance for tailoring personalized treatment and improving prognostic evaluation in HN. Future studies are needed to elucidate the underlying mechanisms of the pain-vitamin D association specifically in female patients.
Date Sharing Statement
This study’s deidentified individual participant data that support the main findings will be shared with researchers who provide a methodologically sound proposal. The data will be made available upon request to the author Wei Zhao ([email protected]) after the manuscript’s publication and for up to 2 years. Access requires approval by the Institutional Review Board and is contingent on the completion of a data use agreement.
Acknowledgments
The authors thank all the participants for their contribution to this study.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Tang J, Zhang Y, Liu C, Zeng A, Song L. Therapeutic strategies for postherpetic neuralgia: mechanisms, treatments, and perspectives. Curr Pain Headache Rep. 2023;27(9):307–319. doi:10.1007/s11916-023-01146-x
2. Sampathkumar P, Drage LA, Martin DP. Herpes zoster (shingles) and postherpetic neuralgia. Mayo Clin Proc. 2009;84(3):274–280. doi:10.4065/84.3.274
3. Mbinta JF, Nguyen BP, Awuni PMA, Paynter J, Simpson CR. Post-licensure zoster vaccine effectiveness against herpes zoster and postherpetic neuralgia in older adults: a systematic review and meta-analysis. Lancet Healthy Longev. 2022;3(4):e263–e275. doi:10.1016/s2666-7568(22)00039-3
4. Szymczak-Tomczak A, Ratajczak AE, Kaczmarek-Ryś M, et al. Pleiotropic effects of vitamin D in patients with inflammatory bowel diseases. J Clin Med. 2022;11(19):5715. doi:10.3390/jcm11195715
5. Zwart SR, Mehta SK, Ploutz-Snyder R, et al. Response to vitamin D supplementation during antarctic winter is related to BMI, and supplementation can mitigate Epstein-Barr Virus Reactivation. J Nutr. 2011;141(4):692–697. doi:10.3945/jn.110.134742
6. McCarty DE, Reddy A, Keigley Q, Kim PY, Cohen S, Marino AA. Nonspecific pain is a marker for hypovitaminosis D in patients undergoing evaluation for sleep disorders: a pilot study. Nat Sci Sleep. 2013;5:37–42. doi:10.2147/nss.S42641
7. Habib AM, Nagi K, Thillaiappan NB, Sukumaran V, Akhtar S. Vitamin D and its potential interplay with pain signaling pathways. Front Immunol. 2020;11:820. doi:10.3389/fimmu.2020.00820
8. Zhang W, Yu S, Jiao B, et al. Vitamin D(3) attenuates neuropathic pain via suppression of mitochondria-associated ferroptosis by inhibiting PKCα/NOX4 signaling pathway. CNS Neurosci Ther. 2024;30(9):e70067. doi:10.1111/cns.70067
9. Lin YT, Wang LK, Hung KC, Wu ZF, Chang CY, Chen JY. Patient characteristics and analgesic efficacy of antiviral therapy in postherpetic neuralgia. Med Hypotheses. 2019;131:109323. doi:10.1016/j.mehy.2019.109323
10. Zhai XY, Cheng RY, Kong LT, et al. A study on the connection between the incidence of postherpetic neuralgia and serum ionized calcium. Chin Med J. 2015;128(22):3106–3108. doi:10.4103/0366-6999.169108
11. Christakos S, Prince R. Estrogen, vitamin D, and calcium transport. J Bone Miner Res. 2003;18(10):1737–1739. doi:10.1359/jbmr.2003.18.10.1737
12. Yan X, Zhang N, Cheng S, Wang Z, Qin Y. Gender differences in vitamin D status in China. Med Sci Monit. 2019;25:7094–7099. doi:10.12659/msm.916326
13. Giannini S, Pitino A, Sella S, et al. Sex-related differences in vitamin D testing in the Veneto Region, Italy: a retrospective analysis from 2005 to 2016. Arch Osteoporos. 2024;19(1):105. doi:10.1007/s11657-024-01460-w
