Back to Journals » International Journal of General Medicine » Volume 13
Severely Impaired Renal Function in Unilateral Atherosclerotic Renal Artery Stenosis Indicated by Renal Slow Perfusion
Authors Ai H ![]() , Zhang HP, Yang GJ
, Zhang HP, Yang GJ ![]() , Zheng NX
, Zheng NX ![]() , Tang GD
, Tang GD ![]() , Li H, Zhou Q
, Li H, Zhou Q ![]() , Ren JH, Zhao Y, Sun FC
, Ren JH, Zhao Y, Sun FC
Received 29 August 2020
Accepted for publication 23 September 2020
Published 14 October 2020 Volume 2020:13 Pages 839—845
DOI https://doi.org/10.2147/IJGM.S279457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Hu Ai,1,* Hui-Ping Zhang,1,* Guo-Jian Yang,1 Nai-Xin Zheng,1 Guo-Dong Tang,1 Hui Li,1 Qi Zhou,2 Jun-Hong Ren,3 Ying Zhao,1 Fu-Cheng Sun1
1Department of Cardiology, Beijing Hospital, National Center of Gerontology, Beijing, 100730, China; 2The MOH Key Laboratory of Geriatrics, Beijing Hospital, National Center of Gerontology, Beijing, 100730, China; 3Department of Sonography, Beijing Hospital, National Center of Gerontology, Beijing, 100730, China
*These authors contributed equally to this work
Correspondence: Ying Zhao; Fu-Cheng Sun
Department of Cardiology, Beijing Hospital, National Center of Gerontology, No. 1 DaHua Road, Dong Dan, Beijing 100730, China
Tel +86 15901059087
; Tel +86 15901059087
Email [email protected]; [email protected]
Purpose: Renal artery stenosis leads to ischemic renal insufficiency, but methods for assessing renal perfusion are limited. This study aimed to evaluate the association between renal slow perfusion and impaired renal function in atherosclerotic renal artery stenosis (ARAS).
Patients and Methods: A total of 79 consecutive patients with uncontrolled hypertension who underwent renal angiography and renal dynamic scintigraphy for suspected ARAS were enrolled in the retrospective descriptive study. Based on the status of renal artery stenosis and renal perfusion, participants were divided into three groups: the control group (n=26), the unilateral ARAS with renal normal perfusion group (RNP, n=30), and the unilateral ARAS with renal slow perfusion group (RSP, n=23). RSP was defined as renal blush grade (RBG) ≤ 1, while RBG> 1 belonged to RNP. Split renal function (SRF) was achieved from 99mTc-DTPA renal scintigraphy. The value of the difference in split renal function (DSRF) is contralateral SRF minus impaired SRF of paired kidneys in ARAS. We compared the SRF and DSRF between different groups to identify the association between renal slow perfusion and renal impairment in ARAS.
Results: We analyzed SRF for paired kidneys and found the following: (1) The SRF of the paired kidney was similar in the RNP group (24.3 ± 10.2 mL/min vs 27.5 ± 8.4 mL/min; P = 0.19); however, the impaired SRF was obviously decreased compared with the contralateral SRF in the RSP group (13.5 ± 8.6 mL/min vs 36.7 ± 16.9 mL/min; P < 0.001); and (2) The difference in SRF in the RSP group was significantly higher than that in the control and RNP groups (19.8 ± 11.9 mL/min vs 4.8 ± 8.1 mL/min; 19.8 ± 11.9 mL/min vs 4.6± 3.7 mL/min; P < 0.05).
Conclusion: As an angiographic phenomenon, renal slow perfusion might be an indicator of severely impaired renal function.
