Back to Journals » Journal of Asthma and Allergy » Volume 19
Severity-Dependent Association Between Allergic Rhinitis and Adenoid Hypertrophy in Dust Mite–Sensitized Children from Northern China: A Cross-Sectional Analysis of 170 Cases
Authors Zhao B, Wang Y, Zhang H ![]() , Jin P
, Jin P ![]() , Jia T
, Jia T
Received 22 February 2026
Accepted for publication 4 May 2026
Published 16 May 2026 Volume 2026:19 598696
DOI https://doi.org/10.2147/JAA.S598696
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Bo Zhao,1 Yang Wang,2 Hongyang Zhang,2 Peng Jin,2 Tao Jia2
1Center of Stomatology, The Second Qilu Hospital of Shandong University, Jinan, Shandong, People’s Republic of China; 2Department of Otolaryngology, The Second Qilu Hospital of Shandong University, Jinan, People’s Republic of China
Correspondence: Tao Jia, Department of Otolaryngology, The Second Qilu Hospital of Shandong University, 247 Beiyuan Avenue, Jinan, Shandong, 250033, People’s Republic of China, Email [email protected]
Background: Allergic rhinitis (AR) and adenoid hypertrophy (AH) frequently coexist in children, yet the relationship between allergic disease severity and the extent of adenoid enlargement remains incompletely defined. This study aimed to investigate the association between AR severity, allergic inflammatory burden, and the degree of AH in dust mite–sensitized children.
Methods: We conducted a cross-sectional analysis of 170 children with dust mite–sensitized AR from Northern China. AH was assessed by nasal endoscopy and classified as grade III or IV. AR severity was evaluated using the Total Nasal Symptom Score (TNSS), visual analogue scale (VAS), and Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ-S). Allergic inflammatory markers included peripheral blood eosinophil counts (EOS), total IgE, and Dermatophagoides pteronyssinus (d1) and Dermatophagoides farinae (d2)-specific IgE. Group comparisons and Spearman correlation analyses were performed.
Results: Children with grade IV AH exhibited significantly higher TNSS, VAS scores, and nasal symptom burden compared with those with grade III hypertrophy (all P < 0.001). Nasal obstruction, rhinorrhea, and nasal itching scores were also significantly increased. TNSS (r = 0.426), VAS (r = 0.458), and PRQLQ-S (r = 0.348) showed moderate positive correlations with the percentage of choanal obstruction (all P < 0.001). In addition, eosinophil counts, total IgE, and dust mite–specific IgE levels demonstrated weaker but significant correlations with adenoid obstruction.
Conclusion: AR severity is positively and dose-dependently associated with AH in dust mite–sensitized children. These findings suggest that adenoid enlargement is associated with clinical and immunological markers of allergic inflammation and highlight the importance of early and effective control of allergic rhinitis to prevent progressive AH.
Keywords: allergic rhinitis, AH, allergen, dust mite-sensitized, allergy
Introduction
Allergic rhinitis (AR) is one of the most common chronic inflammatory airway diseases in childhood, characterized by IgE-mediated immune responses, and the global prevalence of pediatric AR continues to rise, particularly in regions with high allergen exposure and urbanization.1–3 House dust mite sensitization remains the dominant allergic trigger in China, contributing to perennial symptoms and sustained inflammatory activity.4–7 Adenoid hypertrophy (AH) is another frequent pediatric condition and a major cause of nasal obstruction, mouth breathing, snoring, and sleep-disordered breathing in children. Traditionally, AH has been attributed to recurrent or chronic infections leading to lymphoid hyperplasia.8,9 However, increasing attention has been directed toward the potential role of allergic inflammation in driving adenoid enlargement.10,11 The adenoid is an immunologically active lymphoid organ located in the nasopharynx and is continuously exposed to inhaled allergens.
Previous studies have demonstrated an increased prevalence of AH in children with AR, suggesting a possible association between allergic disease and adenoid enlargement.12–14 Nevertheless, most available data are based on binary comparisons, such as the presence or absence of AR or AH. Such approaches do not adequately address whether the severity of allergic rhinitis is associated with the extent of AH. As a result, it remains unclear whether adenoid enlargement simply coexists with allergic rhinitis or reflects the cumulative burden of chronic allergic inflammation on nasopharyngeal lymphoid tissue.