14. Hussain MM, Nijstad N, Franceschini L. Regulation of microsomal triglyceride transfer protein. Clin Lipidol. 2011;6(3):293–303. doi:10.2217/clp.11.21
15. Chen JY, Lin YT, Wang LK, et al. Hypovitaminosis din postherpetic neuralgia-high prevalence and inverse association with pain: a retrospective study. Nutrients. 2019;11(11):2787. doi:10.3390/nu11112787
16. Alkhatatbeh M, Abdul-Razzak KK. Neuropathic pain is not associated with serum vitamin D but is associated with female gender in patients with type 2 diabetes mellitus. BMJ Open Diabetes Res Care. 2019;7(1):e000690. doi:10.1136/bmjdrc-2019-000690
17. Rutstein BH, Gmuca S, Gerber JS, Lim T, Argraves M, Ogdie A. Validation of coding algorithms for the identification of herpes zoster among children. Pharmacoepidemiol Drug Saf. 2021;30(9):1162–1167. doi:10.1002/pds.5264
18. Fischer V, Haffner-Luntzer M, Amling M, Ignatius A. Calcium and vitamin D in bone fracture healing and post-traumatic bone turnover. Eur Cell Mater. 2018;35:365–385. doi:10.22203/eCM.v035a25
19. Harrison SR, Li D, Jeffery LE, Raza K, Hewison M. Vitamin D, autoimmune disease and rheumatoid arthritis. Calcif Tissue Int. 2020;106(1):58–75. doi:10.1007/s00223-019-00577-2
20. AlGhamdi SA. Effectiveness of vitamin D on neurological and mental disorders. Diseases. 2024;12(6):131. doi:10.3390/diseases12060131
21. Durá-Travé T, Gallinas-Victoriano F. Pregnancy, breastfeeding, and vitamin D. Int J Mol Sci. 2023;24(15):11881. doi:10.3390/ijms241511881
22. Sempos CT, Heijboer AC, Bikle DD, et al. Vitamin D assays and the definition of hypovitaminosis D: results from the first international conference on controversies in vitamin D. Br J Clin Pharmacol. 2018;84(10):2194–2207. doi:10.1111/bcp.13652
23. Bertoldo F, Cianferotti L, Di Monaco M, et al. Definition, assessment, and management of vitamin D inadequacy: suggestions, recommendations, and warnings from the italian society for osteoporosis, mineral metabolism and bone diseases (SIOMMMS). Nutrients. 2022;14(19):4148. doi:10.3390/nu14194148
24. Ross AC. The 2011 report on dietary reference intakes for calcium and vitamin D. Public Health Nutr. 2011;14(5):938–939. doi:10.1017/S1368980011000565
25. Seetan K, Albashir S, Jarrar B, et al. Assessment of serum vitamin D levels in the serum of patients with postherpetic neuralgia and its correlation to pain severity: a cross-sectional comparative study. Int J Clin Pract. 2021;75(11):e14750. doi:10.1111/ijcp.14750
26. Mut Surmeli D, Surmeli ZG, Bahsi R, et al. Vitamin D deficiency and risk of Helicobacter pylori infection in older adults: a cross-sectional study. Aging Clin Exp Res. 2019;31(7):985–991. doi:10.1007/s40520-018-1039-1
27. Forbes HJ, Bhaskaran K, Thomas SL, et al. Quantification of risk factors for postherpetic neuralgia in herpes zoster patients: a cohort study. Neurology. 2016;87(1):94–102. doi:10.1212/wnl.0000000000002808
28. Garcion E, Sindji L, Montero-Menei C, Andre C, Brachet P, Darcy F. Expression of inducible nitric oxide synthase during rat brain inflammation: regulation by 1,25-dihydroxyvitamin D3. Glia. 1998;22(3):282–294. doi:10.1002/(SICI)1098-1136(199803)22:3<282::AID-GLIA7>3.0.CO;2-7
