Back to Journals » Infection and Drug Resistance » Volume 15
Severe Intravascular Hemolysis from Clostridium perfringens Septicemia in a Neonate with Necrotizing Enterocolitis in China: A Case Report
Authors Li Z, Yan C, Gong X, Wang J ![]()
Received 7 January 2022
Accepted for publication 21 March 2022
Published 2 April 2022 Volume 2022:15 Pages 1461—1465
DOI https://doi.org/10.2147/IDR.S355621
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sahil Khanna
Zhiqi Li,1 Chongbing Yan,2 Xiaohui Gong,2 Junfang Wang2
1Department of Neonatology, ChangNing Maternity and Infant Health Institute, Shanghai, 200051, People’s Republic of China; 2Department of Neonatology, Shanghai Children’s Hospital, Shanghai Jiao Tong University, Shanghai, 200062, People’s Republic of China
Correspondence: Junfang Wang, Department of Neonatology, Shanghai Children’s Hospital, Shanghai Jiao Tong University, Shanghai, 200062, People’s Republic of China, Tel +86 21 52976179, Email [email protected]
Abstract: Clostridium perfringens (C. perfringens) is a gram-positive anaerobic bacillus. As an opportunistic pathogen, C. perfringens can colonize the intestine of infants, but highly pathogenic forms are uncommon in newborns. Sporadic cases of neonatal infection have been reported worldwide, but no case has yet been reported in Chinese neonates. We herein report the first Chinese neonate who developed severe intravascular hemolysis and necrotizing enterocolitis following C. perfringens septicemia. A 7-day-old full-term female newborn was admitted to our hospital with necrotizing enterocolitis. The patient developed severe intravascular hemolysis on the day of admission and underwent continuous renal replacement therapy for hyperkalemia and severe acute kidney injury. Despite optimal treatment, this baby died at 20 hours after admission. Clinical metagenomic next-generation sequencing for pathogen detection showed a positive result for C. perfringens. Literature on C. perfringens-associated sepsis in neonates was reviewed to offer a reference for clinical practice. Our case demonstrates that neonatologists should consider a diagnosis of C. perfringens infection in a newborn when symptoms of severe intestinal infection and intravascular hemolysis are present, so that early treatment can be initiated.
Keywords: Clostridium perfringens, neonate, intravascular hemolysis, necrotizing enterocolitis
Introduction
Clostridium perfringens (C. perfringens) was first identified by William H. Welch in 1891 from the autopsy of a 38-year-old man. It is a gram-positive, spore-forming, anaerobic, rod-shaped bacillus. Clinically, C. perfringens has been associated with a variety of systemic and intestinal diseases in humans and animals including gas gangrene, food poisoning, and non-foodborne diarrhea and enterocolitis.1 Massive intravascular hemolysis (MIH) is the most serious complication of C. perfringens sepsis and has a poor prognosis. The course of blood-culture confirmed C. perfringens sepsis with MIH has been reported as fulminant, with shock or death occurring in most patients.2 Therefore, clinicians need to use various detection methods to identify C. perfringens infection rapidly so that it may be treated aggressively with antibiotics.
C. perfringens infections are infrequently encountered in neonates, and no such case has been previously reported in China. Since C. perfringens may be normally found in the human intestinal tract, it should be considered as a potential opportunistic pathogen when a newborn shows symptoms of severe intestinal infection and intravascular hemolysis.3 Neonatologists should be aware of the epidemiology and pathogenicity of C. perfringens so that an early diagnosis could be made and treatment can be instituted promptly.
Case Report
The patient was a 7-day-old female newborn admitted to the Department of Neonatology for poor feeding and bloody stools. She was delivered at term by cesarean section, the indication being a scarred uterus in the mother. Her birth weight was 3300g. The antenatal period was uncomplicated, and there was no history suggestive of infections in the mother. The baby was apparently well till the 6th day of life, when she developed poor feeding and bloody stools, followed by loss of consciousness the next day, while she was transported to our Neonatal Intensive Care Unit (NICU). On admission, her vital parameters were as follows: temperature 35.6°C, heart rate 170 beats per minute, respiratory rate 65 times per minute, capillary refill time >3 seconds and blood pressure 35/23mmHg. The baby was unresponsive, had dry mucous membranes, diminished pulses, mottled cold extremities and decreased urine output (<1 mL/kg/h). In addition, significant abdominal distention was noted, without abdominal wall cellulitis.