In this context, we conducted a cross-sectional study in a well-defined cohort of dust mite–sensitized children with allergic rhinitis from Northern China. By combining validated symptom-based severity assessments, quality-of-life measures, laboratory markers of allergic inflammation, and endoscopic evaluation of AH, we aimed to investigate the association between AR severity, allergic inflammatory burden, and the degree of adenoid obstruction. We hypothesized that increasing AR severity would be associated with progressively greater AH, consistent with a severity-dependent effect of chronic allergic inflammation.
Methods and Materials
Study Design and Population
This was a cross-sectional study conducted in a pediatric population from Northern China. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Institutional Review Board of the Second Qilu Hospital of Shandong University (Ethics Approval Number KYLL-2018 (KJ) P-0028). Between 1 December 2020 and 30 November 2025, a total of 170 consecutive children diagnosed with allergic rhinitis were enrolled from outpatient clinics. All participants had confirmed sensitization to house dust mites and completed clinical evaluation, laboratory testing, and nasal endoscopic examination within the same clinical period.
Allergic rhinitis was diagnosed according to established international and national guidelines. The diagnosis required the presence of typical allergic nasal symptoms, including nasal obstruction, rhinorrhea, sneezing, and/or nasal itching, persisting for at least four weeks, together with objective evidence of allergen sensitization. Sensitization was confirmed by serum-specific IgE testing to Dermatophagoides pteronyssinus (d1) and/or Dermatophagoides farinae (d2), with a level of ≥0.35 kUA/L considered positive.
Children aged 3–12 years with confirmed dust mite–sensitized AR were eligible for inclusion. Exclusion criteria were defined to minimize potential confounding factors affecting nasal symptoms or adenoid size and included: (1) acute upper respiratory tract infection at the time of assessment; (2) chronic rhinosinusitis with nasal polyps; (3) significant nasal structural abnormalities, such as severe septal deviation; (4) previous adenoidectomy or tonsillectomy; (5) known systemic immunodeficiency; (6) current systemic immunosuppressive therapy; and (7) concurrent diagnosis of asthma. Written informed consent was obtained from the parents or legal guardians of all participating children.
Assessment of Adenoid Hypertrophy
Adenoid size was assessed using flexible nasal endoscopy performed by experienced clinicians who were blinded to laboratory results at the time of examination. The degree of AH was classified according to a modified endoscopic grading system based on the percentage of choanal obstruction, as previously described and validated in the literature.15 Briefly, adenoid size was graded according to the proportion of choanal obstruction observed during endoscopy, with higher grades indicating greater airway compromise. In general, lower grades correspond to minimal-to-moderate obstruction, whereas higher grades (III–IV) represent substantial to near-complete obstruction of the choanal airway. For the purpose of analysis, patients were grouped into grade III and grade IV AH, representing moderate and severe obstruction, respectively. Grades I and II were not included in the analysis, as the present study focused on clinically significant adenoid hypertrophy. The percentage of choanal obstruction was also recorded as a continuous variable for correlation analyses.
Assessment of AR Severity and Symptom Burden
The severity of allergic rhinitis was evaluated using multiple validated instruments to capture both symptom burden and patient-reported disease impact. The Total Nasal Symptom Score (TNSS) was calculated as the sum of individual scores for nasal obstruction, rhinorrhea, sneezing, and nasal itching, with higher scores indicating greater symptom severity. Overall symptom severity was further assessed using a visual analogue scale (VAS), in which patients or their caregivers rated the overall impact of nasal symptoms on a scale from 0 (no symptoms) to 10 (most severe symptoms). In addition, disease-related quality of life was evaluated using the Pediatric Rhinoconjunctivitis Quality of Life Questionnaire (PRQLQ-S), focusing on the symptom domain. All symptom assessments were completed during the same clinical visit as nasal endoscopy to ensure temporal consistency between clinical evaluation and adenoid assessment.
Laboratory Measurements
Peripheral venous blood samples were collected from all participants for laboratory analysis. Eosinophil counts were measured as part of routine complete blood cell counts. Total serum IgE levels and dust mite–specific IgE (d1 and d2) levels were quantified using standardized immunoassay techniques. All laboratory analyses were performed in a certified clinical laboratory following manufacturer instructions and quality control procedures.
