Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Sex -Specific Differences in the Association Between Metabolic Syndrome and Carotid Intima-Media Thickness Among a Low-Income Population in China: A Cross-Sectional Study
Authors Fan L, Yang Q, Zhang X, Lin Q, Guo D ![]() , Liu J
, Liu J ![]() , Tu J, Wang J
, Tu J, Wang J ![]() , Li Y
, Li Y ![]() , Ning X
, Ning X
Received 31 March 2021
Accepted for publication 26 June 2021
Published 15 July 2021 Volume 2021:14 Pages 3263—3272
DOI https://doi.org/10.2147/DMSO.S313702
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Liming Fan,1,* Qiaoxia Yang,2,* Xin Zhang,3,* Qiuxing Lin,3– 5 Dandan Guo,3 Jie Liu,2– 4 Jun Tu,3– 5 Jinghua Wang,3– 5 Yan Li,6 Xianjia Ning3– 5
1Department of Medical Clinical Laboratory, Tianjin Medical University General Hospital, Tianjin, 300052, People’s Republic of China; 2Department of Cardiology, Tianjin Medical University General Hospital, Tianjin, 300052, People’s Republic of China; 3Department of Neurology, Tianjin Medical University General Hospital, Tianjin, 300052, People’s Republic of China; 4Laboratory of Epidemiology, Tianjin Neurological Institute, Tianjin, 300052, People’s Republic of China; 5Tianjin Neurological Institute, Key Laboratory of Post-Neuroinjury Neuro-repair and Regeneration in Central Nervous System, Ministry of Education and Tianjin City, Tianjin, 300052, People’s Republic of China; 6Department of Anesthesiology, Tianjin Jizhou People’s Hospital, Tianjin, 301900, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xianjia Ning
Department of Neurology, Tianjin Medical University General Hospital, Laboratory of Epidemiology, Tianjin Neurological Institute & Tianjin Neurological Institute, Key Laboratory of Post-Neuroinjury Neuro-repair and Regeneration in Central Nervous System, Ministry of Education and Tianjin City, 154 Anshan Road, Heping District, Tianjin, 300052, People’s Republic of China
Tel +86-22-60817505
Fax +86-22-60817448
Email [email protected]
Yan Li
Department of Anesthesiology, Tianjin Jizhou People’s Hospital, 18 Nanhuan Road, Jizhou District, Tianjin, 301900, People’s Republic of China
Tel/Fax +86-22- 60733586
Email [email protected]
Introduction: Carotid atherosclerosis is a well-established biomarker associated with future cardiovascular disease and stroke. We explored the influence of sex on the relationship between metabolic syndrome (MetS) and its components with carotid intima-media thickness (CIMT) among a low-income population in China, which has a high incidence of stroke.
Methods: This population-based study recruited participants aged ≥ 45 years from rural areas of Tianjin, China between April 2014 and January 2015. Anthropometric characteristics and biochemical profiles were measured. CIMT was assessed using ultrasonography. Diagnosis of MetS and its components was made using the modified International Diabetes Federation criteria for the Asian population. A multivariate linear regression model was used to evaluate the effects of sex on the relationship between the presence of MetS and its components and CIMT.
Results: A total of 3583 individuals (men, 41.4%; women, 58.6%) were included in the analyses. MetS was prevalent in 54.5% (men, 42.3%; women, 63.2%) of the participants. Mean CIMT was 0.57 ± 0.09 mm. In the multivariate analysis, for both sexes, CIMT increased significantly when MetS was present compared with when it was not (both P < 0.001). A common trend was observed in both sexes, in that CIMT increased as the number of MetS components increased, with β (95% confidence interval [CI]) = 0.021 (0.000, 0.042) for men and 0.014 (0.002, 0.026) for women (both P < 0.05). Of the five MetS components, elevated blood pressure was an independent risk factor for increased CIMT in both sexes (men: β = 0.013; 95% CI: 0.003, 0.023; P = 0.008; women: β = 0.024; 95% CI: 0.016, 0.033; P < 0.001). Moreover, abdominal obesity was also an independent risk factor for increased CIMT in men (β = 0.013; 95% CI: 0.003, 0.023; P = 0.008) but not in women.
Conclusion: The presence and number of components of MetS were associated with CIMT in both men and women. Sex differences were found in the impact of individual components of MetS on CIMT. Early identification and management of MetS according to sex-specific risk of MetS should be considered to reduce the prevalence and burden of carotid atherosclerosis in rural China, which has a high incidence of stroke, a known consequence of carotid atherosclerosis.
Keywords: atherosclerosis, carotid intima-media thickness, metabolic syndrome, components, sex differences
Introduction
The Global Burden of Diseases, Injuries, and Risk Factors Study found that stroke is a major cause of mortality and disability worldwide.1 In 2016, there were 5.5 million deaths and 116.4 million disability-adjusted life-years (DALYs) due to stroke.2 In China, stroke is the main cause of death,3 and it is associated with major expenses related to treatment and post-stroke care as well as the loss of quite substantial potential economic activity.
One of the main mechanisms of stroke is atherosclerosis, which is associated with an increased risk of recurrent stroke events.4 Epidemiological and clinical trial evidence has supported the use of carotid intima-media thickness (CIMT) as a validated and accepted marker for atherosclerosis burden4 and for predicting the risk of stroke and cardiovascular events.5–7
More than 90% of stroke burden is attributable to modifiable risk factors.8 A cluster of metabolic factors (ie, high systolic blood pressure [SBP], high body mass index [BMI], high fasting plasma glucose [FPG], high total cholesterol [TC], and low glomerular filtration rate) is the second largest contributor to DALYs.8 Metabolic syndrome (MetS) is a recognizable clinical cluster of risk factors, including abdominal obesity, insulin resistance, hypertension, and hyperlipidemia,9 which are known to be associated with an increased risk for cardiovascular disease and stroke.10 Previous studies have shown that the aggregation of components of MetS was associated with the occurrence and progression of carotid atherosclerosis11–13 and increased mortality and morbidity from cardiovascular disease and stroke.14
Sex difference have been reported previously in the risk factors for carotid atherosclerosis15–17 and the contributing risk profiles for MetS.18,19 Moreover, atherosclerosis in men has presented with distinct inflammatory and histologic features when compared with those in women.20 Previous studies also found that the effect of MetS on carotid atherosclerosis varied by sex.16,21 However, most previous studies evaluated the relationship between MetS and CIMT among populations in developed countries and urban areas of developing countries. In contrast, few data are available regarding sex-specific effects on the relationship between MetS and its components with CIMT in low-income areas, where income levels are insufficient and the burden of stroke and other medical conditions remains severe. Our previous study reported that the age-standardized incidence of first-ever stroke per 100,000 person-years was 318.2 in 2012 and that the incidence of stroke had increased annually by 6.5% overall from 1992 to 2012,22 and a greater proportion of women than men experiencing an annual increase (8.0% versus 5.8%).23
Therefore, the present study explored the effect of sex on the relationship between MetS and its components and CIMT among a low-income population in China with a high incidence of stroke.