Keywords: renal angiography, renal dynamic scintigraphy, renal dysfunction
Introduction
Atherosclerosis is the primary cause of renal artery stenosis (RAS), leading to structural obstruction in the renal artery that retards kidney perfusion and hampers renal function.1 The pathophysiological mechanisms of renal insufficiency in atherosclerotic renal artery stenosis (ARAS) involve multiple factors, including ischemia, essential hypertension, diabetes mellitus, and aging. Several randomized controlled studies demonstrated that revascularization provided no clear benefits for ARAS patients with preserved renal function.2–4 The assessment of anatomical stenoses in the renal artery may not be sufficient to predict renal hypoperfusion, which leads to ischemia and excretory dysfunction. In the past, the index of estimated glomerular filtration rate (eGFR) was widely adopted to assess renal function. However, eGFR was not appropriate for further evaluation of renal function change.5,6 In contrast, it has been reported that renal dynamic scintigraphy can be more sensitive than eGFR and is capable of measuring split renal function in ARAS.7,8 Furthermore, similar to coronary slow flow phenomenon,9 renal slow perfusion (RSP), characterized by delayed opacification of the distal vasculature, may further specify insufficient blood perfusion to uncover severe hypoperfusion in ARAS patients. To explore the relationship between renal perfusion and renal function, patients with only unilateral RAS may be excellent candidates for study because the contralateral and nonstenotic kidney can be utilized as the comparative reference. In this study, we hypothesized that the phenomenon of RSP in ARAS is a type of hemodynamic response to impaired renal function. We further conducted a retrospective study to investigate the relationship between RSP and impaired renal function in unilateral ARAS.
Materials and Methods
Study Population
From June 2016 to December 2019, 128 inpatients with uncontrolled hypertension who underwent renal angiography and renal dynamic scintigraphy for suspected ARAS at the Chinese National Center of Gerontology were retrospectively enrolled in this study. Patients with renal parenchymal diseases, dialysis or bilateral ARAS were excluded. Uncontrolled hypertension was identified if the average SBP was ≥130 mm Hg, or the average DBP was ≥80 mm Hg, regardless of medication use.10 In total, seventy-nine patients (61.7%) were enrolled in the retrospective descriptive study. The control group consisted of 26 consecutive patients with a normal renal artery or stenosis in the renal artery with a diameter < 50%. According to the status of renal perfusion, all unilateral ARAS patients were categorized into the RNP (n=30) and RSP (n=23) groups (Figure 1). ARAS was defined as a diameter reduction of ≥ 50% by renal angiography and had to meet the following two criteria as previously described:11 (1) at least one risk factor for atherosclerosis (diabetes, hyperlipidemia, age > 40 years old, or long-term smoking) and (2) at least two imaging findings for atherosclerosis (tapered stenosis or occlusion of the renal artery, eccentric stenosis, irregular plaque, calcification, primary involvement of the proximal portion or ostium of the renal artery, atherosclerosis present in other abdominal vasculature). Based on renal dynamic scintigraphy, split renal function (SRF) and total glomerular filtration rate (GFR) were evaluated. The difference in split renal function (DSRF) was defined as the difference in split GFR between the two kidneys. Baseline clinical data included age, sex, body mass index (BMI), creatinine (Cr), fasting blood glucose (FBG), cholesterol and serum low-density lipoprotein cholesterol (LDL-C). Histories of disease (hypertension duration, diabetes mellitus, hyperlipidemia, coronary heart disease, peripheral artery disease) were recorded as comorbid conditions. The category of the antihypertensive agent was collected during the process of admission.
 |
Figure 1 Study flow diagram. |
Classification of Renal Perfusion Based on Renal Blush Grade
Selective renal angiography was performed with the soldering technique through the femoral artery or radial artery using a 6F JR4 angiographic catheter near the first lumbar vertebra body post injection of contrast agent. The angiography film was recorded at 15 frames/s. Renal blush grade (RBG) measurement was adapted from the method described by Ehtisham Mahmud et al12 as follows: Grade 0: no parenchymal blush/contrast opacification of cortical vessels or inability of contrast clearance from renal parenchyma after initial opacification; Grade 1: minimal parenchymal blush/contrast opacification of cortical vessels; Grade 2: complete parenchymal blush/contrast opacification of cortical vessels; and Grade 3: hyperemic parenchymal blush/brisk clearance of contrast from cortical vessels. By referring to the criteria for coronary slow flow,13 RSP was defined as RBG ≤ 1, and RNP was defined as RBG > 1. Individual angiography was evaluated by two cardiologists blinded to the results of the renal dynamic scintigraphy (Figure 2).
