Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Sex Differences in Failure to Achieve Geriatric-Adjusted Glycemic Targets Among Older Adults with Type 2 Diabetes in Vietnam
Authors Le TD, Le PH ![]() , Bang VA, Nguyen HT
, Bang VA, Nguyen HT ![]()
Received 9 February 2026
Accepted for publication 31 May 2026
Published 10 June 2026 Volume 2026:19 601696
DOI https://doi.org/10.2147/DMSO.S601696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hillary Keenan
Thanh Dinh Le,1,2 Phuc Hoang Le,3 Vien Ai Bang,3 Huan Thanh Nguyen1,3
1Department of Cardiology, Thong Nhat Hospital, Ho Chi Minh City, Vietnam; 2Department of Geriatrics and Gerontology, Pham Ngoc Thach University of Medicine, Ho Chi Minh City, Vietnam; 3Department of Geriatrics and Gerontology, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh City, Vietnam
Correspondence: Huan Thanh Nguyen, Department of Geriatrics and Gerontology, School of Medicine, University of Medicine and Pharmacy at Ho Chi Minh City, 217 Hong Bang, Cho Lon Ward, Ho Chi Minh City, Vietnam, Tel +84 909 097 849, Email [email protected]
Background: Older adults with type 2 diabetes mellitus (T2DM) often face challenges in achieving glycemic targets due to geriatric conditions. However, evidence on sex differences in failure to achieve glycemic targets in low- and middle-income countries remains limited.
Aim: To examine sex differences in the prevalence of failure to achieve individualized glycemic targets and to identify associated factors among older adults with T2DM in Vietnam.
Methods: This cross-sectional study was conducted between September and December 2025 among outpatients aged ≥ 60 years with T2DM. Failure to achieve glycemic targets was defined based on individualized HbA1c targets according to geriatric conditions, including comorbidities, cognitive function, and functional status, in accordance with recommendations from the American Diabetes Association. Multivariable logistic regression analyses were performed in the overall population and stratified by sex.
Results: Among 537 patients, 306 (57.0%) were male and 231 (43.0%) were female. Overall, 25.5% of patients failed to achieve their glycemic targets, with a similar prevalence in males (24.8%) and females (26.4%). In the overall population, polypharmacy (adjusted odds ratio [aOR] 1.98, 95% confidence interval [CI] 1.14– 3.44), limitations in instrumental activities of daily living (IADL) (aOR 1.72, 95% CI 1.14– 2.61), and diabetes duration ≥ 5 years (aOR 2.07, 95% CI 1.15– 3.75) were independently associated with failure to achieve glycemic targets. In sex-stratified analyses, diabetes duration ≥ 5 years was associated with failure to achieve glycemic targets among males (aOR 3.30, 95% CI 1.34– 8.13), whereas dependent income (aOR 3.60, 95% CI 1.18– 10.9), polypharmacy (aOR 2.46, 95% CI 1.02– 5.95), and limitations in IADL (aOR 2.39, 95% CI 1.28– 4.46) were significantly associated with failure to achieve glycemic targets among females.
Conclusion: Failure to achieve glycemic targets remains common among older adults with T2DM in Vietnam, with sex-specific associated factors. These findings suggest that incorporating geriatric assessment and sex-sensitive approaches into outpatient diabetes management may be beneficial; however, they should be interpreted as hypothesis-generating and may not be generalizable to all settings.
Keywords: type 2 diabetes, older adults, sex differences, failure to achieve glycemic targets, geriatric assessment, Vietnam
Introduction
The world is undergoing a profound demographic transition toward population aging, and Vietnam is among the countries experiencing one of the most rapid shifts in Asia.1 In 2025, individuals aged ≥60 years accounted for approximately 14.5% of the Vietnamese population.2 Among older age groups, women outnumber men, with a sex ratio, defined as the number of females per 100 males, of 137 nationwide.3 Parallel to this demographic transition, type 2 diabetes mellitus (T2DM) has emerged as a major public health challenge, disproportionately affecting older adults. Current estimates indicate that nearly 29% of Vietnamese individuals aged ≥60 years are living with T2DM.4 In this population, T2DM frequently coexists with geriatric conditions such as frailty, depressive symptoms, and sarcopenia,5,6 which complicate disease management and challenge conventional approaches to glycemic control.
In older adults with T2DM, glycemic management extends beyond the achievement of numerical hemoglobin A1c (HbA1c) thresholds and instead reflects the need to balance potential metabolic benefits against competing risks related to comorbidity burden, functional impairment, and treatment-related adverse events.7 Age-related physiological changes, longer diabetes duration, and increasing therapeutic complexity further increase vulnerability to hypoglycemia and other adverse outcomes in this population.8–10 In recognition of these complexities, the American Diabetes Association (ADA) Standards of Care advocate for individualized glycemic targets that incorporate geriatric conditions, functional status, and treatment burden when determining appropriate HbA1c goals.11,12 Despite these recommendations, real-world evidence on the achievement of individualized glycemic targets among older adults in low- and middle-income countries remains limited. A recent study conducted in Northern Vietnam reported that 18.4% of older adults failed to achieve HbA1c targets.13 However, data from Southern Vietnam, characterized by distinct geographic, socioeconomic, and healthcare contexts, remain scarce.
Beyond chronological age, sex differences are increasingly recognized as important determinants of diabetes pathophysiology, clinical presentation, and treatment outcomes. Biological differences in body composition, insulin sensitivity, and hormonal regulation, together with sex-specific patterns of comorbidity, functional dependency, socioeconomic vulnerability, and structural factors such as access to healthcare and support systems, may influence glycemic target achievement in later life.14–16 Despite growing recognition of these factors, evidence on sex-specific patterns of glycemic target achievement in older populations remains limited globally and is particularly scarce in rapidly aging low- and middle-income settings such as Vietnam. Therefore, this study aimed to quantify the prevalence of failure to achieve individualized glycemic targets based on geriatric assessment among older adults with T2DM treated at a tertiary hospital in Southern Vietnam and to examine sex-specific differences and associated factors.
Material and Methods
Study Design, Patients, and Data Collection
This cross-sectional study was conducted between September and December 2025 among outpatients aged ≥60 years with T2DM at the Endocrinology Clinic of Thong Nhat Hospital. T2DM was diagnosed and managed in accordance with the 2025 ADA recommendations by experienced endocrinologists. All patients received standardized care, including dietary counseling, lifestyle modification, and individualized pharmacological treatment. Eligible patients were those who had received continuous T2DM management and attended monthly follow-up visits at the clinic for at least one year before enrollment.
Data were collected through face-to-face interviews conducted by trained geriatricians. When necessary, caregivers assisted in providing information. All interview data were cross-checked with electronic medical records to ensure accuracy. Exclusion criteria included acute medical conditions requiring hospitalization at baseline, severe psychiatric disorders, incomplete or missing data, or refusal to participate. All patients provided written informed consent before study participation. The study was conducted in accordance with the Declaration of Helsinki and reported in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Ethical approval was obtained from the Ethics Committee of Thong Nhat Hospital.