Statistical Analysis
Statistical analyses were performed using GraphPad Prism (GraphPad Software, San Diego, CA, USA). Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were expressed as counts and percentages. Data distribution was assessed using the Shapiro–Wilk normality test. For comparisons between two groups (grade III vs. grade IV AH), normally distributed continuous variables were analyzed using the unpaired Student’s t-test, while non-normally distributed variables were analyzed using the Mann–Whitney U-test. Categorical variables were compared using the χ2-test. Correlations between the percentage of choanal obstruction and clinical or laboratory parameters were assessed using Spearman’s rank correlation analysis. Correlation coefficients (r) and corresponding P values were reported. All statistical tests were two-sided, and a P value < 0.05 was considered statistically significant.
Results
Baseline Characteristics
A total of 170 children with dust mite–sensitized allergic rhinitis were included in the final analysis. Based on nasal endoscopic evaluation, 120 children (70.6%) were classified as having grade III AH, while 50 children (29.4%) were classified as having grade IV hypertrophy. The distribution of age and sex was comparable between the two groups, with no statistically significant differences observed, indicating good baseline demographic comparability (Table 1). The mean age of children with grade III hypertrophy was 6.38 ± 1.48 years, compared with 5.92 ± 1.72 years in the grade IV group. Male-to-female ratios were similar between groups. These findings suggest that differences observed in subsequent analyses were unlikely to be driven by baseline demographic imbalance.
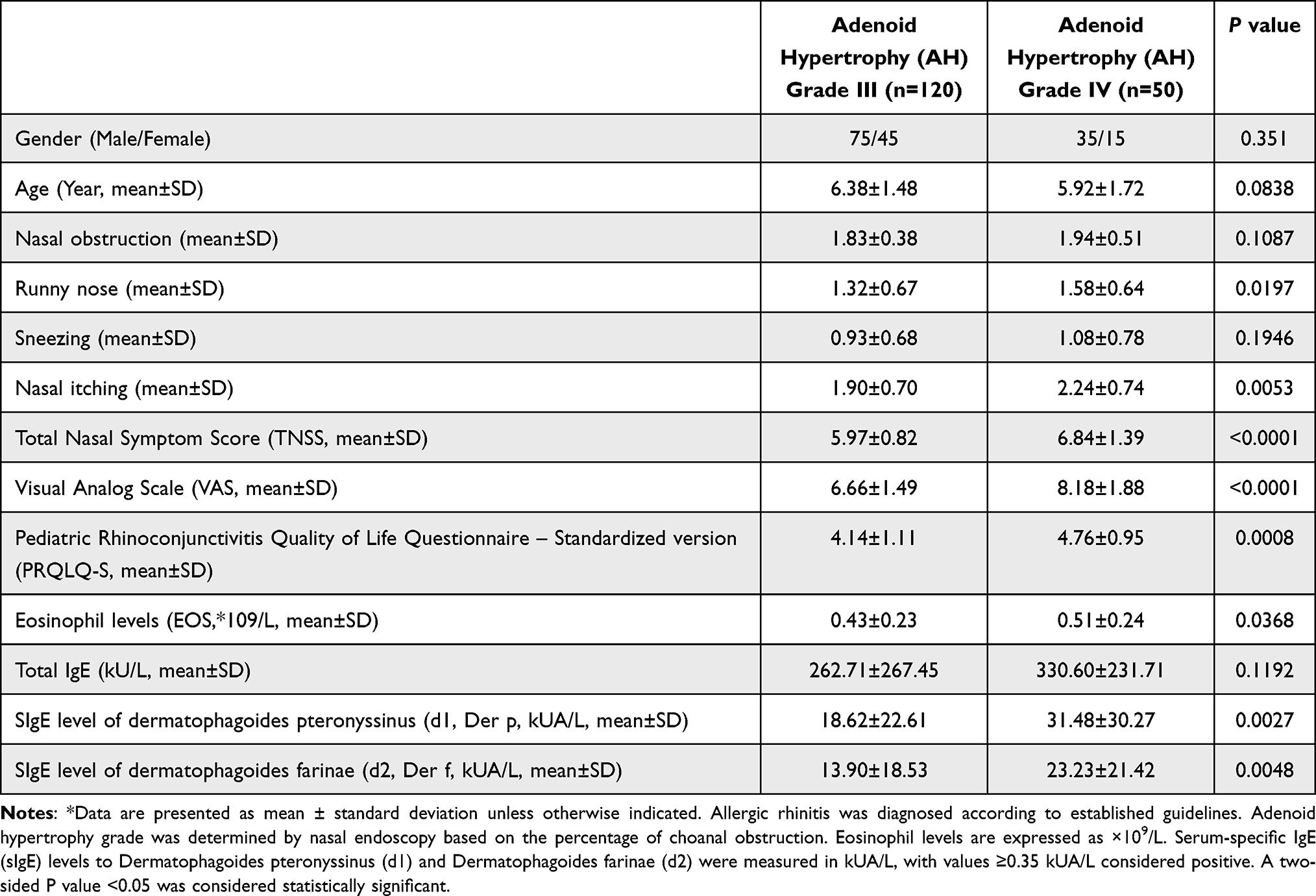 |
Table 1 Clinical Characteristics, Allergic Symptom Severity, and Immunological Profiles of Dust Mite–Sensitized Children with Allergic Rhinitis Stratified by Adenoid Hypertrophy Grade |
Allergic Rhinitis Symptom Severity According to AH Grade