 |
Figure 2 Example of renal slow/normal perfusion.Images were obtained from renal angiography of 4 subjects in the study. (A) Renal blush grade 0: no contrast opacification of cortical vessels, for ostium of the renal artery close to occlusion; (B) Renal blush grade 1: minimal contrast opacification of cortical vessels, for ostium of the renal artery with severe stenosis; (C) Renal blush grade 2: complete contrast opacification of cortical vessels from a patient with normal renal artery; (D) Renal blush grade 3: hyperemic contrast opacification of cortical vessels when renal hyperperfusion occurred. RSP: RBG 0+1; RNP: RBG 2+3. RSP: Renal Slow Perfusion. RNP: Renal normal perfusion. RBG: Renal Blush Grade. |
SPF Measurement by Renal Dynamic Scintigraphy
Renal dynamic scintigraphy was performed on hydrated patients. Single-photon emission computed tomography (SPECT, GE Millennium TM VG5) was employed to complete the test. Diethylenetriamine pentaacetate acid (DTPA) was provided by the isotope department of the China Institute of Atomic Energy. Tc-99m DTPA (370 MBq) was injected into the cubital vein, followed by rapid acquisition in perfusion mode (3 s/frame, total 20 frames). Dynamic images for functional assessment were acquired with imaging parameters of 256×256 matrix, 30 s/frame and a total 38 frames. The region of interest, extrarenal background and outer renal margin were drawn manually for correcting renography. After the patient’s weight and height were typed into an online computer, the SRF and GFR were automatically calculated by the system according to Gate’s algorithm.
Statistical Analysis
Statistical analyses were conducted using SPSS software (Version 24.0) (IBM Corp., Armonk, NY). Categorical data are presented as counts and percentages, and continuous data are summarized as the mean with standard deviation (SD). Student’s t-test and Chi-square test were employed to compare group differences for continuous and categorical variables, respectively. All P values were two-sided, and the significance level was set at < 0.05.
Results
Study Population
Patients with ARAS had higher serum creatinine and lower GFR than control subjects (108.8 ± 37.7 μmol/L vs 81.8 ± 16.4 μmol/L; 49.6 ± 15.8 mL/min vs 62.6 ± 15.1 mL/min; P < 0.05), and there was no significant difference between the RNP and RSP groups (105.8 ± 39.1 μmol/L vs 112.7 ± 36.3 μmol/L, P = 0.78; 51.7 ± 16.4 mL/min vs 46.7 ± 14.9 mL/min, P = 0.48). The levels of FBG among the control, RNP and RSP groups were significantly different (5.6 ± 1.2 mmol/L vs 6.5 ± 1.7 mmol/L vs 6.9 ± 2.5 mmol/L, P < 0.05). The angiographic stenoses in the renal artery for the RSP group were more severe than those of the control or RNP group (13.5 ± 13.0 vs 72.5 ± 11.5 vs 88.8 ± 9.9, P < 0.05). No significant differences in age, BMI, smoking, long-term hypertension, diabetes, dyslipidemia, peripheral artery disease, or other clinical characteristics were observed for the three groups. The detailed features of the enrolled patients are shown in Table 1.
