Back to Journals » Infection and Drug Resistance » Volume 19
Severe Plasmodium falciparum Malaria Presenting with Gastrointestinal Symptoms in South Sudan: A Case Report
Authors Tran AD, Nguyen HT ![]() , Pham HK
, Pham HK
Received 7 February 2026
Accepted for publication 18 April 2026
Published 3 June 2026 Volume 2026:19 601904
DOI https://doi.org/10.2147/IDR.S601904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Arif Siddiqui
Anh Duc Tran,1,2,* Hoang Trung Nguyen,3,* Hong Khanh Pham1,4
1Vietnamese Level-2 Field Hospital No. 6, Bentiu, South Sudan; 2Department of Neurosurgery, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam; 3Department of Military Hygiene, Vietnam Military Medical University, Hanoi, Vietnam; 4Department of Gastroenterology, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam
*These authors contributed equally to this work
Correspondence: Hong Khanh Pham, Department of Gastroenterology, Military Hospital 103, Vietnam Military Medical University, Hanoi, Vietnam, Tel +84 973432282, Email [email protected]
Abstract: Severe Plasmodium falciparum malaria typically presents with fever, chills, and features of multiple organ dysfunction; however, gastrointestinal manifestations may occur early and can be mistaken for gastrointestinal infection. We report the case of a 29-year-old Ghanaian man working in South Sudan who initially presented with nausea, vomiting, and diarrhea. He had not taken malaria chemoprophylaxis and reported inconsistent use of mosquito-prevention measures. He was first diagnosed with acute gastrointestinal infection and treated accordingly. After 24 hours, he developed high-grade fever, headache, tachycardia, and hypotension. On admission, a malaria rapid diagnostic test (RDT) (Bioline Malaria Ag P.f/Pan, Abbott Diagnostics Korea Inc.) was positive; peripheral blood smear microscopy revealed P. falciparum parasitemia graded as (++). Vital signs showed a heart rate of 120 beats/min and blood pressure of 85– 90/55 mmHg. Laboratory findings included elevated total bilirubin (39.6 μmol/L) and creatinine (120 μmol/L), prolonged prothrombin time (22.4s), INR 1.84, and thrombocytopenia (platelet count 50 × 109/L). The patient was diagnosed with severe malaria and was treated promptly with intravenous fluids and intravenous artesunate, along with resuscitation and supportive care. After 3 days, he became afebrile, hemodynamically stable, and was transferred to a primary-level hospital for follow-up. This case highlights that gastrointestinal-onset severe malaria may delay diagnosis; early recognition and timely treatment are critical determinants of a favorable prognosis.
Keywords: severe malaria, Plasmodium falciparum, gastrointestinal symptoms, artesunate
Introduction
Malaria is an infectious disease caused by Plasmodium parasites transmitted by Anopheles mosquitoes, and is classified into uncomplicated malaria and severe malaria.1 P. falciparum is responsible for the most severe cases and the highest mortality; parasite cytoadherence to the vascular endothelium, particularly in the brain, leads to microvascular obstruction and multiple organ failure.1 Initial manifestations commonly include fever, chills, headache, and myalgia; some patients may present with nausea, vomiting, and diarrhea.2 The incubation period ranges from 7 to 30 days but may be prolonged by the use of chemoprophylaxis.1 Without timely diagnosis and treatment, severe malaria can progress rapidly, resulting in death within hours to days.3 Specific therapy includes intravenous artesunate or quinine, and guidelines recommend initiating treatment as early as possible.3 In Africa, malaria remains highly prevalent and is a leading cause of death in children and in non-immune adults.4,5 This diagnostic challenge is particularly relevant in South Sudan, where malaria remains highly endemic and continues to impose a substantial clinical burden.6
Although gastrointestinal symptoms may be part of the clinical spectrum of malaria, overlap with gastroenteritis or gastrointestinal infections can make early diagnosis challenging.2 The literature has reported atypical presentations of severe malaria such as ileus or acute colonic pseudo-obstruction; these cases underscore the heterogeneity of clinical manifestations and the importance of considering malaria in any febrile patient with a history of residence in or travel to endemic areas.7 While gastrointestinal symptoms can occur in malaria, a prominent onset with vomiting/diarrhea may lead to misdiagnosis and management as gastrointestinal infection, thereby delaying specific treatment. We report a case of severe P. falciparum malaria at the Vietnamese Level-2 Field No.6 Hospital (VNL2FH) in South Sudan with gastrointestinal-onset symptoms, to emphasize the value of epidemiological history-taking, early parasitological testing, and timely initiation of artesunate.