Sample Size Calculation
The sample size was calculated to estimate the prevalence of failure to achieve glycemic targets among older adults with T2DM in Vietnam using the following formula: n=Z21- α/2*[p*(1-p)/d2], where n is the required minimum sample size, Z1-α/2 = 1.96 corresponds to a two-sided significance level of α = 0.05 and a 95% confidence interval; p denotes the estimated prevalence of failure to achieve glycemic targets; and d is the margin of error, set at 0.035. Based on a previous study, the expected prevalence (p) was assumed to be 0.184.13 To account for potential missing data or non-response, an additional 10% was added to the calculated sample size. Accordingly, the minimum required sample size was 518 patients.
Sociodemographic, Lifestyle, and Anthropometric Variables and Comorbidities
Sociodemographic variables included age, sex (male or female), educational attainment (below senior high school or senior high school and above), and source of income (independent or dependent). Dependent income was defined as reliance on financial support from others (eg., family members or caregivers) for basic living expenses. Self-reported lifestyle factors included regular self-monitoring of blood glucose, defined as at least three times per week; regular physical activity, defined as engagement on at least five days per week; adherence to a low-sodium diet, defined as self-reported reduced salt intake; alcohol consumption, defined as intake of ≥5 units of alcohol per week; smoking status, defined as current smoking regardless of quantity or type of tobacco; and current sexual activity. Body mass index (BMI) was categorized according to the World Health Organization Asian-specific criteria. Comorbidities were ascertained through patient interviews, review of current medication prescriptions, and electronic medical records. The ten most prevalent comorbid conditions in the study population were included in the analysis.
Geriatric Assessment
All patients underwent a comprehensive geriatric assessment encompassing four domains: physical, psychological, functional, and socioeconomic. Within the physical domain, comorbidity burden was assessed using the Charlson Comorbidity Index (CCI).17 Multimorbidity was defined as the presence of two or more chronic diseases.18 Polypharmacy was defined as the concurrent use of five or more prescribed medications. Frailty was evaluated using the Program of Research to Integrate the Services for the Maintenance of Autonomy 7 (PRISMA-7), with a score ≥3 indicating frailty.19 Nutritional status was assessed using the Mini Nutritional Assessment–Short Form (MNA-SF), with scores ≤7 indicating malnutrition.20 Risk of falls was assessed using the Stopping Elderly Accidents, Deaths, and Injuries (STEADI) screening tool; patients were classified as being at risk of falls if they responded affirmatively to any of the screening questions.21
Within the psychological domain, cognitive function was assessed using the Mini-Cog, which combines a three-item recall test with a clock-drawing task. A score <3 was considered indicative of possible cognitive impairment.22 Depressive symptoms were assessed using the 15-item Geriatric Depression Scale (GDS-15), with scores ≥5 indicating depression.23
Within the functional domain, basic activities of daily living (ADL) were assessed using the Katz Index of Independence in ADL, which evaluates six functions: bathing, dressing, toileting, transferring, continence, and feeding. Limitations in ADL were defined as a Katz Index score of 0–5.24 Instrumental activities of daily living (IADL) were assessed using the Lawton–Brody IADL Scale, which evaluates abilities including use of the telephone, shopping, meal preparation, housekeeping, laundry, transportation, medication management, and financial management. Limitations in IADL were defined as a score of 0–7.25
Within the socioeconomic domain, social engagement was assessed using the Lubben Social Network Scale–6 (LSNS-6), which evaluates the size and frequency of social interactions with family and friends. A score <12 was considered indicative of social isolation and limited social support.26 Health-related quality of life (HRQoL) was assessed using the EQ-5D-5L instrument.27 Poor HRQoL was defined using a combined criterion: patients were classified as having poor HRQoL if they had an EQ-5D-5L utility score <0.8 and an EQ visual analogue scale (EQ-VAS) score <70. These thresholds were used to indicate clinically relevant impairment in overall health status and for both descriptive and analytical purposes. Social frailty was assessed using the Makizako Social Frailty Index, with a score ≥2 indicating social frailty.28
Diabetes-Related Characteristics, Laboratory Assessment, and Glycemic Control Classification
Diabetes-related characteristics included diabetes duration and current antidiabetic treatment. Diabetes duration was defined as the time interval, in years, from the initial diagnosis of diabetes to the date of study enrollment. Information on antidiabetic medications was obtained from current prescriptions and included metformin, sulfonylureas, dipeptidyl peptidase-4 inhibitors, glucagon-like peptide-1 receptor agonists, sodium–glucose cotransporter-2 inhibitors, and insulin, as predefined variables. Blood samples were collected at baseline according to standard hospital procedures. HbA1c was measured from venous whole blood using high-performance liquid chromatography with the ADAMS A1c HA-8190V analyzer (ARKRAY Inc., Japan) and reported as a percentage.
Glycemic targets were individualized according to overall health status, in accordance with the 2025 ADA Standards of Care for older adults with T2DM.11 In this study, glycemic targets were defined as follows. Patients with a healthy status, characterized by few comorbidities (CCI <3), preserved cognitive function (Mini-Cog score = 5), and intact functional status (ADL score = 6 and IADL score = 8), were assigned a target HbA1c of <7.0%. Patients with an intermediate health status, defined by multiple comorbidities (CCI ≥3) or mild cognitive impairment (Mini-Cog score 3–4), together with functional limitations (ADL score = 4–5 and IADL score = 7), were assigned a target HbA1c of <7.5%. Patients with a complex health status, characterized by severe comorbidities, significant cognitive impairment (Mini-Cog score <3), marked functional limitations (ADL score 0–3 or IADL score 0–6), or frailty, were assigned a target HbA1c of <8.0%.
Patients were subsequently categorized into two groups according to glycemic control status: achieved and failed to achieve. Failure to achieve glycemic targets was defined as an HbA1c value equal to or exceeding the individualized threshold for each health status category. Medication adherence was assessed using the 5-item Medication Adherence Report Scale (MARS-5), with total scores ranging from 5 to 25. Good adherence was defined as a total score of 25, and suboptimal adherence as a score <25.29
Statistical Analysis
All statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were presented as mean ± standard deviation (SD) for normally distributed data or as median with interquartile range (IQR; 25th–75th percentiles) for non-normally distributed data. Normality was assessed using the Kolmogorov–Smirnov test. Between-group comparisons were conducted using the independent-samples t test for normally distributed variables and the Mann–Whitney U-test for non-normally distributed variables. Categorical variables were presented as frequencies and percentages and compared using the chi-square test or Fisher’s exact test, as appropriate.
Logistic regression analyses were performed to identify factors associated with failure to achieve glycemic targets. Variables were selected for multivariable models based on both univariate screening (P <0.20) and clinical relevance informed by prior literature. Multicollinearity was assessed using the variance inflation factor (VIF), with values >5 indicating multicollinearity. Model adequacy and stability were evaluated using the events-per-variable (EPV) criterion, with a predefined threshold of ≥15 events per variable. Sensitivity analyses were performed to assess the robustness of the findings under alternative model specifications. Results are reported as odds ratios (ORs) with 95% confidence intervals (CIs). All tests were two-tailed, and a P value <0.05 was considered statistically significant.
Results
Of the 589 patients with T2DM attending the Endocrinology Clinic during the study period, 42 were excluded because they had been diagnosed with T2DM for less than one year (n = 31), required hospitalization at baseline (n = 5), or had missing data (n = 6). The flow diagram of patient selection is presented in Supplementary Figure S1. The final study sample comprised 537 older adults with T2DM, with a median age of 70 years (IQR, 64.5–75.0; range, 60–90 years). Males accounted for 57.0% of the study population. A total of 311 participants (57.9%) were classified as having a healthy status, 9 (1.7%) as intermediate status, and 217 (40.4%) as complex status. Overall, 25.5% of patients (n = 137) failed to achieve glycemic targets, with a similar prevalence in males (24.8%) and females (26.4%).