Children with grade IV AH exhibited a significantly greater overall burden of allergic rhinitis symptoms compared with those with grade III hypertrophy. The Total Nasal Symptom Score (TNSS) was significantly higher in the grade IV group (6.84 ± 1.39) than in the grade III group (5.97 ± 0.82; P < 0.0001), indicating more severe cumulative nasal symptoms (Figure 1A). Similarly, overall symptom severity assessed by the visual analogue scale (VAS) was markedly increased in children with grade IV hypertrophy (8.18 ± 1.88 vs. 6.66 ± 1.49; P < 0.0001; Figure 1F). When individual nasal symptoms were analyzed, children with grade IV hypertrophy reported significantly higher scores for nasal obstruction, rhinorrhea, and nasal itching compared with those with grade III hypertrophy (Figure 1B, 1C and E).In contrast, sneezing scores did not differ significantly between the two groups (Figure 1D), suggesting that not all symptom domains were equally associated with adenoid enlargement. Disease-related quality of life was also more adversely affected in children with severe AH. PRQLQ-S scores were significantly higher in the grade IV group than in the grade III group (4.76 ± 0.95 vs. 4.14 ± 1.11; P = 0.0008), reflecting a greater negative impact of allergic symptoms on daily activities and well-being (Figure 1G).
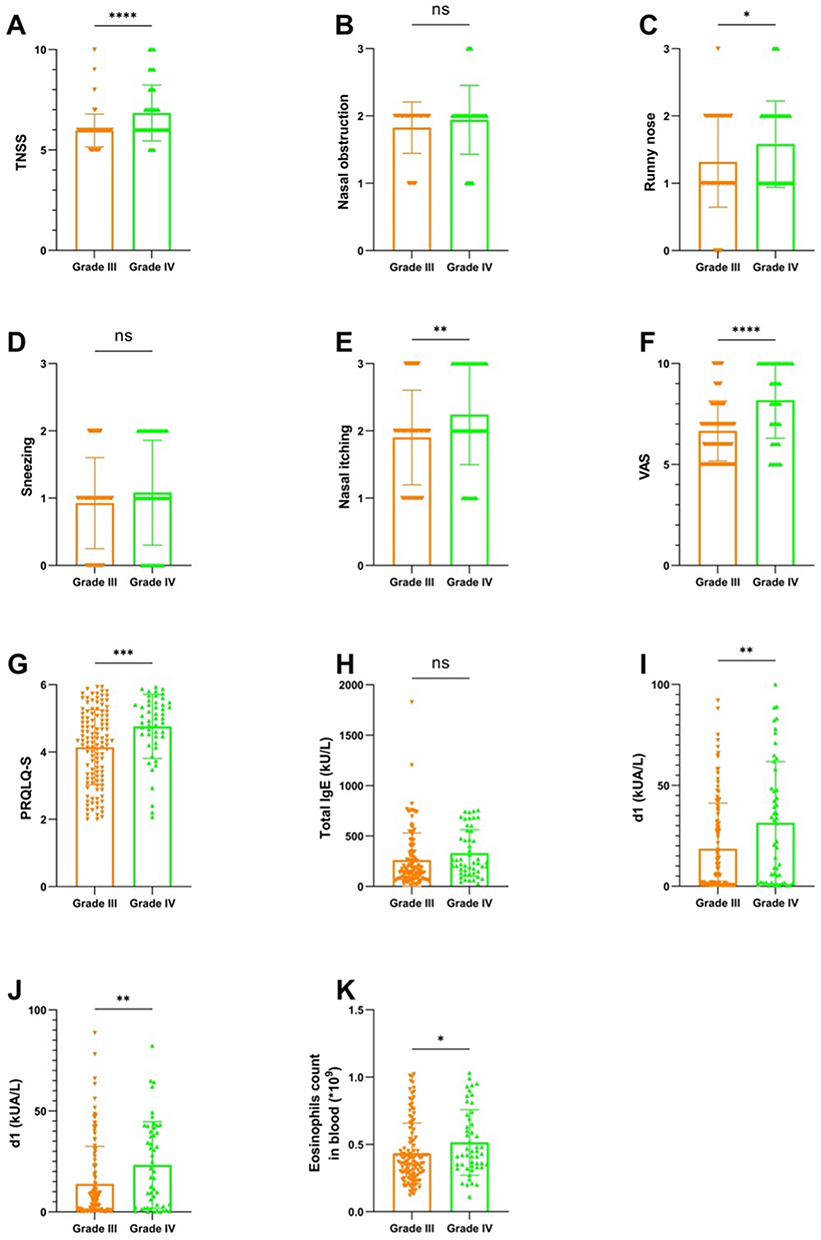 |
Figure 1 Comparison of allergic symptom severity and immunological parameters between grade III and grade IV adenoid hypertrophy in dust mite–sensitized children with allergic rhinitis. Box-and-scatter plots show comparisons of (A) Total Nasal Symptom Score (TNSS), (B) nasal obstruction score, (C) runny nose score, (D) sneezing score, (E) nasal itching score, (F) visual analogue scale (VAS), (G) Pediatric Rhinoconjunctivitis Quality of Life Questionnaire—symptom domain (PRQLQ-S), (H) total serum IgE, (I) Dermatophagoides pteronyssinus–specific IgE (d1), (J) Dermatophagoides farinae–specific IgE (d2), and (K) peripheral blood eosinophil counts between children with grade III and grade IV adenoid hypertrophy as assessed by nasal endoscopy. P values are indicated as follows: ns, not significant (P ≥ 0.05); *P < 0.05; **P < 0.01; ***P < 0.001; ****P < 0.0001. |