Case Presentation
History and Onset
A 29-year-old man of Ghanaian nationality, previously healthy, was working in South Sudan. The patient did not take malaria chemoprophylaxis and reported only intermittent use of mosquito-prevention measures (mosquito net/insect repellent). On 23/10/2024, he developed vomiting (approximately 6 episodes/day) and diarrhea (4 episodes/day); the stools contained no mucus or blood and were associated with dehydration (dry oral mucosa, reduced sweating, and oliguria). He first received treatment at a Level-1 field facility, a lower-level primary medical post providing initial assessment, basic treatment, and stabilization. At the Level-1 field hospital, he was diagnosed with acute gastroenteritis/gastrointestinal infection and was treated with intravenous 0.9% NaCl and 5% glucose, ciprofloxacin 750 mg twice daily, and antiemetic therapy with intramuscular metoclopramide 10 mg. However, his symptoms did not improve and progressively worsened. On day 2 (24/10/2024), he continued to have frequent vomiting, developed tachycardia and hypotension, and then high fever (39.5°C), chills/rigors, headache, and generalized myalgia/arthralgia. Given suspicion of malaria, he was urgently transferred overnight to the Vietnamese Level-2 Field Hospital in South Sudan, a higher-level referral field hospital with inpatient, laboratory, and emergency management capability.
Examination on Admission and Investigations
In the emergency department, the patient was alert, made good contact, and was oriented to time. He was tachycardic (120 beats/min), hypotensive (blood pressure 85/55 mmHg), and tachypneic (25 breaths/min). Physical examination revealed dehydration without overt jaundice. A rapid diagnostic