Table 1 summarizes the sociodemographic, anthropometric, geriatric, and lifestyle characteristics of the study population according to glycemic target achievement status. Sociodemographic variables, anthropometric measures, and self-reported lifestyle factors were largely comparable between patients who achieved glycemic targets and those who failed to achieve them. In contrast, polypharmacy (38.7% vs 27.0%) and limitations in IADL (52.6% vs 38.3%) were more prevalent among patients who failed to achieve glycemic targets.
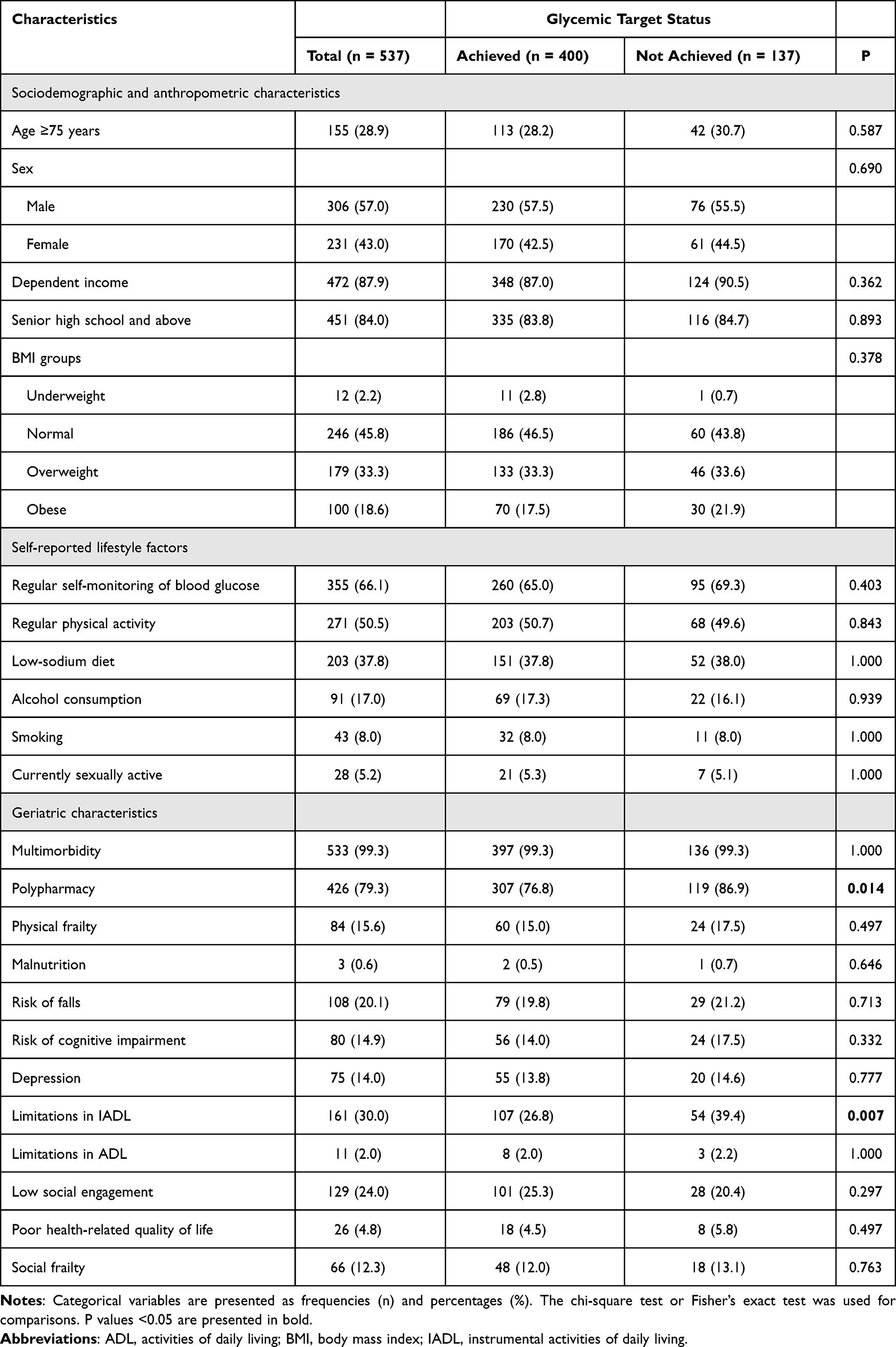 |
Table 1 Sociodemographic, Anthropometric, Geriatric, and Lifestyle Characteristics of the Study Population |
Table 2 presents diabetes-related characteristics and comorbidities of the study population. Patients who failed to achieve glycemic targets more frequently had a longer diabetes duration (≥5 years: 78.1% vs 64.1%). The distribution of glucose-lowering therapies, including oral antidiabetic agents and insulin, was similar between groups. Comorbid conditions were common across the study population and did not differ substantially by glycemic target achievement status.