Methods
Participant Selection and Study Design
This population-based cross-sectional study was performed in rural areas of Tianjin, China from April 2014 to January 2015. Participants came from the previously described Tianjin Brain Study.24 Briefly, the Tianjin Brain Study was a population-based stroke surveillance project that included 14,251 participants from 18 administrative villages in rural Tianjin, China. Approximately 95% of the participants were low-income farmers, with a per capita disposable income of <1600 US dollars in 2014. According to our previous research, the incidence of stroke in this area was as high as 318.2 per 100,000 person-years.22
The current study recruited all local permanent residents aged ≥45 years using the cluster sampling method. Residents who had undergone carotid endarterectomy or carotid stenting and those with a previous disease history of stroke or coronary heart disease were excluded. All eligible participants underwent anthropometric, biochemical, and CIMT measurements.
Data Collection
Data in the present study were collected by well-trained epidemiology researchers through face-to-face interviews based on a pre-designed questionnaire. Sociodemographic factors included name, sex, date of birth, and educational level. Participants were categorized into three age groups: 45–54, 55–64, and ≥65 years. Educational level was categorized into two groups: no formal education and some formal education. Individual and family medical histories were determined by a previous diagnosis of diabetes, hypertension, and/or hyperlipidemia and medication history based on medical records. Lifestyle factors included cigarette smoking (defined as smoking more than one cigarette per day for at least 1 year; participants were divided into never smoking and now or ever smoking groups) and alcohol consumption (defined as drinking more than 500 g of alcohol per week for at least 1 year; participants were divided into never drinking and now or ever drinking groups), which were based on medical records or self-reports.
Physical Examinations and Measurements
Physical examination included measurements of waist circumference (cm), body mass index (BMI, kg/m2), and blood pressure (mmHg), and the measurement processes have been described in detail in our previous report.25 Fasting blood samples were collected in the morning after the participant had fasted for at least 12 hours and were sent to the Ji County People’s Hospital within 2 hours for biochemical examination. Serum fasting blood glucose (FBG), TC, triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C) concentrations were determined.
Ultrasonography Measurements
Each participant underwent detailed carotid ultrasound examinations to evaluate CIMT. A well-trained technician blinded to subject identification performed ultrasound examinations while subjects were in the supine position. All scans were performed using B-mode ultrasonography (Terasont3000; Burlington, MA, USA) with a 5- to 12-MHz linear array transducer. Both extracranial carotid artery trees (including the common carotid artery, carotid sinus, and internal and external carotid arteries) were screened. The CIMTs at the near and far walls of the common carotid artery were measured on both the left and right sides, and the maximum CIMT, minimum CIMT, and average CIMT per side were obtained. Images were obtained and digitally stored in accordance with a standard protocol.26
Criteria for Metabolic Syndrome
MetS was defined according to the modified International Diabetes Federation criteria for the Asian population (2009) as the presence of 3 or more abnormal components:27 (1) abdominal obesity (WC ≥90 cm in men and ≥80 cm in women); (2) hypertriglyceridemia (TG ≥1.70 mmol/L or using medications for elevated TG); (3) low HDL-C (HDL-C <1.03 mmol/L in men and <1.3 mmol/L in women, or using medications to increase HDL-C); (4) increased blood pressure (SBP ≥130 mmHg or diastolic blood pressure [DBP] ≥85 mmHg [hypertension], or using antihypertensive medications); (5) high fasting glucose (FPG ≥5.6 mmol/L or using antidiabetic medications).
MetS components in the present study refer to the five diagnostic criteria noted above. The number of MetS components per individual was classified into three groups, namely 1–2, 3–4, and 5 components.
Statistical Analysis
Continuous variables, including age, education length, CIMT, BMI, WC, FPG, TC, TG, HDL-C, LDL-C, SBP, and DBP, were presented as means and standard deviations. Categorical variables, including sex, age group, education level, smoking status, alcohol consumption, medications, presence of MetS and its components, and number of components, were presented as frequencies and percentages. Student’s t-tests and Pearson’s chi-squared tests are used to analyze the differences in means and proportions between groups. Multiple group comparisons were performed with an analysis of variance. A linear regression model was applied to estimate independent correlates of CIMT and presented as β-coefficients and 95% confidence intervals (CIs). A two-tailed P value <0.05 was considered significant. All statistical analyses were performed with SPSS software (version 25.0; SPSS, Chicago, IL, USA).
Results
Of the 5380 residents aged ≥45 years identified after cluster sampling, 3956 residents participated in this survey. After excluding 373 residents who met exclusion criteria, 3583 participants were ultimately included in this study (Figure 1).