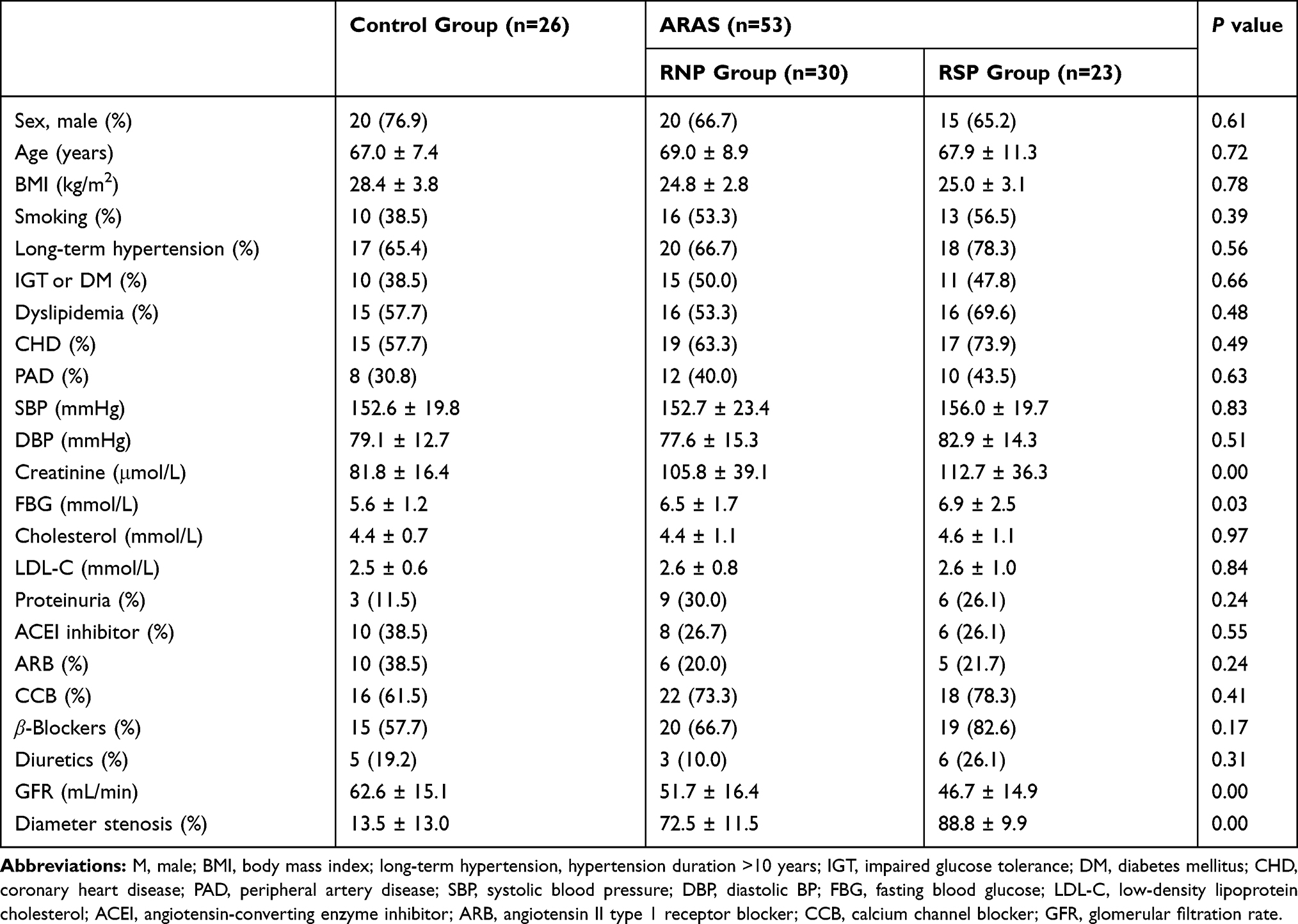 |
Table 1 Patient Characteristics |
Renal Slow Perfusion in Impaired SRF
We compared the impaired SRF with contralateral SRF in 53 unilateral ARAS patients (Figure 3). There were slight differences in SRF in the RNP group (24.3 ± 10.2 vs 27.5 ± 8.4, P = 0.19), but the value of impaired SRF was obviously decreased compared with that of contralateral SRF in the RSP group (13.5 ± 8.6 vs 36.7 ± 16.9, P < 0.001). The impaired SRF of the RSP group was significantly lower than that of the RNP group (13.5 ± 8.6 vs 24.3 ± 10.2, P < 0.05). In contrast, the contralateral SRF in the RSP group was much higher than that in the RNP group (36.7 ± 16.9 vs 27.5 ± 8.4, P < 0.05). The DSRF in the RSP group was significantly higher than that of the control group or RNP group (19.8 ± 11.9 mL/min vs 4.8 ± 8.1 mL/min, 19.8 ± 11.9 mL/min vs 4.6 ± 3.7 mL/min, P < 0.001), and there was no significant difference in DSRF between the control and RNP groups (4.6 ± 3.7 mL/min vs 4.8 ± 8.1 mL/min, P = 0.92) (Figure 4).
