Back to Journals » Infection and Drug Resistance » Volume 16
Severe Cutaneous Adverse Reaction Caused by Carbamazepine and Levofloxacin After Varicella Zoster Virus Infection
Authors Wang M, Lin L, Wang L, Li L ![]()
Received 21 December 2022
Accepted for publication 16 March 2023
Published 23 March 2023 Volume 2023:16 Pages 1705—1711
DOI https://doi.org/10.2147/IDR.S402267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Meifang Wang,* Li Lin,* Leyi Wang, Linfeng Li
Department of Dermatology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Linfeng Li, Department of Dermatology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China, Tel +86-13693620186, Email [email protected]
Abstract: Severe cutaneous adverse reactions (SCARs) to drugs are associated with morbidity, mortality, healthcare costs, and challenges in drug development. It is important to identify the SCAR type early by using strict diagnostic criteria because they may require different treatments, follow-ups, and short- or long-term prognoses. A 68-year-old woman admitted to our hospital presented with fever and rashes for 10 days. This case exhibited many features that suggested acute generalized exanthematous pustulosis (AGEP). However, the course of treatment and verified clinical features led to a diagnosis of AGEP and drug rash with eosinophilia and systemic symptoms (DRESS) syndrome that was induced by carbamazepine and levofloxacin after a herpes zoster infection. AGEP combined with DRESS syndrome is a complicated and rare drug-induced dermatological eruption that follows a course similar to DRESS syndrome and more recalcitrant than the course seen with typical AGEP. The associated factors for the SCARs in our patient included age, history of allergy, viral infection, and drugs interacting with specific HLA loci. Improving our understanding of these factors can improve the treatment and prevention of SCARs in these patients.
Keywords: severe cutaneous adverse reaction, SCARs, acute generalized exanthematous pustulosis, AGEP, drug reaction with eosinophilia and systematic syndrome, DRESS syndrome, overlapping feature, carbamazepine, varicella zoster virus infection
Introduction