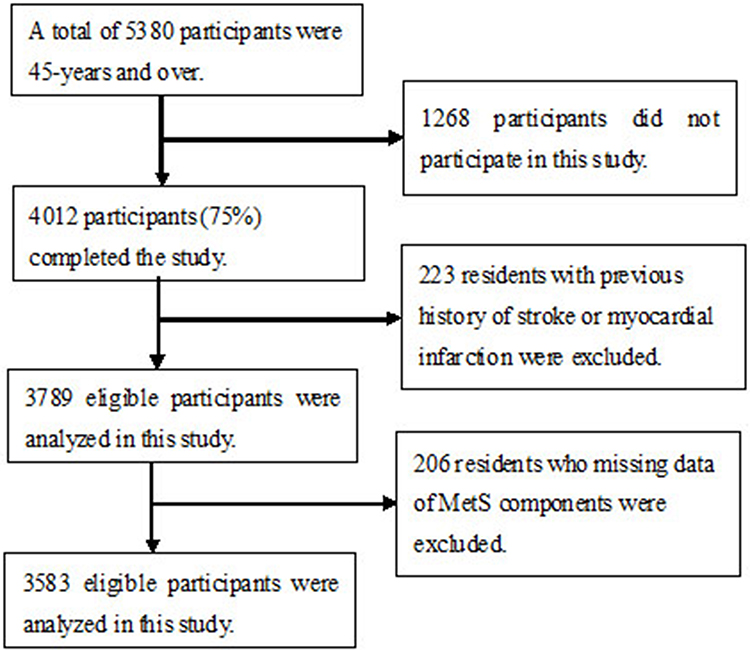 |
Figure 1 Flow chat of participants selection. Figure 1 showed that there were 5380 residents aged ≥45 years identified after cluster sampling, 3956 residents participated in this survey. After excluding 373 residents who met exclusion criteria, 3583 participants were ultimately included in this study. |
Demographic Characteristics
As shown in Table 1, a total of 3583 individuals aged ≥45 years (mean age, 60.06 years) participated in the study, with 1482 (41.4%) men and 2101 (58.6%) women included in the analysis. The median length of formal education was 6 years, and 17.6% had no formal education. Among men, 57% were current or ever smokers, and 36.1% currently or had ever consumed alcohol. Few individuals took anti-diabetes and lipid-lowering agents, accounting for 5.5 and 0.5% respectively, and 29.0% of individuals took anti-hypertensive drugs. The average BMI, WC, FBG, TC, TG, HDL-C, LDL-C, SBP, DBP, and CIMT measurements were 25.53 kg/m2, 89.15 cm, 5.92 mmol/L, 4.86 mmol/L, 1.75 mmol/L, 1.46 mmol/L, 2.70 mmol/L, 146.53 mmHg, 86.84 mmHg, and 0.57 mm respectively.
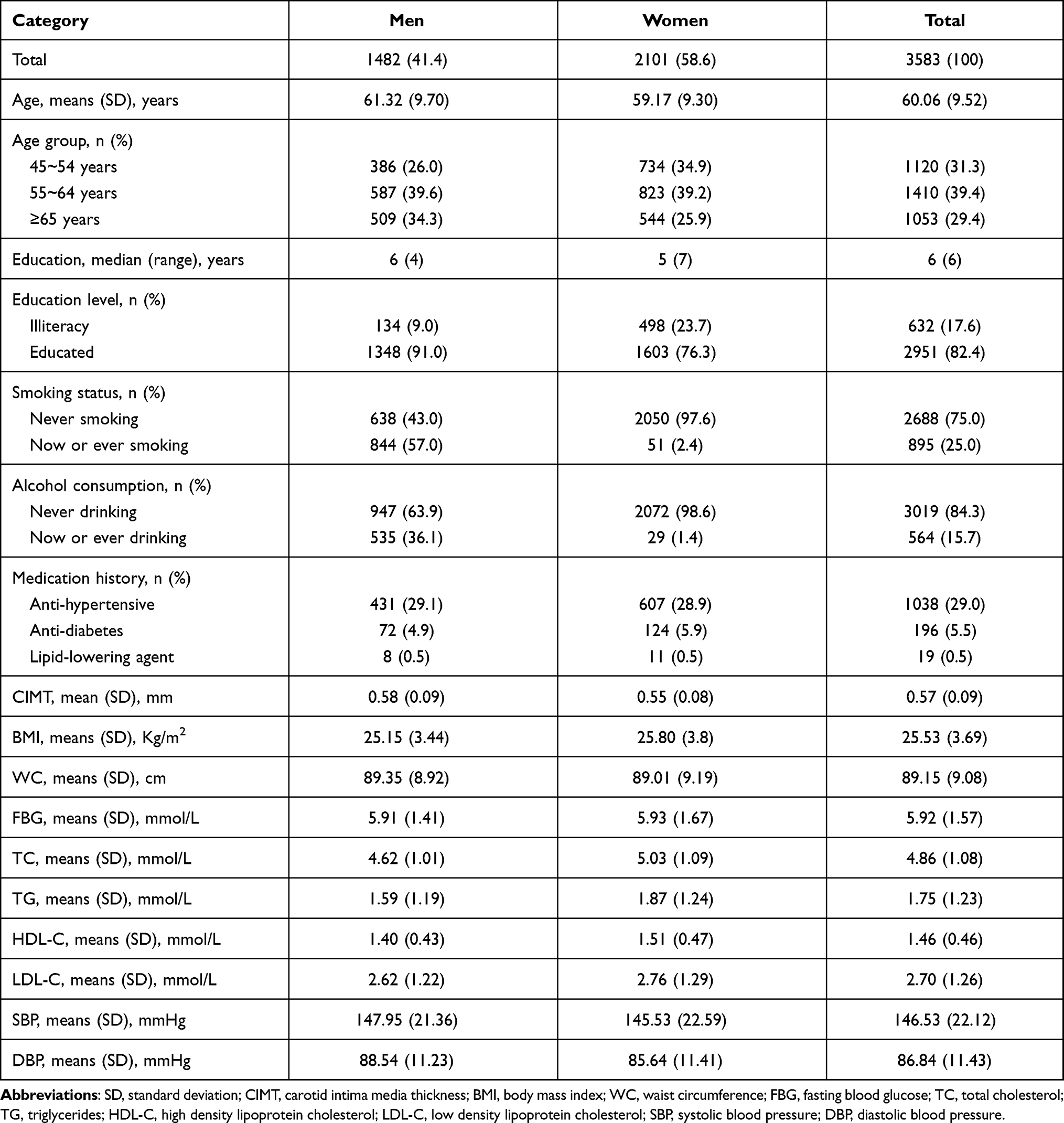 |
Table 1 Characteristics of Participants by Sex |
Characteristics of MetS and Its Components and CIMT by Sex
As shown in Table 2, 1954 participants (54.5%) met the AHA/NHLBI criteria for MetS (men, 42.3%; women, 63.2%) in the middle-aged and elderly groups, and the prevalence of MetS was significantly higher in women than in men (P < 0.001). More women than men were in the 3–4 and 5 MetS components groups, with 52.3 and 10.9% in women, 37.2 and 5.1% in men (all P<0.001). Among all MetS components, increased BP was a major component for both men (84.6%) and women (79.2%). Women had higher prevalences of abdominal obesity, hypertriglyceridemia, and reduced HDL-C than did men (all P < 0.001). Moreover, the component of abdominal obesity accounted for the largest proportion in women, but less than half of men (86.4% versus 48.9%, P < 0.001).