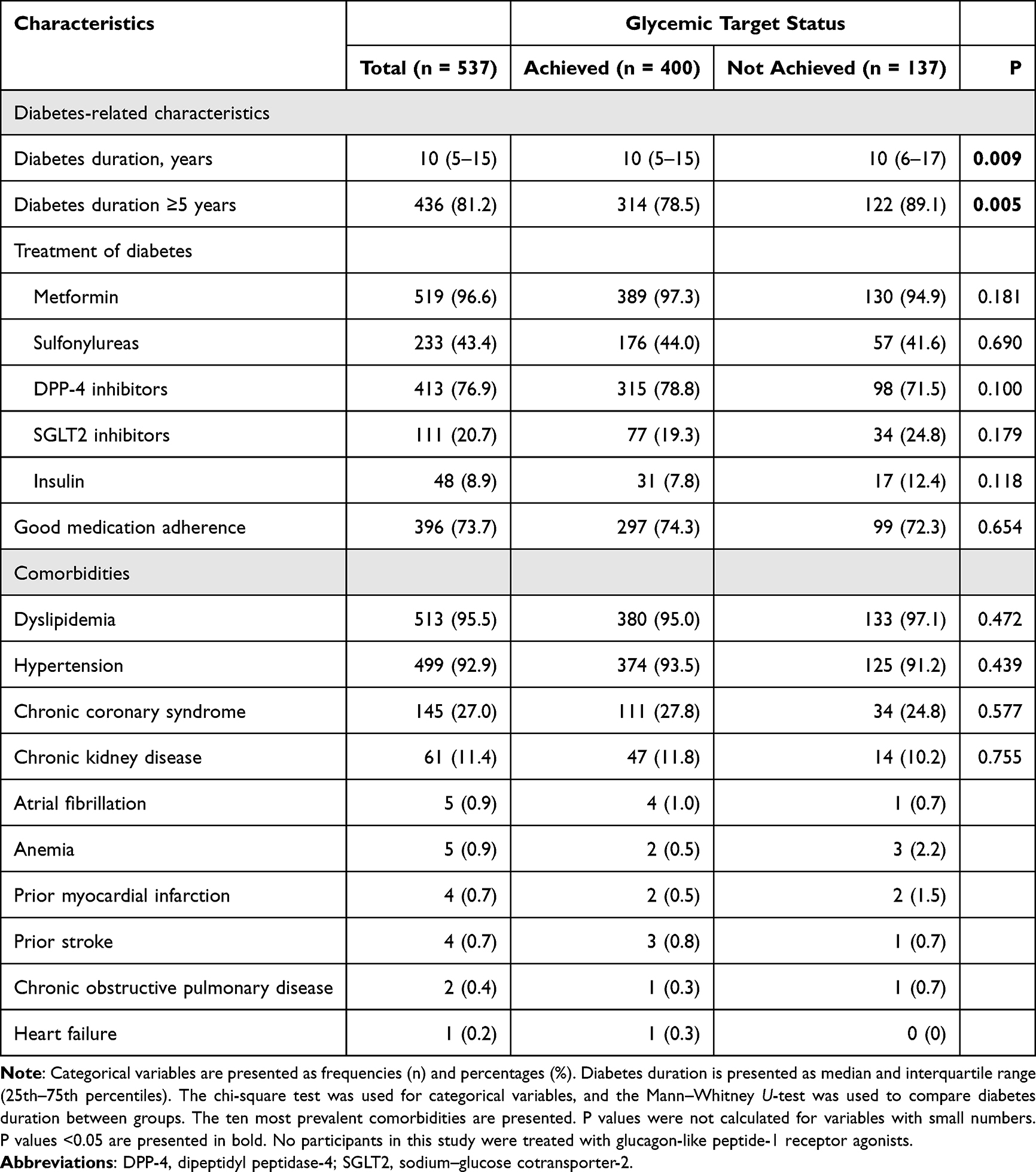 |
Table 2 Diabetes-Related Characteristics and Comorbidities of the Study Population |
To further characterize older adults with T2DM by sex, characteristics of males (Table 3) and females (Table 4) were analyzed according to glycemic target achievement status. Sex-based comparisons are presented in Supplementary Table S1. Among males, most characteristics were similar between groups; however, a longer diabetes duration was more common among those who failed to achieve glycemic targets (84.2% vs 67.4%). Among females, failure to achieve glycemic targets was primarily associated with socioeconomic and functional characteristics, including dependent income (21.3% vs 9.4%) and limitations in IADL (60.7% vs 41.8%), whereas other characteristics were generally comparable between groups.
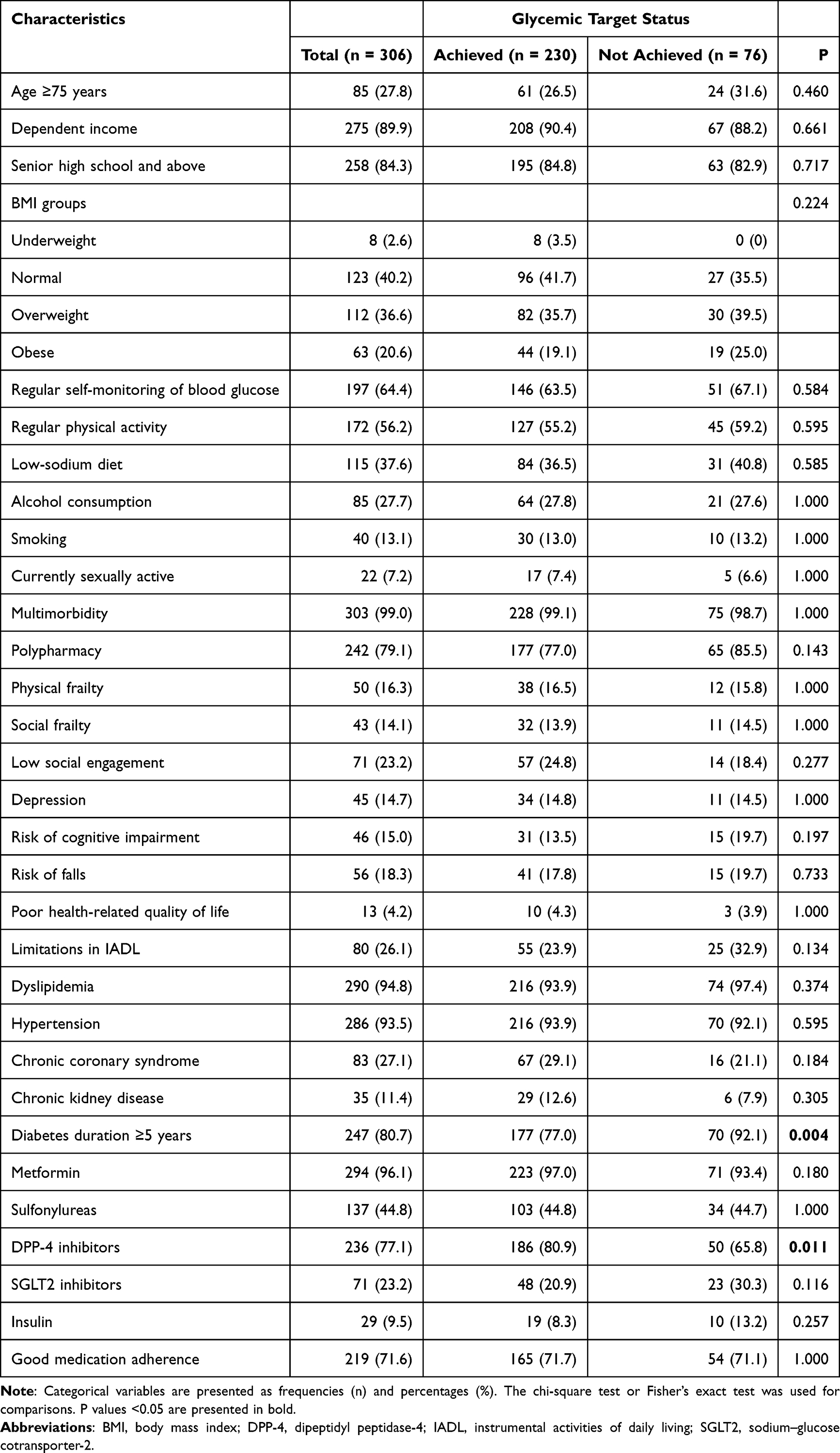 |
Table 3 Baseline Characteristics of Males |
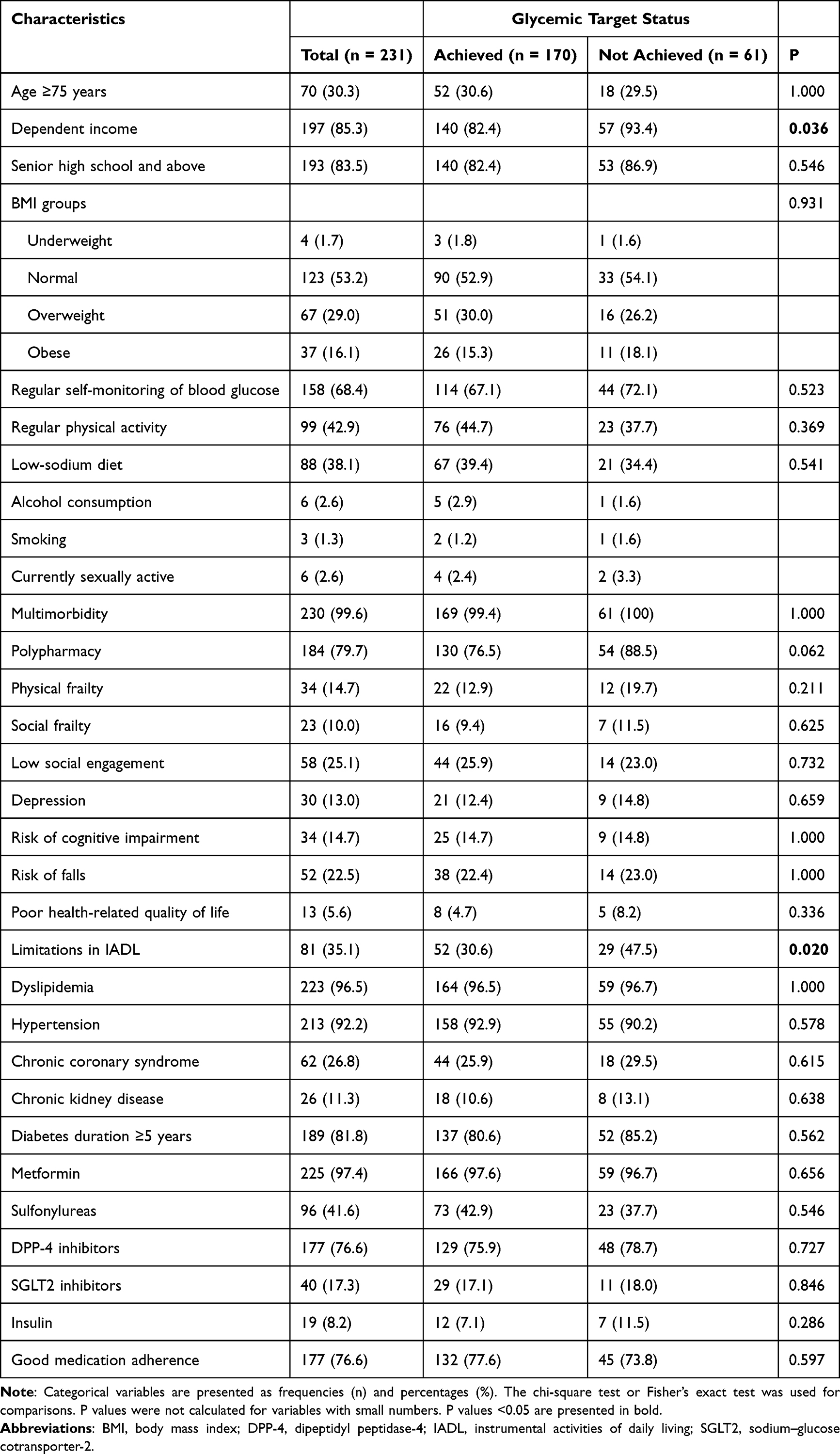 |
Table 4 Baseline Characteristics of Females |
Table 5 summarizes factors associated with failure to achieve glycemic targets in the overall study population and in sex-stratified analyses. In the overall population, polypharmacy (adjusted odds ratio [aOR] 1.98, 95% confidence interval [CI] 1.14–3.44), limitations in IADL (aOR 1.72, 95% CI 1.14–2.61), and diabetes duration ≥5 years (aOR 2.07, 95% CI 1.15–3.75) were independently associated with failure to achieve glycemic targets. In sex-stratified analyses, diabetes duration ≥5 years was associated with failure to achieve glycemic targets