Adverse cutaneous reactions to drugs are common and affect 2–3% of all hospitalized patients. About 2% of these are classified as severe cutaneous adverse reactions (SCARs).1 SCARs to drugs are clinically heterogeneous with atypical symptoms in their initial stage. A large area of skin lesions may lead to skin damage and/or infection and can involve various visceral symptoms.2 Therefore, it is important to pay attention to cutaneous and internal changes in response to SCARs because early identification can improve support and treatment of the affected patients.3
Acute generalized exanthematous pustulosis (AGEP) is a less severe SCAR that is characterized by rapidly arising nonfollicular pustules caused by drugs such as antibiotics and is considered a self-limiting disease with a good prognosis.4,5 More severe SCARs include Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, all of which are even potentially life threatening.2 It was rarely reported that the AGEP and DRESS syndrome coexisted in the same patient except for few cases owing to several antibiotics6,7 COVID-19 vaccines,8,9 and other causative drugs10–13 (Table 1). Here, we report a case of AGEP overlapping with DRESS syndrome caused by carbamazepine (CBZ) and levofloxacin treatment after varicella zoster virus infection.
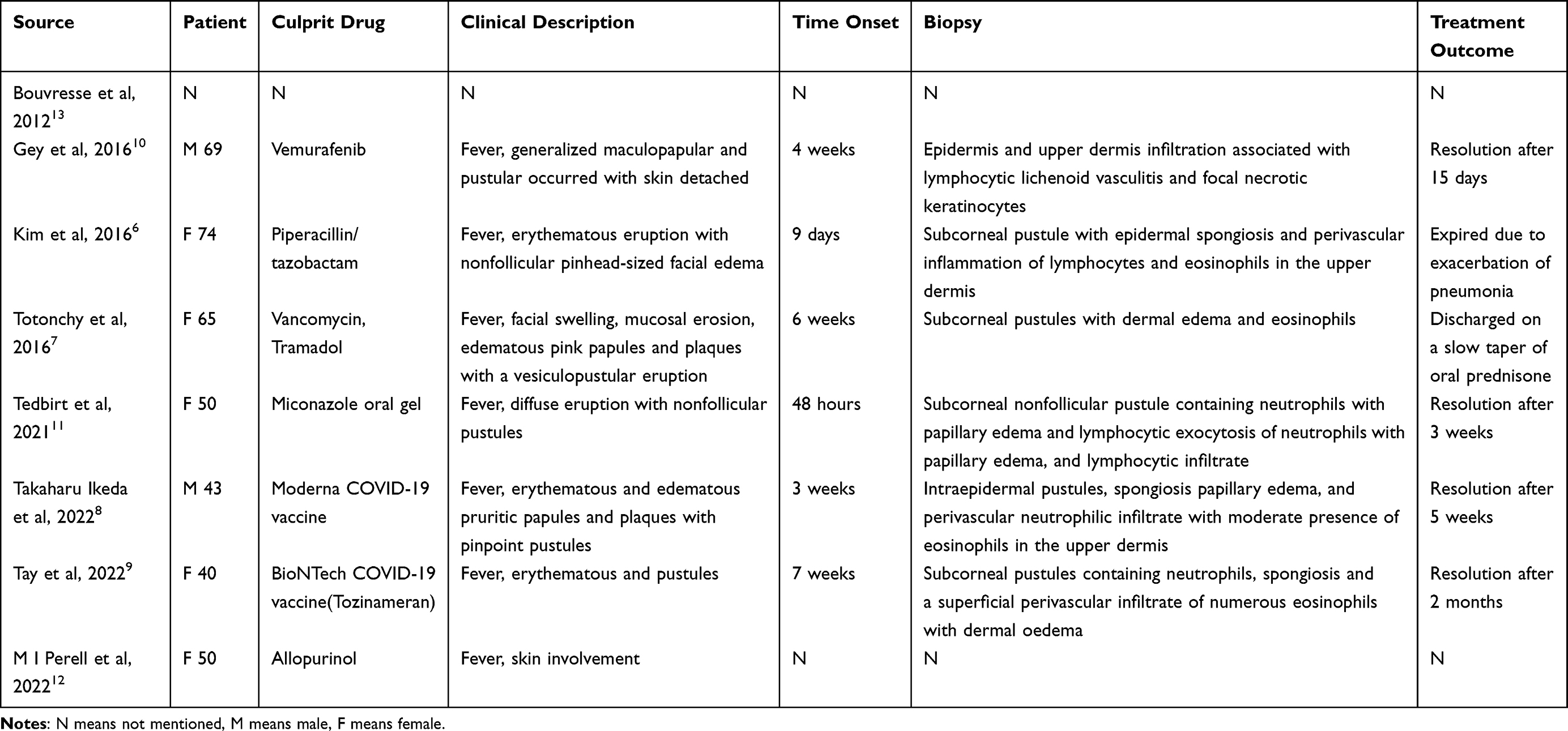 |
Table 1 AGEP and DRESS Overlap Cases-Literature Review |
Case Report
A 68-year-old Chinese woman was admitted to our hospital and presented with a fever (38.5 °C), flushing, and mucosal rashes for 10 days before admission. After taking the drug of ebastine and levofloxacin prescribed by community doctor, the rash spread rapidly and diffusely 9 days ago. Morphological features included oral and vulval mucosal inflammation, erosion with pus on the mucosal surface, diffuse pruritic erythematous eruptions with nonfollicular pinhead-sized pustules on the neck, trunk, and both upper extremities, along with purpura on the lower extremities (Figure 1). Three months before admission, she had a herpes zoster infection. One month after infection, she had post-herpetic neuralgia for which she took CBZ for 1 week to treat the pain. Her previous medical history included allergic reactions to rifampin and levofloxacin 6 years ago.