Immunological Characteristics According to AH Grade
Differences in immunological parameters were also observed between children with grade III and grade IV AH. Peripheral blood eosinophil counts were modestly but significantly higher in the grade IV group compared with the grade III group (0.51 ± 0.24 ×109/L vs. 0.43 ± 0.23 ×109/L; P = 0.0368; Figure 1K). Total serum IgE levels showed considerable inter-individual variability and did not differ significantly between the two groups (Figure 1H). In contrast, dust mite–specific IgE levels were significantly higher in children with grade IV hypertrophy. Both Dermatophagoides pteronyssinus–specific IgE (d1) and Dermatophagoides farinae–specific IgE (d2) levels were elevated in the grade IV group compared with the grade III group (Figure 1I and J), indicating a higher allergen-specific sensitization burden in children with more severe adenoid obstruction.
Correlation Between Adenoid Obstruction and Allergic Rhinitis Severity
To further explore the relationship between AH and allergic disease severity, Spearman correlation analyses were performed using the percentage of choanal obstruction as a continuous variable. Significant positive correlations were observed between choanal obstruction and multiple measures of allergic rhinitis severity. Specifically, the degree of adenoid obstruction was moderately correlated with TNSS (r = 0.4263, P < 0.001) and VAS scores (r = 0.4584, P < 0.001), indicating that greater adenoid enlargement was associated with increased overall symptom burden (Figure 2B and C). A significant correlation was also observed between choanal obstruction and PRQLQ-S scores (r = 0.3475, P < 0.001; Figure 2A), suggesting that AH was associated with worse disease-related quality of life.