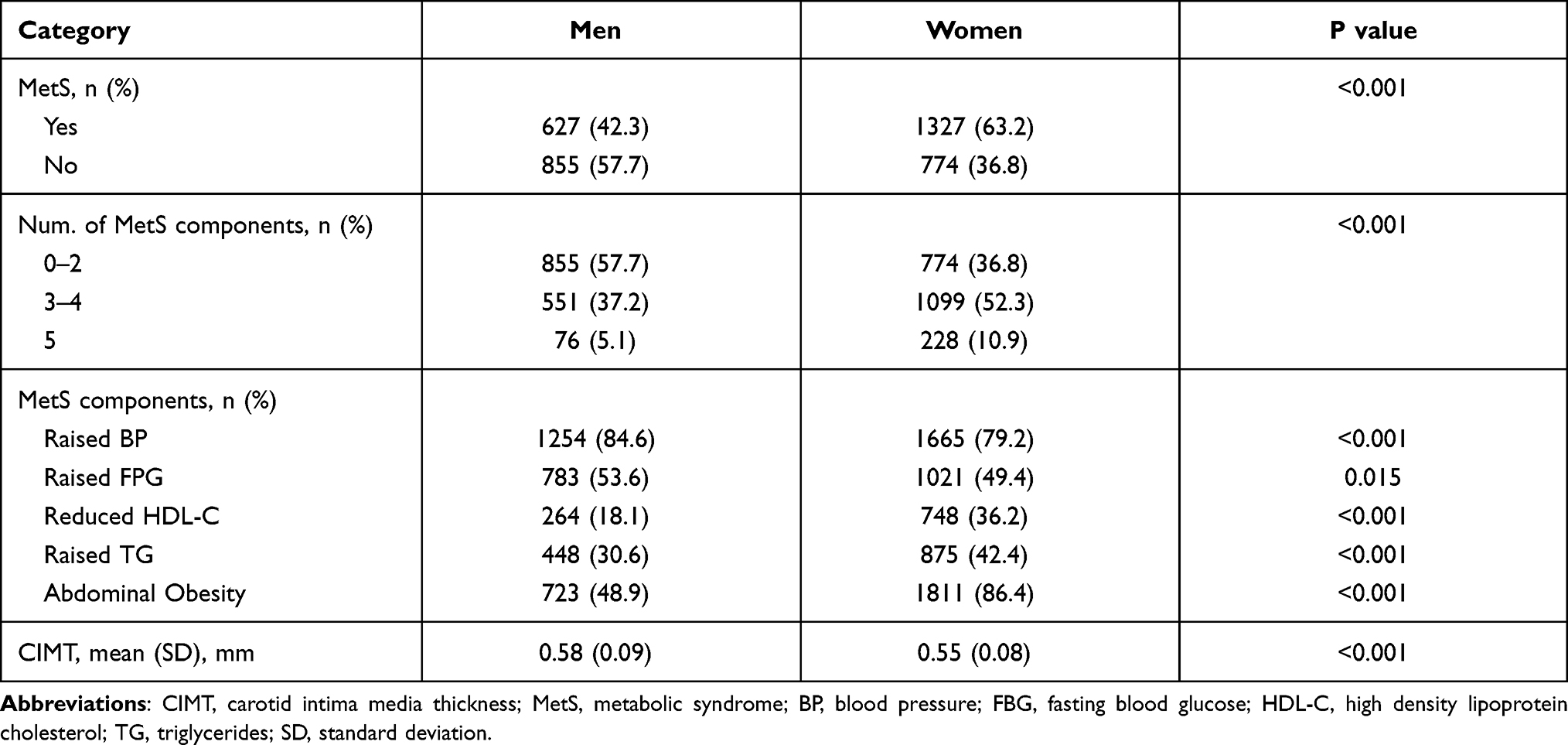 |
Table 2 Characteristics of MetS and Its Components, and CIMT by Sex |
The average CIMT values in men and women were 0.58 mm and 0.55 mm, respectively. Compared with women, we found that men had greater CIMT values (P < 0.001).
Sex Differences in Factors Associated with CIMT in the Univariate Analysis
Table 3 shows that age, educational level, LDL-C concentrations, and increased blood pressure (BP) were associated with CIMT in both men and women in the univariate analysis (all P < 0.001). The risk of greater CIMT increased with older age, low education level, high LDL-C concentrations, and increased BP in the overall population. In the univariate analysis, a positive correlation was identified between CIMT and the presence and number of components of MetS in women but not in men.