 |
Figure 3 Comparison of split renal function between impaired and contralateral kidneys in unilateral ARAS. The value of impaired SRF was obviously decreased compared with that of contralateral SRF in the RSP group (13.5 ± 8.6 vs 36.7 ± 16.9, P < 0.001). The impaired SRF of the RSP group was significantly lower than that of the RNP group (13.5 ± 8.6 vs 24.3 ± 10.2, P < 0.05). In contrast, the contralateral SRF was much higher than that in the RNP group (36.7 ± 16.9 vs 27.5 ± 8.4, P < 0.05), and there were slight differences in SRF in the RNP group (24.3 ± 10.2 vs 27.5 ± 8.4, P = 0.19). |
 |
Figure 4 The difference in SRF in the control, RNP and RSP groups. The difference in SRF in the RSP group was significantly higher than that of the control group and RNP group (19.8 ± 11.9 mL/min vs 4.8 ± 8.1 mL/min, 19.8 ± 11.9 mL/min vs 4.6 ± 3.7 mL/min, P < 0.001). Between the control group and RNP group, there was no significant difference in DSRF (4.6±3.7 vs 4.8±8.1, P = 0.92). |
Discussion
In this study, the major findings included the following: ⑴ ARAS can be divided into two categories, normal renal perfusion and slow renal perfusion, for evaluating restricted blood flow. ⑵ At the time of ARAS diagnosis, most patients presented impaired renal function. ⑶ Renal slow perfusion, shown by angiography, might be connected to severely impaired renal function.
All seventy-nine study subjects were suspected to have ARAS due to uncontrolled hypertension with multiple atherosclerosis risk factors, which gave consistent clinical characteristics for each group. However, with the elevation of serum creatinine and GFR, renal function deteriorated significantly in ARAS patients. Clinically, the progression of renal impairment in patients with ARAS is chronic and usually asymptomatic. In addition to obstruction of the renal artery, there are other risk factors that can continuously affect kidney function, such as aging, hypertension, and diabetes mellitus. Therefore, at the time of diagnosis of ARAS, kidney function had already experienced long-term silent damage and was aggravated by renal ischemia. There were similar representations in several major randomized controlled trials: the average serum creatinine level of each subject was above 140 µmol/l, and the mean eGFR was lower than 50 mL/min in the STAR study.2 These values were more than 170 µmol/l and less than 42 mL/min, respectively, in ASTRAL research.3 The average eGFR of the population was under 60 mL/min in three other clinical studies.4,14,15
Although RAS leads to renal dysfunction, the exact level of reduced renal perfusion can lead to hemodynamic changes. Visual assessment is widely used in diagnosing vascular diseases, but it is not accurate alone in evaluating the stenotic degree of lesions. There was only 41% to 59% agreement on the severity of the lesion in the left main coronary artery,16 and visual assessment tends to overestimate the stenotic severity in coronary lesions.17 It was confirmed that angiographic lesions determined by visual evaluation could not accurately discriminate hemodynamic significance from nonsignificant RAS.18,19 The renal blush grade was first proposed in 2008 and used as a quantitative index of renal perfusion as a complement to angiographic visual assessment.12 Based on the renal blush grade, we first present the renal slow perfusion phenomenon. RSP indicates insufficient blood supply to the kidney due to arterial lumen obstruction in the study.