test for malaria was positive for P. falciparum (++) (Figure 1). Laboratory tests showed elevated serum creatinine (120 µmol/L), elevated liver enzymes (AST/ALT), hyperbilirubinemia (39 µmol/L), prolonged prothrombin time (22.4s) with INR 1.84, thrombocytopenia (50 ×109/L), and mild hypokalemia (K⁺ 3.2 mmol/L) (Table 1). The patient met the 2023 WHO criteria for severe P. falciparum malaria (hypotension/shock and impaired perfusion with hepatic and renal involvement).8
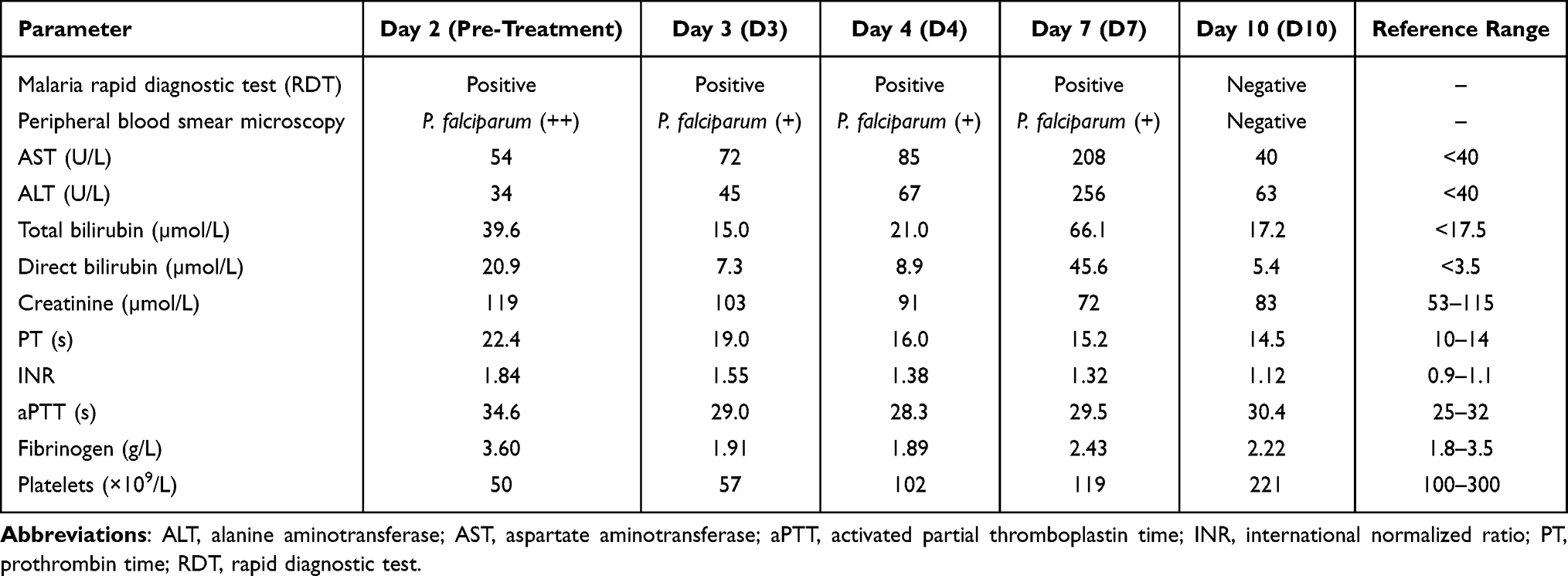 |
Table 1 Key Laboratory Results Over Time |
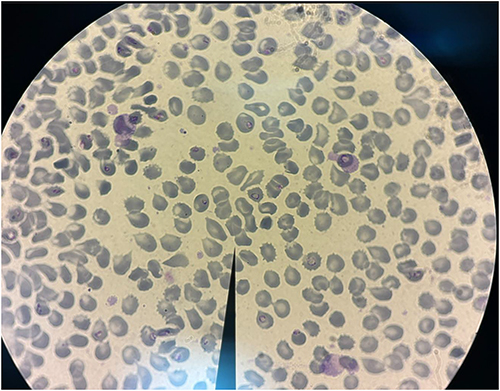 |
Figure 1 Giemsa-stained thin peripheral blood smear showing intraerythrocytic ring-form trophozoites of Plasmodium falciparum on illness day 2 (pre-treatment). |
Treatment and Clinical Course
Immediately after admission, the patient underwent intensive resuscitation with intravenous fluid therapy, hemodynamic monitoring (blood pressure, heart rate, SpO2), urine output monitoring, and antipyretic measures. Specific antimalarial treatment was initiated with intravenous artesunate at 2.4 mg/kg at 0, 12, and 24 hours on 24/10/2024, followed by 2.4 mg/kg once daily on 25/10/2024. Intravenous artesunate was discontinued after the last dose on 25/10/2024. Once he was clinically stable and able to tolerate oral medication, he was transitioned to an oral artemisinin-based combination therapy (ACT), pyronaridine–artesunate (Pyramax®), 4 tablets once daily after meals for 3 days from 26/10/2024 to 28/10/2024, after which the ACT course was completed. Supportive therapy included intravenous fluids, vitamin K1, and hepatoprotective treatment. After 6 hours of treatment, blood pressure improved, and mental status became clearer.