Laboratory data on admission showed a white blood cell count (WBC) of 38.51×109/L, of which polymorphonuclear cells were 49%, lymphocytes 38.8%, and monocytes 12.2%. Hemoglobin (Hb) concentration was 14.6g/dL, and platelet count was 279×109/L. C-reactive protein was 37mg/L. Coagulation results (prothrombin time 16.2 sec; activated partial thromboplastin time 34 sec) were normal on arrival at the NICU. Necrotizing enterocolitis (NEC) was confirmed by abdominal X-ray and computed tomography (CT) scan of the abdomen showing pneumatosis intestinalis and portal venous gas (Figure 1). Ascitic fluid examination performed six hours after initiation of antibiotics showed a WBC count of 2815×106/L, with 56% polymorphonuclear cells, 15% lymphocytes, and 29% monocytes/macrophages and a red blood cell count of 55×106/L. Blood culture and fecal culture collected before antibiotic administration did not show any bacterial growth.
 |
Figure 1 Computed tomography (CT) scan of abdomen showing pneumatosis intestinalis (A and B) and portal venous gas (C) (indicated by the red arrows). |
At admission, normal saline was administered immediately as rapid fluid resuscitation along with dopamine to ameliorate shock. Empiric antibiotic therapy was started with intravascular ceftazidime and penicillin G sodium. Despite initiation of antibiotics, the infant continued to deteriorate. Two hours after admission, abdominal distension had increased, and the baby had developed soy sauce-colored urine and jaundice. This was accompanied by a progressive decrease in hemoglobin concentration from 14.6 g/dL to 5.1 g/dL (Figure 2). The direct antiglobulin test (DAT) and acid elution results were negative. The infant received a transfusion of 60 mL of red blood cells (RBCs). The blood potassium was 8.7mmol/L and premature ventricular contractions were frequently observed. Continuous renal replacement therapy (CRRT) was initiated because of acute kidney failure and hyperkalemia. Antibacterial therapy was switched to vancomycin (15mg/kg/dose intravenously every eight hours) and meropenem (40mg/kg/ dose intravenously every eight hours) based on standard dose empirically. Antibiotics for meningitis were administered when the patient was in critical condition and we could not obtain cerebrospinal fluid to confirm the presence of a central nervous system infection. Repeated coagulation tests were abnormal (prothrombin time >180 sec; activated partial thromboplastin time >120 sec), and there was an increase in the concentration of fibrin degradation products and D-Dimer, indicating disseminated intravascular coagulation (DIC) (Table 1). Clinical metagenomic next-generation sequencing (NGS) for pathogen detection showed a positive result for C. perfringens. However, an explorative laparotomy could not be performed due to the poor general condition of the patient. Despite all measures, our patient died from multi-organ failure on the second hospital day.
 |
Table 1 Changes in the Laboratory Tests and Outcomes of the Disease in Different Days of the Infection |
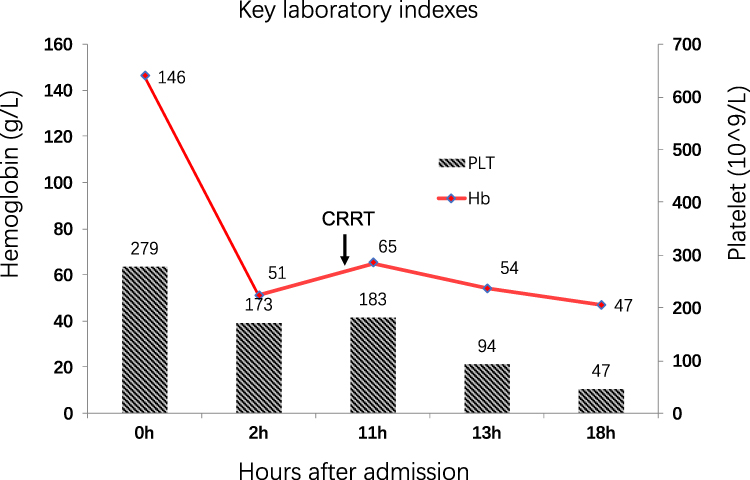 |
Figure 2 Changes in platelet count (black) and hemoglobin (Hb) levels (red) during hospitalization. The initiation of CRRT is indicated by the black arrow. The X axis shows the number of hours after admission. |
Discussion
C. perfringens is an aero-tolerant anaerobe and can survive in aerobic environments such as the surfaces in hospital wards. It can cause disease in aerophilic environments such as the intestinal tract of adults and infants. The immature and underdeveloped immune system of newborns and premature infants is ineffective against pathogenic bacteria. When C. perfringens invades the human body, it multiplies rapidly and releases a large amount of toxin into the blood.4 C. perfringens sepsis is uncommon but fatal.5 Its invasiveness is due to its capacity to generate an array of lethal toxins and enzymes. C. perfringens has seven major toxinotypes A–G (previously only types A–E),6 and is further classified based on the production of the six major toxins: alpha toxin (CPA), beta toxin (CPB), epsilon toxin (ETX), iota toxin (ITX), enterotoxin (CPE), and necrotic enteritis B-like toxin (NetB).7 In addition, C. perfringens produces many enzymes, such as lecithinase, fibrinase, hyaluronidase, collagenase and DNA enzyme, which contribute to its invasiveness.