Renal blood supply is a very complicated process, as the total blood volume to the kidney per minute is highest in relation to weight.20 Adapted to such an abundant blood supply, the regulation mechanism of the kidney’s blood flow is powerful. It was confirmed that the kidney’s self-regulatory mechanisms can still avoid renal parenchymal hypoxia, even if RAS reduces blood flow.21,22 When the renal blood perfusion is partially restricted, renal function can still remain stable due to compensatory effects. Nevertheless, the compensation is insufficient for seriously reduced renal blood perfusion, which will result in renal dysfunction for cortical hypoxia.23 Like coronary slow flow, renal slow perfusion represents a sign of severe kidney hypoperfusion. When renal slow perfusion occurs, ischemia may be the leading cause of impaired renal function, and SRF will be mismatched in unilateral RAS. As a result of decompensation, the function of the affected kidney deteriorated more seriously than the contralateral kidney in the RSP group, but the SRF of the paired kidney remained stable for compensation in the RNP group (Figure 3). In patients with renal slow perfusion, the stenotic kidney had a lower SRF for hypofiltration, while the contralateral (nonstenotic) kidney had a higher SRF for compensatory hyperfiltration. Consequently, the difference in SRF in the renal slow perfusion group increased significantly for inconsistent renal perfusion of the paired kidney (Figure 4). The inconsistency of split renal function in ARAS can be corrected by revascularization.8
Despite the fact that revascularization for ARAS was considered overtreatment,24 several clinical studies have demonstrated that only appropriate patients would benefit from this procedure.25–27 The patients with the serious manifestations would be more likely to benefit from revascularization, the current challenge is to adopt an accurate technique for distinguishing the hemodynamic significance of ARAS and identify which lesions are suitable for interventional treatment.28,29 Patients with insufficient perfusion are more likely to experience a drop in blood pressure after renal artery stenting.12,30 As a marker of renal hypoperfusion, RSP represents deterioration in renal function due to hemodynamic lesions in the renal artery. If validated in future research, the implementation of RSP may be useful for screening appropriate patients for revascularization.
The present research is limited by the retrospective study design in a single center, with a relatively small sample size. RBG is a semiquantitative assessment for renal perfusion, and no other quantitative assessments were performed simultaneously in the study, such as translesional pressure gradients or renal fractional flow reserve. Microcirculation dysfunction in the kidney is another major factor responsible for renal slow perfusion, which is not covered in this study and needs to be explored in future studies. Finally, the subjects were not followed up, and we did not evaluate the long-term effect of RSP on the prognosis of patients.
Conclusion
This retrospective study shows that most patients had renal impairment when ARAS was diagnosed; therefore, the prevention of atherosclerotic diseases and the control of risk factors should be considered the focused treatment. RBG can be used as a semiquantitative assessment of renal perfusion, and it is more reproducible. Renal slow perfusion is a type of invasive imaging procedure to specify the severe reduction in renal flow that can be simply performed in the catheter intervention center. Furthermore, the observed phenomenon provides a hint of impaired renal function and may help identify clinical cohorts who are most likely to benefit from renal revascularization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the Dr. Hu Ai (email: [email protected]) on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the institutional Ethics Committee at Beijing Hospital (decision no. 2019BJYYEC-017-05). This study was conducted in accordance with the Declaration of Helsinki. All patients signed informed consent to undergo renal artery angiography and use of their data for research.