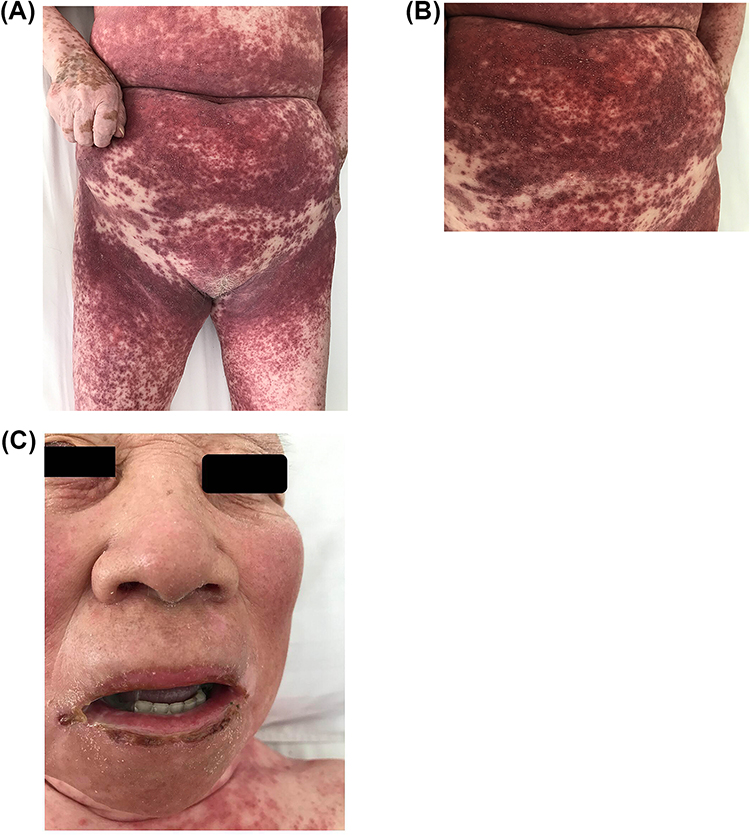 |
Figure 1 (A and B) Diffuse pruritic erythematous eruptions with nonfollicular pinhead-sized pustules (C) Perioral erosion and pus on the mucosal surface. |
Laboratory analysis revealed leukocytosis (46.35×109), neutrophilia (26.21×109), achroocytosis (12.25×109), eosinophilia (1.82×109), anti-RO/SSA52(+++), anti-RO/SSA60(+++), Epstein-Barr virus (EBV) DNA load (+,832 copies/mL), and a total immunoglobulin E (IgE)>1000. Her blood test showed normal functioning of her kidney, liver, and heart. A chest computerized tomography scan showed multiple enlarged lymph nodes in the mediastinum, bimaxillary region, and cardio-diaphragmatic angle, as well as interstitial lung disease. An ultrasound showed splenomegaly. A skin biopsy revealed subcorneal pustules with epidermal spongiosis and perivascular inflammation of lymphocytes and eosinophils in the upper dermis and papillary edema (Figure 2).
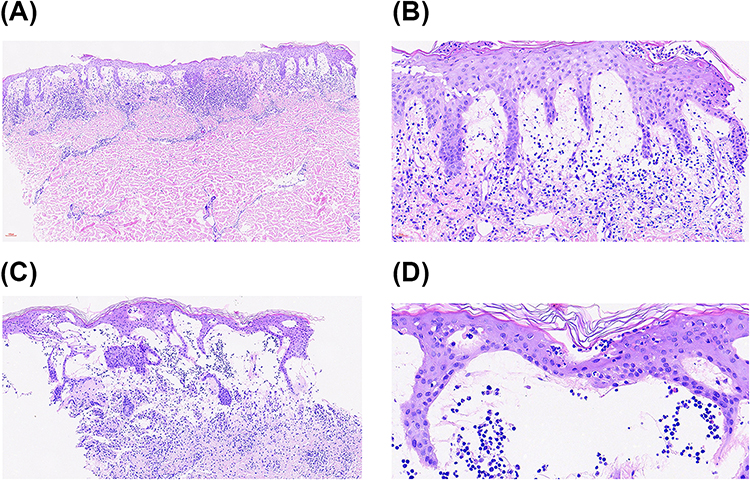 |
Figure 2 Histopathology showing subcorneal pustules containing neutrophils on stratum corneum, papillary edema and perivascular infiltrate of lymphocytes on the superficial dermis ((A and B) for erythematous lesions); Skin biopsy showing basketweave stratum corneum with subcorneal pustules containing neutrophils, subepidermal and perivascular infiltrate of abundant lymphocytes and a small number of neutrophils and eosinophils on the superficial dermis ((C and D) for pustular lesions) (hematoxylineosin-saffron stain, original magnification ×10, 2A and 2C: ×20, 2B:×40, 2D). |
Based on the clinical and histopathological findings, the patient was first diagnosed with AGEP. With an initial dose of methylprednisolone (80 mg/d), the pustules became desquamations after three days and most of the rashes disappeared after 2 weeks. However, red itching papules beside the flexures erupted again when the dose was decreased to 32 mg/day. Based on the recurring rash and laboratory examination, we considered a diagnosis of DRESS syndrome. To address this, we increased her dose of methylprednisolone back to 80 mg/day together with intravenous immunoglobulin (IVIG) for approximately 10 days, after which the rashes and itching improved. We proceeded cautiously with the withdrawal of the glucocorticoid according to our clinical observations (Figure 3). She was discharged from our hospital on the 52nd day on a regimen of oral methylprednisolone 50 mg/day. After 18 months of treatment, we reduced her cortisone dose to 10 mg/day. According to the RegiSCAR criteria and EuroSCAR AGEP validation score,4,8 the clinical features of our patient could be classified as “probable” for both AGEP and DRESS syndrome. Therefore, our final diagnosis was AGEP that overlapped with DRESS syndrome.