Acute hemolytic anemia due to C. perfringens has been mainly described in adults. Reports in newborns are less common. Severe intravascular hemolysis associated with C. perfringens occurs in 7% to 15% of patients with C. perfringens bacteremia and has a mortality rate of 70% to 100%.8 Two studies of 40 and 50 adult patients showed that median times from onset of symptoms to death were 8 hours and 9.7 hours, respectively.2,9 It has been suggested that initiation of antibiotics after clostridium infection may trigger bacterial lysis and release a large number of biologically active enzymes and toxins.10 Bacterial-derived toxins and enzymes may cause cell lysis and tissue necrosis, and may participate in intravascular hemolysis through different mechanisms. In our patient, the urine color was dark yellow at admission and gradually deepened to soy sauce color two hours after admission (after initiation of antibiotics), accompanied by a significant decrease in hemoglobin.
Acute hemolysis may also be caused by potent extracellular toxins produced by C. perfringens, such as alpha (α) toxin and perfringolysin O (PFO), which have hemolytic activity in vitro. The α toxin is a phospholipase C that lyses sphingomyelin and phosphatidylcholine, which are the main components of cell membranes. The destruction of cell membrane integrity can cause sphericity and hemolysis of RBCs and expose free cholesterol molecules in the cell membrane. PFO belongs to the cholesterol-dependent cytolysin (CDC) family, which acts as a pore-forming toxin on cholesterol-containing membranes.11 Suzaki et al analyzed the pathogenic characteristics of C. perfringens strains isolated from patients with MIH and showed that PFO was the main factor responsible for hemolysis in these patients.5
In the 1970s, C. perfringens type A was isolated from the necrotic tissues of many premature NEC patients. Myonecrosis was found in the intestine on histological examination.12 Most studies on the association between NEC and C. perfringens have been conducted in premature infants,13 with very few reports in full-term infants. Several predisposing factors have been identified in these patients, such as an immature gut, the presence of bacteria, universal administration of broad-spectrum antibiotics, and hypoxia and ischemia around pathological sites.13 Our patient however, had no known predisposing factors. She developed the disease at home and had no history of antibiotic use. This may be due to the ubiquitousness and resilience of C. perfringens in habitable environments, allowing easy transmission to newborns. Therefore, neonatologists should be vigilant about C. perfringens infection when NEC occurs in full-term infants.
The clinical manifestations of C. perfringens infection vary widely, ranging from asymptomatic infections to severe life-threatening septic shock. In addition to inducing intravascular hemolysis, C. perfringens sepsis may present with fever, shock, and organ failure (especially renal failure). Liu et al reported that 6 of their 17 patients presented with renal failure. Four of these patients received blood purification treatment.14 Our patient also presented with septic shock and renal failure and received continuous renal replacement therapy to remove inflammatory factors and stabilize the internal environment. Despite the early use of antibiotics and blood purification, the disease progressed, probably due to a high concentration of C. perfringens bacteria and extracellular toxins in the patient’s blood. We could not inoculate the anaerobic blood culture bottle due to an inadequate sample, hence could not get a positive blood culture for C. perfringens. We identified the pathogen using NGS. It has been reported that NGS testing can be used for the targeted detection of a specific pathogen with high sensitivity, specificity and culture-independence.15
When neonates develop necrotizing enterocolitis and unexplained hemolysis, clinicians should be on high alert for the possibility of C. perfringens infection. Due to its high mortality, early blood smears, anaerobic blood cultures or metagenomic tests are required for early detection and timely initiation of appropriate antibiotic treatment.