29. Chao CT, Chiang CK, Huang JW, Hung KY. Vitamin D is closely linked to the clinical courses of herpes zoster: from pathogenesis to complications. Med Hypotheses. 2015;85(4):452–457. doi:10.1016/j.mehy.2015.06.027
30. Lin LY, Bhate K, Forbes H, Smeeth L, Warren-Gash C, Langan SM. Vitamin D deficiency or supplementation and the risk of human herpesvirus infections or reactivation: a systematic review and meta-analysis. Open Forum Infect Dis. 2021;8(1):ofaa570. doi:10.1093/ofid/ofaa570
31. Tripepi G, Fusaro M, Arcidiacono G, Sella S, Giannini S. Evaluating benefit from vitamin D supplementation: defining the area for treatment. Osteoporos Int. 2023;34(9):1531–1533. doi:10.1007/s00198-023-06802-x
32. Barbarisi M, Pace MC, Passavanti MB, et al. Pregabalin and transcutaneous electrical nerve stimulation for postherpetic neuralgia treatment. Clin J Pain. 2010;26(7):567–572. doi:10.1097/AJP.0b013e3181dda1ac
33. Sasaki A, Inomata Y, Serizawa K, Andoh T, Kuraishi Y. Contribution of sensory C-fiber neuron injury to mechanical dynamic allodynia in a murine model of postherpetic neuralgia. Neuroreport. 2013;24(3):137–141. doi:10.1097/WNR.0b013e32835df4d9
34. Guida F, Boccella S, Belardo C, et al. Altered gut microbiota and endocannabinoid system tone in vitamin D deficiency-mediated chronic pain. Brain Behav Immun. 2020;85:128–141. doi:10.1016/j.bbi.2019.04.006
35. Zhong YQ, Li KC, Zhang X. Potentiation of excitatory transmission in substantia gelatinosa neurons of rat spinal cord by inhibition of estrogen receptor alpha. Mol Pain. 2010;6:92. doi:10.1186/1744-8069-6-92
36. Ciarambino T, Crispino P, Minervini G, Giordano M. Vitamin D: can gender medicine have a role? Biomedicines. 2023;11(6):1762. doi:10.3390/biomedicines11061762
37. Tague SE, Smith PG. Vitamin D receptor and enzyme expression in dorsal root ganglia of adult female rats: modulation by ovarian hormones. J Chem Neuroanat. 2011;41(1):1–12. doi:10.1016/j.jchemneu.2010.10.001
38. Xiang Q, Xu H, Zhan J, et al. Association between the triglyceride-glucose index and vitamin D status in type 2 diabetes mellitus. Nutrients. 2023;15(3):639. doi:10.3390/nu15030639
39. Gholamzad A, Khakpour N, Kabipour T, Gholamzad M. Association between serum vitamin D levels and lipid profiles: a cross-sectional analysis. Sci Rep. 2023;13(1):21058. doi:10.1038/s41598-023-47872-5
40. Zhang L, Wan Q, Zhou Y, et al. Age-related and gender-stratified differences in the association between high triglyceride and risk of hyperuricemia. Lipids Health Dis. 2019;18(1):147. doi:10.1186/s12944-019-1077-5
41. Xia Z, Hu Y, Han Z, et al. Association of vitamin D receptor gene polymorphisms with diabetic dyslipidemia in the elderly male population in North China. Clin Interv Aging. 2017;12:1673–1679. doi:10.2147/cia.S145700
42. Hajj A, Chedid R, Chouery E, Megarbané A, Gannagé-Yared MH. Relationship between vitamin D receptor gene polymorphisms, cardiovascular risk factors and adiponectin in a healthy young population. Pharmacogenomics. 2016;17(15):1675–1686. doi:10.2217/pgs-2016-0045
43. He L, Wang M. Association of vitamin d receptor-a gene polymorphisms with coronary heart disease in Han Chinese. Int J Clin Exp Med. 2015;8(4):6224–6229.
44. Morvaridzadeh M, Agah S, Alibakhshi P, et al. Effects of calcium and vitamin D Co-supplementation on the lipid profile: a systematic review and meta-analysis. Clin Ther. 2021;43(9):274–296. doi:10.1016/j.clinthera.2021.07.018
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.