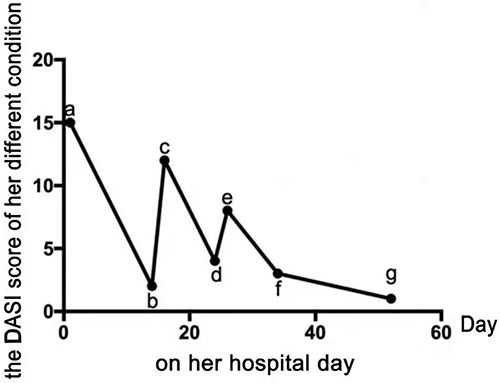 |
Figure 3 (A) On her hospital day 1: Just admission to hospital; (B) On her hospital day 14: After methylprednisolone (80 mg/4 days, 60 mg/4 days, 40 mg/4 days, ivgtt) treatment; (C) On her hospital day 16: Decreased dose to 32mg (po); (D) On her hospital day 24: After methylprednisolone (80 mg/10 days) and IVIG (10g/5 days); (E) On her hospital day 26: Decreased dose to 60 mg(ivgtt); (F) On her hospital day 34: After methylprednisolone (60 mg/5 days) and IVIG (10g/5 days). (G) On her hospital day 52: After methylprednisolone (60/40 mg 7 days) and discharged home from the hospital on a regimen of oral methylprednisolone (60 mg on odd days and 40 mg on even days). |
Discussion
In this case, our initial diagnosis of AGEP was based on her medical history of allergy to levofloxacin along with her presentation of rash, hyperleukocytosis, and neutrophilia, and the almost resolved lesions after the 15-day treatment with methylprednisolone. However, the subsequent disease course with papules and itching was unexpected. Combined with a history of oral CBZ for herps zoster infection, morphological features, and positivity for EBV, we considered the possibility of DRESS syndrome. In support of this, the EuroSCAR AGEP and RegiSCAR DRESS scores for this case were 6 and 5, respectively, which classified the condition as “probable” for both AGEP4 and DRESS syndrome.14 Overlapping SCARs are defined as cases that fulfill the criteria for a definite or probable diagnosis of at least two SCARs according to these scoring systems.13 Therefore, we diagnosed this patient with AGEP overlapping with DRESS syndrome caused by CBZ and levofloxacin.
Despite the limited possibility of internal organ involvement in AGEP, there are some reports showing lymph node enlargement, slight reduction in creatinine clearance, or slight elevation in liver enzyme levels.4,15 DRESS syndrome is a severe systemic drug eruption commonly associated with antibiotics and other drugs1,16 such as CBZ, which is the most common cause for this condition.17 Patients with DRESS syndrome typically present with fever, facial edema, skin rashes, eosinophilia, and internal organ involvement, which can be life threatening and carry a non-negligible risk of severe sequelae.1,16–18 The skin manifestations in DRESS syndrome can be polymorphous, the most common of which is a morbilliform rash that is characterized by a diffuse, pruritic, and macular exanthema.18
The pathogenesis of SCARs is still not yet completely understood. Recent studies have found a link between SCARs and genetic biomarkers, particularly genetic variants of human leukocyte antigens (HLA), T cell receptors (TCR), drug-metabolizing enzymes, and drug transporters.19 Commonly, culprit drugs are found to be phenotype- and ethnicity-specific. CBZ is an aromatic and antiepileptic drug and is a common culprit drug in the Chinese population associated with HLA-B*15:02 and HLA-A*31:01 alleles.19,20 HLA screening can be performed to prevent disease in susceptible patients and may help identify additional culprit drugs in the future. However, in our case, these tests could not be performed because of the patient’s poor condition.