Abbreviations
MIH, massive intravascular hemolysis; NICU, neonatal intensive care unit; WBC, white blood cell; Hb, hemoglobin; NEC, necrotizing enterocolitis; CT, computed tomography; DAT, direct antiglobulin test; RBC, red blood cell; CRRT, continuous renal replacement therapy; DIC, disseminated intravascular coagulation; NGS, next-generation sequencing; PFO, perfringolysin O; CDC, cholesterol-dependent cytolysin.
Data Sharing Statement
All data generated or analyzed during this study are included in this article.
Ethics Approval and Informed Consent
The study was reviewed and approved by the Ethics Committee of Shanghai Children’s Hospital in China (20Z11900605). The parents of the patient provided written informed consent for publication of medical data.
Acknowledgments
We are thankful for the members of the family for their participation and help in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
References
1. Sim K, Shaw AG, Randell P, et al. Dysbiosis anticipating necrotizing enterocolitis in very premature infants. Clin Infect Dis. 2015;60(3):389–397. doi:10.1093/cid/ciu822
2. van Bunderen CC, Bomers MK, Wesdorp E, Peerbooms P, Veenstra J. Clostridium perfringens septicaemia with massive intravascular haemolysis: a case report and review of the literature. Neth J Med. 2010;68(9):343–346.
3. Shaw AG, Cornwell E, Sim K, et al. Dynamics of toxigenic Clostridium perfringens colonisation in a cohort of prematurely born neonatal infants. BMC Pediatr. 2020;20(1):75. doi:10.1186/s12887-020-1976-7
4. Law ST, Lee MK. A middle-aged lady with a pyogenic liver abscess caused by Clostridium perfringens. World J Hepatol. 2012;4(8):252–255. doi:10.4254/wjh.v4.i8.252
5. Suzaki A, Ohtani K, Komine-Aizawa S, Matsumoto A, Kamiya S, Hayakawa S. Pathogenic characterization of Clostridium perfringens strains isolated from patients with massive intravascular hemolysis. Front Microbiol. 2021;12:713509. doi:10.3389/fmicb.2021.713509
6. Rood JI, Adams V, Lacey J, et al. Expansion of the Clostridium perfringens toxin-based typing scheme. Anaerobe. 2018;53:5–10. doi:10.1016/j.anaerobe.2018.04.011
7. Petit L, Gibert M, Popoff MR. Clostridium perfringens: toxinotype and genotype. Trends Microbiol. 1999;7(3):104–110. doi:10.1016/S0966-842X(98)01430-9
8. Kapoor JR, Monteiro B, Tanoue L, Siegel MD. Massive intravascular hemolysis and a rapidly fatal outcome. Chest. 2007;132(6):2016–2019. doi:10.1378/chest.07-0853
9. Simon TG, Bradley J, Jones A, Carino G. Massive intravascular hemolysis from Clostridium perfringens septicemia: a review. J Intensive Care Med. 2014;29(6):327–333. doi:10.1177/0885066613498043
10. Moh-Klaren J, Bodivit G, Jugie M, et al. Severe hemolysis after plasma transfusion in a neonate with necrotizing enterocolitis, Clostridium perfringens infection, and red blood cell T-polyagglutination. Transfusion. 2017;57(11):2571–2577. doi:10.1111/trf.14196
11. Heuck AP, Savva CG, Holzenburg A, Johnson AE. Conformational changes that effect oligomerization and initiate pore formation are triggered throughout perfringolysin O upon binding to cholesterol. J Biol Chem. 2007;282(31):22629–22637. doi:10.1074/jbc.M703207200
12. Pedersen PV, Hansen FH, Halveg AB, Christiansen ED, Justesen T, Høgh P. Necrotising enterocolitis of the newborn–is it gas-gangrene of the bowel. Lancet. 1976;308(7988):715–716. doi:10.1016/S0140-6736(76)90009-X
13. Neu J, Walker WA. Necrotizing enterocolitis. N Engl J Med. 2011;364(3):255–264. doi:10.1056/NEJMra1005408
14. Liu F, Xue S, Zhang Y, et al. Clostridium perfringens sepsis in three patients with acute leukemia and review of the literature. Int J Hematol. 2021;113(4):508–517. doi:10.1007/s12185-020-03060-z
15. Schmoch T, Westhoff JH, Decker SO, et al. Next-generation sequencing diagnostics of bacteremia in pediatric sepsis. Medicine. 2021;100(25):e26403. doi:10.1097/MD.0000000000026403
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.