By treatment day 3 (26/10/2024), the patient was afebrile, alert, and hemodynamically stable Total bilirubin normalized within 48 hours. On 27/10/2024 (treatment day 4; after completion of intravenous artesunate and with stable hemodynamics), the patient was transferred to a Level-1 facility to complete the ACT course and for follow-up.
At follow-up on illness day 7 (30/10/2024), laboratory testing showed a rebound increase in bilirubin accompanied by elevated liver enzymes; however, the patient remained clinically stable and received supportive treatment per the local facility’s regimen, including silymarin (Silymax® 140 mg, 4 tablets/day) and spironolactone (Verospiron® 25 mg, 4 tablets/day). Clinical reassessment at day 7 showed that the patient was afebrile, alert, and hemodynamically stable, with no recurrent vomiting, diarrhea, or other new warning signs. Follow-up investigations included repeat liver biochemistry, renal function tests, coagulation parameters, platelet count, malaria rapid diagnostic testing, and peripheral blood smear microscopy. On 01/11/2024, blood biochemical indices returned to normal. Repeat clinical assessment remained unremarkable, and no complications or severe sequelae were identified during continued follow-up.
Post-treatment malaria parasitological testing (peripheral blood smear) was negative on 05/11/2024, and the patient returned to normal daily activities and work. At 6-month follow-up (04/2025), the patient reported no recurrent symptoms and had returned to normal daily activities without clinical evidence of relapse.
Discussion
Severe malaria caused by P. falciparum is the most severe form of malaria and may lead to hepatic and renal failure, as well as neurological and respiratory complications; mortality is high if treatment is not initiated early.3 Parasitized erythrocytes adhere to the vascular endothelium, particularly in the brain and other organs, resulting in microvascular obstruction and a pronounced inflammatory response.1 Clinical manifestations are heterogeneous; in addition to fever and chills, patients may present with headache, myalgia, fatigue, dyspnea, jaundice, gastrointestinal disturbances, and, rarely, atypical features such as intestinal pseudo-obstruction or ileus, as reported in case studies.7 Gastrointestinal manifestations in P. falciparum malaria are likely multifactorial. Systemic inflammatory responses with cytokine release, together with microvascular sequestration of parasitized erythrocytes causing relative ischemia in the splanchnic/mesenteric circulation, may contribute to nausea, vomiting, abdominal pain, or diarrhea. Reduced hepatic blood flow and malaria-associated hepatic dysfunction may further amplify gastrointestinal symptoms, particularly in severe disease.9–11
This case highlights a common diagnostic pitfall in malaria-endemic settings: an initial presentation dominated by gastrointestinal symptoms may lead to a preliminary diagnosis of gastrointestinal infection, while the patient can deteriorate rapidly. In our patient, day 0 (23/10) was characterized mainly by vomiting and diarrhea without typical features; by day 1 (24/10), he developed high-grade fever (39.5°C) accompanied by hypotension (85/55 mmHg) and altered mental status, with thrombocytopenia (50 ×109/L), INR 1.84, total bilirubin 39 µmol/L, and creatinine 120 µmol/L; parasitological testing confirmed P. falciparum (++). This clinical course is consistent with current criteria for severe malaria, in which hypotension/shock and impaired consciousness are warning signs requiring emergency treatment.8 Gastrointestinal symptoms (vomiting, diarrhea, abdominal pain) may occur in malaria, with a wide-ranging frequency depending on population characteristics and epidemiological context;2 therefore, if early assessment relies primarily on gastrointestinal manifestations, clinicians may be biased toward common gastrointestinal conditions.12 Moreover, the patient had no prior history of malaria, and the epidemiological history obtained at the initial assessment was incomplete, which further increased the risk of misdiagnosis. In this case, a key clue was that the patient was working in a high-transmission area and had not taken chemoprophylaxis; thus, malaria testing (RDT/blood smear) should be requested early, even when gastrointestinal symptoms are prominent. Delayed diagnosis may result in severe complications, and severe malaria can progress rapidly to death if not treated promptly.3 Therefore, in clinical practice, any patient with fever, headache, or gastrointestinal symptoms and a history of residence in or travel to malaria-endemic areas should undergo parasitological testing to exclude malaria.