among males (aOR 3.30, 95% CI 1.34–8.13), whereas dependent income (aOR 3.60, 95% CI 1.18–10.9), polypharmacy (aOR 2.46, 95% CI 1.02–5.95), and limitations in IADL (aOR 2.39, 95% CI 1.28–4.46) were associated with failure to achieve glycemic targets among females. Factors associated with failure to achieve fixed glycemic targets in the overall population and in sex-stratified analyses are presented in Supplementary Table S2. A summary of model performance and multicollinearity diagnostics is provided in Supplementary Table S3.
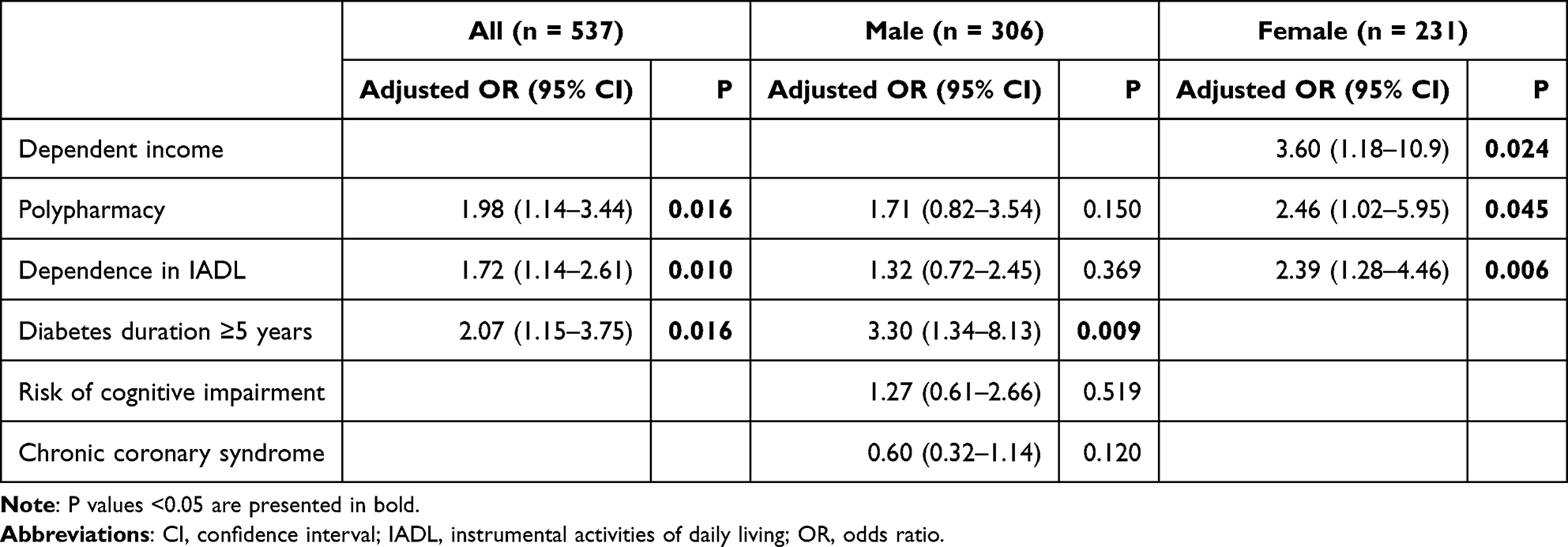 |
Table 5 Factors Associated with Failure to Achieve Glycemic Targets in the Overall Population and by Sex |
Discussion
In this cross-sectional study of older outpatients with T2DM in Southern Vietnam, approximately one-quarter of patients failed to achieve individualized glycemic targets. Although the overall prevalence of failure to achieve glycemic targets was similar between males and females, the factors associated with failure to achieve glycemic targets differed by sex. In the overall study population, polypharmacy, limitations in IADL, and longer diabetes duration were independently associated with failure to achieve glycemic targets. Sex-stratified analyses demonstrated distinct patterns, whereby longer diabetes duration was the primary factor associated with failure to achieve glycemic targets among males, whereas dependent income, polypharmacy, and functional limitations were more strongly associated with failure to achieve glycemic targets among females.