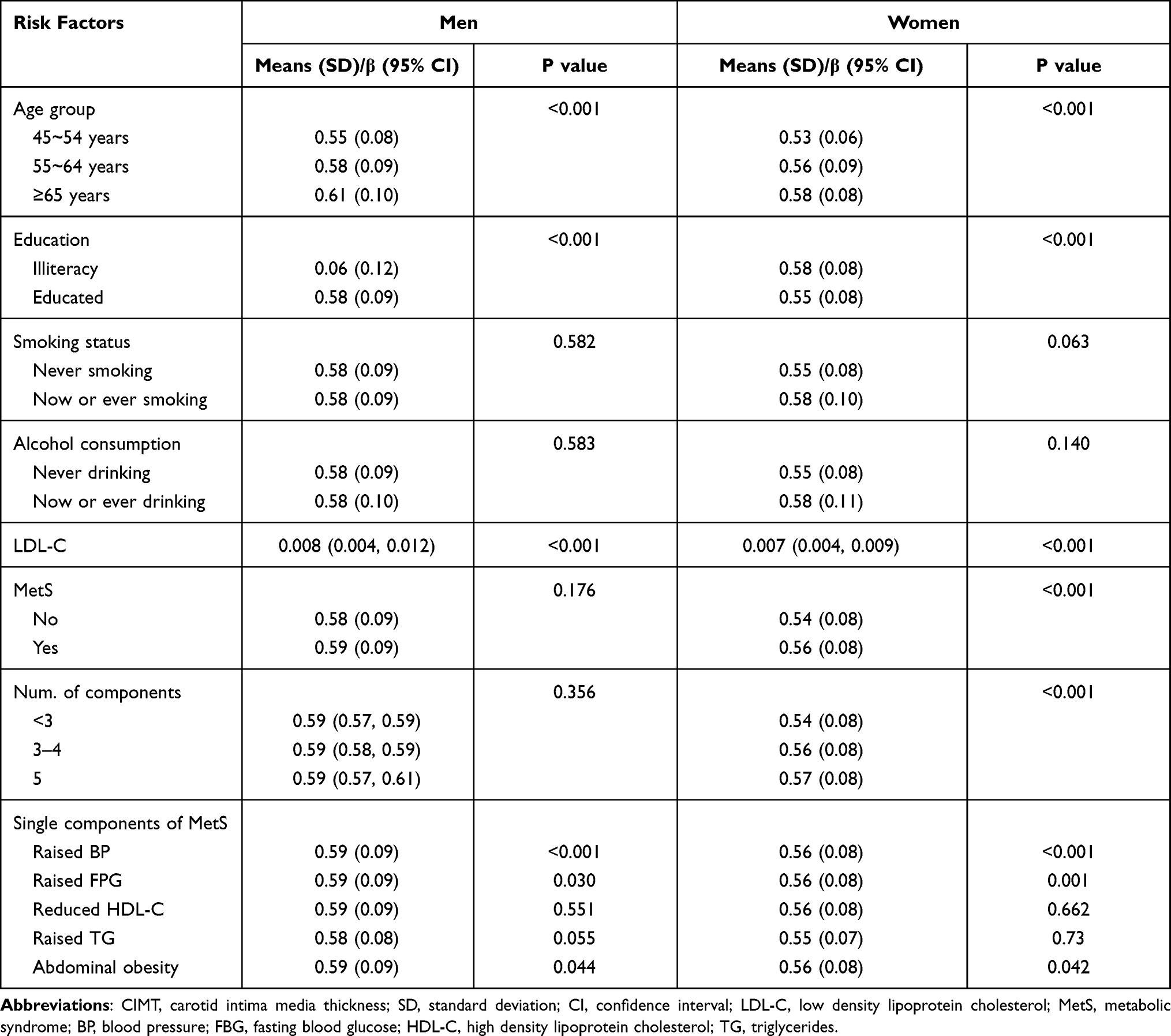 |
Table 3 Associated Factors of CIMT by Sex in the Univariate Analysis |
Sex Differences in Associations Between MetS and CIMT in the Multivariate Analysis
As shown in Table 4, the multivariate linear analysis revealed that the presence and number of components of MetS were associated with the risk of increased CIMT in both men and women after adjusting for age, educational level, and LDL-C. Compared with those in the group without MetS, the mean CIMTs for men and women with MetS were 0.010 and 0.009 mm greater, respectively (men: β = 0.010; 95% CI: 0.000, 0.019; P = 0.044; women: β = 0.009; 95% CI: 0.001, 0.016; P = 0.019). A common trend was observed in both sexes in which CIMT increased in line as the number of MetS components increased, and individuals with five MetS components had the greatest risk of increased CIMT, with β (95% CI) of 0.021 (0.000, 0.042) for men and 0.014 (0.002, 0.026) for women (both P < 0.05).
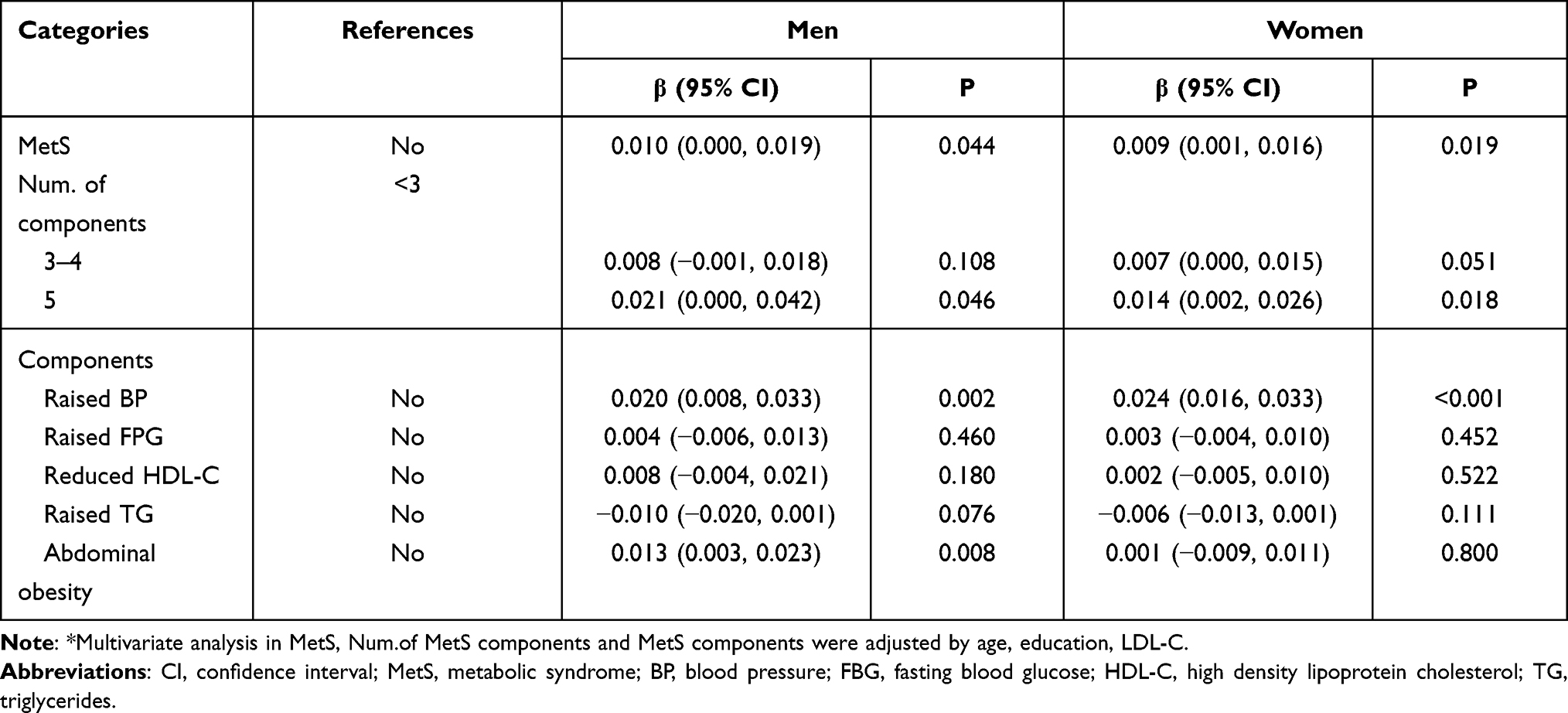 |
Table 4 Relationship Between Metabolic Syndrome and Carotid Atherosclerosis by Sex in Multivariate Analysis* |
Among the components of MetS, only increased BP was an independent risk factor for increased CIMT in women (β = 0.024; 95% CI: 0.016, 0.033; P < 0.001). In men, increased BP and abdominal obesity were independent risk factors for increased CIMT, with β = 0.020; 95% CI: 0.008, 0.033; P = 0.002 for increased BP and β = 0.013; 95% CI: 0.003, 0.023; P = 0.008 for abdominal obesity.