P. falciparum is transmitted through the bite of infected female Anopheles mosquitoes.13 Our patient, a Ghanaian national, a country with a high malaria burden, was working in South Sudan, a malaria-endemic region, and did not use bed nets or chemoprophylaxis, placing him at high risk of infection. The incubation period of P. falciparum is typically 7–14 days but may be longer or shorter depending on host immunity and chemoprophylaxis.1 In addition, mosquito activity peaks at dusk; sleeping under insecticide-treated nets, using insect repellents, and environmental sanitation are effective preventive measures.
Current management of severe malaria prioritizes intravenous artesunate. Clinical studies and practice guidelines have shown that artesunate is highly effective, with more rapid parasite clearance and lower mortality than quinine.3,14,15 According to current WHO recommendations, parenteral artesunate is the first-line initial treatment for severe P. falciparum malaria and should be started as early as possible, but it should not be regarded as isolated definitive single-agent therapy. Instead, once the patient is clinically stable and able to tolerate oral medication, treatment should be completed with a full course of oral artemisinin-based combination therapy (ACT).8 In this case, the patient received aggressive resuscitation, intravenous artesunate according to protocol, and was subsequently transitioned to oral ACT once his clinical condition improved, which is consistent with stepwise guideline-concordant management of severe malaria; by treatment day 3 (26/10/2024; D3), he was afebrile, alert, and hemodynamically stable Total bilirubin decreased within the first 48 hours; however, at follow-up on illness day 7 (30/10/2024), the RDT remained positive and bilirubin rebounded with concurrent elevation of liver enzymes, despite clinical stability. These indices improved at the subsequent assessment on illness day 10 (02/11/2024).
To explain the persistence of RDT positivity and the rebound increase in bilirubin/transaminases around day 7, we propose several considerations. First, RDTs—particularly HRP2-based tests—may remain positive after effective treatment due to persistent circulating antigen. A meta-analysis reported that approximately half of HRP2-RDTs remain positive about 15 days after treatment initiation, and a small proportion may persist even longer.16 Therefore, RDT should not be used alone to determine treatment failure; follow-up should be based on peripheral blood smear microscopy or quantitative parasitemia in conjunction with clinical course. Second, the rise in bilirubin and liver enzymes around day 7 may be multifactorial, including malaria-related hepatic dysfunction with incomplete recovery, and/or biochemical adverse effects associated with certain ACT regimens.17 A systematic review of pyronaridine–artesunate reported transient transaminase elevations, typically peaking around day 7 and subsequently declining, with most cases not resulting in clinically significant outcomes.18 In our patient, clinical stability and the return of laboratory indices toward normal on subsequent testing support a benign recovery course; nevertheless, this finding underscores the need for post-treatment monitoring of hepatic function, particularly when bilirubin and aminotransferases rise during the first week. The patient had no documented neurological or respiratory complications, peripheral blood smear was negative on 05/11/2024, and no relapse occurred at 6-month follow-up.