In our case, two drugs commonly implicated in DRESS syndrome include levofloxacin, a fluoroquinolone antibiotic that can cause fever, and CBZ, which is used to treat herpes zoster neuralgia.20 There have been various reports of SCARs, especially DRESS syndrome, being caused by antimicrobial agents, including vancomycin, β-lactams, fluoroquinolones, and other antibiotics, while the severity of the cases is controversial.21 It seems that fluoroquinolone-induced SCARs are milder with a shorter latency period and can be controlled a few days after drug discontinuation without any other intervention.21 Another potential contributing factor is the role of viral infection or reactivation in SCARs. Numerous studies demonstrate the reactivation of human herpes virus 6, EBV, and cytomegalovirus, or even sequential reactivation of several of these herpes family viruses associated with both short- and long-term morbidity and mortality.20,22 Consistent with this, our case had a history of varicella zoster virus infection and EBV duplication that may have been implicated in the pathophysiology of her disease.
Although AGEP and DRESS syndrome have different clinical presentations, they have a common T-cell–mediated pathogenesis.23 We assume that this mechanism, together with EBV and herpes virus infection, allowed for the presentation of overlapping features of these two SCARs. The coexistence of AGEP and DRESS syndrome in the same patient is rare as there are few reports of overlapping features in the literature.
Conclusions
We report a case of AGEP overlapping with DRESS syndrome that was aggravated after its initial control, likely caused by the patient’s previous treatment with CBZ and levofloxacin. This case demonstrates the importance of reviewing the complete medication history of patients with suspected SCARs because the culprit drug may have been taken months before admission. It is also important to check the history of drug allergies and virus infections with suspected DRESS syndrome because they may increase the severity of the disease. Early identification of factors involved in the pathogenesis of AGEP and DRESS syndrome is an important step in determining the appropriate management of the patient. Furthermore, identifying different SCARs affecting the patient is also important to help determine the appropriate course of treatment, follow-up, and short- and long-term prognosis.
Abbreviations
SCARs, Severe cutaneous adverse reactions; AGEP, Acute Generalized Exanthematous pustulosis; DRESS, drug reaction with eosinophilia and systemic symptoms; SJS, Stevens-Johnson syndrome; TEN, toxic epidermal necrolysis; CBZ, carbamazepine; HLA, human leukocyte antigens; TCR, T cell receptor; IgE, immunoglobulin E; IVIG, intravenous immunoglobulin; EBV, Epstein-Barr virus; HHV, Human Herpesvirus; CMV, Cytomegalovirus.
Statement of Ethics
The study protocol as a case study was approved by the Beijing Friendship Hospital Ethics Committee for Human Research (2021-P2-047-01). A written informed consent has been provided by the patient to have the case details and the accompanying images published.
Acknowledgment
We gratefully appreciate my patient and her family members made the selfless contribution to provide the clinical picture and her condition to let us published the case so more dermatologists can learn, let wishes her will be well soon. Meifang Wang and Li Lin share the first authorship for this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang J, Lei Z, Xu C, Zhao J, Kang X. Current perspectives on severe drug eruption. Clin Rev Allergy Immunol. 2021;61(3):282–298. doi:10.1007/s12016-021-08859-0
2. Roujeau JC, Stern RS. Severe adverse cutaneous reactions to drugs. N Engl J Med. 1994;331:1272–1285. doi:10.1056/NEJM199411103311906
3. Zheng L, Jin H-B, Guan Y-Y, Yang J. Pharmacovigilance of cutaneous adverse drug reactions in associations with drugs and medical conditions: a retrospective study of hospitalized patients. BMC Pharmacol Toxicol. 2022;23:62. doi:10.1186/s40360-022-00603-4
4. Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP): a review and update. J Am Acad Dermatol. 2015;73(5):843–848. doi:10.1016/j.jaad.2015.07.017