Discussion
In the present study, we evaluated for the first time the association between MetS presence, number of MetS components, and single components of MetS with CIMT in low-income, middle-aged and elderly men and women living in a rural area of China that has a high incidence of stroke. We found that MetS presence and number of components were associated with the risk of increased CIMT in both men and women. With respect to the influence of sex on the relationship between MetS components and CIMT, increased BP was a common independent risk factor for and the greatest contributor to CIMT in both men and women. Abdominal obesity was a risk factor for increased CIMT only in man but not in women.
In recent years, with changes in lifestyle and dietary habits, the prevalence of MetS has increased dramatically in China.27 In the present study, the overall prevalence of MetS was 54.5% (42.3% in men and 63.2% in women) among this low-income population using the modified International Diabetes Federation (IDF) criteria for the Asian population (2009). Another study conducted in rural areas of China showed that the MetS prevalence in the elderly reached 56.9% using the same defining criteria, which is greater than was identified using three other criteria: 42.4% using the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) criteria, 54.0% using the IDF (2005) criteria, and 30.6% using the Chinese Diabetes Society criteria.28 What is more, studies revealed that MetS definitions using the IDF and AHA/NHLBI criteria were the best among four sets of criteria for detecting subclinical atherosclerosis in non-diabetic Chinese subjects.29
Epidemiological studies in various populations have demonstrated that individuals with MetS had a larger CIMT and greater risk of cardiovascular events and stroke11,12 compared with individuals without MetS. In the present study, we also found that MetS presence was an independent risk for increased CIMT in both sexes. The results are consistent with those of studies among various populations.11,16,30 The population-based Tromsø Study showed that both men and women with MetS had greater CIMT at follow-up than did those without MetS.11 However, several studies reported different results. Data from cross-sectional studies in Caucasian31 and Taiwanese32 subjects indicated no correlation between MetS and CIMT in the subgroup of men. More prospective cohort studies with larger sample sizes should be conducted to resolve this controversial issue.
Several studies have shown that interrelated components of MetS might promote endothelial dysfunction leading to progressive arterial injury and that the clustering of three or more components exerted a synergistic negative effect on vascular structure and function.12 In the present study, we assessed sex differences in the effect of the number of MetS components on CIMT and found that individuals of both sexes with more MetS components tended to have a higher risk of increased CIMT. This finding is consistent with those in other previous studies in overall populations.33,34 A previous study reported that using the number of components of MetS was better than using the binary diagnosis of MetS for predicting subclinical atherosclerosis.34 Our findings further confirm that MetS is associated with an increased risk of CIMT in both men and women. With the aging population and accelerated changes in lifestyles, the overall prevalence of MetS is increasing,35,36 and more attention should be paid to individuals with MetS, especially those with more components, whether they are male or female.
Hypertension has consistently been considered to be associated with an increased prevalence of preclinical atherosclerosis and with an increased risk of clinical atherosclerotic cardiovascular disease.37 Studies in various populations have found an association between elevated blood pressure and increased CIMT in both sexes.31,38 Consistent with our results, we found that elevated blood pressure was an independent risk factor for increased CIMT in both men and women, with β (95% CI) of 0.020 (0.008, 0.033) in men and 0.024 (0.016, 0.033) in women. Furthermore, the results provided further evidence that elevated BP, as a traditional risk factor, made the greatest contribution to increased CIMT compared with the other four components of MetS in both men and women. Similarly, an earlier cross-sectional study showed that, when comparing individuals with an equal number of components of MetS, the prevalence of carotid atherosclerosis was significantly higher in subjects with elevated BP than in those without, and it increased with the number of components in the elevated BP group (P= 0.0277).39 Therefore, more attention should be paid to individuals with both MetS and elevated BP with respect to the progression of carotid atherosclerosis and in the evaluation of cardiovascular disease risk.
Although obesity is a risk factor for insulin resistance and type 2 diabetes and a significant risk factor for cardiovascular disease, not every obese individual is insulin resistant or at high risk of diabetes and cardiovascular disease.40 In the present study, WC was used to measure abdominal obesity, and a significant correlation was found between WC and CIMT in men but not in women. In the male group, WC was an independent risk factor for CIMT, second to increased BP as a contributor to increased CIMT. This result is similar to results of an earlier study in Finnish men, in which abdominal obesity was associated with a 4-year increase in CIMT.41 Contrary to our findings, the Italian SardiNIA study showed that abdominal obesity was correlated with increased CIMT in both sexes, but the correlation was stronger in women.42 Another cross-sectional study in a Caucasian population showed that WC was an independent CIMT determinant in women, while no significant correlation was found between CIMT and increased WC in men.31 In view of these inconsistent research results, further epidemiological studies are needed to provide stronger evidence.