More broadly, the case reports summarized in Table 2 indicate that malaria with gastrointestinal-onset or predominant gastrointestinal symptoms encompasses a wide clinical spectrum, ranging from abdominal pain, vomiting, and diarrhea to severe and atypical presentations such as acute pancreatitis, ileus, or acute colonic pseudo-obstruction. A notable shared feature is that many cases were initially oriented toward a gastrointestinal diagnosis; however, patients subsequently deteriorated rapidly with high fever, hemodynamic instability, (in some reports, altered mental status), and malaria was only confirmed after parasitological testing. When recognized promptly and treated according to guidelines with intravenous artesunate, together with fluid resuscitation, close monitoring, and supportive care (with additional interventions when indicated), most patients demonstrated a favorable response and recovered.7,19–21
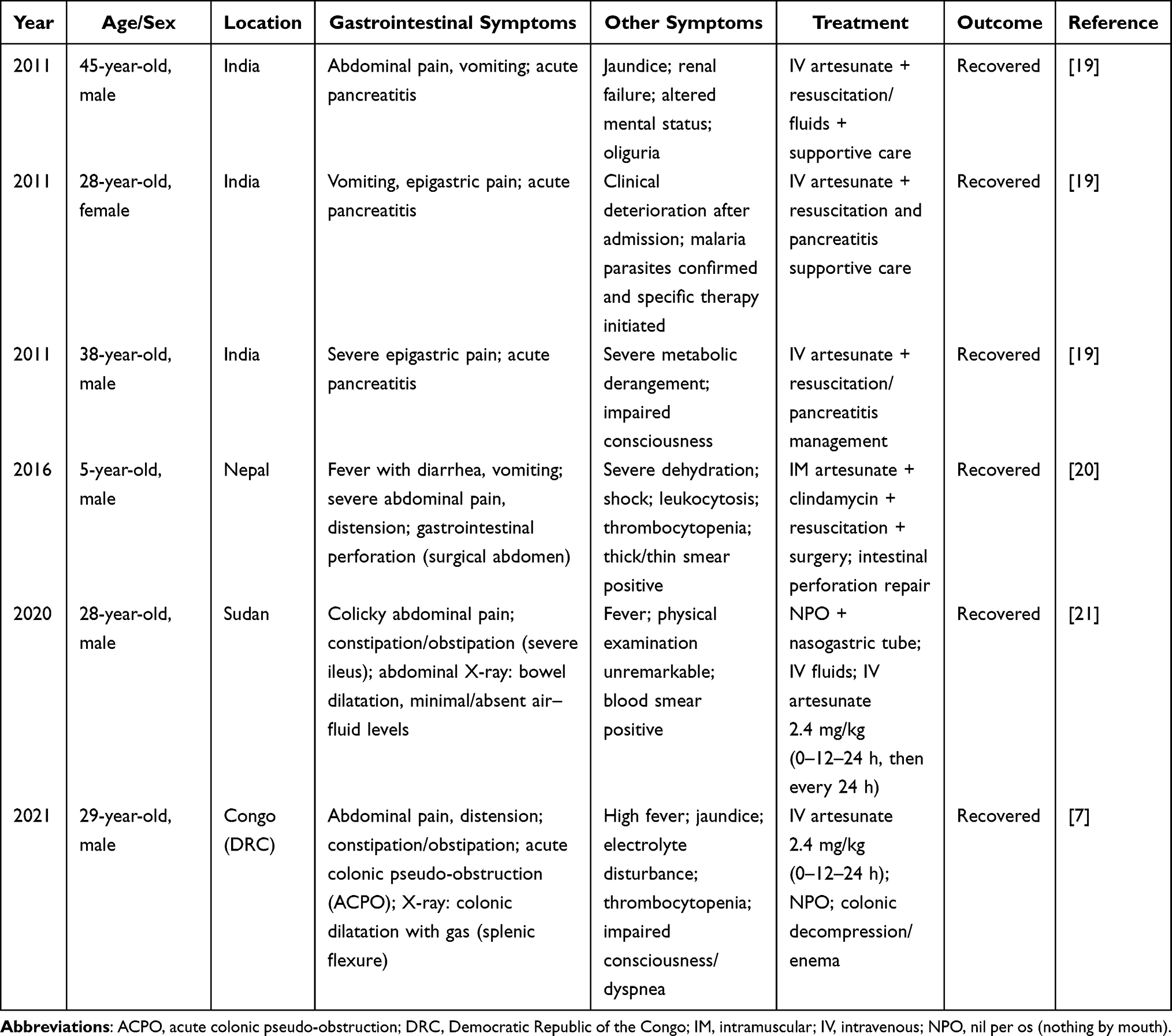 |
Table 2 Summary of Selected Cases of Severe P. falciparum Malaria Presenting with Gastrointestinal Symptoms |
This report has several limitations. First, it describes a single case and therefore cannot be used to infer causality or generalize the frequency or clinical course of gastrointestinal-predominant severe malaria. Second, some early clinical and laboratory data from the initial Level-1 facility were unavailable, which limited reconstruction of the full early disease trajectory. Third, no molecular characterization of the parasite or antimalarial resistance testing was performed. Fourth, although the patient remained well at 6-month follow-up, longer-term follow-up and serial laboratory monitoring might have provided additional information regarding the transient rebound in bilirubin and liver enzyme levels observed during the first week after treatment.