 |
Figure 2 Correlation between adenoid obstruction and allergic symptom severity and inflammatory markers in dust mite–sensitized children with allergic rhinitis. Scatter plots illustrate the associations between the percentage of choanal obstruction assessed by nasal endoscopy and (A) Total Nasal Symptom Score (TNSS), (B) visual analogue scale (VAS), (C) Pediatric Rhinoconjunctivitis Quality of Life Questionnaire—symptom domain (PRQLQ-S), (D) peripheral blood eosinophil count, (E) total serum IgE, (F) Dermatophagoides pteronyssinus–specific IgE (d1), and (G) Dermatophagoides farinae–specific IgE (d2). |
Correlation Between Adenoid Obstruction and Allergic Inflammatory Markers
In addition to symptom-based measures, adenoid obstruction was positively correlated with laboratory markers of allergic inflammation. Peripheral blood eosinophil counts showed a significant but relatively weak correlation with the percentage of choanal obstruction (r = 0.2008, P < 0.001; Figure 2D). Similarly, total serum IgE levels were positively correlated with adenoid obstruction (r = 0.2663, P < 0.001; Figure 2E). Dust mite–specific IgE levels also demonstrated significant positive correlations with adenoid obstruction. Both d1-specific IgE (r = 0.2224, P < 0.001; Figure 2F) and d2-specific IgE (r = 0.1899, P < 0.001; Figure 2G) increased with increasing degrees of choanal obstruction. Compared with symptom-based measures, these correlations were weaker in magnitude, indicating that clinical symptom severity may more closely reflect the integrated impact of chronic allergic inflammation on AH.
Discussions
In this cross-sectional study of dust mite–sensitized children with allergic rhinitis from Northern China, we demonstrated a clear association between allergic disease severity and the degree of AH. Children with more severe adenoid obstruction exhibited higher allergic symptom burden, worse disease-related quality of life, and increased markers of allergic inflammation. Moreover, when adenoid obstruction was analyzed as a continuous variable, significant positive correlations were observed with both symptom-based severity scores and immunological parameters, supporting a severity-dependent relationship between allergic rhinitis and AH.
One important observation of this study is that overall allergic rhinitis severity, as reflected by TNSS and VAS scores, increased in parallel with the degree of adenoid obstruction. Among individual nasal symptoms, nasal obstruction, rhinorrhea, and nasal itching were more strongly associated with severe AH, whereas sneezing did not differ significantly between groups. This finding is consistent with the concept that symptoms related to persistent mucosal inflammation and airflow limitation are more closely linked to structural upper airway changes, while reflex-mediated symptoms such as sneezing may be less dependent on anatomical obstruction. In addition, higher PRQLQ-S scores in children with severe AH indicate that adenoid enlargement is associated not only with increased symptom intensity but also with a broader negative impact on daily functioning and quality of life.16
Beyond symptom-based assessments, we observed significant associations between AH and markers of allergic inflammation. Children with grade IV AH had higher peripheral blood eosinophil counts and higher dust mite–specific IgE levels compared with those with grade III hypertrophy. When analyzed continuously, eosinophil counts, total serum IgE, and dust mite–specific IgE levels all showed positive correlations with the percentage of choanal obstruction. Similar associations between systemic allergic markers and AH have been reported previously, although the strength of these correlations has varied across studies.17,18 The relatively modest magnitude of these correlations in the present study likely reflects the multifactorial nature of AH, in which allergic inflammation interacts with local immune responses, microbial exposure, and host susceptibility.10,19–21
Our findings extend previous reports describing an increased prevalence of AH in children with allergic rhinitis by demonstrating a graded, severity-dependent relationship between allergic disease burden and the degree of adenoid obstruction.22 Most earlier studies relied on binary classifications of allergic rhinitis or AH, which limited their ability to capture dose–response relationships. By stratifying AH severity and integrating clinical symptom scores with immunological parameters, our study provides additional evidence supporting a pathophysiological link between chronic allergic inflammation and adenoid tissue remodeling.
From a mechanistic perspective, the adenoid is an immunologically active lymphoid organ that is continuously exposed to inhaled allergens. In children sensitized to house dust mites, persistent allergen exposure may result in sustained immune activation within nasopharyngeal lymphoid tissue, potentially promoting lymphoid proliferation and progressive adenoid enlargement over time. These findings have important clinical implications. First, AH in children with allergic rhinitis should not be considered solely a mechanical or infection-related condition, but rather as part of a broader allergic inflammatory spectrum. In clinical practice, assessment of allergic rhinitis severity using standardized tools such as TNSS or VAS may help identify children at higher risk of significant adenoid obstruction, thereby enabling earlier risk stratification and closer clinical monitoring. Second, our results suggest that optimization of anti-allergic therapy may have broader benefits beyond symptom control. In children with moderate-to-severe allergic rhinitis and persistent nasal obstruction, treatments such as intranasal corticosteroids, antihistamines, or allergen immunotherapy may not only alleviate symptoms but could also potentially influence the progression of adenoid hypertrophy, although prospective evidence is still needed. Third, integrating allergic disease assessment into the evaluation of pediatric AH may help inform clinical decision-making, particularly regarding the timing of referral, imaging, or consideration of surgical intervention such as adenoidectomy. Conversely, optimized anti-allergic management may improve nasal symptoms and potentially influence adenoid-related outcomes in selected patients, although current evidence remains limited and inconsistent.