5. Duong TA, Valeyrie-Allanore L, Wolkenstein P, Chosidow O. Severe cutaneous adverse reactions to drugs. Lancet. 2017;390(10106):1996–2011. doi:10.1016/S0140-6736(16)30378-6
6. Kim TI, Jeong KH, Shin MK, Kim NI. Piperacillin/Tazobactam-Associated Hypersensitivity Syndrome with Overlapping Features of Acute Generalized Exanthematous Pustulosis and Drug-Related Rash with Eosinophilia and Systemic Symptoms Syndrome. Ann Dermatol. 2016;28(1):98–101. doi:10.5021/ad.2016.28.1.98
7. Totonchy MB. Koebnerization of Hailey-Hailey disease into a cutaneous drug eruption of acute generalized exanthematous pustulosis associated with systemic symptoms. Case Reports, J Cutan Pathol. 2016;43(11):1031–1035. doi:10.1111/cup.12771
8. Ikeda T, Yokoyama K, Kawakami T. Overlapping acute generalized exanthematous pustulosis drug reaction with eosinophilia and systemic symptoms induced by a second dose of the Moderna COVID- 19 vaccine. J Dermatol. 2022;49(12):e446–e447. doi:10.1111/1346-8138.16541
9. Tay WC, Lee JSS, Chong WS. Tozinameran (Pfizer-BioNTech COVID-19 vaccine)-induced AGEP-DRESS syndrome.Ann. Acad Med Singap. 2022;51(12):796–797. doi:10.47102/annals-acadmedsg.2022338
10. Gey A, Milpied B, Dutriaux C, et al. cutaneous adverse reaction associated with vemurafenib: DRESS, AGEP or overlap reaction? J Eur Acad Dermatol Venereol. 2016;30(1):178–179. doi:10.1111/jdv.12685
11. Tedbirt B, Viart-Commin M-H, Carvalho P, Courville P, Florence T. Severe acute generalized exanthematous pustulosis (AGEP) induced by miconazole oral gel with overlapping features of drug reaction with eosinophilia and systemic symptoms (DRESS). Contact Dermatitis. 2021;84(6):474–476. doi:10.1111/cod.13773
12. Perelló MI, de Maria Castro A, Nogueira Arraes AC. Severe cutaneous adverse drug reactions: diagnostic approach and genetic study in a Brazilian case series. Eur Ann Allergy Clin Immunol. 2022;54(5):207–217. doi:10.23822/EurAnnACI.1764-1489.193
13. Bouvresse S, Valeyrie-Allanore L, Ortonne N, et al. Toxic epidermal necrolysis, DRESS, AGEP: do overlap cases exist? Orphanet J Rare Dis. 2012;25(7):72. doi:10.1186/1750-1172-7-72
14. Shiohara T, Iijima M, Ikezawa Z, Hashimoto K. The diagnosis of a DRESS syndrome has been sufficiently established on the basis of typical clinical features and viral reactivations. Br J Dermatol. 2007;156:1083–1084. doi:10.1111/j.1365-2133.2007.07807.x
15. Sussman M, Napodano A, Huang S, Are A, Hsu S, Motaparthi K. Pustular Psoriasis and Acute Generalized Exanthematous Pustulosis. Medicina. 2021;57(10):1004. doi:10.3390/medicina57101004
16. Sharifzadeh S, Mohammadpour AH, Tavanaee A, Elyasi S. Antibacterial antibiotic-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: a literature review. Eur J Clin Pharmacol. 2021;77(3):275–289. doi:10.1007/s00228-020-03005-9
17. Stirton H, Shear NH, Dodiuk-Gad RP. Drug Reaction with Eosinophilia and Systemic Symptoms (DReSS)/Drug-Induced Hypersensitivity Syndrome (DiHS)—Readdressing the DReSS. Biomedicines. 2022;10(5):999. doi:10.3390/biomedicines10050999
18. Miyagawa F, Asada H. Current Perspective Regarding the Immunopathogenesis of Drug-Induced Hypersensitivity Syndrome/Drug Reaction with Eosinophilia and Systemic Symptoms (DIHS/DRESS).Int. J Mol Sci. 2021;22(4):2147. doi:10.3390/ijms22042147
19. Wang C-W. An Updated Review of Genetic Associations With Severe Adverse Drug Reactions: translation and Implementation of Pharmacogenomic Testing in Clinical Practice. Front Pharmacol. 2022;13:886377. doi:10.3389/fphar.2022.886377
20. Cardones AR. Drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome. Clin Dermatol. 2020;38(6):702–711. doi:10.1016/j.clindermatol.2020.06.008
21. Sharifzadeh S, Mohammadpour AH, Tavanaee A, Elyasi S. Antibacterial antibiotic-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: a literature review. Eur J Clin Pharmacol. 2021;77(3):275–289.
22. Schunkert EM, Divito SJ. Updates and Insights in the Diagnosis and Management of DRESS Syndrome. Curr Dermatol Rep. 2021;10(4):192–204. doi:10.1007/s13671-021-00348-z
23. Mockenhaupt M. Severe drug-induced skin reactions: clinical pattern, diagnostics and therapy. J Dtsch Dermatol Ges. 2009;7(2):142–160. doi:10.1111/j.1610-0387.2008.06878.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.