Prevalence of Failure to Achieve Glycemic Targets in Older Adults with T2DM
In the general population with T2DM, failure to achieve glycemic targets remains highly prevalent worldwide despite advances in glucose-lowering therapies and the implementation of updated clinical guidelines. A large meta-analysis including 63 studies and more than 1.6 million individuals reported that approximately 56% of patients with T2DM failed to achieve guideline-recommended HbA1c targets in routine clinical practice.30 This burden appears even greater in low- and middle-income countries, where a recent systematic review demonstrated that nearly 69% of adults with T2DM had inadequate glycemic control, defined as an HbA1c level ≥7.0%.31 In Vietnam, available evidence similarly indicates that failure to achieve glycemic targets remains common, with one study reporting that 51.9% of adults with T2DM failed to achieve an HbA1c level <7.0%.32 Together, these findings indicate that failure to achieve glycemic targets is a global challenge across diverse healthcare settings.
Among older adults with T2DM, glycemic management is further complicated by the need to balance potential metabolic benefits against increased risks of hypoglycemia, treatment burden, and adverse outcomes related to multimorbidity, cognitive impairment, and functional decline. Accordingly, contemporary clinical guidelines emphasize the individualization of glycemic targets based on overall health status, life expectancy, and cognitive and functional capacity, rather than applying uniform HbA1c goals to all patients.11 However, at the global level, data on failure to achieve individualized glycemic targets remain limited. Most existing studies continue to classify glycemic control using fixed HbA1c thresholds and do not systematically incorporate geriatric conditions when evaluating glycemic outcomes in older adults. Consequently, the prevalence of failure to achieve glycemic targets based on health status–specific criteria remains poorly characterized.
This limitation is illustrated by the KASEHPAD study conducted among nursing home residents aged ≥60 years, in which 57.3% of patients with T2DM failed to achieve a fixed HbA1c threshold of <7.0%.33 In contrast, studies applying individualized HbA1c targets have reported lower rates of failure to achieve glycemic targets. For example, a study conducted among outpatients aged ≥60 years in Northern Vietnam, which individualized HbA1c targets according to geriatric conditions, reported that 18.4% of patients failed to achieve their glycemic targets.13 Consistent with these findings, our study in Southern Vietnam found that 25.5% of older adults with T2DM failed to achieve individualized glycemic targets. Taken together, these findings suggest that when glycemic targets are appropriately individualized based on geriatric health status, the prevalence of failure to achieve glycemic targets among older adults may be lower than that observed in the general population with T2DM.
This distinction is clinically relevant, as older adults with complex health status may be appropriately assigned less stringent glycemic targets, such as an HbA1c level <8.0%, to minimize the risk of hypoglycemia and other treatment-related adverse events, rather than aiming for a universal target of <7.0%. Beyond the use of individualized HbA1c targets, certain characteristics of our study population may also explain the relatively lower prevalence of failure to achieve glycemic targets. First, our study included stable outpatients receiving regular follow-up at a tertiary care center, which may reflect better treatment adherence and closer clinical monitoring than community-based older populations. Second, the exclusion of patients with acute medical conditions may have contributed to the lower observed prevalence of failure to achieve glycemic targets. Together, these factors may explain the lower frequency of failure to achieve glycemic targets observed in our study compared with previous investigations using fixed HbA1c thresholds.
Sex-related differences in failure to achieve glycemic targets among individuals with T2DM have been reported inconsistently across studies. Several investigations in the general T2DM population have suggested that women may have a higher likelihood of failure to achieve glycemic targets than men, potentially attributable to differences in adiposity, hormonal factors, socioeconomic status, and access to healthcare.34–37 However, a large study involving more than 200,000 adults with T2DM in a multi-ethnic middle-income Asian country demonstrated that sex differences in glycemic control varied by age group, with women exhibiting poorer glycemic control than men in middle age but better control after the age of 60 years.38 In the present study, the prevalence of failure to achieve glycemic targets was numerically higher among females than males, although the difference was not statistically significant, highlighting the complex interplay of biological, functional, and social determinants of glycemic control in later life.
In older adults, sex-specific patterns of failure to achieve glycemic targets may be further shaped by differences in functional status and social context. Studies in older Asian populations with T2DM have reported that women are more likely to experience physical frailty,6 lower health-related quality of life, socioeconomic dependency, and longer survival with chronic disease,39 all of which may adversely affect diabetes self-management and medication adherence. In addition, biological factors such as age-related changes in body composition, hormonal milieu, and insulin sensitivity may differentially influence glycemic regulation between older men and women.14,40 Social determinants, including access to resources, caregiving roles, and health-seeking behaviors, may further contribute to these differences.41 In contrast, older men more frequently have a longer diabetes duration and a higher cardiometabolic risk burden,39 factors that may predispose them to failure to achieve glycemic targets through different pathways. These mechanisms may contribute to a similar overall prevalence of failure to achieve glycemic targets despite distinct sex-specific associated factors.
Factors Associated with Failure to Achieve Glycemic Targets in Older Adults with T2DM
In the overall study population, failure to achieve glycemic targets was independently associated with polypharmacy, limitations in IADL, and longer diabetes duration, reflecting the potential interplay of treatment burden, functional vulnerability, and disease chronicity in relation to glycemic target achievement in older adults. Notably, polypharmacy and longer diabetes duration were each associated with approximately twofold higher odds of failure to achieve glycemic targets, suggesting a potential impact of treatment complexity and disease chronicity. Polypharmacy not only reflects greater clinical complexity but has also been associated with adverse diabetes-related outcomes, including poorer glycemic control and an increased risk of hypoglycemia, as well as broader health outcomes.42 Similarly, limitations in IADL were associated with a moderate increase in risk, underscoring the importance of functional capacity in diabetes self-management. Limitations in IADL may reflect reduced ability to perform essential diabetes self-management tasks, highlighting the potential role of functional status, beyond chronological age, in achieving individualized glycemic targets.43,44 In addition, longer diabetes duration reflects cumulative metabolic burden and disease progression, which may be associated with increasing difficulty in maintaining glycemic control over time.45 However, given the cross-sectional design, these associations should be interpreted with caution, as reverse causality cannot be excluded.
In males, longer diabetes duration was the only independent factor associated with failure to achieve glycemic targets, suggesting a role of disease chronicity and biological progression in this group. Long-standing T2DM is characterized by progressive β-cell dysfunction and declining endogenous insulin secretion,46 which may outweigh the influence of functional or socioeconomic factors in older men. The absence of significant associations with functional dependence or income status among males suggests that failure to achieve glycemic targets in this group may be more closely related to intrinsic disease severity rather than contextual factors. These findings support the importance of timely treatment optimization and proactive clinical monitoring in older men with long-standing T2DM to mitigate the impact of disease progression on glycemic target achievement.