Several limitations of this study should be acknowledged. First, the cross-sectional design precludes causal inference, and longitudinal studies are required to determine whether worsening allergic inflammation directly contributes to adenoid growth over time. Second, although strict inclusion and exclusion criteria were applied, residual confounding cannot be fully excluded. Factors such as environmental allergen exposure, microbial colonization, and individual susceptibility may influence both allergic inflammation and adenoid hypertrophy. Third, adenoid size was assessed by nasal endoscopy without histological evaluation, limiting insight into local immune mechanisms within adenoid tissue. Fourth, this was a single-center study focusing on dust mite–sensitized children from Northern China, which may limit the generalizability of the findings to populations with different allergen profiles or environmental conditions. Finally, although multiple systemic markers were included, local inflammatory markers within the nasopharynx were not assessed. Future studies incorporating tissue-level or local immune profiling may provide deeper mechanistic insight into the link between allergic inflammation and adenoid remodeling.
In conclusion, this study demonstrates that increasing severity of allergic rhinitis is associated with greater AH in dust mite–sensitized children. Both clinical symptom burden and allergic inflammatory markers show positive associations with the degree of adenoid obstruction, supporting a severity-dependent relationship between chronic allergic inflammation and adenoid enlargement.
Conclusions
In dust mite-sensitized children with allergic rhinitis, greater disease severity is associated with more severe AH. Adenoid obstruction correlates with allergic symptom burden, impaired quality of life, and markers of allergic inflammation, supporting a severity-dependent relationship between chronic allergic inflammation and adenoid enlargement. Consideration of allergic rhinitis severity may be important in the evaluation of pediatric AH.
IRB Approval Status
This study was approved by the IRB of the Second Qilu Hospital of Shandong University.
Funding
This work was supported by the Qilu “Peak Climbing” Clinical Specialty Construction Program of Jinan.
Disclosure
The authors declare that they have no relevant conflicts of interest in this work.
References
1. Licari A, Magri P, De Silvestri A, et al. Epidemiology of allergic rhinitis in children: a systematic review and meta-analysis. J Allergy Clin Immunol Pract. 2023;11(8):2547–9. doi:10.1016/j.jaip.2023.05.016
2. Bousquet J, Anto JM, Bachert C, et al. Allergic rhinitis. Nat Rev Dis Primers. 2020;6(1):95. doi:10.1038/s41572-020-00227-0
3. Cheng M, Dai Q, Liu Z, et al. New progress in pediatric allergic rhinitis. Front Immunol. 2024;15:1452410. doi:10.3389/fimmu.2024.1452410
4. Anderson HM, Wood RA, Busse WW. Dust mite-induced perennial allergic rhinitis in pediatric patients and sublingual immunotherapy. J Allergy Clin Immunol Pract. 2017;5(1):46–51. doi:10.1016/j.jaip.2016.07.013
5. Zeng Q, Yang C, Li J, et al. Aeroallergen sensitization patterns and related factors in children with allergic rhinitis in guangzhou. Mediators Inflamm. 2025;2025:5887915. doi:10.1155/mi/5887915
6. Xu Q, Shang Y, Li X, et al. Exploring the role of allergenic components in children with house dust mite-induced allergic diseases. J Asthma Allergy. 2025;18:183–193. doi:10.2147/JAA.S505471
7. Xiao X, Feng G, Zhang Y, et al. Young children allergic rhinitis questionnaire is a novel tool for allergy screening in children. Pediatr Allergy Immunol. 2022;33(2):e13738. doi:10.1111/pai.13738
8. Niedzielski A, Chmielik LP, Mielnik-Niedzielska G, et al. Adenoid hypertrophy in children: a narrative review of pathogenesis and clinical relevance. BMJ Paediatr Open. 2023;7(1):e001710. doi:10.1136/bmjpo-2022-001710