Acknowledgments
We thank all participants in the study.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This project was supported by the Non-profit Central Research Institute Fund of the Chinese Academy of Medical Sciences (2019PT320012) and the Beijing Hospital Clinical Research 121 Project (BJ-2018-198). The funding bodies played an important role in research process, that includes on the design of the study and collection, on writing the manuscript, and were not involved in data processing.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Safian RD, Textor SC. Renal-artery stenosis. N Engl J Med. 2001;344(6):431–442. doi:10.1056/NEJM200102083440607
2. Bax L, et al. Stent placement in patients with atherosclerotic renal artery stenosis and impaired renal function: a randomized trial. Ann Intern Med. 2009;150(12):840–W151. doi:10.7326/0003-4819-150-12-200906160-00119
3. Investigators A, Wheatley K, Ives N, et al. Revascularization versus medical therapy for renal-artery stenosis. N Engl J Med. 2009;361(20):1953–1962. doi:10.1056/NEJMoa0905368
4. Cooper CJ, Murphy TP, Cutlip DE, et al. Stenting and medical therapy for atherosclerotic renal-artery stenosis. N Engl J Med. 2014;370(1):13–22. doi:10.1056/NEJMoa1310753
5. Madder RD, Hickman L, Crimmins GM, et al. Validity of estimated glomerular filtration rates for assessment of baseline and serial renal function in patients with atherosclerotic renal artery stenosis: implications for clinical trials of renal revascularization. Circ Cardiovasc Interv. 2011;4(3):219–225. doi:10.1161/CIRCINTERVENTIONS.110.960971
6. Crimmins GM, Madder RD, Marinescu V, Safian RD. Validity of estimated glomerular filtration rates for assessment of renal function after renal artery stenting in patients with atherosclerotic renal artery stenosis. JACC Cardiovasc Interv. 2008;1(3):543–549. doi:10.1016/j.jcin.2008.03.012
7. Cheung CM, Chrysochou C, Shurrab AE, Buckley DL, Cowie A, Kalra PA. Effects of renal volume and single-kidney glomerular filtration rate on renal functional outcome in atherosclerotic renal artery stenosis. Nephrol Dial Transplant. 2010;25(4):1133–1140. doi:10.1093/ndt/gfp623
8. Saeed A, Fortuna EN, Jensen G. Split renal function in patients with unilateral atherosclerotic renal artery stenosis-effect of renal angioplasty. Clin Kidney J. 2017;10(4):496–502. doi:10.1093/ckj/sfx052
9. Beltrame JF. Defining the coronary slow flow phenomenon. Circ J. 2012;76(4):818–820. doi:10.1253/circj.cj-12-0205
10. Miao H, Liu Y, Tsai TC, Schwartz J, Ji JS. Association Between Blood Lead Level and Uncontrolled Hypertension in the US Population (NHANES 1999–2016). J Am Heart Assoc. 2020;9(13):e015533. doi:10.1161/JAHA.119.015533
11. Xiong H-L, Peng M, Jiang X-J, et al. Time trends regarding the etiology of renal artery stenosis: 18 years’ experience from the China Center for Cardiovascular Disease. J Clin Hypertens. 2018;20(9):1302–1309. doi:10.1111/jch.13356
12. Mahmud E, Smith TWR, Palakodeti V, et al. Renal frame count and renal blush grade: quantitative measures that predict the success of renal stenting in hypertensive patients with renal artery stenosis. JACC Cardiovasc Interv. 2008;1(3):286–292. doi:10.1016/j.jcin.2008.03.012
13. Diver DJ, Bier JD, Ferreira PE, et al. Clinical and arteriographic characterization of patients with unstable angina without critical coronary arterial narrowing (from the TIMI-IIIA Trial). Am J Cardiol. 1994;74(6):531–537. doi:10.1016/0002-9149(94)90739-0
14. Courand P-Y, Dinic M, Lorthioir A, et al. Resistant Hypertension and Atherosclerotic Renal Artery Stenosis: effects of Angioplasty on Ambulatory Blood Pressure. A Retrospective Uncontrolled Single-Center Study. Hypertension. 2019;74(6):1516–1523. doi:10.1161/HYPERTENSIONAHA.119.13393