In contrast, among females, failure to achieve glycemic targets was independently associated with dependent income, polypharmacy, and limitations in IADL, highlighting the role of socioeconomic and functional vulnerability in shaping glycemic outcomes. The magnitude of these associations suggests that financial dependency and functional impairment may affect glycemic management in older women. Economic dependency may limit access to healthcare resources and continuity of treatment, while polypharmacy increases regimen complexity and may affect medication adherence.42,47 Limitations in IADL further reflect reduced ability to manage complex diabetes-related tasks required for glycemic control.43,44 Unlike in males, these findings suggest that contextual and geriatric factors may contribute to failure to achieve glycemic targets in older women. Accordingly, interventions focusing on treatment simplification, functional support, and the mitigation of socioeconomic barriers may be relevant for improving glycemic outcomes in this population.
This study has some features that may strengthen the validity of the findings, including the use of individualized glycemic targets based on geriatric assessment and the incorporation of sex-stratified analyses. However, several limitations should be acknowledged. First, the cross-sectional design precludes causal inference between the identified factors and failure to achieve glycemic targets. Second, the study was conducted at a single tertiary care center and required ongoing follow-up, which may have selected patients with more stable disease and greater engagement with healthcare services. As a result, the findings may not fully reflect glycemic control patterns in the broader community, particularly in primary care or underserved settings, and the prevalence of failure to achieve glycemic targets may be underestimated. Third, although a comprehensive geriatric assessment was performed, some variables were self-reported and may be subject to recall and social desirability bias. Fourth, the assessment of glycemic control relied solely on HbA1c, which may not fully capture the complexity and appropriateness of glycemic management in older adults. Clinically relevant measures, such as hypoglycemic events, glycemic variability, time in range, and detailed treatment-related factors (including medication dosage, treatment intensity, and therapeutic adjustments), were not systematically collected, which may limit the interpretation of glycemic control in a geriatric context. Fifth, variable selection for multivariable models was partly based on statistical criteria from univariate analyses, which may have resulted in the exclusion of some clinically relevant confounders. Sixth, residual confounding from unmeasured factors, including caregiver involvement and healthcare access, cannot be excluded. In addition, some variables, such as medication adherence and nutritional status, were not included in multivariable models due to limited relevance or variability. Finally, although analyses were stratified by sex, the sample size within subgroups may have limited statistical power to detect smaller sex-specific associations. Residual confounding by unmeasured factors, such as social support or caregiver involvement, also cannot be excluded.
Conclusions
Failure to achieve individualized glycemic targets remains common among older adults with T2DM in Vietnam when assessed using geriatric-based criteria. Although the overall prevalence was similar between males and females, the associated factors differed by sex, with longer diabetes duration predominating among males and functional, socioeconomic, and treatment-related factors more relevant among females. These findings suggest that incorporating comprehensive geriatric assessment and sex-sensitive approaches may help individualize glycemic targets and optimize diabetes management in older adults with T2DM.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Ethics Committee of Thong Nhat Hospital (Approval No. 153/2025/CN-BVTN-HĐĐĐ). Patient confidentiality and data anonymity were strictly maintained throughout data collection and analysis. Written informed consent was obtained from all patients or their legal representatives prior to participation.
Consent for Publication
All patients provided written consent for the publication of the study results, including anonymized data.
Acknowledgments
The authors thank the patients for their participation in this study.
Author Contributions
Thanh Dinh Le: Conceptualization, Funding acquisition, Investigation, Methodology, Resources, Software, Writing – original draft, Writing – review & editing. Phuc Hoang Le: Data curation, Formal analysis, Investigation, Resources, Software, Writing – original draft. Vien Ai Bang: Data curation, Formal analysis, Investigation, Resources, Software, Writing – original draft. Huan Thanh Nguyen: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Handong L, Ngoc NH, Tianmin Z. Vietnam’s Population Projections and Aging Trends from 2010 to 2049. J Popul Ageing. 2021;14(2):165–15. doi:10.1007/s12062-019-09257-3
2. Global Population Demographics. Vietnam Population Pyramid. 2025. Available from: https://www.populationpyramids.org/vietnam.
3. General Statistics Office of Viet Nam. Older persons in Viet Nam: an analysis of the Population Change and Family Planning Survey. 2021. Available from: https://vietnam.unfpa.org/en/publications/older-persons-viet-nam-analysis-population-change-and-family-planning-survey-2021.
4. Nguyen HT, Nguyen AH, Nguyen GTX. Prevalence and associated factors of frailty in patients attending rural and urban geriatric clinics. Australas J Ageing. 2022;41(2):e122–e130. doi:10.1111/ajag.13016
5. Trinh AN, Lvh H, Dinh TH, et al. Sarcopenia and depression: a strong association in older adults with type 2 diabetes in Vietnam. BMC Geriatr. 2026. doi:10.1186/s12877-026-07044-2
6. Nguyen HT, Nguyen AH, Ptm L. Sex differences in frailty of geriatric outpatients with type 2 diabetes mellitus: a multicentre cross-sectional study. Sci Rep. 2022;12(1):16122. doi:10.1038/s41598-022-20678-7
7. Lee SJ, Eng C. Goals of glycemic control in frail older patients with diabetes. JAMA. 2011;305(13):1350–1351. doi:10.1001/jama.2011.404
8. Kim KS, Kim SK, Sung KM, Cho YW, Park SW. Management of type 2 diabetes mellitus in older adults. Diabetes Metab J. 2012;36(5):336–344. doi:10.4093/dmj.2012.36.5.336
9. Gates BJ, Walker KM. Physiological Changes in Older Adults and Their Effect on Diabetes Treatment. Diabetes Spectr. 2014;27(1):20–28. doi:10.2337/diaspect.27.1.20
10. Bellary S, Kyrou I, Brown JE, Bailey CJ. Type 2 diabetes mellitus in older adults: clinical considerations and management. Nat Rev Endocrinol. 2021;17(9):534–548. doi:10.1038/s41574-021-00512-2
11. American Diabetes Association Professional Practice C. Older Adults: standards of Care in Diabetes-2025. Diabetes Care. 2025;48(Suppl 1):S266–S282. doi:10.2337/dc25-S013.