Conclusion
In summary, severe P. falciparum malaria is a medical emergency that can progress rapidly and cause death if diagnosis and treatment are delayed. Our case demonstrates that gastrointestinal disturbances (vomiting, diarrhea) may be prominent presenting features, potentially leading to misdiagnosis and delayed management when epidemiological risk factors are not adequately elicited. Therefore, heightened clinical vigilance is required, with careful assessment of residence/occupational history or travel to endemic areas, and early malaria testing (RDT and/or peripheral blood smear) in patients with fever or atypical infectious syndromes in the presence of exposure risk. Timely initiation of parenteral artesunate in accordance with recommendations, followed by transition to an oral ACT once the patient is clinically stable, is pivotal to improving treatment outcomes.
AI Statement
During the preparation of this manuscript, the authors used ChatGPT (Model 5.2) solely to assist with English language editing, grammar, and spelling correction in order to improve clarity and readability. After using this tool, the authors carefully reviewed and revised the manuscript as necessary and take full responsibility for the scientific content, interpretations, and conclusions presented in the published article.
Abbreviations
AST, aspartate aminotransferase; ALT, alanine aminotransferase; PT, prothrombin time; INR, International Normalized Ratio; RDT, rapid diagnostic test; VNL2FH, Vietnamese Level-2 Field Hospital No. 6 in South Sudan.
Data Sharing Statement
Anonymized clinical data related to this case report may be made available from the corresponding author upon reasonable request, in accordance with institutional regulations and patient confidentiality requirements.
Ethical Approval
All procedures performed in relation to this case were in accordance with the ethical standards of the responsible institutional committee and with the principles of the Declaration of Helsinki. According to institutional policy, formal ethics committee approval was not required for publication of a single anonymized case report. Written informed consent for publication was obtained from the patient.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Written consent is available by request.
Acknowledgments
The authors would like to thank all physicians and staff of the Vietnamese Level-2 Field Hospital No. 6 in South Sudan for their support and assistance in the data collection for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no financial support for the research and publication of this article.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. US Centers for Disease Control and Prevention. Clinical features of malaria [Internet]. Available from: https://www.cdc.gov/malaria/hcp/clinical-features/index.html.
2. Sey IC, Ehimiyein AM, Bottomley C, Riley EM, Mooney JP. Does malaria cause diarrhoea? A systematic review. Front Med. 2020;7:589379. doi:10.3389/fmed.2020.589379
3. Trampuz A, Jereb M, Muzlovic I, Prabhu RM. Clinical review: severe malaria. Crit Care. 2003;7(4):315. doi:10.1186/cc2183
4. Doolan DL, Dobaño C, Baird JK. Acquired immunity to malaria. Clin Microbiol Rev. 2009;22(1):13–7. doi:10.1128/CMR.00025-08
5. Kulohoma BW, Wesonga CS. Malaria prevention in children and pregnant women: a review of gaps and emerging challenges in sub-Saharan Africa. NPJ Womens Health. 2026;4(1):1. doi:10.1038/s44294-025-00124-5
6. Molina-De la Fuente I, Sagrado Benito MJ, Lasry E, et al. Seasonal malaria chemoprevention in a context of high presumed sulfadoxine-pyrimethamine resistance: malaria morbidity and molecular drug resistance profiles in South Sudan. Malar J. 2023;22(1):345. doi:10.14740/jmc3801
7. Yao PF, Zhang PJ, Dong H, Sun Y. Acute colonic pseudo-obstruction in severe falciparum malaria: a case report. J Med Cases. 2021;12(12):481. doi:10.14740/jmc3801