15. Zeller T, Krankenberg H, Erglis A, et al. A randomized, multi-center, prospective study comparing best medical treatment versus best medical treatment plus renal artery stenting in patients with hemodynamically relevant atherosclerotic renal artery stenosis (RADAR) - one-year results of a pre-maturely terminated study. Trials. 2017;18(1):380. doi:10.1186/s13063-017-2126-x
16. Cameron A, Kemp HG, Fisher LD, et al. Left main coronary artery stenosis: angiographic determination.. Circulation. 1983;68(3):484–489. doi:10.1161/01.cir.68.3.484
17. Zhang H, Mu L, Hu S, et al. Comparison of Physician Visual Assessment With Quantitative Coronary Angiography in Assessment of Stenosis Severity in China. JAMA Intern Med. 2018;178(2):239–247. doi:10.1001/jamainternmed.2017.7821
18. Subramanian R, White CJ, Rosenfield K, et al. Renal fractional flow reserve: a hemodynamic evaluation of moderate renal artery stenoses. Catheter Cardiovasc Interv. 2005;64(4):480–486. doi:10.1002/ccd.20318
19. Jones NJ, Bates ER, Chetcuti SJ, Lederman RJ, Grossman PM. Usefulness of translesional pressure gradient and pharmacological provocation for the assessment of intermediate renal artery disease. Catheter Cardiovasc Interv. 2006;68(3):429–434. doi:10.1002/ccd.20697
20. Epstein FH. Oxygen and renal metabolism. Kidney Int. 1997;51(2):381–385. doi:10.1038/ki.1997.50
21. Gloviczki ML, Glockner JF, Lerman LO, et al. Preserved oxygenation despite reduced blood flow in poststenotic kidneys in human atherosclerotic renal artery stenosis. Hypertension. 2010;55(4):961–966. doi:10.1161/HYPERTENSIONAHA.109.145227
22. Rognant N, Guebre-Egziabher F, Bacchetta J, et al. Evolution of renal oxygen content measured by BOLD MRI downstream a chronic renal artery stenosis. Nephrol Dial Transplant. 2011;26(4):1205–1210. doi:10.1093/ndt/gfq538
23. Gloviczki ML, Glockner JF, Crane JA, et al. Blood Oxygen Level–Dependent Magnetic Resonance Imaging Identifies Cortical Hypoxia in Severe Renovascular Disease. Hypertension. 2011;58(6):1066–1072. doi:10.1161/HYPERTENSIONAHA.111.171405
24. Morgan DJ, Dhruva SS, Wright SM, Korenstein D. Update on Medical Practices That Should Be Questioned in 2015. JAMA Intern Med. 2015;175(12):1960–1964. doi:10.1001/jamainternmed.2015.5614
25. Mangiacapra F, Trana C, Sarno G, et al. Translesional pressure gradients to predict blood pressure response after renal artery stenting in patients with renovascular hypertension. Circ Cardiovasc Interv. 2010;3(6):537–542. doi:10.1161/CIRCINTERVENTIONS.110.957704
26. Ritchie J, Green D, Chrysochou C, Chalmers N, Foley RN, Kalra PA. High-Risk Clinical Presentations in Atherosclerotic Renovascular Disease: prognosis and Response to Renal Artery Revascularization. Am J Kidney Dis. 2014;63(2):186–197. doi:10.1053/j.ajkd.2013.07.020
27. Vassallo D, Ritchie J, Green D, Chrysochou C, Kalra PA. The effect of revascularization in patients with anatomically significant atherosclerotic renovascular disease presenting with high-risk clinical features. Nephrol Dial Transplant. 2018;33(3):497–506. doi:10.1093/ndt/gfx025
28. Mishima E, Suzuki T, Ito S. Selection of Patients for Angioplasty for Treatment of Atherosclerotic Renovascular Disease: predicting Responsive Patients. Am J Hypertens. 2020;33(5):391–401. doi:10.1093/ajh/hpaa016
29. Iwashima Y, Ishimitsu T. How should we define appropriate patients for percutaneous transluminal renal angioplasty treatment? [published online ahead of print, 2020 Jun 22]. Hypertens Res. 2020. doi:10.1038/s41440-020-0496-z
30. Naghi J, Palakodeti S, Ang L, Reeves R, Patel M, Mahmud E. Renal frame count: a measure of renal flow that predicts success of renal artery stenting in hypertensive patients. Catheter Cardiovasc Interv. 2015;86(2):304–309. doi:10.1002/ccd.25946
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.