12. American Diabetes Association Professional Practice Committee for D. Older Adults: standards of Care in Diabetes-2026. Diabetes Care. 2026;49(Supplement_1):S277–S296. doi:10.2337/dc26-S013
13. Htt V, Nguyen TTH, Dinh HT, et al. Achievement of Glycated Hemoglobin Targets and Some Associated Factors in Older Adults with Type 2 Diabetes in Vietnam: a Cross-Sectional Study. Clinical Diabetol. 2026. doi:10.5603/cd.109316
14. Kautzky-Willer A, Harreiter J, Pacini G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr Rev. 2016;37(3):278–316. doi:10.1210/er.2015-1137
15. Joung KI, Jung GW, Park HH, Lee H, Park SH, Shin JY. Gender differences in adverse event reports associated with antidiabetic drugs. Sci Rep. 2020;10(1):17545. doi:10.1038/s41598-020-74000-4
16. Kautzky-Willer A, Leutner M, Harreiter J. Sex differences in type 2 diabetes. Diabetologia. 2023;66(6):986–1002. doi:10.1007/s00125-023-05891-x
17. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
18. Vetrano DL, Palmer K, Marengoni A, et al. Frailty and Multimorbidity: a Systematic Review and Meta-analysis. J Gerontol a Biol Sci Med Sci. 2019;74(5):659–666. doi:10.1093/gerona/gly110
19. Raiche M, Hebert R, Dubois MF. PRISMA-7: a case-finding tool to identify older adults with moderate to severe disabilities. Arch Gerontol Geriatr. 2008;47(1):9–18. doi:10.1016/j.archger.2007.06.004
20. Kaiser MJ, Bauer JM, Ramsch C, et al. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging. 2009;13(9):782–788. doi:10.1007/s12603-009-0214-7
21. Stevens JA, Phelan EA. Development of STEADI: a fall prevention resource for health care providers. Health Promot Pract. 2013;14(5):706–714. doi:10.1177/1524839912463576
22. Borson S, Scanlan J, Brush M, Vitaliano P, Dokmak A. The mini-cog: a cognitive ‘vital signs’ measure for dementia screening in multi-lingual elderly. Int J Geriatr Psychiatry. 2000;15(11):1021–1027. doi:10.1002/1099-1166(200011)15:11<1021::aid-gps234>3.0.co;2-6
23. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. Clin Gerontologist. 1986;5:165–173. doi:10.1300/J018v05n01_09
24. Shelkey M, Wallace M. Katz Index of Independence in Activities of Daily Living. J Gerontol Nurs. 1999;25(3):8–9. doi:10.3928/0098-9134-19990301-05
25. Graf C. The Lawton instrumental activities of daily living scale. Am J Nurs Apr. 2008;108(4):
26. Lubben J, Blozik E, Gillmann G, et al. Performance of an abbreviated version of the Lubben Social Network Scale among three European community-dwelling older adult populations. Gerontologist. 2006;46(4):503–513. doi:10.1093/geront/46.4.503
27. Zhou T, Guan H, Wang L, Zhang Y, Rui M, Ma A. Health-Related Quality of Life in Patients With Different Diseases Measured With the EQ-5D-5L: a Systematic Review. Front Public Health. 2021;9:675523. doi:10.3389/fpubh.2021.675523
28. Makizako H, Shimada H, Tsutsumimoto K, et al. Social Frailty in Community-Dwelling Older Adults as a Risk Factor for Disability. J Am Med Dir Assoc. 2015;16(11):1003. doi:10.1016/j.jamda.2015.08.023
29. Chan AHY, Horne R, Hankins M, Chisari C. The Medication Adherence Report Scale: a measurement tool for eliciting patients’ reports of nonadherence. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/bcp.14193
30. Kacha G, Highton PJ, Funnell MP, et al. Global guideline recommended target achievements in glycaemic, blood pressure, and lipid control in type 2 diabetes: an updated meta-analysis of 1,618,972 participants. Diabet Res Clin Pract. 2025;230:113001. doi:10.1016/j.diabres.2025.113001
31. Siddiquea BN, Magliano DJ, Chowdhury HA, et al. Glycaemic control and its related factors among people with type 2 diabetes in low- and middle-income countries: a systematic review and meta-analysis. Front Clin Diabetes Healthc. 2025;6:1695235. doi:10.3389/fcdhc.2025.1695235
32. Nguyen VB, Thi KHP, Nguyen TX, Pham NTL, Nguyen VVH, Van Le C. Diabetes self-management and its associated factors among patients with diabetes in central Vietnam: a cross-sectional study. PLoS One. 2022;17(7):e0270901. doi:10.1371/journal.pone.0270901
33. Tabue-Teguo M, Simo N, Rambhojan C, et al. Prevalence and characteristics of older adults with type 2 diabetes mellitus living in French Caribbean nursing homes: results from the baseline KASEHPAD study. Aging Clin Exp Res. 2025;37(1):103. doi:10.1007/s40520-025-03008-5
34. Arnetz L, Ekberg NR, Alvarsson M. Sex differences in type 2 diabetes: focus on disease course and outcomes. Diabetes Metab Syndr Obes. 2014;7:409–420. doi:10.2147/DMSO.S51301
35. Gd F, da Silva Moreira S, Almeida M, et al. Sex differences and correlates of poor glycaemic control in type 2 diabetes: a cross-sectional study in Brazil and Venezuela. BMJ Open. 2019;9(3):e023401. doi:10.1136/bmjopen-2018-023401
36. Cambra K, Galbete A, Forga L, et al. Sex and age differences in the achievement of control targets in patients with type 2 diabetes: results from a population-based study in a South European region. BMC Fam Pract. 2016;17(1):144. doi:10.1186/s12875-016-0533-9
37. Choe SA, Kim JY, Ro YS, Cho SI. Women are less likely than men to achieve optimal glycemic control after 1 year of treatment: a multi-level analysis of a Korean primary care cohort. PLoS One. 2018;13(5):e0196719. doi:10.1371/journal.pone.0196719
38. Ang SH, Lim LL, Mustapha FI, Ahmad E, Rampal S. Association between sex, age, temporal trends, and glycemic control of 221,769 adults with type 2 diabetes in a multi-ethnic middle-income Asian country. Diabet Res Clin Pract. 2025;220:111976. doi:10.1016/j.diabres.2024.111976
39. Jeong H, Park K. Sex differences in health-related quality of life among older Korean adults with type 2 diabetes mellitus: a cross-sectional study. Korean J Community Nutr. 2024;29(4):336–347. doi:10.5720/kjcn.2024.00003
40. Mauvais-Jarvis F. Gender differences in glucose homeostasis and diabetes. Physiol Behav. 2018;187:20–23. doi:10.1016/j.physbeh.2017.08.016
41. Agardh E, Allebeck P, Hallqvist J, Moradi T, Sidorchuk A. Type 2 diabetes incidence and socio-economic position: a systematic review and meta-analysis. Int J Epidemiol. 2011;40(3):804–818. doi:10.1093/ije/dyr029
42. Remelli F, Ceresini MG, Trevisan C, Noale M, Volpato S. Prevalence and impact of polypharmacy in older patients with type 2 diabetes. Aging Clin Exp Res. 2022;34(9):1969–1983. doi:10.1007/s40520-022-02165-1
43. Kalyani RR, Saudek CD, Brancati FL, Selvin E. Association of diabetes, comorbidities, and A1C with functional disability in older adults: results from the National Health and Nutrition Examination Survey (NHANES), 1999–2006. Diabetes Care. 2010;33(5):1055–1060. doi:10.2337/dc09-1597
44. Yau CK, Eng C, Cenzer IS, Boscardin WJ, Rice-Trumble K, Lee SJ. Glycosylated hemoglobin and functional decline in community-dwelling nursing home-eligible elderly adults with diabetes mellitus. J Am Geriatr Soc. 2012;60(7):1215–1221. doi:10.1111/j.1532-5415.2012.04041.x
45. Khattab M, Khader YS, Al-Khawaldeh A, Ajlouni K. Factors associated with poor glycemic control among patients with type 2 diabetes. J Diabetes Complications. 2010;24(2):84–89. doi:10.1016/j.jdiacomp.2008.12.008
46. Porte Jr D, Kahn SE. Beta-cell dysfunction and failure in type 2 diabetes: potential mechanisms. Diabetes. 2001;50(Suppl 1):S160–S163. doi:10.2337/diabetes.50.2007.s160.
47. Pourhabibi N, Mohebbi B, Sadeghi R, et al. Determinants of Poor Treatment Adherence among Patients with Type 2 Diabetes and Limited Health Literacy: a Scoping Review. J Diabetes Res. 2022;2022:2980250. doi:10.1155/2022/2980250
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.