8. World Health Organization. WHO Guidelines for Malaria. Geneva: World Health Organization; 2023.
9. Sriboonvorakul N, Chotivanich K, Silachamroon U, et al. Intestinal injury and the gut microbiota in patients with Plasmodium falciparum malaria. PLoS Pathog. 2023;19(10):e1011661. doi:10.1371/journal.ppat.1011661
10. Day NPJ, Hien TT, Schollaardt T, et al. The prognostic and pathophysiologic role of pro- and antiinflammatory cytokines in severe malaria. J Infect Dis. 1999;180(4):1288–1297. doi:10.1086/315016
11. Molyneux ME, Looareesuwan S, Menzies IS, et al. Reduced hepatic blood flow and intestinal malabsorption in severe falciparum malaria. Am J Trop Med Hyg. 1989;40(5):470–476. doi:10.4269/ajtmh.1989.40.470
12. Kästner M, Hemmer CJ, Reisinger EC. Gastrointestinal symptoms may reflect complicated falciparum malaria. Dtsch Med Wochenschr. 2024;149(8):454–457. doi:10.1055/a-2274-4182
13. Djihinto OY, Medjigbodo AA, Gangbadja AR, et al. Malaria-transmitting vectors microbiota: overview and interactions with anopheles mosquito biology. Front Microbiol. 2022;13:891573. doi:10.3389/fmicb.2022.891573
14. Malaria SEAQUAMAT Study Group. Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial. Lancet. 2005;366(9487):717–725. doi:10.1016/S0140-6736(05)67176-0
15. Dondorp AM, Fanello CI, Hendriksen IC, et al. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet. 2010;376(9753):1647–1657. doi:10.1016/S0140-6736(10)61924-1
16. Dalrymple U, Arambepola R, Gething PW, Cameron E. How long do rapid diagnostic tests remain positive after anti-malarial treatment? Malar J. 2018;17(1):228. doi:10.1186/s12936-018-2371-9
17. Sagara I, Beavogui AH, Zongo I, et al. Safety and efficacy of re-treatments with pyronaridine-artesunate in African patients with malaria: a substudy of the WANECAM randomised trial. Lancet Infect Dis. 2016;16(2):189–198. doi:10.1016/S1473-3099(15)00318-7
18. Duparc S, Borghini-Fuhrer I, Craft CJ, et al. Safety and efficacy of pyronaridine-artesunate in uncomplicated acute malaria: an integrated analysis of individual patient data from six randomized clinical trials. Malar J. 2013;12(1):70. doi:10.1186/1475-2875-12-70
19. Mohapatra M, Gupta M. Falciparum malaria complicated with acute pancreatitis: a report of case series. J Vector Borne Dis. 2011;48(3):177.
20. Bhandari TR, Shahi S, Poudel R, Chaudhary N. A child with severe malaria presenting with acute surgical abdomen (Duodenal Perforation). Case Rep Pediatr. 2016;2016(1):3092130. doi:10.1155/2016/3092130
21. Albashir AAD. A case of Falciparum malaria presenting with features of functional bowel obstruction. Oxf Med Case Reports. 2020;2020(10):omaa098. doi:10.1093/omcr/omaa098
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Malaria-Associated Acute Kidney Injury: A Key Driver of Mortality in Endemic Regions
Olwit G, Gutanamuka TB, Chris-Uchendu HC, Mugisha AI
International Journal of Nephrology and Renovascular Disease 2026, 19:600266
Published Date: 30 March 2026