9. Ahmad Z, Krüger K, Lautermann J, et al. Adenoid hypertrophy-diagnosis and treatment: the new S2k guideline. HNO. 2023;71(Suppl 1):67–72. doi:10.1007/s00106-023-01299-6
10. Hu L, He W, Li J, et al. The role of adenoid immune phenotype in polysensitized children with allergic rhinitis and adenoid hypertrophy. Pediatr Allergy Immunol. 2024;35(6):e14166. doi:10.1111/pai.14166
11. Hua HL, Deng Y-Q, Tang Y-C, et al. Allergen immunotherapy for a year can effectively reduce the risk of postoperative recurrence of adenoid hypertrophy in children with concurrent allergic rhinitis (IMPROVEII). J Asthma Allergy. 2024;17:1115–1125. doi:10.2147/JAA.S477376
12. Dogru M, Evcimik MF, Calim OF. Does adenoid hypertrophy affect disease severity in children with allergic rhinitis? Eur Arch Otorhinolaryngol. 2017;274(1):209–213. doi:10.1007/s00405-016-4196-x
13. Lou Z. Adenoid hypertrophy in children and allergic rhinitis. Eur Arch Otorhinolaryngol. 2018;275(3):831–832. doi:10.1007/s00405-017-4737-y
14. Arslan E, Tulaci KG, Canakci H, et al. Evaluation of the intranasal steroid treatment outcomes in adenoid tissue hypertrophy with or without allergic rhinitis. Am J Otolaryngol. 2021;42(4):102983. doi:10.1016/j.amjoto.2021.102983
15. Liu H, Feng X, Sun Y, et al. Modified adenoid grading system for evaluating adenoid size in children: a prospective validation study. Eur Arch Otorhinolaryngol. 2021;278(6):2147–2153. doi:10.1007/s00405-021-06768-8
16. Wei X, Yang F, Nong G, et al. The impact of adenoid hypertrophy on obstructive sleep apnea in children with allergic rhinitis: a retrospective analysis of ventilation function and treatment outcomes. Transl Pediatr. 2025;14(10):2765–2774. doi:10.21037/tp-2025-163
17. Zhang H, Sun Y, Shen C, et al. Evaluation value of allergy in adenoid hypertrophy through blood inflammatory cells and total immunoglobulin E. Pediatr Allergy Immunol Pulmonol. 2022;35(4):139–144. doi:10.1089/ped.2022.0114
18. Zhu F, Sun K, Yu L, Sun S, Wan Y, Shi L. Tissue cytokine adenoid experssion in hypertrophic adenoid gland in children with allergic rhinitis. J Coll Physicians Surg Pak. 2021;31(8):903–909.
19. Xu Y, Yu M, Huang X, et al. Differences in salivary microbiome among children with tonsillar hypertrophy and/or adenoid hypertrophy. mSystems. 2024;9(10):e0096824. doi:10.1128/msystems.00968-24
20. Marazzato M, Zicari AM, Aleandri M, et al. 16S Metagenomics reveals dysbiosis of nasal core microbiota in children with chronic nasal inflammation: role of adenoid hypertrophy and allergic rhinitis. Front Cell Infect Microbiol. 2020;10:458. doi:10.3389/fcimb.2020.00458
21. Hao Y, Hu T-Y, Zhao M-Z, et al. The role of type 2 innate lymphoid cells in adenoid hypertrophy with allergic rhinitis among children and related potential therapeutic targets. J Inflamm Res. 2025;18:8593–8605. doi:10.2147/JIR.S515707
22. Evcimik MF, Dogru M, Cirik AA, et al. Adenoid hypertrophy in children with allergic disease and influential factors. Int J Pediatr Otorhinolaryngol. 2015;79(5):694–697. doi:10.1016/j.ijporl.2015.02.017
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Attitude Among Patients and Physicians on Allergic Rhinitis (KAPPA): An International Survey
Bhargave C, Verma M, Jakes RW, Okamoto Y
Journal of Asthma and Allergy 2022, 15:1645-1664
Published Date: 14 November 2022
LINC00998 Modulating M2 Macrophage Activation in Allergic Rhinitis by Stabilizing BOB.1 mRNA

He Y, Tang Y, Wen S, Dong L, Li F, Deng Y, Tao Z
Journal of Inflammation Research 2024, 17:2309-2326
Published Date: 16 April 2024
The Role of Type 2 Innate Lymphoid Cells in Adenoid Hypertrophy with Allergic Rhinitis Among Children and Related Potential Therapeutic Targets
Hao Y, Hu TY, Zhao MZ, Zeng XH, Li K, Cheng BH, Liu DB
Journal of Inflammation Research 2025, 18:8593-8605
Published Date: 1 July 2025