In present study, the other three components of MetS (ie, increased FPG, reduced HDL-C, and increased TG) were not correlated with CIMT in either sex. Literature reports on sex-specific relationships between the other three single MetS components and CIMT are contradictory. A longitudinal study in Japan reported that reduced HDL-C, increased TG, and increased FPG levels compared with baseline were related to greater CIMT in both sexes, except for high FPG in men. After the 1.2±0.4-year follow-up period, the annual increase in CIMT was only associated with reduced HDL-C in women and was not related to the three single MetS components in men.43 Similar results were obtained in a longitudinal adult health study in Norway, which reported that these three single MetS components were not independent risk factors for the progression of atherosclerosis in either men and women.11
Our study has some limitations. First, the study used a cross-sectional design; further follow-up and cohort studies may be used to reveal causality. Second, the study population came from a rural area in Tianjin, China, so our findings from this low-income population regarding the association between MetS and its components with CIMT may not be generalizable to other populations. Third, CIMT is considered to be an early indicator of carotid atherosclerosis. In the future, adding in measurement of carotid plaque and plaque burden may strengthen our results.
Conclusions
In this population-based cross-sectional study, we confirmed that the presence and number of components of MetS were associated with increased CIMT among both men and women aged ≥45 years in a low-income area with a high incidence of stroke. The association between MetS components and CIMT varied by sex. Increased BP was a common independent risk factor for increased CIMT in men and women, and WC was significantly associated with CIMT in men but not in women. Early intervention and management of MetS and its components based on sex-specific differences, such as blood pressure and weight in men and blood pressure in women, are essential for reducing the occurrence and progression of carotid atherosclerosis.
Abbreviations
MetS, metabolic syndrome; CIMT, carotid intima-media thickness; DALYs, disability-adjusted life-years; SBP, systolic blood pressure; BMI, body mass index; FPG, fasting plasma glucose; TC, total cholesterol; FBG, fasting blood glucose; TG, triglycerides; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; DBP, diastolic blood pressure; CIs, confidence intervals; BP, blood pressure.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All procedures in the present study were approved by the Ethics Committee of Tianjin Medical University General Hospital and were carried out in accordance with the approved guidelines. All participants received information and provided written informed consent to participate. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We thank all participants of the Tianjin Brain Study, and local medical care professionals for their valuable contributions.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vos T, Lim SS, Abbafati Cet al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222.
2. Johnson CO, Nguyen M, Roth GA. Global, regional, and national burden of stroke, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):439–458. doi:10.1016/S1474-4422(19)30034-1
3. Liu L, Wang D, Wong KS, Wang Y. Stroke and stroke care in China: huge burden, significant workload, and a national priority. Stroke. 2011;42(12):3651–3654. doi:10.1161/STROKEAHA.111.635755
4. de Groot E, van Leuven SI, Duivenvoorden R, et al. Measurement of carotid intima-media thickness to assess progression and regression of atherosclerosis. Nat Clin Pract Cardiovasc Med. 2008;5(5):280–288. doi:10.1038/ncpcardio1163
5. Nambi V, Chambless L, Folsom AR, et al. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. J Am Coll Cardiol. 2010;55(15):1600–1607. doi:10.1016/j.jacc.2009.11.075
6. Seo WK, Kim YJ, Lee J, Kwon SU; PICASSO Investigators. Design and rationale of the intima-medial thickness sub-study of the prevention of cardiovascular events in ischemic stroke patients with high risk of cerebral hemorrhage (PICASSO-IMT) study. J Stroke Cerebrovasc Dis. 2017;26(9):1892–1898. doi:10.1016/j.jstrokecerebrovasdis.2017.06.035
7. Selwaness M, Bos D, van den Bouwhuijsen Q, et al. Carotid atherosclerotic plaque characteristics on magnetic resonance imaging relate with history of stroke and coronary heart disease. Stroke. 2016;47(6):1542–1547. doi:10.1161/STROKEAHA.116.012923
8. Feigin VL, Roth GA, Naghavi M, et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016;15(9):913–924. doi:10.1016/S1474-4422(16)30073-4
9. Saklayen MG. The global epidemic of the metabolic syndrome. Curr Hypertens Rep. 2018;20(2):12. doi:10.1007/s11906-018-0812-z
10. Salsberry PJ, Corwin E, Reagan PB. A complex web of risks for metabolic syndrome: race/ethnicity, economics, and gender. Am J Prev Med. 2007;33(2):114–120. doi:10.1016/j.amepre.2007.03.017
11. Herder M, Arntzen KA, Johnsen SH, Mathiesen EB. The metabolic syndrome and progression of carotid atherosclerosis over 13 years. The Tromsø study. Cardiovasc Diabetol. 2012;11:77. doi:10.1186/1475-2840-11-77
12. Cuspidi C, Sala C, Provenzano F, et al. Metabolic syndrome and subclinical carotid damage: a meta-analysis from population-based studies. J Hypertens. 2018;36(1):23–30. doi:10.1097/HJH.0000000000001575
13. Jung JM, Young Kwon D, Han C, Park MH. Metabolic syndrome and early carotid atherosclerosis in the elderly. J Atheroscler Thromb. 2014;21(5):435–444. doi:10.5551/jat.18655
14. Mihic M, Modi P. Metabolic syndrome--risk factors for atherosclerosis and diabetes. Curr Diabetes Rev. 2008;4(2):122–128. doi:10.2174/157339908784220750
15. Sangiorgi G, Roversi S, Biondi Zoccai G, et al. Sex-related differences in carotid plaque features and inflammation. J Vasc Surg. 2013;57(2):338–344. doi:10.1016/j.jvs.2012.07.052
16. Yin JH, Song ZY, Shan PF, et al. Age- and gender-specific prevalence of carotid atherosclerosis and its association with metabolic syndrome in Hangzhou, China. Clin Endocrinol (Oxf). 2012;76(6):802–809. doi:10.1111/j.1365-2265.2011.04198.x
17. Zhao W, Wu Y, Shi M, et al. Sex differences in prevalence of and risk factors for carotid plaque among adults: a population-based cross-sectional study in rural China. Sci Rep. 2016;6:38618. doi:10.1038/srep38618
18. Pucci G, Alcidi R, Tap L, Battista F, Mattace-Raso F, Schillaci G. Sex- and gender-related prevalence, cardiovascular risk and therapeutic approach in metabolic syndrome: a review of the literature. Pharmacol Res. 2017;120:34–42. doi:10.1016/j.phrs.2017.03.008
19. Santilli F, D’Ardes D, Guagnano MT, Davi G. Metabolic syndrome: sex-related cardiovascular risk and therapeutic approach. Curr Med Chem. 2017;24(24):2602–2627. doi:10.2174/0929867324666170710121145
20. Frink RJ. Gender gap, inflammation and acute coronary disease: are women resistant to atheroma growth? Observations at autopsy. J Invasive Cardiol. 2009;21(6):270–277.
21. Rexrode K. Sex differences in sex hormones, carotid atherosclerosis, and stroke. Circ Res. 2018;122(1):17–19. doi:10.1161/CIRCRESAHA.117.312336
22. Zhan C, Shi M, Yang Y, et al. Prevalence and risk factors of carotid plaque among middle-aged and elderly adults in rural Tianjin, China. Sci Rep. 2016;6:23870. doi:10.1038/srep23870
23. Wang J, An Z, Li B, et al. Increasing stroke incidence and prevalence of risk factors in a low-income Chinese population. Neurology. 2015;84(4):374–381. doi:10.1212/WNL.0000000000001175
24. Pan J, Liu J, Wang H, et al. Association of carotid atherosclerosis with lipid components in asymptomatic low-income Chinese: a population-based cross-sectional study. Front Neurol. 2020;11:276. doi:10.3389/fneur.2020.00276
25. Touboul PJ, Hennerici MG, Meairs S, et al. Mannheim carotid intima-media thickness and plaque consensus (2004–2006–2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European stroke conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc Dis. 2012;34(4):290–296. doi:10.1159/000343145
26. Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American heart association/National heart, lung, and blood institute scientific statement. Circulation. 2005;112(17):2735–2752. doi:10.1161/CIRCULATIONAHA.105.169404
27. Cuspidi C, Sala C, Lonati L, et al. Metabolic syndrome, left ventricular hypertrophy and carotid atherosclerosis in hypertension: a gender-based study. Blood Press. 2013;22(3):138–143. doi:10.3109/08037051.2012.744151
28. Łoboz-rudnicka M, Jaroch J, Bociąga Z, et al. Impact of cardiovascular risk factors on carotid intima-media thickness: sex differences. Clin Interv Aging. 2016;11:721–731. doi:10.2147/CIA.S103521
29. Lin HF, Liu CK, Liao YC, Lin RT, Chen CS, Juo SH. The risk of the metabolic syndrome on carotid thickness and stiffness: sex and age specific effects. Atherosclerosis. 2010;210(1):155–159. doi:10.1016/j.atherosclerosis.2009.11.027
30. Panayiotou AG, Griffin M, Kouis P, et al. Association between presence of the metabolic syndrome and its components with carotid intima-media thickness and carotid and femoral plaque area: a population study. Diabetol Metab Syndr. 2013;5:44. doi:10.1186/1758-5996-5-44
31. Ishizaka N, Ishizaka Y, Toda E, Hashimoto H, Nagai R, Yamakado M. Hypertension is the most common component of metabolic syndrome and the greatest contributor to carotid arteriosclerosis in apparently healthy Japanese individuals. Hypertens Res. 2005;28(1):27–34. doi:10.1291/hypres.28.27
32. Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28(4):629–636. doi:10.1161/ATVBAHA.107.151092
33. Jiang B, Li B, Wang Y, et al. The nine-year changes of the incidence and characteristics of metabolic syndrome in China: longitudinal comparisons of the two cross-sectional surveys in a newly formed urban community. Cardiovasc Diabetol. 2016;15:84. doi:10.1186/s12933-016-0402-9
34. Lakka TA, Salonen R, Kaplan GA, Salonen JT. Blood pressure and the progression of carotid atherosclerosis in middle-aged men. Hypertension. 1999;34(1):51–56. doi:10.1161/01.HYP.34.1.51
35. Sinning C, Wild PS, Echevarria FM, et al. Sex differences in early carotid atherosclerosis (from the community-based Gutenberg-Heart Study). Am J Cardiol. 2011;107(12):1841–1847. doi:10.1016/j.amjcard.2011.02.318
36. Kawamoto R, Tomita H, Oka Y, Ohtsuka N, Kamitani A. Metabolic syndrome and carotid atherosclerosis: role of elevated blood pressure. J Atheroscler Thromb. 2005;12(5):268–275. doi:10.5551/jat.12.268
37. Abbasi F, Brown BW, Lamendola C, McLaughlin T, Reaven GM. Relationship between obesity, insulin resistance, and coronary heart disease risk. J Am Coll Cardiol. 2002;40(5):937–943. doi:10.1016/S0735-1097(02)02051-X
38. Lakka TA, Lakka HM, Salonen R, Kaplan GA, Salonen JT. Abdominal obesity is associated with accelerated progression of carotid atherosclerosis in men. Atherosclerosis. 2001;154(2):497–504. doi:10.1016/S0021-9150(00)00514-1
39. Scuteri A, Orru’ M, Morrell CH, et al. Associations of large artery structure and function with adiposity: effects of age, gender, and hypertension. The SardiNIA study. Atherosclerosis. 2012;221(1):189–197. doi:10.1016/j.atherosclerosis.2011.11.045
40. Abbasi F, Brown BW Jr, Lamendola C, McLaughlin T, Reaven GM. Relationship between obesity, insulin resistance, and coronary heart disease risk. Am Coll Cardiol. 2002;40(5):937–943. doi: 10.1016/s0735-1097(02)02051-x
41. Lakka TA, Lakka HM, Salonen R, Kaplan GA, Salonen JT. Abdominal obesity is associated with accelerated progression of carotid atherosclerosis in men. Atherosclerosis. 2001;154(2):497–504. doi: 10.1016/s0021-9150(00)00514-1
42. Scuteri A, Orru’ M, Morrell CH, et al. Associations of large artery structure and function with adiposity: effects of age, gender, and hypertension. The SardiNIA study. Atherosclerosis. 2012;221(1):189–197. doi: 10.1016/j.atherosclerosis.2011.11.045
43. Matoba Y, Inoguchi T, Suzuki S, et al. Impact of metabolic syndrome on the progression of Intima-Media Thickening in Japanese--a follow-up study. Diabetes Res Clin Pract. 2009;86(3):e50-53. doi: 10.1016/j.diabres.2009.09.013
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.